
Stress-Induced Cardiomyopathy—Considerations for Diagnosis and Management during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Takotsubo Syndrome in the Setting of Acute COVID-19
2.1. Epidemiology
2.2. Pathways and Potential Mechanisms
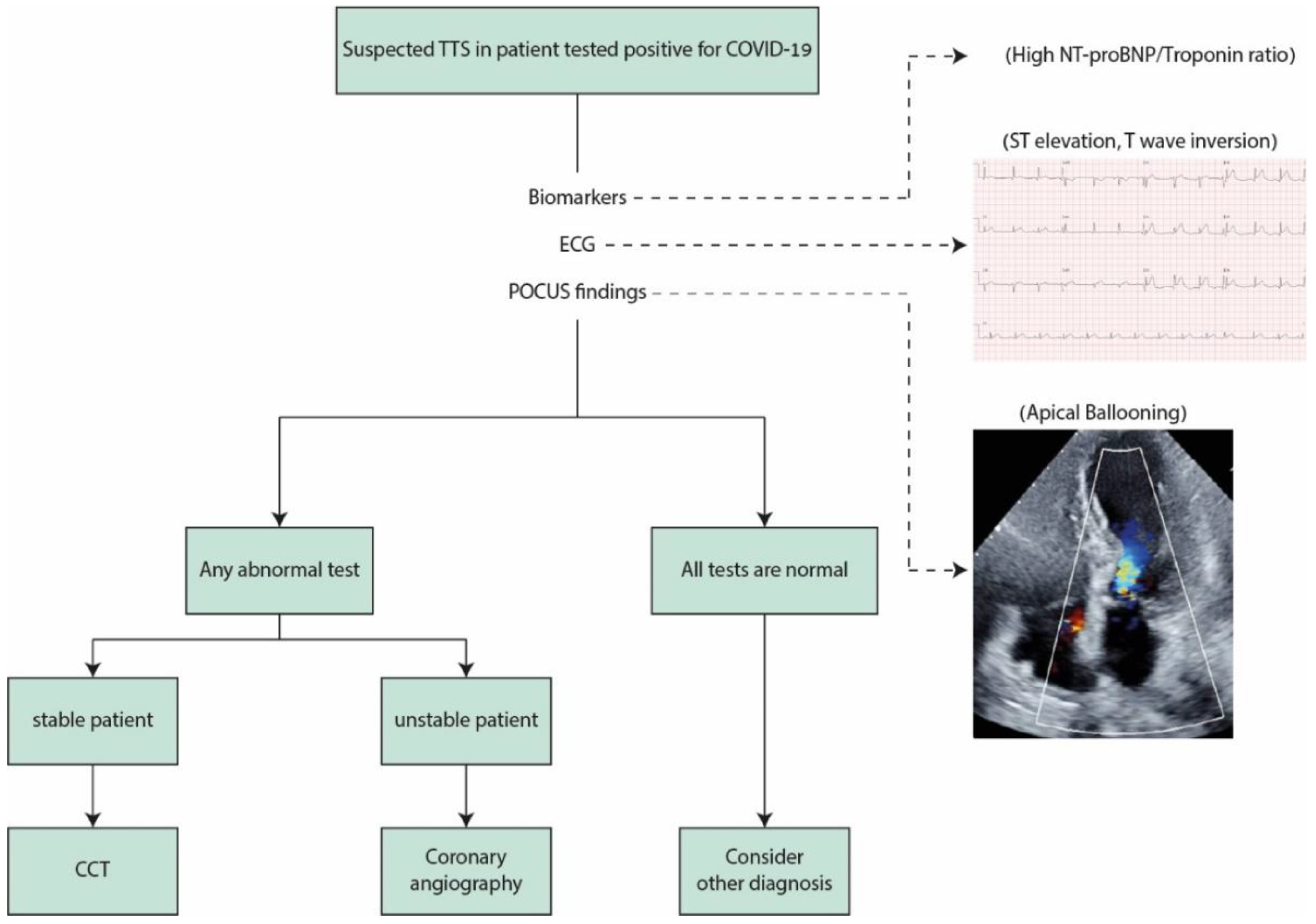
2.3. Diagnostic Considerations
2.3.1. Echocardiography
2.3.2. ECG
2.3.3. Biomarkers
2.3.4. Coronary Angiography and Cardiac Computed Tomography
2.4. Clinical Course and Outcomes
2.5. Treatment
2.6. Stress-Induced Takotsubo during Lockdown and Self Isolation
3. Prevention
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giustino, G.; Pinney, S.P.; Lala, A.; Reddy, V.Y.; Johnston-Cox, H.A.; Mechanick, J.I.; Halperin, J.L.; Fuster, V. Coronavirus and Cardiovascular Disease, Myocardial Injury, and Arrhythmia: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 76, 2011–2023. [Google Scholar] [CrossRef] [PubMed]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, S.; Qin, M.; Cai, Y.; Liu, T.; Shen, B.; Yang, F.; Cao, S.; Liu, X.; Xiang, Y.; Zhao, Q.; et al. Characteristics and clinical significance of myocardial injury in patients with severe coronavirus disease 2019. Eur. Heart J. 2020, 41, 2070–2079. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [Green Version]
- Okura, H. Update of takotsubo syndrome in the era of COVID-19. J. Cardiol. 2021, 77, 361–369. [Google Scholar] [CrossRef]
- Kato, K.; Lyon, A.R.; Ghadri, J.R.; Templin, C. Takotsubo syndrome: Aetiology, presentation and treatment. Heart 2017, 103, 1461–1469. [Google Scholar] [CrossRef]
- Lyon, A.R.; Bossone, E.; Schneider, B.; Sechtem, U.; Citro, R.; Underwood, S.R.; Sheppard, M.N.; Figtree, G.A.; Parodi, G.; Akashi, Y.J.; et al. Current state of knowledge on Takotsubo syndrome: A Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2016, 18, 8–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Templin, C.; Ghadri, J.R.; Diekmann, J.; Napp, L.C.; Bataiosu, D.R.; Jaguszewski, M.; Cammann, V.L.; Sarcon, A.; Geyer, V.; Neumann, C.A.; et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N. Engl. J. Med. 2015, 373, 929–938. [Google Scholar] [PubMed] [Green Version]
- Moady, G.; Vons, S.; Atar, S. A Comparative Retrospective Study of Patients with Takotsubo Syndrome and Acute Coronary Syndrome. Isr. Med. Assoc. J. 2021, 23, 107–110. [Google Scholar] [PubMed]
- Ghadri, J.R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef] [Green Version]
- Hegde, S.; Khan, R.; Zordok, M.; Maysky, M. Characteristics and outcome of patients with COVID-19 complicated by Takotsubo cardiomyopathy: Case series with literature review. Open Heart 2020, 7, e001360. [Google Scholar] [CrossRef]
