

Alveolar Ridge Augmentation Assessment Using a Minimalistic Approach, with and without Low-Level Laser Therapy (LLLT)—A Comparative Clinical Trial

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
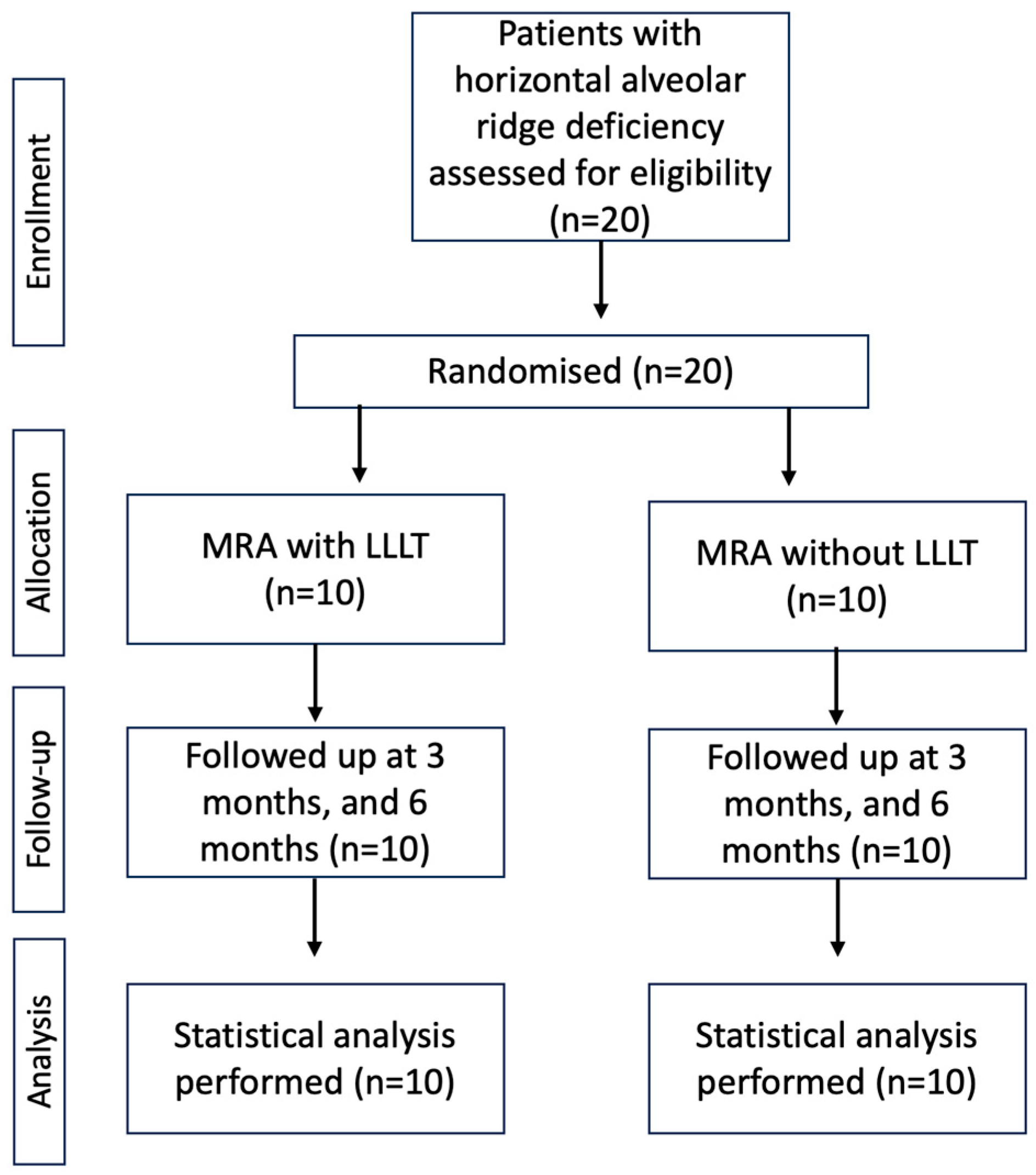
2.1. Study Design and Patients
2.2. Clinical Measurement, Radiological Assessment, and Pre-Surgical Procedures
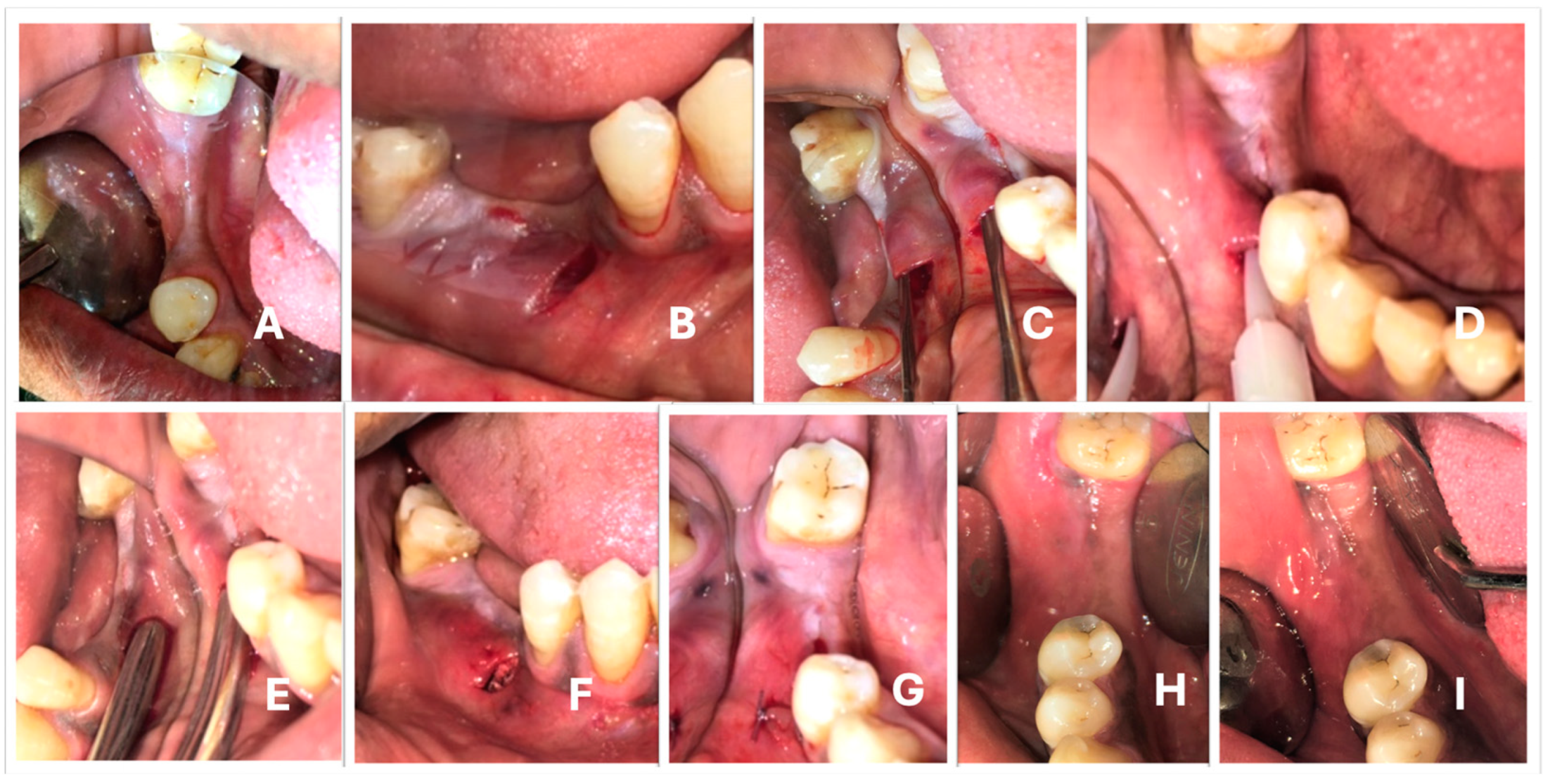
2.3. Surgical Procedure
2.3.1. Minimalistic Alveolar Ridge Augmentation Technique
2.3.2. LLLT Test Sites
2.4. Statistical Analysis
3. Results
3.1. Clinical Observation
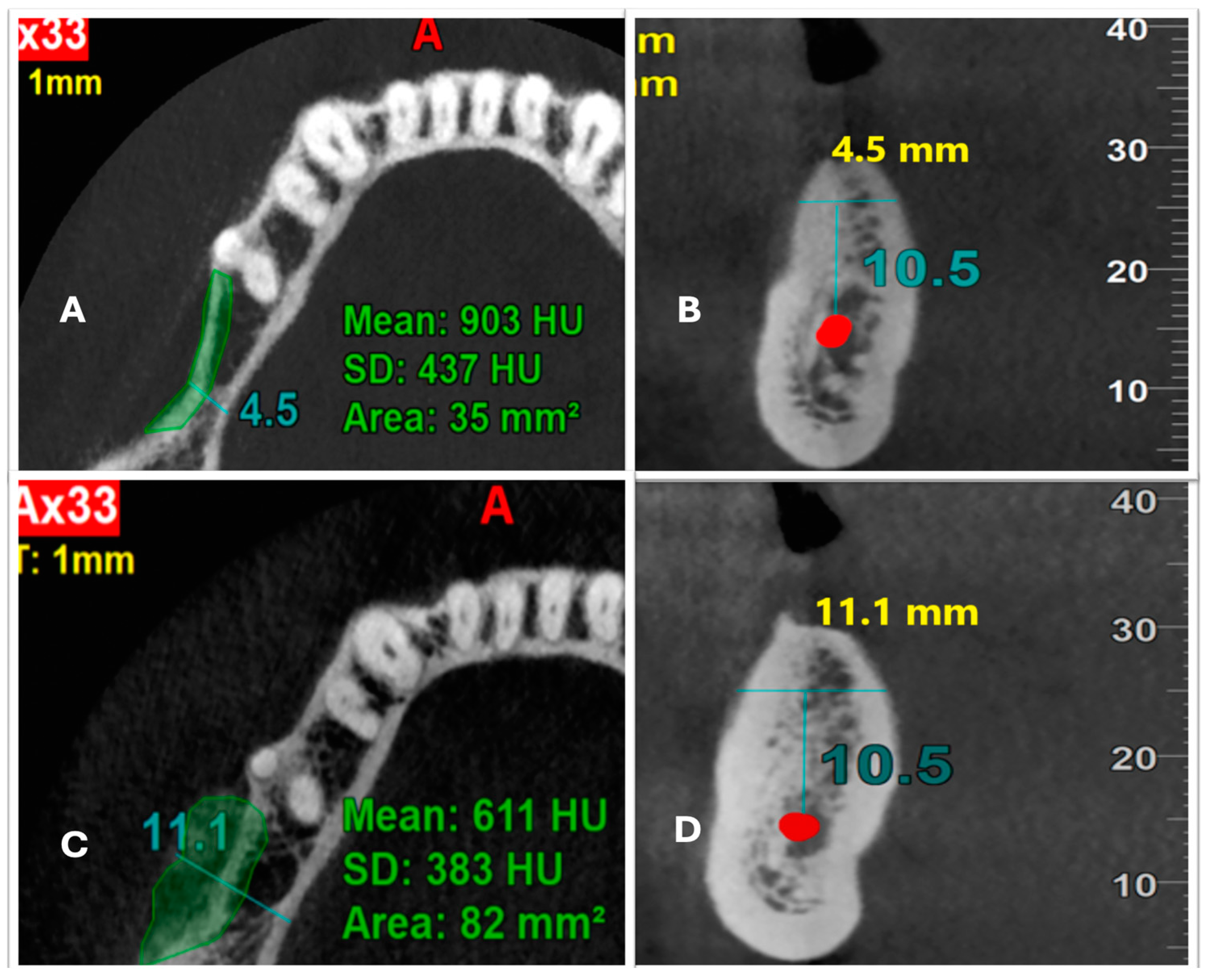
3.2. Radiological Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Misch, C.M. Autogenous bone: Is it still the gold standard? Implant Dent. 2010, 19, 361–363. [Google Scholar] [CrossRef] [PubMed]
- LeGeros, R.Z. Properties of osteoconductive biomaterials: Calcium phosphates. Clin. Orthop. Relat. Res. 2002, 395, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Hasson, O. Augmentation of Deficient Lateral Alveolar Ridge Using the Subperiosteal Tunneling Dissection Approach. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2007, 103, e14–e19. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Dula, K.; Hirt, H.P.; Schenk, R.K. Lateral Ridge Augmentation Using Autografts and Barrier Membranes: A Clinical Study With 40 Partially Edentulous Patients. J. Oral Maxillofac. Surg. 1996, 54, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S. Treatment of The Single Tooth Extraction Site. Oral Maxillofac. Surg. Clin. N. Am. 2004, 16, 41–63. [Google Scholar]
- Scipioni, A.; Bruschi, G.B.; Calesini, G. The edentulous ridge expansion technique: A five-year study. Int. J. Periodont. Restor. Dent. 1994, 14, 451–459. [Google Scholar] [CrossRef]
