
Syncope Time Frames for Adverse Events after Emergency Department Presentation: An Individual Patient Data Meta-Analysis

 ,
,  , ,
on behalf of the SYNERGI (SYNcope Expert Research Group International)
, ,
on behalf of the SYNERGI (SYNcope Expert Research Group International)
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Outcomes and Definitions
2.3. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
3.2. Data Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.-C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martín, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef]
- Shen, W.-K.; Sheldon, R.S.; Benditt, D.G.; Cohen, M.I.; Forman, D.E.; Goldberger, Z.D.; Grubb, B.P.; Hamdan, M.H.; Krahn, A.D.; Link, M.S.; et al. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2017, 136, e60–e122. [Google Scholar] [CrossRef] [PubMed]
- Costantino, G.; Casazza, G.; Reed, M.; Bossi, I.; Sun, B.; Del Rosso, A.; Ungar, A.; Grossman, S.; D’Ascenzo, F.; Quinn, J.; et al. Syncope Risk Stratification Tools vs. Clinical Judgment: An Individual Patient Data Meta-analysis. Am. J. Med. 2014, 127, 1126.e13–1126.e25. [Google Scholar] [CrossRef]
- Costantino, G.; Sun, B.C.; Barbic, F.; Bossi, I.; Casazza, G.; Dipaola, F.; McDermott, D.; Quinn, J.; Reed, M.J.; Sheldon, R.S.; et al. Syncope clinical management in the emergency department: A consensus from the first international workshop on syncope risk stratification in the emergency department. Eur. Heart J. 2016, 37, 1493–1498. [Google Scholar] [CrossRef] [Green Version]
- Dipaola, F.; Costantino, G.; Perego, F.; Borella, M.; Galli, A.; Cantoni, G.; Barbic, F.; Casella, F.; Duca, P.G.; Furlan, R. San Francisco Syncope Rule, Osservatorio Epidemiologico sulla Sincope nel Lazio risk score, and clinical judgment in the assessment of short-term outcome of syncope. Am. J. Emerg. Med. 2010, 28, 432–439. [Google Scholar] [CrossRef]
- Solbiati, M.; Bozzano, V.; Barbic, F.; Casazza, G.; Dipaola, F.; Quinn, J.V.; Reed, M.J.; Sheldon, R.S.; Shen, W.-K.; Sun, B.C.; et al. Outcomes in syncope research: A systematic review and critical appraisal. Intern. Emerg. Med. 2018, 13, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Thiruganasambandamoorthy, V.; Rowe, B.H.; Sivilotti, M.L.A.; McRae, A.D.; Arcot, K.; Nemnom, M.-J.; Huang, L.; Mukarram, M.; Krahn, A.D.; Wells, G.A.; et al. Duration of Electrocardiographic Monitoring of Emergency Department Patients With Syncope. Circulation 2019, 139, 1396–1406. [Google Scholar] [CrossRef]
- Kaul, P.; Tran, D.T.; Sandhu, R.K.; Solbiati, M.; Costantino, G.; Sheldon, R.S. Lack of benefit from hospitalization in patients with syncope: A propensity analysis. J. Am. Coll. Emerg. Physicians Open 2020, 1, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.J.; Mukarram, M.; Ghaedi, B.; Sivilotti, M.L.A.; Le Sage, N.; Yan, J.W.; Huang, P.; Hegdekar, M.; Mercier, E.; Nemnom, M.-J.; et al. Benefit of hospital admission for detecting serious adverse events among emergency department patients with syncope: A propensity-score-matched analysis of a multicentre prospective cohort. CMAJ 2020, 192, E1198–E1205. [Google Scholar] [CrossRef]