- Giustino, G.; Croft, L.B.; Oates, C.P.; Rahman, K.; Lerakis, S.; Reddy, V.Y.; Goldman, M. Takotsubo Cardiomyopathy in COVID-19. J. Am. Coll. Cardiol. 2020, 76, 628–629. [Google Scholar] [CrossRef]
- Dweck, M.R.; Bularga, A.; Hahn, R.T.; Bing, R.; Lee, K.K.; Chapman, A.R.; White, A.; Salvo, G.D.; Sade, L.E.; Pearce, K.; et al. Global evaluation of echocardiography in patients with COVID-19. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 949–958. [Google Scholar] [CrossRef]
- Bottiroli, M.; De Caria, D.; Belli, O.; Calini, A.; Andreoni, P.; Siragusa, A.; Moreo, A.; Ammirati, E.; Mondino, M.; Fumagalli, R. Takotsubo syndrome as a complication in a critically ill COVID-19 patient. ESC Heart Fail. ESC Heart Fail. 2020, 7, 4297–4300. [Google Scholar] [CrossRef]
- Faqihi, F.; Alharthy, A.; Alshaya, R.; Papanikolaou, J.; Kutsogiannis, D.J.; Brindley, P.G.; Karakitsos, D. Reverse takotsubo cardiomyopathy in fulminant COVID-19 associated with cytokine release syndrome and resolution following therapeutic plasma exchange: A case-report. BMC Cardiovasc. Disord. 2020, 20, 389. [Google Scholar]
- Nguyen, D.; Nguyen, T.; De Bels, D.; Castro Rodriguez, J. A case of Takotsubo cardiomyopathy with COVID 19. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 1052. [Google Scholar]
- Panchal, A.; Kyvernitakis, A.; Biederman, R. An Interesting Case of COVID-19 Induced Reversed Takotsubo Cardiomyopathy and Insight on Cardiac Biomarkers. Cureus 2020, 12, e11296. [Google Scholar] [CrossRef] [PubMed]
- Sala, S.; Peretto, G.; Gramegna, M.; Palmisano, A.; Villatore, A.; Vignale, D.; De Cobelli, F.; Tresoldi, M.; Cappelletti, A.M.; Basso, C.; et al. Acute myocarditis presenting as a reverse Tako-Tsubo syndrome in a patient with SARS-CoV-2 respiratory infection. Eur. Heart J. 2020, 41, 1861–1862. [Google Scholar] [CrossRef] [PubMed]
- Dabbagh, M.F.; Aurora, L.; D’Souza, P.; Weinmann, A.J.; Bhargava, P.; Basir, M.B. Cardiac Tamponade Secondary to COVID-19. JACC Case Rep. 2020, 2, 1326–1330. [Google Scholar] [CrossRef] [PubMed]
- Kariyanna, P.T.; Chandrakumar, H.P.; Jayarangaiah, A.; Khan, A.; Vulkanov, V.; Ashamalla, M.; Salifu, M.O.; McFarlane , S.I. Apical Takotsubo Cardiomyopathy in a COVID-19 Patient Presenting with Stroke: A Case Report and Pathophysiologic Insights. Am. J. Med. Case Rep. 2020, 8, 350–357. [Google Scholar] [CrossRef]
- Akashi, Y.J.; Nef, H.M.; Lyon, A.R. Epidemiology and pathophysiology of Takotsubo syndrome. Nat. Rev. Cardiol. 2015, 12, 387–397. [Google Scholar] [CrossRef] [Green Version]
- Citro, R.; Radano, I.; Bellino, M.; Mauro, C.; Okura, H.; Bossone, E.; Akashy, Y.J. Epidemiology, Pathogenesis, and Clinical Course of Takotsubo Syndrome. Heart Fail. Clin. 2022, 18, 125–137. [Google Scholar] [CrossRef]
- Moady, G.; Atar, S. Takotsubo Syndrome during the COVID-19 Pandemic: State-of-the-Art Review. CJC Open 2021, 3, 1249–1256. [Google Scholar] [CrossRef]
