
Early Enteral Nutrition with High-Protein Whey Peptide Digestive Nutrients May Improve Prognosis in Subarachnoid Hemorrhage Patients
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
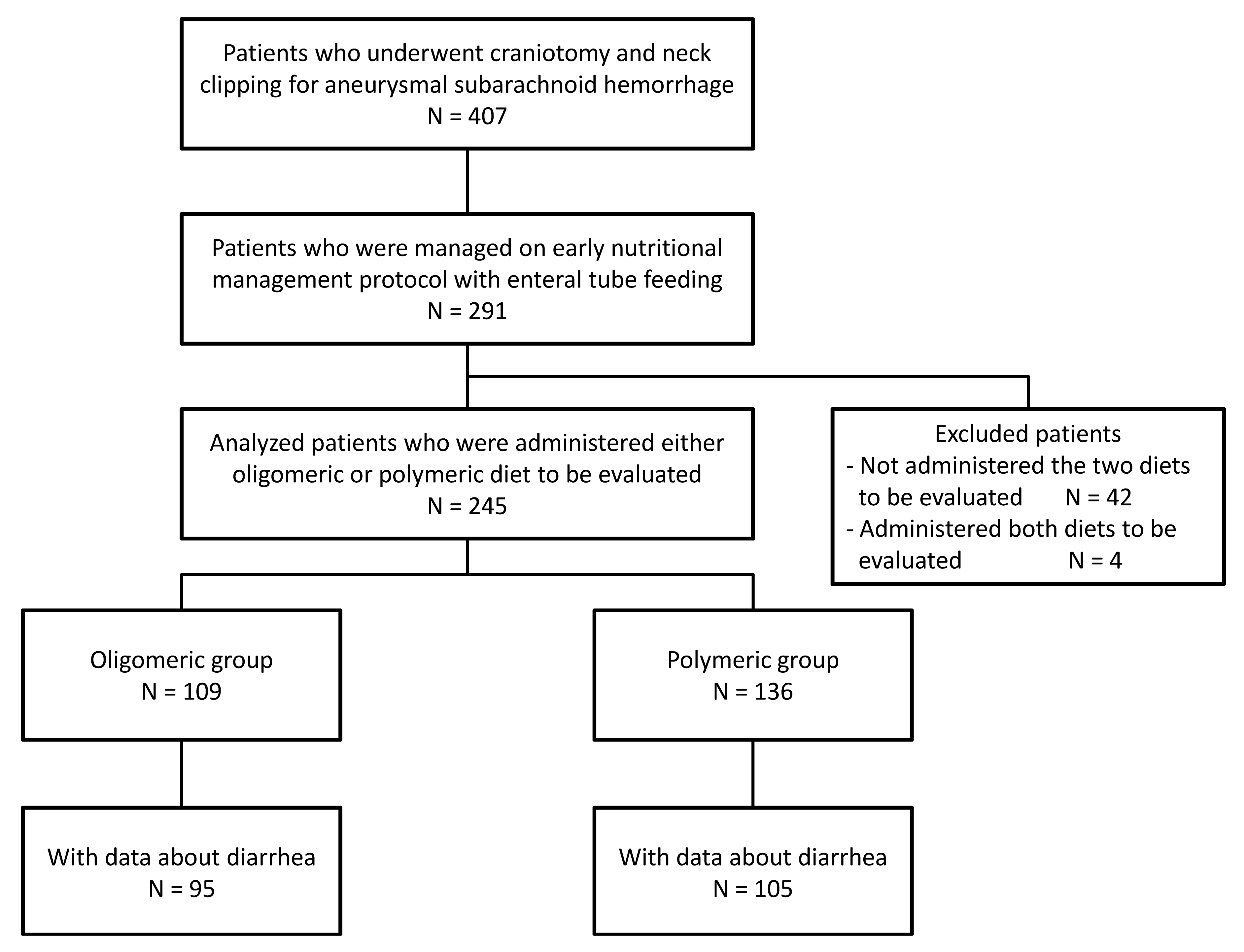
2.2. Patients
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Nieuwkamp, D.J.; Setz, L.E.; Algra, A.; Linn, F.H.; de Rooij, N.K.; Rinkel, G.J. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: A meta-analysis. Lancet Neurol. 2009, 8, 635–642. [Google Scholar] [CrossRef]
- Dubovoy, A.; Lekchnov, E.; Galaktionov, D.; Ovsyannikov, K.; Bervitskiy, A.; Sosnov, A.; Rzaev, J. Microsurgical management of complex middle cerebral artery aneurysms: Literature review and a series of cases. Serb. J. Neurosurg. 2021, 1. [Google Scholar] [CrossRef]
- Shimauchi-Ohtaki, H.; Tosaka, M.; Ohtani, T.; Iijima, K.; Sasaguchi, N.; Kurihara, H.; Yoshimoto, Y. Systemic metabolism and energy consumption after microsurgical clipping and endovascular coiling for aneurysmal subarachnoid hemorrhage. Acta Neurochir. 2018, 160, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Long, C.L.; Schaffel, N.; Geiger, J.W.; Schiller, W.R.; Blakemore, W.S. Metabolic response to injury and illness: Estimation of energy and protein needs from indirect calorimetry and nitrogen balance. JPEN J. Parenter. Enteral. Nutr. 1979, 3, 452–456. [Google Scholar] [CrossRef]
- Esper, D.H.; Coplin, W.M.; Carhuapoma, J.R. Energy expenditure in patients with nontraumatic intracranial hemorrhage. JPEN J. Parenter. Enteral. Nutr. 2006, 30, 71–75. [Google Scholar] [CrossRef]
- Yoo, S.H.; Kim, J.S.; Kwon, S.U.; Yun, S.C.; Koh, J.Y.; Kang, D.W. Undernutrition as a predictor of poor clinical outcomes in acute ischemic stroke patients. Arch. Neurol. 2008, 65, 39–43. [Google Scholar] [CrossRef]
- Badjatia, N.; Ryan, A.; Choi, H.A.; Parikh, G.Y.; Jiang, X.; Day, A.G.; Heyland, D.K. Relationship Between Nutrition Intake and Outcome After Subarachnoid Hemorrhage: Results From the International Nutritional Survey. J. Intensive Care Med. 2021, 36, 1141–1148. [Google Scholar] [CrossRef]
- Nishioka, S.; Takayama, M.; Watanabe, M.; Urusihara, M.; Kiriya, Y.; Hijioka, S. Prevalence of malnutrition in convalescent rehabilitation wards in Japan and correlation of malnutrition with ADL and discharge outcome in elderly stroke patients. J. Parenter. Enteral. Nutr. 2015, 30, 1145–1151. [Google Scholar] [CrossRef]
