
Minilaparoscopic Versus Conventional Laparoscopic Hysterectomy: Insights from a Single-Center Retrospective Cohort Study with Legal Considerations

 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
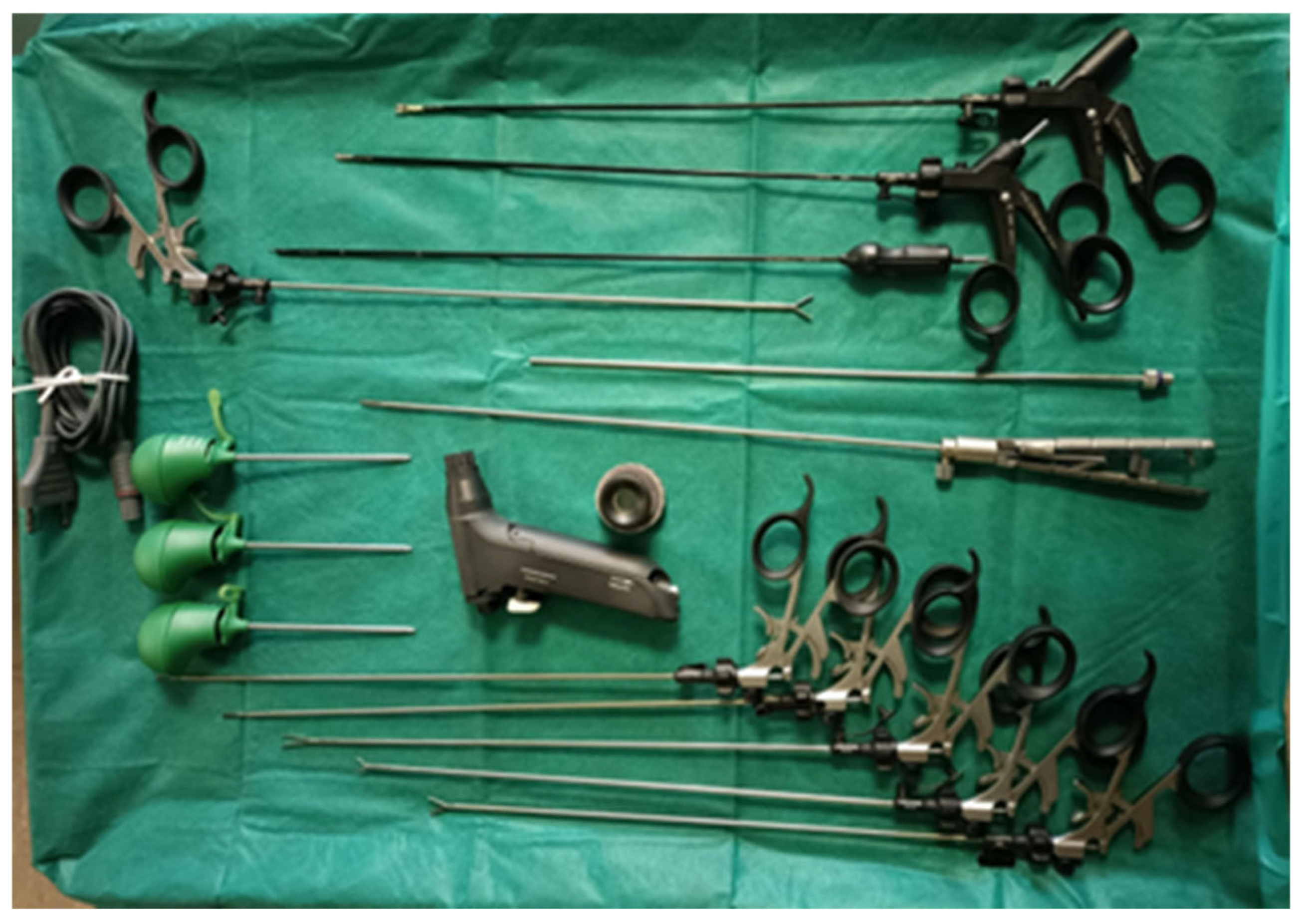
2.2. Operative Technique
2.3. Data Collection
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Committee Opinion No 701: Choosing the Route of Hysterectomy for Benign Disease. Obstet. Gynecol. 2017, 129, e155–e159. [CrossRef] [PubMed]
- Wu, J.M.; Wechter, M.E.; Geller, E.J.; Nguyen, T.V.; Visco, A.G. Hysterectomy Rates in the United States, 2003. Obstet. Gynecol. 2007, 110, 1091–1095. [Google Scholar] [CrossRef] [PubMed]
- Nieboer, T.E.; Johnson, N.; Lethaby, A.; Tavender, E.; Curr, E.; Garry, R.; van Voorst, S.; Mol, B.W.J.; Kluivers, K.B. Surgical Approach to Hysterectomy for Benign Gynaecological Disease. Cochrane Database Syst. Rev. 2009, CD003677. [Google Scholar] [CrossRef]
- Giannini, A.; D’Oria, O.; Bogani, G.; Di Donato, V.; Vizza, E.; Chiantera, V.; Laganà, A.S.; Muzii, L.; Salerno, M.G.; Caserta, D.; et al. Hysterectomy: Let’s Step Up the Ladder of Evidence to Look Over the Horizon. J. Clin. Med. 2022, 11, 6940. [Google Scholar] [CrossRef]
- Paraiso, M.F.R.; Ridgeway, B.; Park, A.J.; Jelovsek, J.E.; Barber, M.D.; Falcone, T.; Einarsson, J.I. A Randomized Trial Comparing Conventional and Robotically Assisted Total Laparoscopic Hysterectomy. Am. J. Obstet. Gynecol. 2013, 208, 368.e1–368.e7. [Google Scholar] [CrossRef]
- Cianci, S.; Perrone, E.; Rossitto, C.; Fanfani, F.; Tropea, A.; Biondi, A.; Scambia, G.; Gueli Alletti, S. Percutaneous-Assisted vs Mini-Laparoscopic Hysterectomy: Comparison of Ultra-Minimally Invasive Approaches. Updates Surg. 2021, 73, 2347–2354. [Google Scholar] [CrossRef]
- Rossitto, C.; Cianci, S.; Gueli Alletti, S.; Perrone, E.; Pizzacalla, S.; Scambia, G. Laparoscopic, Minilaparoscopic, Single-Port and Percutaneous Hysterectomy: Comparison of Perioperative Outcomes of Minimally Invasive Approaches in Gynecologic Surgery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 216, 125–129. [Google Scholar] [CrossRef]
- Ghezzi, F.; Cromi, A.; Siesto, G.; Uccella, S.; Boni, L.; Serati, M.; Bolis, P. Minilaparoscopic versus Conventional Laparoscopic Hysterectomy: Results of a Randomized Trial. J. Minim. Invasive Gynecol. 2011, 18, 455–461. [Google Scholar] [CrossRef]
- Delgado-Sánchez, E.; Fanfani, F.; Malzoni, M.; Couso, A.; Zapico, Á.; Bogliolo, S.; Sánchez-Torres, D.A.; Gardella, B.; Thuissard-Vasallo, I.J.; Zapardiel, I. Laparoscopic Single-Port versus Mini-Laparoscopic Hysterectomy: An International Study. Gynecol. Obstet. Investig. 2022, 87, 381–388. [Google Scholar] [CrossRef]