- Wittstein, I.S. The Sympathetic Nervous System in the Pathogenesis of Takotsubo Syndrome. Heart Fail. Clin. 2016, 12, 485–498. [Google Scholar] [CrossRef]
- Wittstein, I.S.; Thiemann, D.R.; Lima, J.A.; Baughman, K.L.; Schulman, S.P.; Gerstenblith, G.; Wu, K.C.; Rade, J.J.; Bivalacqua, T.J.; Champion, H.C. Neurohumoral features of myocardial stunning due to sudden emotional stress. N. Engl. J. Med. 2005, 352, 539–548. [Google Scholar] [CrossRef]
- Pelliccia, F.; Kaski, J.C.; Crea, F.; Camici, P.G. Pathophysiology of Takotsubo Syndrome. Circulation 2017, 135, 2426–2441. [Google Scholar] [CrossRef]
- Abraham, J.; Mudd, J.O.; Kapur, N.K.; Klein, K.; Champion, H.C.; Wittstein, I.S. Stress cardiomyopathy after intravenous administration of catecholamines and beta-receptor agonists. J. Am. Coll. Cardiol. 2009, 53, 1320–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kido, K.; Guglin, M. Drug-Induced Takotsubo Cardiomyopathy. J. Cardiovasc. Pharmacol. Ther. 2017, 22, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Paur, H.; Wright, P.T.; Sikkel, M.B.; Tranter, M.H.; Mansfield, C.; O’Gara, P.; Stuckey, D.J.; Nikolaev, V.O.; Diakonov, I.; Pannell, L.; et al. High levels of circulating epinephrine trigger apical cardiodepression in a β2-adrenergic receptor/Gi-dependent manner: A new model of Takotsubo cardiomyopathy. Circulation 2012, 126, 697–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiermaier, T.; Santoro, F.; Graf, T.; Guastafierro, F.; Tarantino, N.; De Gennaro, L.; Caldarola, P.; Di Biase, M.; Thiele, H.; Brunetti, N.D.; et al. Prognostic value of N-Terminal Pro-B-Type Natriuretic Peptide in Takotsubo syndrome. Clin. Res. Cardiol. 2018, 107, 597–606. [Google Scholar] [CrossRef]
- Fröhlich, G.M.; Schoch, B.; Schmid, F.; Keller, P.; Sudano, I.; Lüscher, T.F.; Noll, G.; Ruschitzka, F.; Enseleit, F. Takotsubo cardiomyopathy has a unique cardiac biomarker profile: NT-proBNP/myoglobin and NT-proBNP/troponin T ratios for the differential diagnosis of acute coronary syndromes and stress induced cardiomyopathy. Int. J. Cardiol. 2012, 154, 328–332. [Google Scholar] [CrossRef] [Green Version]
- Gubbi, S.; Nazari, M.A.; Taieb, D.; Klubo-Gwiezdzinska, J.; Pacak, K. Catecholamine physiology and its implications in patients with COVID-19. Lancet Diabetes Endocrinol. 2020, 8, 978–986. [Google Scholar] [CrossRef]
- Boonen, E.; Vervenne, H.; Meersseman, P.; Andrew, R.; Mortier, L.; Declercq, P.E.; Vanwijngaerden, Y.M.; Spriet, I.; Wouters, P.J.; Vander Perre, S.; et al. Reduced cortisol metabolism during critical illness. N. Engl. J. Med. 2013, 368, 1477–1488. [Google Scholar] [CrossRef] [Green Version]
