
Sex Differences in Sarcopenia in Patients Undergoing Total Knee Arthroplasty for Advanced Knee Osteoarthritis

Abstract
1. Introduction
2. Materials and Methods
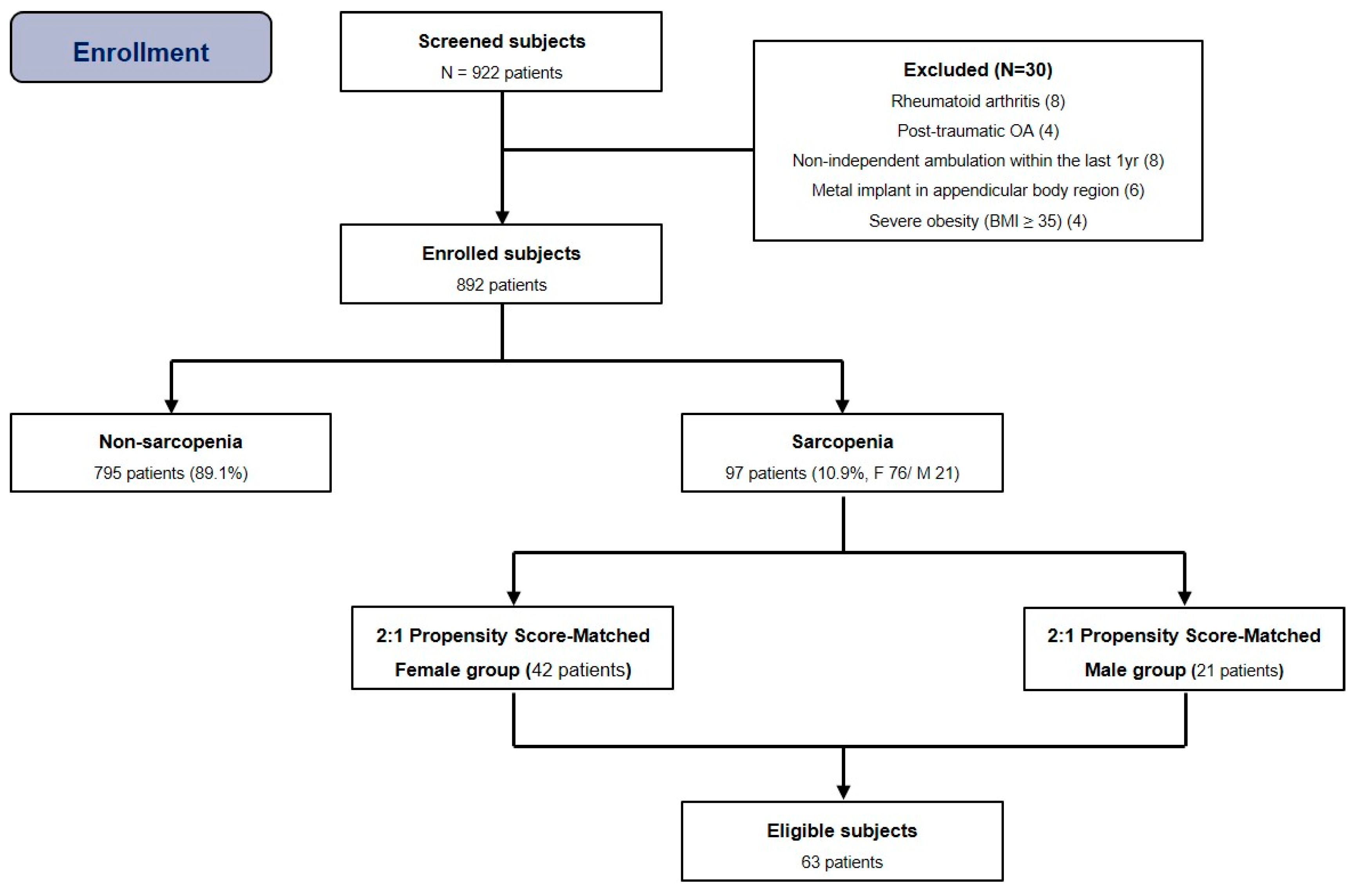
2.1. Study Subjects
2.2. Definition of Sarcopenia
2.3. Matched-Pair Analysis
2.4. Operative Details and Postoperative Protocol
2.5. Outcome Assessment
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evans, W.J. Sarcopenia should reflect the contribution of age-associated changes in skeletal muscle to risk of morbidity and mortality in elderly people. J. Am. Med. Dir. Assoc. 2015, 16, 546–547. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A. Sarcopenia: Revised european consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M. Sarcopenia: European consensus on definition and diagnosisreport of the european working group on sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Bokshan, S.L.; Han, A.L.; DePasse, J.M.; Eltorai, A.E.; Marcaccio, S.E.; Palumbo, M.A.; Daniels, A.H. Effect of sarcopenia on postoperative morbidity and mortality after thoracolumbar spine surgery. Orthopedics 2016, 39, e1159–e1164. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Goates, S.; Du, K.; Arensberg, M.; Gaillard, T.; Guralnik, J.; Pereira, S. Economic impact of hospitalizations in us adults with sarcopenia. J. Frailty Aging 2019, 8, 93–99. [Google Scholar] [CrossRef]
- Ho, K.K.-W.; Lau, L.C.-M.; Chau, W.-W.; Poon, Q.; Chung, K.-Y.; Wong, R.M.-Y. End-stage knee osteoarthritis with and without sarcopenia and the effect of knee arthroplasty–A prospective cohort study. BMC Geriatr. 2021, 21, 2. [Google Scholar] [CrossRef] [PubMed]
- Babu, J.M.; Kalagara, S.; Durand, W.; Antoci, V.; Deren, M.E.; Cohen, E. Sarcopenia as a risk factor for prosthetic infection after total hip or knee arthroplasty. J. Arthroplast. 2019, 34, 116–122. [Google Scholar] [CrossRef]
- Koh, I.J.; Kim, T.K.; Chang, C.B.; Cho, H.J.; In, Y. Trends in use of total knee arthroplasty in Korea from 2001 to 2010. Clin. Orthop. Relat. Res. 2013, 471, 1441–1450. [Google Scholar] [CrossRef]
- Hwang, D.; Han, H.-S.; Lee, M.C.; Ro, D.H. Low muscle mass is an independent risk factor for postoperative blood transfusion in total knee arthroplasty: A retrospective, propensity score-matched cohort study. BMC Geriatr. 2022, 22, 218. [Google Scholar] [CrossRef]
- Kim, T.W.; Kang, S.-B.; Chang, C.B.; Moon, S.-Y.; Lee, Y.-K.; Koo, K.-H. Current trends and projected burden of primary and revision total knee arthroplasty in Korea between 2010 and 2030. J. Arthroplast. 2021, 36, 93–101. [Google Scholar] [CrossRef]
