
Does Melatonin Associated with Nanostructured Calcium Phosphate Improve Alveolar Bone Repair?

 , , , , ,
, , , , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Animal Model
2.3. Sample Size Calculation
2.4. Synthesis and Physical Chemical Characterization of Nanostructured Carbonated Hydroxyapatite
2.5. Melatonin Gel
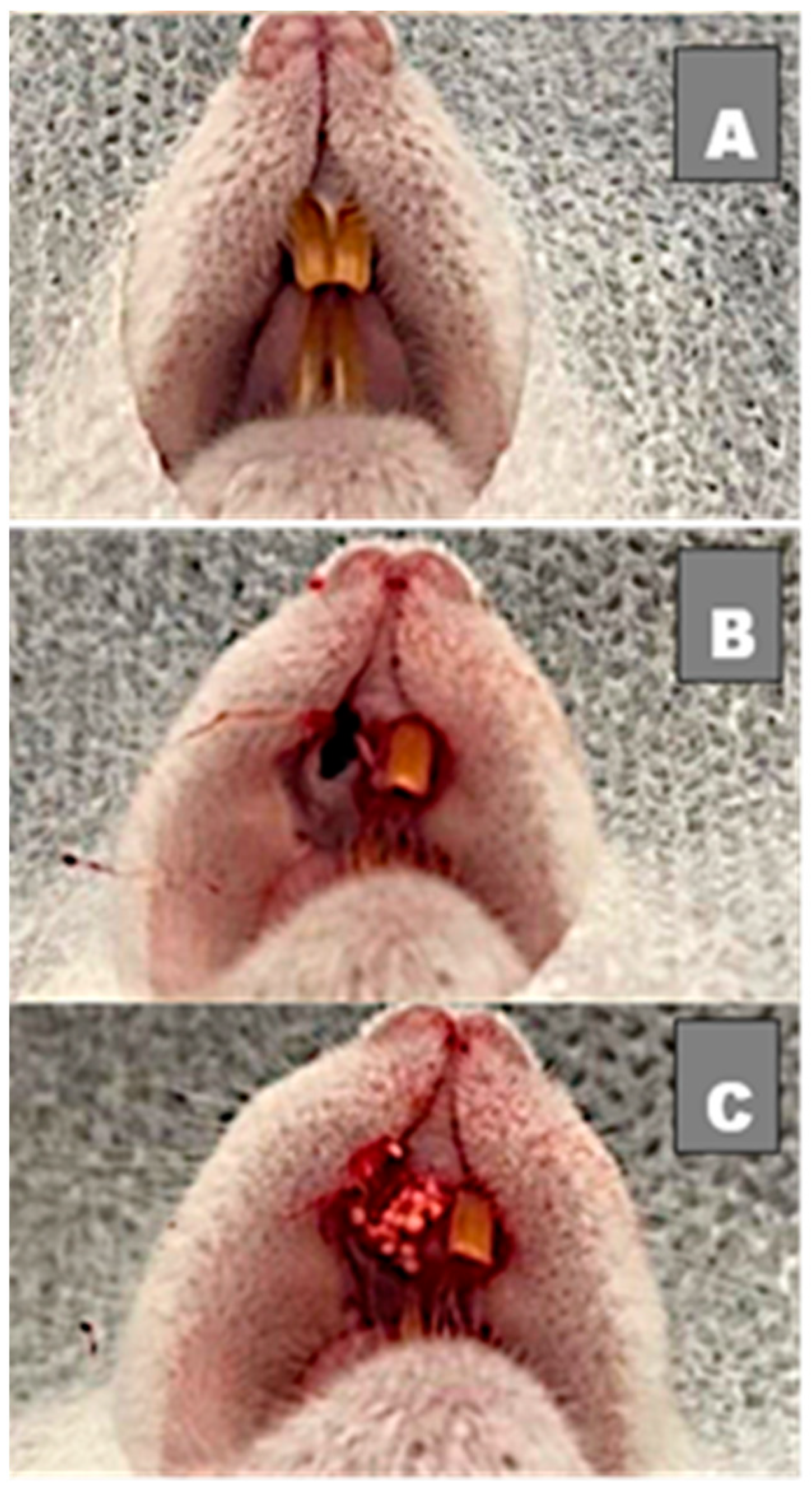
2.6. Surgical Procedures
2.7. Procedures and Postoperative Care
2.8. Obtaining Samples
2.9. Samples Processing
2.10. Histomorphometric Analysis
2.11. Statistical Analysis
3. Results
3.1. Histological Evaluation
3.2. Histomorphometric Results
3.2.1. Newly Formed Bone
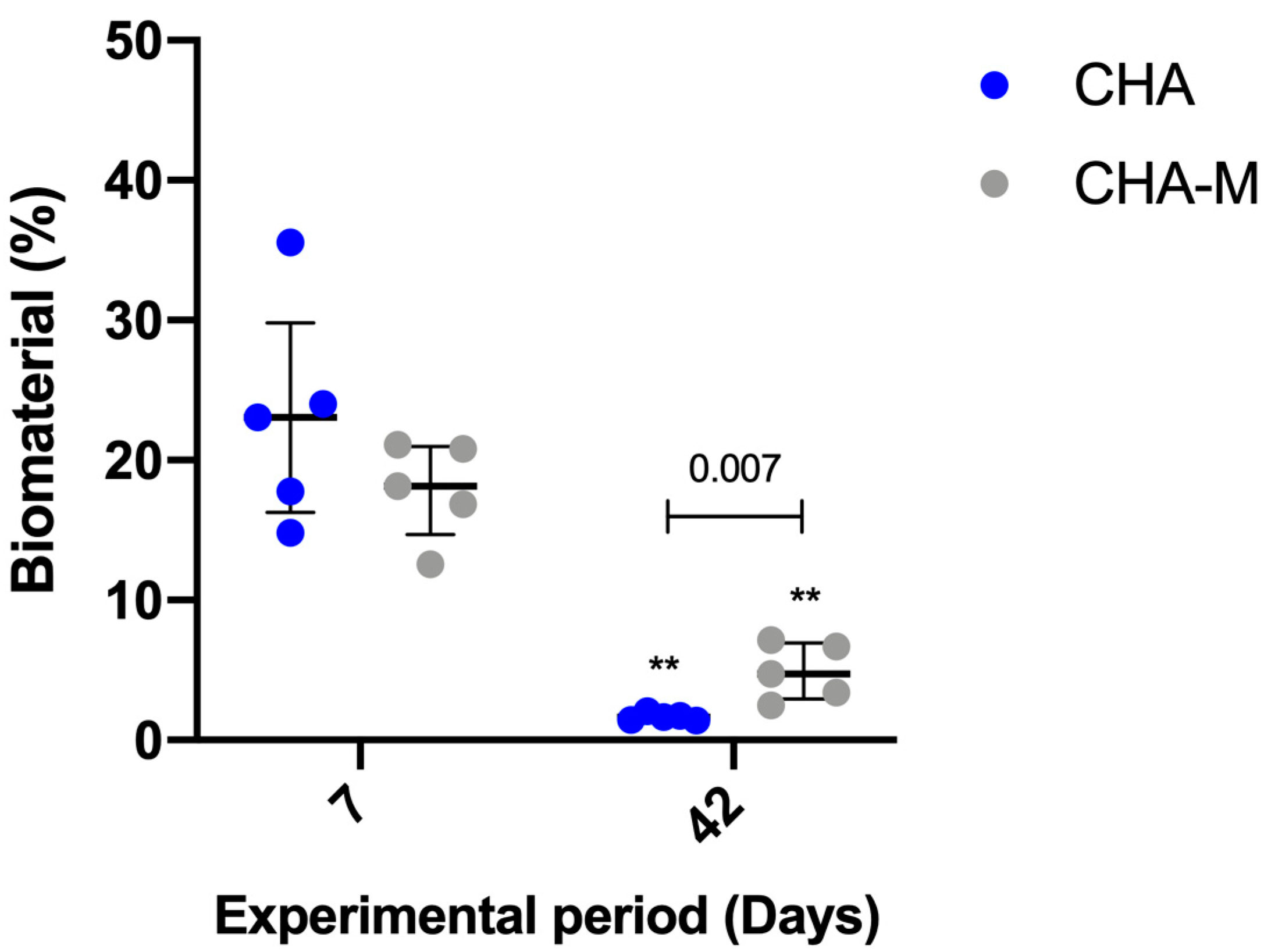
3.2.2. Biomaterial
3.2.3. Connective Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Landi, E.; Celotti, G.; Loproscino, G.; Tampieri, A. Carbonated hydroxyapatite as bone substitute. J. Eur. Ceram. Soc. 2003, 23, 2931–2937. [Google Scholar] [CrossRef]
- Habibovic, P.; Juhl, M.V.; Clyens, S.; Martinetti, R.; Dolcini, L.; Theilgaard, N.; van Blitterswijr, C.A. Comparison of two carbonated apatite ceramics in vivo. Acta Biomater. 2010, 6, 2219–2226. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Huang, F.; He, H.W. Melatonin effects on hard tissues: Bone and tooth. Int. J. Mol. Sci. 2013, 14, 10063–10074. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Li, J.; Xing, H.-L.; Tao, Z.-S.; Yang, M. Melatonin improves the osseointegration of hydroxyapatite-coated titanium implants in senile female rats. Z. Gerontol Geriatr. 2020, 53, 770–779. [Google Scholar] [CrossRef]
- Witt-Enderby, P.A.; Slater, J.P.; Johnson, N.A.; Bondi, C.D.; Dodda, B.R.; Kotlarczyk, M.P.; Clafshenkel, W.P.; Sethi, S.; Higginbotham, S.; Rutkowski, J.L.; et al. Effects on bone by the light/dark cycle and chronic treatment with melatonin and/or hormone replacement therapy in intact female mice. J. Pineal Res. 2012, 53, 374–384. [Google Scholar] [CrossRef]
- Histing, T.; Anton, C.; Scheuer, C.; Garcia, P.; Holstein, J.H.; Klein, M.; Matthys, R.; Pohlemann, T.; Menger, M.D. Melatonin impairs fracture healing by suppressing rankl-mediated bone remodeling. J. Surg. Res. 2012, 173, 83–90. [Google Scholar] [CrossRef]
