
Cytochrome 4Z1 Expression Connotes Unfavorable Prognosis in Ovarian Cancers

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Tissue Specimens
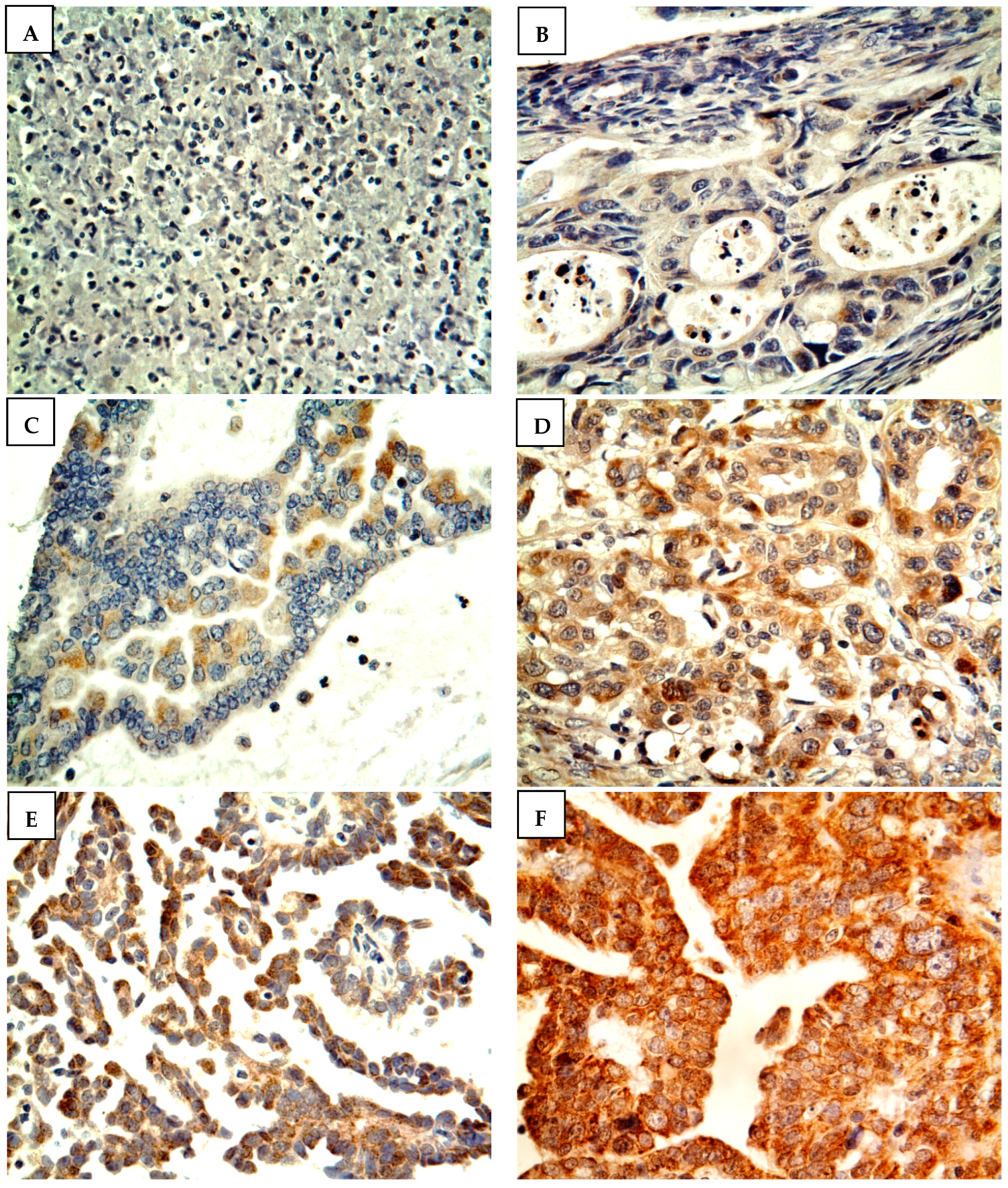
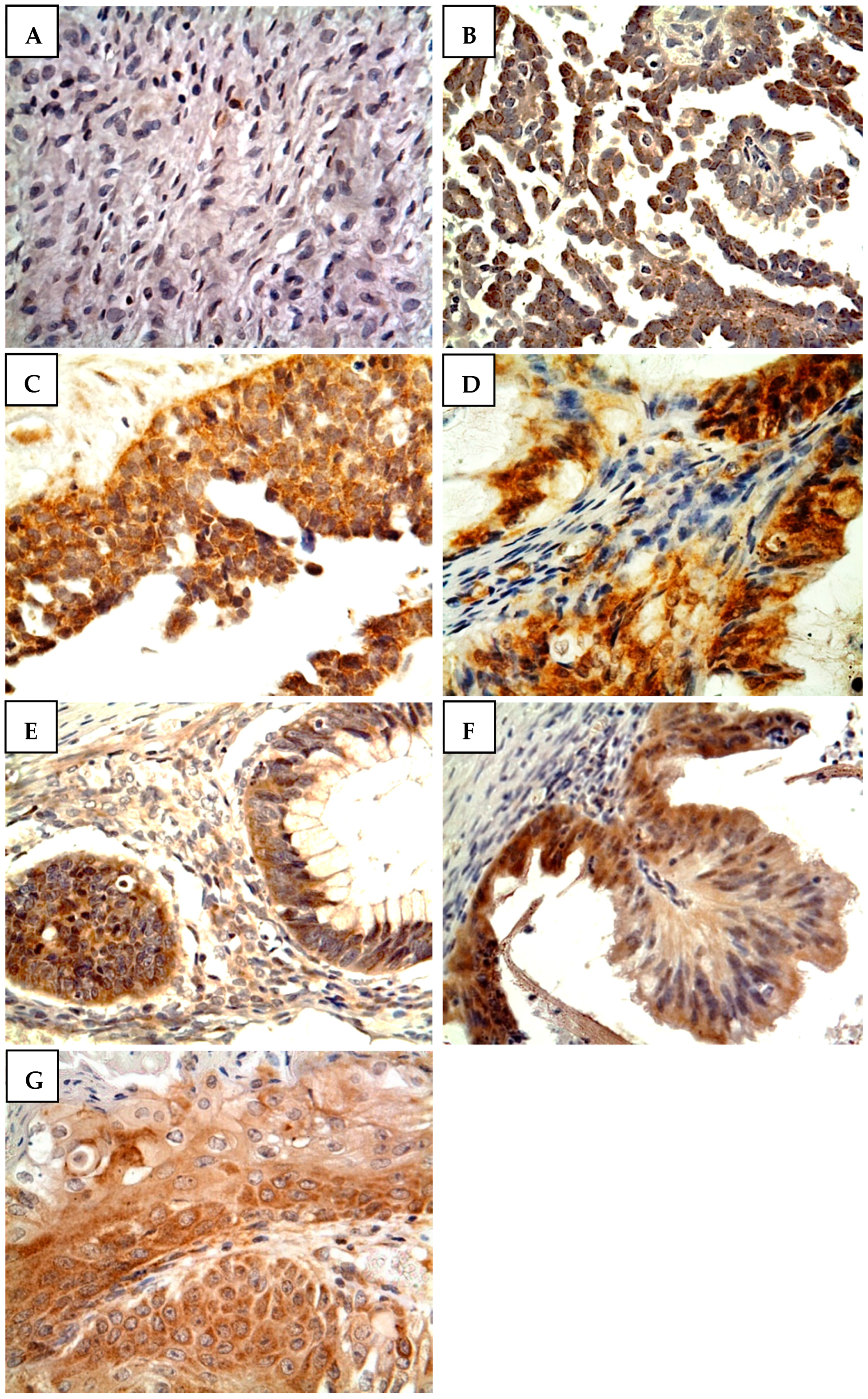
2.2. Immunohistochemistry
2.3. Scoring
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographics and Clinicopathological Characteristics
3.2. Prevalence of CYP4Z1 Expression and Its Relation to Clinicopathological Features
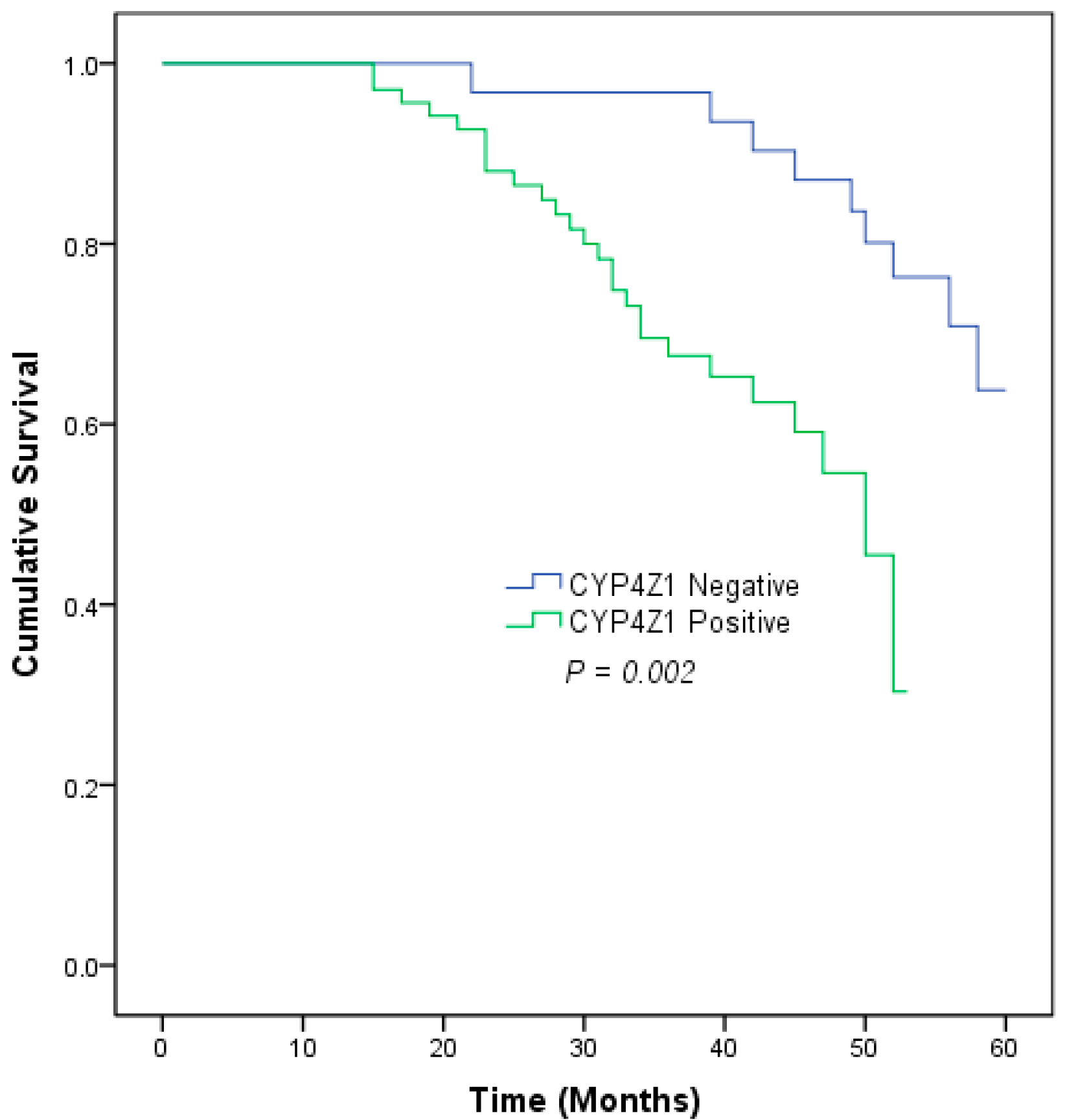
3.3. The Correlation between CYP4Z1 Expression and Prognosis in Ovarian Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berek, J.S.; Renz, M.; Kehoe, S.; Kumar, L.; Friedlander, M. Cancer of the ovary, fallopian tube, and peritoneum: 2021 update. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2021, 155 (Suppl. S1), 61–85. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Doubeni, C.A.; Doubeni, A.R.; Myers, A.E. Diagnosis and Management of Ovarian Cancer. Am. Fam. Physician 2016, 93, 937–944. [Google Scholar]
- Grabska, K.; Pilarska, I.; Fudalej, M.M.; Deptała, A.; Badowska-Kozakiewicz, A. What is new about ovarian malignancies? Contemp. Oncol. Pozn. Pol. 2021, 25, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Matulonis, U.A.; Sood, A.K.; Fallowfield, L.; Howitt, B.E.; Sehouli, J.; Karlan, B.Y. Ovarian cancer. Nat. Rev. Dis. Primers 2016, 2, 16061. [Google Scholar] [CrossRef] [PubMed]
- Al Bakir, M.; Gabra, H. The molecular genetics of hereditary and sporadic ovarian cancer: Implications for the future. Br. Med. Bull. 2014, 112, 57–69. [Google Scholar] [CrossRef]
- Carter, J.S.; Downs, L.S., Jr. Ovarian Cancer Tests and Treatment. Female Patient 2011, 36, 30–35. [Google Scholar]
- Guengerich, F.P.; Cheng, Q. Orphans in the human cytochrome P450 superfamily: Approaches to discovering functions and relevance in pharmacology. Pharmacol. Rev. 2011, 63, 684–699. [Google Scholar] [CrossRef]
