
Quantitative Electroencephalography Markers for an Accurate Diagnosis of Frontotemporal Dementia: A Spectral Power Ratio Approach


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. EEG Acquisition and Preprocessing
2.3. Spectral Analysis
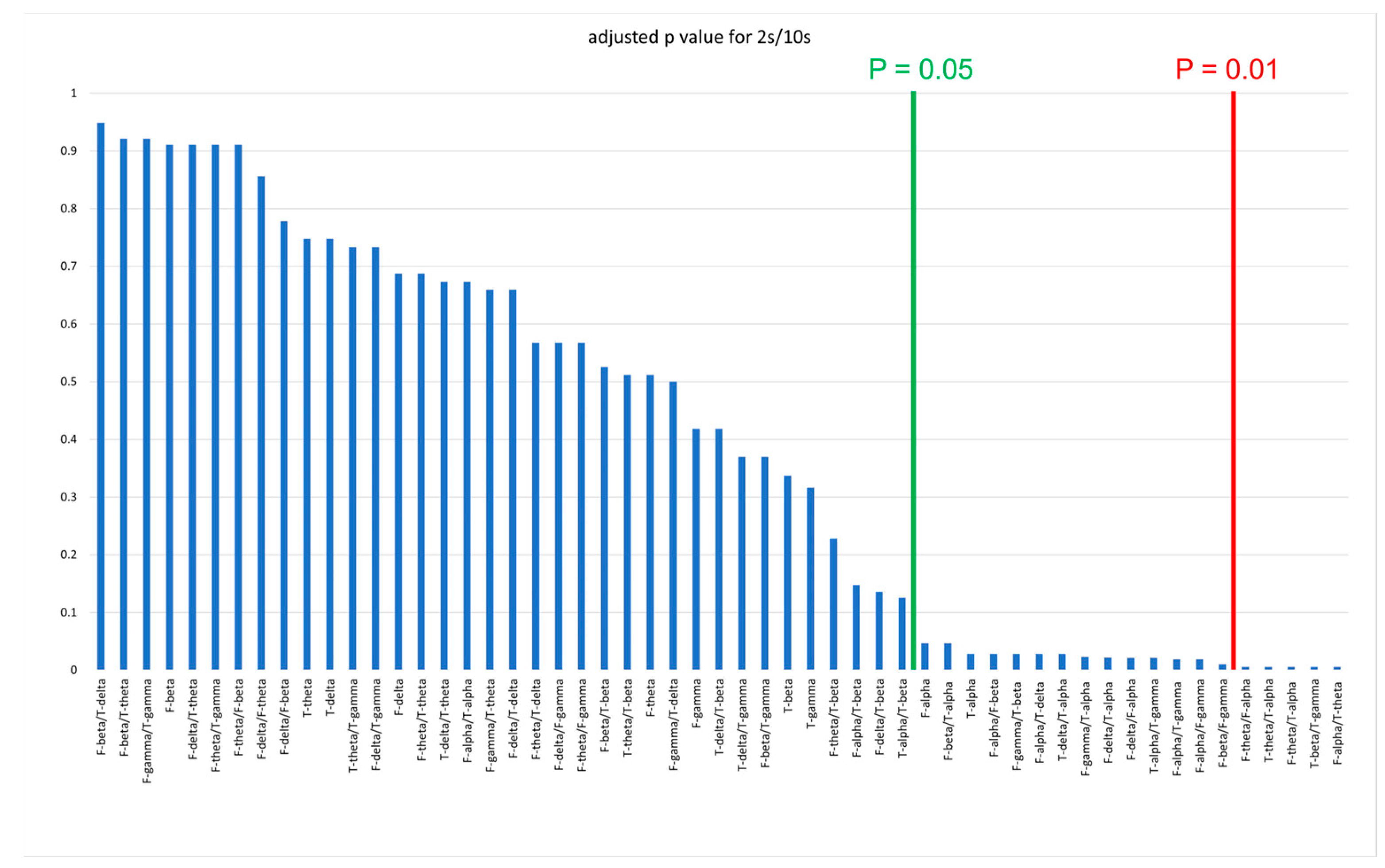
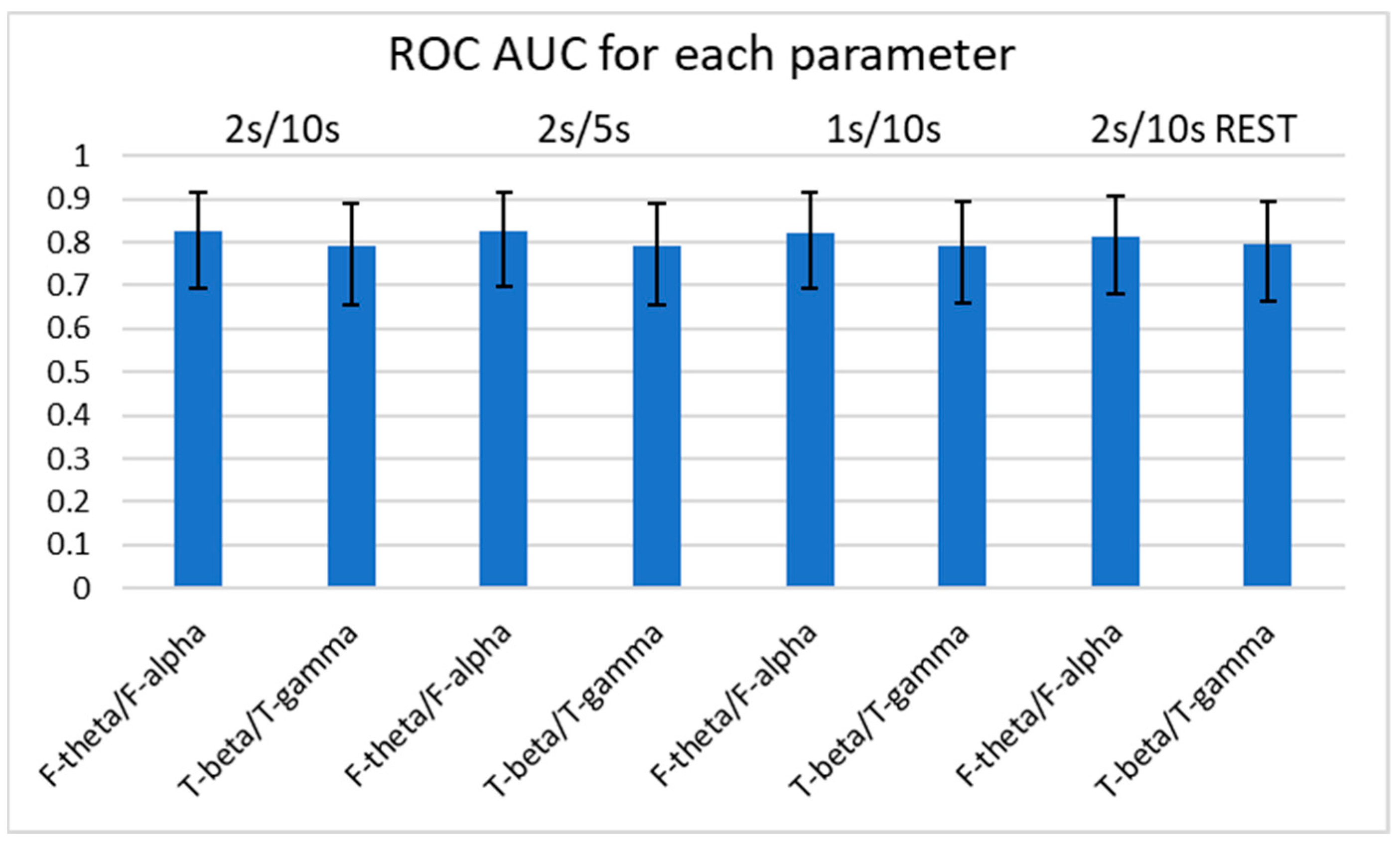
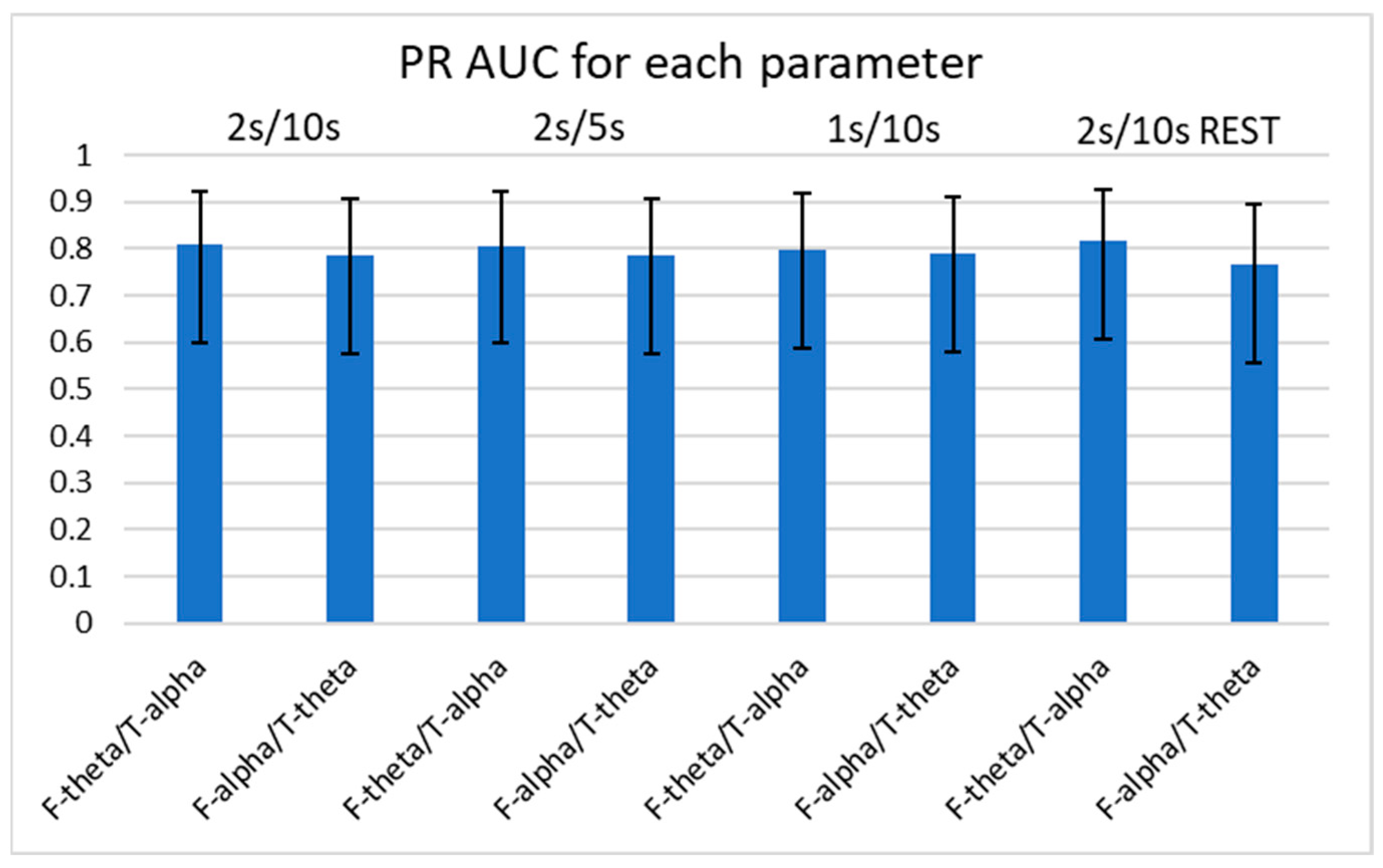
2.4. Statistical Analysis
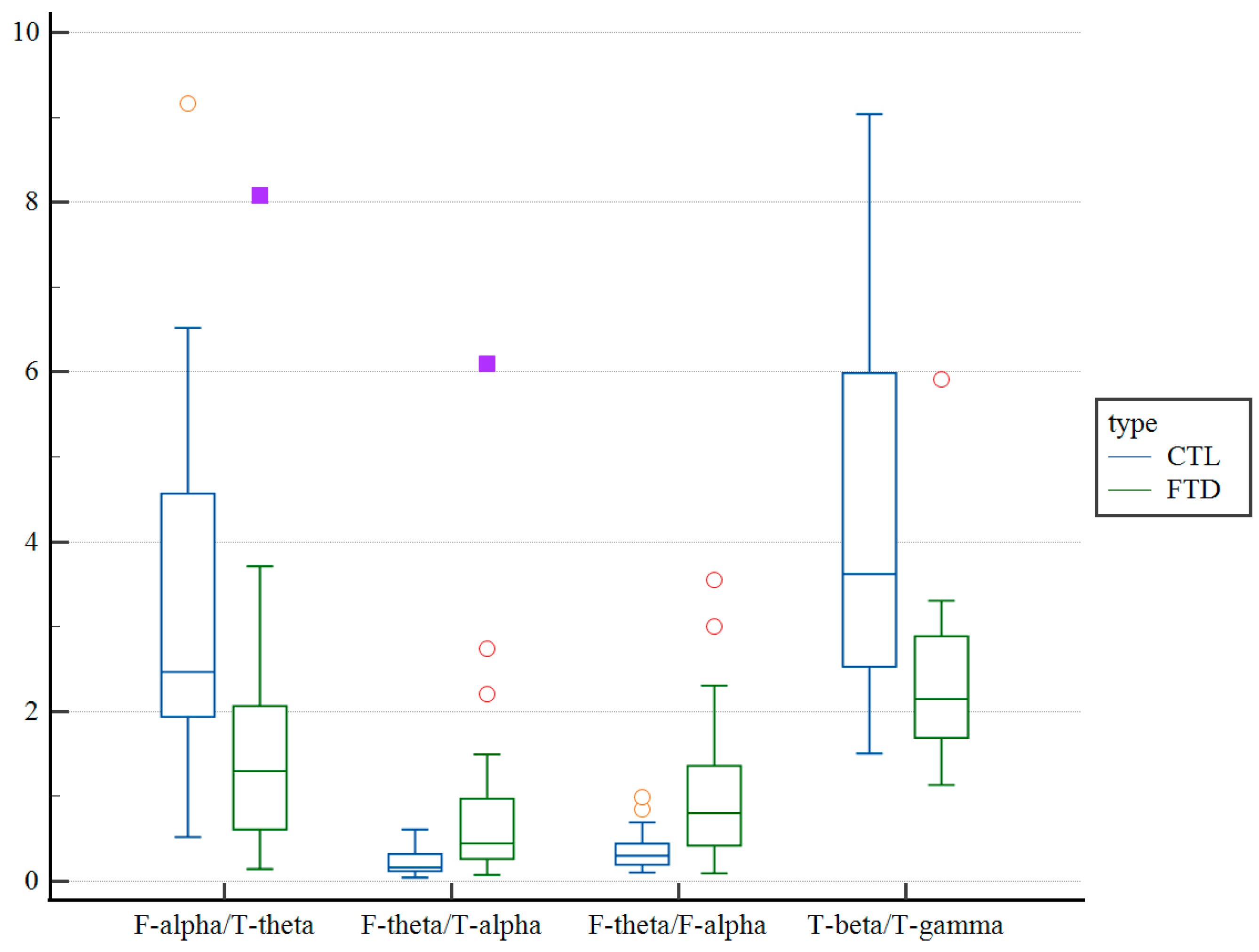
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hogan, D.B.; Jetté, N.; Fiest, K.M.; Roberts, J.I.; Pearson, D.; Smith, E.E.; Roach, P.; Kirk, A.; Pringsheim, T.; Maxwell, C.J. The prevalence and incidence of frontotemporal dementia: A systematic review. Can. J. Neurol. Sci. 2016, 43 (Suppl. S1), S96–S109. [Google Scholar] [CrossRef] [PubMed]
- Mayeux, R.; Stern, Y. Epidemiology of Alzheimer disease. Cold Spring Harb. Perspect. Med. 2012, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Woolley, J.D.; Khan, B.K.; Murthy, N.K.; Miller, B.L.; Rankin, K.P. The diagnostic challenge of psychiatric symptoms in neurodegenerative disease: Rates of and risk factors for prior psychiatric diagnosis in patients with early neurodegenerative disease. J. Clin. Psychiatry 2011, 72, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Nardone, R.; Sebastianelli, L.; Versace, V.; Saltuari, L.; Lochner, P.; Frey, V.; Golaszewski, S.; Brigo, F.; Trinka, E.; Höller, Y. Usefulness of EEG techniques in distinguishing frontotemporal dementia from Alzheimer’s disease and other dementias. Dis. Markers 2018, 2018, 6581490. [Google Scholar] [CrossRef] [PubMed]
