
Biomechanics of Double Poling in Paralympic Cross-Country Skiing—A Cross-Sectional Study Comparing the Standing and Sitting Positions in Healthy Male Subjects

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
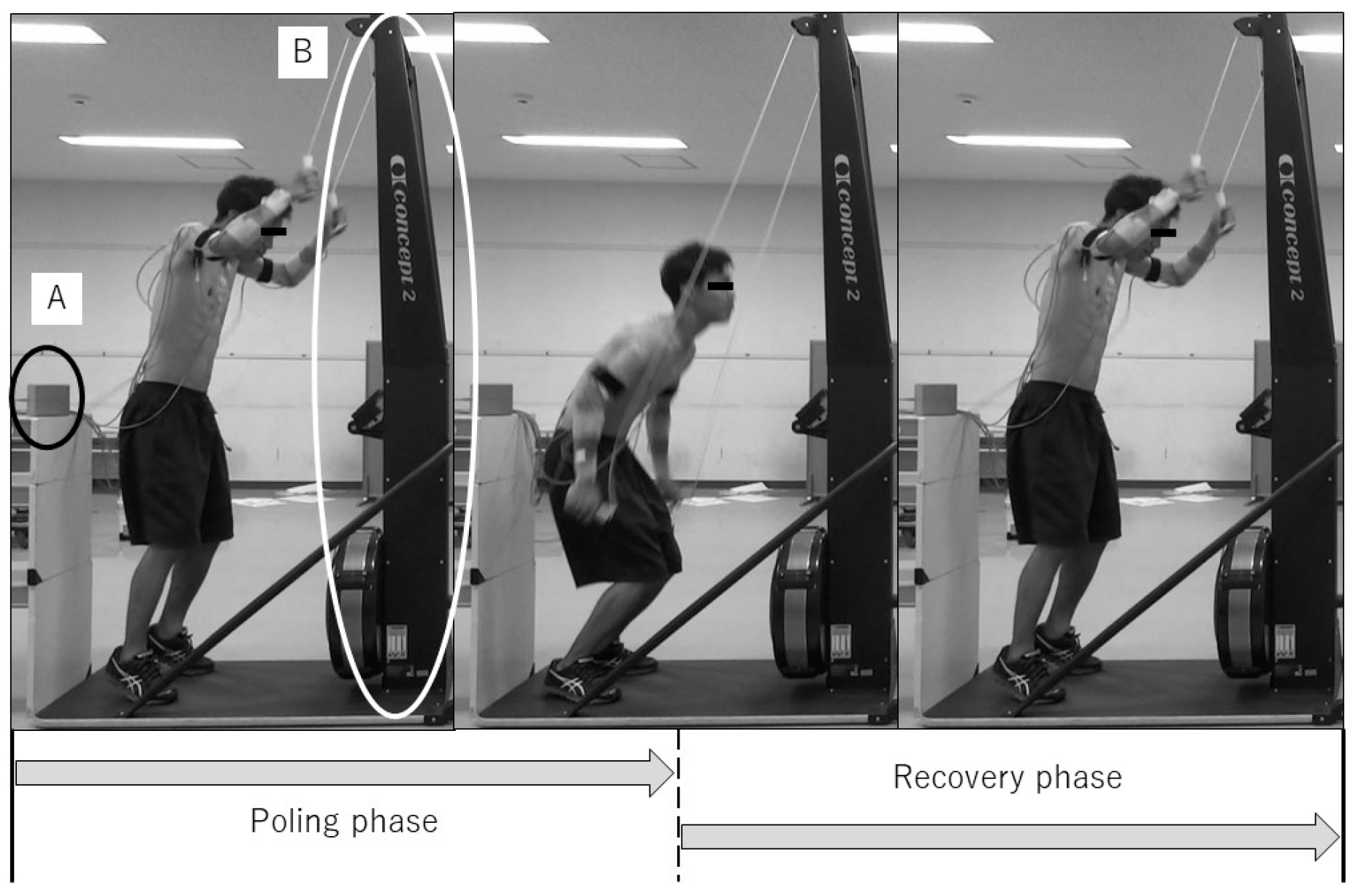
2.2. Design
2.3. Measurement
2.4. Statistical Analysis
3. Results
3.1. Variables of Double-Poling Performance
3.2. Kinematics of Double Poling
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Official Website of World Para Nordic Skiing; History of Para Nordic Skiing. Available online: https://www.paralympic.org/nordic-skiing/about (accessed on 23 January 2022).