- Costantino, G.; Dipaola, F.; Solbiati, M.; Bulgheroni, M.; Barbic, F.; Furlan, R. Is hospital admission valuable in managing syncope? Results from the STePS study. Cardiol. J. 2014, 21, 606–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantino, G.; Perego, F.; Dipaola, F.; Borella, M.; Galli, A.; Cantoni, G.; Dell’Orto, S.; Dassi, S.; Filardo, N.; Duca, P.G.; et al. Short- and long-term prognosis of syncope, risk factors, and role of hospital admission: Results from the STePS (Short-Term Prognosis of Syncope) study. J. Am. Coll. Cardiol. 2008, 51, 276–283. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.C.; Thiruganasambandamoorthy, V.; Cruz, J.D. Standardized reporting guidelines for emergency department syncope risk-stratification research. Acad. Emerg. Med. 2012, 19, 694–702. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.C.; Costantino, G.; Barbic, F.; Bossi, I.; Casazza, G.; Dipaola, F.; McDermott, D.; Quinn, J.; Reed, M.; Sheldon, R.S.; et al. Priorities for Emergency Department Syncope Research. Ann. Emerg. Med. 2014, 64, 649–655.e2. [Google Scholar] [CrossRef] [Green Version]
- Solbiati, M.; Casazza, G.; Dipaola, F.; Rusconi, A.M.; Cernuschi, G.; Barbic, F.; Montano, N.; Sheldon, R.S.; Furlan, R.; Costantino, G. Syncope recurrence and mortality: A systematic review. Europace 2015, 17, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodon, J.; Martínez-Alday, J.; Barón-Esquivias, G.; Martín, A.; García-Civera, R.; Del Arco, C.; Cano-Gonzalez, A.; Moya-Mitjans, A. Prognostic value of the electrocardiogram in patients with syncope: Data from the group for syncope study in the emergency room (GESINUR). Heart Rhythm 2014, 11, 2035–2044. [Google Scholar] [CrossRef]
- Reed, M.J.; Henderson, S.S.; Newby, D.E.; Gray, A.J. One-year prognosis after syncope and the failure of the ROSE decision instrument to predict one-year adverse events. Ann. Emerg. Med. 2011, 58, 250–256. [Google Scholar] [CrossRef]
- Ungar, A.; Del Rosso, A.; Giada, F.; Bartoletti, A.; Furlan, R.; Quartieri, F.; Lagi, A.; Morrione, A.; Mussi, C.; Lunati, M.; et al. Early and late outcome of treated patients referred for syncope to emergency department: The EGSYS 2 follow-up study. Eur. Heart J. 2010, 31, 2021–2026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, B.C.; Mangione, C.M.; Merchant, G.; Weiss, T.; Shlamovitz, G.Z.; Zargaraff, G.; Shiraga, S.; Hoffman, J.R.; Mower, W.R. External validation of the San Francisco Syncope Rule. Ann. Emerg. Med. 2007, 49, 420–427.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Numeroso, F.; Mossini, G.; Giovanelli, M.; Lippi, G.; Cervellin, G. Short-term Prognosis and Current Management of Syncopal Patients at Intermediate Risk: Results from the IRiS (Intermediate-Risk Syncope) Study. Acad. Emerg. Med. 2016, 23, 941–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiruganasambandamoorthy, V.; Kwong, K.; Wells, G.A.; Sivilotti, M.L.A.; Mukarram, M.; Rowe, B.H.; Lang, E.; Perry, J.J.; Sheldon, R.; Stiell, I.G.; et al. Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope. Can. Med. Assoc. J. 2016, 188, E289–E298. [Google Scholar] [CrossRef] [Green Version]