- Gallotta, V.; Nero, C.; Chiantera, V.; Scambia, G. Minilaparoscopic Aortic Lymphadenectomy. J. Minim. Invasive Gynecol. 2015, 22, 546–547. [Google Scholar] [CrossRef]
- Ghezzi, F.; Cromi, A.; Colombo, G.; Uccella, S.; Bergamini, V.; Serati, M.; Bolis, P. Minimizing Ancillary Ports Size in Gynecologic Laparoscopy: A Randomized Trial. J. Minim. Invasive Gynecol. 2005, 12, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Bruhat, M.A.; Goldchmit, R. Minilaparoscopy in Gynecology. Eur. J. Obstet. Gynecol. Reprod. Biol. 1998, 76, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Fanfani, F.; Fagotti, A.; Gagliardi, M.L.; Monterossi, G.; Rossitto, C.; Costantini, B.; Gueli Alletti, S.; Vizzielli, G.; Ercoli, A.; Scambia, G. Minilaparoscopic versus Single-Port Total Hysterectomy: A Randomized Trial. J. Minim. Invasive Gynecol. 2013, 20, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, F.; Fanfani, F.; Malzoni, M.; Uccella, S.; Fagotti, A.; Cosentino, F.; Cromi, A.; Scambia, G. Minilaparoscopic Radical Hysterectomy for Cervical Cancer: Multi-Institutional Experience in Comparison with Conventional Laparoscopy. Eur. J. Surg. Oncol. 2013, 39, 1094–1100. [Google Scholar] [CrossRef]
- Wattiez, A.; Goldchmit, R.; Durruty, G.; Mage, G.; Canis, M.; Cucinella, G.; Pouly, J.L.; Bruhat, M.A. Minilaparoscopic Hysterectomy. J. Am. Assoc. Gynecol. Laparosc. 1999, 6, 97–100. [Google Scholar] [CrossRef]
- Ghezzi, F.; Marconi, N.; Casarin, J.; Cromi, A.; Serati, M.; Uccella, S. Minilaparoscopic Myomectomy with Trans-Vaginal Specimen Extraction: A Case Report. J. Obstet. Gynaecol. 2017, 37, 960–962. [Google Scholar] [CrossRef]
- Simion, L.; Chitoran, E.; Cirimbei, C.; Stefan, D.-C.; Neicu, A.; Tanase, B.; Ionescu, S.O.; Luca, D.C.; Gales, L.; Gheorghe, A.S.; et al. A Decade of Therapeutic Challenges in Synchronous Gynecological Cancers from the Bucharest Oncological Institute. Diagnostics 2023, 13, 2069. [Google Scholar] [CrossRef]
- Ghezzi, F.; Serati, M.; Casarin, J.; Uccella, S. Minilaparoscopic Single-Site Total Hysterectomy. Obstet. Gynecol. 2015, 126, 151–154. [Google Scholar] [CrossRef]
- Piergentili, R.; Gullo, G.; Basile, G.; Gulia, C.; Porrello, A.; Cucinella, G.; Marinelli, E.; Zaami, S. Circulating miRNAs as a Tool for Early Diagnosis of Endometrial Cancer-Implications for the Fertility-Sparing Process: Clinical, Biological, and Legal Aspects. Int. J. Mol. Sci. 2023, 24, 11356. [Google Scholar] [CrossRef]
- Cucinella, G.; Gullo, G.; Catania, E.; Perino, A.; Billone, V.; Marinelli, S.; Napoletano, G.; Zaami, S. Stem Cells and Infertility: A Review of Clinical Applications and Legal Frameworks. J. Pers. Med. 2024, 14, 135. [Google Scholar] [CrossRef]
