
Worsening Symptoms Is Associated with Larger Cerebral Blood Flow Abnormalities during Tilt-Testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
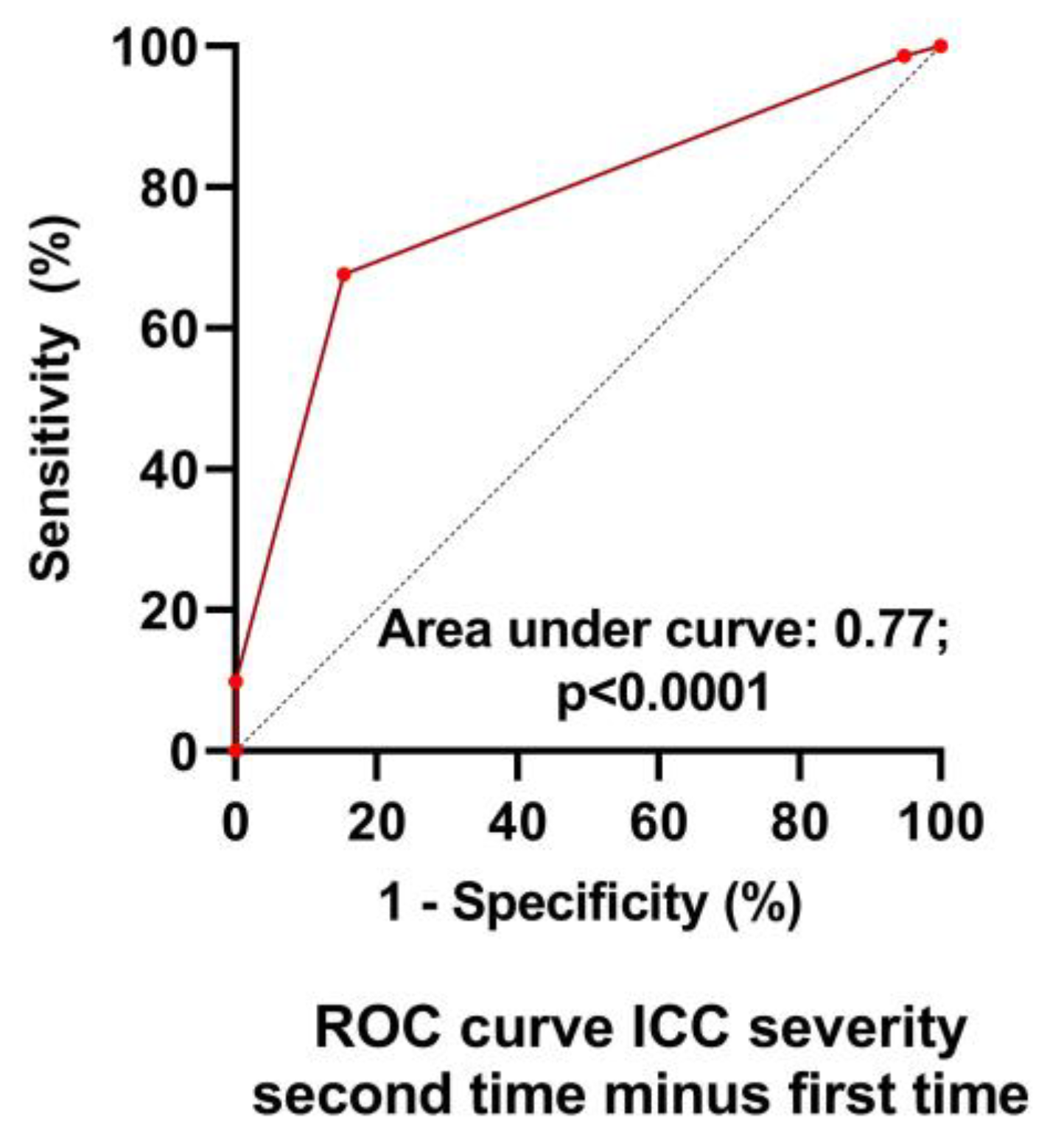
2.2. International Consensus Criteria (ICC) Severity of Disease
2.3. Tilt Test Protocol
2.4. Extracranial Doppler: Cerebral Blood Flow Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carruthers, B.M.; van de Sande, M.I.; Meirleir, K.L.D.E.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International consensus criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IOM). Beyond Mayalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a fatigue scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Sunnquist, M. The development of the depaul symptom questionnaire: Original, expanded, brief, and pediatric versions. Front. Pediatr. 2018, 6, 330. [Google Scholar] [CrossRef] [PubMed]
- Cotler, J.; Holtzman, C.; Dudun, C.; Jason, L.A. A brief questionnaire to assess post-exertional malaise. Diagnostics 2018, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Hewlett, S.; Dures, E.; Almeida, C. Measures of fatigue: Bristol rheumatoid arthritis fatigue multi-dimensional questionnaire (braf mdq), bristol rheumatoid arthritis fatigue numerical rating scales (braf nrs) for severity, effect, and coping, chalder fatigue questionnaire (cfq), checklist individual strength (cis20r and cis8r), fatigue severity scale (fss), functional assessment chronic illness therapy (fatigue) (facit-f), multi-dimensional assessment of fatigue (maf), multi-dimensional fatigue inventory (mfi), pediatric quality of life (pedsql) multi-dimensional fatigue scale, profile of fatigue (prof), short form 36 vitality subscale (sf-36 vt), and visual analog scales (vas). Arthritis Care Res. 2011, 63 (Suppl. S11), S263–S286. [Google Scholar] [CrossRef]
- Bell, D.S. Illness onset characteristics in children with chronic fatigue syndrome and idiopathic chronic fatigue. J. Chronic Fatigue Syndr. 1997, 3, 43–51. [Google Scholar] [CrossRef]
- Miwa, K. Variability of postural orthostatic tachycardia in patients with myalgic encephalomyelitis and orthostatic intolerance. Heart Vessel. 2016, 31, 1522–1528. [Google Scholar] [CrossRef]
- Sulheim, D.; Hurum, H.; Helland, I.B.; Thaulow, E.; Wyller, V.B. Adolescent chronic fatigue syndrome; a follow-up study displays concurrent improvement of circulatory abnormalities and clinical symptoms. Biopsychosoc. Med. 2012, 6, 10. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Heart rate thresholds to limit activity in myalgic encephalomyelitis/chronic fatigue syndrome patients (pacing): Comparison of heart rate formulae and measurements of the heart rate at the lactic acidosis threshold during cardiopulmonary exercise testing. Adv. Phys. Educ. 2020, 10, 138–154. [Google Scholar] [CrossRef]