- Lindau, M.; Jelic, V.; Johansson, S.E.; Andersen, C.; Wahlund, L.O.; Almkvist, O. Quantitative EEG abnormalities and cognitive dysfunctions in frontotemporal dementia and Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2003, 15, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Nishida, K.; Yoshimura, M.; Isotani, T.; Yoshida, T.; Kitaura, Y.; Saito, A.; Mii, H.; Kato, M.; Makekita, M.Y.; Suwa, A.; et al. Differences in quantitative EEG between frontotemporal dementia and Alzheimer’s disease as revealed by LORETA. Clin. Neurophysiol. 2011, 122, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Yener, G.G.; Leuchter, A.F.; Jenden, D.; Read, S.L.; Cummings, J.L.; Miller, B.L. Quantitative EEG in frontotemporal dementia. Clin. Electroencephalogr. 1996, 27, 61–68. [Google Scholar] [CrossRef]
- Stigsby, B.; Jóhannesson, G.; Ingvar, D.H. Regional EEG analysis and regional cerebral blood flow in Alzheimer’s and Pick’s diseases. Electroencephalogr. Clin. Neurophysiol. 1981, 51, 537–547. [Google Scholar] [CrossRef]
- Caso, F.; Cursi, M.; Magnani, G.; Fanelli, G.; Falautano, M.; Comi, G.; Leocani, L.; Minicucci, F. Quantitative EEG and LORETA: Valuable tools in discerning FTD from AD. Neurobiol. Aging 2012, 33, 2343–2356. [Google Scholar] [CrossRef]
- Newson, J.J.; Thiagarajan, T.C. EEG frequency bands in psychiatric disorders: A review of resting state studies. Front. Hum. Neurosci. 2018, 12, 521. [Google Scholar] [CrossRef] [PubMed]
- Pijnenburg, Y.A.L.; Strijers, R.L.M.; Made, Y.V.; van der Flier, W.M.; Scheltens, P.; Stam, C.J. Investigation of resting-state EEG functional connectivity in frontotemporal lobar degeneration. Clin. Neurophysiol. 2008, 119, 1732–1738. [Google Scholar] [CrossRef] [PubMed]
