
Sleep Disorders and Their Associated Factors during the COVID-19 Pandemic: Data from Peruvian Medical Students

 , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Procedures
2.3. Variable Definition
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Population Characteristics
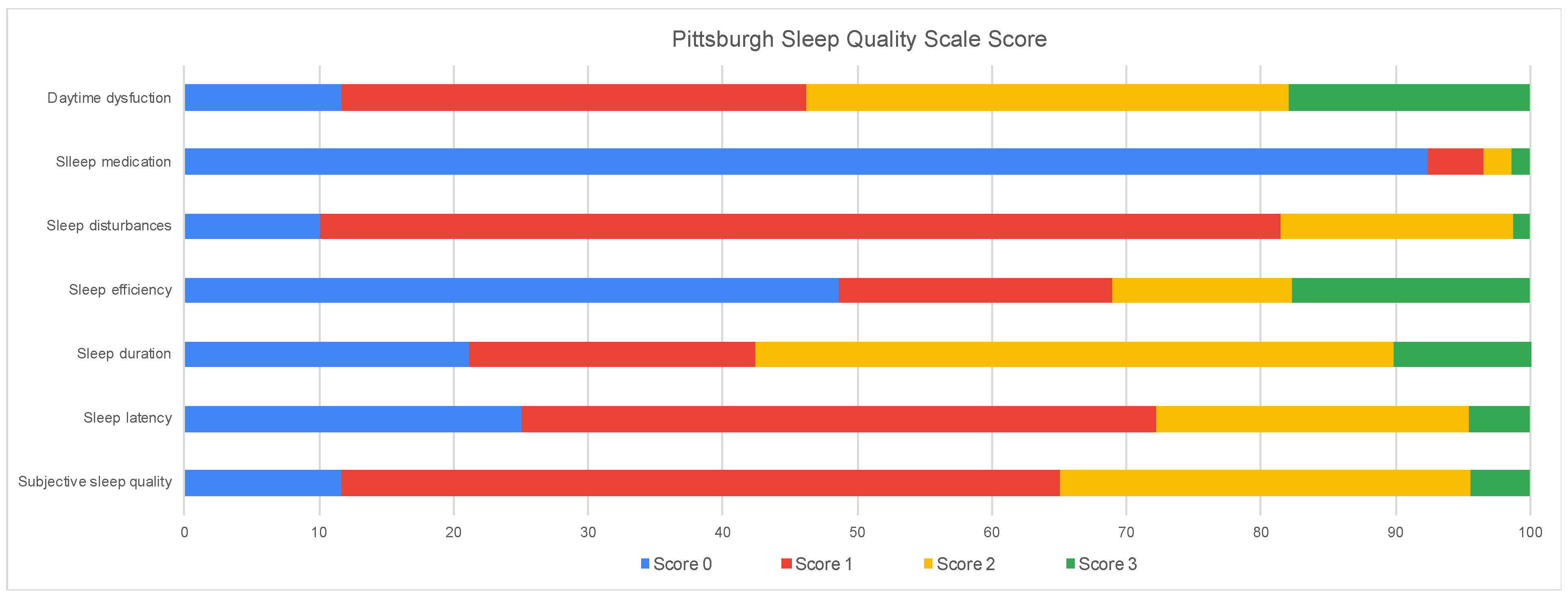
3.2. Distribution of Sleep Quality Score
3.3. Factors Associated with Sleep Quality
4. Discussion
4.1. Sleep Quality
4.2. Nomophobia Associated with Poor Sleep Quality
4.3. Anxiety and Depression Associated with Poor Sleep Quality
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martínez-de-Quel, Ó.; Suárez-Iglesias, D.; López-Flores, M.; Pérez, C.A. Physical activity, dietary habits and sleep quality before and during COVID-19 lockdown: A longitudinal study. Appetite 2021, 158, 105019. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud. Gobierno Oficializa Suspensión del Toque de Queda a Nivel Nacional, el Cual Rige Desde el 31 de Enero. Available online: https://www.gob.pe/institucion/minsa/noticias/580026-gobierno-oficializa-suspension-del-toque-de-queda-a-nivel-nacional-el-cual-rige-desde-el-31-de-enero (accessed on 28 July 2022).
