
Relation of Dietary n-3 and n-6 Fatty Acid Intakes to Metabolic Syndrome in Middle-Aged People Depending on the Level of HbA1c: A Review of National Health and Nutrition Survey Data from 2014 to 2016


Abstract
1. Introduction
1.1. Need for Study
1.2. Recent Study Trends
1.3. Study Purpose
2. Materials and Methods
2.1. Study Design
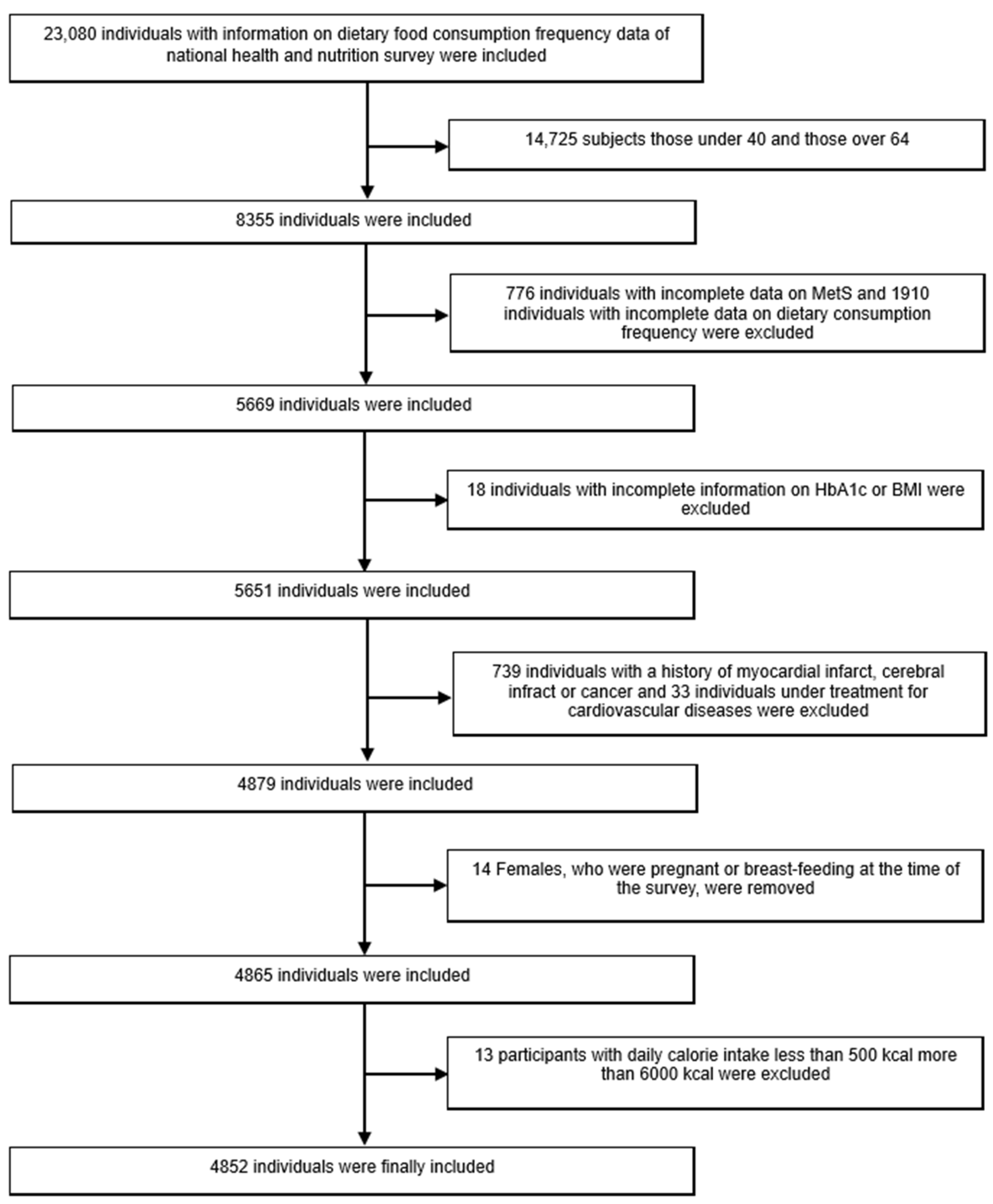
2.2. Study Participants and Data Collection
2.3. Study Tools
2.3.1. Evaluating Variables
- (1)
- Variables Related to Metabolic Syndrome
- (2)
- Variables for Dietary Intake
- (3)
- Variables for Lifestyles and Demography
2.3.2. Evaluating Metabolic Syndrome
- Waist circumference: male ≥ 90 cm, female ≥ 85 cm;
- TG: ≥150 mg/dL;
- HDL cholesterol: male ≥ 40 mg/dL, female ≥ 50 mg/dL;
- Blood pressure: systolic ≥ 130 mmHg or diastolic ≥ 85 mmHg;
- Fasting blood glucose: ≥100 mg/dL.
2.3.3. Defining Confounding Variables
2.3.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hulbert, A.J.; Turner, N.; Storlien, L.; Else, P. Dietary fats and membrane function: Implications for metabolism and disease. Biol. 2005, 80, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Scollan, N.D.; Choi, N.-J.; Kurt, E.; Fisher, A.V.; Enser, M.; Wood, J.D. Manipulating the fatty acid composition of muscle and adipose tissue in beef cattle. Br. J. Nutr. 2001, 85, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Mazereeuw, G.; Lanctot, K.L.; Chau, S.A.; Swardfager, W.; Herrmann, N. Effects of omega-3 fatty acids on cognitive performance: A meta-analysis. Neurobiol. Aging 2012, 33, 1482.e17–1482.e29. [Google Scholar] [CrossRef] [PubMed]
- Mangano, K.M.; Kerstetter, J.E.; Kenny, A.M.; Insogna, K.; Walsh, S. An investigation of the association between omega 3 FA and bone mineral density among older adults: Results from the National Health and Nutrition Examination Survey years 2005–2008. Osteoporos. Int. 2014, 25, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.-S. Effects of Omega-3 on Lipid and Liver Function Tests. Korean J. Clin. Lab. Sci. 2018, 50, 183–189. [Google Scholar] [CrossRef]
- Chen, J.; Sun, B.; Zhang, D. Association of dietary n3 and n6 fatty acids intake with hypertension: NHANES 2007–2014. Nutrients 2019, 11, 1232. [Google Scholar] [CrossRef]
- Simopoulos, A.P. An increase in the omega-6/omega-3 fatty acid ratio increases the risk for obesity. Nutrients 2016, 8, 128. [Google Scholar] [CrossRef]
- Romacho, T.; Glosse, P.; Richter, I.; Elsen, M.; Schoemaker, M.H.; Van Tol, E.A.; Eckel, J. Nutritional ingredients modulate adipokine secretion and inflammation in human primary adipocytes. Nutrients 2015, 7, 865–886. [Google Scholar] [CrossRef]
- Tortosa-Caparrós, E.; Navas-Carrillo, D.; Marín, F.; Orenes-Piñero, E. Anti-inflammatory effects of omega 3 and omega 6 polyunsaturated fatty acids in cardiovascular disease and metabolic syndrome. Crit. Rev. Food Sci. Nutr. 2017, 57, 3421–3429. [Google Scholar] [CrossRef]
- Lee, T.C.; Ivester, P.; Hester, A.G.; Sergeant, S.; Case, L.D.; Morgan, T.; Kouba, E.O.; Chilton, F.H. The impact of polyunsaturated fatty acid-based dietary supplements on disease biomarkers in a metabolic syndrome/diabetes population. Lipids Health Dis. 2014, 13, 196. [Google Scholar] [CrossRef]
- Isomaa, B.; Almgren, P.; Tuomi, T.; Forsen, B.; Lahti, K.; Nissen, M.; Taskinen, M.-R.; Groop, L. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001, 24, 683–689. [Google Scholar] [CrossRef]
- Statistics Korea. Annual Report on the Cause of Death Statistics in Korea; Statistics Korea: Daegeon, Korea, 2012.