- Tay, L.; Ding, Y.; Leung, B.; Ismail, N.; Yeo, A.; Yew, S.; Tay, K.; Tan, C.; Chong, M. Sex-specific differences in risk factors for sarcopenia amongst community-dwelling older adults. Age 2015, 37, 121. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Smith, R.; Aulet, M.; Bensen, B.; Lichtman, S.; Wang, J.; Pierson, R., Jr. Appendicular skeletal muscle mass: Measurement by dual-photon absorptiometry. Am. J. Clin. Nutr. 1990, 52, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in new mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V.; Kashman, N.; Volland, G.; Weber, K.; Dowe, M.; Rogers, S. Grip and pinch strength: Normative data for adults. Arch. Phys. Med. Rehabil. 1985, 66, 69–74. [Google Scholar] [PubMed]
- Shon, O.-J.; Kim, G.B.; Cho, S.J. Does sarcopenia accompanying end-stage knee osteoarthritis affect the outcomes following total knee arthroplasty? Medicina 2023, 59, 1078. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Statistical criteria for selecting the optimal number of untreated subjects matched to each treated subject when using many-to-one matching on the propensity score. Am. J. Epidemiol. 2010, 172, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Daines, B.K.; Dennis, D.A. Gap balancing vs. Measured resection technique in total knee arthroplasty. Clin. Orthop. Surg. 2014, 6, 1–8. [Google Scholar] [CrossRef]
- Shon, O.-J.; Kim, G.B. Does the degree of intraoperatively identified cartilage loss affect the outcomes of primary total knee arthroplasty without patella resurfacing? A prospective comparative cohort study. Knee Surg. Relat. Res. 2022, 34, 36. [Google Scholar] [CrossRef]
- Lakomkin, N.; Zuckerman, S.L.; Stannard, B.; Montejo, J.; Sussman, E.S.; Virojanapa, J.; Kuzmik, G.; Goz, V.; Hadjipanayis, C.G.; Cheng, J.S. Preoperative risk stratification in spine tumor surgery: A comparison of the modified charlson index, frailty index, and asa score. Spine 2019, 44, E782–E787. [Google Scholar] [CrossRef] [PubMed]
- Lyman, S.; Lee, Y.-Y.; Franklin, P.D.; Li, W.; Cross, M.B.; Padgett, D.E. Validation of the koos, jr: A short-form knee arthroplasty outcomes survey. Clin. Orthop. Relat. Res. 2016, 474, 1461–1471. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of womac: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar] [PubMed]