- Carvalho, M.R.; Berto, B.S.D.; Rodrigues, A.M.; Prudente, L.O.B.; Moura, E.L.B. Nutritional assessment of patients with aneurysmal subarachnoid hemorrhage using the modified “Nutrition Risk in the Critically ill” score, and its association with outcomes. Nutr. Hosp. 2022, 39, 709–715. [Google Scholar] [CrossRef]
- Burgos, R.; Breton, I.; Cereda, E.; Desport, J.C.; Dziewas, R.; Genton, L.; Gomes, F.; Jesus, P.; Leischker, A.; Muscaritoli, M.; et al. ESPEN guideline clinical nutrition in neurology. Clin. Nutr. 2018, 37, 354–396. [Google Scholar] [CrossRef] [PubMed]
- Martindale, R.G.; McClave, S.A.; Vanek, V.W.; McCarthy, M.; Roberts, P.; Taylor, B.; Ochoa, J.B.; Napolitano, L.; Cresci, G.; American College of Critical Care Medicine the A.S.P.E.N. Board of Directors; et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition: Executive Summary. Crit. Care Med. 2009, 37, 1757–1761. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, H.; Suzuki, M. Japanese Guidelines for the Management of Stroke 2015: Overview of the chapter on Subarachnoid Hemorrhage. Nihon Rinsho Jpn. J. Clin. Med. 2016, 74, 677–680. [Google Scholar]
- Kofler, M.; Schiefecker, A.J.; Beer, R.; Gaasch, M.; Rhomberg, P.; Stover, J.; Pfausler, B.; Thome, C.; Schmutzhard, E.; Helbok, R. Enteral nutrition increases interstitial brain glucose levels in poor-grade subarachnoid hemorrhage patients. J. Cereb. Blood Flow Metab. 2018, 38, 518–527. [Google Scholar] [CrossRef]
- Ehrlein, H.; Haas-Deppe, B. Comparison of absorption of nutrients and secretion of water between oligomeric and polymeric enteral diets in pigs. Br. J. Nutr. 1998, 80, 545–553. [Google Scholar] [CrossRef]
- Koopman, R.; Crombach, N.; Gijsen, A.P.; Walrand, S.; Fauquant, J.; Kies, A.K.; Lemosquet, S.; Saris, W.H.; Boirie, Y.; van Loon, L.J. Ingestion of a protein hydrolysate is accompanied by an accelerated in vivo digestion and absorption rate when compared with its intact protein. Am. J. Clin. Nutr. 2009, 90, 106–115. [Google Scholar] [CrossRef]
- Tang, J.E.; Moore, D.R.; Kujbida, G.W.; Tarnopolsky, M.A.; Phillips, S.M. Ingestion of whey hydrolysate, casein, or soy protein isolate: Effects on mixed muscle protein synthesis at rest and following resistance exercise in young men. J. Appl. Physiol. (1985) 2009, 107, 987–992. [Google Scholar] [CrossRef]