- Gomez-Moreno, G.; Aguilar-Salvatierra, A.; Boquete-Castro, A.; Guardia, J.; Piatelli, A.; Perrotti, V.; Delgado-Ruiz, R.A.; Calvo-Guirado, J.L. Outcomes of topical applications of melatonin in implant dentistry: A systematic review. Implant. Dent. 2015, 24, 25–30. [Google Scholar] [CrossRef]
- Ferry, G.; Ubeaud, C.; Lambert, P.-H.; Bertin, S.; Cogé, F.; Chomarat, P.; Delagrange, P.; Serkiz, B.; Bouchet, J.-P.; Truscott, R.J.W.; et al. Molecular evidence that melatonin is enzymatically oxidized in a different manner than tryptophan: Investigations with both indoleamine 2,3-dioxygenase and myeloperoxidase. Biochem. J. 2005, 388, 205–215. [Google Scholar] [CrossRef]
- Cutando, A.; Gomez-Moreno, G.; Arana, C.; Munoz, F.; Lopez-Pena, M.; Stephenson, J.; Reiter, R.J. Melatonin stimulates osteointegration of dental implants. J. Pineal Res. 2008, 45, 174–179. [Google Scholar] [CrossRef]
- Luchetti, F.; Canonico, B.; Bartolini, D.; Arcangeletti, M.; Ciffolilli, S.; Murdolo, G.; Piroddi, M.; Papa, S.; Reiter, R.J.; Galli, F. Melatonin regulates mesenchymal stem cell differentiation: A review. J. Pineal Res. 2014, 56, 382–397. [Google Scholar] [CrossRef]
- Zhou, L.; Chen, X.; Yan, J.; Li, M.; Liu, T.; Zhu, C.; Pan, G.; Guo, Q.; Yang, H.; Pei, M.; et al. Melatonin at pharmacological concentrations suppresses osteoclastogenesis via the attenuation of intracellular ROS. Osteoporos. Int. 2017, 28, 3325–3337. [Google Scholar] [CrossRef]
- Sethi, S.; Radio, N.M.; Kotlarczyk, M.P.; Chen, C.-T.; Wei, Y.-H.; Jockers, R.; Witt-Enderby, P.A. Determination of the minimal melatonin exposure required to induce osteoblast differentiation from human mesenchymal stem cells and these effects on downstream signaling pathways. J. Pineal Res. 2010, 49, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Palin, L.P.; Polo, T.O.B.; Batista, F.R.D.S.; Gomes-Ferreira, P.H.S.; Junior, I.R.G.; Rossi, A.C.; Freire, A.; Faverani, L.P.; Sumida, D.H.; Okamoto, R. Daily melatonin administration improves osseointegration in pinealectomized rats. J. Appl. Oral Sci. 2018, 26, 1–10. [Google Scholar] [CrossRef]
- Tresguerres, I.F.; Clemente, C.; Blanco, L.; Khraisat, A.; Tamim, F.; Tresguerres, J.A. Effects of Local Melatonin Application on Implant Osseointegration. Clin. Implant. Dent. Relat. Res. 2012, 14, 395–399. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Ramírez-Fernández, M.P.; Gómez-Moreno, G.; Maté-Sánchez, J.E.; Delgado-Ruiz, R.; Guardia, J.; López-Marí, L.; Barone, A.; Ortiz-Ruiz, A.J.; Martínez-González, J.M.; et al. Melatonin stimulates the growth of new bone around implants in the tibia of rabbits. J. Pineal Res. 2010, 49, 356–363. [Google Scholar] [CrossRef]
