

Clinical Validation of Dental Implant Stability by Newly Designed Damping Capacity Assessment Device during the Healing Period

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
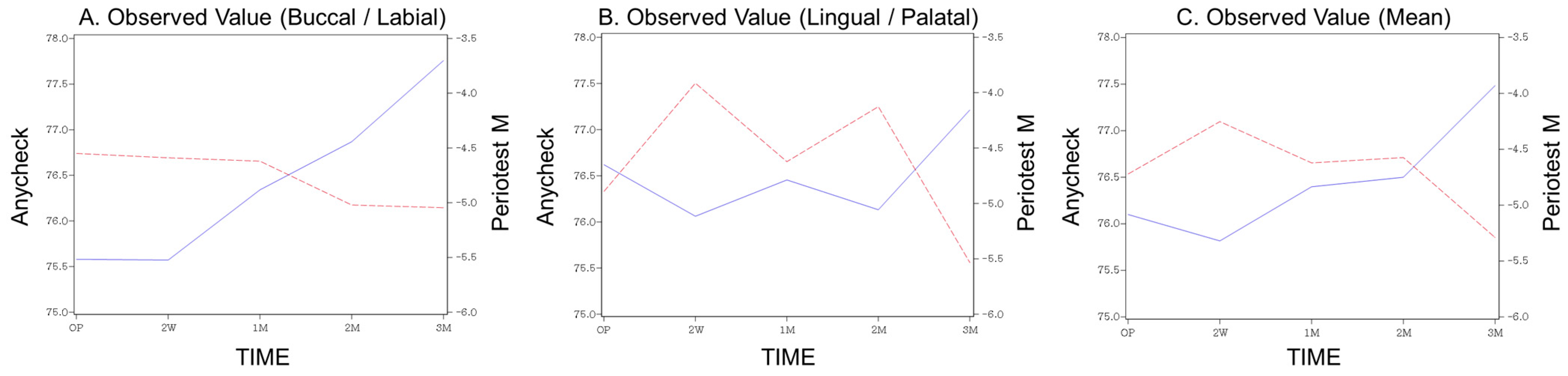
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Juboori, M.J.; Bin Ismail, I.H.; Ab Rahman, S. Dental implant stability and its measurement. Dent Implant. Update 2012, 23, 57–61. [Google Scholar]
- Gupta, R.K.; Padmanabhan, T.V. An evaluation of the resonance frequency analysis device: Examiner reliability and repeatability of readings. J. Oral Implant. 2013, 39, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Lachmann, S.; Jager, B.; Axmann, D.; Gomez-Roman, G.; Groten, M.; Weber, H. Resonance frequency analysis and damping capacity assessment. Part I: An in vitro study on measurement reliability and a method of comparison in the determination of primary dental implant stability. Clin. Oral Implant. Res. 2006, 17, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Al-Jetaily, S.; Al-Dosari, A.A. Assessment of Osstell and Periotest(R) systems in measuring dental implant stability (in vitro study). Saudi Dent. J. 2011, 23, 17–21. [Google Scholar] [CrossRef]
- Lee, D.H.; Shin, Y.H.; Park, J.H.; Shim, J.S.; Shin, S.W.; Lee, J.Y. The reliability of Anycheck device related to healing abutment diameter. J. Adv. Prosthodont. 2020, 12, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Pyo, S.W.; Cho, H.J.; An, J.S.; Lee, J.H.; Koo, K.T.; Lee, Y.M. Comparison of implant stability measurements between a resonance frequency analysis device and a modified damping capacity analysis device: An in vitro study. J. Periodontal Implant. Sci. 2020, 50, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Andreotti, A.M.; Goiato, M.C.; Nobrega, A.S.; Freitas da Silva, E.V.; Filho, H.G.; Pellizzer, E.P.; Micheline Dos Santos, D. Relationship Between Implant Stability Measurements Obtained by Two Different Devices: A Systematic Review. J. Periodontol. 2017, 88, 281–288. [Google Scholar] [CrossRef]
- Tozum, T.F.; Bal, B.T.; Turkyilmaz, I.; Gulay, G.; Tulunoglu, I. Which device is more accurate to determine the stability/mobility of dental implants? A human cadaver study. J. Oral Rehabil. 2010, 37, 217–224. [Google Scholar] [CrossRef]
- Scarano, A.; Carinci, F.; Quaranta, A.; Iezzi, G.; Piattelli, M.; Piattelli, A. Correlation between implant stability quotient (ISQ) with clinical and histological aspects of dental implants removed for mobility. Int. J. Immunopathol. Pharmacol. 2007, 20, 33–36. [Google Scholar] [CrossRef]
- Bilhan, H.; Cilingir, A.; Bural, C.; Bilmenoglu, C.; Sakar, O.; Geckili, O. The Evaluation of the Reliability of Periotest for Implant Stability Measurements: An In Vitro Study. J. Oral Implant. 2015, 41, e90–e95. [Google Scholar] [CrossRef]
