
L3 Skeletal Muscle Index Dynamics in Patients with HCV-Related Compensated Cirrhosis Following Sustained Virological Response after Direct Acting Antiviral Treatment

 ,
,  ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Scanning Protocols
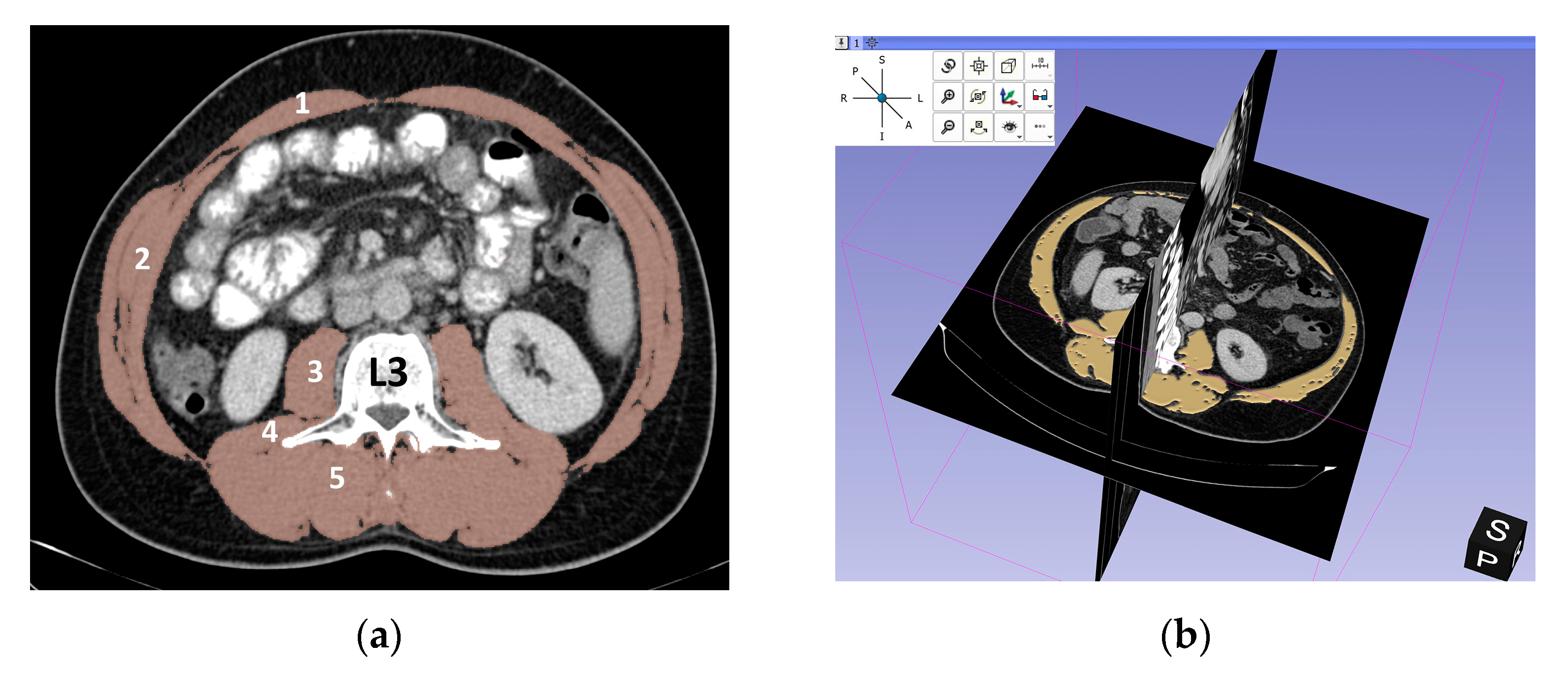
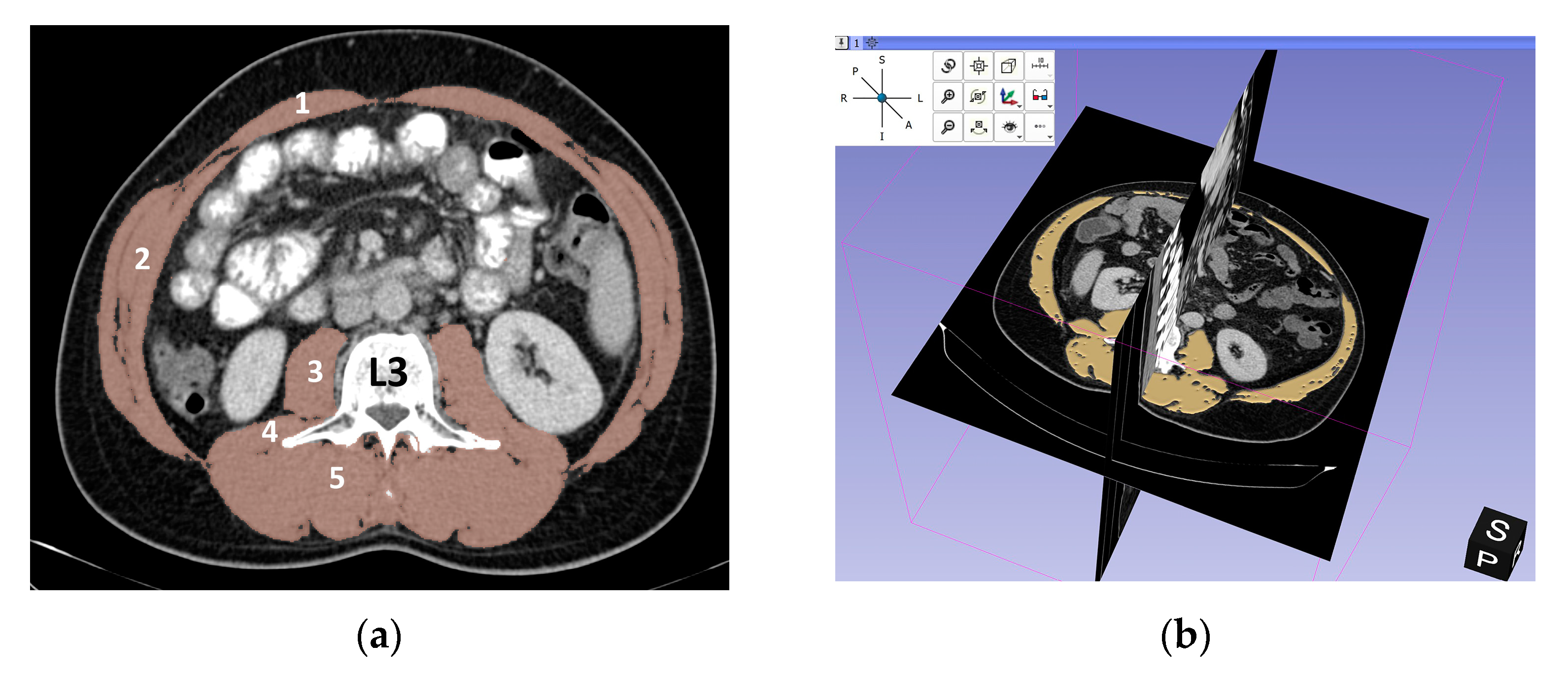
2.3. Assessment of L3-SMI (Skeletal Muscle Index)
2.4. Statistical Analysis
3. Results
3.1. Baseline Data
3.2. Comparison of Baseline Characteristics between Patients with Low L3-SMI and Normal L3-SMI
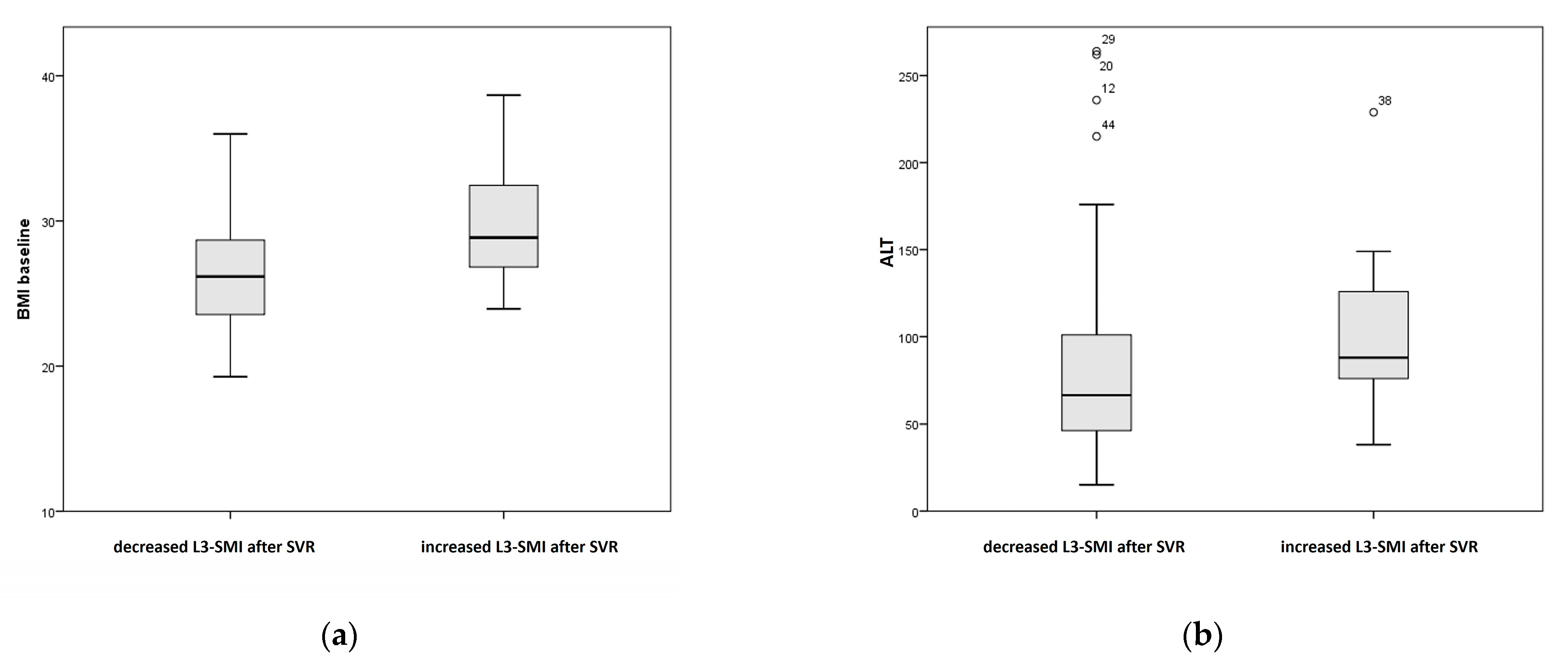
3.3. Comparison of Baseline Characteristics between Patients with Decreased L3-SMI and with Increased L3-SMI Assessed after Sustained Virological Response (SVR)
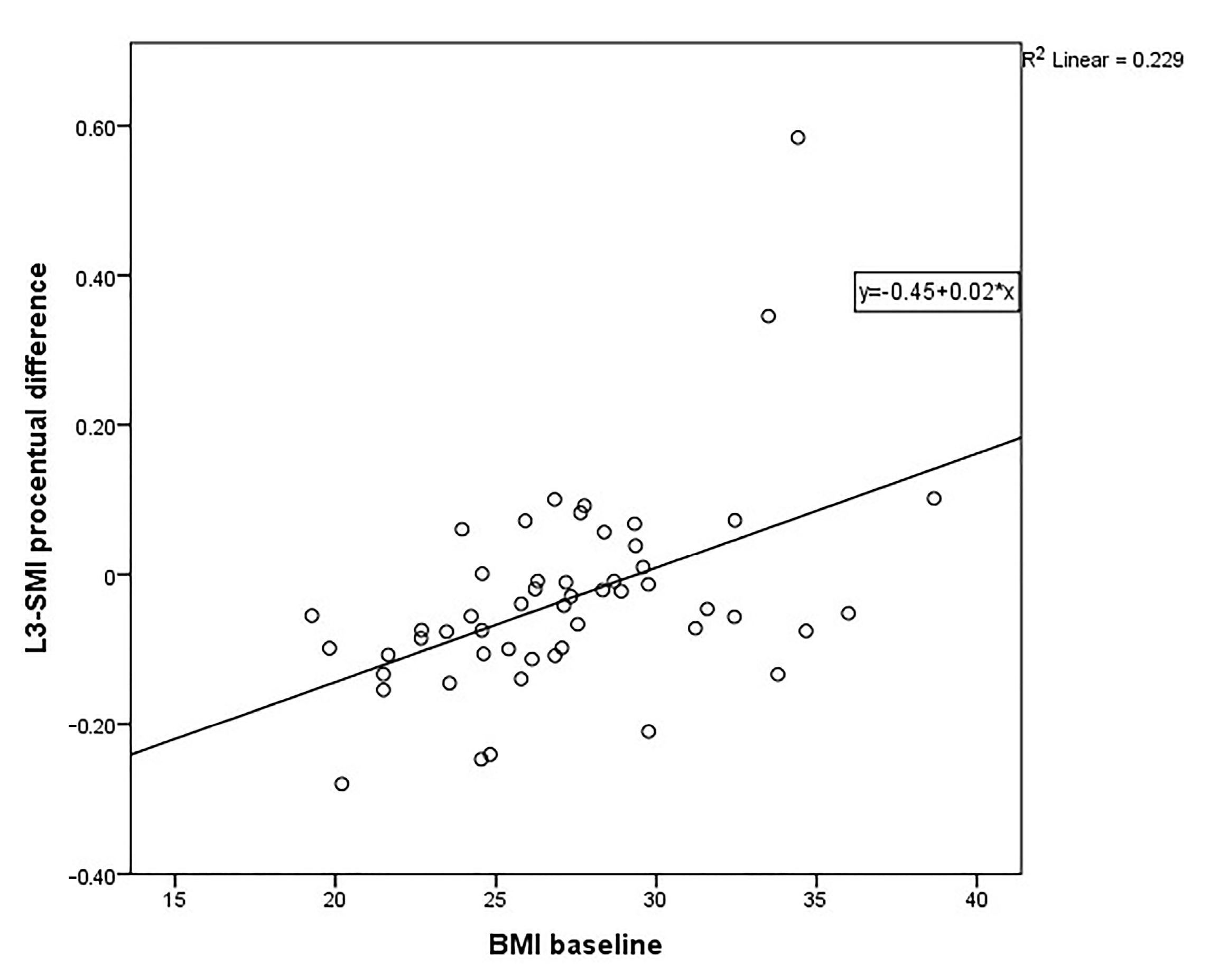
3.4. Linear Regression Model
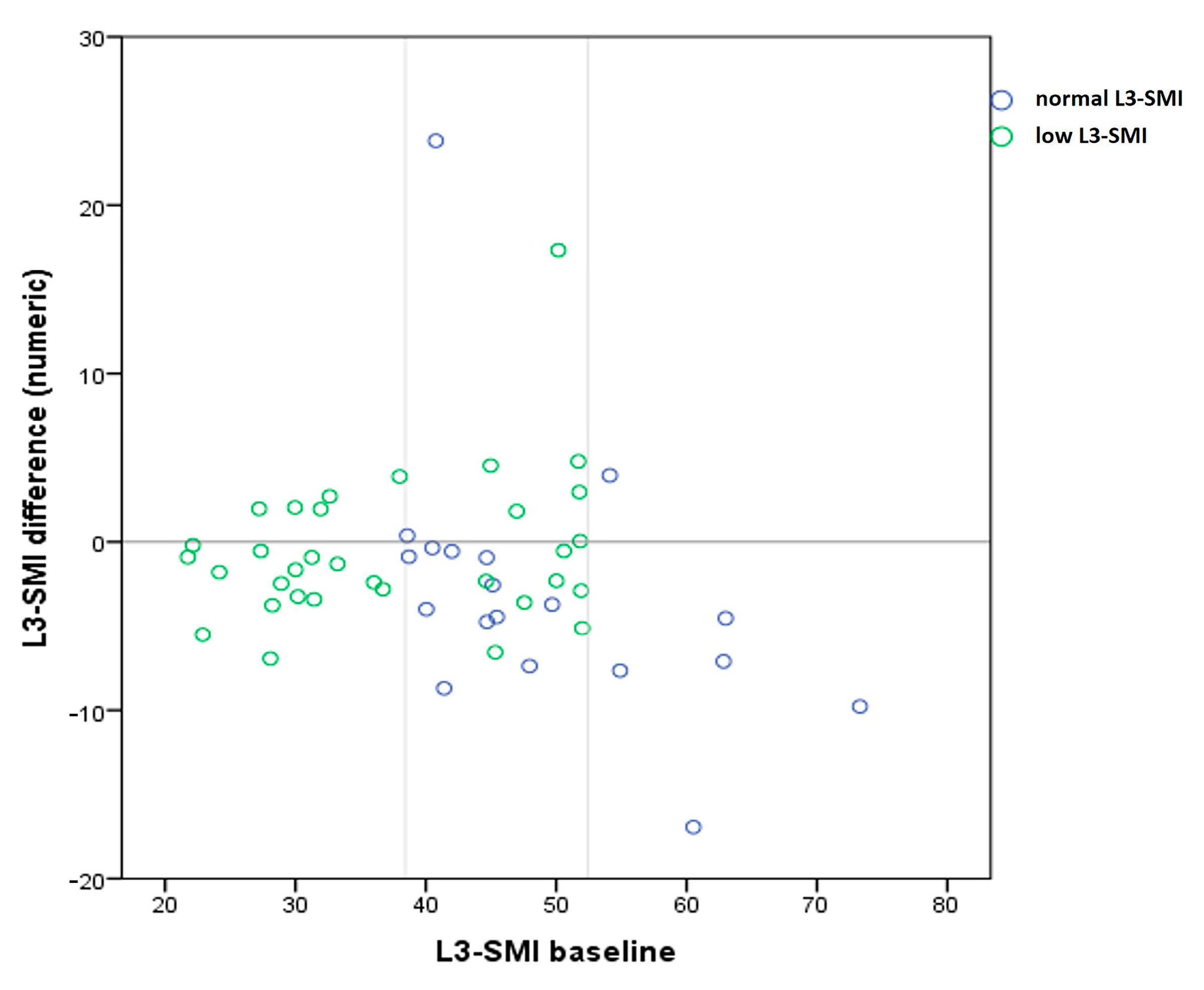
