
Recurrence Outcome in Hepatocellular Carcinoma within Milan Criteria Undergoing Microwave Ablation with or without Transarterial Chemoembolization

 ,
,
Abstract
1. Introduction
2. Materials and Methods
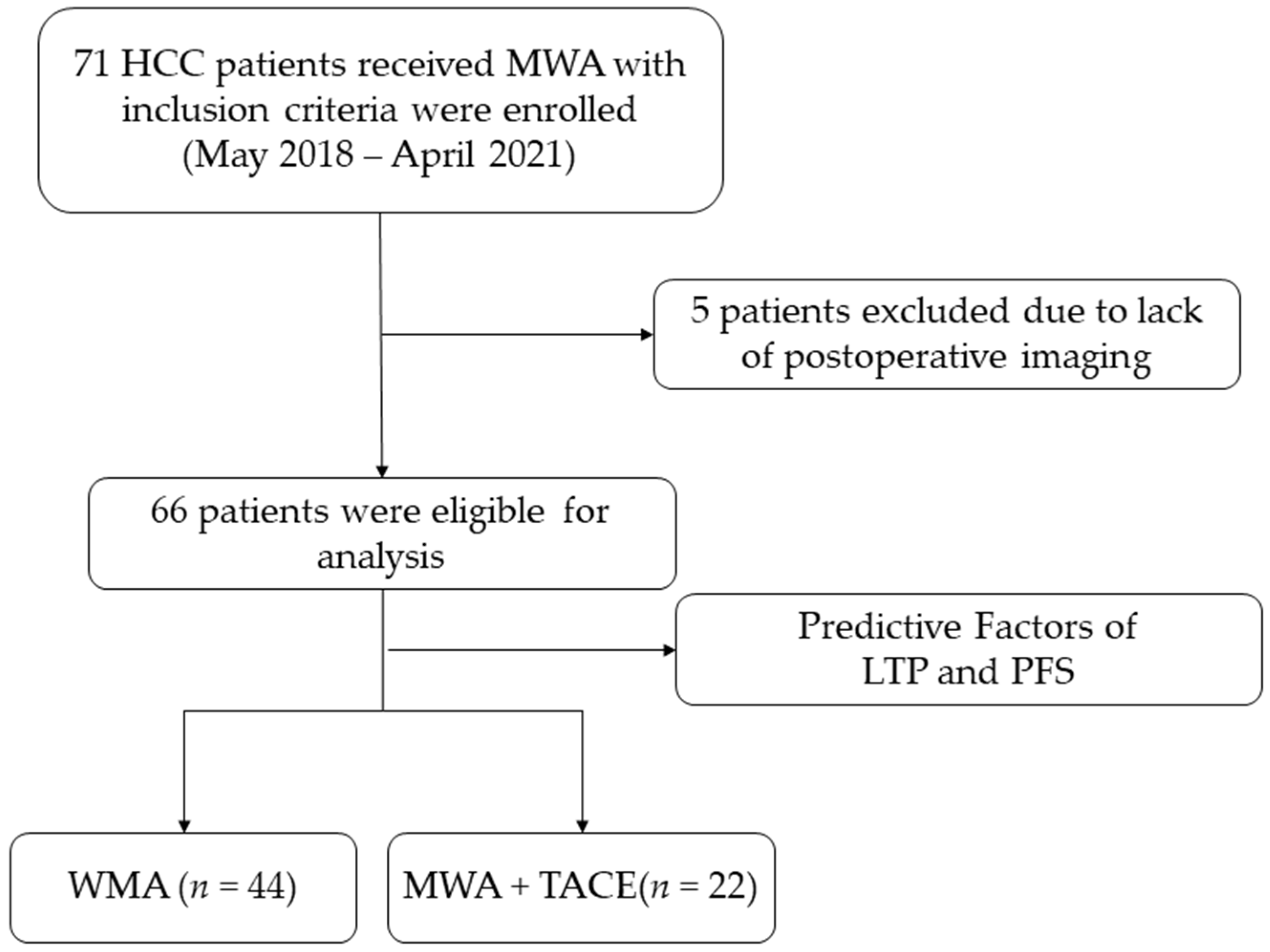
2.1. Study Population
2.2. MWA Procedure
2.3. TACE Combined with MWA Procedure
2.4. Follow-Up
2.5. Evaluation of Therapeutic Outcomes
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
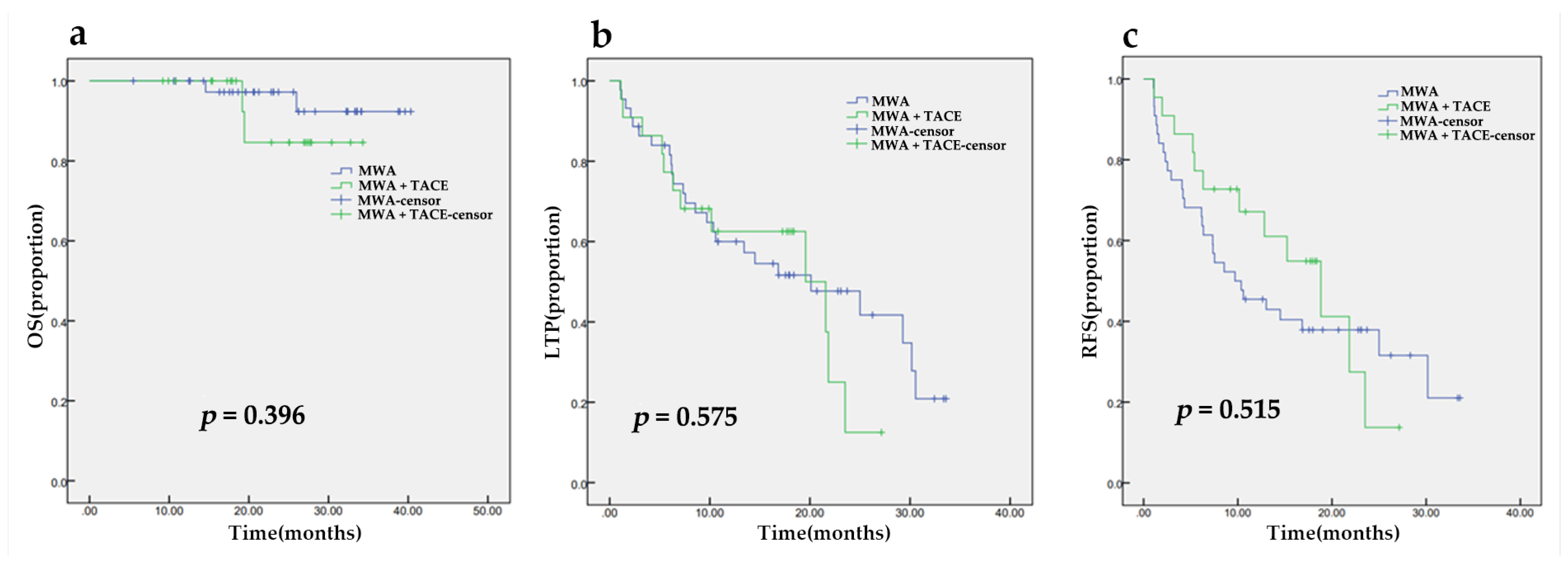
3.2. Treatment Outcomes and Complications
3.3. Univariable and Multivariable Analyses for LTP and RFS
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Xie, D.Y.; Ren, Z.G.; Zhou, J.; Fan, J.; Gao, Q. 2019 Chinese clinical guidelines for the management of hepatocellular carcinoma: Updates and insights. Hepatobiliary Surg. Nutr. 2020, 9, 452–463. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Zhu, A.X. Evolution of Systemic Therapy for Hepatocellular Carcinoma. Hepatology 2021, 73, 150–157. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Mason, A.C. Rising incidence of hepatocellular carcinoma in the United States. N. Engl. J. Med. 1999, 340, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Dou, J.; Cheng, Z.; Han, Z.; Liu, F.; Wang, Z.; Yu, X.; Yu, J.; Liang, P. Microwave ablation vs. surgical resection for treatment naive hepatocellular carcinoma within the Milan criteria: A follow-up of at least 5 years. Cancer. Biol. Med. 2021. [Google Scholar] [CrossRef]
- Llovet, J.M.; De Baere, T.; Kulik, L.; Haber, P.K.; Greten, T.F.; Meyer, T.; Lencioni, R. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 293–313. [Google Scholar] [CrossRef] [PubMed]
- Andreano, A.; Huang, Y.; Meloni, M.F.; Lee, F.T., Jr.; Brace, C. Microwaves create larger ablations than radiofrequency when controlled for power in ex vivo tissue. Med. Phys. 2010, 37, 2967–2973. [Google Scholar] [CrossRef] [PubMed]
- Smolock, A.R.; Shaw, C. Hepatic Microwave Ablation in Challenging Locations. Semin. Interv. Radiol. 2019, 36, 392–397. [Google Scholar] [CrossRef]