- Escorihuela, R.M.; Capdevila, L.; Castro, J.R.; Zaragozà, M.C.; Maurel, S.; Alegre, J.; Castro-Marrero, J. Reduced heart rate variability predicts fatigue severity in individuals with chronic fatigue syndrome/myalgic encephalomyelitis. J. Transl. Med. 2020, 18, 4. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Verheugt, F.W.A.; Visser, F.C. Physical activity measures in patients with myalgic encephalomyalitis/chronic fatigue syndrome: Correlations between peak oxygen consumption, the physical functioning scale of the sf-36 scale, and the number of steps from an activity meter. J. Transl. Med. 2020, 18, 228–238. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Two-day cardiopulmonary exercise testing in females with a severe grade of myalgic encephalomyelitis/chronic fatigue syndrome: Comparison with patients with mild and moderate disease. Healthcare 2020, 8, 192. [Google Scholar] [CrossRef]
- Maksoud, R.; Magawa, C.; Eaton-Fitch, N.; Thapaliya, K.; Marshall-Gradisnik, S. Biomarkers for myalgic encephalomyelitis/chronic fatigue syndrome (me/cfs): A systematic review. BMC Med. 2023, 21, 189. [Google Scholar] [CrossRef] [PubMed]
- Nacul, L.C.; Mudie, K.; Kingdon, C.C.; Clark, T.G.; Lacerda, E.M. Hand grip strength as a clinical biomarker for me/cfs and disease severity. Front. Neurol. 2018, 9, 992. [Google Scholar] [CrossRef]
- Maksoud, R.; Preez, S.D.; Eaton-Fitch, N.; Thapaliya, K.; Barnden, L.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. A systematic review of neurological impairments in myalgic encephalomyelitis/chronic fatigue syndrome using neuroimaging techniques. PLoS ONE 2020, 15, e0232475. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.R.; Isaacson-Barash, C. Three cases of severe me/cfs in adults. Healthcare 2021, 9, 215. [Google Scholar] [CrossRef] [PubMed]
- Devendorf, A.R.; Brown, A.A.; Jason, L.A. Patients’ hopes for recovery from myalgic encephalomyelitis and chronic fatigue syndrome: Toward a “recovery in” framework. Chronic Illn. 2018, 16, 307–321. [Google Scholar] [CrossRef]
- Ghali, A.; Lacout, C.; Fortrat, J.-O.; Depres, K.; Ghali, M.; Lavigne, C. Factors influencing the prognosis of patients with myalgic encephalomyelitis/chronic fatigue syndrome. Diagnostics 2022, 12, 2540. [Google Scholar] [CrossRef]
- Low, P.A.; Sandroni, P.; Joyner, M.; Shen, W.K. Postural tachycardia syndrome (pots). J. Cardiovasc. Electrophysiol. 2009, 20, 352–358. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Verheugt, F.W.A.; Rowe, P.C.; Visser, F.C. Cerebral blood flow is reduced in me/cfs during head-up tilt testing even in the absence of hypotension or tachycardia: A quantitative, controlled study using doppler echography. Clin. Neurophysiol. Pr. Pract. 2020, 5, 50–58. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. The myalgic encephalomyelitis/chronic fatigue syndrome patients with joint hypermobility show larger cerebral blood flow reductions during orthostatic stress testing than patients without hypermobility: A case control study. Med. Res. Arch. 2021, 9. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Visser, F.C. Long-haul covid patients: Prevalence of pots are reduced but cerebral blood flow abnormalities remain abnormal with longer disease duration. Healthcare 2022, 10, 2105. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International chronic fatigue syndrome study group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Van Campen, C.L.M.C.; Verheugt, F.W.A.; Visser, F.C. Cerebral blood flow changes during tilt table testing in healthy volunteers, as assessed by doppler imaging of the carotid and vertebral arteries. Clin. Neurophysiol. Pract. 2018, 3, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Eeftinck Schattenkerk, D.W.; van Lieshout, J.J.; van den Meiracker, A.H.; Wesseling, K.R.; Blanc, S.; Wieling, W.; van Montfrans, G.A.; Settels, J.J.; Wesseling, K.H.; Westerhof, B.E. Nexfin noninvasive continuous blood pressure validated against riva-rocci/korotkoff. Am. J. Hypertens. 2009, 22, 378–383. [Google Scholar] [CrossRef]