- Meredith, N.; Friberg, B.; Sennerby, L.; Aparicio, C. Relationship between contact time measurements and PTV values when using the Periotest to measure implant stability. Int. J. Prosthodont. 1998, 11, 269–275. [Google Scholar] [PubMed]
- Berglundh, T.; Abrahamsson, I.; Lang, N.P.; Lindhe, J. De novo alveolar bone formation adjacent to endosseous implants. Clin. Oral Implant. Res. 2003, 14, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Moreno, F.J.; Herrera-Briones, F.J.; Bassam, T.; Vallecillo-Capilla, M.F.; Reyes-Botella, C. Factors Affecting Dental Implant Stability Measured Using the Ostell Mentor Device: A Systematic Review. Implant Dent. 2015, 24, 565–577. [Google Scholar] [CrossRef]
- Degidi, M.; Scarano, A.; Piattelli, M.; Perrotti, V.; Piattelli, A. Bone remodeling in immediately loaded and unloaded titanium dental implants: A histologic and histomorphometric study in humans. J. Oral Implant. 2005, 31, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Rincon-Castro, M.V.; Poveda-Marin, A.E.; Diazgranados-Lozano, M.P.; Fajardo-Escolar, C.E.; Bocanegra-Puerta, M.C.; Palma, L.F. Histological healing outcomes at the bone-titanium interface of loaded and unloaded dental implants placed in humans: A systematic review of controlled clinical trials. Int. J. Oral Implant. 2020, 13, 321–342. [Google Scholar]
- Lai, H.C.; Zhang, Z.Y.; Wang, F.; Zhuang, L.F.; Liu, X. Resonance frequency analysis of stability on ITI implants with osteotome sinus floor elevation technique without grafting: A 5-month prospective study. Clin. Oral Implant. Res. 2008, 19, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.X.; Shi, J.Y.; Zhuang, L.F.; Qian, S.J.; Mo, J.J.; Lai, H.C. Transalveolar sinus floor elevation using osteotomes without grafting in severely atrophic maxilla: A 5-year prospective study. Clin. Oral Implant. Res. 2016, 27, 120–125. [Google Scholar] [CrossRef]
- Tirachaimongkol, C.; Pothacharoen, P.; Reichart, P.A.; Khongkhunthian, P. Relation between the stability of dental implants and two biological markers during the healing period: A prospective clinical study. Int. J. Implant Dent. 2016, 2, 27. [Google Scholar] [CrossRef]
- Raghavendra, S.; Wood, M.C.; Taylor, T.D. Early wound healing around endosseous implants: A review of the literature. Int. J. Oral Maxillofac. Implant. 2005, 20, 425–431. [Google Scholar]
- Charatchaiwanna, A.; Rojsiraphisa, T.; Aunmeungtong, W.; Reichart, P.A.; Khongkhunthian, P. Mathematical equations for dental implant stability patterns during the osseointegration period, based on previous resonance frequency analysis studies. Clin. Implant. Dent. Relat. Res. 2019, 21, 1028–1040. [Google Scholar] [CrossRef]