- Yu, J.; Yu, X.L.; Han, Z.Y.; Cheng, Z.G.; Liu, F.Y.; Zhai, H.Y.; Mu, M.J.; Liu, Y.M.; Liang, P. Percutaneous cooled-probe microwave versus radiofrequency ablation in early-stage hepatocellular carcinoma: A phase III randomised controlled trial. Gut 2017, 66, 1172–1173. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Abd El Aziz, M.A.; Tartaglia, N.; Ramai, D.; Mohan, B.P.; Cotsoglou, C.; Pusceddu, S.; Giacomelli, L.; Ambrosi, A.; Sacco, R. Microwave Ablation Versus Radiofrequency Ablation for Treatment of Hepatocellular Carcinoma: A Meta-Analysis of Randomized Controlled Trials. Cancers 2020, 12, 3796. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.L.; Liang, P.; Dong, B.W.; Yu, X.L.; Yu, D.J. Prognostic factors and recurrence of small hepatocellular carcinoma after hepatic resection or microwave ablation: A retrospective study. J. Gastrointest. Surg. 2008, 12, 327–337. [Google Scholar] [CrossRef]
- Chang, Y.; Jeong, S.W.; Young Jang, J.; Jae Kim, Y. Recent Updates of Transarterial Chemoembolilzation in Hepatocellular Carcinoma. Int. J. Mol. Sci. 2020, 21, 8165. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Hao, D.; Jiao, D.; Zhang, W.; Han, X. Transcatheter Arterial Chemoembolization Combined with Simultaneous Cone-beam Computed Tomography-guided Microwave Ablation in the Treatment of Small Hepatocellular Carcinoma: Clinical Experiences From 50 Procedures. Acad. Radiol. 2021, 28, S64–S70. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Huang, W.; Guo, Y.; Cai, M.; Zhou, J.; Lin, L.; Zhu, K. Risk Factors, Patterns, and Long-Term Survival of Recurrence After Radiofrequency Ablation With or Without Transarterial Chemoembolization for Hepatocellular Carcinoma. Front. Oncol. 2021, 11, 638428. [Google Scholar] [CrossRef]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Bacchetti, P.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Comparison of the proposed UCSF criteria with the Milan criteria and the Pittsburgh modified TNM criteria. Liver. Transplant. 2002, 8, 765–774. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Iezzi, R.; Pompili, M.; Gasbarrini, A.; Bonomo, L. Sequential or combined treatment? That is the question. Radiology 2014, 272, 612–613. [Google Scholar] [CrossRef][Green Version]
- Renzulli, M.; Peta, G.; Vasuri, F.; Marasco, G.; Caretti, D.; Bartalena, L.; Spinelli, D.; Giampalma, E.; D’Errico, A.; Golfieri, R. Standardization of conventional chemoembolization for hepatocellular carcinoma. Ann. Hepatol. 2021, 22, 100278. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef]