- Ware, J.E., Jr.; Kosinski, M.; Keller, S.D. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Norkin, C.C.; White, D.J. Measurement of Joint Motion: A Guide to Goniometry; FA Davis: Philadelphia, PA, USA, 2016. [Google Scholar]
- Song, S.J.; Kim, K.I.; Bae, D.K.; Park, C.H. Mid-term lifetime survivals of octogenarians following primary and revision total knee arthroplasties were satisfactory: A retrospective single center study in contemporary period. Knee Surg. Relat. Res. 2020, 32, 50. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J. Arthroplast. 2018, 33, 1309–1314.e1302. [Google Scholar] [CrossRef] [PubMed]
- Jo, C.; Ko, S.; Shin, W.C.; Han, H.-S.; Lee, M.C.; Ko, T.; Ro, D.H. Transfusion after total knee arthroplasty can be predicted using the machine learning algorithm. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 1757–1764. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Goisser, S.; Bebenek, M.; von Stengel, S.; Bollheimer, L.C.; Sieber, C.C.; Freiberger, E. Prevalence of sarcopenia in germany and the corresponding effect of osteoarthritis in females 70 years and older living in the community: Results of the formosa study. Clin. Interv. Aging 2015, 2015, 1565–1573. [Google Scholar] [CrossRef]
- Roh, Y.H.; Koh, Y.D.; Noh, J.H.; Gong, H.S.; Baek, G.H. Evaluation of sarcopenia in patients with distal radius fractures. Arch. Osteoporos. 2017, 12, 5. [Google Scholar] [CrossRef]
- Ho, A.W.; Lee, M.M.; Chan, E.W.; Ng, H.M.; Lee, C.; Ng, W.; Wong, S. Prevalence of pre-sarcopenia and sarcopenia in hong kong chinese geriatric patients with hip fracture and its correlation with different factors. Hong Kong Med. J. 2016, 22, 23. [Google Scholar] [CrossRef]
- Yoo, J.-I.; Ha, Y.-C.; Kwon, H.-B.; Lee, Y.-K.; Koo, K.-H.; Yoo, M.-J. High prevalence of sarcopenia in korean patients after hip fracture: A case-control study. J. Korean Med. Sci. 2016, 31, 1479–1484. [Google Scholar] [CrossRef]
- Hashemi, R.; Shafiee, G.; Motlagh, A.D.; Pasalar, P.; Esmailzadeh, A.; Siassi, F.; Larijani, B.; Heshmat, R. Sarcopenia and its associated factors in iranian older individuals: Results of sarir study. Arch. Gerontol. Geriatr. 2016, 66, 18–22. [Google Scholar] [CrossRef]
- Yamada, M.; Nishiguchi, S.; Fukutani, N.; Tanigawa, T.; Yukutake, T.; Kayama, H.; Aoyama, T.; Arai, H. Prevalence of sarcopenia in community-dwelling japanese older adults. J. Am. Med. Dir. Assoc. 2013, 14, 911–915. [Google Scholar] [CrossRef]
