
Impact of Insurance Benefits and Education on Point-of-Care Ultrasound Use in a Single Emergency Department: An Interrupted Time Series Analysis

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Site
2.3. Intervention
2.3.1. Expansion of Benefit Coverage of the NHI for EUS
2.3.2. Ultrasonography Workshops
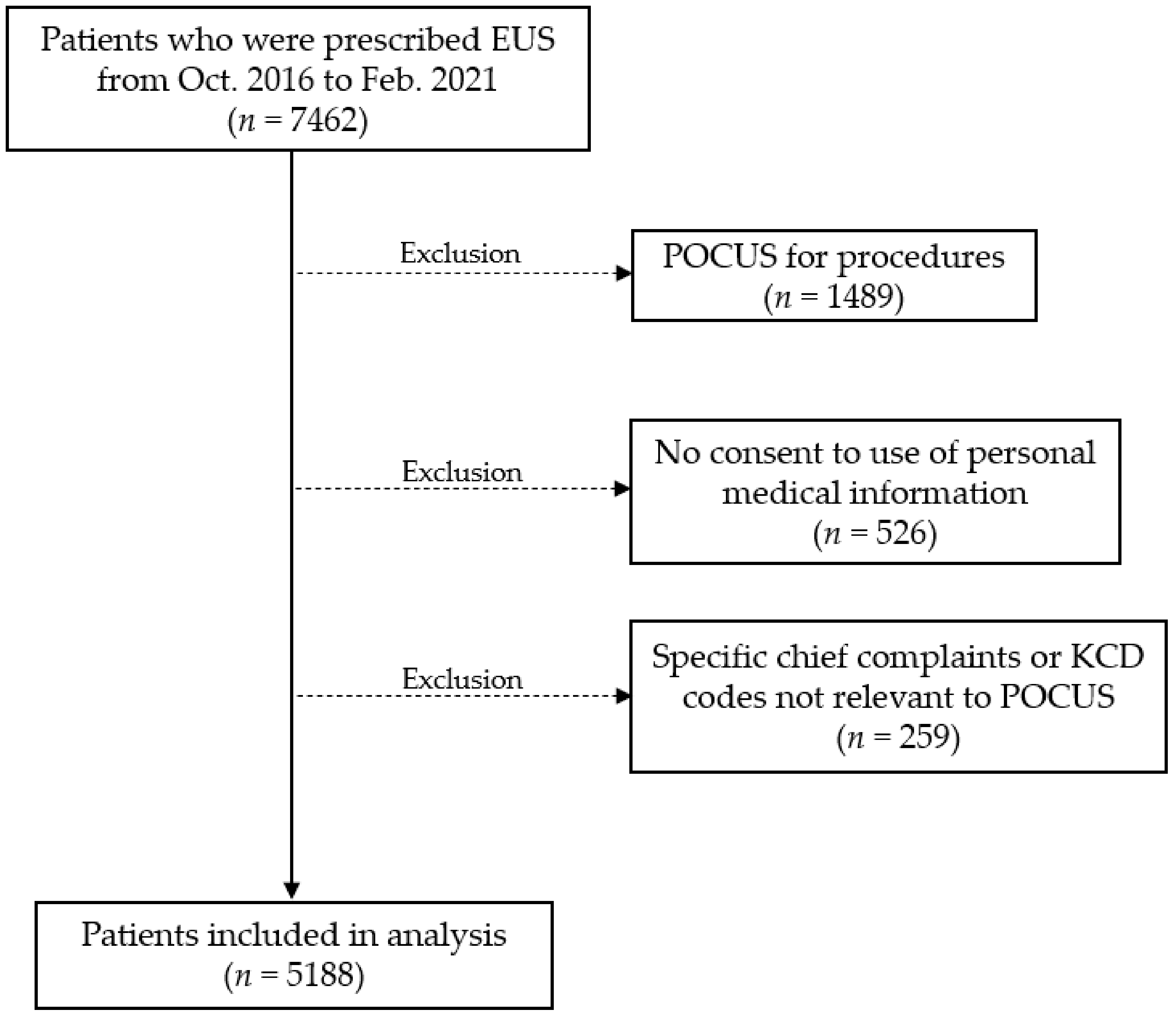
2.4. Data Collection
2.5. Outcomes
2.6. Statistical Analysis
3. Results
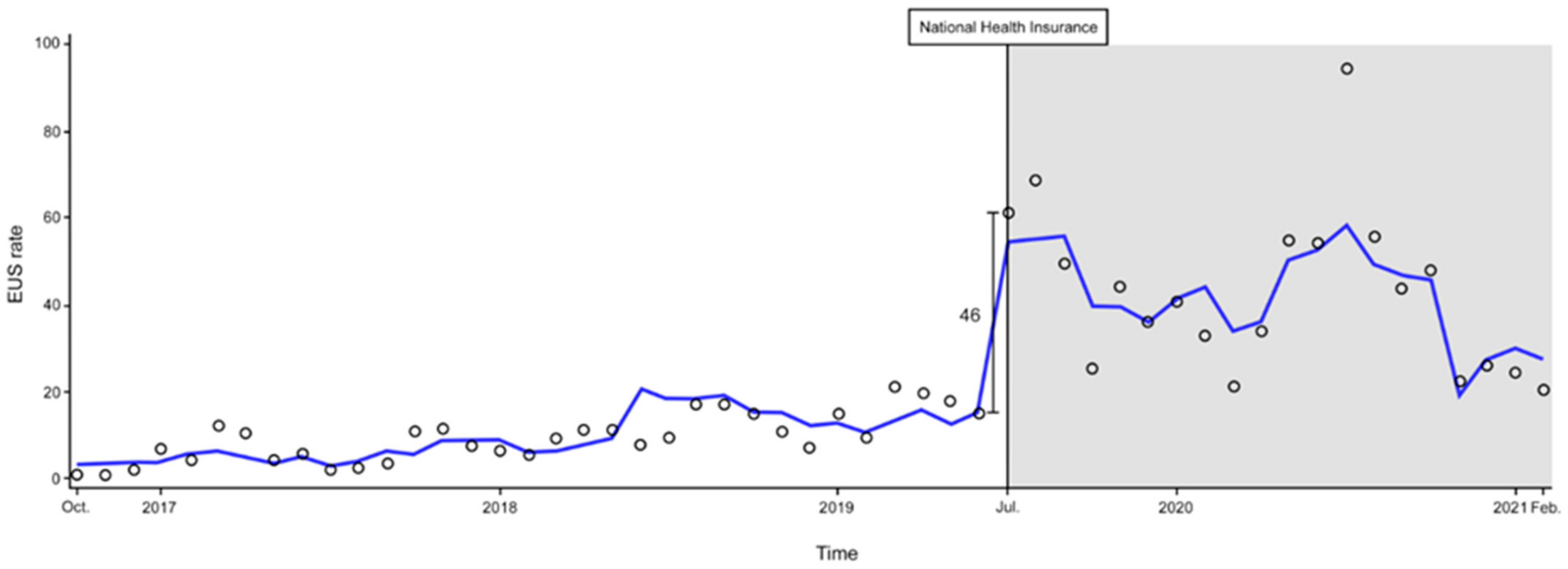
3.1. Changes in the EUS Rate after NHI Expansion
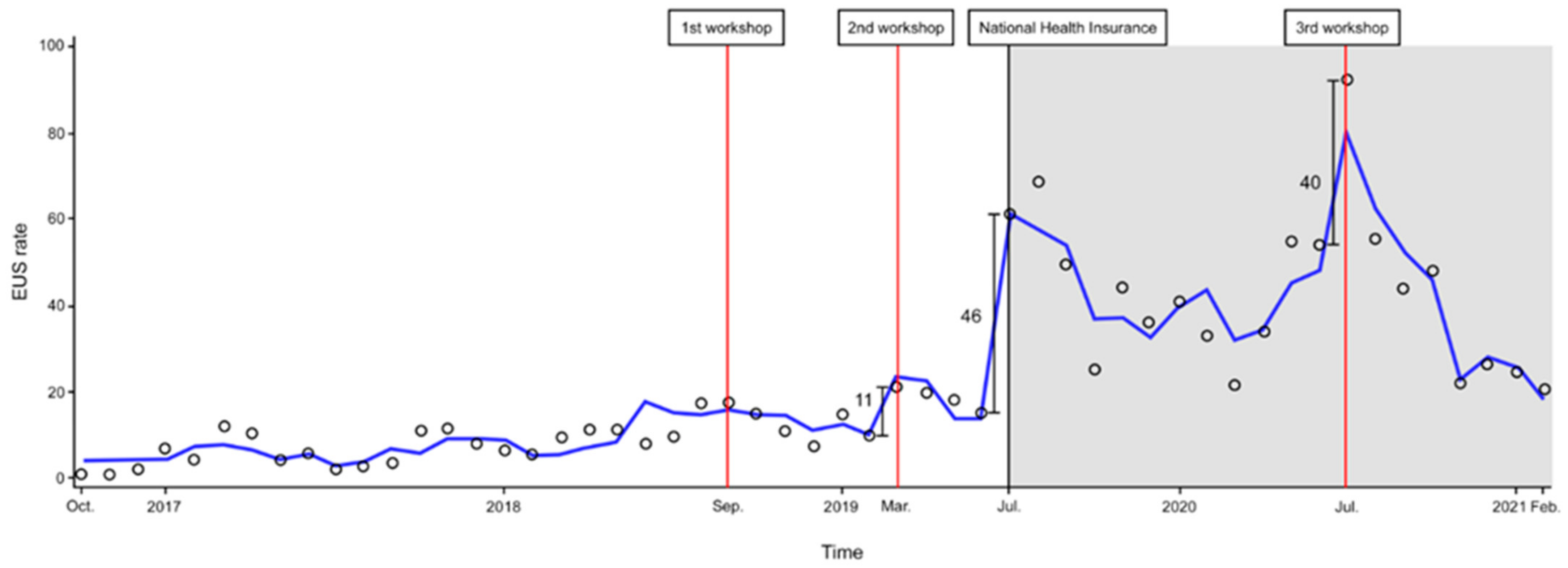
3.2. Changes in the EUS Rate after Three Ultrasound Workshops and NHI Expansion
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bashir, K.; Azad, A.M.; Hereiz, A.; Bashir, M.T.; Masood, M.; Elmoheen, A. Current Use, Perceived Barriers, and Learning Preference of Point of Care Ultrasound (POCUS) in the Emergency Medicine in Qatar—A Mixed Design. Open Access Emerg. Med. 2021, 13, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Jehle, D.; Davis, E.; Evans, T.; Harchelroad, F.; Martin, M.; Zaiser, K.; Lucid, J. Emergency department sonography by emergency physicians. Am. J. Emerg. Med. 1989, 7, 605–611. [Google Scholar] [CrossRef]