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Chavez, B.; Copaja-Corzo, C.; Rivarola-Hidalgo, M.; Taype-Rondan, Á. Fear of Death in Medical Students from a Peruvian University during the COVID-19 Pandemic. Behav. Sci. 2022, 12, 142. [Google Scholar] [CrossRef]
- Rana, W.; Mukhtar, S.; Mukhtar, S. Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102080. [Google Scholar] [CrossRef]
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2017, 12, 1–22. [Google Scholar] [CrossRef]
- Molla, A.; Wondie, T. Magnitude of Poor Sleep Hygiene Practice and Associated Factors among Medical Students in Ethiopia: A Cross-Sectional Study. Sleep Disord. 2021, 2021, 6611338. [Google Scholar] [CrossRef] [PubMed]
- Surani, A.A.; Zahid, S.; Surani, A.; Ali, S.; Mubeen, M.; Khan, R.H. Sleep quality among medical students of Karachi, Pakistan. J. Pak. Med. Assoc. 2015, 65, 380–382. [Google Scholar] [PubMed]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.D.C.; Hernández-Martínez, A. Sleep Pattern Changes in Nursing Students during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2020, 17, 5222. [Google Scholar] [CrossRef] [PubMed]
- Luciano, F.; Cenacchi, V.; Vegro, V.; Pavei, G. COVID-19 lockdown: Physical activity, sedentary behaviour and sleep in Italian medicine students. Eur. J. Sport Sci. 2021, 21, 1459–1468. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, B.; Acimis, N.M. Sleep Quality in Pamukkale University Students and its relationship with smartphone addiction. Pak. J. Med. Sci. 2021, 37, 206–211. [Google Scholar] [CrossRef]
- Almojali, A.I.; Almalki, S.A.; Alothman, A.S.; Masuadi, E.M.; Alaqeel, M.K. The prevalence and association of stress with sleep quality among medical students. J. Epidemiol. Glob. Health 2017, 7, 169–174. [Google Scholar] [CrossRef]
- Rao, W.W.; Li, W.; Qi, H.; Hong, L.; Chen, C.; Li, C.Y.; Ng, C.H.; Ungvari, G.S.; Xiang, Y.T. Sleep quality in medical students: A comprehensive meta-analysis of observational studies. Sleep Breath. 2020, 24, 1151–1165. [Google Scholar] [CrossRef]
- Copaja-Corzo, C.; Aragón-Ayala, C.J.; Taype-Rondan, A.; Nomotest-Group. Nomophobia and Its Associated Factors in Peruvian Medical Students. Int. J. Environ. Res. Public Health 2022, 19, 5006. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Royuela, A.; Macias, J.A. Propiedades clinimetricas de la versión castellana del cuestionario de Pittsburgh. Vigilia-Sueño 1997, 9, 81–94. [Google Scholar]
- Ministerio de Salud. Atención de Víctimas de Violencia, Derechos de Las Personas: Guía Práctica Para Uso en Servicios de Emergencia y Consulta Externa. Available online: https://www.gob.pe/institucion/minsa/informes-publicaciones/314088-atencion-de-victimas-de-violencia-derechos-de-las-personas-guia-practica-para-uso-en-servicios-de-emergencia-y-consulta-externa (accessed on 28 July 2022).