- Tovoli, F.; Renzulli, M.; Negrini, G.; Brocchi, S.; Ferrarini, A.; Andreone, A.; Benevento, F.; Golfieri, R.; Morselli-Labate, A.M.; Mastroroberto, M.; et al. Inter-operator variability and source of errors in tumour response assessment for hepatocellular carcinoma treated with sorafenib. Eur. Radiol. 2018, 28, 3611–3620. [Google Scholar] [CrossRef]
- Chen, G.; Xie, X.; Wang, M.; Guo, X.; Zhang, Z.; Zhang, L.; Zhang, B. Prognostic Significance of Tumor Growth Rate (TGR) in Patients with Huge Hepatocellular Carcinoma Undergoing Transcatheter Arterial Chemoembolization. Curr. Oncol. 2022, 29, 423–432. [Google Scholar] [CrossRef]
- Rubin, D.B. Estimating causal effects from large data sets using propensity scores. Ann. Intern. Med. 1997, 127, 757–763. [Google Scholar] [CrossRef]
- Gupta, P.; Maralakunte, M.; Kumar, M.P.; Chandel, K.; Chaluvashetty, S.B.; Bhujade, H.; Kalra, N.; Sandhu, M.S. Overall survival and local recurrence following RFA, MWA, and cryoablation of very early and early HCC: A systematic review and Bayesian network meta-analysis. Eur. Radiol. 2021, 31, 5400–5408. [Google Scholar] [CrossRef]
- Zaitoun, M.M.A.; Elsayed, S.B.; Zaitoun, N.A.; Soliman, R.K.; Elmokadem, A.H.; Farag, A.A.; Amer, M.; Hendi, A.M.; Mahmoud, N.E.M.; Salah El Deen, D.; et al. Combined therapy with conventional trans-arterial chemoembolization (cTACE) and microwave ablation (MWA) for hepatocellular carcinoma >3–<5 cm. Int. J. Hyperth. 2021, 38, 248–256. [Google Scholar] [CrossRef]
- Li, Z.; Jiao, D.; Han, X.; Si, G.; Li, Y.; Liu, J.; Xu, Y.; Zheng, B.; Zhang, X. Transcatheter arterial chemoembolization combined with simultaneous DynaCT-guided microwave ablation in the treatment of small hepatocellular carcinoma. Cancer Imaging 2020, 20, 13. [Google Scholar] [CrossRef]
- Hermida, M.; Cassinotto, C.; Piron, L.; Aho-Glele, S.; Guillot, C.; Schembri, V.; Allimant, C.; Jaber, S.; Pageaux, G.P.; Assenat, E.; et al. Multimodal Percutaneous Thermal Ablation of Small Hepatocellular Carcinoma: Predictive Factors of Recurrence and Survival in Western Patients. Cancers 2020, 12, 313. [Google Scholar] [CrossRef]