- Schmidt, C.; Bergström, G.M. The metabolic syndrome predicts cardiovascular events: Results of a 13-year follow-up in initially healthy 58-year-old men. Metab. Syndr. Relat. Disord. 2012, 10, 394–399. [Google Scholar] [CrossRef]
- Park, Y.-W.; Zhu, S.; Palaniappan, L.; Heshka, S.; Carnethon, M.R.; Heymsfield, S.B. The metabolic syndrome: Prevalence and associated risk factor findings in the US population from the Third National Health and Nutrition Examination Survey, 1988–1994. Arch. Intern. Med. 2003, 163, 427–436. [Google Scholar] [CrossRef]
- Jeon, J.; Kim, S. Depression, stress and how they are related with health behaviors and metabolic syndrome among women over 40 years. J. Korean Soc. Matern. Child Health 2012, 16, 263–273. [Google Scholar]
- Zhang, R.; Sun, J.; Li, Y.; Zhang, D. Associations of n-3, n-6 fatty acids intakes and n-6: N-3 ratio with the risk of depressive symptoms: NHANES 2009–2016. Nutrients 2020, 12, 240. [Google Scholar] [CrossRef]
- Cho, D.Y.; Koo, J.-W. Differences in metabolic syndrome prevalence by employment type and sex. Int. J. Environ. Res. Public Health 2018, 15, 1798. [Google Scholar] [CrossRef]
- Demiral, Y.; Arik, H.; Toğrul, B.U. The association between employment status and metabolic syndrome in women: Modifying effect of education. Women Health 2012, 52, 755–770. [Google Scholar] [CrossRef]
- Kondo, T.; Osugi, S.; Shimokata, K.; Honjo, H.; Morita, Y.; Yamashita, K.; Maeda, K.; Muramatsu, T.; Shintani, S.; Matsushita, K. Metabolic syndrome and all-cause mortality, cardiac events, and cardiovascular events: A follow-up study in 25,471 young-and middle-aged Japanese men. Eur. J. Prev. Cardiol. 2011, 18, 574–580. [Google Scholar] [CrossRef]
- Kwon, H.S.; Park, Y.M.; Lee, H.J.; Lee, J.H.; Choi, Y.H.; Ko, S.H.; Lee, J.M.; Kim, S.R.; Kang, S.Y.; Lee, W.C. Prevalence and clinical characteristics of the metabolic syndrome in middle-aged Korean adults. Korean J. Intern. Med. 2005, 20, 310. [Google Scholar] [CrossRef]
- Kim, M.-h.; Lee, S.-h.; Shin, K.-S.; Son, D.-Y.; Kim, S.-H.; Joe, H.; Yoo, B.-W.; Hong, S.-H.; Cho, C.-Y.; Shin, H.-S. The change of metabolic syndrome prevalence and its risk factors in Korean adults for decade: Korea National Health and Nutrition Examination Survey for 2008–2017. Korean J. Fam. Pract. 2020, 10, 44–52. [Google Scholar] [CrossRef]
- Yoon, Y.S.; Oh, S.W. Optimal waist circumference cutoff values for the diagnosis of abdominal obesity in Korean adults. Endocrinol. Metab. 2014, 29, 418–426. [Google Scholar] [CrossRef]
- Kim, S.-H.; Choi, H.-S.; Ji, S.-H.; Park, Y.-M. The relationship of the prevalence metabolic syndrome and the difference of life style in Korean adult. Korean J. Fam. Pract. 2015, 5, 500–509. [Google Scholar]
- DeFronzo, R.A. The triumvirate: β-cell, muscle, liver: A collusion responsible for NIDDM. Diabetes 1988, 37, 667–687. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Bonadonna, R.C.; Ferrannini, E. Pathogenesis of NIDDM: A balanced overview. Diabetes Care 1992, 15, 318–368. [Google Scholar] [CrossRef]
- Shulman, G.I. Cellular mechanisms of insulin resistance. J. Clin. Investig. 2000, 106, 171–176. [Google Scholar] [CrossRef]