- Lachmann, S.; Laval, J.Y.; Jager, B.; Axmann, D.; Gomez-Roman, G.; Groten, M.; Weber, H. Resonance frequency analysis and damping capacity assessment. Part 2: Peri-implant bone loss follow-up. An in vitro study with the Periotest and Osstell instruments. Clin. Oral Implant. Res. 2006, 17, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Zix, J.; Hug, S.; Kessler-Liechti, G.; Mericske-Stern, R. Measurement of dental implant stability by resonance frequency analysis and damping capacity assessment: Comparison of both techniques in a clinical trial. Int. J. Oral Maxillofac. Implant. 2008, 23, 525–530. [Google Scholar]
- Winter, W.; Mohrle, S.; Holst, S.; Karl, M. Parameters of implant stability measurements based on resonance frequency and damping capacity: A comparative finite element analysis. Int. J. Oral Maxillofac. Implant. 2010, 25, 532–539. [Google Scholar]
- Lachmann, S.; Laval, J.Y.; Axmann, D.; Weber, H. Influence of implant geometry on primary insertion stability and simulated peri-implant bone loss: An in vitro study using resonance frequency analysis and damping capacity assessment. Int. J. Oral Maxillofac. Implant. 2011, 26, 347–355. [Google Scholar]
- Feng, S.W.; Lin, C.T.; Chang, W.J.; Lee, S.Y.; Cheng, C.H.; Huang, H.M. Influence of simulated bone quality and cortical bone thickness on implant stability detection using resonance frequency and damping factor analysis. Int. J. Oral Maxillofac. Implant. 2014, 29, 105–112. [Google Scholar] [CrossRef][Green Version]
- Kwon, T.K.; Kim, H.Y.; Yang, J.H.; Wikesjo, U.M.; Lee, J.; Koo, K.T.; Yeo, I.S. First-Order Mathematical Correlation Between Damping and Resonance Frequency Evaluating the Bone-Implant Interface. Int. J. Oral Maxillofac. Implant. 2016, 31, 1008–1015. [Google Scholar] [CrossRef]
- Pyo, S.W.; Kim, H.G.; Kwon, O.; Otgonbold, J.; Lee, K.W. Reliability Verification of Damping Capacity Assessment Through In Vitro Analysis of Implant Micromotion in Peri-implant Bone Loss Model. Int. J. Oral Maxillofac. Implant. 2021, 36, 106–114. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Investigated Item | Number |
|---|---|
| Patients | 38 |
| Age, mean (range) | 66 (36–89) |
| Sex | |
| Male | 20 (53%) |
| Female | 18 (47%) |
| Total implants | 50 |
| Jaw | |
| Maxilla | 23 (46%) |
| Mandible | 27 (54%) |
| Location | |
| Anterior | 4 (8%) |
| Posterior | 46 (92%) |
| Fixture (manufacturer) | |
| LUNA (Shinhung) | 22 (44%) |
| ISⅡ (Neobiotech) | 20 (40%) |
| ISⅢ (Neobiotech) | 8 (16%) |
| Fixture (size) | |
| Length | |
| Short (<8.0 mm) | 6 (12%) |
| Regular (8.0–11.5 mm) | 43 (86%) |
| Long (>11.5 mm) | 1 (2%) |
| Diameter | |
| Narrow (≤3.5 mm) | 1 (2%) |
| Regular (4.0–5.0 mm) | 49 (98%) |
| Wide (>5.0 mm) | 0 |
| Healing abutment (GH) | |
| 3 mm | 4 (8%) |
| 4 mm | 26 (52%) |