- Gullo, G.; Cucinella, G.; Chiantera, V.; Dellino, M.; Cascardi, E.; Török, P.; Herman, T.; Garzon, S.; Uccella, S.; Laganà, A.S. Fertility-Sparing Strategies for Early-Stage Endometrial Cancer: Stepping towards Precision Medicine Based on the Molecular Fingerprint. Int. J. Mol. Sci. 2023, 24, 811. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Park, S.; Kim, S.H. Supporting Decision-Making Regarding Fertility Preservation in Patients with Cancer: An Integrative Review. Eur. J. Cancer Care 2022, 31, e13748. [Google Scholar] [CrossRef] [PubMed]
- Zaami, S.; Stark, M.; Signore, F.; Gullo, G.; Marinelli, E. Fertility Preservation in Female Cancer Sufferers: (Only) a Moral Obligation? Eur. J. Contracept. Reprod. Health Care 2022, 27, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, L.; Manavella, D.D.; Gullo, G.; McNamara, B.; Santin, A.D.; Patrizio, P. Endometrial Cancer in Reproductive Age: Fertility-Sparing Approach and Reproductive Outcomes. Cancers 2022, 14, 5187. [Google Scholar] [CrossRef]
- Chitoran, E.; Rotaru, V.; Mitroiu, M.-N.; Durdu, C.-E.; Bohiltea, R.-E.; Ionescu, S.-O.; Gelal, A.; Cirimbei, C.; Alecu, M.; Simion, L. Navigating Fertility Preservation Options in Gynecological Cancers: A Comprehensive Review. Cancers 2024, 16, 2214. [Google Scholar] [CrossRef]
- Danoff, J.R.; Goel, R.; Sutton, R.; Maltenfort, M.G.; Austin, M.S. How Much Pain Is Significant? Defining the Minimal Clinically Important Difference for the Visual Analog Scale for Pain After Total Joint Arthroplasty. J. Arthroplast. 2018, 33, e2. [Google Scholar] [CrossRef]
- Timerbulatov, V.M.; Timerbulatov, S.V.; Timerbulatov, M.V. Classification of surgical complications. Khirurgiia 2018, 62–67. [Google Scholar] [CrossRef]
- Chaykin, A.A.; Chaykin, D.A.; Chaykin, A.N.; Vinnik, Y.S.; Teplyakova, O.V.; Beloborodov, A.A.; Ilinov, A.V. Short-term outcomes of mechanical and hand-sewn laparoscopic one-anastomosis mini-gastric bypass. Khirurgiia 2024, 29–37. [Google Scholar] [CrossRef]
- Fagotti, A.; Boruta, D.M.; Scambia, G.; Fanfani, F.; Paglia, A.; Escobar, P.F. First 100 Early Endometrial Cancer Cases Treated with Laparoendoscopic Single-Site Surgery: A Multicentric Retrospective Study. Am. J. Obstet. Gynecol. 2012, 206, 353.e1–353.e6. [Google Scholar] [CrossRef]
- Ghezzi, F.; Cromi, A.; Fasola, M.; Bolis, P. One-Trocar Salpingectomy for the Treatment of Tubal Pregnancy: A “marionette-like” Technique. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 1417–1419. [Google Scholar] [CrossRef]
- Fanfani, F.; Monterossi, G.; Fagotti, A.; Scambia, G. Laparoendoscopic Single-Site Hysterectomy: Is It Safe and Feasible? Curr. Opin. Obstet. Gynecol. 2014, 26, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, F.; Cromi, A.; Ciravolo, G.; Rampinelli, F.; Braga, M.; Boni, L. A New Laparoscopic-Transvaginal Technique for Rectosigmoid Resection in Patients with Endometriosis. Fertil. Steril. 2008, 90, 1964–1968. [Google Scholar] [CrossRef] [PubMed]