- Nakamura, H.; Hara, A.; Tsujiguchi, H.; Thi Thu Nguyen, T.; Kambayashi, Y.; Miyagi, S.; Yamada, Y.; Suzuki, K.; Shimizu, Y.; Nakamura, H. Relationship between dietary n-6 fatty acid intake and hypertension: Effect of glycated hemoglobin levels. Nutrients 2018, 10, 1825. [Google Scholar] [CrossRef]
- Lin, T.C.; Lee, H.M.; Seo, H.N.; Oh, J.S.; Kong, H.R.; Cho, S.A.; Choi, B.G. Correlation between non-alcoholic fatty liver disease and hemoglobin A1c level in adult males without diabetes. Korean J. Fam. Pract. 2018, 8, 131–135. [Google Scholar] [CrossRef]
- Das, U.N. A defect in the activity of Δ6 and Δ5 desaturases may be a factor predisposing to the development of insulin resistance syndrome. Prostaglandins Leukot. Essent. Fat. Acids 2005, 72, 343–350. [Google Scholar] [CrossRef]
- Russo, G.L. Dietary n− 6 and n− 3 polyunsaturated fatty acids: From biochemistry to clinical implications in cardiovascular prevention. Biochem. Pharmacol. 2009, 77, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Weylandt, K.H.; Kang, J.X.; Wiedenmann, B.; Baumgart, D.C. Lipoxins and resolvins in inflammatory bowel disease. Inflamm. Bowel Dis. 2007, 13, 797–799. [Google Scholar] [CrossRef] [PubMed]
- Galli, C. Dietary ω3 and ω6 Fatty Acids: Biological Effects and Nutritional Essentiality; Springer Science & Business Media: New York, NY, USA, 2013; Volume 171. [Google Scholar]
- Mirmiran, P.; Hosseinpour-Niazi, S.; Naderi, Z.; Bahadoran, Z.; Sadeghi, M.; Azizi, F. Association between interaction and ratio of ω-3 and ω-6 polyunsaturated fatty acid and the metabolic syndrome in adults. Nutrition 2012, 28, 856–863. [Google Scholar] [CrossRef]
- Chien, K.-L.; Chao, C.-L.; Kuo, C.-H.; Lin, H.-J.; Liu, P.-H.; Chen, P.-R.; Hsu, H.-C.; Lee, B.-C.; Lee, Y.-T.; Chen, M.-F. Plasma fatty acids and the risk of metabolic syndrome in ethnic Chinese adults in Taiwan. Lipids Health Dis. 2011, 10, 33. [Google Scholar] [CrossRef]
- Vanhala, M.; Saltevo, J.; Soininen, P.; Kautiainen, H.; Kangas, A.J.; Ala-Korpela, M.; Mäntyselkä, P. Serum omega-6 polyunsaturated fatty acids and the metabolic syndrome: A longitudinal population-based cohort study. Am. J. Epidemiol. 2012, 176, 253–260. [Google Scholar] [CrossRef]
- Lee, E.; Lee, S.; Park, Y. n-3 Polyunsaturated fatty acids and trans fatty acids in patients with the metabolic syndrome: A case–control study in Korea. Br. J. Nutr. 2008, 100, 609–614. [Google Scholar] [CrossRef]
- Baik, I.; Abbott, R.D.; Curb, J.D.; Shin, C. Intake of fish and n-3 fatty acids and future risk of metabolic syndrome. J. Am. Diet. Assoc. 2010, 110, 1018–1026. [Google Scholar] [CrossRef]
- Jang, H.; Park, K. Omega-3 and omega-6 polyunsaturated fatty acids and metabolic syndrome: A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 765–773. [Google Scholar] [CrossRef]
- Steiner, C.A.; Friedman, B. Peer reviewed: Hospital utilization, costs, and mortality for adults with multiple chronic conditions, nationwide inpatient sample, 2009. Prev. Chronic Dis. 2013, 10, E62. [Google Scholar] [CrossRef][Green Version]
- Bosworth, H.B.; Bastian, L.A.; Kuchibhatla, M.N.; Steffens, D.C.; McBride, C.M.; Skinner, C.S.; Rimer, B.K.; Siegler, I.C. Depressive symptoms, menopausal status, and climacteric symptoms in women at midlife. Psychosom. Med. 2001, 63, 603–608. [Google Scholar] [CrossRef]