| 5 mm | 12 (24%) |
| 6 mm | 7 (14%) |
| 7 mm | 1 (2%) |
| Bone grafting | 21 (42%) |
| Device | Post-op Period | Mean | SD |
|---|---|---|---|
| Periotest M | Op | −4.72 | 2.92 |
| 2 W | −4.25 | 4.37 | |
| 1 M | −4.62 | 3.50 | |
| 2 M | −4.57 | 3.34 | |
| 3 M | −5.29 | 2.84 | |
| Anycheck | Op | 76.10 | 6.89 |
| 2 W | 75.82 | 9.87 | |
| 1 M | 76.40 | 8.42 | |
| 2 M | 76.50 | 7.85 | |
| 3 M | 77.48 | 6.92 |
| Tapping Location | Mean | SD | LSMEAN | SE | p-Value | |
|---|---|---|---|---|---|---|
| Periotest M | both | 0.000 | 0.999 | 0.04322 | 0.07911 | 0.6626 |
| Anycheck | 0.000 | 0.999 | −0.0030 | 0.07911 | ||
| OP | −0.014 | 0.861 | −0.014 | 0.06071 | <0.0001 | |
| 2 W | −0.090 | 1.219 | −0.107 | 0.08685 | ||
| 1 M | −0.005 | 1.025 | −0.037 | 0.07259 | ||
| 2 M | 0.005 | 0.942 | 0.028 | 0.07063 | ||
| 3 M | 0.157 | 0.837 | 0.231 | 0.06275 | ||
| Periotest M | Buccal | 0.000 | 1.000 | 0.021 | 0.1192 | 0.9275 |
| Anycheck | 0.000 | 1.000 | 0.006 | 0.1192 | ||
| OP | −0.078 | 0.933 | −0.078 | 0.09283 | 0.0325 | |
| 2 W | −0.072 | 1.172 | −0.096 | 0.1178 | ||
| 1 M | −0.016 | 1.061 | −0.058 | 0.1053 | ||
| 2 M | 0.086 | 0.875 | 0.099 | 0.08901 | ||
| 3 M | 0.148 | 0.861 | 0.201 | 0.09207 | ||
| Periotest M | Lingual | 0.000 | 1.000 | 0.066 | 0.1058 | 0.5173 |
| Anycheck | 0.000 | 1.000 | −0.024 | 0.1058 | ||
| OP | 0.049 | 0.782 | 0.049 | 0.07777 | 0.0031 | |
| 2 W | −0.108 | 1.270 | −0.120 | 0.1278 | ||
| 1 M | 0.006 | 0.995 | −0.012 | 0.0998 | ||
| 2 M | −0.076 | 1.003 | −0.050 | 0.1093 | ||
| 3 M | 0.165 | 0.819 | 0.238 | 0.08636 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, H.-K.; Lee, S.-J.; Jeong, Y.; Lee, J.-S.; Ryu, J.-J.; Shim, J.-S.; Song, I.-S. Clinical Validation of Dental Implant Stability by Newly Designed Damping Capacity Assessment Device during the Healing Period. Medicina 2022, 58, 1570. https://doi.org/10.3390/medicina58111570
Lim H-K, Lee S-J, Jeong Y, Lee J-S, Ryu J-J, Shim J-S, Song I-S. Clinical Validation of Dental Implant Stability by Newly Designed Damping Capacity Assessment Device during the Healing Period. Medicina. 2022; 58(11):1570. https://doi.org/10.3390/medicina58111570
Chicago/Turabian StyleLim, Ho-Kyung, Sung-Jae Lee, Yujin Jeong, Jong-Seok Lee, Jae-Jun Ryu, Ji-Suk Shim, and In-Seok Song. 2022. "Clinical Validation of Dental Implant Stability by Newly Designed Damping Capacity Assessment Device during the Healing Period" Medicina 58, no. 11: 1570. https://doi.org/10.3390/medicina58111570
APA StyleLim, H.-K., Lee, S.-J., Jeong, Y., Lee, J.-S., Ryu, J.-J., Shim, J.-S., & Song, I.-S. (2022). Clinical Validation of Dental Implant Stability by Newly Designed Damping Capacity Assessment Device during the Healing Period. Medicina, 58(11), 1570. https://doi.org/10.3390/medicina58111570