- Licznerska, B.; Baer-Dubowska, W. What might the presence of ‘orphan’ CYP450 isoforms in breast epithelial cells mean for the future of targeted therapeutics? Expert Opin. Drug Metab. Toxicol. 2021, 17, 135–137. [Google Scholar] [CrossRef]
- Bruno, R.D.; Njar, V.C.O. Targeting cytochrome P450 enzymes: A new approach in anti-cancer drug development. Bioorg. Med. Chem. 2007, 15, 5047–5060. [Google Scholar] [CrossRef]
- Evangelista, E.A.; Cho, C.W.; Aliwarga, T.; Totah, R.A. Expression and Function of Eicosanoid-Producing Cytochrome P450 Enzymes in Solid Tumors. Front. Pharmacol. 2020, 11, 828. [Google Scholar] [CrossRef]
- Rieger, M.A.; Ebner, R.; Bell, D.R.; Kiessling, A.; Rohayem, J.; Schmitz, M.; Temme, A.; Rieber, E.P.; Weigle, B. Identification of a novel mammary-restricted cytochrome P450, CYP4Z1, with overexpression in breast carcinoma. Cancer Res. 2004, 64, 2357–2364. [Google Scholar] [CrossRef] [Green Version]
- Al-Saraireh, Y.M.; Alshammari, F.; Youssef, A.M.M.; Al-Tarawneh, F.; Al-Sarayreh, S.; Almuhaisen, G.H.; Satari, A.O.; Al-Shuneigat, J.; Alrawashdeh, H.M. Cytochrome 4Z1 Expression is Associated with Unfavorable Survival in Triple-Negative Breast Cancers. Breast Cancer Dove Med. Press 2021, 13, 565–574. [Google Scholar] [CrossRef]
- Al-Saraireh, Y.M.; Alshammari, F.; Youssef, A.M.M.; Al-Sarayreh, S.; Almuhaisen, G.H.; Alnawaiseh, N.; Al-Shuneigat, J.M.; Alrawashdeh, H.M. Cytochrome 4Z1 Expression is Associated with Poor Prognosis in Colon Cancer Patients. OncoTargets Ther. 2021, 14, 5249–5260. [Google Scholar] [CrossRef]
- Tradonsky, A.; Rubin, T.; Beck, R.; Ring, B.; Seitz, R.; Mair, S. A search for reliable molecular markers of prognosis in prostate cancer: A study of 240 cases. Am. J. Clin. Pathol. 2012, 137, 918–930. [Google Scholar] [CrossRef]