- Casarin, J.; Cimmino, C.; Artuso, V.; Cromi, A.; Ghezzi, F. Minilaparoscopy in Gynecology: Applications, Benefits and Limitations. Minerva Obstet. Gynecol. 2021, 73, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, F.; Casarin, J.; Uccella, S. Mini-Laparoscopic Sentinel Node Detection in Endometrial Cancer: Further Reducing Invasiveness for Patients with Early-Stage Disease. Ann. Surg. Oncol. 2015, 22, S342. [Google Scholar] [CrossRef]
- Porpiglia, F.; Morra, I.; Bertolo, R.; Manfredi, M.; Mele, F.; Fiori, C. Pure Mini-Laparoscopic Transperitoneal Pyeloplasty in an Adult Population: Feasibility, Safety, and Functional Results after One Year of Follow-Up. Urology 2012, 79, 728–732. [Google Scholar] [CrossRef]
- Krpata, D.M.; Ponsky, T.A. Needlescopic Surgery: What’s in the Toolbox? Surg. Endosc. 2013, 27, 1040–1044. [Google Scholar] [CrossRef]
- Sajid, M.S.; Khan, M.A.; Ray, K.; Cheek, E.; Baig, M.K. Needlescopic versus Laparoscopic Cholecystectomy: A Meta-Analysis. ANZ J. Surg. 2009, 79, 437–442. [Google Scholar] [CrossRef]
- Kadar, N.; Reich, H.; Liu, C.Y.; Manko, G.F.; Gimpelson, R. Incisional Hernias after Major Laparoscopic Gynecologic Procedures. Am. J. Obstet. Gynecol. 1993, 168, 1493–1495. [Google Scholar] [CrossRef]
- Tica, V.I.; Tica, A.A.; De Wilde, R.L. The Future in Standards of Care for Gynecologic Laparoscopic Surgery to Improve Training and Education. J. Clin. Med. 2022, 11, 2192. [Google Scholar] [CrossRef]
- Ghezzi, F.; Cromi, A.; Uccella, S.; Bogani, G.; Sturla, D.; Serati, M.; Bolis, P. Nerve-Sparing Minilaparoscopic versus Conventional Laparoscopic Radical Hysterectomy plus Systematic Pelvic Lymphadenectomy in Cervical Cancer Patients. Surg. Innov. 2013, 20, 493–501. [Google Scholar] [CrossRef]
- Rai, R.; Roy, K.K.; Nair, V.; Kachhawa, G.; Zangmo, R.; Garg, D.; Vanamail, P. Feasibility and Efficacy of Modern Minilaparoscopy with 2.9 Mm Laparoscope for Diagnostic and Level II Gynaecological Procedure. Obstet. Gynecol. Sci. 2021, 64, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Bisgaard, T.; Klarskov, B.; Trap, R.; Kehlet, H.; Rosenberg, J. Microlaparoscopic vs Conventional Laparoscopic Cholecystectomy: A Prospective Randomized Double-Blind Trial. Surg. Endosc. 2002, 16, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, F.; Cromi, A.; Siesto, G.; Zefiro, F.; Franchi, M.; Bolis, P. Microlaparoscopy: A Further Development of Minimally Invasive Surgery for Endometrial Cancer Staging—Initial Experience. Gynecol. Oncol. 2009, 113, 170–175. [Google Scholar] [CrossRef]
- Total Microlaparoscopic Radical Hysterectomy in Early Cervical Cancer–PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/23743381/ (accessed on 18 December 2024).
