
Anterolateral Ligament Reconstruction Combined with Anterior Cruciate Ligament Reconstruction: Clinical and Functional Outcomes

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Technique
2.2. Biomechanical Test
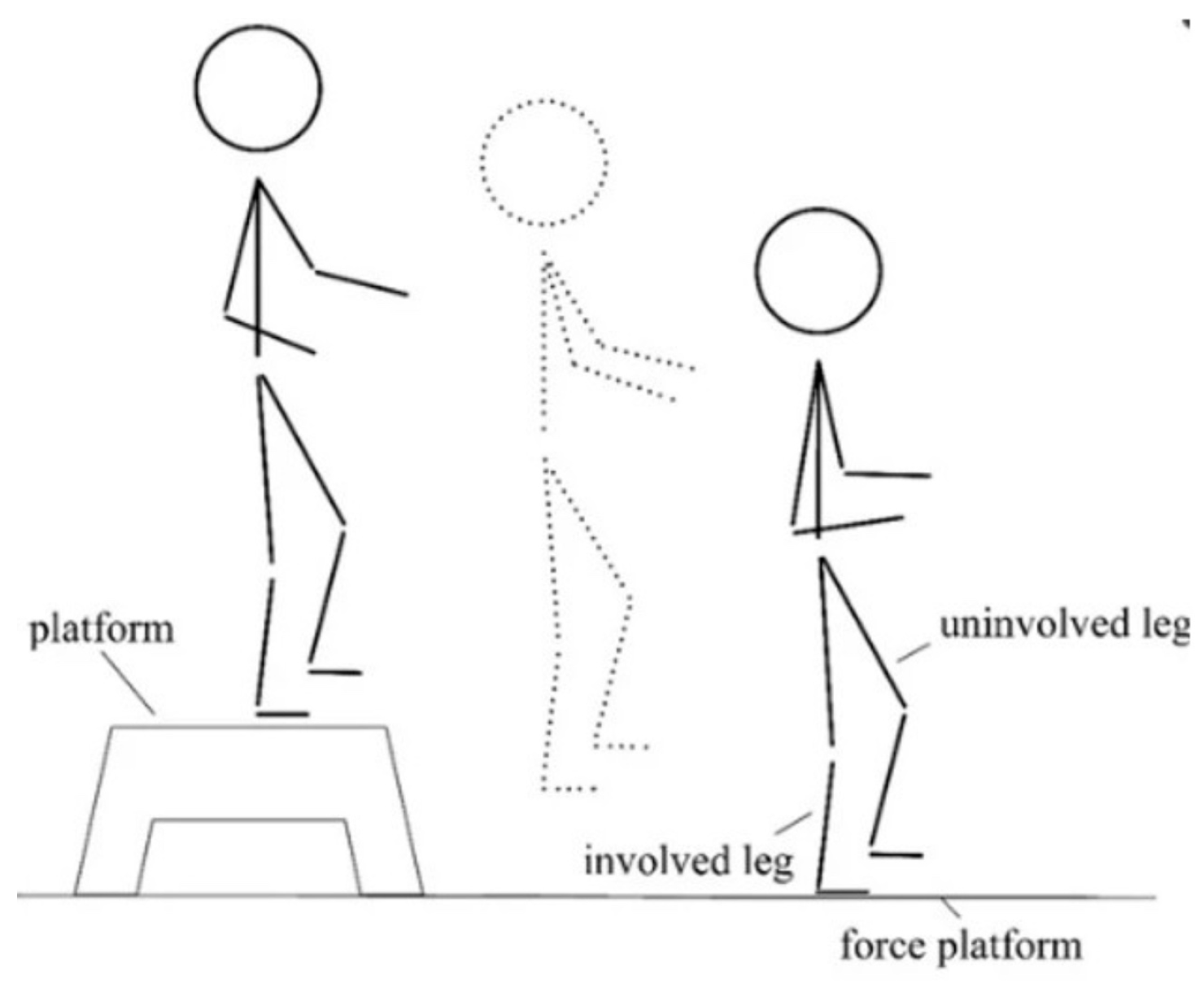
- Unilateral Drop Jump (Figure 1) [17] in which the subject stands on a 30 cm high platform. At the therapist’s start, the subject had to drop, with one limb, onto the force platform in front of the step, stabilize, and remain there until the therapist’s stop warning. This test assesses the strength of the lower limbs (performed first with the healthy limb and then with the limb undergoing surgery).