- Downie, D.; McFadyen, M.C.; Rooney, P.H.; Cruickshank, M.E.; Parkin, D.E.; Miller, I.D.; Telfer, C.; Melvin, W.T.; Murray, G.I. Profiling cytochrome P450 expression in ovarian cancer: Identification of prognostic markers. Clin. Cancer Res. 2005, 11, 7369–7375. [Google Scholar] [CrossRef]
- Al-Saraireh, Y.M.; Alshammari, F.; Youssef, A.M.M.; Al-Sarayra, Y.M.; Al-Saraireh, R.A.; Al-Muhaisen, G.H.; Al-Mahdy, Y.S.; Al-Kharabsheh, A.M.; Abufraijeh, S.M.; Alrawashdeh, H.M. Cytochrome 4Z1 Expression Is Correlated with Poor Prognosis in Patients with Cervical Cancer. Curr. Oncol. 2021, 28, 3573–3584. [Google Scholar] [CrossRef] [PubMed]
- Al-Saraireh, Y.M.; Alshammari, F.; Youssef, A.M.M.; Al-Sarayreh, S.; Almuhaisen, G.H.; Alnawaiseh, N.; Al Shuneigat, J.M.; Alrawashdeh, H.M. Profiling of CYP4Z1 and CYP1B1 expression in bladder cancers. Sci. Rep. 2021, 11, 5581. [Google Scholar] [CrossRef]
- Khayeka-Wandabwa, C.; Ma, X.; Jia, Y.; Bureik, M. Monitoring of autoantibodies against CYP4Z1 in patients with colon, ovarian, or prostate cancer. Immunobiology 2022, 227, 152174. [Google Scholar] [CrossRef]
- Nunna, V.; Jalal, N.; Bureik, M. Anti-CYP4Z1 autoantibodies detected in breast cancer patients. Cell. Mol. Immunol. 2017, 14, 572–574. [Google Scholar] [CrossRef]
- Savas, U.; Hsu, M.H.; Griffin, K.J.; Bell, D.R.; Johnson, E.F. Conditional regulation of the human CYP4X1 and CYP4Z1 genes. Arch. Biochem. Biophys. 2005, 436, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Machalz, D.; Yan, Q.; Sorensen, E.J.; Wolber, G.; Bureik, M. Importance of asparagine-381 and arginine-487 for substrate recognition in CYP4Z1. Biochem. Pharmacol. 2020, 174, 113850. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Machalz, D.; Zöllner, A.; Sorensen, E.J.; Wolber, G.; Bureik, M. Efficient substrate screening and inhibitor testing of human CYP4Z1 using permeabilized recombinant fission yeast. Biochem. Pharmacol. 