- de Haan, W.; Pijnenburg, Y.A.; Strijers, R.L.; van der Made, Y.; van der Flier, W.M.; Scheltens, P.; Stam, C.J. Functional neural network analysis in frontotemporal dementia and Alzheimer’s disease using EEG and graph theory. BMC Neurosci. 2009, 10, 101. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Gouw, A.A.; Hillebrand, A.; Tijms, B.M.; Stam, C.J.; van Straaten, E.C.; Pijnenburg, Y.A. Different functional connectivity and network topology in behavioral variant of frontotemporal dementia and Alzheimer’s disease: An EEG study. Neurobiol. Aging 2006, 42, 150–162. [Google Scholar] [CrossRef]
- Dottori, M.; Sedeño, L.; Martorell Caro, M.; Alifano, F.; Hesse, E.; Mikulan, E.; García, A.M.; Ruiz-Tagle, A.; Lillo, P.; Slachevsky, A.; et al. Towards affordable biomarkers of frontotemporal dementia: A classification study via network’s information sharing. Sci. Rep. 2017, 7, 3822. [Google Scholar] [CrossRef] [PubMed]
- Bastos, A.M.; Schoffelen, J.M. A tutorial review of functional connectivity analysis methods and their interpretational pitfalls. Front. Syst. Neurosci. 2015, 9, 175. [Google Scholar]
- Vink, J.J.T.; Klooster, D.C.W.; Ozdemir, R.A.; Westover, M.B.; Pascual-Leone, A.; Shafi, M.M. EEG Functional Connectivity is a Weak Predictor of Causal Brain Interactions. Brain Topogr. 2020, 33, 221–237. [Google Scholar] [CrossRef] [PubMed]
- Passant, U.; Rosén, I.; Gustafson, L.; Englund, E. The heterogeneity of frontotemporal dementia with regard to initial symptoms, qEEG and neuropathology. Int. J. Geriatric. Psych. 2005, 20, 983–988. [Google Scholar] [CrossRef]
- Julin, P.; Wahlund, L.O.; Basun, H.; Persson, A.; Måre, K.; Rudberg, U. Clinical diagnosis of frontal lobe dementia and Alzheimer’s disease: Relation to cerebral perfusion, brain atrophy and electroencephalography. Dementia 1995, 6, 142–147. [Google Scholar] [CrossRef]