- Na, S.-K.; Cheon, S.-H.; Choi, Y.-J.; Lee, H.-J.; Roh, Y.-K.; Choi, M.-K. Relationship between abdominal obesity and proportion of supper and late-night meals. Korean J. Obes. 2016, 25, 92–98. [Google Scholar] [CrossRef]
- Athyros, V.G.; Ganotakis, E.S.; Elisaf, M.; Mikhailidis, D.P. The prevalence of the metabolic syndrome using the National Cholesterol Educational Program and International Diabetes Federation definitions. Curr. Med. Res. Opin. 2005, 21, 1157–1159. [Google Scholar] [CrossRef]
- Park, H.-A. An introduction to logistic regression: From basic concepts to interpretation with particular attention to nursing domain. J. Korean Acad. Nurs. 2013, 43, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.-J.; Lee, H.-S.; Lee, J.-W. Association of carbohydrate and fat intake with metabolic syndrome. Clin. Nutr. 2018, 37, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Hartweg, J.; Perera, R.; Montori, V.M.; Dinneen, S.F.; Neil, A.H.; Farmer, A.J. Omega-3 polyunsaturated fatty acids (PUFA) for type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2008, 2008, CD003205. [Google Scholar] [CrossRef] [PubMed]
- Delarue, J.; Couet, C.; Cohen, R.; Brechot, J.-F.; Antoine, J.-M.; Lamisse, F. Effects of fish oil on metabolic responses to oral fructose and glucose loads in healthy humans. Am. J. Physiol. Endocrinol. Metab. 1996, 270, E353–E362. [Google Scholar] [CrossRef] [PubMed]
- Patti, L.; Maffettone, A.; Iovine, C.; Di Marino, L.; Annuzzi, G.; Riccardi, G.; Rivellese, A.A. Long-term effects of fish oil on lipoprotein subfractions and low density lipoprotein size in non-insulin-dependent diabetic patients with hypertriglyceridemia. Atherosclerosis 1999, 146, 361–367. [Google Scholar] [CrossRef]
- Rivellese, A.A.; Maffettone, A.; Iovine, C.; Di Marino, L.; Annuzzi, G.; Mancini, M.; Riccardi, G. Long-term effects of fish oil on insulin resistance and plasma lipoproteins in NIDDM patients with hypertriglyceridemia. Diabetes Care 1996, 19, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Sirtori, C.R.; Paoletti, R.; Mancini, M.; Crepaldi, G.; Manzato, E.; Rivellese, A.; Pamparana, F.; Stragliotto, E. N-3 fatty acids do not lead to an increased diabetic risk in patients with hyperlipidemia and abnormal glucose tolerance. Italian Fish Oil Multicenter Study. Am. J. Clin. Nutr. 1997, 65, 1874–1881. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp. Biol. Med. 2008, 233, 674–688. [Google Scholar] [CrossRef]
- Petersson, H.; Basu, S.; Cederholm, T.; Risérus, U. Serum fatty acid composition and indices of stearoyl-CoA desaturase activity are associated with systemic inflammation: Longitudinal analyses in middle-aged men. Br. J. Nutr. 2008, 99, 1186–1189. [Google Scholar] [CrossRef]
- Ratnayake, W.N.; Galli, C. Fat and fatty acid terminology, methods of analysis and fat digestion and metabolism. Ann. Nutr. Metab. 2009, 55, 8–43. [Google Scholar] [CrossRef]
- Jia, Z.; Aoyagi, T.; Yang, T. mPGES-1 protects against DOCA-salt hypertension via inhibition of oxidative stress or stimulation of NO/cGMP. Hypertension 2010, 55, 539–546. [Google Scholar] [CrossRef]