- Martina, J.R.; Westerhof, B.E.; van Goudoever, J.; de Beaumont, E.M.; Truijen, J.; Kim, Y.S.; Immink, R.V.; Jobsis, D.A.; Hollmann, M.W.; Lahpor, J.R.; et al. Noninvasive continuous arterial blood pressure monitoring with nexfin(r). Anesthesiology 2012, 116, 1092–1103. [Google Scholar] [CrossRef]
- Fedorowski, A.; Burri, P.; Melander, O. Orthostatic hypotension in genetically related hypertensive and normotensive individuals. J. Hypertens. 2009, 27, 976–982. [Google Scholar] [CrossRef]
- Sheldon, R.S.; Grubb, B.P.; Olshansky, B.; Shen, W.K.; Calkins, H.; Brignole, M.; Raj, S.R.; Krahn, A.D.; Morillo, C.A.; Stewart, J.M.; et al. 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015, 12, e41–e63. [Google Scholar] [CrossRef]
- Freeman, R.; Wieling, W.; Axelrod, F.B.; Benditt, D.G.; Benarroch, E.; Biaggioni, I.; Cheshire, W.P.; Chelimsky, T.; Cortelli, P.; Gibbons, C.H.; et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton. Neurosci. 2011, 161, 46–48. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Cerebral blood flow is reduced in severe myalgic encephalomyelitis/chronic fatigue syndrome patients during mild orthostatic stress testing: An exploratory study at 20 degrees of head-up tilt testing. Healthcare 2020, 8, 169. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Reductions in cerebral blood flow can be provoked by sitting in severe myalgic encephalomyelitis/chronic fatigue syndrome patients. Healthcare 2020, 8, 394. [Google Scholar] [CrossRef]
- Medow, M.S.; Sood, S.; Messer, Z.; Dzogbeta, S.; Terilli, C.; Stewart, J.M. Phenylephrine alteration of cerebral blood flow during orthostasis: Effect on n-back performance in chronic fatigue syndrome. J. Appl. Physiol. 2014, 117, 1157–1164. [Google Scholar] [CrossRef]
- Shin, K.J.; Kim, S.E.; Park, K.M.; Park, J.; Ha, S.Y.; Kim, S.E.; Kwon, O.Y. Cerebral hemodynamics in orthostatic intolerance with normal head-up tilt test. Acta Neurol. Scand. 2016, 134, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Novak, P. Hypocapnic cerebral hypoperfusion: A biomarker of orthostatic intolerance. PLoS ONE 2018, 13, e0204419. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Verheugt, F.W.A.; Visser, F.C. Orthostatic stress testing in myalgic encephalomyelitis/chronic fatigue syndrome patients with or without concomitant fibromyalgia: Effects on pressure pain thresholds and temporal summation. Clin. Exp. Rheumatol. 2021, 39, 39–47. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Verheugt, F.W.A.; Visser, F.C. Cognitive function declines following orthostatic stress in adults with myalgic encephalomyelitis/chronic fatigue syndrome (me/cfs). Front. Neurosci. 