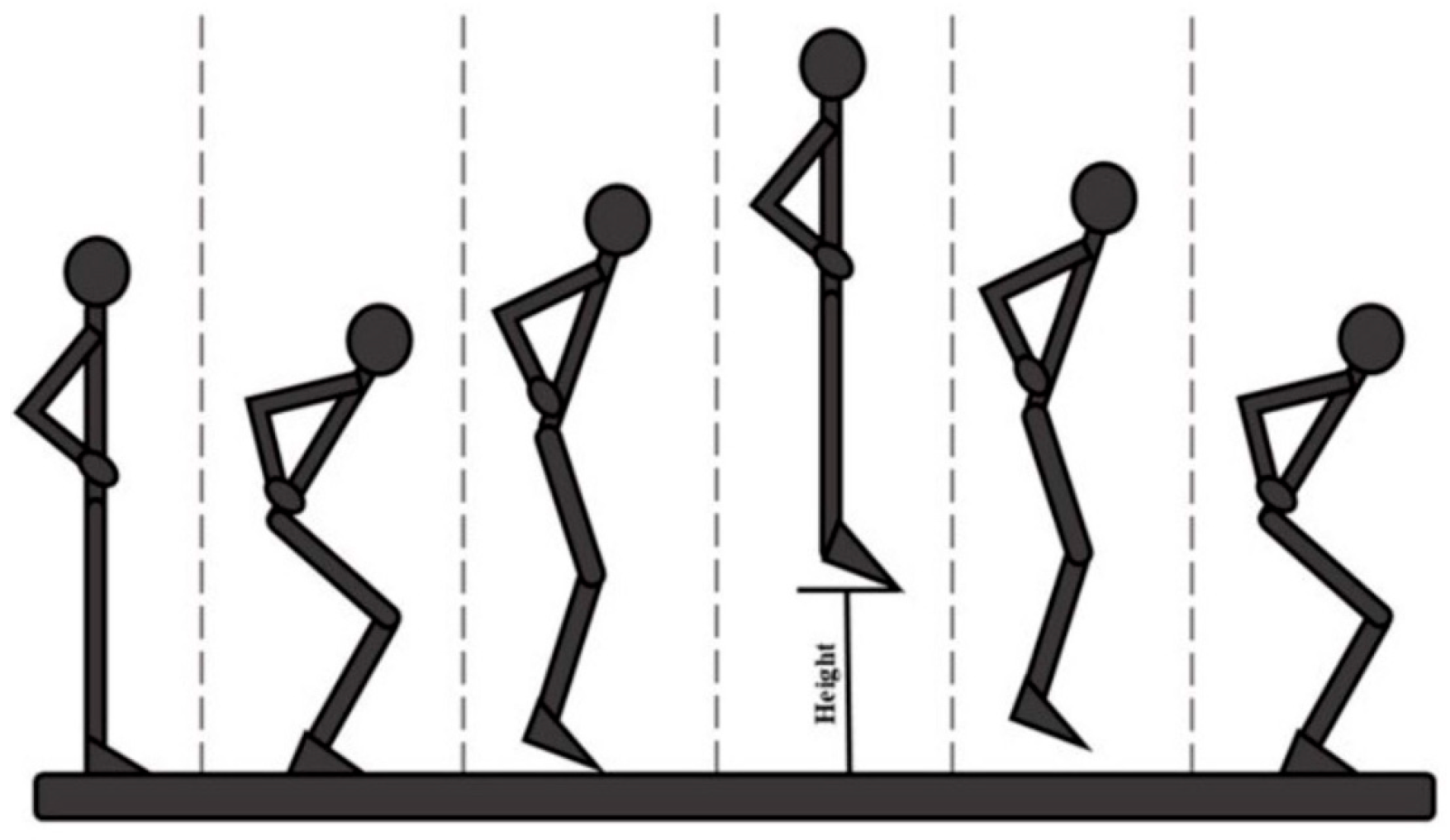
- Countermovement Jump (Figure 2) [18] with the change in knee direction: this consists of a jump squat performed from a standing position, with both feet positioned on the force platforms. At the end of the traditional exercise, our protocol included the execution of an internal rotation of the knee so that the foot is rotated approximately 90° from its natural position (performed first with the healthy limb and then with the operated limb).
- The five-repetition Sit-To-Stand (5-STS) test is a widely used clinical assessment for detecting motor problems [19]. The subject had to stand up and sit down from the chair five times, starting from a seated position with arms crossed over the chest so that only the lower limbs were used to perform the movement.