3.5. Comparison of Muscle Mass Dynamics after SVR between Groups with Low L3-SMI and Normal L3-SMI at Baseline
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponziani, F.R.; Gasbarrini, A. Sarcopenia in Patients with Advanced Liver Disease. Curr. Protein Pept. Sci. 2018, 19, 681–691. [Google Scholar] [CrossRef]
- Kim, H.Y.; Jang, J.W. Sarcopenia in the prognosis of cirrhosis: Going beyond the MELD score. World J. Gastroenterol. 2015, 21, 7637–7647. [Google Scholar] [CrossRef]
- Montano-Loza, A.J.; Duarte-Rojo, A.; Meza-Junco, J.; Baracos, V.E.; Sawyer, M.B.; Pang, J.X.; Beaumont, C.; Esfandiari, N.; Myers, R.P. Inclusion of Sarcopenia Within MELD (MELD-Sarcopenia) and the Prediction of Mortality in Patients with Cirrhosis. Clin. Transl. Gastroenterol. 2015, 6, e102. [Google Scholar] [CrossRef]
- Mauro, E.; Crespo, G.; Martinez-Garmendia, A.; Gutierrez-Acevedo, M.N.; Diaz, J.M.; Saidman, J.; Bermudez, C.; Ortiz-Patron, J.; Garcia-Olveira, L.; Zalazar, F. Cystatin C and Sarcopenia Predict Acute on Chronic Liver Failure Development and Mortality in Patients on the Liver Transplant Waiting List. Transplantation 2020, 104, e188–e198. [Google Scholar] [CrossRef]
- DiMartini, A.; Cruz, R.J., Jr.; Dew, M.A.; Myaskovsky, L.; Goodpaster, B.; Fox, K.; Kim, K.H.; Fontes, P. Muscle mass predicts outcomes following liver transplantation. Liver Transpl. 2013, 19, 1172–1180. [Google Scholar] [CrossRef] [Green Version]
- Dasarathy, S.; Merli, M. Sarcopenia from mechanism to diagnosis and treatment in liver disease. J. Hepatol. 2016, 65, 1232–1244. [Google Scholar] [CrossRef] [Green Version]
- Dasarathy, S. Consilience in sarcopenia of cirrhosis. J. Cachexia Sarcopenia Muscle 2012, 3, 225–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majumdar, A.; Kitson, M.T.; Roberts, S.K. Systematic