2020, 14, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Van Campen, C.L.M.C.; Rowe, P.C.; Verheugt, F.W.A.; Visser, F.C. Numeric rating scales show prolonged post-exertional symptoms after orthostatic testing of adults with myalgic encephalomyelitis/chronic fatigue syndrome. Front. Med. 2021, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Van Campen, C.L.M.C.; Verheugt, F.W.A.; Visser, F.C. Quantification of the beneficial effects of compression stockings on symptoms of exercise and orthostatic intolerance in chronic fatigue/myalgic encephalomyelitis patients. Int. J. Clin. Med. 2018, 9, 367–376. [Google Scholar] [CrossRef][Green Version]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Compression stockings improve cardiac output and cerebral blood flow during tilt testing in myalgic encephalomyelitis/chronic fatigue syndrome (me/cfs) patients: A randomized crossover trial. Medicina 2021, 58, 51. [Google Scholar] [CrossRef]
- Streeten, D.H.; Thomas, D.; Bell, D.S. The roles of orthostatic hypotension, orthostatic tachycardia, and subnormal erythrocyte volume in the pathogenesis of the chronic fatigue syndrome. Am. J. Med. Sci. 2000, 320, 1–8. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Validation of the severity of myalgic encephalomyelitis/chronic fatigue syndrome by other measures than history: Activity bracelet, cardiopulmonary exercise testing and a validated activity questionnaire: Sf-36. Healthcare 2020, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Mathew, S.J.; Mao, X.; Keegan, K.A.; Levine, S.M.; Smith, E.L.; Heier, L.A.; Otcheretko, V.; Coplan, J.D.; Shungu, D.C. Ventricular cerebrospinal fluid lactate is increased in chronic fatigue syndrome compared with generalized anxiety disorder: An in vivo 3.0 t (1)h mrs imaging study. NMR Biomed. 2009, 22, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Murrough, J.W.; Mao, X.; Collins, K.A.; Kelly, C.; Andrade, G.; Nestadt, P.; Levine, S.M.; Mathew, S.J.; Shungu, D.C. Increased ventricular lactate in chronic fatigue syndrome measured by 1h mrs imaging at 3.0 t. Ii: Comparison with major depressive disorder. NMR Biomed. 2010, 23, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Wallis, A.; Ball, M.; McKechnie, S.; Butt, H.; Lewis, D.P.; Bruck, D. Examining clinical similarities between myalgic encephalomyelitis/chronic fatigue syndrome and d-lactic acidosis: A systematic review. J. Transl. Med. 2017, 15, 129. [Google Scholar] [CrossRef] [PubMed]
- McHenry, L.C., Jr.; Fazekas, J.F.; Sullivan, J.F. Cerebral hemodynamics of syncope. Am. J. Med. Sci. 1961, 241, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Finnerty, F.A., Jr.; Witkin, L.; Fazekas, J.F. Cerebral hemodynamics during cerebral ischemia induced by acute hypotension. J. Clin. Invest. 1954, 33, 1227–1232. [Google Scholar] [CrossRef]
- Lewis, N.C.; Bain, A.R.; MacLeod, D.B.; Wildfong, K.W.; Smith, K.J.; Willie, C.K.; Sanders, M.L.; Numan, T.; Morrison, S.A.; Foster, G.E.; et al. Impact of hypocapnia and cerebral perfusion on orthostatic tolerance. J. Physiol. 2014, 592, 5203–5219. [Google Scholar] [CrossRef]
- Kloner, R.A. Stunned and hibernating myocardium: Where are we nearly 4 decades later? J. Am. Heart Assoc. 2020, 9, e015502. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Cerebral blood flow remains reduced after tilt testing in myalgic encephalomyelitis/chronic fatigue syndrome patients. Clin. Neurophysiol. Pract. 2021, 6, 245–255. [Google Scholar] [CrossRef]