2017, 146, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Zollner, A.; Dragan, C.A.; Pistorius, D.; Muller, R.; Bode, H.B.; Peters, F.T.; Maurer, H.H.; Bureik, M. Human CYP4Z1 catalyzes the in-chain hydroxylation of lauric acid and myristic acid. Biol. Chem. 2009, 390, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, J.P.; McDonald, M.G.; Pelletier, R.D.; Hanenberg, H.; Wiek, C.; Rettie, A.E. Design and Characterization of the First Selective and Potent Mechanism-Based Inhibitor of Cytochrome P450 4Z1. J. Med. Chem. 2020, 63, 4824–4836. [Google Scholar] [CrossRef]
- Machalz, D.; Li, H.; Du, W.; Sharma, S.; Liu, S.; Bureik, M.; Wolber, G. Discovery of a novel potent cytochrome P450 CYP4Z1 inhibitor. Eur. J. Med. Chem. 2021, 215, 113255. [Google Scholar] [CrossRef]
- Daldorff, S.; Mathiesen, R.M.R.; Yri, O.E.; Ødegård, H.P.; Geisler, J. Cotargeting of CYP-19 (aromatase) and emerging, pivotal signalling pathways in metastatic breast cancer. Br. J. Cancer 2017, 116, 10–20. [Google Scholar] [CrossRef]
- Al-Saraireh, Y.M.; Alboaisa, N.S.; Alrawashdeh, H.M.; Hamdan, O.; Al-Sarayreh, S.; Al-Shuneigat, J.M.; Nofal, M.N. Screening of cytochrome 4Z1 expression in human non-neoplastic, pre-neoplastic and neoplastic tissues. Ecancermedicalscience 2020, 14, 1114. [Google Scholar] [CrossRef]
- Allred, D.C. Problems and solutions in the evaluation of hormone receptors in breast cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 2433–2435. [Google Scholar] [CrossRef]
- Daltoé, R.D.; Madeira, K.P.; de Carvalho, A.A.; de Rezende, L.C.D.; Silva, I.V.; Rangel, L.B.A. Evaluation of the progesterone receptor status in breast cancer using three different antibodies: A comparison by Allred score system. Int. J. Clin. Exp. Pathol. 2013, 7, 331–339. [Google Scholar]