review: Current concepts and challenges for the direct-acting antiviral era in hepatitis C cirrhosis. Aliment. Pharmacol. Ther. 2016, 43, 1276–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poynard, T.; Moussalli, J.; Munteanu, M.; Thabut, D.; Lebray, P.; Rudler, M.; Ngo, Y.; Thibault, V.; Mkada, H.; Charlotte, F. FibroFrance-GHPS group. Slow regression of liver fibrosis presumed by repeated biomarkers after virological cure in patients with chronic hepatitis C. J. Hepatol. 2013, 59, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, M.; Gow, P.J.; Grossmann, M.; Angus, P.W. Review article: Sarcopenia in cirrhosis—Aetiology, implications and potential therapeutic interventions. Aliment. Pharmacol Ther. 2016, 43, 765–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paternostro, R.; Lampichler, K.; Bardach, C.; Asenbaum, U.; Landler, C.; Bauer, D.; Mandorfer, M.; Schwarzer, R.; Trauner, M.; Reiberger, T.; et al. The value of different CT-based methods for diagnosing low muscle mass and predicting mortality in patients with cirrhosis. Liver Int. 2019, 39, 2374–2385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutin, R.D.; Yao, L.; Canter, R.J.; Lenchik, L. Sarcopenia: Current Concepts and Imaging Implications. Am. J. Roentgenol. 2015, 205, W255–W266. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Wang, C.W.; Lai, J.C.; Dasarathy, S.; Kappus, M.R.; Dunn, M.A.; Carey, E.J.; Montano-Loza, A.J. Poor performance of psoas muscle index for identification of patients with higher waitlist mortality risk in cirrhosis. J. Cachexia Sarcopenia Muscle. 2018, 9, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- 3D Slicer Image Computing Platform 3D Slicer. Available online: https://www.slicer.org/ (accessed on 20 September 2021).