- Echeverría, F.; Ortiz, M.; Valenzuela, R.; Videla, L.A. Long-chain polyunsaturated fatty acids regulation of PPARs, signaling: Relationship to tissue development and aging. Prostaglandins Leukot. Essent. Fat. Acids 2016, 114, 28–34. [Google Scholar] [CrossRef]
- Volcik, K.A.; Nettleton, J.A.; Ballantyne, C.M.; Boerwinkle, E. Peroxisome proliferator–activated receptor α genetic variation interacts with n− 6 and long-chain n− 3 fatty acid intake to affect total cholesterol and LDL-cholesterol concentrations in the Atherosclerosis Risk in Communities Study. Am. J. Clin. Nutr. 2008, 87, 1926–1931. [Google Scholar] [CrossRef]
- Yary, T.; Voutilainen, S.; Tuomainen, T.P.; Ruusunen, A.; Nurmi, T.; Virtanen, J. Omega-6 polyunsaturated fatty acids, serum zinc, delta-5-and delta-6-desaturase activities and incident metabolic syndrome. J. Hum. Nutr. Diet. 2017, 30, 506–514. [Google Scholar] [CrossRef]
- Hu, F.B.; Stampfer, M.J.; Manson, J.E.; Rimm, E.B.; Wolk, A.; Colditz, G.A.; Hennekens, C.H.; Willett, W.C. Dietary intake of α-linolenic acid and risk of fatal ischemic heart disease among women. Am. J. Clin. Nutr. 1999, 69, 890–897. [Google Scholar] [CrossRef]
- Cicero, A.F.; Tartagni, E.; Ertek, S. Nutraceuticals for metabolic syndrome management: From laboratory to benchside. Curr. Vasc. Pharmacol. 2014, 12, 565–571. [Google Scholar] [CrossRef]
- Clarke, S.D. Polyunsaturated fatty acid regulation of gene transcription: A molecular mechanism to improve the metabolic syndrome. J. Nutr. 2001, 131, 1129–1132. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men (n = 1875) | Women (n = 2977) | |||||
|---|---|---|---|---|---|---|
| Non-MetS | MetS | p-Value | Non-MetS | MetS | p-Value | |
| Participants (n) | 1139 | 736 | 2130 | 847 | ||
| Age | 51.2 ± 7.2 | 52.9 ± 7.0 | <0.001 | 50.6 ± 6.9 | 54.7 ± 6.6 | <0.001 |
| BMI | 23.6 ± 2.6 | 26.2 ± 3.1 | <0.001 | 22.7 ± 2.7 | 26.3 ± 3.5 | <0.001 |
| Physical activity index | 24.2 ± 21.6 | 22.8 ± 21.8 | 0.154 | 22.1 ± 19.2 | 18.1 ± 14.8 | <0.001 |
| HbA1c | 5.6 ± 0.6 | 6.14 ± 1.1 | <0.001 | 5.5 ± 0.5 | 6.1 ± 1.0 | <0.001 |
| Smoking status (n, %) | <0.001 | 0.062 | ||||
| Current | 414 (36.3%) | 294 (39.9%) | 81 (3.8%) | 47 (5.5%) | ||
| Non | 249 (21.9%) | 105 (14.3%) | 1974 (92.7%) | 777 (91.7%) | ||
| Ex | 476 (41.8%) | 337 (45.8%) | 75 (3.5%) | 23 (2.7%) | ||
| Drinking frequency (n, %) | <0.001 | 0.008 | ||||
| 0~1/month | 424 (37.2%) | 212 (28.8%) | 1448 (68%) | 625 (73.8%) | ||
| 2–4/month | 326 (28.6%) | 184 (25.0%) | 432 (20.3%) | 141 (16.6%) | ||
| More than 2/week | 389 (34.2%) | 340 (46.2%) | 250 (11.7%) | 81 (9.6%) | ||
| Educational level (n, %) | <0.001 | <0.001 | ||||
| Below high school | 584 (51.3%) | 450 (61.1%) | 1422 (66.8%) | 695 (82.1%) | ||
| University | 555 (48.7%) | 286 (38.9%) | 708 (33.2%) | 152 (17.9%) | ||
| Occupational status (n, %) | 0.025 | <0.001 | ||||
| Unemployed | 107 (9.4%) | 97 (13.2%) | 825 (38.7%) | 363 (42.9%) | ||
| Employed | 1017 (89.3%) | 626 (85.1%) | 1193 (56%) | 406 (47.9%) | ||
| Housework | 15 (1.3%) | 13 (1.8%) | 112 (5.3%) | 78 (9.2%) | ||
| Night/shift work (n,%) | 0.584 | 0.816 | ||||
| Yes | 82 (7.2%) | 58 (7.9%) | 56 (2.6%) | 21 (2.5%) | ||
| No | 1057 (92.8%) | 678 (92.1%) | 2074 (97.4%) | 825 (97.5%) | ||
| Lowest income quartile (n, %) | 69 (6.1%) | 70 (9.5%) | 0.005 | 172 (8.1%) | 139 (16.4%) | <0.001 |