- Solbiati, M.; Dipaola, F.; Villa, P.; Seghezzi, S.; Casagranda, I.; Rabajoli, F.; Fiorini, E.; Porta, L.; Casazza, G.; Voza, A.; et al. Predictive Accuracy of Electrocardiographic Monitoring of Patients With Syncope in the Emergency Department: The SyMoNE Multicenter Study. Acad. Emerg. Med. 2020, 27, 15–23. [Google Scholar] [CrossRef]
- Probst, M.A.; Gibson, T.; Weiss, R.E.; Yagapen, A.N.; Malveau, S.E.; Adler, D.H.; Bastani, A.; Baugh, C.W.; Caterino, J.M.; Clark, C.L.; et al. Risk Stratification of Older Adults Who Present to the Emergency Department With Syncope: The FAINT Score. Ann. Emerg. Med. 2019, 75, 147–158. [Google Scholar] [CrossRef]
- Solbiati, M.; Talerico, G.; Villa, P.; Dipaola, F.; Furlan, R.; Furlan, L.; Fiorelli, E.M.; Rabajoli, F.; Casagranda, I.; Cazzola, K.; et al. Multicentre external validation of the Canadian Syncope Risk Score to predict adverse events and comparison with clinical judgement. Emerg. Med. J. 2021, 38, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Leafloor, C.W.; Hong, P.J.; Mukarram, M.; Sikora, L.; Elliott, J.; Thiruganasambandamoorthy, V. Long-term outcomes in syncope patients presenting to the emergency department: A systematic review. CJEM 2020, 22, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantino, G.; Ruwald, M.H.; Quinn, J.; Camargo, C.A.; Dalgaard, F.; Gislason, G.; Goto, T.; Hasegawa, K.; Kaul, P.; Montano, N.; et al. Prevalence of Pulmonary Embolism in Patients With Syncope. JAMA Intern. Med. 2018, 178, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, W.K.; Decker, W.W.; Smars, P.A.; Goyal, D.G.; Walker, A.E.; Hodge, D.O.; Trusty, J.M.; Brekke, K.M.; Jahangir, A.; Brady, P.A.; et al. Syncope Evaluation in the Emergency Department Study (SEEDS): A multidisciplinary approach to syncope management. Circulation 2004, 110, 3636–3645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, B.C.; McCreath, H.; Liang, L.-J.; Bohan, S.; Baugh, C.; Ragsdale, L.; Henderson, S.O.; Clark, C.; Bastani, A.; Keeler, E.; et al. Randomized clinical trial of an emergency department observation syncope protocol versus routine inpatient admission. Ann. Emerg. Med. 2014, 64, 167–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Study | N of Patients | Mean Age (SD) (Years) | N of Females (%) | N of Admitted (%) |
|---|---|---|---|---|
| Sun_2007 | 312 | 56 (24) | 179 (57) | 182 (58) |
| Costantino_2008 | 689 | 64 (18) | 386 (56) | 236 (34) |
| Ungar_2010 | 371 | 66 (21) | 168 (45) | 144 (39) |
| Reed_2011 | 1100 | 63 (22) | 587 (53) | 538 (49) |
| Pérez-Rodon_2014 | 616 | 57 (20) | 259 (42) | 154 (25) |
| Numeroso_2016 | 347 | 73 (14) | 162 (47) | 157 (45) |
| Thiruganasambandamoorthy_2016 | 6454 | 53 (23) | 3526 (55) | 789 (12) |
| Solbiati_2020 | 345 | 65 (20) | 171 (50) | 102 (30) |
| Probst_2020 | 2035 | 73 (9) | 989 (49) | 1682 (83) |