- Yun, K.I.; Choi, H.; Wright, R.F.; Ahn, H.S.; Chang, B.M.; Kim, H.J. Efficacy of alveolar vertical distraction osteogenesis and autogenous bone grafting for dental implants: Systematic review and meta-analysis. Int. J. Oral Maxillofac. Implant. 2016, 31, 26–36. [Google Scholar] [CrossRef]
- Jeong, S.M.; Choi, B.H.; Li, J.; Xuan, F. Simultaneous flapless implant placement and peri-implant defect correction: An experimental pilot study in dogs. J. Periodontol. 2008, 79, 876–880. [Google Scholar] [CrossRef]
- Block, M.S.; Degen, M. Horizontal ridge augmentation using human mineralized particulate bone: Preliminary results. J. Oral Maxillofac. Surg. 2004, 62 (Suppl. S2), 67–72. [Google Scholar] [CrossRef]
- Lee, E.A. Subperiosteal Minimally Invasive Aesthetic Ridge Augmentation Technique (SMART): A New Standard For Bone Reconstruction of The Jaws. Int. J. Periodont. Restor. Dent. 2017, 37, 165–173. [Google Scholar] [CrossRef]
- Machtei, E.E. The effect of membrane exposure on the outcome of regenerative procedures in humans: A meta-analysis. J. Periodontol. 2001, 72, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Kent, J.N.; Quinn, J.H.; Zide, M.F.; Guerra, L.; Boyne, P. Correction of alveolar ridge deficiencies with nonresorbable hydroxyapatite. J. Am. Dent. Assoc. 1982, 105, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.W.; Meyers, J.F.; Robinson, R.R. Hydroxyapatite augmentation of the anterior portion of the maxilla with a modified transpositional flap technique. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 395–399. [Google Scholar] [CrossRef]
- Marshall, S.G. The combined use of endosseous dental implants and collagen/hydroxylapatite augmentation procedures for reconstruction/augmentation of the edentulous and atrophic mandible: A preliminary report. Oral Surg. Oral Med. Oral Pathol. 1989, 68, 517–526. [Google Scholar] [CrossRef]