| Daily dietary intake | ||||||
| Total energy (kcal) | 2144.7 ± 690.9 | 2230.8 ± 757.7 | 0.013 | 1698.9 ± 591.7 | 1621.0 ± 570.8 | 0.001 |
| Carbohydrate (g) | 339.4 ± 98.7 | 339.3 ± 104.0 | 0.975 | 282.8 ± 94.6 | 278.2 ± 92.0 | 0.227 |
| Protein (g) | 66.67 ± 27.1 | 67.7 ± 30.3 | 0.471 | 57.8 ± 24.7 | 52.9 ± 22.8 | <0.001 |
| Fat (g) | 38.6 ± 21.0 | 38.2 ± 22.1 | 0.67 | 33.7 ± 18.7 | 28.3 ± 17.1 | <0.001 |
| SFA (g) | 11.3 ± 6.5 | 11.7 ± 6.6 | 0.515 | 9.4 ± 5.47 | 7.8 ± 5.0 | <0.001 |
| MUFA (g) | 12.0± 7.0 | 11.9 ± 7.4 | 0.865 | 10.1 ± 6.0 | 8.4 ± 5.57 | <0.001 |
| PUFA (g) | 10.2 ± 5.4 | 10.2 ± 5.9 | 0.904 | 9.5 ± 5.3 | 8.18 ± 4.8 | <0.001 |
| n-6 FA (g) | 9.1 ± 4.8 | 9.1 ± 5.3 | 0.943 | 8.37 ± 4.7 | 7.2 ± 4.3 | <0.001 |
| n-3 FA (g) | 1.25 ± 0.7 | 1.3 ± 0.8 | 0.812 | 1.2 ± 0.7 | 1.06 ± 0.6 | <0.001 |
| Cholesterol (mg) | 241.5 ± 152.3 | 240.9 ± 160.8 | 0.938 | 224.2 ± 148.9 | 190.9 ± 144.9 | <0.001 |
| Total fiber (g) | 20.7 ± 8.7 | 21.1 ± 9.6 | 0.307 | 21.1 ± 9.4 | 20.3 ± 8.7 | 0.048 |
| n-6/n-3 FA ratio | 7.5 ± 1.6 | 7.4 ± 1.5 | 0.543 | 7.1 ± 1.4 | 7.0 ± 1.5 | 0.056 |
| Men (n = 1875) Tertiles of PUFA Intake | Women (n = 2977) Tertiles of PUFA Intake | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | |
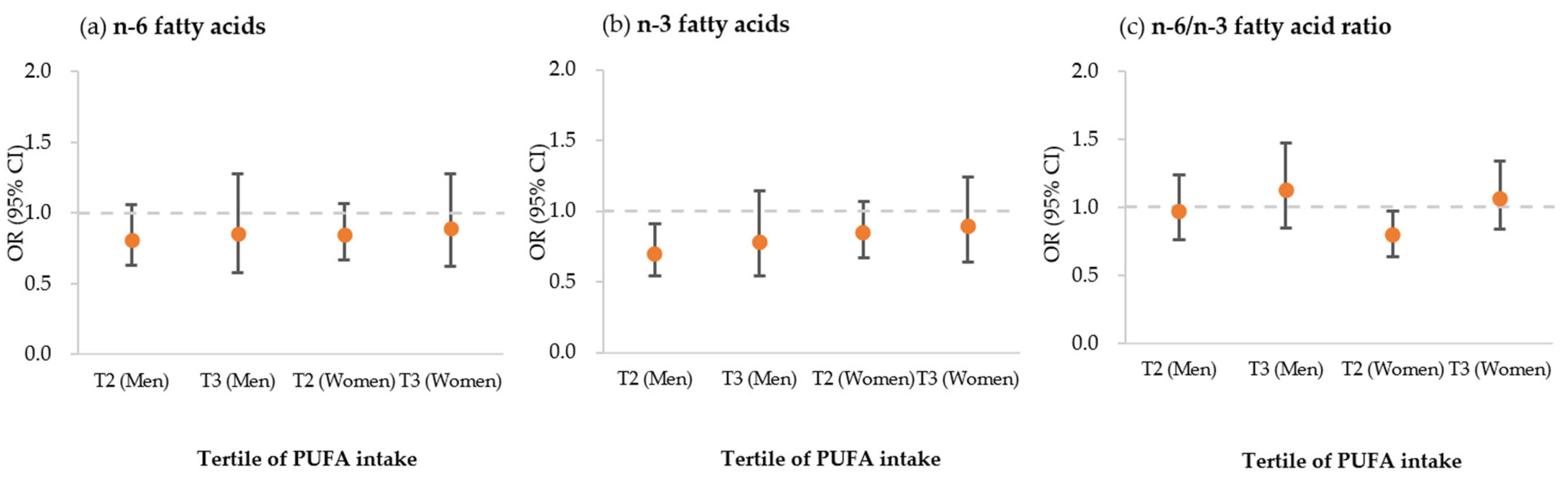
| n-6 Fatty Acid | ||||||
| Range of intake(g/day) | <6.4 | 6.4–10.1 | >10.1 | <5.62 | 5.6–8.9 | >8.9 |
| Metabolic syndrome | 1 | 0.81 (0.63–1.06) | 0.86 (0.58–1.28) | 1 | 0.85 (0.67–1.07) | 0.89 (0.62–1.28) |
| High BP (SBP > 130 or DBP > 85 mmHg) | 1 | 0.77 (0.59–0.99) | 0.97 (0.65–1.44) | 1 | 0.92 (0.74–1.15) | 1.17 (0.83–1.66) |
| Increased waist circumference (>90 cm) | 1 | 0.77 (0.59–1.01) | 1.00 (0.67–1.50) | 1 | 0.84 (0.66–1.06) | 0.88 (0.61–1.26) |
| Increased fasting blood sugar (>100 mg/dL) | 1 | 0.86 (0.66–1.12) | 0.82 (0.55–1.22) | 1 | 0.94 (0.75–1.17) | 0.99 (0.70–1.40) |
| Low blood HDL cholesterol (<40 mg/dL) | 1 | 1.03 (0.78–1.35) | 1.08 (0.71–1.63) | 1 | 0.78 (0.63–0.96) | 0.71 (0.52–0.97) |
| High blood triglycerides (>150 mg/dL) | 1 | 1.00 (0.77–1.31) | 0.92 (0.61–1.37) | 1 | 0.85 (0.68–1.06) | 0.87 (0.61–1.23) |
| n-3 Fatty Acid | ||||||
| Range of intake(g/day) | <0.87 | 0.87–1.40 | >1.40 | <0.80 | 0.80–1.29 | >1.29 |
| Metabolic syndrome | 1 | 0.70 (0.54–0.91) | 0.78 (0.54–1.14) | 1 | 0.85 (0.68–1.06) | 0.89 (0.64–1.24) |
| High BP (SBP > 130 or DBP > 85 mmHg) | 1 | 0.71 (0.55–0.92) | 0.83 (0.57–1.20) | 1 | 1.04 (0.84–1.29) | 1.24 (0.91–1.70) |
| Increased waist circumference (>90 cm) | 1 | 0.87 (0.67–1.14) | 0.99 (0.68–1.45) | 1 | 0.79 (0.63–0.99) | 0.91 (0.65–1.26) |
| Increased fasting blood sugar (>100 mg/dL) | 1 | 0.73 (0.57–0.95) | 0.70 (0.48–1.02) | 1 | 0.78 (0.62–0.97) | 0.86 (0.63–1.18) |
| Low blood HDL cholesterol (<40 mg/dL) | 1 | 0.89 (0.68–1.17) | 0.94 (0.63–1.39) | 1 | 0.75 (0.61–0.92) | 0.67 (0.50–0.90) |
| High blood triglycerides (>150 mg/dL) | 1 | 0.83 (0.64–1.08) | 0.76 (0.52–1.12) | 1 | 0.82 (0.66–1.02) | 0.80 (0.58–1.10) |
| n-6/n-3 Ratio | ||||||
| Range of intake | <6.8 | 6.8–7.8 | >7.8 | <6.6 | 6.6–7.5 | >7.5 |
| Metabolic syndrome | 1 | 0.97 (0.76–1.24) | 1.12 (0.85–1.47) | 1 | 0.79 (0.64–0.97) | 1.06 (0.84–1.34) |