- Tekin, E.; Aydin, M.E.; Turgut, M.C.; Karagoz, S.; Ates, I.; Ahiskalioglu, E.O. Can ultrasound-guided infraclavicular block be an alternative option for forearm reduction in the emergency department? A prospective randomized study. Clin. Exp. Emerg. Med. 2021, 8, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Schlager, D.; Lazzareschi, G.; Whitten, D.; Sanders, A.B. A prospective study of ultrasonography in the ED by emergency physicians. Am. J. Emerg. Med. 1994, 12, 185–189. [Google Scholar] [CrossRef]
- American College of Emergency Physicians. Appropriate Use Criteria for Handheld Pocket Ultrasound Devices: ACEP Policy Statement. 2018. Available online: https://www.acep.org/patient-care/policy-statements/appropriate-use-criteria-for-handheldpocket-ultrasound-devices (accessed on 28 November 2021).
- Kjesbu, I.E.; Laursen, C.B.; Graven, T.; Holden, H.M.; Rømo, B.; Andersen, G.N.; Mjølstad, O.C.; Lassen, A.; Dalen, H. Feasibility and Diagnostic Accuracy of Point-of-Care Abdominal Sonography by Pocket-Sized Imaging Devices, Performed by Medical Residents. J. Ultrasound Med. 2017, 36, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- American College of Emergency Physicians. Ultrasound Guidelines: Emergency, Point-of-Care and Clinical Ultrasound Guidelines in Medicine. Ann. Emerg. Med. 2017, 69, e27–e54. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, C.F.; Goudie, A.; Chiorean, L.; Cui, X.W.; Gilja, O.H.; Dong, Y.; Abramowicz, J.S.; Vinayak, S.; Westerway, S.C.; Nolsøe, C.P.; et al. Point of Care Ultrasound: A WFUMB Position Paper. Ultrasound Med. Biol. 2017, 43, 49–58. [Google Scholar] [CrossRef]
- Moore, C.L.; Copel, J.A. Point-of-Care Ultrasonography. N. Engl. J. Med. 2011, 364, 749–757. [Google Scholar] [CrossRef] [Green Version]
- Ahn, C.; Kim, C.; Kang, B.S.; Choi, H.J.; Cho, J.H. Variation of availability and frequency of emergency physician-performed ultrasonography between adult and pediatric patients in the academic emergency department in Korea. Clin. Exp. Emerg. Med. 2015, 2, 16–23. [Google Scholar] [CrossRef]
- Lee, J.J.; Kang, B.S.; Cho, Y.S.; Lee, Y.J.; Lee, J.H.; Park, Y.S.; Chung, H.S.; Ha, Y.R.; Kim, Y.S.; Ahn, J.H. The Current Status and Activities of Emergency Physician-Performed Ultrasonography in Seoul and Gyeonggi do. J. Korean Soc. Emerg. Med. 2010, 21, 166–174. Available online: https://ir.ymlib.yonsei.ac.kr/handle/22282913/101806 (accessed on 28 November 2021).