| N of Studies | N of Patients with Events | N of Patients | Pooled Rate (%) | 95% CI (%) | I2 (%) | |
|---|---|---|---|---|---|---|
| 24 h | 8 | 545 | 11,653 | 5.1 | 3.4–7.7 | 94 |
| 72 h | 7 | 602 | 10,553 | 7.0 | 4.9–9.9 | 93 |
| 7–10 days | 8 | 766 | 11,284 | 8.4 | 6.2–11.3 | 94 |
| 1 month | 8 | 902 | 11,175 | 10.3 | 7.8–13.3 | 93 |
| 1 year | 5 | 599 | 2917 | 21.3 | 15.8–28.0 | 94 |
| N of Studies | N of Events | N of Patients | Pooled Rate (%) | 95% CI (%) | I2 (%) | ||
|---|---|---|---|---|---|---|---|
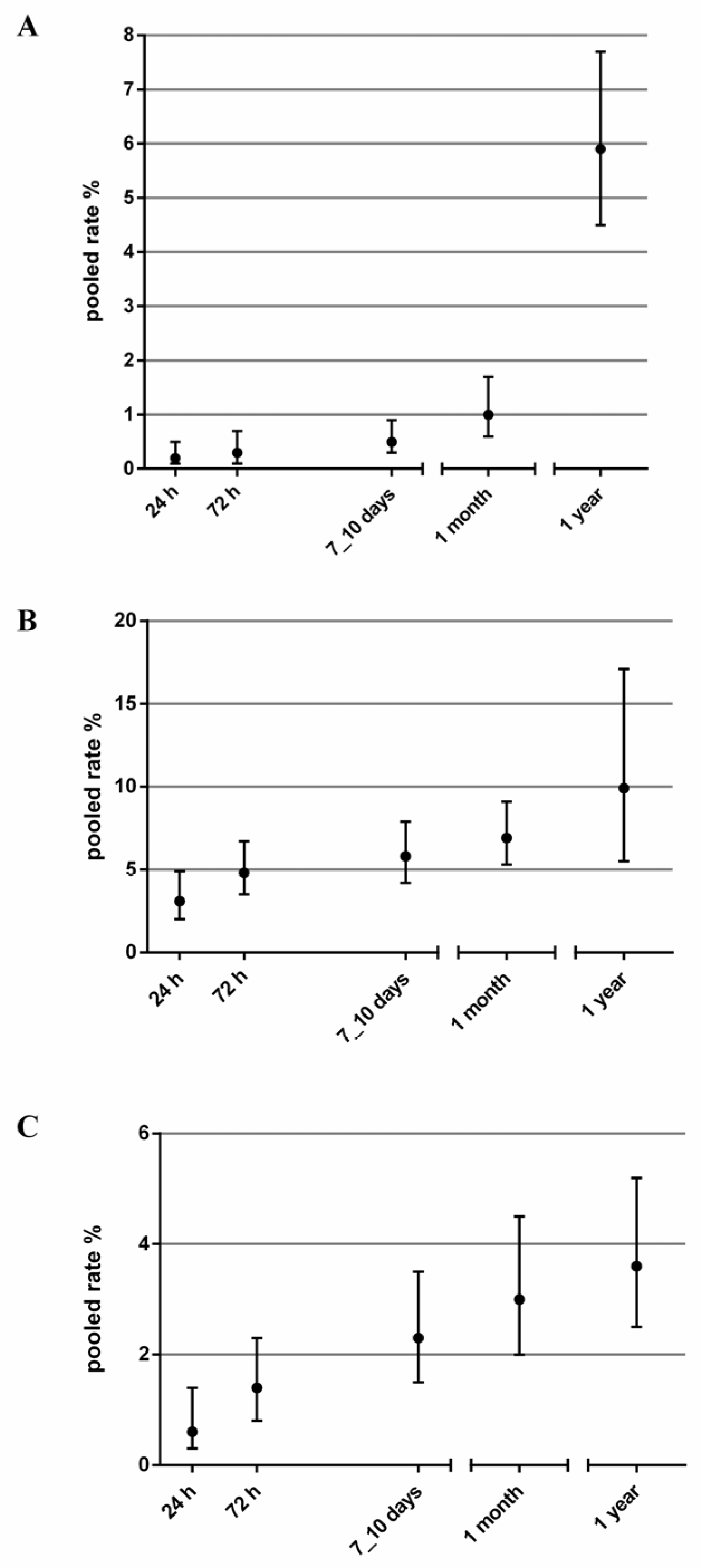
| Death | |||||||
| 24 h | 8 | 13 | 11,653 | 0.2 | 0.1–0.5 | 62 | |
| 72 h | 7 | 19 | 10,553 | 0.3 | 0.1–0.7 | 72 | |
| 7–10 days | 8 | 40 | 11,284 | 0.5 | 0.3–0.9 | 69 | |
| 1 month | 8 | 81 | 11,175 | 1.0 | 0.6–1.7 | 80 | |
| 1 year | 5 | 177 | 2917 | 5.9 | 4.5–7.7 | 66 | |
| Arrhythmia | |||||||
| 24 h | 8 | 388 | 11,653 | 3.1 | 2.0–4.9 | 91 | |
| 72 h | 7 | 450 | 10,553 | 4.8 | 3.5–6.7 | 88 | |
| 7–10 days | 8 | 582 | 11,284 | 5.8 | 4.2–7.9 | 91 | |
| 1 month | 8 | 676 | 11,175 | 6.9 | 5.3–9.1 | 90 | |
| 1 year | 5 | 282 | 2917 | 9.9 | 5.5–17.1 | 96 | |
| PM or ICD implant | |||||||
| 24 h | 6 | 86 | 10,593 | 0.6 | 0.3–1.4 | 78 | |
| 72 h | 5 | 123 | 9493 | 1.4 | 0.8–2.3 | 79 | |
| 7–10 days | 7 | 228 | 10,913 | 2.3 | 1.5–3.5 | 87 | |
| 1 month | 7 | 273 | 10,804 | 3.0 | 2.0–4.5 | 89 | |
| 1 year | 5 | 107 | 2917 | 3.6 | 2.5–5.2 | 73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furlan, L.; Trombetta, L.; Casazza, G.; Dipaola, F.; Furlan, R.; Marta, C.; Numeroso, F.; Pérez-Rodon, J.; Quinn, J.V.; Reed, M.J.; et al. Syncope Time Frames for Adverse Events after Emergency Department Presentation: An Individual Patient Data Meta-Analysis. Medicina 2021, 57, 1235. https://doi.org/10.3390/medicina57111235
Furlan L, Trombetta L, Casazza G, Dipaola F, Furlan R, Marta C, Numeroso F, Pérez-Rodon J, Quinn JV, Reed MJ, et al. Syncope Time Frames for Adverse Events after Emergency Department Presentation: An Individual Patient Data Meta-Analysis. Medicina. 2021; 57(11):1235. https://doi.org/10.3390/medicina57111235
Chicago/Turabian StyleFurlan, Ludovico, Lucia Trombetta, Giovanni Casazza, Franca Dipaola, Raffaello Furlan, Chiara Marta, Filippo Numeroso, Jordi Pérez-Rodon, James V. Quinn, Matthew J. Reed, and et al. 2021. "Syncope Time Frames for Adverse Events after Emergency Department Presentation: An Individual Patient Data Meta-Analysis" Medicina 57, no. 11: 1235. https://doi.org/10.3390/medicina57111235
APA StyleFurlan, L., Trombetta, L., Casazza, G., Dipaola, F., Furlan, R., Marta, C., Numeroso, F., Pérez-Rodon, J., Quinn, J. V., Reed, M. J., Sheldon, R. S., Shen, W.-K., Sun, B. C., Thiruganasambandamoorthy, V., Ungar, A., Costantino, G., & Solbiati, M., on behalf of the SYNERGI (SYNcope Expert Research Group International). (2021). Syncope Time Frames for Adverse Events after Emergency Department Presentation: An Individual Patient Data Meta-Analysis. Medicina, 57(11), 1235. https://doi.org/10.3390/medicina57111235