- Johannesson, G.; Hagberg, B.; Gustafson, L.; Ingvar, D.H. EEG and cognitive impairment in presenile dementia. Acta Neurol. Scand. 1979, 59, 225–240. [Google Scholar] [CrossRef]
- Rosén, I.; Gustafson, L.; Risberg, J. Multichannel EEG frequency analysis and somatosensory-evoked potentials in patients with different types of organic dementia. Dementia 1993, 4, 43–49. [Google Scholar] [CrossRef]
- Olney, N.T.; Spina, S.; Miller, B.L. Frontotemporal Dementia. Neurol. Clin. 2017, 35, 339–374. [Google Scholar] [CrossRef] [PubMed]
- Thammasan, N.; Miyakoshi, M. Cross-frequency power-power coupling analysis: A useful cross-frequency measure to classify ICA-decomposed EEG. Sensors 2020, 20, 7040. [Google Scholar] [CrossRef] [PubMed]
- Wen, T.Y.; Aris, S.M. Electroencephalogram (EEG) stress analysis on alpha/beta ratio and theta/beta ratio. Indones. J. Electr. 2020, 17, 175–182. [Google Scholar]
- Schmidt, M.T.; Kanda, P.A.; Basile, L.F.; da Silva Lopes, H.F.; Baratho, R.; Demario, J.L.; Jorge, M.S.; Nardi, A.E.; Machado, S.; Ianof, J.N.; et al. Index of alpha/theta ratio of the electroencephalogram: A new marker for Alzheimer’s disease. Front. Aging Neurosci. 2013, 5, 60. [Google Scholar] [CrossRef] [PubMed]
- Özbek, Y.; Fide, E.; Yener, G.G. Resting-state EEG alpha/theta power ratio discriminates early-onset Alzheimer’s disease from healthy controls. Clin. Neurophysiol. 2021, 132, 2019–2031. [Google Scholar] [CrossRef]
- Baik, K.; Jung, J.H.; Jeong, S.H.; Chung, S.J.; Yoo, H.S.; Lee, P.H.; Sohn, Y.H.; Kang, S.W.; Ye, B.S. Implication of EEG theta/alpha and theta/beta ratio in Alzheimer’s and Lewy body disease. Sci. Rep. 2022, 12, 18706. [Google Scholar] [CrossRef]