- Carter, J.; Penson, R.; Barakat, R.; Wenzel, L. Contemporary quality of life issues affecting gynecologic cancer survivors. Hematol./Oncol. Clin. N. Am. 2012, 26, 169–194. [Google Scholar] [CrossRef] [PubMed]
- Uhlen, M.; Zhang, C.; Lee, S.; Sjöstedt, E.; Fagerberg, L.; Bidkhori, G.; Benfeitas, R.; Arif, M.; Liu, Z.; Edfors, F.; et al. A pathology atlas of the human cancer transcriptome. Science 2017, 357, eaan2507. [Google Scholar] [CrossRef]
- Yu, W.; Chai, H.; Li, Y.; Zhao, H.; Xie, X.; Zheng, H.; Wang, C.; Wang, X.; Yang, G.; Cai, X.; et al. Increased expression of CYP4Z1 promotes tumor angiogenesis and growth in human breast cancer. Toxicol. Appl. Pharmacol. 2012, 264, 73–83. [Google Scholar] [CrossRef] [Green Version]
- McDonald, M.G.; Ray, S.; Amorosi, C.J.; Sitko, K.A.; Kowalski, J.P.; Paco, L.; Nath, A.; Gallis, B.; Totah, R.A.; Dunham, M.J.; et al. Expression and Functional Characterization of Breast Cancer-Associated Cytochrome P450 4Z1 in Saccharomyces cerevisiae. Drug Metab. Dispos. 2017, 45, 1364–1371. [Google Scholar] [CrossRef]
- Zheng, L.; Guo, Q.; Xiang, C.; Liu, S.; Jiang, Y.; Gao, L.; Ni, H.; Wang, T.; Zhao, Q.; Liu, H.; et al. Transcriptional factor six2 promotes the competitive endogenous RNA network between CYP4Z1 and pseudogene CYP4Z2P responsible for maintaining the stemness of breast cancer cells. J. Hematol. Oncol. 2019, 12, 23. [Google Scholar] [CrossRef]
- Zheng, L.; Li, X.; Gu, Y.; Lv, X.; Xi, T. The 3’UTR of the pseudogene CYP4Z2P promotes tumor angiogenesis in breast cancer by acting as a ceRNA for CYP4Z1. Breast Cancer Res. Treat. 2015, 150, 105–118. [Google Scholar] [CrossRef]
- Sausville, L.N.; Williams, S.M.; Pozzi, A. Cytochrome P450 epoxygenases and cancer: A genetic and a molecular perspective. Pharmacol. Ther. 2019, 196, 183–194. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| CYP4Z1 Expression | |||