- Wickboldt, N.; Pache, J.C.; Dietrich, P.Y.; Toso, C.; Gallay, C.; Brochard, L.; Merlani, P.; Pugin, D. Takotsubo syndrome secondary to adrenal adenocarcinoma: Cortisol as a possible culprit. Am. J. Respir. Crit. Care Med. 2012, 186, 1061–1062. [Google Scholar] [CrossRef]
- Sakihara, S.; Kageyama, K.; Nigawara, T.; Kidani, Y.; Suda, T. Ampulla (takotsubo) cardiomyopathy caused by secondary adrenal insufficiency in ACTH isolated deficiency. Endocr. J. 2007, 54, 631–636. [Google Scholar] [CrossRef] [Green Version]
- Tanasa, I.A.; Manciuc, C.; Carauleanu, A.; Navolan, D.B.; Bohiltea, R.E.; Nemescu, D. Anosmia and ageusia associated with coronavirus infection (COVID-19)—what is known? Exp. Ther. Med. 2020, 20, 2344–2347. [Google Scholar] [CrossRef]
- Staedtke, V.; Bai, R.Y.; Kim, K.; Darvas, M.; Davila, M.L.; Riggins, G.J.; Rothman, P.B.; Papadopoulos, N.; Kinzler, K.W.; Vogelstein, B.; et al. Disruption of a self-amplifying catecholamine loop reduces cytokine release syndrome. Nature 2018, 564, 273–277. [Google Scholar] [CrossRef]
- Lozano, A.; Bastante, T.; Salamanca, J.; Aguilar, R.; Montes de Oca, R.; Rodríguez, D.; Alfonso, F. Tako-tsubo cardiomyopathy triggered by Influenza A virus infection. Int. J. Cardiol. 2014, 174, e52–e53. [Google Scholar] [CrossRef] [PubMed]
- Elikowski, W.; Małek-Elikowska, M.; Lisiecka, M.; Trypuć, Z.; Mozer-Lisewska, I. Takotsubo cardiomyopathy triggered by influenza B. Pol. Merkur. Lek. 2018, 45, 67–70. [Google Scholar]
- Buzon, J.; Roignot, O.; Lemoine, S.; Perez, P.; Kimmoun, A.; Levy, B.; Novy, E. Takotsubo Cardiomyopathy Triggered by Influenza A Virus. Intern. Med. 2015, 54, 2017–2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golfeyz, S.; Kobayashi, T.; Aoi, S.; Harrington, M. Possible association of influenza A infection and reverse takotsubo syndrome. BMJ Case Rep. 2018, 11, e226289. [Google Scholar] [CrossRef]
- Faircloth, E.L.; Memon, S. Stressing Out from the Flu: A Case of Influenza A-associated Transient Cardiomyopathy. Cureus 2019, 11, e4918. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, M.; Nakagaito, M.; Hori, M.; Ueno, H.; Kinugawa, K. A case of Takotsubo cardiomyopathy with cardiogenic shock after influenza infection successfully recovered by IMPELLA support. J. Artif. Organs 2019, 22, 330–333. [Google Scholar] [CrossRef]
- Fazlollahi, A.; Zahmatyar, M.; Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Shekarriz-Foumani, R.; Kolahi, A.A.; Singh, K.; Safiri, S. Cardiac complications following mRNA COVID-19 vaccines: A systematic review of case reports and case series. Rev. Med. Virol. 2021, 17, e2318. [Google Scholar] [CrossRef]
- Madias, J.E. COVID-19, POCUS, and Takotsubo. Am. J. Cardiol. 2021, 141, 157. [Google Scholar] [CrossRef]