- Jaramillo-Jimenez, A.; Suarez-Revelo, J.X.; Ochoa-Gomez, J.F.; Carmona Arroyave, J.A.; Bocanegra, Y.; Lopera, F.; Buriticá, O.; Pineda-Salazar, D.A.; Moreno Gómez, L.; Tobón Quintero, C.A.; et al. Resting-state EEG alpha/theta ratio related to neuropsychological test performance in Parkinson’s Disease. Clin. Neurophysiol. 2021, 132, 756–764. [Google Scholar] [CrossRef]
- Zawiślak-Fornagiel, K.; Ledwoń, D.; Bugdol, M.; Romaniszyn-Kania, P.; Małecki, A.; Gorzkowska, A.; Mitas, A.W. The increase of theta power and decrease of alpha/theta ratio as a manifestation of cognitive impairment in parkinson’s disease. J. Clin. Med. 2023, 12, 1569. [Google Scholar] [CrossRef]
- Miltiadous, A.; Tzimourta, K.D.; Afrantou, T.; Ioannidis, P.; Grigoriadis, N.; Tsalikakis, D.G.; Angelidis, P.; Tsipouras, M.G.; Glavas, E.; Giannakeas, N.; et al. A Dataset of Scalp EEG Recordings of Alzheimer’s Disease, Frontotemporal Dementia and Healthy Subjects from Routine EEG. Data 2023, 8, 95. [Google Scholar] [CrossRef]
- Miltiadous, A.; Tzimourta, K.D.; Giannakeas, N.; Tsipouras, M.G.; Afrantou, T.; Ioannidis, P.; Tzallas, A.T. Alzheimer’s disease and frontotemporal dementia: A robust classification method of EEG signals and a comparison of validation methods. Diagnostics 2021, 11, 1437. [Google Scholar] [CrossRef]
- Miltiadous, A.; Tzimourta, K.D.; Afrantou, T.; Ioannidis, P.; Grigoriadis, N.; Tsalikakis, D.G.; Angelidis, P.; Tsipouras, M.G.; Glavas, E.; Giannakeas, N.; et al. A Dataset of EEG Recordings from: Alzheimer’s Disease, Frontotemporal Dementia and Healthy Subjects. OpenNeuro 2023. Available online: https://openneuro.org/datasets/ds004504/versions/1.0.2/file-display/README (accessed on 10 November 2023).
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Miyakoshi, M.; Kothe, C. Clean_Rawdata. Version 2.1. 2019. Available online: https://github.com/sccn/clean_rawdata/wiki (accessed on 5 December 2023).