- Cui, R.; Wang, X.H.; Ma, C.; Liu, T.; Cheng, Z.G.; Han, Z.Y.; Liu, F.Y.; Yu, X.L.; Yu, J.; Liang, P. Comparison of Microwave Ablation and Transarterial Chemoembolization for Single-Nodule Hepatocellular Carcinoma Smaller Than 5cm: A Propensity Score Matching Analysis. Cancer Manag. Res. 2019, 11, 10695–10704. [Google Scholar] [CrossRef]
- Lee, S.H.; Jin, Y.J.; Lee, J.W. Survival benefit of radiofrequency ablation for solitary (3-5 cm) hepatocellular carcinoma: An analysis for nationwide cancer registry. Medicine 2017, 96, e8486. [Google Scholar] [CrossRef] [PubMed]
- Salas, S.; Resseguier, N.; Blay, J.Y.; Le Cesne, A.; Italiano, A.; Chevreau, C.; Rosset, P.; Isambert, N.; Soulie, P.; Cupissol, D.; et al. Prediction of local and metastatic recurrence in solitary fibrous tumor: Construction of a risk calculator in a multicenter cohort from the French Sarcoma Group (FSG) database. Ann. Oncol. 2017, 28, 1979–1987. [Google Scholar] [CrossRef]
- Suh, Y.G.; Lee, E.J.; Cha, H.; Yang, S.H.; Seong, J. Prognostic values of vascular endothelial growth factor and matrix metalloproteinase-2 in hepatocellular carcinoma after radiotherapy. Dig. Dis. 2014, 32, 725–732. [Google Scholar] [CrossRef]
- Wang, Q.; Xia, D.; Bai, W.; Wang, E.; Sun, J.; Huang, M.; Mu, W.; Yin, G.; Li, H.; Zhao, H.; et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: A multicentre observational study. J. Hepatol. 2019, 70, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.I.; Bag, H.G.; Ince, V.; Akbulut, S.; Ersan, V.; Usta, S.; Isik, B.; Ogut, Z.; Tuncer, A.; Yilmaz, S. A Combination of Blood Lymphocytes and AST Levels Distinguishes Patients with Small Hepatocellular Carcinomas from Non-cancer Patients. J Gastrointest. Cancer 2021, 52, 1211–1216. [Google Scholar] [CrossRef] [PubMed]
- Ni, J.Y.; Fang, Z.T.; An, C.; Sun, H.L.; Huang, Z.M.; Zhang, T.Q.; Jiang, X.Y.; Chen, Y.T.; Xu, L.F.; Huang, J.H. Comparison of albumin-bilirubin grade, platelet-albumin-bilirubin grade and Child-Turcotte-Pugh class for prediction of survival in patients with large hepatocellular carcinoma after transarterial chemoembolization combined with microwave ablation. Int. J. Hyperth. 2019, 36, 841–853. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Overall (N = 66) | MWA (N = 44) | MWA + TACE (N = 22) | p Value |
|---|---|---|---|---|
| age | 61.14 ± 11.18 | 61.36 ± 10.89 | 60.68 ± 11.98 | 0.817 |
| Sex | ||||