- Health Insurance Review & Assessment Service. Medical Information: Easy-to-Understand Salary Benefits-Ultrasonography. 2019. Available online: https://www.hira.or.kr/rd/insuadtcrtr/bbsView.do?pgmid=HIRAA030069000400&brd-ScnBltNo=4&brdBltNo=51292 (accessed on 28 November 2021).
- Choi, J.-I. Prospects on the increase of radiological examinations in Korea. J. Korean Med. Assoc. 2020, 63, 136–139. [Google Scholar] [CrossRef]
- Mengel-Jorgensen, T.; Jensen, M.B. Variation in the use of point-of-care ultrasound in general practice in various European countries. Results of a survey among experts. Eur. J. Gen. Pract. 2016, 22, 274–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micks, T.; Sue, K.; Rogers, P. Barriers to point-of-care ultrasound use in rural emergency departments. Can. Assoc. Emerg. Physicians 2016, 18, 475–479. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.; Kang, S.Y.; Jo, I.J.; Kim, T.; Lee, G.; Park, J.E.; Hwang, S.Y.; Cha, W.C.; Shin, T.G.; Yoon, H. The Use of Point-of-care Ultrasound in Emergency Medical Centers in Korea: A National Cross-sectional Survey. J. Korean Med. Sci. 2021, 36, e141. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Montague, S.; Wallace, P.; Negishi, K.; Liteplo, A.; Ringrose, J.; Dversdal, R.; Buchanan, B.; Desy, J.; Ma, I.W.Y. Barriers to learning and using point-of-care ultrasound: A survey of practicing internists in six North American institutions. Ultrasound J. 2020, 12, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnittke, N.; Damewood, S. Identifying and Overcoming Barriers to Resident Use of Point-of-Care Ultrasound. West J. Emerg. Med. 2019, 20, 918–925. [Google Scholar] [CrossRef]
- Myklestul, H.C.; Skonnord, T.; Brekke, M. Point-of-care ultrasound (POCUS) in Norwegian general practice. Scand. J. Prim. Health Care 2020, 38, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Rosenkrantz, A.B.; Bilal, N.H.; Hughes, D.R.; Duszak, R., Jr. National specialty trends in billable diagnostic ultrasound in the ED: Analysis of Medicare claims data. Am. J. Emerg. Med. 2014, 32, 1470–1475. [Google Scholar] [CrossRef]
- Kwon, S. Thirty years of national health insurance in South Korea: Lessons for achieving universal health care coverage. Health Policy Plan. 2009, 24, 63–71. [Google Scholar] [CrossRef]
- Kwon, S. Advancing Universal Health Coverage: What Developing Countries Can Learn from the Korean Experience? Universal Health Coverage Study Series; World Bank: Washington, DC, USA, 2018. [Google Scholar] [CrossRef]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef]
- Hall, J.W.W.; Holman, H.; Bornemann, P.; Barreto, T.; Henderson, D.; Bennett, K.; Chamberlain, J.; Maurer, D.M. Point of Care Ultrasound in Family medicine residency programs; A CERA study. Fam. Med. 2015, 47, 706–711. [Google Scholar] [PubMed]
- Amini, R.; Wyman, M.T.; Hernandez, N.C.; Guisto, J.A.; Adhikari, S. Use of Emergency Ultrasound in Arizona Community Emergency Departments. J. Ultrasound Med. 2017, 36, 913–921. [Google Scholar] [CrossRef] [PubMed]