2.3. Biomechanical Data Processing
- From the sEMG data the duration of muscle activation (preATT_OVL_o, preATT_HVL_o, preATT_OVM_o, preATT_HVM_o, preATT_OVL_h, preATT_HVL_h, prerATT_OVM_h, preATT_HVM_h) and the maximum envelope (env_OVL_o, env_HVL_o, env_OVM_o, env_HVM_o, env_OVL_h, env_HVL_h, env_OVM_h, env_HVM_h) during the entire exercise for the 4 muscles, for a total of 16 muscle variables. To better understand the significance of the variables, it is specified that “O” or “H” refers to the muscle of the operated limb (O) or the contralateral (healthy) limb (H);
- From the kinetic data obtained from the force platforms, the vertical force peak (VGRF_o, VGRF_h), the number of vertical force peaks recorded at landing (NPTS_Fy_o, NPTS_FY_h), the off-axis parameter [25] indicating how much of the vertical component of the force was distributed over the horizontal and transverse component to stabilize the landing (Off-axis_x_o, Off-axis_z_o, Off-axis_x_h, Off-axis_z_h) were obtained for a total of 8 variables;
- From the video analysis, the range of motion [26] (ROM_o, ROM_h) of the knee joint was extracted using videos obtained during the execution of the task performed.
- From the processing of the electromyographic signal, the envelope peak (peak_envOVL_1o, peak_envOVL_2o, peak_envHVL_1o, peak_envHVL_2o, peak_envOVM_1o, peak_envOVM_2o, peak_envHVM_1o, peak_envHVM_2o, peak_envOVL_1h, peak_envOVL_2h, peak_envHVL_1h, peak_envHVL_2h, peak_envOVM_1h, peak_envOVM_2h, peak_envHVM_1h, peak_envHVM_2h) and the duration of muscular activation (onset_OVL_1o, onset_OVL_2o, onset_HVL_1o, onset_HVL_2o, onset_OVM_1o, onset_OVM_2o, onset_HVM_1o, onset_HVM_2o, onset_OVL_1h, onset_OVL_2h, onset_HVL_1h, onset_HVL_2h, onset_OVM_1h, onset_OVM_2h, onset_HVM_1h, onset_HVM_2h) were calculated during each phase of the task for the 4 muscles, listed above, resulting in 32 variables. The letters “O” or “H” refer to the muscle of the operated limb (O) or the contralateral (healthy) limb (H);
- From a kinetic point of view, the vertical force peak (GRF_1o, GRF_2o, GRF_1o, GRF_2o) was derived, resulting in 4 variables.
- From the analysis of the electromyographic signal, the peak of the envelope (max_env_OVL, max_env_HVL, max_env_OVM, max_env_HVM) and the duration of muscle activation during exercise (att_OVL, att_HVL, att_OVM, att_HVM) were extracted for a total of 8 features. The letters “O” or “H” refer to the muscle of the operated limb (O) or the contralateral (healthy) limb (H).
- The analysis of the force exchanged with the ground made it possible to obtain the duration of the entire exercise (duration_STS), the average duration of the lift–seat cycles (dur_cycles_mean), the peak vertical force (peak_F_rise) for the ascent phase alone, the time required to reach this peak (t_peak), and the average vertical force during each cycle (mean_F_rise) for the ascent phase alone for a total of 5 variables.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tavlo, M.; Eljaja, S.; Jensen, J.T.; Siersma, V.D.; Krogsgaard, M.R. The role of the anterolateral ligament in ACL insufficient and reconstructed knees on rotatory stability: A biomechanical study on human cadavers. Scand. J. Med. Sci. Sports 2016, 26, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Monaco, E.; Ferretti, A.; Labianca, L.; Maestri, B.; Speranza, A.; Kelly, M.J.; D’Arrigo, C. Navigated knee kinematics after cutting of the ACL and its secondary restraint. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Sonnery-Cottet, B.; Daggett, M.; Fayard, J.M.; Ferretti, A.; Helito, C.P.; Lind, M.; Monaco, E.; de Pádua, V.B.C.; Thaunat, M.; Wilson, A.; et al. Anterolateral Ligament Expert Group consensus paper on the management of internal rotation and instability of the anterior cruciate ligament—Deficient knee. J. Orthop. Traumatol. 2017, 18, 91–106. [Google Scholar] [CrossRef]
- Claes, S.; Vereecke, E.; Maes, M.; Victor, J.; Verdonk, P.; Bellemans, J. Anatomy of the anterolateral ligament of the knee. J. Anat. 2013, 223, 321–328. [Google Scholar] [CrossRef]
- Vincent, J.P.; Magnussen, R.A.; Gezmez, F.; Uguen, A.; Jacobi, M.; Weppe, F.; Al-Saati, M.F.; Lustig, S.; Demey, G.; Servien, E.; et al. The anterolateral ligament of the human knee: An anatomic and histologic study. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Helito, C.P.; Helito, P.V.; Bonadio, M.B.; Pécora, J.R.; Bordalo-Rodrigues, M.; Camanho, G.L.; Demange, M.K. Correlation of magnetic resonance imaging with knee anterolateral ligament anatomy: A cadaveric study. Orthop. J. Sports Med. 2015, 3, 2325967115621024. [Google Scholar] [CrossRef]
- Monaco, E.; Fabbri, M.; Mazza, D.; Daggett, M.; Redler, A.; Lanzetti, R.M.; De Carli, A.; Ferretti, A. The effect of sequential tearing of the anterior cruciate and anterolateral ligament on anterior translation and the pivot-shift phenomenon: A cadaveric study using navigation. Arthroscopy 2018, 34, 1009–1014. [Google Scholar] [CrossRef]
- Sonnery-Cottet, B.; Haidar, I.; Rayes, J.; Fradin, T.; Ngbilo, C.; Vieira, T.D.; Freychet, B.; Ouanezar, H.; Saithna, A. Long-term graft rupture rates after combined ACL and anterolateral ligament reconstruction versus isolated ACL reconstruction: A matched-pair analysis from the SANTI study group. Am. J. Sports Med. 2021, 49, 2889–2897. [Google Scholar] [CrossRef]
- Chahla, J.; Menge, T.J.; Mitchell, J.J.; Dean, C.S.; LaPrade, R.F. Anterolateral ligament reconstruction technique: An anatomic-based approach. Arthrosc. Tech. 2016, 5, e453–e457. [Google Scholar] [CrossRef]
- Green, D.W.; Hidalgo Perea, S.; Brusalis, C.M.; Chipman, D.E.; Asaro, L.A.; Cordasco, F.A. A modified Lemaire lateral extra-articular tenodesis in high-risk adolescents undergoing anterior cruciate ligament reconstruction with quadriceps tendon autograft: 2-year clinical outcomes. Am. J. Sports Med. 2023, 51, 1441–1446. [Google Scholar] [CrossRef]
- Helito, C.P.; Bonadio, M.B.; Gobbi, R.G.; da Mota e Albuquerque, R.F.; Pécora, J.R.; Camanho, G.L.; Demange, M.K. Combined intra- and extra-articular reconstruction of the anterior cruciate ligament: The reconstruction of the knee anterolateral ligament. Arthrosc. Tech. 2015, 4, e239–e244. [Google Scholar] [CrossRef] [PubMed]
- Sonnery-Cottet, B.; Barbosa, N.C.; Tuteja, S.; Daggett, M.; Kajetanek, C.; Thaunat, M. Minimally invasive anterolateral ligament reconstruction in the setting of anterior cruciate ligament injury. Arthrosc. Tech. 2016, 5, e211–e215. [Google Scholar] [CrossRef] [PubMed]