- Stöggl, T.; Ohtonen, O.; Takeda, M.; Miyamoto, N.; Snyder, C.; Lemmettylä, T.; Linnamo, V.; Lindinger, S.J. Comparison of exclusive double poling to classic techniques of cross-country skiing. Med. Sci. Sports Exerc. 2019, 51, 760–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindinger, S.J.; Holmberg, H.C.; Müller, E.; Rapp, W. Changes in upper body muscle activity with increasing double poling velocities in elite cross-country skiing. Eur. J. Appl. Physiol. 2009, 106, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, M.; Janssen, T.W.; Bortolan, L.; Pellegrini, B.; Fischer, G.; Schena, F. Kinematics of cross-country sit skiing during a Paralympic race. J. Electromyogr. Kinesiol. 2013, 23, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Rosso, V.; Gastaldi, L.; Rapp, W.; Lindinger, S.J.; Vanlandewijck, Y.; Linnamo, V. Biomechanics of simulated versus natural cross-country sit skiing. J. Electromyogr. Kinesiol. 2017, 32, 15–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegge, A.M.; Myhre, K.; Welde, B.; Holmberg, H.C.; Sandbakk, Ø. Are gender differences in upper-body power generated by elite cross-country skiers augmented by increasing the intensity of exercise? PLoS ONE 2015, 10, e0127509. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.; Tinmark, F.; Halvorsen, K.; Arndt, A. Kinematic, kinetic and electromyographic adaptation` to speed and resistance in double poling cross country skiing. Eur. J. Appl Physiol. 2013, 113, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, H.C.; Lindinger, S.; Stöggl, T.; Eitzlmair, E.; Müller, E. Biomechanical analysis of double poling in elite cross-country skiers. Med. Sci. Sports Exerc. 2005, 37, 807–818. [Google Scholar] [CrossRef] [Green Version]
- Stöggl, T.L.; Holmberg, H.C. Double-Poling Biomechanics of Elite Cross-country Skiers: Flat versus Uphill Terrain. Med. Sci. Sports Exerc. 2016, 48, 1580–1589. [Google Scholar] [CrossRef] [Green Version]
- Holmberg, H.C.; Lindinger, S.; Stöggl, T.; Björklund, G.; Müller, E. Contribution of the legs to double-poling performance in elite cross-country skiers. Med. Sci. Sports Exerc. 2006, 38, 1853–1860. [Google Scholar] [CrossRef]
- Tervo, J.L.; Watts, P.B.; Jensen, R.L. Electromyographical analysis of double pole ergometry: Standing vs. sitting. In Proceedings of the 28th International Conference on Biomechanics in Sports, Marquette, MI, USA, 19–23 July 2010; pp. 1–4. [Google Scholar]
- Bahr, R.; Andersen, S.O.; Løken, S.; Fossan, B.; Hansen, T.; Holme, I. Low back pain among endurance athletes with and without specific back loading—A cross-sectional survey of cross-country skiers, rowers, orienteerers, and nonathletic controls. Spine 2004, 29, 449–454. [Google Scholar] [CrossRef]
- Derman, W.E.; Runciman, P.; Jordaan, E.R.; Schwellnus, M. High incidence of injuries at the Pyeongchang 2018 Paralympic Winter Games: A prospective cohort study of 6804 athlete days. Br. J. Sports Med. 2019, 54, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ohlsson, M.L.; Danvind, J.; Holmberg, L.J. Shoulder and lower back joint reaction forces in seated double poling. J. Appl. Biomech. 2018, 34, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, J.; Sandbakk, Ø.; McGhile, D.; Ettema, G. The effect of exercise intensity on joint power and dynamics in ergometer double-poling performed by cross-country skiers. Hum. Mov. Sci. 2018, 57, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Zoppirolli, C.; Pellegrini, B.; Bortolan, L.; Schena, F. Energetics and biomechanics of double poling in regional and high-level cross-country skiers. Eur. J. Appl. Physiol. 2015, 115, 969–979. [Google Scholar] [CrossRef]