- Soni, N.J.; Reyes, L.F.; Keyt, H.; Arango, A.; Gelfond, J.A.; Peters, J.I.; Levine, S.M.; Adams, S.G.; Restrepo, M.I. Use of ultrasound guidance for central venous catheterization: A national survey of intensivists and hospitalists. J. Crit. Care 2016, 36, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Bang, S.; Bahl, A. Impact of Early Educational Intervention on Coding for First-year Emergency Medicine Residents. AEM Educ. Train. 2018, 2, 213–220. [Google Scholar] [CrossRef]
- Adhikari, S.; Fiorello, A. Emergency ultrasound fellowship training: A novel team-based approach. J. Ultrasound Med. 2014, 33, 1821–1826. [Google Scholar] [CrossRef]
- Shin, D.A. Health insurance policies for magnetic resonance imaging tests in Korea. J. Korean Med. Assoc. 2021, 64, 172–176. [Google Scholar] [CrossRef]
- Choi, W.J.; Ha, Y.-R.; Oh, J.H.; Cho, Y.S.; Lee, W.W.; Sohn, Y.D.; Cho, G.C.; Koh, C.-Y.; Do, H.H.; Jeong, W.J.; et al. Clinical Guidance for Point-of-Care Ultrasound in the Emergency and Critical Care Areas after Implementing Insurance Coverage in Korea. J. Korean Med. Sci. 2020, 35, e54. [Google Scholar] [CrossRef]
- Central Government for National Disease Control and Healthcare System Epidemiological Survey and Analysis Team. 1-year report on the COVID-19 situation in the Republic of Korea (As of 19 January 2021). Wkly. Health Dis. 2021, 14, 472–481. Available online: https://www.kdca.go.kr/board/board.es?mid=a20602010000&bid=0034&list_no=712538&act=view# (accessed on 28 November 2021).
- Boserup, B.; McKenney, M.; Elkbuli, A. The impact of the COVID-19 pandemic on emergency department visits and patient safety in the United States. Am. J. Emerg. Med. 2020, 38, 1732–1736. [Google Scholar] [CrossRef]
- Jeffery, M.M.; D’Onofrio, G.; Paek, H.; Platts-Mills, T.F.; Soares, W.E.; Hoppe, J.A.; Genes, N.; Nath, B.; Melnick, E.R. Trends in Emergency Department Visits and Hospital Admissions in Health Care Systems in 5 States in the First Months of the COVID-19 Pandemic in the US. JAMA Intern. Med. 2020, 180, 1328–1333. [Google Scholar] [CrossRef]
- Mantica, G.; Riccardi, N.; Terrone, C.; Gratarola, A. Non-COVID-19 visits to emergency departments during the pandemic: The impact of fear. Public Health 2020, 183, 40–41. [Google Scholar] [CrossRef]
- Agricola, E.; Beneduce, A.; Esposito, A.; Ingallina, G.; Palumbo, D.; Palmisano, A.; Ancona, F.; Baldetti, L.; Pagnesi, M.; Melisurgo, G.; et al. Heart and Lung Multimodality Imaging in COVID-19. JACC Cardiovasc. Imaging 2020, 13, 1792–1808. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Jelic, T.; Woo, M.Y.; Heslop, C.; Olszynski, P. Just the Facts: Recommendations on point-of-care ultrasound use and machine infection control during the coronavirus disease 2019 pandemic. Can. J. Emerg. Med. 2020, 22, 445–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piscaglia, F.; Stefanini, F.; Cantisani, V.; Sidhu, P.S.; Barr, R.; Berzigotti, A.; Chammas, M.C.; Correas, J.-M.; Dietrich, C.F.; Feinstein, S.; et al. Benefits, Open questions and Challenges of the use of Ultrasound in the COVID-19 pandemic era. The views of a panel of worldwide international experts. Ultraschall Med. 2020, 41, 228–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lokuge, A.; Alexander, J.; Land, B.; McAllister, A. Lung ultrasound in a respiratory pandemic. Emerg. Med. Australas. 2020, 32, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Schmid, B.; Feuerstein, D.; Lang, C.N.; Fink, K.; Steger, R.; Rieder, M.; Duerschmied, D.; Busch, H.-J.; Damjanovic, D. Lung ultrasound in the emergency department—A valuable tool in the management of patients presenting with respiratory symptoms during the SARS-CoV-2 pandemic. BMC Emerg. Med. 2020, 20, 96. [Google Scholar] [CrossRef]