- Power, O.; Hallihan, A.; Jakeman, P. Human insulinotropic response to oral ingestion of native and hydrolysed whey protein. Amino Acids 2009, 37, 333–339. [Google Scholar] [CrossRef]
- Boirie, Y.; Dangin, M.; Gachon, P.; Vasson, M.P.; Maubois, J.L.; Beaufrere, B. Slow and fast dietary proteins differently modulate postprandial protein accretion. Proc. Natl. Acad. Sci. USA 1997, 94, 14930–14935. [Google Scholar] [CrossRef]
- Xue, H.; Han, J.; He, B.; Yi, M.; Liu, X.; Song, H.; Li, J. Bioactive peptide release and the absorption tracking of casein in the gastrointestinal digestion of rats. Food Funct. 2021, 12, 5157–5170. [Google Scholar] [CrossRef]
- Gelder, C.L.; Bautista, M.; Awan, S.A.; Anderson, I.A. Unaccounted for enteral volume loss linked to delayed cerebral ischemia after subarachnoid hemorrhage. Neurosurg. Focus 2022, 52, E5. [Google Scholar] [CrossRef] [PubMed]
- Jack, L.; Coyer, F.; Courtney, M.; Venkatesh, B. Diarrhoea risk factors in enterally tube fed critically ill patients: A retrospective audit. Intensive Crit. Care Nurs. 2010, 26, 327–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Oligomeric Group | Polymeric Group | p-Value | |
|---|---|---|---|
| n = 109 | n = 136 | ||
| Female, n (%) | 66 (42.6) | 89 (57.4) | 0.505 |
| Age, (years) mean ± SD | 65.2 ± 13.8 | 63.1 ± 12.6 | 0.209 |
| Body weight, (kg) mean ± SD | 59.3 ± 13.2 | 55.9 ± 10.4 | 0.088 |
| Comorbidities, n (%) | |||
| Atrial fibrillation | 1 (0.9) | 1 (0.7) | 1 |
| Hypertension | 32 (29.4) | 27 (19.9) | 0.099 |
| Diabetes mellitus | 7 (6.4) | 3 (2.2) | 0.114 |
| Hyperlipidemia | 7 (6.4) | 2 (1.5) | 0.082 |
| Bleeding complication | 8 (7.3) | 13 (9.6) | 0.648 |
| HK grade, n (%) | |||
| Grade 1 | 14 (12.8) | 6 (4.4) | 0.933 |
| Grade 2 | 24 (22.0) | 42 (30.9) | |
| Grade 3 | 22 (20.2) | 24 (17.6) | |
| Grade 4 | 25 (22.9) | 47 (34.6) | |
| Grade 5 | 24 (22.0) | 17 (12.5) | |
| Fisher classification, n (%) | |||
| I | 0 (0.0) | 2 (100) | 0.536 |
| II | 11 (64.7) | 6 (35.3) | |
| III | 73 (43.5) | 95 (56.5) | |
| IV | 25 (43.9) | 32 (56.1) | |
| Albumin, (g/dl) mean ± SD | 4.0 ± 0.6 | 4.0 ± 0.7 | 0.638 |
| Na, (mEq/L) mean ± SD | 139.8 ± 3.7 | 139.4 ± 3.1 | 0.42 |
| K, (mEq/L) mean ± SD | 3.6 ± 0.5 | 3.5 ± 0.4 | 0.069 |
| Blood glucose, (mg/dl) mean ± SD | 169.6 ± 53.5 | 173.1 ± 49.5 | 0.606 |
| Lymphocyte count, mean ± SD | 2318.3 ± 1820.8 | 1923.2 ± 1550.2 | 0.072 |
| Time to enteral nutrition (day), mean ± SD | 2.8 ± 2.3 | 2.9 ± 2.2 | 0.783 |