- Morote, R.; Hjemdal, O.; Martinez Uribe, P.; Corveleyn, J. Psychometric properties of the Resilience Scale for Adults (RSA) and its relationship with life-stress, anxiety and depression in a Hispanic Latin-American community sample. PLoS ONE 2017, 12, e0187954. [Google Scholar] [CrossRef]
- Yildirim, C.; Correia, A.-P. Exploring the Dimensions of Nomophobia: Development and Validation of a Self-Reported Questionnaire. Comput. Hum. Behav. 2015, 49, 130–137. [Google Scholar] [CrossRef]
- León-Mejía, A.; Calvete, E.; Patino-Alonso, C.; Machimbarrena, J.M.; González-Cabrera, J. Cuestionario de Nomofobia (NMP-Q): Estructura Factorial y Puntos de Corte de La Versión Española. Adicciones 2020, 33, 137. [Google Scholar] [CrossRef]
- Del Pielago Meoño, A.F.; Failoc Rojas, V.E.; Plasencia Dueñas, E.A.; Díaz Vélez, C. Calidad de sueño y estilo de aprendizaje en estudiantes de Medicina Humana de la Universidad Nacional Pedro Ruiz Gallo. Acta Médica Peru. 2013, 30, 63–68. [Google Scholar]
- Granados-Carrasco, Z.; Bartra-Aguinaga, A.; Bendezú-Barnuevo, D.; Huamanchumo-Merino, J.; Hurtado-Noblecilla, E.; Jiménez-Flores, J.; León-Jiménez, F.; Chang-Dávila, D. Calidad del sueño en una facultad de medicina de Lambayeque. An. Fac. Med. 2013, 74, 311–314. [Google Scholar] [CrossRef]
- Lim, J.; Dinges, D.F. A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychol. Bull. 2010, 136, 375–389. [Google Scholar] [CrossRef] [PubMed]
- Al-Khani, A.M.; Sarhandi, M.I.; Zaghloul, M.S.; Ewid, M.; Saquib, N. A cross-sectional survey on sleep quality, mental health, and academic performance among medical students in Saudi Arabia. BMC Res. Notes 2019, 12, 665. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.F.; Al-Musa, H.; Al-Amri, H.; Al-Qahtani, A.; Al-Shahrani, M.; Al-Qahtani, M. Sleep Patterns and Predictors of Poor Sleep Quality among Medical Students in King Khalid University, Saudi Arabia. Malays. J. Med. Sci. 2016, 23, 94–102. [Google Scholar] [CrossRef] [PubMed]
- James, B.O.; Omoaregba, J.O.; Igberase, O.O. Prevalence and correlates of poor sleep quality among medical students at a Nigerian university. Ann. Niger. Med. 2011, 5, 1–5. [Google Scholar] [CrossRef]
- Yazdi, Z.; Loukzadeh, Z.; Moghaddam, P.; Jalilolghadr, S. Sleep Hygiene Practices and Their Relation to Sleep Quality in Medical Students of Qazvin University of Medical Sciences. J. Caring Sci. 2016, 5, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, D.; Adhikari, S.P.; Rawal, N.; Budhathoki, P.; Pokharel, S.; Adhikari, Y.; Rokaya, P.; Raut, U. Sleep quality among undergraduate students of a medical college in Nepal during COVID-19 pandemic: An online survey. F1000Research 2021, 10, 505. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.K.; Baharoon, B.S.; Banjar, W.F.; Jar, A.A.; Ashor, R.M.; Aman, A.A.; Al-Ahmadi, J.R. Mobile Phone Addiction and Its Relationship to Sleep Quality and Academic Achievement of Medical Students at King Abdulaziz University, Jeddah, Saudi Arabia. J. Res. Health Sci. 2018, 18, e00420. [Google Scholar]