- Devitt, B.M.; Bouguennec, N.; Barfod, K.W.; Porter, T.; Webster, K.E.; Feller, J.A. Combined anterior cruciate ligament reconstruction and lateral extra-articular tenodesis does not result in an increased rate of osteoarthritis: A systematic review and best evidence synthesis. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1149–1160. [Google Scholar] [CrossRef]
- Lysholm, J.; Gillquist, J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sports Med. 1982, 10, 150–154. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)--development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Cerulli, G.; Zamarra, G.; Vercillo, F.; Pelosi, F. ACL reconstruction with “the original all-inside technique”. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 829–831. [Google Scholar] [CrossRef]
- Chen, S.-F.; Wang, Y.; Peng, Y.; Zhang, M. Effects of attrition shoes on balance control ability and postural stability following a single-leg drop jump landing. Healthcare 2023, 11, 1127. [Google Scholar] [CrossRef]
- Vanegas, E.; Salazar, Y.; Igual, R.; Plaza, I. Force-sensitive mat for vertical jump measurement to assess lower limb strength: Validity and reliability study. JMIR MHealth UHealth 2021, 9, e27336. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Bermejo, L.; Adsuar, J.C.; Mendoza-Muñoz, M.; Barrios-Fernández, S.; Garcia-Gordillo, M.A.; Pérez-Gómez, J.; Carlos-Vivas, J. Test-retest reliability of Five Times Sit to Stand Test (FTSST) in adults: A systematic review and meta-analysis. Biology 2021, 10, 510. [Google Scholar] [CrossRef]
- Jones, H.S.R.; Moore, I.S.; King, E.; Stiles, V.H.; Laudani, L.; McCarthy-Ryan, M.; McFadden, C.; Daniels, K.A.J. Movement strategy correspondence across jumping and cutting tasks after anterior cruciate ligament reconstruction. Scand. J. Med. Sci. Sports 2022, 32, 612–621. [Google Scholar] [CrossRef]
- King, E.; Richter, C.; Franklyn-Miller, A.; Daniels, K.; Wadey, R.; Jackson, M.; Moran, R.; Strike, S. Biomechanical but not timed performance asymmetries persist between limbs 9 months after ACL reconstruction during planned and unplanned change of direction. J. Biomech. 2018, 81, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Badiola-Zabala, A.; Massó-Ortigosa, N.; Cabedo-Sanromà, J.; Rey-Abella, F.; Milà, R.; Oviedo, G.R. Observational study with the objective of determining possible correlations between GRF and muscle activation at reception after a jump in an ACL injury. Apunt. Sports Med. 2020, 55, 63–70. [Google Scholar] [CrossRef]
- Gustavsson, A.; Neeter, C.; Thomeé, P.; Silbernagel, K.G.; Augustsson, J.; Thomeé, R.; Karlsson, J. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 778–788. [Google Scholar] [CrossRef]
- Hodges, P.W.; Bui, B.H. A comparison of computer-based methods for the determination of onset of muscle contraction using electromyography. Electroencephalogr. Clin. Neurophysiol. 1996, 101, 511–519. [Google Scholar] [PubMed]
- Davis, J.J.; Vollmar, J.E.; Nguyen, A.B.; Wagoner, E.G.; Frankston, N.E.; Gruber, A.H. The role of off-axis force in running-related overuse injury. Med. Sci. Sports Exerc. 2018, 50, 141. [Google Scholar] [CrossRef]
- Solarino, G.; Bortone, I.; Vicenti, G.; Bizzoca, D.; Coviello, M.; Maccagnano, G.; Moretti, B.; D’Angelo, F. Role of biomechanical assessment in rotator cuff tear repair: Arthroscopic vs mini-open approach. World J. Orthop. 2021, 12, 991–1000. [Google Scholar] [CrossRef]