- Dong, L.; Li, F.; Liu, Q.; Wen, X.; Lai, Y.; Xu, P.; Yao, D. MATLAB Toolboxes for Reference Electrode Standardization Technique (REST) of Scalp EEG. Front. Neurosci. 2017, 11, 601. [Google Scholar] [CrossRef] [PubMed]
- Yao, D.; Qin, Y.; Hu, S.; Dong, L.; Bringas Vega, M.L.; Valdés Sosa, P.A. Which Reference Should We Use for EEG and ERP practice? Brain Topogr. 2019, 32, 530–549. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Boyd, K.; Eng, K.H.; Page, C.D. Area under the Precision-Recall Curve: Point Estimates and Confidence Intervals. Adv. Inf. Syst. Eng. 2013, 8190, 451–466. [Google Scholar]
- Davis, J.; Goadrich, M. The relationship between Precision-Recall and ROC curves. In Proceedings of the 23rd International Conference on Machine Learning, Pittsburgh, PA, USA, 25–29 June 2006; ACM Press Association for Computing Machinery: New York, NY, USA, 2006; pp. 233–240. [Google Scholar]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Trevethan, R. Sensitivity, specificity, and predictive values: Foundations, pliabilities, and pitfalls in research and practice. Front. Public Health 2017, 5, 307. [Google Scholar] [CrossRef]
- Heston, T.F. Standardizing predictive values in diagnostic imaging research. J. Magn. Reson. Imaging 2011, 33, 505, author reply 506–507. [Google Scholar] [CrossRef]
- Simundic, A.M. Diagnostic accuracy-part 1: Basic concepts: Sensitivity and specificity, ROC analysis, STARD statement. Point Care 2012, 11, 6–8. [Google Scholar] [CrossRef]
- García-Cordero, I.; Sedeño, L.; Fraiman, D.; Craiem, D.; de la Fuente, L.A.; Salamone, P.; Serrano, C.; Sposato, L.; Manes, F.; Ibañez, A. Stroke and Neurodegeneration Induce Different Connectivity Aberrations in the Insula. Stroke 2015, 46, 2673–2677. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W.; Crawford, R.; Rascovsky, K.; Kramer, J.H.; Weiner, M.; Miller, B.L.; Gorno-Tempini, M.L. Frontal paralimbic network atrophy in very mild behavioral variant frontotemporal dementia. Arch. Neurol. 2008, 65, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Melloni, M.; Billeke, P.; Baez, S.; Hesse, E.; de la Fuente, L.; Forno, G.; Birba, A.; García-Cordero, I.; Serrano, C.; Plastino, A.; et al. Your perspective and my benefit: Multiple lesion models of self-other integration strategies during social bargaining. Brain 2016, 139, 3022–3040. [Google Scholar] [CrossRef] [PubMed]
- Agosta, F.; Sala, S.; Valsasina, P.; Meani, A.; Canu, E.; Magnani, G.; Cappa, S.F.; Scola, E.; Quatto, P.; Horsfield, M.A.; et al. Brain network connectivity assessed using graph theory in frontotemporal dementia. Neurology 2013, 81, 134–343. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Sato, W.; Toichi, M.; Murai, T.; Okada, T.; Hayashi, A.; Sengoku, A. Frontal midline theta rhythm is correlated with cardiac autonomic activities during the performance of an attention demanding meditation procedure. Brain Res. Cogn. Brain Res. 2001, 11, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Robles Bayón, A.; Gude Sampedro, F.; Torregrosa Quesada, J.M. Bradycardia in frontotemporal dementia. Neurología 2014, 29, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Schreckenberger, M.; Lange-Asschenfeldt, C.; Lochmann, M.; Mann, K.; Siessmeier, T.; Buchholz, H.G.; Bartenstein, P.; Gründer, G. The thalamus as the generator and modulator of EEG alpha rhythm: A combined PET/EEG study with lorazepam challenge in humans. NeuroImage 2004, 22, 637–644. [Google Scholar] [CrossRef]
- Garrett, L.R.; Niccoli, T. Frontotemporal dementia and glucose metabolism. Front. Neurosci. 2022, 16, 812222. [Google Scholar] [CrossRef]
- Goldman, R.I.; Stern, J.M.; Engel, J.; Cohen, M.S. Simultaneous EEG and fMRI of the alpha rhythm. Neuroreport 2002, 13, 2487–2492. [Google Scholar] [CrossRef]
- Hughes, S.W.; Crunelli, V. Thalamic mechanisms of EEG alpha rhythms and their pathological implications. Neuroscientist 2005, 11, 357–372. [Google Scholar] [CrossRef]