- Boot, A.M.; de Ridder, M.A.; van der Sluis, I.M.; van Slobbe, I.; Krenning, E.P.; de Muinck Keizer-Schrama, S.M. Peak bone mineral density, lean body mass and fractures. Bone 2010, 46, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C. Grip strength across the life course: Normative data from twelve british studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef] [PubMed]
- Schultz, K.A.; Westcott, B.A.; Barber, K.R.; Sandrock, T.A. Elevated 1-year mortality rate in males sustaining low-energy proximal femur fractures and subgroup analysis utilizing age-adjusted charlson comorbidity index. Geriatr. Orthop. Surg. Rehabil. 2020, 11, 2151459319898644. [Google Scholar] [CrossRef] [PubMed]
- Schnell, S.; Friedman, S.M.; Mendelson, D.A.; Bingham, K.W.; Kates, S.L. The 1-year mortality of patients treated in a hip fracture program for elders. Geriatr. Orthop. Surg. Rehabil. 2010, 1, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.J.; Patten, C.; Reid, K.F.; Carabello, R.J.; Phillips, E.M.; Fielding, R.A. Impaired voluntary neuromuscular activation limits muscle power in mobility-limited older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Zhai, J.; Ma, B.; Qin, J.; Lyu, Q.; Khatun, P.; Liang, R.; Cong, M.; Guo, L.; Kong, Y. Alcohol consumption patterns and the risk of sarcopenia: A population-based cross-sectional study among chinese women and men from henan province. BMC Public Health 2022, 22, 1894. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, J.; Zhao, L.; Wang, Z.; Yu, D.; He, Y.; Ding, G. The drinking status and associated factors in adults in china. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 898–903. [Google Scholar] [PubMed]
- World Health Organization. World Health Organization (WHO) Report on the Global Tobacco Epidemic 2017-Country Profile Portugal; World Health Organization: Geneva, Switzerland, 2017; Volume 10, p. 9781410610348. [Google Scholar]
- Park, H.-R.; Cho, S.-K.; Im, S.G.; Jung, S.-Y.; Kim, D.; Jang, E.J.; Sung, Y.-K. Treatment patterns of knee osteoarthritis patients in korea. Korean J. Intern. Med. 2019, 34, 1145. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Score |
|---|---|
| Peripheral vascular disease or pain at rest | 1 |
| Congestive heart failure | 1 |
| Prior myocardial infarction | 1 |
| Diabetes mellitus | 1 |
| Prior transient ischemic attack or stroke | 1 |
| Chronic obstructive pulmonary disease | 1 |
| Renal failure | 2 |
| Hemiplegia or paraplegia | 2 |
| Ascites or esophageal varices | 3 |
| Disseminated cancer | 6 |
| (Age) | |
| ≤40 years old | 0 |