- Moretti, L.; Bortone, I.; Delmedico, M.; Cassano, D.G.; Caringella, N.; Bizzoca, D.; Moretti, B. Clinical, biomechanical, and self-reported health status after ACL reconstruction with meniscal repair in soccer players: Results at minimum 1-year follow-up. Orthop. J. Sports Med. 2023, 11, 23259671231177309. [Google Scholar] [CrossRef]
- Brophy, R.H.; Schafer, K.A.; Knapik, D.M.; Motley, J.; Haas, A.; Matava, M.J.; Wright, R.W.; Smith, M.V. Changes in dynamic postural stability after ACL reconstruction: Results over 2 years of follow-up. Orthop. J. Sports Med. 2022, 10, 23259671221098989. [Google Scholar] [CrossRef]
- Mohammadi, F.; Salavati, M.; Akhbari, B.; Mazaheri, M.; Khorrami, M.; Negahban, H. Static and dynamic postural control in competitive athletes after anterior cruciate ligament reconstruction and controls. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1603–1610. [Google Scholar] [CrossRef]
- Schon, J.M.; Moatshe, G.; Brady, A.W.; Serra Cruz, R.; Chahla, J.; Dornan, G.J.; Turnbull, T.L.; Engebretsen, L.; LaPrade, R.F. Anatomic anterolateral ligament reconstruction of the knee leads to overconstraint at any fixation angle. Am. J. Sports Med. 2016, 44, 2546–2556. [Google Scholar] [CrossRef]
- Królikowska, A.; Czamara, A.; Kentel, M. Does gracilis tendon harvest during ACL reconstruction with a hamstring autograft affect torque of muscles responsible for shin rotation? Med. Sci. Monit. 2015, 21, 2084–2093. [Google Scholar] [CrossRef] [PubMed]
- Janssen, R.P.A.; van der Velden, M.J.F.; Pasmans, H.L.M.; Sala, H.A.G.M. Regeneration of hamstring tendons after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Coats-Thomas, M.S.; Miranda, D.L.; Badger, G.J.; Fleming, B.C. Effects of ACL reconstruction surgery on muscle activity of the lower limb during a jump-cut maneuver in males and females: Muscle activity during a jump-cut. J. Orthop. Res. 2013, 31, 1890–1896. [Google Scholar] [CrossRef] [PubMed]
- Zunzarren, G.; Garet, B.; Vinciguerra, B.; Murgier, J. Persistence of neuromuscular activation deficit in the lower limb at 3-years of follow-up after ACL reconstruction surgery. Knee 2023, 43, 97–105. [Google Scholar] [CrossRef]
- Delaloye, J.R.; Hartog, C.; Blatter, S.; Schläppi, M.; Müller, D.; Denzler, D.; Murar, J.; Koch, P.P. Anterolateral ligament reconstruction and modified Lemaire lateral extra-articular tenodesis similarly improve knee stability after anterior cruciate ligament reconstruction: A biomechanical study. Arthroscopy 2020, 36, 1942–1950. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | ACL | ACL-ALL | |||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Effect Size | |
| Age [years] | 24 | 11 | 18 | 11 | 0.20 (−0.15–0.45) |
| Distance to surgery [months] | 13 | 21 | 10 | 2 | 0.18 (−0.21–0.45) |
| KOOS | 85 | 18 | 87 | 7 | 0.07 (−0.31–0.21) |
| LYSHOLM | 90 | 23 | 88 | 5 | 0.14 (−0.20–0.37) |
| TROPHISM (Operated Side) [cm] | 45 | 4 | 44 | 1 | 0.20 (−0.17–0.47) |
| TROPHISM (Healthy Side) [cm] | 46 | 6 | 46 | 1 | 0.16 (−0.20–0.39) |
| Variable | ACL | ACL-ALL | ||||
|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Effect Size | ||
| preATT_OVL_o | 0.09 | 0.19 | 0.23 | 0.27 | 0.48 (0.17–0.8) | moderate |