- Barnicle, R.; Bracey, A.; Secko, M. Early Identification of Takotsubo syndrome in the emergency department using point-of-care echocardiography: A case series. J. Clin. Ultrasound 2021, 49, 413–419. [Google Scholar] [CrossRef]
- Picard, M.H.; Weiner, R.B. Echocardiography in the Time of COVID-19. J. Am. Soc. Echocardiogr. 2020, 33, 674–675. [Google Scholar] [CrossRef] [PubMed]
- Frangieh, A.H.; Obeid, S.; Ghadri, J.R.; Imori, Y.; D’Ascenzo, F.; Kovac, M.; Ruschitzka, F.; Lüscher, T.F.; Duru, F.; Templin, C.; et al. ECG Criteria to Differentiate Between Takotsubo (Stress) Cardiomyopathy and Myocardial Infarction. J. Am. Heart Assoc. 2016, 5, e003418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chhabra, L.; Butt, N.; Ahmad, S.A.; Kayani, W.T.; Sangong, A.; Patel, V.; Bharaj, G.; Khalid, N. Electrocardiographic changes in Takotsubo cardiomyopathy. J. Electrocardiol. 2021, 65, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Thakar, S.; Chandra, P.; Hollander, G.; Lichstein, E. Electrocardiographic changes in Takotsubo cardiomyopathy. Pacing Clin. Electrophysiol. 2011, 34, 1278–1282. [Google Scholar] [CrossRef]
- Kochi, A.N.; Tagliari, A.P.; Forleo, G.B.; Fassini, G.M.; Tondo, C. Cardiac and arrhythmic complications in patients with COVID-19. J. Cardiovasc. Electrophysiol. 2020, 31, 1003–1008. [Google Scholar] [CrossRef] [Green Version]
- Dherange, P.; Lang, J.; Qian, P.; Oberfeld, B.; Sauer, W.H.; Koplan, B.; Tedrow, U. Arrhythmias and COVID-19: A Review. JACC Clin. Electrophysiol. 2020, 6, 1193–1204. [Google Scholar] [CrossRef]
- Chao, C.J.; DeValeria, P.A.; Sen, A.; Lee, H.; Pedrotty, D.M.; Patel, B.; Arsanjani, R.; Naqvi, T.Z. Reversible cardiac dysfunction in severe COVID-19 infection, mechanisms and case report. Echocardiography 2020, 37, 1465–1469. [Google Scholar] [CrossRef]
- Bernardi, N.; Calvi, E.; Cimino, G.; Pascariello, G.; Nardi, M.; Cani, D.; Faggiano, P.; Vizzardi, E.; Nunzia, D.M.; Marco, M. COVID-19 Pneumonia, Takotsubo Syndrome, and Left Ventricle Thrombi. JACC Case Rep. 2020, 2, 1359–1364. [Google Scholar] [CrossRef]
- Sattar, Y.; Connerney, M.; Ullah, W.; Philippou, A.; Slack, D.; McCarthy, B.; Kroll, S.; Luddington, S.; Ruiz Maya, T.; Alraies, M.C. COVID-19 Presenting as Takotsubo Cardiomyopathy Complicated with Atrial Fibrillation. Int. J. Cardiol. Heart Vasc. 2020, 29, 100580. [Google Scholar] [CrossRef]
- Tsao, C.W.; Strom, J.B.; Chang, J.D.; Manning, W.J. COVID-19-Associated Stress (Takotsubo) Cardiomyopathy. Circ. Cardiovasc. Imaging 2020, 13, e011222. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef] [PubMed]
- Titi, L.; Magnanimi, E.; Mancone, M.; Infusino, F.; Coppola, G.; Del Nonno, F.; Colombo, D.; Nardacci, R.; Falasca, L.; d’Amati, G.; et al. Fatal Takotsubo syndrome in critical COVID-19 related pneumonia. Cardiovasc. Pathol. 2020, 51, 107314. [Google Scholar] [CrossRef] [PubMed]