- Biswal, B.; Kunwar, P.; Natelson, B.H. Cerebral blood flow is reduced in chronic fatigue syndrome as assessed by arterial spin labeling. J. Neurol. Sci. 2011, 301, 9–11. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Change (n = 39) | Worsening (n = 71) | p-Value | |
|---|---|---|---|
| Male/female * | 6/33 | 11/60 | 0.82 |
| Age (years) | 42 (13) | 39 (12) | 0.13 |
| Height (cm) | 171 (7) | 172 (8) | 0.35 |
| Weight (kg) # | 70 (59–85) | 73 (62–85) | 0.29 |
| BMI (kg/m2) # | 24.2 (20.3–27.7) | 24.0 (21–29.4) | 0.46 |
| BSA (m2) | 1.83 (0.20) | 1.87 (0.20) | 0.22 |
| Disease duration (years) # | 8 (3–13) | 11 (6–21) | 0.054 |
| No Change (n = 39) | Worsening (n = 71) | p-Value | |
|---|---|---|---|
| Test 1: mild/moderate/severe * | 14/20/5 (36/51/13%) | 36/32/3 (51/45/4%) | 0.004 |
| Test 2: mild/moderate/severe * | 13/19/7 (33/49/18%) | 1/51/19 (1/72/27%) | <0.0001 |
| No Change (n = 39) | Worsening (n = 71) | p-Value | |
|---|---|---|---|
| Hemodynamic result tilt test (normHRBP/OH/POTS) | 26/7/6 (67/18/15%) | 47/4/17 (69/6/25%) | 0.10 |
| HR supine (bpm) | 70 (11) | 71 (11) | 0.78 |
| HR end-tilt (bpm) | 88 (17) | 92 (16) | 0.28 |
| SBP supine (mmHg) | 139 (22) | 132 (23) | 0.11 |
| SBP end-tilt (mmHg) | 132 (22) | 131 (18) | 0.73 |
| DBP supine (mmHg) | 81 (11) | 78 (12) | 0.18 |
| DBP end-tilt (mmHg) | 86 (14) | 85 (9) | 0.64 |
| CBF supine (mL/min) | 608 (90) | 605 (103) | 0.88 |
| CBF end-tilt (mL/min) | 463 (78) | 494 (108) | 0.12 |
| %CBF reduction (%) | 24 (9) | 19 (10) | 0.01 |
| No Change (n = 39) | Worsening (n = 71) | p-Value | |
|---|---|---|---|
| Hemodynamic result tilt test (normHRBP/OH/POTS) | 28/4/7 (72/10/18%) | 41/8/22 (59/10/31%) | 0.30 |
| HR supine (bpm) | 70 (8) | 70 (11) | 0.74 |
| HR end-tilt (bpm) | 87 (17) | 92 (17) | 0.17 |
| SBP supine (mmHg) | 136 (21) | 134 (17) | 0.58 |
| SBP end-tilt (mmHg) | 128 (25) | 126 (18) | 0.70 |
| DBP supine (mmHg) | 81 (11) | 78 (12) | 0.22 |
| DBP end-tilt (mmHg) | 86 (14) | 85 (10) | 0.74 |
| CBF supine (ml/min) | 586 (88) | 616 (103) | 0.13 |
| CBF end-tilt (ml/min) | 441 (73) | 426 (88) | 0.36 |
| %CBF reduction (%) | 24 (9) | 31 (6) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Campen, C.M.C.; Rowe, P.C.; Visser, F.C. Worsening Symptoms Is Associated with Larger Cerebral Blood Flow Abnormalities during Tilt-Testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medicina 2023, 59, 2153. https://doi.org/10.3390/medicina59122153
van Campen CMC, Rowe PC, Visser FC. Worsening Symptoms Is Associated with Larger Cerebral Blood Flow Abnormalities during Tilt-Testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medicina. 2023; 59(12):2153. https://doi.org/10.3390/medicina59122153
Chicago/Turabian Stylevan Campen, C. (Linda) M. C., Peter C. Rowe, and Frans C. Visser. 2023. "Worsening Symptoms Is Associated with Larger Cerebral Blood Flow Abnormalities during Tilt-Testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)" Medicina 59, no. 12: 2153. https://doi.org/10.3390/medicina59122153
APA Stylevan Campen, C. M. C., Rowe, P. C., & Visser, F. C. (2023). Worsening Symptoms Is Associated with Larger Cerebral Blood Flow Abnormalities during Tilt-Testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medicina, 59(12), 2153. https://doi.org/10.3390/medicina59122153