- Leggett, P.L.; Churchman-Winn, R.; Miller, G. Minimizing Ports to Improve Laparoscopic Cholecystectomy. Surg. Endosc. 2000, 14, 32–36. [Google Scholar] [CrossRef]
- Novitsky, Y.W.; Kercher, K.W.; Czerniach, D.R.; Kaban, G.K.; Khera, S.; Gallagher-Dorval, K.A.; Callery, M.P.; Litwin, D.E.M.; Kelly, J.J. Advantages of Mini-Laparoscopic vs Conventional Laparoscopic Cholecystectomy: Results of a Prospective Randomized Trial. Arch. Surg. 2005, 140, 1178–1183. [Google Scholar] [CrossRef]
- Cheah, W.K.; Lenzi, J.E.; So, J.B.; Kum, C.K.; Goh, P.M. Randomized Trial of Needlescopic versus Laparoscopic Cholecystectomy. Br. J. Surg. 2001, 88, 45–47. [Google Scholar] [CrossRef]
- Lau, D.H.W.; Yau, K.K.K.; Chung, C.C.; Leung, F.C.S.; Tai, Y.P.; Li, M.K.W. Comparison of Needlescopic Appendectomy versus Conventional Laparoscopic Appendectomy: A Randomized Controlled Trial. Surg. Laparosc. Endosc. Percutan Tech. 2005, 15, 75–79. [Google Scholar] [CrossRef]
- Medical Malpractice–I principali Rischi per le Aziende Sanitarie. Available online: https://www.marsh.com/content/marsh2/europe/it/it_it/industries/healthcare/insights/medmal-report.html (accessed on 6 December 2023).
- Harper Macleod LLP. Successful Claim in Medical Negligence Case Related to Hysterectomy. Available online: https://www.harpermacleod.co.uk/insights/successful-claim-in-medical-negligence-case-related-to-hysterectomy/ (accessed on 18 December 2024).
- Albolino, S.; Bellandi, T.; Cappelletti, S.; Di Paolo, M.; Fineschi, V.; Frati, P.; Offidani, C.; Tanzini, M.; Tartaglia, R.; Turillazzi, E. New Rules on Patient’s Safety and Professional Liability for the Italian Health Service. Curr. Pharm. Biotechnol. 2019, 20, 615–624. [Google Scholar] [CrossRef]
- Giannini, A.; Di Donato, V.; Schiavi, M.C.; May, J.; Panici, P.B.; Congiu, M.A. Predictors of Postoperative Overall and Severe Complications after Surgical Treatment for Endometrial Cancer: The Role of the Fragility Index. Int. J. Gynaecol. Obstet. 2020, 148, 174–180. [Google Scholar] [CrossRef]
- Barr, C.E.; Crosbie, E.J. The Mirena Coil Is a Suitable Treatment of Early-Stage Endometrial Cancer in Obese Women: FOR: Careful Selection and Monitoring Is Key. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 1001. [Google Scholar] [CrossRef]
- Kreisman, R. $1.5 Million Settlement in Negligent Laparoscopic Hysterectomy. Available online: https://www.robertkreisman.com/medical-malpractice-lawyer/1-5-million-settlement-in-negligent-laparoscopic-hysterectomy/ (accessed on 18 December 2024).