| preATT_HVL_o | 1.07 | 0.54 | 1.11 | 0.28 | 0.11 (−0.24–0.31) | |
| preATT_OVM_o | 0.09 | 0.14 | 0.29 | 0.09 | 0.38 (0.04–0.72) | moderate |
| preATT_HVM_o | 1.27 | 0.74 | 1.09 | 0.86 | 0.01 (−0.41–0.11) | |
| preATT_OVL_h | 1.05 | 0.86 | 1.11 | 0.54 | 0.01 (−0.38–0.1) | |
| preATT_HVL_h | 0.12 | 0.31 | 0.25 | 0.14 | 0.04 (−0.36–0.15) | |
| preATT_OVM_h | 0.81 | 0.41 | 0.81 | 0.69 | 0.04 (−0.36–0.16) | |
| preATT_HVM_h | 0.22 | 0.22 | 0.35 | 0.36 | 0.04 (−0.42–0.17) | |
| env_OVL_o | 187.39 | 191.89 | 141.95 | 87.85 | 0.01 (−0.4–0.11) | |
| env_HVL_o | 47.68 | 55.08 | 49.63 | 64.58 | 0.14 (−0.19–0.36) | |
| env_OVM_o | 227.68 | 92.7 | 187.24 | 162.09 | 0.19 (−0.18–0.46) | |
| env_HVM_o | 87.11 | 156.02 | 38.67 | 75.59 | 0.09(−0.27–0.27) | |
| env_OVL_h | 56.96 | 49.15 | 69.45 | 58.71 | 0.12 (−0.23–0.31) | |
| env_HVL_h | 215.8 | 170.72 | 152.83 | 32.72 | 0.27 (−0.09–0.61) | |
| env_OVM_h | 59.24 | 59.83 | 62.82 | 33.89 | 0.01 (−0.38–0.1) | |
| env_HVM_h | 318.22 | 225.69 | 247.01 | 114.88 | 0.30 (−0.06–0.61) | |
| VGRF_o | 1617.018 | 583.39 | 1437.221 | 328.35 | 0.27 (−0.07–0.59) | |
| VGRF_h | 1833.156 | 514.46 | 1742.171 | 380.10 | 0.19 (−0.15–0.46) | |
| NPTS_Fy_o | 4 | 3 | 1 | 1 | 0.45(0.11–0.8) | moderate |
| NPTS_Fy_h | 5 | 4 | 2 | 0 | 0.49(0.16–0.84) | moderate |
| ROM_o | 44.36 | 11.58 | 35.69 | 5.65 | 0.51(0.21–0.82) | large |
| ROM_h | 47.86 | 14.80 | 43.49 | 6.92 | 0.35 (−0.0043–0.69) | |
| Off-axis_x_o | 2.87 | 3.73 | 1.99 | 5.71 | 0.14 (−0.24–0.38) | |
| Off-axis_z_o | 2.96 | 1.80 | 3.59 | 2.16 | 0.30 (−0.03–0.61) | |
| Off-axis_x_h | 3.62 | 3.77 | 3.96 | 2.96 | 0.04 (−0.35–0.16) | |
| Off-axis_z_h | 3.23 | 1.58 | 3.51 | 0.72 | 0.22 (−0.14–0.52) | |
| Variable | ACL | ACL-ALL | ||||
|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Effect Size | ||
| duration_STS | 8.25 | 1.73 | 7.76 | 3.72 | 0.04 (−0.13–0.12) | |
| dur_cycles_mean | 1.19 | 0.25 | 1.21 | 0.31 | 0.18 (0.0014–0.34) | |
| peak_F_rise | 541.6 | 112.41 | 452.87 | 134.8 | 0.37 (0.21–0.53) | moderate |
| mean_F_rise | 333.6 | 92.2 | 304.65 | 45.25 | 0.20 (0.01–0.37) | |
| t_peak | 0.14 | 0.03 | 0.14 | 0.03 | 0.18 (0.0036–0.35) | |
| max_env_OVL | 0.2 | 0.15 | 0.1 | 0.26 | 0.27 (0.08–0.47) | |
| max_env_HVL | 0.2 | 0.09 | 0.22 | 0.1 | 0.14 (−0.03–0.3) | |
| max_env_OVM | 0.17 | 0.13 | 0.11 | 0.19 | 0.19 (0.0094–0.37) | |
| max_env_HVM | 0.17 | 0.19 | 0.18 | 0.11 | 0.02 (−0.16–0.08) | |
| att_OVL | 1.04 | 0.27 | 1.11 | 0.46 | 0.20 (0.02–0.38) | |
| att_HVL | 1.08 | 0.27 | 1.19 | 0.24 | 0.26 (0.09–0.42) | |
| att_OVM | 1.05 | 0.3 | 1.03 | 0.29 | 0.04 (−0.12–0.13) | |
| att_HVM | 1.1 | 0.19 | 1.14 | 0.36 | 0.26 (0.08–0.44) | |
| Variable | ACL | ACL-ALL | ||||
|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Effect Size | ||
| peak_envOVL_1o | 0.486 | 0.214 | 0.356 | 0.264 | 0.32 (−0.02–0.64) | |
| peak_envOVL_2o | 0.097 | 0.081 | 0.058 | 0.036 | 0.01 (−0.4–0.1) | |
| peak_envHVL_1o | 0.466 | 0.306 | 0.311 | 0.281 | 0.17 (−0.17–0.41) | |
| peak_envHVL_2o | 0.095 | 0.055 | 0.069 | 0.01 | 0.14 (−0.21–0.37) | |
| peak_envOVM_1o | 0.51 | 0.15 | 0.342 | 0.109 | 0.30 (−0.06–0.61) | |
| peak_envOVM_2o | 0.125 | 0.157 | 0.065 | 0.078 | 0.08 (−0.26–0.23) | |
| peak_envHVM_1o | 0.561 | 0.254 | 0.493 | 0.261 | 0.35 (0.05–0.66) | moderate |