- Salomó-Coll, O.; de Maté-Sánchez, J.V.; Ramirez-Fernandez, M.P.; Hernandez-Alfaro, F.; Gargallo-Albion, J.; Calvo-Guirado, J.L. Osseoinductive elements around immediate implants for better osteointegration: A pilot study in foxhound dogs. Clin. Oral Implant. Res. 2018, 29, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Kim, Y.-M.; Kim, H.S.; Lee, K.Y. Melatonin promotes osteoblast differentiation by regulating Osterix protein stability and expression. Sci. Rep. 2017, 7, 5716. [Google Scholar] [CrossRef] [PubMed]
- Hazzaa, H.; El-Kilani, N.S.; Elsayed, S.A.-E.; Massieh, P.M.A. Evaluation of Immediate Implants Augmented with Autogenous Bone/Melatonin Composite Graft in the Esthetic Zone: A Randomized Controlled Trial. J. Prosthodont. 2017, 28, 637–642. [Google Scholar] [CrossRef]
- Son, J.H.; Cho, Y.-C.; Jung, L.-Y.; Kim, I.-R.; Park, B.-S.; Kim, Y.-D. Melatonin promotes osteoblast differentiation and mineralization of MC3T3-E1 cells under hypoxic conditions through activation of PKD/p38 pathways. J. Pineal Res. 2014, 57, 385–392. [Google Scholar] [CrossRef]
- López-Martínez, F.; Ponce, P.N.O.; Rodriguez, M.G.; Pedroza, R.M. Melatonin: Bone Metabolism in Oral Cavity. Int. J. Dent. 2012, 2012, 1–5. [Google Scholar] [CrossRef]
- Krajewski, A.; Mazzocchi, M.; Buldini, P.L.; Ravaglioli, A.; Tinti, A.; Taddei, P.; Fagnano, C. Synthesis of carbonated hydroxyapatites: Efficiency of the substitution and critical evaluation of analytical methods. J. Mol. Struct. 2005, 744–747, 221–228. [Google Scholar] [CrossRef]
- Soriano-Souza, C.A.; Rossi, A.L.; Mavropoulos, E.; Hausen, M.A.; Tanaka, M.N.; Calasans-Maia, M.D.; Granjeiro, J.M.; Rocha-Leão, M.H.M.; Rossi, A.M. Chlorhexidine-loaded hydroxyapatite microspheres as an antimicrobial delivery system and its effect on in vivo osteo-conductive properties. J. Mater. Sci. Mater. Med. 2015, 26, 166. [Google Scholar] [CrossRef] [PubMed]