- Bocchetta, M.; Gordon, E.; Cardoso, M.J.; Modat, M.; Ourselin, S.; Warren, J.D.; Rohrer, J.D. Thalamic atrophy in frontotemporal dementia—Not just a C9orf72 problem. NeuroImage Clin. 2018, 18, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Fries, P.; Reynolds, J.H.; Rorie, A.E.; Desimone, R. Modulation of oscillatory neuronal synchronization by selective visual attention. Science 2001, 291, 1560–1563. [Google Scholar] [CrossRef] [PubMed]
- Laakso, M.P.; Frisoni, G.B.; Könönen, M.; Mikkonen, M.; Beltramello, A.; Geroldi, C.; Bianchetti, A.; Trabucchi, M.; Soininen, H.; Aronen, H.J. Hippocampus and entorhinal cortex in frontotemporal dementia and Alzheimer’s disease: A morphometric MRI study. Biol. Psychiatry 2000, 47, 1056–1063. [Google Scholar] [CrossRef] [PubMed]
- Ribary, U.; Ioannides, A.A.; Singh, K.D.; Hasson, R.; Bolton, J.P.; Lado, F.; Mogilner, A.; Llinás, R. Magnetic field tomography of coherent thalamocortical 40-Hz oscillations in humans. Proc. Natl. Acad. Sci. USA 1991, 88, 11037–11041. [Google Scholar] [CrossRef]
- Cotelli, M.; Adenzato, M.; Cantoni, V.; Manenti, R.; Alberici, A.; Enrici, I.; Benussi, A.; Dell’Era, V.; Bonetta, E.; Padovani, A.; et al. Enhancing theory of mind in behavioural variant frontotemporal dementia with transcranial direct current stimulation. Cogn. Affect. Behav. Neurosci. 2018, 18, 1065–1075. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, H.; Sohn, J.; Choi, J.; Kim, S. EEG Beta Oscillations in the Temporoparietal Area Related to the Accuracy in Estimating Others’ Preference. Front. Hum. Neurosci. 2018, 12, 43. [Google Scholar] [CrossRef]
- Helm, K.; Viol, K.; Weiger, T.M.; Tass, P.A.; Grefkes, C.; Del Monte, D.; Schiepek, G. Neuronal connectivity in major depressive disorder: A systematic review. Neuropsychiat. Dis. Treat. 2018, 14, 2715–2737. [Google Scholar] [CrossRef]
- Stopford, C.L.; Thompson, J.C.; Neary, D.; Richardson, A.M.; Snowden, J.S. Working memory, attention, and executive function in Alzheimer’s disease and frontotemporal dementia. Cortex 2012, 48, 429–446. [Google Scholar] [CrossRef]
- Ramanan, S.; El-Omar, H.; Roquet, D.; Ahmed, R.M.; Hodges, J.R.; Piguet, O.; Lambon Ralph, M.A.; Irish, M. Mapping behavioural, cognitive and affective transdiagnostic dimensions in frontotemporal dementia. Brain Commun. 2023, 5, fcac344. [Google Scholar] [CrossRef]
- Murley, A.G.; Coyle-Gilchrist, I.; Rouse, M.A.; Jones, P.S.; Li, W.; Wiggins, J.; Lansdall, C.; Rodríguez, P.V.; Wilcox, A.; Tsvetanov, K.A.; et al. Redefining the multidimensional clinical phenotypes of frontotemporal lobar degeneration syndromes. Brain J. Neurol. 2020, 143, 1555–1571. [Google Scholar] [CrossRef]
- Walters, G.D. Dementia: Continuum or distinct entity? Psychol. Aging 2010, 25, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Kane, N.; Acharya, J.; Benickzy, S.; Caboclo, L.; Finnigan, S.; Kaplan, P.W.; Shibasaki, H.; Pressler, R.; van Putten, M.J.A.M. A revised glossary of terms most commonly used by clinical electroencephalographers and updated proposal for the report format of the EEG findings. Revision 2017. Clin. Neurophysiol. Pract. 2017, 2, 170–185. [Google Scholar] [CrossRef] [PubMed]
- Klug, M.; Gramann, K. Identifying key factors for improving ICA-based decomposition of EEG data in mobile and stationary experiments. Eur. J. Neurosci. 2021, 54, 8406–8420. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FTD Group | CTL Group | Significance | |
|---|---|---|---|
| MMSE | 22.17 (8.22) | 30 (0) | p < 0.001 |
| Age | 63.6 (8.2) | 67.9 (5.4) | p = 0.068 |
| Sex | 0.39 | 0.38 | p = 0.930 |
| 2 s/10 s | 2 s/5 s | 1 s/10 s | 2 s/10 s REST | |||||
|---|---|---|---|---|---|---|---|---|
| F-Theta/T-Alpha | F-Alpha/T-Theta | F-Theta/T-Alpha | F-Alpha/T-Theta | F-Theta/T-Alpha | F-Alpha/T-Theta | F-Theta/T-Alpha | F-Alpha/T-Theta | |