| Oligomeric group, Peptamen AF group; Polymeric group, Oxipa group; HK grade, Hunt and Kosnik grading; Na, sodium; K, potassium; SD, standard deviation. | |||
| Oligomeric Group | Polymeric Group | p-Value | ||
|---|---|---|---|---|
| n = 109 | n = 136 | |||
| mRS at discharge, n (%) | 0 | 7 (6.4) | 9 (6.6) | 0.826 |
| 1 | 21 (19.3) | 11 (8.1) | ||
| 2 | 12 (11.0) | 22 (16.2) | ||
| 3 | 9 (8.3) | 23 (16.9) | ||
| 4 | 24 (22.0) | 30 (22.1) | ||
| 5 | 33 (30.3) | 39 (28.7) | ||
| 6 | 3 (2.8) | 2 (1.5) | ||
| mRS 0–1, n (%) | 28 (25.7) | 20 (14.7) | 0.036 | |
| Diarrhea, n (%) | 43 (45.3) | 70 (66.7) | 0.003 | |
| Watery stool, n (%) | 15 (15.8) | 36 (34.3) | 0.003 | |
| Duration of hospital stay, (day), mean ± SD | 54.8 ± 28.6 | 50.9 ± 22.6 | 0.237 | |
| mRS, modified Rankin Scale; Oligomeric group, Peptamen AF group; Polymeric group, Oxipa group; SD, standard deviation. | ||||
| Evaluated Factor | mRS 0–1 | mRS ≥ 2 | Odds Ratio and 95% CI | |||
|---|---|---|---|---|---|---|
| n = 48 | n = 197 | Odds Ratio | Lower | Upper | p-Value | |
| Enteral nutrition, n (%) | ||||||
| Oxipa | 20 (14.7) | 116 (85.3) | 0.033 | |||
| Peptamen | 28 (25.7) | 81 (74.3) | 2.005 | 1.057 | 3.803 | |
| Albumin (g/dl) | 42 (19.5) | 173 (80.5) | 1.42 | 0.7 | 2.884 | 0.331 |
| Sex, n (%) | ||||||
| Male | 18 (20) | 72 (80) | 0.902 | |||
| Female | 30 (19.4) | 125 (80.6) | 0.96 | 0.5 | 1.843 | |
| HK, n (%) | ||||||
| Grade < III | 29 (33.7) | 57 (66.3) | <0.0001 | |||
| Grade ≥ III | 19 (11.9) | 140 (88.1) | 0.267 | 0.139 | 0.514 | |
| Age category (years), n (%) | ||||||
| <65 | 32 (29.1) | 78 (70.9) | 0.001 | |||
| 65 £ | 16 (11.9) | 119 (88.1) | 0.328 | 0.169 | 0.637 | |
| Age (cont.) | 48 (19.6) | 197 (80.4) | 0.955 | 0.932 | 0.979 | 0.0002 |
| Body weight (cont.) | 43 (19.6) | 176 (80.4) | 1.038 | 1.008 | 1.068 | 0.012 |
| Evaluated Factor | mRS 0–1 | mRS ≥ 2 | Odds Ratio 95% CI | |||
|---|---|---|---|---|---|---|
| n = 43 | n = 176 | Odds Ratio | Lower | Upper | p-Value | |
| Enteral nutrition, n (%) | ||||||
| Oxipa | 20 (15.2) | 112 (84.8) | 0.023 | |||
| Peptamen | 23 (26.4) | 64 (73.6) | 2.447 | 1.134 | 5.284 | |
| Sex, n (%) | ||||||
| Male | 16 (20.3) | 63 (79.7) | 0.095 | |||
| Female | 27 (19.3) | 113 (80.7) | 2.175 | 0.873 | 5.417 | |
| HK, n (%) | ||||||
| Grade < III | 27 (36.0) | 48 (64.0) | <0.0001 | |||
| Grade ≥ III | 16 (11.1) | 128 (88.9) | 0.146 | 0.066 | 0.325 | |