- Gastaldi, L.; Pastorelli, S.; Frassinelli, S. A biomechanical approach to paralympic cross-country sit-ski racing. Clin. J. Sport Med. 2012, 22, 58–64. [Google Scholar] [CrossRef]
- Codman, E.A. Normal Motions of the Shoulder Joint. In The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions in or about the Subacromial Bursa; Thomas Todd Co.: Boston, MA, USA, 1934; pp. 32–64. [Google Scholar]
- Yoshizaki, K.; Hamada, J.; Tamai, K.; Sahara, R.; Fujiwara, T.; Fujimoto, T. Analysis of the scapulohumeral rhythm and electromyography of the shoulder muscles during elevation and lowering: Comparison of dominant and nondominant shoulders. J. Shoulder Elb. Surg. 2009, 18, 756–763. [Google Scholar] [CrossRef]
- Konda, S.; Yanai, T.; Sakurai, S. Configuration of the shoulder complex during the arm-cocking phase in baseball pitching. Am. J. Sports Med. 2015, 43, 2445–2451. [Google Scholar] [CrossRef]
- Neer, C.S. Impingement lesions. Clin. Orthop. Relat. Res. 1983, 173, 70–77. [Google Scholar] [CrossRef]
- Hawkins, R.J.; Brock, R.M.; Abrams, J.S.; Hobeika, P. Acromioplasty for impingement with an intact rotator cuff. J. Bone Jt. Surg. Br. 1988, 70, 795–797. [Google Scholar] [CrossRef]
- Kibler, W.B. The Role of the Scapula in Athletic Shoulder Function. Am. J. Sports Med. 1998, 26, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Kobesova, A.; Dzvonik, J.; Kolar, P.; Sardina, A.; Andel, R. Effects of shoulder girdle dynamic stabilization exercise on hand muscle strength. Isokinet. Exerc. Sci. 2015, 23, 21–32. [Google Scholar] [CrossRef] [Green Version]
- Horyna, R.; Bacakova, R.; Charástková, M.; Sedlák, R.; Cmejla, R.; Kračmar, B. Activity of upper body muscles in double poling and skierg workout. Balt. J. Sport Health Sci. 2016, 2, 31–37. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Standing | Sitting | p-Value | |
|---|---|---|---|
| Stroke rate (strokes/min) | 63.99 ± 8.70 | 58.47 ± 12.12 | 0.275 a |
| Stroke length of poling phase (cm) | 109.37 ± 12.46 | 99.59 ± 9.89 | 0.036 a |
| Stroke speed of poling phase (cm/s) | 213.93 ± 17.50 | 189.00 ± 15.78 | 0.004 a |
| Stroke length of recovery phase (cm) | 108.67 ± 13.11 | 99.17 ± 10.01 | 0.045 a |
| Stroke speed of recovery phase (cm/s) | 260.54 ± 60.54 | 231.69 ± 33.29 | 0.026 b |
| Power output (W) | 226.93 ± 47.71 | 145.20 ± 26.57 | <0.001 a |
| Standing | Sitting | p-Value | ||
|---|---|---|---|---|
| Scapulothoracic Protraction (degree) | Upward | 22.98 ± 10.18 | 27.48 ± 7.40 | 0.138 a |
| Downward | 38.96 ± 7.46 | 40.23 ± 8.46 | 0.458 a | |
| ROM | −15.98 ± 7.62 | −12.76 ± 9.50 | 0.268 a | |
| Scapulothoracic Upward Rotation (degree) | Upward | 34.78 ± 12.11 | 40.99 ± 5.21 | 0.083 a |
| Downward | 6.45 ± 6.75 | 8.78 ± 3.95 | 0.062 b | |
| ROM | 28.32 ± 12.20 | 32.20 ± 5.25 | 0.212 a | |
| Scapulothoracic Posterior Tilt (degree) | Upward | 11.68 ± 15.11 | 9.19 ± 17.53 | 0.366 a |
| Downward | −7.96 ± 10.72 | −11.03 ± 6.05 | 0.150 a | |
| ROM | 19.64 ± 12.77 | 20.23 ± 18.09 | 0.929 b | |