- Napoletano, G.; Paola, L.D.; Circosta, F.; Vergallo, G.M. Right to Be Forgotten: European Instruments to Protect the Rights of Cancer Survivors. Acta Biomed. Atenei Parm. 2024, 95, e2024114. [Google Scholar] [CrossRef]
- Cavaliere, A.F.; Perelli, F.; Zaami, S.; Piergentili, R.; Mattei, A.; Vizzielli, G.; Scambia, G.; Straface, G.; Restaino, S.; Signore, F. Towards Personalized Medicine: Non-Coding RNAs and Endometrial Cancer. Healthcare 2021, 9, 965. [Google Scholar] [CrossRef] [PubMed]
- Salari, P.; Larijani, B. Ethical Issues Surrounding Personalized Medicine: A Literature Review. Acta Med. Iran. 2017, 55, 209–217. [Google Scholar] [PubMed]
- Santurro, A.; Vullo, A.M.; Borro, M.; Gentile, G.; La Russa, R.; Simmaco, M.; Frati, P.; Fineschi, V. Personalized Medicine Applied to Forensic Sciences: New Advances and Perspectives for a Tailored Forensic Approach. Curr. Pharm. Biotechnol. 2017, 18, 263–273. [Google Scholar] [CrossRef]
- Chen, M.; Kong, W.; Li, B.; Tian, Z.; Yin, C.; Zhang, M.; Pan, H.; Bai, W. Revolutionizing Hysteroscopy Outcomes: AI-Powered Uterine Myoma Diagnosis Algorithm Shortens Operation Time and Reduces Blood Loss. Front. Oncol. 2023, 13, 1325179. [Google Scholar] [CrossRef]
- Marinelli, S.; De Paola, L.; Stark, M.; Montanari Vergallo, G. Artificial Intelligence in the Service of Medicine: Current Solutions and Future Perspectives, Opportunities, and Challenges. Clin. Ter. 2025, 176, 77–82. [Google Scholar] [CrossRef]
- Ferrara, M.; Bertozzi, G.; Di Fazio, N.; Aquila, I.; Di Fazio, A.; Maiese, A.; Volonnino, G.; Frati, P.; La Russa, R. Risk Management and Patient Safety in the Artificial Intelligence Era: A Systematic Review. Healthcare 2024, 12, 549. [Google Scholar] [CrossRef]
- Marinelli, S.; Basile, G.; De Paola, L.; Napoletano, G.; Zaami, S. Consequences of COVID-19 Restrictions on Adolescent Mental Health and Drug Abuse Dynamics. Eur. Rev. Med. Pharmacol. Sci. 2024, 28, 836–851. [Google Scholar]
- La Rosa, V.L.; Valenti, G.; Sapia, F.; Gullo, G.; Rapisarda, A. Psychological Impact of Gynecological Diseases: The Importance of a Multidisciplinary Approach. Ital. J. Gynaecol. Obstet. 2018, 30, 23–26. [Google Scholar] [CrossRef]
- Giannini, A.; D’Oria, O.; Vizza, E.; Congiu, M.A.; Cuccu, I.; Golia D’Augè, T.; Saponara, S.; Capalbo, G.; Di Donato, V.; Raspagliesi, F.; et al. Robotic-Assisted, Laparoscopic, and Vaginal Hysterectomy in Morbidly Obese Patients with Endometrial Hyperplasia and Endometrial Cancer. Minim. Invasive Ther. Allied Technol. 2024, 33, 358–364. [Google Scholar] [CrossRef]
- Buzzaccarini, G.; Török, P.; Vitagliano, A.; Petousis, S.; Noventa, M.; Hortu, I.; Giannin, A.; Laganà, A.S. Predictors of Pain Development after Laparoscopic Adnexectomy: A Still Open Challenge. J. Investig. Surg. 2022, 35, 1392–1393. [Google Scholar] [CrossRef] [PubMed]
- Lenfant, L.; Canlorbe, G.; Belghiti, J.; Kreaden, U.S.; Hebert, A.E.; Nikpayam, M.; Uzan, C.; Azaïs, H. Robotic-Assisted Benign Hysterectomy Compared with Laparoscopic, Vaginal, and Open Surgery: A Systematic Review and Meta-Analysis. J. Robot. Surg. 2023, 17, 2647–2662. [Google Scholar] [CrossRef] [PubMed]