- Bapat, A.; Maan, A.; Heist, E.K. Stress-Induced Cardiomyopathy Secondary to COVID-19. Case Rep Cardiol. 2020, 2020, 8842150. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, P.J.; Attri, P.K.; Farooqui, W. Takotsubo cardiomyopathy in early term pregnancy: A rare cardiac complication of SARS-CoV-2 infection. BMJ Case Rep. 2020, 13, e239104. [Google Scholar] [CrossRef] [PubMed]
- Dave, S.; Thibodeau, J.T.; Styrvoky, K.; Bhatt, S.H. Takotsubo Cardiomyopathy in a Coronavirus Disease-2019-Positive Patient: A Case Report. A&A Pract. 2020, 14, e01304. [Google Scholar]
- Gomez, J.M.D.; Nair, G.; Nanavaty, P.; Rao, A.; Marinescu, K.; Suboc, T. COVID-19-associated takotsubo cardiomyopathy. BMJ Case Rep. 2020, 13, e236811. [Google Scholar] [CrossRef]
- Torabi, A.J.; Villegas-Galaviz, J.; Guglin, M.; Frick, K.; Rao, R. Cardiogenic shock following cardiac tamponade and Takotsubo in COVID-19. Future Cardiol. 2021, 17, 631–635. [Google Scholar] [CrossRef]
- Koh, M.C.Y.; Li, T.Y.W.; Ong, J.S.Y.; Somani, J.; Ambhore, A.A. Stress Cardiomyopathy with Transient Biventricular Dysfunction Following Recent COVID-19 Infection. Acta Cardiol. Sin. 2021, 37, 204–207. [Google Scholar]
- Khalid, Y.; Dasu, N.; Dasu, K. A case of novel coronavirus (COVID-19)-induced viral myocarditis mimicking a Takotsubo cardiomyopathy. HeartRhythm Case Rep. 2020, 6, 473–476. [Google Scholar] [CrossRef]
- Manzur-Sandoval, D.; Carmona-Levario, P.; García-Cruz, E. Giant inverted T waves in a patient with COVID-19 infection. Ann. Emerg. Med. 2021, 77, 264–267. [Google Scholar] [CrossRef]
- Minhas, A.S.; Scheel, P.; Garibaldi, B.; Liu, G.; Horton, M.; Jennings, M.; Jones, S.R.; Michos, E.D.; Hays, A.G. Takotsubo Syndrome in the Setting of COVID-19. JACC Case Rep. 2020, 2, 1321–1325. [Google Scholar] [CrossRef] [PubMed]
- Moderato, L.; Monello, A.; Lazzeroni, D.; Binno, S.; Giacalone, R.; Ferraro, S.; Piepoli, M.F.; Villani, G.Q. Sindrome Takotsubo in corso di polmonite da SARS-CoV-2: Una possibile complicanza cardiovascolare [Takotsubo syndrome during SARS-CoV-2 pneumonia: A possible cardiovascular complication]. G. Ital. Cardiol. 2020, 21, 417–420. [Google Scholar]
- Oyarzabal, L.; Gómez-Hospital, J.A.; Comin-Colet, J. Tako-tsubo syndrome associated with COVID-19. Rev. Esp. Cardiol. 2020, 73, 846. [Google Scholar] [CrossRef] [PubMed]
- Pasqualetto, M.C.; Secco, E.; Nizzetto, M.; Scevola, M.; Altafini, L.; Cester, A.; Rigo, F. Stress Cardiomyopathy in COVID-19 Disease. Eur. J. Case Rep. Intern. Med. 2020, 7, 001718. [Google Scholar] [PubMed]