- Batista, J.D.; Zanetta-Barbosa, D.; Cardoso, S.V.; Dechichi, P.; Rocha, F.S.; Pagnoncelli, R.M. Effect of low-level laser therapy on repair of the bone compromised by radiotherapy. Lasers Med. Sci. 2014, 29, 1913–1983. [Google Scholar] [CrossRef]
- Law, D.; McDonough, S.; Bleakley, C.; Baxter, G.D.; Tumilty, S. Laser acupuncture for treating musculoskeletal pain: A systematicreview with meta-analysis. J. Acupunct. Meridian Stud. 2015, 8, 2–164. [Google Scholar] [CrossRef] [PubMed]
- Eslamian, L.; Borzabadi-Farahani, A.; Hassanzadeh-Azhiri, A.; Badiee, M.R.; Fekrazad, R. The effect of 810-nm low-level laser therapy on pain caused by orthodontic elastomeric separators. Lasers Med. Sci. 2014, 29, 559–564. [Google Scholar] [CrossRef]
- Blumenfeld, I.; Srouji, S.; Lanir, Y.; Laufer, D.; Livne, E. Enhancement of bone defect healing in old rats by TGF-beta and IGF-1. Exp. Gerontol. 2002, 37, 553–565. [Google Scholar] [CrossRef]
- Renno, A.C.; McDonnell, P.A.; Parizotto, N.A.; Laakso, E.L. The effects of laser irradiation on osteoblast and osteosarcoma cell proliferation and differentiation in vitro. Photomed. Laser Surg. 2007, 25, 275–280. [Google Scholar] [CrossRef]
- Parker, C. The Growth of Implant Dentistry. The Dentist; George Warman Publications: Surrey, UK, 2012. [Google Scholar]
- Kfir, E.; Kfir, V.; Eliav, E.; Kaluski, E. Minimally invasive guided bone regeneration. J. Oral Implantol. 2007, 33, 205–210. [Google Scholar] [CrossRef]
- Panday, V.; Upadhyaya, V.; Berwal, V.; Jain, K.; Sah, N.; Sarathi, P.; Swami, P.C. Comparative evalution of G bone (hydroxyapatite) and G-graft (hydroxyapatite with collagen) as bone graft material in mandibular III molar extraction socket. J. Clin. Diagn. Res. 2015, 9, ZC48–ZC52. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, C.; Hallman, M.; Sennerby, L.; Sammons, R. Back-scattered electron imaging and elemental analysis of retrieved bone tissue following sinus augmentation with deproteinized bovine bone or biphasic calcium phosphate. Clin. Oral Implant. Res. 2010, 21, 924–930. [Google Scholar] [CrossRef] [PubMed]
- García-Morales, J.M.; Tortamano-Neto, P.; Todescan, F.F.; de Andrade, J.C.; Marotti, J.; Zezell, D.M. Stability of dental implants after irradiation with an 830-nm low-level laser: A double-blind randomized clinical study. Lasers Med. Sci. 2012, 27, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Mandić, B.; Lazić, Z.; Marković, A.; Mandić, B.; Mandić, M.; Đinić, A.; Miličić, B. Influence of postoperative low-level laser therapy on the osseointegration of self-tapping implants in the posterior maxilla: A 6-week split-mouth clinical study. Vojnosanit. Pregl. 2015, 72, 233–240. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Description of Patients and Graft Sites | ||
|---|---|---|
| Patients | Number | Percent |
| Total | 20 | 100 |
| Sex (Male | 17 | 85 |
| Sex (Female) | 3 | 15 |
| Graft sites | ||
| Maxillary anterior | 0 | 0 |
| Maxillary posterior | 4 | 20 |
| Mandibular anterior | 0 | 0 |
| Mandibular posterior | 16 | 80 |
| Groups | Patient Reported Outcomes | p Value | ||
|---|---|---|---|---|
| None | Mild Pain | Moderate Pain | ||
| Test | 7 | 2 | 1 | 0.81 |
| 70.0% | 20.0% | 10.0% | ||
| Control | 8 | 1 | 1 | |
| 80.0% | 10.0% | 10.0% | ||
| Test Group | Control Group | |||||
|---|---|---|---|---|---|---|
| Baseline | 6 Months | p Value | Baseline | 6 Months | p Value | |
| Mean Ridge Width (MRW) in mm | 5.05 ± 1.43 | 6.51 ± 1.57 | 0.001 * | 5.03 ± 0.82 | 7.17 ± 1.98 | 0.003 * |
| Mean Bone Density (MBD) in HU | 1040.70 ± 490 | 904.30 ± 402.55 | 0.101 | 1138.20 ± 342.50 | 1093.9 ± 380.36 | 0.45 |