- Yang, J.; Fu, X.; Liao, X.; Li, Y. Association of problematic smartphone use with poor sleep quality, depression, and anxiety: A systematic review and meta-analysis. Psychiatry Res. 2020, 284, 112686. [Google Scholar] [CrossRef]
- Nowreen, N.; Ahad, F. Effect of smartphone usage on quality of sleep in medical students. Natl. J. Physiol. Pharm. Pharmacol. 2018, 8, 1366. [Google Scholar] [CrossRef]
- Jniene, A.; Errguig, L.; El Hangouche, A.J.; Rkain, H.; Aboudrar, S.; El Ftouh, M.; Dakka, T. Perception of Sleep Disturbances due to Bedtime Use of Blue Light-Emitting Devices and Its Impact on Habits and Sleep Quality among Young Medical Students. BioMed Res. Int. 2019, 2019, 7012350. [Google Scholar] [CrossRef]
- Thomée, S.; Härenstam, A.; Hagberg, M. Mobile phone use and stress, sleep disturbances, and symptoms of depression among young adults—A prospective cohort study. BMC Public Health 2011, 11, 66. [Google Scholar] [CrossRef]
- Christensen, M.A.; Bettencourt, L.; Kaye, L.; Moturu, S.T.; Nguyen, K.T.; Olgin, J.E.; Pletcher, M.J.; Marcus, G.M. Direct Measurements of Smartphone Screen-Time: Relationships with Demographics and Sleep. PLoS ONE 2016, 11, e0165331. [Google Scholar] [CrossRef]
- Riemann, D.; Spiegelhalder, K.; Feige, B.; Voderholzer, U.; Berger, M.; Perlis, M.; Nissen, C. The hyperarousal model of insomnia: A review of the concept and its evidence. Sleep Med. Rev. 2010, 14, 19–31. [Google Scholar] [CrossRef]
- Kalmbach, D.A.; Cuamatzi-Castelan, A.S.; Tonnu, C.V.; Tran, K.M.; Anderson, J.R.; Roth, T.; Drake, C.L. Hyperarousal and sleep reactivity in insomnia: Current insights. Nat. Sci. Sleep 2018, 10, 193–201. [Google Scholar] [CrossRef]
- Bonnet, M.H.; Arand, D.L. Hyperarousal and insomnia. Sleep Med. Rev. 1997, 1, 97–108. [Google Scholar] [CrossRef]
- Saguem, B.N.; Nakhli, J.; Romdhane, I.; Nasr, S.B. Predictors of sleep quality in medical students during COVID-19 confinement. L’encephale 2022, 48, 3–12. [Google Scholar] [CrossRef]
- Feng, G.S.; Chen, J.W.; Yang, X.Z. Study on the status and quality of sleep-related influencing factors in medical college students. Zhonghua Liu Xing Bing Xue Za Zhi 2005, 26, 328–331. (In Chinese) [Google Scholar]
- Perotta, B.; Arantes-Costa, F.M.; Enns, S.C.; Figueiro-Filho, E.A.; Paro, H.; Santos, I.S.; Lorenzi-Filho, G.; Martins, M.A.; Tempski, P.Z. Sleepiness, sleep deprivation, quality of life, mental symptoms and perception of academic environment in medical students. BMC Med. Educ. 2021, 21, 111. [Google Scholar] [CrossRef]
- Ghoreishi, A.; Aghajani, A.H. Sleep quality in Zanjan university medical students. Tehran Univ. Med. J. 2008, 66, 61–67. [Google Scholar]
- Chang, P.P.; Ford, D.E.; Mead, L.A.; Cooper-Patrick, L.; Klag, M.J. Insomnia in young men and subsequent depression. The Johns Hopkins Precursors Study. Am. J. Epidemiol. 1997, 146, 105–114. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Caulet, M.; Priest, R.G.; Guilleminault, C. DSM-IV and ICSD-90 insomnia symptoms and sleep dissatisfaction. Br. J. Psychiatry 1997, 171, 382–388. [Google Scholar] [CrossRef]