| High BP (SBP > 130 or DBP > 85 mmHg) | 1 | 1.05 (0.83–1.34) | 1.29 (0.98–1.71) | 1 | 0.74 (0.61–0.90) | 0.72 (0.58–0.91) |
| Increased waist circumference (>90 cm) | 1 | 0.94 (0.73–1.21) | 1.10 (0.83–1.46) | 1 | 0.79 (0.64–0.98) | 1.07 (0.84–1.35) |
| Increased fasting blood sugar (>100 mg/dL) | 1 | 0.86 (0.67–1.09) | 0.87 (0.66–1.14) | 1 | 0.81 (0.66–0.99) | 0.81 (0.64–1.01) |
| Low blood HDL cholesterol (<40 mg/dL) | 1 | 1.02 (0.79–1.32) | 0.97 (0.73–1.30) | 1 | 0.85 (0.70–1.02) | 0.92 (0.74–1.14) |
| High blood triglycerides (>150 mg/dL) | 1 | 0.88 (0.69–1.13) | 1.14 (0.86–1.51) | 1 | 0.82 (0.67–1.00) | 0.96 (0.76–1.20) |
| Odds Ratio—HbA1c 1/3 (<5.4) | Odds Ratio—HbA1c 2/3 (5.4—5.7) | Odds Ratio—HbA1c 3/3 (>5.7) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Tertiles of PUFA Intake | Tertiles of PUFA Intake | Tertiles of PUFA Intake | |||||||
| Men (n = 1875) | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 |
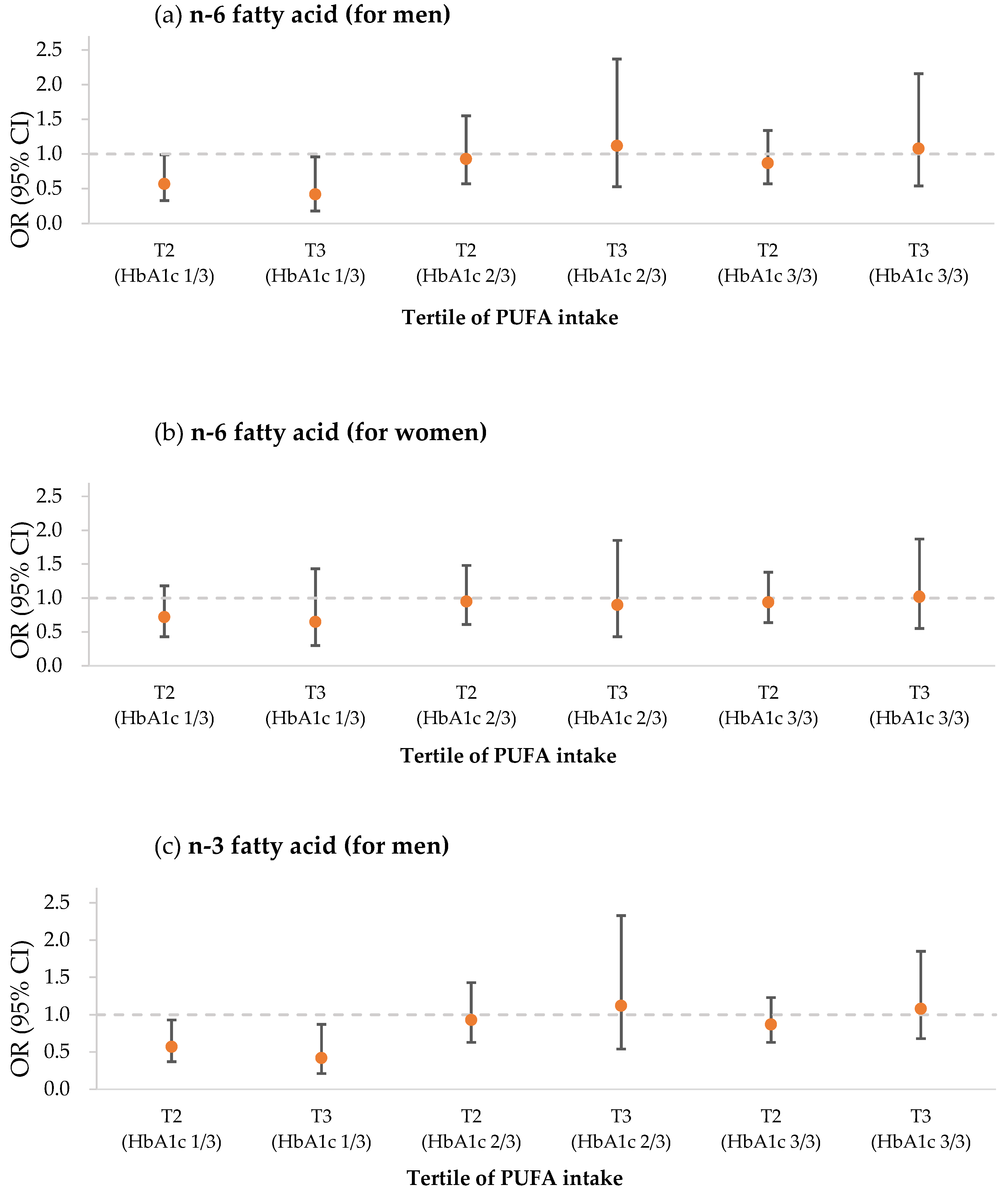
| n-6 Fatty Acid | |||||||||
| Range of intake | <6.4 | 6.4–10.1 | >10.1 | <6.4 | 6.4–10.1 | >10.1 | <6.4 | 6.4–10.1 | >10.1 |
| Crude | 1 | 0.24 (0.17–0.34) | 0.25 (0.18–0.35) | 1 | 0.50 (0.37–0.67) | 0.56 (0.42–0.75) | 1 | 1.27 (0.98–1.64) | 1.64 (1.24–2.16) |
| Model 1 | 1 | 0.57 (0.36–0.89) | 0.57 (0.37–0.88) | 1 | 0.86 (0.57–1.30) | 0.96 (0.64–1.42) | 1 | 0.88 (0.62–1.26) | 1.15 (0.80–1.66) |
| Model 2 | 1 | 0.67 (0.42–1.09) | 0.59 (0.36–0.96) | 1 | 0.98 (0.63–1.53) | 1.27 (0.82–1.98) | 1 | 0.90 (0.62–1.30) | 1.16 (0.78–1.71) |
| Model 3 | 1 | 0.57 (0.33–0.99) | 0.42 (0.18–0.96) | 1 | 0.93 (0.57–1.55) | 1.12 (0.53–2.37) | 1 | 0.87 (0.57–1.34) | 1.08 (0.54–2.16) |
| n-3 Fatty Acid | |||||||||
| Range of intake | <0.9 | 0.9–1.4 | >1.4 | <0.9 | 0.9–1.4 | >1.4 | <0.9 | 0.9–1.4 | >1.4 |
| Crude | 1 | 0.23 (0.16–0.32) | 0.24 (0.17–0.35) | 1 | 0.40 (0.29–0.56) | 0.61 (0.46–0.81) | 1 | 1.18 (0.92–1.53) | 1.69 (1.28–2.23) |
| Model 1 | 1 | 0.50 (0.32–0.79) | 0.54 (0.35–0.85) | 1 | 0.64 (0.42–0.98) | 0.96 (0.65–1.42) | 1 | 0.79 (0.55–1.13) | 1.14 (0.79–1.64) |
| Model 2 | 1 | 0.57 (0.35–0.93) | 0.56 (0.35–0.91) | 1 | 0.77 (0.49–1.22) | 1.24 (0.80–1.91) | 1 | 0.78 (0.54–1.13) | 1.13 (0.77–1.68) |
| Model 3 | 1 | 0.47 (0.27–0.83) | 0.37 (0.16–0.82) | 1 | 0.75 (0.45–1.25) | 1.13 (0.55–2.34) | 1 | 0.70 (0.46–1.06) | 0.85 (0.45–1.62) |
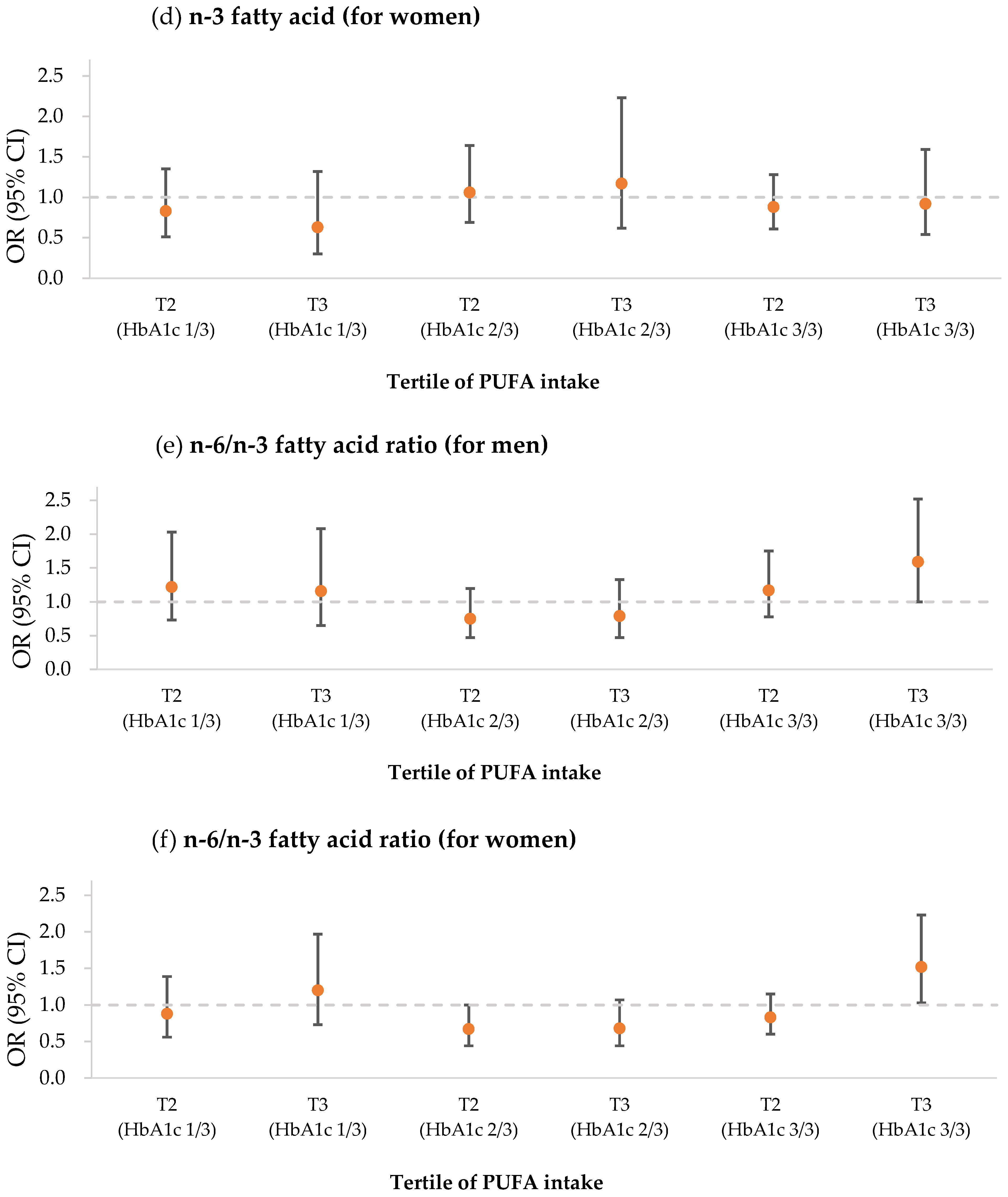
| n-6/n-3 Ratio | |||||||||
| Range of intake | <6.9 | 6.9–7.8 | >7.8 | <6.9 | 6.9–7.8 | >7.8 | <6.9 | 6.9–7.8 | >7.8 |
| Crude | 1 | 0.29 (0.21–0.39) | 0.30 (0.22–0.41) | 1 | 0.42 (0.31–0.58) | 0.55 (0.41–0.74) | 1 | 1.34 (1.03–1.76) | 1.51 (1.15–1.97) |
| Model 1 | 1 | 0.87 (0.56–1.35) | 0.90 (0.58–1.40) | 1 | 0.62 (0.41–0.94) | 0.81 (0.54–1.22) | 1 | 0.94 (0.66–1.35) | 1.06 (0.74–1.51) |
| Model 2 | 1 | 1.81 (0.68–1.75) | 1.00 (0.62–1.60) | 1 | 0.78 (0.50–1.21) | 0.88 (0.58–1.35) | 1 | 0.98 (0.67–1.41) | 1.08 (0.75–1.55) |
| Model 3 | 1 | 1.22 (0.73–2.03) | 1.16 (0.65–2.08) | 1 | 0.75 (0.47–1.20) | 0.79 (0.47–1.33) | 1 | 1.17 (0.78–1.75) | 1.59 (1.00–2.52) |
| Women (n = 2977) | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 |
| n-6 Fatty Acid | |||||||||
| Range of intake | <5.6 | 5.6–8.9 | >8.9 | <5.6 | 5.6–8.9 | >8.9 | <5.6 | 5.6–8.9 | >8.9 |