- Calasans-Maia, M.D.; Junior, C.A.B.B.; Soriano-Souza, C.A.; Alves, A.T.N.N.; Uzeda, M.J.D.P.; Martínez-Zelaya, V.R.; Mavropoulos, E.; Leão, M.H.R.; Santana, R.; Granjeiro, J.M.; et al. Microspheres of alginate encapsulated minocycline-loaded nanocrystalline carbonated hydroxyapatite: Therapeutic potential and effects on bone regeneration. Int. J. Nanomed. 2019, 14, 4559–4571. [Google Scholar] [CrossRef] [PubMed]
- Bose, S.; Roy, M.; Bandyopadhyay, A. Recent advances in bone tissue engineering scaffolds. Trends Biotechnol. 2012, 30, 546–554. [Google Scholar] [CrossRef]
- Soriano-Souza, C.; Valiense, H.; Mavropoulos, E.; Martinez-Zelaya, V.; Costa, A.M.; Alves, A.T.; Longuinho, M.; Resende, R.; Mourão, C.F.; Granjeiro, J.; et al. Doxycycline containing hydroxyapatite ceramic microspheres as a bone-targeting drug delivery system. J. Biomed. Mater. Res. 2019, 108, 1351–1362. [Google Scholar] [CrossRef]
- Vianna, T.S.W.; Sartoretto, S.C.; Alves, A.T.N.N.; Resende, R.F.D.B.; Mourão, C.F.D.A.B.; Calasans-Maia, J.D.A.; Martinez-Zelaya, V.R.; Rossi, A.M.; Granjeiro, J.M.; Calasans-Maia, M.D.; et al. Nanostructured Carbonated Hydroxyapatite Associated to rhBMP-2 Improves Bone Repair in Rat Calvaria. J. Funct. Biomater. 2020, 11, 87. [Google Scholar] [CrossRef]
- Ten Heggeler, J.M.A.G.; Slot, D.E.; Van der Weijden, G.A. Effect of socket preservation therapies following tooth extraction in non-molar regions in humans: A systematic review. Clin. Oral Implant. Res. 2011, 22, 779–788. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post extractional sockets hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23, 1–21. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Animal research: Reporting in vivo experiments: The ARRIVE guidelines. Br. J. Pharmacol. 2010, 160, 1577–1579. [Google Scholar] [CrossRef]
- Smith, A.J.; Clutton, R.E.; Lilley, E.; Hansen, K.E.A.; Brattelid, T. PREPARE: Guidelines for planning animal research and testing. Lab. Anim. 2018, 52, 135–141. [Google Scholar] [CrossRef]
- European Medicines Agency. Guideline on the Principles of Regulatory Acceptance of 3Rs (Replacement, Reduction, Refinement) Testing Approaches; European Medicines Agency: London, UK, 2016. [Google Scholar]