- Gibson, R.; Shetty, H.; Carter, M.; Münch, M. Sleeping in a bubble: Factors affecting sleep during New Zealand’s COVID-19 lockdown. Sleep Adv. 2022, 3, zpac017. [Google Scholar] [CrossRef]
- Santini, Z.I.; Koyanagi, A. Loneliness and its association with depressed mood, anxiety symptoms, and sleep problems in Europe during the COVID-19 pandemic. Acta Neuropsychiatr. 2021, 33, 160–163. [Google Scholar] [CrossRef]
- Pesonen, A.K.; Lipsanen, J.; Halonen, R.; Elovainio, M.; Sandman, N.; Mäkelä, J.M.; Antila, M.; Béchard, D.; Ollila, H.M.; Kuula, L. Pandemic Dreams: Network Analysis of Dream Content During the COVID-19 Lockdown. Front. Psychol. 2020, 11, 573961. [Google Scholar] [CrossRef]
- Lavie, P. Sleep disturbances in the wake of traumatic events. N. Engl. J. Med. 2001, 345, 1825–1832. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | n (%) |
|---|---|
| Sex | |
| Female | 1919 (61.1) |
| Male | 1220 (38.9) |
| Age * | 22 (20–24) |
| 18 to 20 | 1086 (34.6) |
| 21 to 23 | 1162 (37.0) |
| 24 to more | 891 (28.4) |
| Have a relationship | |
| Nope | 2168 (69.1) |
| Yes | 971 (30.9) |
| Financing your university | |
| Public | 1544 (49.2) |
| Private | 1595 (50.8) |
| Year of studies | |
| 1st to 3rd | 1609 (51.3) |
| 4th to 6th | 1530 (48.7) |
| Failed a course the previous semester | |
| Nope | 2714 (86.5) |
| Yes | 425 (13.5) |
| Number of brothers | 2 (1–2) |
| None | 264 (8.4) |
| 1 to 2 | 2122 (67.6) |
| More than 3 | 753 (24.0) |
| Do any sports | |
| Nope | 1660 (52.9) |
| Yes | 1479 (47.1) |
| The level of education of the parents is higher technical or university | |
| Mother | 2359 (75.2) |
| Father | 2469 (78.7) |
| How often do you check your cell phone? | |
| 5 min | 360 (11.5) |
| 20 min | 1841 (58.7) |
| 1 h | 598 (19.1) |
| 3 h | 340 (10.8) |
| What part of the day do you use your cell phone? | |
| All time | 411 (13.1) |
| Mornings | 686 (21.9) |
| Afternoon | 934 (29.8) |
| Night | 1108 (35.3) |
| Anxiety (HSCL-25) | |
| Score (Range: 10 to 40 points) * | 15 (12–20) |
| Average score ≥ 1.75 | 1091 (34.8) |
| Depression (HSCL-25) | |
| Score (Range: 15 to 60 points) * | 25 (19–32) |
| Average score ≥ 1.75 | 1343 (42.8) |
| Nomophobia (NMP-Q) | |
| Score (Range: 20 to 140 points) * | 47 (33–69) |
| Tertile 1 | 1047 (33.4) |
| Tertile 2 | 1052 (33.5) |
| Tertile 3 | 1040 (33.1) |
| Sleep quality (PSQI) | |
| Score (Range: 0 to 21 points) * | 6 (5–8) |
| No sleep problem (<5 points) | 714 (22.8) |
| Deserves medical attention (5 to 7 points) | 1361 (43.4) |
| Deserves medical attention and treatment (8 to 14 points) | 1042 (33.2) |
| It is a severe sleep problem (<15 points) | 22 (0.7) |
| Statements | Score (Median ± Interquartile Range) |
|---|---|
| Dimension 1: Subjective sleep quality | |
| How would you rate the quality of your sleep during the last four weeks? | 1 (1–2) |