| Cutoff | >0.35 (0.16–0.61) | ≤1.60 (1.44–5.12) | >0.35 (0.16–0.61) | ≤1.60 (1.44–5.12) | >0.37 (0.18–0.63) | ≤1.43 (0.77–1.79) | >0.24 (>0.12–0.36) | ≤1.48 (1.30–4.92) |
| Sensitivity (%) | 69.6 (47.1–86.8) | 69.6 (47.1–86.8) | 69.6 (47.1–86.8) | 69.6 (47.1–86.8) | 69.6 (47.1–86.8) | 65.2 (42.7–83.6 | 78.3 (56.3–92.5) | 73.9 (51.6–89.8) |
| Specificity (%) | 79.3 (60.3–92.0) | 86.2 (68.3–96.1) | 79.3 (60.3–92.0) | 86.2 (68.3–96.1) | 79.3 (60.3–92.0) | 89.7 (72.6–97.8) | 72.4 (52.8–87.3) | 75.9 (56.5–89.7) |
| Youden’s Index | 0.489 (0.260–0.619) | 0.558 (0.305–0.739) | 0.489 (0.255–0.619) | 0.558 (0.305–0.739) | 0.489 (0.250–0.636) | 0.549 (0.286–0.706) | 0.507 (0.261–0.636) | 0.498 (0.224–0.670) |
| PPV (%) | 77.1 (61.1–87.8) | 83.5 (66.1–92.9) | 77.1 (61.1–87.8) | 83.5 (66.1–92.9) | 77.1 (61.1–87.8) | 86.3 (67.5–95.0) | 73.9 (60.2–84.2) | 75.4 (60.6–85.9) |
| NPV (%) | 72.3 (57.8–83.2) | 73.9 (60.0–84.2) | 72.3 (57.8–83.2) | 73.9 (60.0–84.2) | 72.3 (57.8–83.2) | 72 (59.2–82.1) | 76.9 (59.8–88.2) | 74.4 (58.7–85.6) |
| 2 s/10 s | 2 s/5 s | 1 s/10 s | 2 s/10 s REST | |||||
|---|---|---|---|---|---|---|---|---|
| F-Theta/F-Alpha | T-Beta/T-Gamma | F-Theta/F-Alpha | T-Beta/T-Gamma | F-Theta/F-Alpha | T-Beta/T-Gamma | F-Theta/F-Alpha | T-Beta/T-Gamma | |
| Cutoff | >0.56 (0.25–0.70) | ≤3.31 (2.98–5.91) | >0.56 (0.25–0.70) | ≤3.31 (2.98–5.91) | >0.60 (0.27–0.86) | ≤3.34 (3.11–5.96) | >0.65 (0.37–1.02) | ≤3.30 (2.91–5.71) |
| Sensitivity (%) | 69.6 (47.1–86.8) | 95.7 (78.1–99.9) | 69.6 (47.1–86.8) | 95.7 (78.1–99.9) | 69.6 (47.1–86.8) | 95.7 (78.1–99.9) | 65.2 (42.7–83.6) | 95.7 (78.1–99.9) |
| Specificity (%) | 86.2 (68.3–96.1) | 55.2 (35.7–73.6) | 86.2 (68.3–96.1) | 55.2 (35.7–73.6) | 86.2 (68.3–96.1) | 55.2 (35.7–73.6) | 86.2 (68.3–96.1) | 55.2 (35.7–73.6) |
| Youden’s Index | 0.558 (0.298–0.705) | 0.508 (0.258–0.655) | 0.558 (0.298–0.697) | 0.508 (0.258–0.655) | 0.558 (0.298–0.705) | 0.508 (0.233–0.646) | 0.514 (0.264–0.636) | 0.508 (0.244–0.652) |
| PPV (%) | 83.5 (66.1–92.9) | 68.1 (58.5–76.3) | 83.5 (66.1–92.9) | 68.1 (58.5–76.3) | 83.5 (66.1–92.9) | 68.1 (58.5–76.3) | 82.5 (64.5–92.5) | 68.1 (58.5–76.3) |
| NPV (%) | 73.9 (60.0–84.2) | 92.7 (64.5–98.9) | 73.9 (60.0–84.2) | 92.7 (64.5–98.9) | 73.9 (60.0–84.2) | 92.7 (64.5–98.9) | 71.3 (58.2–81.5) | 92.7 (64.5–98.9) |
| 2 s/10 s | ||||||
| Wald | Coefficient | SE | OR | 95% CI | Accuracy | |
| F-theta/F-alpha | 9.641 | 3.947 | 1.271 | 51.782 | 4.287–625.529 | 76.92% |
| 2 s/5 s | ||||||
| Wald | Coefficient | SE | OR | 95% CI | Accuracy | |
| F-theta/F-alpha | 9.636 | 3.943 | 1.270 | 51.594 | 4.278–622.182 | 76.92% |
| 1 s/10 s | ||||||
| Wald | Coefficient | SE | OR | 95% CI | Accuracy | |
| F-theta/F-alpha | 9.646 | 3.851 | 1.240 | 47.020 | 4.140–534.080 | 76.92% |
| 2 s/10 s REST | ||||||
| Wald | Coefficient | SE | OR | 95% CI | Accuracy | |
| F-theta/F-alpha | 9.439 | 3.500 | 1.139 | 33.115 | 3.551–308.830 | 76.92% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, J.; Chang, C. Quantitative Electroencephalography Markers for an Accurate Diagnosis of Frontotemporal Dementia: A Spectral Power Ratio Approach. Medicina 2023, 59, 2155. https://doi.org/10.3390/medicina59122155
Chang J, Chang C. Quantitative Electroencephalography Markers for an Accurate Diagnosis of Frontotemporal Dementia: A Spectral Power Ratio Approach. Medicina. 2023; 59(12):2155. https://doi.org/10.3390/medicina59122155
Chicago/Turabian StyleChang, Jinwon, and Chul Chang. 2023. "Quantitative Electroencephalography Markers for an Accurate Diagnosis of Frontotemporal Dementia: A Spectral Power Ratio Approach" Medicina 59, no. 12: 2155. https://doi.org/10.3390/medicina59122155
APA StyleChang, J., & Chang, C. (2023). Quantitative Electroencephalography Markers for an Accurate Diagnosis of Frontotemporal Dementia: A Spectral Power Ratio Approach. Medicina, 59(12), 2155. https://doi.org/10.3390/medicina59122155