- Calasans-Maia, M.D.; Melo, B.R.; Alves, A.T.N.N.; Resende, R.F.B.; Louro, R.S.; Sartoretto, S.C.; Granjeiro, J.M.; Alves, G.G. Cytocompatibility and biocompatibility of nanostructured carbonated hydroxyapatite spheres for bone repair. J. Appl. Oral Sci. 2016, 23, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Hesaraki, S.; Nazarian, H.; Pourbaghi-Masouleh, M.; Borhan, S. Comparative study of mesenchymal stem cells osteogenic differentiation on low-temperature biomineralized Nanocrystalline carbonated hydroxyapatite and sintered hydroxyapatite. J. Biomed. Mater Res. B Appl. Biomater. 2014, 102, 108–118. [Google Scholar] [CrossRef]
- Mourão, C.F.A.B.; Lourenço, E.S.; Nascimento, J.R.B.; Machado, R.C.M.; Rossi, A.M.; Leite, P.E.C.; Granjeiro, J.M.; Alves, G.G.; Calasans-Maia, M.D. Does the association of blood-derived growth factors to nanostructured carbonated hydroxyapatite contributes to the maxillary sinus floor elevation? A randomized clinical trial. Clin. Oral Investig. 2019, 23, 369–379. [Google Scholar] [CrossRef]
- Valiense, H.; Barreto, M.; Resende, R.F.B.; Alves, A.T.N.N.; Rossi, A.M.; Mavropoulos, E.; Granjeiro, J.M.; Calasans-Maia, M.D. In vitro and in vivo evaluation of strontium-containing nanostructured carbonated hydroxyapatite/sodium alginate for sinus lift in rabbits. J. Biomed. Mater. Res.—Part B Appl. Biomater. 2016, 104, 274–282. [Google Scholar] [CrossRef] [PubMed]
- El-Gammal, M.; Salem, A.S.; Anees, M.M.; Tawfik, M.A. Clinical and radiographic evaluation of immediate loaded dental implants with local application of melatonin: A preliminary randomized controlled clinical trial. J. Oral Implantol. 2016, 42, 119–125. [Google Scholar] [CrossRef]
- Resende, R.F.B.; Fernandes, G.V.O.; Santos, S.R.A.; Rossi, A.M.; Lima, I.; Granjeiro, J.M.; Calasans-Maia, M.D. Long-term biocompatibility evaluation of 0.5% zinc containing hydroxyapatite in rabbits. J. Mater. Sci. Mater. Med. 2013, 24, 1455–1463. [Google Scholar] [CrossRef] [PubMed]
- Arabacı, T.; Kermen, E.; Özkanlar, S.; Köse, O.; Kara, A.; Kızıldağ, A.; Duman, S.B.; Ibişoğlu, E. Therapeutic Effects of Melatonin on Alveolar Bone Resorption After Experimental Periodontitis in Rats: A Biochemical and Immunohistochemical Study. J. Periodontol. 2015, 86, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; López-López, P.J.; Domínguez, M.F.; Gosálvez, M.M.; Prados-Frutos, J.C.; Gehrke, S.A. Histologic evaluation of new bone in post-extraction sockets induced by melatonin and apigenin: An experimental study in American fox hound dogs. Clin. Oral Implant. Res. 2016, 29, 1–9. [Google Scholar]