|---|---|---|---|
| Characteristic | Negative n = 42 (21%) | Positive n = 158 (79%) | p Value |
| Age: | |||
| <50 (n = 123, 61.5%) | 23 (18.7%) | 100 (81.3%) | 0.373 |
| ≥50 (n = 77, 38.5%) | 19 (24.7%) | 58 (75.3%) | |
| Pathology subtype: | |||
| Serous adenocarcinoma (n = 86,43%) | 20 (23.3%) | 66 (76.7%) | 0.005 |
| Serous papillary adenocarcinoma (n = 48, 24%) | 4 (8.3%) | 44 (91.7%) | |
| Mucinous adenocarcinoma (n = 22, 11%) | 5 (22.7%) | 17 (77.3%) | |
| Mucinous papillary adenocarcinoma (n = 14, 7%) | 0 (0%) | 14 (100%) | |
| Endometrioid adenocarcinoma (n = 8, 4%) | 3 (37.5%) | 5 (62.5%) | |
| Krukenberg tumor (n = 14, 7%) | 3 (21.4%) | 11 (78.6%) | |
| Normal (n = 8, 4%) | 7 (87.5%) | 1 (12.5%) | |
| Histological grade: | |||
| I (n = 25, 14.2%) | 4 (16%) | 21 (84%) | 0.082 |
| II (n = 36, 20.5%) | 2 (5.6%) | 34 (94.4%) | |
| III (n = 115, 65.3%) | 25 (21.7%) | 90 (78.3%) | |
| Histological stage: | |||
| I (n = 149, 84.7%) | 31 (20.8%) | 118 (79.2%) | 0.033 |
| II (n = 14, 8%) | 0 (0%) | 14 (100%) | |
| III (n = 13, 7.4%) | 0 (0%) | 13 (100%) | |
| Tumor depth of invasion: | |||
| T1 (n = 148, 84.1%) | 31 (20.9%) | 117 (79.1%) | 0.028 |
| T2 (n = 21, 11.9%) | 0 (0%) | 21 (100%) | |
| T3 (n = 7, 4%) | 0 (0%) | 7 (100%) | |
| Lymph node metastasis: | |||
| Negative (n = 163, 92.6%) | 31 (19%) | 132 (81%) | 0.073 |
| Positive (n = 13, 7.4%) | 0 (0%) | 13 (100%) | |
| Prognostic Variable | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95%Cl | p-Value | HR | 95%Cl | p-Value | |
| Age | 0.756 | 0.383–1.494 | 0.421 | 0.631 | 0.297–1.340 | 0.231 |
| Pathology subtype | 1.081 | 0.824–1.417 | 0.575 | 1.153 | 0.851–1.561 | 0.358 |
| Histological grade | 1.255 | 0.770–2.045 | 0.361 | 1.288 | 0.766–2.168 | 0.340 |