| Dimension 2: Sleep latency | |
| In the last four weeks, how long did it usually take to fall asleep (fall asleep) at night? (In minutes) | 20 (10–30) |
| In the last four weeks, how long did it usually take to fall asleep (fall asleep) at night? (In hours) | 1 (0–2) |
| Dimension 3: Duration of sleep | |
| In the last four weeks, how many effective hours have you slept per night? (In hours) | 6 (5–7) |
| Dimension 4: Sleep Efficiency | |
| In the past four weeks, write the usual time you went to bed | 24 (1–23) |
| In the last four weeks, what time did you usually get out of bed in the morning and have not gone back to sleep? | 6 (6–8) |
| Dimension 5: Sleep disturbances | |
| In the last four weeks, how many times have you had trouble sleeping because of waking up at night or early in the morning? | 1 (0–2) |
| How many times have you had trouble sleeping for other reasons in the last four weeks? | 0 (0–1) |
| Dimension 6: Use of sleep medications | |
| During the past four weeks, how often have you taken sleeping medicine (prescribed by the doctor or on your own)? | 0 (0–0) |
| Dimension 7: Diurnal dysfunction | |
| During the last four weeks, how often have you felt drowsy (or very sleepy) when driving, eating, working, studying, or doing some other activity? | 1 (0–2) |
| Over the past few weeks, how much trouble have you had staying upbeat or excited about doing your tasks or activities? | 1 (1–2) |
| Characteristic | Participants with Good Sleep Quality (%) | Participants with Poor Sleep Quality (%) | Crude PR (95% CI) | PR Adjusted (95% CI) |
|---|---|---|---|---|
| Sex | ||||
| Male | 861 (70.6) | 359 (29.4) | Ref. | Ref. |
| Female | 1214 (63.3) | 705 (36.7) | 1.24 (1.09–1.40) | 1.07 (0.94–1.22) |
| Age | ||||
| 18 to 20 | 695 (64.0) | 391 (36.0) | Ref. | Ref. |
| 21 to 23 | 757 (65.2) | 405 (34.9) | 0.98 (0.85–1.13) | 1.05 (0.89–1.24) |
| 24 or more | 623 (69.9) | 268 (30.1) | 0.85 (0.73–1.00) | 1.06 (0.88–1.28) |
| Have a relationship | ||||
| Nope | 1415 (65.3) | 753 (34.7) | Ref. | - |
| Yes | 660 (68.0) | 311 (32.0) | 0.92 (0.81–1.05) | - |
| Financing your university | ||||
| Public | 1058 (68.5) | 486 (31.5) | Ref. | - |
| Private | 1017 (63.8) | 578 (36.2) | 1.16 (0.99–1.35) | - |
| Year of studies | ||||
| 1st to 3rd | 1025 (63.7) | 584 (36.3) | Ref. | Ref. |
| 4th to 6th | 1050 (68.6) | 480 (31.4) | 0.87 (0.77–0.98) | 0.96 (0.83–1.12) |
| Failed a course the previous semester | ||||
| Nope | 1825 (67.2) | 889 (32.8) | Ref. | Ref. |
| Yes | 250 (58.8) | 175 (41.2) | 1.26 (1.07–1.48) | 1.16 (0.98–1.37) |
| Number of brothers | ||||
| None | 161 (61.0) | 103 (39.0) | Ref. | - |
| 1 to 2 | 1405 (66.2) | 717 (33.8) | 0.87 (0.71–1.07) | - |
| More than 3 | 509 (67.6) | 244 (32.4) | 0.84 (0.66–1.06) | - |
| Do any sports | ||||
| Nope | 1032 (62.2) | 628 (37.8) | Ref. | Ref. |
| Yes | 1043 (70.5) | 436 (29.5) | 0.77 (0.69–0.88) | 0.94 (0.82–1.06) |