| male | 51 (77.3%) | 31 (70.5%) | 20 (90.9%) | 0.062 |
| female | 15 (22.7%) | 13 (29.5%) | 2 (9.1%) | |
| Hepatic Cirrhosis | ||||
| yes | 50 (75.8%) | 34 (77.3%) | 16 (72.7%) | 0.685 |
| no | 16 (24.2%) | 10 (22.7%) | 6 (27.3%) | |
| Diabetes | ||||
| yes | 12 (18.2%) | 8 (18.2%) | 4 (18.2%) | >0.999 |
| no | 54 (81.8%) | 36 (81.8%) | 18 (81.8%) | |
| Hypertension | ||||
| yes | 17 (25.8%) | 13 (29.5%) | 4 (18.2%) | 0.320 |
| no | 49 (74.2%) | 31 (70.5%) | 18 (81.8%) | |
| HBV | ||||
| yes | 58 (87.9%) | 39 (88.6%) | 19 (86.4%) | >0.999 |
| no | 8 (12.1%) | 5 (11.4%) | 3 (13.6%) | |
| Tumor diameter (mm) | 20.61 ± 9.59 | 18.36 ± 8.47 | 25.09 ± 10.31 | 0.006 |
| BCLC | ||||
| A | 56 (84.8%) | 39 (88.6%) | 17 (77.3%) | 0.396 |
| B | 10 (15.2%) | 5 (11.4%) | 5 (22.7%) | |
| Tumor location | ||||
| special location | 48 (72.7%) | 33 (75%) | 15 (68.2%) | 0.716 |
| traditional location | 18 (27.3%) | 11 (25%) | 7 (31.8%) | |
| Tumor number | ||||
| single | 53 (80.3%) | 39 (88.6%) | 14 (63.6%) | 0.038 |
| multiple | 13 (19.7%) | 5 (11.4%) | 8 (36.4%) | |
| Treatment before ablation | ||||
| yes | 24 (36.4%) | 18 (40.9%) | 6(27.3%) | 0.278 |
| no | 42 (63.6%) | 26 (59.1%) | 16(72.7%) | |
| Baseline AFP(ng/mL) | 433.81 ± 1666.24 | 285.50 ± 1219.54 | 730.44 ± 2325.90 | 0.310 |
| Baseline Lymphocytes (×109/L) | 1.59 ± 0.58 | 1.70 ± 0.61 | 1.37 ± 0.43 | 0.034 |
| Baseline Monocytes(×109/L) | 0.50 ± 0.17 | 0.51 ± 0.17 | 0.47 ± 0.18 | 0.452 |
| Baseline ALB (g/L) | 44.51 ± 3.21 | 43.86 ± 3.18 | 45.77 ± 2.94 | 0.022 |
| Baseline ALT (U/L) | 28.49 ± 14.91 | 30.61 ± 16.70 | 24.36 ± 9.64 | 0.061 |
| Baseline AST (U/L) | 30.06 ± 13.79 | 31.56 ± 15.90 | 27.14 ± 7.77 | 0.137 |
| Baseline rGT (U/L) | 60.56 ± 53.02 | 64.48 ± 56.12 | 52.73 ± 46.44 | 0.400 |
| Baseline LDH(U/L) | 197.89 ± 44.45 | 192.88 ± 43.41 | 207.68 ± 45.83 | 0.207 |
| CD4/CD8 | 1.98 ± 1.21 | 2.04 ± 1.38 | 1.87 ± 0.85 | 0.626 |
| IL-6 (pg/mL) | 6.61 ± 7.11 | 7.11 ± 8.57 | 5.65 ± 2.71 | 0.474 |
| TNF-α (pg/mL) | 12.07 ± 12.21 | 10.43 ± 11.14 | 15.09 ± 13.77 | 0.203 |
| Baseline ALBI | −3.13 ± 0.31 | −3.07 ± 0.31 | −3.25 ± 0.27 | 0.027 |
| Baseline CRP(mg/L) | 3.10 ± 8.28 | 6.85 ± 16.84 | 2.13 ± 2.38 | 0.627 |
| Categories | Overall (N = 66) | MWA (N = 44) | MWA + TACE (N = 22) | ||||
|---|---|---|---|---|---|---|---|