| 41–50 years old | 1 |
| 51–60 years old | 2 |
| 61–70 years old | 3 |
| ≥70 years old | 4 |
| Total | Sarcopenia | Non-Sarcopenia | p Value | |
|---|---|---|---|---|
| Patients, n (%) † | 892 (100) | 97 (10.9) | 795 (89.1) | - |
| Age (years) * | 71.6 (60–88) | 75.8 (69–88) | 68.7 (60–76) | 0.871 |
| Sex, n † | ||||
| Female, n | 785 (88.0) | 76 (78.4) | 709 (89.2) | 0.002 |
| Male, n | 107 (11.2) | 21 (21.6) | 86 (10.8) | |
| BMI (kg/m2) ‡ | 26.9 ± 3.7 | 23.2 ± 3.4 | 27.5 ± 3.2 | <0.001 |
| Mean f/u (mon) * | 24.5 (12–37) | 24.7 (12–37) | 24.4 (12–37) | 0.791 |
| Bilaterality, n (%) † | 381 (42.7) | 40 (41.2) | 337 (42.4) | 0.810 |
| Preop K–L grade, n (%) † | ||||
| Grade III | 226 (25.3) | 26 (26.8) | 200 (25.2) | 0.745 |
| Grade IV | 666 (74.7) | 71 (73.2) | 595 (74.8) | |
| Current smoker, n (%) † | 76 (8.5) | 12 (12.4) | 64 (8.1) | 0.165 |
| Alcohol drinker, n (%) † | 87 (9.8) | 15 (15.5) | 72 (9.1) | 0.060 |
| mCCI † | ||||
| 2 | 40 (4.5) | - | 40 (5.0) | <0.001 |
| 3 and 4 | 419 (47.0) | 7 (7.2) | 412 (51.8) | |
| 5–8 | 316 (35.4) | 46 (47.4) | 270 (34.0) | |
| ≥9 | 117 (13.1) | 44 (45.4) | 73 (9.2) | |
| Hb level (g/dL) ‡ | 12.5 ± 2.1 | 11.1 ± 3.2 | 12.8 ± 1.0 | 0.021 |
| Total protein (g/dL) ‡ | 6.8 ± 1.0 | 5.9 ± 1.2 | 7.0 ± 0.9 | 0.037 |
| ASM index (ASM/height2), kg/m2 ‡ | 6.0 ± 0.6 | 5.0 ± 0.8 | 6.3 ± 0.6 | 0.004 |
| Grip strength, kg ‡ | 18.0 ± 3.4 | 16.1 ± 4.5 | 19.2 ± 3.1 | 0.030 |
| 6 m walking speed, m/s ‡ | 1.2 ± 0.2 | 0.8 ± 0.1 | 1.4 ± 0.2 | 0.025 |
| 2:1 Propensity-Matched Population (n = 63) | |||
|---|---|---|---|
| Female Sarcopenia (n = 42) | Male Sarcopenia (n = 21) | p Value | |
| Age (years) * | 75.6 (70–83) | 76.1 (70–82) | 0.501 |
| BMI (kg/m2) ‡ | 23.0 ± 3.0 | 23.5 ± 2.9 | 0.762 |
| Mean f/u (mon) * | 24.6 (12–37) | 24.6 (12–37) | 0.791 |
| Bilaterality, n (%) † | 18 (42.9) | 9 (42.9) | - |
| Preop K-L grade, n (%) † | |||
| Grade III | 11 (26.2) | 5 (23.8) | 0.838 |
| Grade IV | 31 (73.8) | 16 (76.2) | |
| Current smoker, n (%) † | 3 (7.1) | 8 (38.1) | 0.002 |
| Alcohol drinker, n (%) † | 3 (7.1) | 10 (47.6) | <0.001 |
| mCCI † | 0.022 | ||
| 2 | - | - | |
| 3 and 4 | 6 (9.5) | 1 (4.8) | |
| 5–8 | 28 (54.8) | 9 (42.9) | |
| ≥9 | 8 (35.7) | 11(52.4) | |
| Hb level (g/dL) ‡ | 9.9 ± 1.3 | 11.2 ± 1.0 | 0.021 |
| Total protein (g/dL) ‡ | 5.2 ± 1.2 | 5.9 ± 1.2 | 0.043 |
| ASM index (ASM/height2), kg/m2 ‡ | 4.2 ± 0.5 | 5.8 ± 0.6 | <0.001 |
| Grip strength, kg ‡ | 15.4 ± 3.3 | 16.5 ± 3.1 | 0.021 |