| His mother’s educational background is higher technical or university | ||||
| Nope | 552 (70.8) | 228 (29.2) | Ref. | - |
| Yes | 1523 (64.6) | 836 (35.4) | 1.19 (1.03–1.39) | - |
| His father’s educational background is higher technical or university | ||||
| Nope | 458 (68.4) | 212 (31.6) | Ref. | - |
| Yes | 1617 (65.5) | 852 (34.5) | 1.07 (0.92–1.25) | - |
| How often do you check your cell phone? | ||||
| 5 min | 200 (55.6) | 160 (44.4) | Ref. | - |
| 20 min | 1213 (65.9) | 628 (34.1) | 0.77 (0.65–0.92) | - |
| 1 h | 419 (70.1) | 179 (29.9) | 0.68 (0.55–0.85) | - |
| 3 h | 243 (71.5) | 97 (28.5) | 0.65 (0.51–0.84) | - |
| What part of the day do you use your cell phone? | ||||
| All time | 545 (58.4) | 389 (41.7) | Ref. | Ref. |
| Morning | 275 (66.9) | 136 (33.1) | 0.79 (0.65–0.96) | 0.91 (0.75–1.11) |
| Afternoon | 486 (70.9) | 200 (29.2) | 0.70 (0.59–0.83) | 0.81 (0.68–0.97) |
| Night | 769 (69.4) | 339 (30.6) | 0.74 (0.64–0.86) | 0.87 (0.75–1.01) |
| Anxiety (HSCL-25) | ||||
| Average score < 1.75 | 1589 (77.6) | 459 (22.4) | Ref. | Ref. |
| Average score ≥ 1.75 | 486 (44.6) | 605 (55.5) | 2.47 (2.19–2.79) | 1.48 (1.27–1.72) |
| Depression (HSCL-25) | ||||
| Average score < 1.75 | 1454 (81.0) | 342 (19.0) | Ref. | Ref. |
| Average score ≥ 1.75 | 621 (46.2) | 722 (53.8) | 2.82 (2.48–3.21) | 2.03 (1.72–2.39) |
| Nomophobia (NMP-Q) | ||||
| Tertile 1 | 801 (76.5) | 246 (23.5) | Ref. | Ref. |
| Tertile 2 | 694 (66.0) | 358 (34.0) | 1.45 (1.23–1.70) | 1.14 (0.97–1.35) |
| Tertile 3 | 580 (55.8) | 460 (44.2) | 1.87 (1.60–2.19) | 1.28 (1.09–1.51) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Copaja-Corzo, C.; Miranda-Chavez, B.; Vizcarra-Jiménez, D.; Hueda-Zavaleta, M.; Rivarola-Hidalgo, M.; Parihuana-Travezaño, E.G.; Taype-Rondan, A. Sleep Disorders and Their Associated Factors during the COVID-19 Pandemic: Data from Peruvian Medical Students. Medicina 2022, 58, 1325. https://doi.org/10.3390/medicina58101325
Copaja-Corzo C, Miranda-Chavez B, Vizcarra-Jiménez D, Hueda-Zavaleta M, Rivarola-Hidalgo M, Parihuana-Travezaño EG, Taype-Rondan A. Sleep Disorders and Their Associated Factors during the COVID-19 Pandemic: Data from Peruvian Medical Students. Medicina. 2022; 58(10):1325. https://doi.org/10.3390/medicina58101325
Chicago/Turabian StyleCopaja-Corzo, Cesar, Brayan Miranda-Chavez, Dariela Vizcarra-Jiménez, Miguel Hueda-Zavaleta, Marco Rivarola-Hidalgo, Edgar G. Parihuana-Travezaño, and Alvaro Taype-Rondan. 2022. "Sleep Disorders and Their Associated Factors during the COVID-19 Pandemic: Data from Peruvian Medical Students" Medicina 58, no. 10: 1325. https://doi.org/10.3390/medicina58101325
APA StyleCopaja-Corzo, C., Miranda-Chavez, B., Vizcarra-Jiménez, D., Hueda-Zavaleta, M., Rivarola-Hidalgo, M., Parihuana-Travezaño, E. G., & Taype-Rondan, A. (2022). Sleep Disorders and Their Associated Factors during the COVID-19 Pandemic: Data from Peruvian Medical Students. Medicina, 58(10), 1325. https://doi.org/10.3390/medicina58101325