| Grade | 1–4 level | ½ level | ¾ level | ½ level | ¾ level | ½ level | ¾ level |
| Adverse events | 53 (80.3%) | 52 (78.8%) | 12 (18.2%) | 36 (81.8%) | 7 (15.9%) | 16 (72.7%) | 5 (22.7%) |
| Fever | 2 (3.0%) | 2 (3.0%) | 0 (0%) | 1 (2.3%) | 0 (0%) | 1 (4.5%) | 0 (0%) |
| Nausea or vomiting | 13 (19.7%) | 13 (19.7%) | 0 (0%) | 8 (18.2%) | 0 (0%) | 5 (22.7%) | 0 (0%) |
| Fatigue | 5 (7.6%) | 5 (7.6%) | 0 (0%) | 2 (4.5%) | 0 (0%) | 3 (13.6%) | 0 (0%) |
| Abdominal pain/distension | 4 (6.1%) | 4 (6.1%) | 0 (0%) | 3 (6.8%) | 0 (0%) | 1 (2.3%) | 0 (0%) |
| Total bilirubin elevation, transient | 1 (1.5%) | 1 (1.5%) | 0 (0%) | 1 (2.3%) | 0 (0%) | 0 (0%) | 0 (0%) |
| ALT elevation | 45 (68.2%) | 42 (63.6%) | 3 (4.5%) | 28 (63.6%) | 2 (4.5%) | 14 (63.6%) | 1 (2.3%) |
| AST elevation | 53 (80.3%) | 43 (65.2%) | 10 (15.2%) | 30 (68.2%) | 7 (15.9%) | 13 (59.1%) | 3 (13.6%) |
| Characteristics | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| age | 0.99 (0.96, 1.02) | 0.571 | ||
| Sex | ||||
| male | 1.00 (Ref) | 0.146 | ||
| female | 0.50 (0.19, 1.28) | |||
| Hepatic Cirrhosis | ||||
| yes | 1.00 (Ref) | 0.166 | ||
| no | 1.68 (0.81, 3.52) | |||
| Diabetes | ||||
| yes | 1.00 (Ref) | 0.455 | ||
| no | 0.75 (0.35, 1.60) | |||
| Hypertension | ||||
| yes | 1.00 (Ref) | 0.638 | ||
| no | 1.20 (0.56, 2.54) | |||
| HBV | ||||
| yes | 1.00 (Ref) | 0.845 | ||
| no | 0.92 (0.38, 2.22) | |||
| Tumor diameter (mm) | 1.01 (0.97, 1.04) | 0.768 | ||
| BCLC | ||||
| A | 1.00 (Ref) | 0.097 | 1.00 (Ref) | 0.845 |
| B | 1.96 (0.89, 4.33) | 1.11 (0.40, 3.04) | ||
| Tumor location | ||||
| special location | 1.00 (Ref) | 0.086 | 1.00 (Ref) | 0.181 |
| traditional location | 0.53 (0.25, 1.10) | 0.55 (0.23, 1.32) | ||
| Tumor number | ||||
| Single | 1.00 (Ref) | |||
| Multiple | 1.46 (0.68, 3.14) | 0.332 | ||
| Treatment before ablation | ||||
| no | 1.00 (Ref) | <0.001 | 1.00 (Ref) | 0.009 |
| yes | 4.77 (2.05, 11.07) | 4.37 (1.44, 13.32) | ||
| Baseline AFP (ng/mL) | 1.00 (1.00, 1.00) | 0.564 | ||
| Baseline Lymphocytes (×109/L) | 0.47 (0.24, 0.90) | 0.024 | 1.32 (0.52, 3.39) | 0.561 |
| Baseline Monocytes (×109/L) | 0.10 (0.01, 0.84) | 0.034 | 0.07 (0.00, 1.45) | 0.086 |
| Baseline ALB (g/L) | 0.93 (0.85, 1.03) | 0.167 | ||
| Baseline ALT (U/L) | 0.99 (0.97, 1.02) | 0.489 | ||