| Mean Gain in Ridge Width (GRW) in mm | 1.46 ± 0.95 | 2.14 ± 1.65 | 0.27 | |||
| Change in Bone Density (CBD) in HU | −136.40 ± 236.08 | −44.30 ± 180.89 | 0.29 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akhil, K.P.; Pramashivaiah, R.; Prabhuji, M.L.V.; Tasleem, R.; Almubarak, H.; Bahamdan, G.K.; Luke, A.M.; Shetty, K.P.; Snigdha, N.T.; Bhavikatti, S.K. Alveolar Ridge Augmentation Assessment Using a Minimalistic Approach, with and without Low-Level Laser Therapy (LLLT)—A Comparative Clinical Trial. Medicina 2023, 59, 1178. https://doi.org/10.3390/medicina59061178
Akhil KP, Pramashivaiah R, Prabhuji MLV, Tasleem R, Almubarak H, Bahamdan GK, Luke AM, Shetty KP, Snigdha NT, Bhavikatti SK. Alveolar Ridge Augmentation Assessment Using a Minimalistic Approach, with and without Low-Level Laser Therapy (LLLT)—A Comparative Clinical Trial. Medicina. 2023; 59(6):1178. https://doi.org/10.3390/medicina59061178
Chicago/Turabian StyleAkhil, K. Padmanabhan, Rashmi Pramashivaiah, Munivenkatappa Laxmaiah Venkatesh Prabhuji, Robina Tasleem, Hussain Almubarak, Ghadah Khaled Bahamdan, Alexander Maniangat Luke, Krishna Prasad Shetty, Niher Tabassum Snigdha, and Shaeesta Khaleelahmed Bhavikatti. 2023. "Alveolar Ridge Augmentation Assessment Using a Minimalistic Approach, with and without Low-Level Laser Therapy (LLLT)—A Comparative Clinical Trial" Medicina 59, no. 6: 1178. https://doi.org/10.3390/medicina59061178
APA StyleAkhil, K. P., Pramashivaiah, R., Prabhuji, M. L. V., Tasleem, R., Almubarak, H., Bahamdan, G. K., Luke, A. M., Shetty, K. P., Snigdha, N. T., & Bhavikatti, S. K. (2023). Alveolar Ridge Augmentation Assessment Using a Minimalistic Approach, with and without Low-Level Laser Therapy (LLLT)—A Comparative Clinical Trial. Medicina, 59(6), 1178. https://doi.org/10.3390/medicina59061178