- Tombini, V.; Di Capua, M.; Capsoni, N.; Lazzati, A.; Bergamaschi, M.; Gheda, S.; Ghezzi, L.; Cassano, G.; Albertini, V.; Porta, L.; et al. Risk Stratification in COVID-19 Pneumonia—Determining the Role of Lung Ultrasound. Ultraschall Med. 2021. [Google Scholar] [CrossRef]
- Garlisi, C.; Licandro, D.; Siani, A.; Rodolfi, S.; Pansini, S.; Navarro, L.I.G.; Carriero, A.; Avanzi, G.C.; Castello, L.M. Impact of the COVID-19 pandemic on the activity of the Radiological Emergency Department: The experience of the Maggiore della Carita Hospital in Novara. Emerg. Radiol. 2021, 28, 705–711. [Google Scholar] [CrossRef]
- Messina, M.D.; Stein, M.W.; Armstrong, I.J.; Wolf, E.L. Impact of the COVID-19 pandemic on radiology department emergency ultrasound utilization. Emerg. Radiol. 2021, 28, 869–875. [Google Scholar] [CrossRef]
- Chen, W.L.; Hsu, C.P.; Wu, P.H.; Chen, J.H.; Huang, C.C.; Chung, J.Y. Comprehensive residency-based point-of-care ultrasound training program increases ultrasound utilization in the emergency department. Medicine 2021, 100, e24644. [Google Scholar] [CrossRef]
- Schott, C.K.; LoPresti, C.M.; Boyd, J.S.; Core, M.; Haro, E.K.; Mader, M.J.; Pascual, S.; Finley, E.P.; Lucas, B.P.; Colon-Molero, A.; et al. Retention of Point-of-Care Ultrasound Skills Among Practicing Physicians: Findings of the VA National POCUS Training Program. Am. J. Med. 2021, 134, 391–399.e8. [Google Scholar] [CrossRef]
- Kim, J.S.; Cho, Y.S.; Kim, Y.S.; Ha, Y.R.; Kang, B.S.; Chung, H.S.; Park, Y.S.; An, J.H.; Do, H.H.; Hong, H.P. Development of an Emergency Abdominal Ultrasound Course in Korea: 1-Year Experience. J. Korean Soc. Emerg. Med. 2010, 21, 382–387. Available online: http://www.jksem.org/journal/view.php?number=605 (accessed on 28 November 2021).
- Kim, J.H.; Kim, J.W.; Kim, S.Y.; Hong, D.Y.; Park, S.O.; Baek, K.J.; Lee, K.R. Validation of the Korean Triage and Acuity Scale Compare to Triage by Emergency Severity Index for Emergency Adult Patient: Preliminary Study in a Tertiary Hospital Emergency Medical Center. J. Korean Soc. Emerg. Med. 2016, 27, 436–441. [Google Scholar] [CrossRef]
- Reynolds, T.A.; Amato, S.; Kulola, I.; Chen, C.-J.J.; Mfinanga, J.; Sawe, H.R. Impact of point-of-care ultrasound on clinical decision-making at an urban emergency department in Tanzania. PLoS ONE 2018, 13, e0194774. [Google Scholar] [CrossRef] [Green Version]
- Shabanzadeh, D.M.; Sorensen, L.T.; Jorgensen, T. A Prediction Rule for Risk Stratification of Incidentally Discovered Gallstones: Results from a Large Cohort Study. Gastroenterology 2016, 150, 156–167.e1. [Google Scholar] [CrossRef]
- Kim, B.W.; Yoon, Y.I. Developing the data analysis-based emergency room congestion predictive model for the resolution of overcrowded emergency room. J. Korean Data Inf. Sci. Soc. 2018, 29, 1201–1214. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | N (%) | Variables | N (%) |
|---|---|---|---|
| Age, years (mean, SD) | 57 (19) | Arrest | 53 (1) |
| Male (%) | 2856 (55) | Others | 75 (1) |
| KTAS (%) | Type of EUS | ||