- Bartels, H.C.; Rogers, A.C.; Janda, M.; Obermair, A.; Brennan, D.J. Quality of Life Following Minimally Invasive Hysterectomy Compared to Abdominal Hysterectomy: A Metanalysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 252, 206–212. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| LH Group (n = 153) | MLH Group (n = 155) | p-Value | |
|---|---|---|---|
| Age (mean ± SD) | 50.0 (±0.6) | 49.5 (±0.6) | n.s. * |
| BMI(mean ± SD) | 27.1 (±0.5) | 28.5 (±0.4) | <0.05 |
| Menopause (%) | 79.7 | 46.5 | <0.0001 |
| Parity (mean ± SD) | 2.1 (±0.1) | 2.0 (±0.1) | n.s. * |
| Previous caesarian section (%) | 55.6 | 22.6 | <0.0001 |
| Previous abdominal surgery (%) | 20.9 | 45.8 | <0.0001 |
| Surgical Outcomes | LH Group | MLH Group | Coeff. (MLH vs. LH) * | Std. Error | t | p-Value | Adj R2 | CI95% Lower Lim. | CI95% Upper Lim. |
|---|---|---|---|---|---|---|---|---|---|
| Surgery duration (mean ± SD) | 105.5 min (±1.2) | 98.8 min (±1.1) | −6.7 | 1.835 | −3.65 | <0.0001 | 0.0395 | −10.3 | −3.1 |
| Blood loss (mean ± SD) | 195.1 (±5.1) | 100.3 (±4.0) | −94.2 | 7.095 | −13.28 | <0.0001 | 0.4049 | −108.2 | −80.2 |
| Length of hospital stay (mean ± SD) | 4.0 (±0.1) | 3.2 (±0.1) | −0.9 | 0.089 | −9.72 | <0.0001 | 0.2518 | −1.0 | −0.7 |
| VAS score at 6 h (mean ± SD) | 7.0 (±0.06) | 7.9 (±0.06) | 0.9 | 0.086 | 10.75 | <0.0001 | 0.2915 | 0.8 | 1.1 |
| VAS score at 12 h (mean ± SD) | 6.0 (±0.04) | 5.5 (±0.06) | −0.5 | 0.087 | −5.67 | <0.0001 | 0.1198 | −0.7 | −0.3 |
| VAS score at 24 h (mean ± SD) | 4.2 (±0.04) | 4.1 (±0.03) | −0.09 | 0.054 | −1.55 | >0.10 | 0.0054 | −0.19 | +0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Billone, V.; Gullo, G.; Conti, E.; Ganduscio, S.; Burgio, S.; Baglio, G.; Cucinella, G.; De Paola, L.; Marinelli, S. Minilaparoscopic Versus Conventional Laparoscopic Hysterectomy: Insights from a Single-Center Retrospective Cohort Study with Legal Considerations. Medicina 2025, 61, 1216. https://doi.org/10.3390/medicina61071216
Billone V, Gullo G, Conti E, Ganduscio S, Burgio S, Baglio G, Cucinella G, De Paola L, Marinelli S. Minilaparoscopic Versus Conventional Laparoscopic Hysterectomy: Insights from a Single-Center Retrospective Cohort Study with Legal Considerations. Medicina. 2025; 61(7):1216. https://doi.org/10.3390/medicina61071216
Chicago/Turabian StyleBillone, Valentina, Giuseppe Gullo, Eleonora Conti, Silvia Ganduscio, Sofia Burgio, Giovanni Baglio, Gaspare Cucinella, Lina De Paola, and Susanna Marinelli. 2025. "Minilaparoscopic Versus Conventional Laparoscopic Hysterectomy: Insights from a Single-Center Retrospective Cohort Study with Legal Considerations" Medicina 61, no. 7: 1216. https://doi.org/10.3390/medicina61071216
APA StyleBillone, V., Gullo, G., Conti, E., Ganduscio, S., Burgio, S., Baglio, G., Cucinella, G., De Paola, L., & Marinelli, S. (2025). Minilaparoscopic Versus Conventional Laparoscopic Hysterectomy: Insights from a Single-Center Retrospective Cohort Study with Legal Considerations. Medicina, 61(7), 1216. https://doi.org/10.3390/medicina61071216