- Van Osch, D.; Asselbergs, F.W.; Teske, A.J. Takotsubo cardiomyopathy in COVID-19: A case report. Haemodynamic and therapeutic considerations. Eur. Heart J. Case Rep. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Roca, E.; Lombardi, C.; Campana, M.; Vivaldi, O.; Bigni, B.; Bertozzi, B.; Passalacqua, G. Takotsubo Syndrome Associated with COVID-19. Eur. J. Case Rep. Intern. Med. 2020, 7, 001665. [Google Scholar] [CrossRef]
- Sang, C.J., III; Heindl, B.; Von Mering, G.; Brott, B.; Kopf, R.S.; Benson, P.V.; Rajapreyar, I. Stress-Induced Cardiomyopathy Precipitated by COVID-19 and Influenza A Coinfection. JACC Case Rep. 2020, 2, 1356–1358. [Google Scholar] [CrossRef]
- Taza, F.; Zulty, M.; Kanwal, A.; Grove, D. Takotsubo cardiomyopathy triggered by SARS-CoV-2 infection in a critically ill patient. BMJ Case Rep. 2020, 13, e236561. [Google Scholar] [CrossRef]
- Solano-López, J.; Sánchez-Recalde, A.; Zamorano, J.L. SARS-CoV-2, a novel virus with an unusual cardiac feature: Inverted takotsubo syndrome. Eur. Heart J. 2020, 41, 3106. [Google Scholar] [CrossRef]
- Medina de Chazal, H.; Del Buono, M.G.; Keyser-Marcus, L.; Ma, L.; Moeller, F.G.; Berrocal, D. Stress Cardiomyopathy Diagnosis and Treatment: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 1955–1971. [Google Scholar] [CrossRef]
- Sattar, Y.; Siew, K.S.W.; Connerney, M.; Ullah, W.; Alraies, M.C. Management of Takotsubo Syndrome: A Comprehensive Review. Cureus 2020, 12, e6556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzetto, F.; Lia, M.; Widmann, M.; Tavella, D.; Zanolla, L.; Pighi, M.; Ferrero, V.; Ribichini, F.L. Prognostic impact of antiplatelet therapy in Takotsubo syndrome: A systematic review and meta-analysis of the literature. Heart Fail. Rev. 2021; Online ahead of print. [Google Scholar]
- Redfors, B.; Jha, S.; Thorleifsson, S.; Jernberg, T.; Angerås, O.; Frobert, O.; Petursson, P.; Tornvall, P.; Sarno, G.; Ekenbäck, C.; et al. Short- and Long-Term Clinical Outcomes for Patients with Takotsubo Syndrome and Patients with Myocardial Infarction: A Report from the Swedish Coronary Angiography and Angioplasty Registry. J. Am. Heart Assoc. 2021, 10, e017290. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Delmas, C.; Bouisset, F.; Lairez, O. COVID-19 pandemic: No increase of takotsubo syndrome occurrence despite high-stress conditions. ESC Heart Fail. 2020, 7, 2143. [Google Scholar] [CrossRef]
- Barbieri, L.; Galli, F.; Conconi, B.; Gregorini, T.; Lucreziotti, S.; Mafrici, A.; Pravettoni, G.; Sommaruga, M.; Carugo, S. Takotsubo syndrome in COVID-19 era: Is psychological distress the key? J. Psychosom. Res. 2021, 140, 110297. [Google Scholar] [CrossRef]
- Jabri, A.; Kalra, A.; Kumar, A.; Alameh, A.; Adroja, S.; Bashir, H.; Nowacki, A.S.; Shah, R.; Khubber, S.; Kanaa’N, A.; et al. Incidence of Stress Cardiomyopathy during the Coronavirus Disease 2019 Pandemic. JAMA Netw. Open 2020, 3, e2014780. [Google Scholar] [CrossRef]