| 6 m walking speed, m/s ‡ | 0.5 ± 0.2 | 0.9 ± 0.2 | 0.018 |
| Total (n = 63) | Female (n = 42) | Male (n = 21) | p-Value | ||
|---|---|---|---|---|---|
| Cardiovascular | 2 (3.2) | 1 (2.4) | 1 (2.4) | 0.559 | |
| Pulmonary | 4 (6.3) | 1 (2.4) | 3 (14.3) | 0.104 | |
| Gastrointestinal | - | 1 (2.3) | - | - | |
| Hepatic | 6 (9.5) | 4 (9.5) | 2 (9.5) | 0.686 | |
| Systemic | Nephrotic | - | - | - | - |
| Endocrinologic | - | - | - | - | |
| Urologic | 13 (20.6) | 6 (14.3) | 7 (33.3) | <0.001 | |
| Cerebral | 2 (3.2) | 1 (2.4) | 1 (4.8) | 0.559 | |
| Delirium | 11 (17.5) | 9 (21.4) | 2 (9.5) | 0.085 | |
| Blood transfusion | 17 (27.0) | 12 (28.6) | 5 (23.8) | 0.466 | |
| Venous thromboembolism | |||||
 | - | - | - | - | |
| Specific | 3 (4.8) | 2 (4.8) | 1 (4.8) | 0.774 | |
| 6 (9.5) | 4 (9.5) | 2 (9.5) | 0.686 | ||
| Infection | 2 (3.2) | 1 (2.4) | 1 (4.8) | 0.559 | |
| Periprosthetic fracture | - | - | - | - |
| Variable | p Value | Odds Radio (95% CI) | ||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |
| Age | 0.501 | 1.8 (0.9–2.7) | ||
| BMI | 0.731 | 1.9 (1.8–2.2) | ||
| Alcohol drinker | <0.001 * | 0.003 † | 1.5 (0.8–1.7) | 1.4 (0.9–1.8) |
| Current smoker | <0.001 * | 0.019 † | 1.3 (1.1–2.5) | 1.2 (0.9–1.4) |
| (Preoperative) | ||||
| K–L grade | 0.751 | 1.2 (0.8–1.6) | ||
| mCCI | 0.012 | 0.036 † | 1.1 (0.8–1.4) | 1.2 (0.8–1.5) |
| Hb level | 0.021 * | 0.253 | 0.8 (0.6–0.9) | 0.7 (0.6–0.9) |
| Total protein | 0.037 * | 0.302 | 0.7 (0.5–0.8) | 0.6 (0.5–0.8) |
| ASMI | <0.001 * | 0.125 | 0.7 (0.5–0.8) | 0.6 (0.5–0.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shon, O.-J.; Kim, G.B.; Jo, S.H. Sex Differences in Sarcopenia in Patients Undergoing Total Knee Arthroplasty for Advanced Knee Osteoarthritis. Medicina 2024, 60, 226. https://doi.org/10.3390/medicina60020226
Shon O-J, Kim GB, Jo SH. Sex Differences in Sarcopenia in Patients Undergoing Total Knee Arthroplasty for Advanced Knee Osteoarthritis. Medicina. 2024; 60(2):226. https://doi.org/10.3390/medicina60020226
Chicago/Turabian StyleShon, Oog-Jin, Gi Beom Kim, and Seong Hyeon Jo. 2024. "Sex Differences in Sarcopenia in Patients Undergoing Total Knee Arthroplasty for Advanced Knee Osteoarthritis" Medicina 60, no. 2: 226. https://doi.org/10.3390/medicina60020226
APA StyleShon, O.-J., Kim, G. B., & Jo, S. H. (2024). Sex Differences in Sarcopenia in Patients Undergoing Total Knee Arthroplasty for Advanced Knee Osteoarthritis. Medicina, 60(2), 226. https://doi.org/10.3390/medicina60020226