| Humerothoracic Plane of Elevation (degree) | Upward | 53.29 ± 12.45 | 52.87 ± 13.30 | 0.908 a |
| Downward | 47.00 ± 13.93 | 39.56 ± 16.67 | 0.110 b | |
| ROM | 6.29 ± 21.21 | 13.30 ± 21.99 | 0.199 a | |
| Humerothoracic Elevation (degree) | Upward | 97.72 ± 11.48 | 116.14 ± 11.18 | 0.006 a |
| Downward | 30.98 ± 10.20 | 27.77 ± 5.26 | 0.353 a | |
| ROM | 66.74 ± 18.33 | 88.37 ± 10.32 | 0.006 a | |
| Humerothoracic Internal Rotation (degree) | Upward | −58.45 ± 13.47 | −51.80 ± 9.77 | 0.037 a |
| Downward | −26.80 ± 22.21 | −16.16 ± 18.83 | 0.030 a | |
| ROM | −31.65 ± 18.00 | −35.64 ± 17.18 | 0.282 a | |
| Glenohumeral Plane of Elevation (degree) | Upward | 28.40 ± 10.39 | 19.85 ± 9.56 | 0.004 a |
| Downward | 29.08 ± 10.36 | 27.41 ± 19.78 | 0.859 b | |
| ROM | 0.68 ± 6.50 | −7.56 ± 20.56 | 0.184 a | |
| Glenohumeral Elevation (degree) | Upward | 62.17 ± 11.46 | 75.27 ± 12.38 | 0.001 a |
| Downward | 26.83 ± 11.06 | 21.99 ± 8.16 | 0.200 a | |
| ROM | −35.34 ± 7.89 | 53.27 ± 12.55 | 0.006 b | |
| Glenohumeral Internal Rotation (degree) | Upward | −66.81 ± 17.53 | −60.59 ± 18.44 | 0.098 a |
| Downward | −46.64 ± 25.99 | −46.19 ± 22.21 | 0.961 a | |
| ROM | −20.16 ± 20.49 | −14.40 ± 29.34 | 0.578 a |
| Standing | Sitting | p-Value | ||
|---|---|---|---|---|
| Thoracopelvic flexion (degree) | Upward | 24.68 ± 12.57 | 22.50 ± 11.21 | 0.641 a |
| Downward | 52.90 ± 11.65 | 64.84 ± 10.05 | <0.001 b | |
| ROM | 28.22 ± 13.96 | 42.34 ± 9.69 | 0.018 a | |
| Thoracopelvic left lateral flexion (degree) | Upward | −3.41 ± 5.48 | 1.48 ± 4.50 | 0.001 a |
| Downward | −0.51 ± 4.52 | 1.40 ± 3.88 | 0.009 a | |
| ROM | −2.91 ± 2.74 | 0.07 ± 4.78 | 0.017 a | |
| Thoracopelvic left rotation (degree) | Upward | 4.88 ± 7.03 | 4.08 ± 5.38 | 0.363 a |
| Downward | 1.80 ± 5.60 | 1.84 ± 7.21 | 0.657 b | |
| ROM | 3.08 ± 4.04 | 2.23 ± 3.69 | 0.605 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasadai, J.; Maeda, N.; Morikawa, M.; Komiya, M.; Shimizu, R.; Fukui, K.; Yoshimi, M.; Kono, Y.; Urabe, Y. Biomechanics of Double Poling in Paralympic Cross-Country Skiing—A Cross-Sectional Study Comparing the Standing and Sitting Positions in Healthy Male Subjects. Medicina 2022, 58, 201. https://doi.org/10.3390/medicina58020201
Sasadai J, Maeda N, Morikawa M, Komiya M, Shimizu R, Fukui K, Yoshimi M, Kono Y, Urabe Y. Biomechanics of Double Poling in Paralympic Cross-Country Skiing—A Cross-Sectional Study Comparing the Standing and Sitting Positions in Healthy Male Subjects. Medicina. 2022; 58(2):201. https://doi.org/10.3390/medicina58020201
Chicago/Turabian StyleSasadai, Junpei, Noriaki Maeda, Masanori Morikawa, Makoto Komiya, Reia Shimizu, Kazuki Fukui, Mitsuhiro Yoshimi, Yoshifumi Kono, and Yukio Urabe. 2022. "Biomechanics of Double Poling in Paralympic Cross-Country Skiing—A Cross-Sectional Study Comparing the Standing and Sitting Positions in Healthy Male Subjects" Medicina 58, no. 2: 201. https://doi.org/10.3390/medicina58020201
APA StyleSasadai, J., Maeda, N., Morikawa, M., Komiya, M., Shimizu, R., Fukui, K., Yoshimi, M., Kono, Y., & Urabe, Y. (2022). Biomechanics of Double Poling in Paralympic Cross-Country Skiing—A Cross-Sectional Study Comparing the Standing and Sitting Positions in Healthy Male Subjects. Medicina, 58(2), 201. https://doi.org/10.3390/medicina58020201