- Calvo-Guirado, J.L.; Fernández-Domínguez, M.; Aragoneses, J.M.; Fernández-Bodereau, E.; Garcés-Villalá, M.A.; Villafranca, F.C.; Cabello-Colás, M.; Jiménez-López, R.; Albacete-Martínez, C.P.; Rafael Delgado-Ruiz, A. Experimental Study on the Influence of Apigenin K and Melatonin in Socket Preservation as Bone Stimulators: An Experimental Study in Beagle Dogs. Appl. Sci. 2020, 10, 5865. [Google Scholar] [CrossRef]
- Koparal, M.; Irtegun, S.; Alan, H.; Deveci, E.; Gulsun, B.; Pektanc, G. Effects of Melatonin on Tibia Bone Defects in Rats. Int. J. Morphol. 2016, 34, 763–769. [Google Scholar] [CrossRef]
- Ramírez-Fernández, M.P.; Calvo-Guirado, J.L.; de-Val, J.E.M.S.; Delgado-Ruiz, R.A.; Negri, B.; Pardo-Zamora, G.; Peñarrocha, D.; Barona, C.; Granero, J.M.; Alcaraz-Baños, M. Melatonin promotes angiogenesis during repair of bone defects: A radiological and histomorphometric study in rabbit tibiae. Clin. Oral Investig. 2013, 17, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, F.; López-Peña, M.; Miño, N.; Gómez-Moreno, G.; Guardia, J.; Cutando, A. Topical Application of Melatonin and Growth Hormone Accelerates Bone Healing around Dental Implants in Dogs. Clin. Implant Dent. Relat. Res. 2012, 14, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Clafshenkel, W.P.; Rutkowski, J.L.; Palchesko, R.N.; Romeo, J.D.; McGowan, K.A.; Gawalt, E.S.; Witt-Enderby, P.A. A novel calcium aluminate-melatonin scaffold enhances bone regeneration within a calvarial defect. J. Pineal Res. 2012, 53, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Shino, H.; Hasuike, A.; Arai, Y.; Honda, M.; Isokawa, K.; Sato, S. Melatonin enhances vertical bone augmentation in rat calvaria secluded spaces. Oral Surgery 2015, 21, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Sifat, M.; Witt-Enderby, P.A. Melatonin effects on bone: Potential use for the prevention and treatment for osteopenia, osteoporosis, and periodontal disease and for use in bone-grafting procedures. J. Pineal Res. 2014, 56, 115–125. [Google Scholar]
- Park, K.H.; Kang, J.W.; Lee, E.M.; Kim, J.S.; Rhee, Y.H.; Kim, M.; Jeong, S.J.; Park, Y.G.; Kim, S.H. Melatonin promotes osteoblastic differentiation through the BMP/ERK/Wnt signaling pathways. J. Pineal Res. 2011, 51, 187–194. [Google Scholar] [CrossRef]