| Histological stage | 2.461 | 1.577–3.840 | 0.001 | 3.061 | 0.652–14.371 | 0.156 |
| Tumor depth of invasion | 2.088 | 1.227–3.555 | 0.007 | 0.487 | 0.125–1.902 | 0.301 |
| Lymph node metastasis | 7.599 | 2.928–19.719 | 0.001 | 2.803 | 0.360–21.839 | 0.325 |
| CYP4Z1 expression | 1.155 | 1.034–1.299 | 0.010 | 1.177 | 1.040–1.332 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-saraireh, Y.M.; Alshammari, F.O.F.O.; Satari, A.O.; Al-mahdy, Y.S.; Almuhaisen, G.H.; Abu-azzam, O.H.; Uwais, A.N.; Abufraijeh, S.M.; Al-Kharabsheh, A.M.; Al-dalain, S.M.; et al. Cytochrome 4Z1 Expression Connotes Unfavorable Prognosis in Ovarian Cancers. Medicina 2022, 58, 1263. https://doi.org/10.3390/medicina58091263
Al-saraireh YM, Alshammari FOFO, Satari AO, Al-mahdy YS, Almuhaisen GH, Abu-azzam OH, Uwais AN, Abufraijeh SM, Al-Kharabsheh AM, Al-dalain SM, et al. Cytochrome 4Z1 Expression Connotes Unfavorable Prognosis in Ovarian Cancers. Medicina. 2022; 58(9):1263. https://doi.org/10.3390/medicina58091263
Chicago/Turabian StyleAl-saraireh, Yousef M., Fatemah O. F. O. Alshammari, Anas O. Satari, Yanal S. Al-mahdy, Ghadeer H. Almuhaisen, Omar H. Abu-azzam, Ala N. Uwais, Seham M. Abufraijeh, Ahlam M. Al-Kharabsheh, Sa’ed M. Al-dalain, and et al. 2022. "Cytochrome 4Z1 Expression Connotes Unfavorable Prognosis in Ovarian Cancers" Medicina 58, no. 9: 1263. https://doi.org/10.3390/medicina58091263
APA StyleAl-saraireh, Y. M., Alshammari, F. O. F. O., Satari, A. O., Al-mahdy, Y. S., Almuhaisen, G. H., Abu-azzam, O. H., Uwais, A. N., Abufraijeh, S. M., Al-Kharabsheh, A. M., Al-dalain, S. M., Al-Qtaitat, A., Al-Tarawneh, F., Al Shuneigat, J. M., & Al-Sarayreh, S. A. (2022). Cytochrome 4Z1 Expression Connotes Unfavorable Prognosis in Ovarian Cancers. Medicina, 58(9), 1263. https://doi.org/10.3390/medicina58091263