| peak_envHVM_2o | 0.117 | 0.066 | 0.091 | 0.276 | 0.17 (−0.16–0.41) | |
| peak_envOVL_1h | 0.5 | 0.166 | 0.401 | 0.214 | 0.34 (−0.0043–0.69) | |
| peak_envOVL_2h | 0.105 | 0.106 | 0.109 | 0.042 | 0.03 (−0.39–0.15) | |
| peak_envHVL_1h | 0.526 | 0.297 | 0.478 | 0.249 | 0.40 (0.07–0.74) | moderate |
| peak_envHVL_2h | 0.13 | 0.13 | 0.097 | 0.156 | 0.30 (−0.04–0.63) | |
| peak_envOVM_1h | 0.536 | 0.103 | 0.364 | 0.049 | 0.38 (0.04–0.71) | moderate |
| peak_envOVM_2h | 0.178 | 0.206 | 0.095 | 0.184 | 0.40 (0.04–0.76) | moderate |
| peak_envHVM_1h | 0.481 | 0.142 | 0.613 | 0.302 | 0.28 (−0.07–0.59) | |
| peak_envHVM_2h | 0.212 | 0.089 | 0.095 | 0.398 | 0.09 (−0.26–0.26) | |
| onset_OVL_1o | 1.46 | 0.4 | 1.39 | 0.44 | 0.22 (−0.13–0.51) | |
| onset_OVL_2o | 0.68 | 0.62 | 0.45 | 0.56 | 0.18 (−0.16–0.44) | |
| onset_HVL_1o | 1.45 | 0.61 | 1.24 | 0.07 | 0.09 (−0.3–0.29) | |
| onset_HVL_2o | 0.3 | 0.46 | 0.36 | 0.53 | 0.09 (−0.26–0.26) | |
| onset_OVM_1o | 1.45 | 0.4 | 1.45 | 0.33 | 0.01 (−0.4–0.1) | |
| onset_OVM_2o | 0.55 | 0.46 | 0.58 | 0.54 | 0.14 (−0.22–0.37) | |
| onset_HVM_1o | 1.4 | 0.43 | 1.14 | 0.35 | 0.09 (−0.27–0.26) | |
| onset_HVM_2o | 28 | 0.72 | 0.25 | 0.29 | 0.15 (−0.19–0.38) | |
| onset_OVL_1h | 1.21 | 0.66 | 1.35 | 0.24 | 0.17 (−0.17–0.41) | |
| onset_OVL_2h | 0.47 | 0.4 | 0.71 | 0.13 | 0.12 (−0.27–0.33) | |
| onset_HVL_1h | 1.25 | 0.43 | 1.27 | 0.5 | 0.01 (−0.41–0.1) | |
| onset_HVL_2h | 0.66 | 0.6 | 0.9 | 0.55 | 0.09 (−0.3–0.27) | |
| onset_OVM_1h | 1.25 | 0.49 | 1.35 | 0.38 | 0.01 (−0.39–0.09) | |
| onset_OVM_2h | 0.59 | 0.51 | 0.62 | 0.27 | 0.01 (−0.4–0.11) | |
| onset_HVM_1h | 1.32 | 0.42 | 1.38 | 0.34 | 0.12 (−0.24–0.31) | |
| onset_HVM_2h | 0.95 | 0.66 | 0.19 | 0.76 | 0.48 (0.16–0.8) | moderate |
| GRF_1o | 1408.853 | 429.844 | 1231.04 | 347.303 | 0.45 (0.14, 0.78) | moderate |
| GRF_2o | 528.246 | 170.058 | 502.406 | 114.002 | 0.12 (−0.23–0.31) | |
| GRF_1h | 1298.828 | 353.556 | 988.729 | 175.458 | 0.53 (0.22, 0.86) | large |
| GRF_2h | 547.945 | 243.83 | 538.605 | 35.761 | 0.14 (−0.21–0.37) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassano, G.D.; Moretti, L.; Coviello, M.; Bortone, I.; Musci, M.; Favilla, E.; Solarino, G. Anterolateral Ligament Reconstruction Combined with Anterior Cruciate Ligament Reconstruction: Clinical and Functional Outcomes. Medicina 2025, 61, 1011. https://doi.org/10.3390/medicina61061011
Cassano GD, Moretti L, Coviello M, Bortone I, Musci M, Favilla E, Solarino G. Anterolateral Ligament Reconstruction Combined with Anterior Cruciate Ligament Reconstruction: Clinical and Functional Outcomes. Medicina. 2025; 61(6):1011. https://doi.org/10.3390/medicina61061011
Chicago/Turabian StyleCassano, Giuseppe Danilo, Lorenzo Moretti, Michele Coviello, Ilaria Bortone, Mariapia Musci, Ennio Favilla, and Giuseppe Solarino. 2025. "Anterolateral Ligament Reconstruction Combined with Anterior Cruciate Ligament Reconstruction: Clinical and Functional Outcomes" Medicina 61, no. 6: 1011. https://doi.org/10.3390/medicina61061011
APA StyleCassano, G. D., Moretti, L., Coviello, M., Bortone, I., Musci, M., Favilla, E., & Solarino, G. (2025). Anterolateral Ligament Reconstruction Combined with Anterior Cruciate Ligament Reconstruction: Clinical and Functional Outcomes. Medicina, 61(6), 1011. https://doi.org/10.3390/medicina61061011