| Crude | 1 | 0.13 (0.10–0.18) | 0.10 (0.07–0.14) | 1 | 0.28 (0.22–0.37) | 0.178 (0.13–0.24) | 1 | 1.12 (0.89–1.41) | 1.18 (0.92–1.50) |
| Model 1 | 1 | 0.46 (0.31–0.69) | 0.35 (0.23–0.53) | 1 | 0.62 (0.43–0.88) | 0.37 (0.26–0.54) | 1 | 0.75 (0.55–1.01) | 0.79 (0.58–1.08) |
| Model 2 | 1 | 0.65 (0.43–0.99) | 0.53 (0.34–0.83) | 1 | 0.81 (0.55–1.18) | 0.57 (0.38–0.86) | 1 | 0.92 (0.67–1.28) | 1.07 (0.76–1.50) |
| Model 3 | 1 | 0.72 (0.43–1.18) | 0.65 (0.30–1.43) | 1 | 0.95 (0.61–1.48) | 0.90 (0.43–1.85) | 1 | 0.94 (0.64–1.38) | 1.02 (0.55–1.87) |
| n-3 Fatty Acid | |||||||||
| Range of intake | <0.8 | 0.8–1.3 | >1.3 | <0.8 | 0.8–1.3 | >1.3 | <0.8 | 0.8–1.3 | >1.3 |
| Crude | 1 | 0.15 (0.11–0.20) | 0.10 (0.07–0.14) | 1 | 0.27 (0.21–0.36) | 0.20 (0.15–0.27) | 1 | 1.11 (0.87–1.40) | 1.20 (0.94–1.53) |
| Model 1 | 1 | 0.54 (0.37–0.80) | 0.37 (0.24–0.56) | 1 | 0.63 (0.44–0.90) | 0.46 (0.32–0.66) | 1 | 0.74 (0.54–1.01) | 0.80 (0.59–1.10) |
| Model 2 | 1 | 0.76 (0.50–1.14) | 0.53 (0.33–0.83) | 1 | 0.85 (0.58–1.24) | 0.70 (0.47–1.06) | 1 | 0.91 (0.66–1.26) | 1.04 (0.75–1.46) |
| Model 3 | 1 | 0.83 (0.51–1.35) | 0.63 (0.30–1.32) | 1 | 1.06 (0.69–1.64) | 1.17 (0.62–2.23) | 1 | 0.88 (0.61–1.28) | 0.92 (0.54–1.59) |
| n-6/n-3 Ratio | |||||||||
| Range of intake | <6.6 | 6.6–7.5 | >7.5 | <6.6 | 6.6–7.5 | >7.5 | <6.6 | 6.6–7.5 | >7.5 |
| Crude | 1 | 0.13 (0.09–0.18) | 0.16 (0.12–0.21) | 1 | 0.23 (0.17–0.31) | 0.22 (0.17–0.30) | 1 | 0.98 (0.78–1.23) | 1.47 (1.16–1.86) |
| Model 1 | 1 | 0.60 (0.40–0.90) | 0.71 (0.48–1.04) | 1 | 0.51 (0.35–0.73) | 0.49 (0.340–0.70) | 1 | 0.67 (0.49–0.91) | 1.01 (0.74–1.39) |
| Model 2 | 1 | 0.84 (0.54–1.30) | 1.07 (0.71–1.63) | 1 | 0.65 (0.44–0.95) | 0.61 (0.42–0.90) | 1 | 0.79 (0.57–1.08) | 1.24 (0.89–1.73) |
| Model 3 | 1 | 0.88 (0.56–1.39) | 1.20 (0.73–1.97) | 1 | 0.67 (0.44–1.00) | 0.68 (0.44–1.07) | 1 | 0.83 (0.60–1.15) | 1.52 (1.03–2.23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-W.; Kim, D.-Y.; Bak, G.-T.; Hyun, D.-S.; Kim, S.-K. Relation of Dietary n-3 and n-6 Fatty Acid Intakes to Metabolic Syndrome in Middle-Aged People Depending on the Level of HbA1c: A Review of National Health and Nutrition Survey Data from 2014 to 2016. Medicina 2022, 58, 1017. https://doi.org/10.3390/medicina58081017
Park S-W, Kim D-Y, Bak G-T, Hyun D-S, Kim S-K. Relation of Dietary n-3 and n-6 Fatty Acid Intakes to Metabolic Syndrome in Middle-Aged People Depending on the Level of HbA1c: A Review of National Health and Nutrition Survey Data from 2014 to 2016. Medicina. 2022; 58(8):1017. https://doi.org/10.3390/medicina58081017
Chicago/Turabian StylePark, Seo-Woo, Do-Yeong Kim, Gyeong-Tae Bak, Dae-Sung Hyun, and Sung-Kyung Kim. 2022. "Relation of Dietary n-3 and n-6 Fatty Acid Intakes to Metabolic Syndrome in Middle-Aged People Depending on the Level of HbA1c: A Review of National Health and Nutrition Survey Data from 2014 to 2016" Medicina 58, no. 8: 1017. https://doi.org/10.3390/medicina58081017
APA StylePark, S.-W., Kim, D.-Y., Bak, G.-T., Hyun, D.-S., & Kim, S.-K. (2022). Relation of Dietary n-3 and n-6 Fatty Acid Intakes to Metabolic Syndrome in Middle-Aged People Depending on the Level of HbA1c: A Review of National Health and Nutrition Survey Data from 2014 to 2016. Medicina, 58(8), 1017. https://doi.org/10.3390/medicina58081017