- Lu, X.; Yu, S.; Chen, G.; Zheng, W.; Peng, J.; Huang, X.; Chen, L. Insight into the roles of melatonin in bone tissue and bone related diseases. Int. J. Mol. Med. 2021, 47, 82. [Google Scholar] [CrossRef]
- Majidiniaa, M.; Reiter, R.J.; Shakouri, S.K.; Mohebbid, I.; Rastegar, M.; Kaviani, M.; Darband, S.G.; Jahanban-Esfahlanhi, R.; Nabavi, S.M.; Yousefi, B. The multiple functions of melatonin in regenerative medicine. Ageing Res. Rev. 2017, 45, 33–52. [Google Scholar] [CrossRef]
- Oryan, A.; Monazzah, S.; Bigham-Sadegh, A. The Effects of Melatonin in Bone Healing. J. Vet. Sci. Res. 2018, 3, 1–7. [Google Scholar]
- Litovka, I.H.; Mazepa-Kryzhanivs’ka, Y.O.; La Berezovskyĭ, V. Effect of Melatonin on Bone Tissue Metabolism. Int. J. Physiol. Pathophysiol. 2015, 6, 165–175. [Google Scholar] [CrossRef]
- Roth, J.A.; Kim, B.G.; Lin, W.L.; Cho, M.I. Melatonin Promotes Osteoblast Differentiation and Bone Formation. J. Biol. Chem. 1999, 274, 22041–22047. [Google Scholar] [CrossRef]
- Meenakshi, S.S.; Malaiappan, S. Role of melatonin in periodontal disease—A systematic review. Indian J. Dent. Res. 2020, 31, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Moreno, P.G.; Ortiz, G.A.; Wang, H.L.; Molina, M.P.; Ollera, I.O.; Ravassa, F.V. The role of melatonin in periodontal and periimplant bone homeostasis and regeneration. J. Oral Sci. Rehabil. 2016, 2, 8–15. [Google Scholar]
- Srinath, R.; Acharya, A.B.; Thakur, S.L. Salivary and Gingival Crevicular Fluid Melatonin in Periodontal Health and Disease. J. Periodontol. 2010, 81, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Cutando, A.; Galindo, P.; Gómez-Moreno, G.; Arana, C.; Bolaños, J.; Acuña-Castroviejo, D.; Wang, H.L. Relationship Between Salivary Melatonin and Severity of Periodontal Disease. J. Periodontol. 2008, 77, 1533–1538. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Moreno, G.; Cutando-Soriano, A.; Arana, C.; Galindo, P.; Bolanos, J.; Acuna-Castroviejo, D.; Wang, H.L. Melatonin expression. Periodontal Dis. J. Periodontal Res. 2007, 42, 536–540. [Google Scholar] [CrossRef]