- Moady, G.; Atar, S. Quarantine-induced Stress Cardiomyopathy (Takotsubo syndrome) during the COVID-19 pandemic. Isr. Med. Assoc. J. 2021, 23, 149–152. [Google Scholar]


{kind=link}
| Complications | Inotropic Support | Mechanical Ventilation | Outcome | |
|---|---|---|---|---|
| Bottiroli et al. [18] | Shock | Y | Y | Recovery |
| Faqihi et al. [19] | Shock | Y | Y | Recovery |
| Nguyen et al. [20] | QT prolongation | N | Y | Recovery |
| Panchal et al. [21] | Shock | Y | Y | Death |
| Sala et al. [22] | - | N | N | Recovery |
| Dabbagh et al. [23] | - | N | N | Recovery |
| Kariyanna et al. [24] | Shock, acute ischemic stroke | Y | N | Death |
| Chao et al. [57] | QT prolongation | Y | Y | Recovery |
| Bernardi et al. [58] | LV thrombi | Y | N | Recovery |
| Sattar et al. [59] | Atrial fibrillation | N | N | Recovery |
| Tsao et al. [60] | Ventricular tachycardia | Y | Y | Recovery |
| Titi et al. [62] | - | Y | Y | Death |
| Bapat et al. [63] | QT prolongation | Y | Y | Recovery |
| Bhattacharyya et al. [64] | - | N | N | Recovery |
| Dave et al. [65] | Shock | Y | Y | Death |
| Gomez et al. [66] | QT prolongation | Y | Y | Recovery |
| Torabi et al. [67] | Cardiac tamponade | N | N | Death |
| Koh MCY et al. [68] | - | N | N | Recovery |
| Khalid et al. [69] | Shock | Y | Y | Recovery |
| Manzur-sandoval et al. [70] | QT prolongation | Y | Y | Recovery |
| Minhas et al. [71] | Shock | Y | N | Recovery |
| Moderato et al. [72] | QT prolongation | N | N | Recovery |
| Oyarzabal et al. [73] | - | N | N | Recovery |
| Pasqualetto et al. [74] | QT prolongation | N | N | Recovery |
| - | Y | Y | Death | |
| - | N | N | Recovery | |
| Van Osch et al. [75] | QT prolongation | N | Y | Recovery |
| Roca et al. [76] | - | N | N | Recovery |
| Sang et al. [77] | - | Y | Y | Death |
| Taza et al. [78] | - | N | N | Recovery |
| Solano-López et al. [79] | - | N | N | Recovery |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moady, G.; Atar, S. Stress-Induced Cardiomyopathy—Considerations for Diagnosis and Management during the COVID-19 Pandemic. Medicina 2022, 58, 192. https://doi.org/10.3390/medicina58020192
Moady G, Atar S. Stress-Induced Cardiomyopathy—Considerations for Diagnosis and Management during the COVID-19 Pandemic. Medicina. 2022; 58(2):192. https://doi.org/10.3390/medicina58020192
Chicago/Turabian StyleMoady, Gassan, and Shaul Atar. 2022. "Stress-Induced Cardiomyopathy—Considerations for Diagnosis and Management during the COVID-19 Pandemic" Medicina 58, no. 2: 192. https://doi.org/10.3390/medicina58020192
APA StyleMoady, G., & Atar, S. (2022). Stress-Induced Cardiomyopathy—Considerations for Diagnosis and Management during the COVID-19 Pandemic. Medicina, 58(2), 192. https://doi.org/10.3390/medicina58020192