| Age category (years), n (%) | ||||||
| <65 | 28 (28.3) | 71 (71.7) | 0.008 | |||
| 65 £ | 15 (12.5) | 105 (87.5) | 0.327 | 0.143 | 0.749 | |
| Body weight (cont.) | 43 (19.6) | 176 (80.4) | 1.047 | 1.008 | 1.089 | 0.022 |
| mRS 0–1 | mRS ≥ 2 | Odds Ratio and 95% CI | ||||
|---|---|---|---|---|---|---|
| n = 31 | n = 146 | Odds Ratio | Lower | Upper | p-Value | |
| Diarrhea, n (%) | ||||||
| No | 17 (26.2) | 48 (73.8) | 0.047 | |||
| Yes | 14 (12.5) | 98 (87.5) | 0.406 | 0.167 | 0.988 | |
| Sex, n (%) | ||||||
| Male | 11 (18.3) | 49 (81.7) | 0.163 | |||
| Female | 20 (17.1) | 97 (82.9) | 2.139 | 0.734 | 6.231 | |
| HK, n (%) | ||||||
| Grade < III | 19 (33.9) | 37 (66.1) | 0.0001 | |||
| Grade ≥ III | 12 (9.9) | 109 (90.1) | 0.132 | 0.05 | 0.347 | |
| Age category (years), n (%) | ||||||
| <65 | 19 (25.7) | 55 (74.3) | 0.051 | |||
| 65 £ | 12 (11.7) | 91 (88.3) | 0.392 | 0.153 | 1.004 | |
| Body weight (cont.) | 31 (17.5) | 146 (82.5) | 1.067 | 1.017 | 1.119 | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, K.; Sato, H.; Mori, H.; Matsumoto, R.; Arimoto, Y.; Sato, H.; Kamide, T.; Ikeda, T.; Kikkawa, Y.; Kurita, H. Early Enteral Nutrition with High-Protein Whey Peptide Digestive Nutrients May Improve Prognosis in Subarachnoid Hemorrhage Patients. Medicina 2022, 58, 1264. https://doi.org/10.3390/medicina58091264
Suzuki K, Sato H, Mori H, Matsumoto R, Arimoto Y, Sato H, Kamide T, Ikeda T, Kikkawa Y, Kurita H. Early Enteral Nutrition with High-Protein Whey Peptide Digestive Nutrients May Improve Prognosis in Subarachnoid Hemorrhage Patients. Medicina. 2022; 58(9):1264. https://doi.org/10.3390/medicina58091264
Chicago/Turabian StyleSuzuki, Kaima, Hiroki Sato, Hiromi Mori, Ryosuke Matsumoto, Yoshihiro Arimoto, Hiroshi Sato, Tomoya Kamide, Toshiki Ikeda, Yuichiro Kikkawa, and Hiroki Kurita. 2022. "Early Enteral Nutrition with High-Protein Whey Peptide Digestive Nutrients May Improve Prognosis in Subarachnoid Hemorrhage Patients" Medicina 58, no. 9: 1264. https://doi.org/10.3390/medicina58091264
APA StyleSuzuki, K., Sato, H., Mori, H., Matsumoto, R., Arimoto, Y., Sato, H., Kamide, T., Ikeda, T., Kikkawa, Y., & Kurita, H. (2022). Early Enteral Nutrition with High-Protein Whey Peptide Digestive Nutrients May Improve Prognosis in Subarachnoid Hemorrhage Patients. Medicina, 58(9), 1264. https://doi.org/10.3390/medicina58091264