| 1 (Resuscitation) | 126 (2) | EUS 1 | 4168 (80) |
| 2 (Emergent) | 850 (17) | EUS 2 | 736 (14) |
| 3 (Urgent) | 2391 (46) | EUS 3 | 284 (6) |
| 4 (Less Urgent) | 1743 (34) | Exam Site of POCUS (%) (n = 7171) | |
| 5 (Non-Urgent) | 78 (1) | Echo | 2573 (36) |
| Initial main chief complaint (%) (n = 5188) | eFAST | 1229 (17) | |
| Abdominal pain | 1422 (27) | Biliary | 1191 (17) |
| Dyspnea | 925 (18) | Lung | 1037 (14) |
| Chest pain | 698 (14) | Kidney | 699 (10) |
| Trauma | 572 (11) | Aorta | 176 (2) |
| Flank pain | 452 (8) | GI tract | 97 (1) |
| General weakness/mental change | 370 (7) | DVT | 80 (1) |
| Fever | 292 (6) | Liver | 49 (1) |
| Shock | 172 (3) | Pancreas | 40 (1) |
| Musculoskeletal/Vascular | 126/31 (4) |
| Variables | Regression Coefficient | Standard Error | p-Value |
|---|---|---|---|
| Intercept | 1.7403 | 0.1949 | <0.001 |
| Time (month) | 0.0613 | 0.0105 | <0.001 |
| NHI expansion | |||
| Changes in level | 2.8319 | 0.3412 | <0.001 |
| Changes in slope | −0.127 | 0.0243 | <0.001 |
| POCUS physician (presence) | 1.3087 | 0.2621 | <0.001 |
| AR4 | 0.4316 | 0.1345 | 0.002 |
| Variables | Regression Coefficient | Standard Error | p-Value |
|---|---|---|---|
| Intercept | 2.005 | 0.7975 | 0.016 |
| Time (month) | 0.0435 | 0.0167 | 0.013 |
| First workshop | |||
| Changes in level | 0.0649 | 0.7307 | 0.930 |
| Changes in slope | 0.0428 | 0.1878 | 0.821 |
| Second workshop | |||
| Changes in level | 1.8004 | 0.8539 | 0.041 |
| Changes in slope | −0.5488 | 0.355 | 0.130 |
| NHI expansion | |||
| Changes in level | 3.0601 | 0.6759 | <0.001 |
| Changes in slope | 0.3895 | 0.2653 | 0.150 |
| Third workshop | |||
| Changes in level | 1.9066 | 0.6695 | 0.007 |
| Changes in slope | −0.3484 | 0.1135 | 0.004 |
| POCUS physician (presence) | 1.1747 | 0.2657 | <0.001 |
| AR4 | 0.5242 | 0.1353 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, S.-Y.; Park, S.; Jo, I.-J.; Jeon, K.; Kim, S.; Lee, G.; Park, J.-E.; Kim, T.; Lee, S.-U.; Hwang, S.-Y.; et al. Impact of Insurance Benefits and Education on Point-of-Care Ultrasound Use in a Single Emergency Department: An Interrupted Time Series Analysis. Medicina 2022, 58, 217. https://doi.org/10.3390/medicina58020217
Kang S-Y, Park S, Jo I-J, Jeon K, Kim S, Lee G, Park J-E, Kim T, Lee S-U, Hwang S-Y, et al. Impact of Insurance Benefits and Education on Point-of-Care Ultrasound Use in a Single Emergency Department: An Interrupted Time Series Analysis. Medicina. 2022; 58(2):217. https://doi.org/10.3390/medicina58020217
Chicago/Turabian StyleKang, Soo-Yeon, Sookyung Park, Ik-Joon Jo, Kyeongman Jeon, Seonwoo Kim, Guntak Lee, Jong-Eun Park, Taerim Kim, Se-Uk Lee, Sung-Yeon Hwang, and et al. 2022. "Impact of Insurance Benefits and Education on Point-of-Care Ultrasound Use in a Single Emergency Department: An Interrupted Time Series Analysis" Medicina 58, no. 2: 217. https://doi.org/10.3390/medicina58020217
APA StyleKang, S.-Y., Park, S., Jo, I.-J., Jeon, K., Kim, S., Lee, G., Park, J.-E., Kim, T., Lee, S.-U., Hwang, S.-Y., Cha, W.-C., Shin, T.-G., & Yoon, H. (2022). Impact of Insurance Benefits and Education on Point-of-Care Ultrasound Use in a Single Emergency Department: An Interrupted Time Series Analysis. Medicina, 58(2), 217. https://doi.org/10.3390/medicina58020217