- Salomo-Coll, O.; de Val Mate-Sanchez, J.E.; Ramirez-Fernandez, M.P.; Satorres-Nieto, M.; Gargallo-Albiol, J.; Calvo-Guirado, J.L. Osseoinductive elements for promoting osseointegration around immediate implants: A pilot study in the foxhound dog. Clin. Oral Implant. Res. 2015, 29, 1061–1069. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Aguilar Salvatierra, A.; Gargallo-Albiol, J.; Delgado-Ruiz, R.A.; Mate Sanchez, J.E.; Satorres-Nieto, M. Zir-conia with laser-modified microgrooved surface vs. titanium implants covered with melatonin stimulates bone forma-tion. Experimental study in tibia rabbits. Clin. Oral Implant. Res. 2015, 26, 1421–1429. [Google Scholar] [CrossRef]
- Horvath, A.; Marda, N.; Mezzomo, L.A.; Ian, G.; Needleman, N.D. Alveolar ridge preservation. A systematic review. Clin. Oral Investig. 2013, 17, 341–363. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Almeida, C.D.; Sartoretto, S.C.; Alves, A.T.N.N.; de Brito Resende, R.F.; de Albuquerque Calasans-Maia, J.; Moraschini, V.; Rossi, A.; Granjeiro, J.M.; Sacco, R.; Calasans-Maia, M.D. Does Melatonin Associated with Nanostructured Calcium Phosphate Improve Alveolar Bone Repair? Medicina 2022, 58, 1720. https://doi.org/10.3390/medicina58121720
de Almeida CD, Sartoretto SC, Alves ATNN, de Brito Resende RF, de Albuquerque Calasans-Maia J, Moraschini V, Rossi A, Granjeiro JM, Sacco R, Calasans-Maia MD. Does Melatonin Associated with Nanostructured Calcium Phosphate Improve Alveolar Bone Repair? Medicina. 2022; 58(12):1720. https://doi.org/10.3390/medicina58121720
Chicago/Turabian Stylede Almeida, Camila Diuana, Suelen Cristina Sartoretto, Adriana Terezinha Neves Novellino Alves, Rodrigo Figueiredo de Brito Resende, Jose de Albuquerque Calasans-Maia, Vittorio Moraschini, Alexandre Rossi, José Mauro Granjeiro, Roberto Sacco, and Mônica Diuana Calasans-Maia. 2022. "Does Melatonin Associated with Nanostructured Calcium Phosphate Improve Alveolar Bone Repair?" Medicina 58, no. 12: 1720. https://doi.org/10.3390/medicina58121720
APA Stylede Almeida, C. D., Sartoretto, S. C., Alves, A. T. N. N., de Brito Resende, R. F., de Albuquerque Calasans-Maia, J., Moraschini, V., Rossi, A., Granjeiro, J. M., Sacco, R., & Calasans-Maia, M. D. (2022). Does Melatonin Associated with Nanostructured Calcium Phosphate Improve Alveolar Bone Repair? Medicina, 58(12), 1720. https://doi.org/10.3390/medicina58121720