| Baseline AST (U/L) | 1.00 (0.97, 1.02) | 0.732 | ||
| Baseline rGT (U/L) | 1.00 (0.99, 1.01) | 0.798 | ||
| Baseline LDH (U/L) | 1.01 (0.99, 1.01) | 0.19 | ||
| CD4/CD8 | 0.89 (0.66, 1.20) | 0.444 | ||
| IL-6 (pg/mL) | 0.98 (0.92, 1.04) | 0.448 | ||
| TNF-α (pg/mL) | 1.03 (1.00, 1.06) | 0.05 | 1.03 (0.99, 1.05) | 0.071 |
| Baseline ALBI | 2.57 (0.95, 6.95) | 0.064 | 4.31 (1.17, 15.92) | 0.028 |
| Baseline CRP (mg/L) | 0.98 (0.94, 1.03) | 0.984 | ||
| Characteristics | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| age | 0.98 (0.95, 1.01) | 0.139 | ||
| Sex | ||||
| male | 1.00 (Ref) | 0.121 | ||
| female | 1.99 (0.83, 4.76) | |||
| Hepatic Cirrhosis | ||||
| yes | 1.00 (Ref) | 0.755 | ||
| no | 1.12 (0.55, 2.30) | |||
| Diabetes | ||||
| yes | 1.00 (Ref) | 0.455 | ||
| no | 0.75 (0.36, 1.59) | |||
| Hypertension | ||||
| yes | 1.00 (Ref) | 0.162 | ||
| no | 1.70 (0.81, 3.59) | |||
| HBV | ||||
| yes | 1.00 (Ref) | 0.734 | ||
| no | 1.16 (0.49, 2.78) | |||
| Tumor diameter (mm) | 0.98 (0.95, 1.02) | 0.38 | ||
| BCLC | ||||
| A | 1.00 (Ref) | 0.373 | ||
| B | 1.42 (0.66, 3.09) | |||
| Tumor location | ||||
| special location | 1.00 (Ref) | 0.705 | ||
| traditional location | 0.87 (0.44, 1.76) | |||
| Tumor number | ||||
| single | 1.00 (Ref) | 0.802 | ||
| multiple | 1.10 (0.52, 2.31) | |||
| Treatment before ablation | ||||
| no | 1.00 (Ref) | 0.003 | 1.00 (Ref) | 0.004 |
| yes | 3.10 (1.47, 6.54) | 3.41 (1.49, 7.81) | ||
| Baseline AFP (ng/mL) | 1.00 (1.00, 1.00) | 0.425 | ||
| Baseline Lymphocytes (×109/L) | 0.57 (0.31, 1.05) | 0.07 | 0.95 (0.43, 2.11) | 0.896 |
| Baseline Monocytes (×109/L) | 0.16 (0.02, 1.13) | 0.067 | 0.21 (0.02, 2.51) | 0.219 |
| Baseline ALB (g/L) | 0.97 (0.88, 1.06) | 0.447 | ||
| Baseline ALT (U/L) | 1.00 (0.98, 1.03) | 0.809 | ||
| Baseline AST (U/L) | 1.00 (0.98, 1.02) | 0.904 | ||
| Baseline rGT (U/L) | 1.00 (0.99, 1.01) | 0.430 | ||
| Baseline LDH (U/L) | 1.00 (0.99, 1.01) | 0.984 | ||
| CD4/CD8 | 0.86 (0.59, 1.26) | 0.447 | ||
| IL-6 (pg/mL) | 0.98 (0.92, 1.04) | 0.491 | ||
| TNF-α (pg/mL) | 1.02 (0.99, 1.04) | 0.295 | ||
| Baseline ALBI | 1.86 (0.73, 4.79) | 0.196 | ||
| Baseline CRP (mg/L) | 0.98 (0.93, 1.03) | 0.435 | ||
| Method | LTP | PFS | |||
|---|---|---|---|---|---|
| Number | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Univariate Analysis | |||||
| TACE | 29 (43.9%) | 4.56 (2.14, 9.75) | <0.001 | 2.27 (1.18, 4.35) | 0.014 |
| Thermal ablation | 17 (25.8%) | 1.43 (0.98, 2.08 | 0.063 | 1.73 (0.86, 3.48) | 0.124 |
| Antiangiogenic therapy | 7 (10.6%) | 2.19 (1.38, 3.46) | 0.001 | 3.54 (1.45, 8.62) | 0.005 |
| Surgery | 24 (36.4%) | 1.05 (0.75, 1.47) | 0.775 | 1.10 (0.58, 2.09) | 0.765 |
| Radiotherapy | 3 (4.5%) | 4.08 (1.98, 8.41) | <0.001 | 8.33 (2.27, 30.54) | 0.001 |
| Multivariate Analysis | |||||
| TACE | 29 (43.9%) | 3.92 (1.72, 8.93) | 0.001 | 1.96 (1.00, 3.88) | 0.053 |
| Thermal ablation | 17 (25.8%) | 1.05 (0.43, 2.58) | 0.912 | —— | —— |
| Antiangiogenic therapy | 7 (10.6%) | 2.59 (0.93, 7.23) | 0.068 | 2.54 (0.99, 6.44) | 0.049 |
| Radiotherapy | 3 (4.5%) | 17.95 (4.10, 78.71) | <0.001 | 8.41 (2.29, 30.89) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, G.; Chen, H.; Huang, X.; Cheng, S.; Zheng, S.; Wu, Y.; Zheng, T.; Chen, X.; Guo, X.; Zhang, Z.; et al. Recurrence Outcome in Hepatocellular Carcinoma within Milan Criteria Undergoing Microwave Ablation with or without Transarterial Chemoembolization. Medicina 2022, 58, 1016. https://doi.org/10.3390/medicina58081016
Chen G, Chen H, Huang X, Cheng S, Zheng S, Wu Y, Zheng T, Chen X, Guo X, Zhang Z, et al. Recurrence Outcome in Hepatocellular Carcinoma within Milan Criteria Undergoing Microwave Ablation with or without Transarterial Chemoembolization. Medicina. 2022; 58(8):1016. https://doi.org/10.3390/medicina58081016
Chicago/Turabian StyleChen, Guobin, Hong Chen, Xing Huang, Sisi Cheng, Susu Zheng, Yanfang Wu, Tanghui Zheng, Xiaochun Chen, Xinkun Guo, Zhenzhen Zhang, and et al. 2022. "Recurrence Outcome in Hepatocellular Carcinoma within Milan Criteria Undergoing Microwave Ablation with or without Transarterial Chemoembolization" Medicina 58, no. 8: 1016. https://doi.org/10.3390/medicina58081016
APA StyleChen, G., Chen, H., Huang, X., Cheng, S., Zheng, S., Wu, Y., Zheng, T., Chen, X., Guo, X., Zhang, Z., Xie, X., & Zhang, B. (2022). Recurrence Outcome in Hepatocellular Carcinoma within Milan Criteria Undergoing Microwave Ablation with or without Transarterial Chemoembolization. Medicina, 58(8), 1016. https://doi.org/10.3390/medicina58081016