- Van Vugt, J.L.A.; Levolger, S.; de Bruin, R.W.F.; van Rosmalen, J.; Metselaar, H.J.; IJzermans, J.N.M. Systematic Review and Meta-Analysis of the Impact of Computed Tomography-Assessed Skeletal Muscle Mass on Outcome in Patients Awaiting or Undergoing Liver Transplantation. Am. J. Transplant. 2016, 16, 2277–2292. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, J. Skeletal muscle abnormalities and outcomes after liver transplantation. Liver Transplant. 2014, 20, 1293–1295. [Google Scholar] [CrossRef]
- Kim, G.; Kang, S.H.; Kim, M.Y.; Baik, S.K. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186990. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Wang, X.; Xie, H.; Zheng, S.; Wu, X.; Zhu, X.; Zhang, X.; Xue, S.; Li, H.; Hong, W. Sex differences in the prevalence and adverse outcomes of sarcopenia and sarcopenic obesity in community dwelling elderly in East China using the AWGS criteria. BMC Endocr. Disord. 2019, 19, 109. [Google Scholar] [CrossRef]
- Chen, Z.; Li, W.-Y.; Ho, M.; Chau, P.-H. The Prevalence of Sarcopenia in Chinese Older Adults: Meta-Analysis and Meta-Regression. Nutrients 2021, 13, 1441. [Google Scholar] [CrossRef]
- Merli, M.; Riggio, O.; Dally, L. Does malnutrition affect survival in cirrhosis? PINC (Policentrica Italiana Nutrizione Cirrosi). Hepatology 1996, 23, 1041–1046. [Google Scholar] [CrossRef]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta-analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 21. [Google Scholar] [CrossRef] [Green Version]
- Stevens, L.A.; Coresh, J.; Greene, T.; Levey, A.S. Assessing kidney function-measured and estimated glomerular filtration rate. N. Engl. J. Med. 2006, 23, 2473–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakamori, R.; Yamada, R.; Shinkai, K.; Doi, A.; Tahata, Y.; Shigekawa, M.; Kodama, T.; Hikita, H.; Yamada, T.; Tatsumi, T.; et al. Improvement of Skeletal Muscle Mass after Ledipasvir and Sofosbuvir Treatment for Hepatitis C Virus in Decompensated Liver Cirrhosis. Intern. Med. 2021, 60, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Tokuchi, Y.; Suda, G.; Kimura, M.; Maehara, O.; Kitagataya, T.; Kubo, A.; Yoshida, S.; Fu, Q.; Yang, Z.; Hosoda, S.; et al. Possible correlation between increased serum free carnitine levels and increased skeletal muscle mass following HCV eradication by direct acting antivirals. Sci. Rep. 2021, 11, 16616. [Google Scholar] [CrossRef]
- Linge, J.; Heymsfield, S.B.; Dahlqvist Leinhard, O. On the Definition of Sarcopenia in the Presence of Aging and Obesity-Initial Results from UK Biobank. J. Gerontol. A. Biol. Sci. Med. Sci. 2020, 75, 1309–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, Z.; Ahmed, U.; Walayat, S.; Ren, J.; Martin, D.K.; Moole, H.; Koppe, S.; Yong, S.; Dhillon, S. Liver function tests in identifying patients with liver disease. Clin. Exp. Gastroenterol. 2018, 11, 301–307. [Google Scholar] [CrossRef] [Green Version]
- Ramaty, E.; Maor, E.; Peltz-Sinvani, N.; Brom, A.; Grinfeld, A.; Kivity, S.; Segev, S.; Sidi, Y.; Kessler, T.; Sela, B.A.; et al. Low ALT blood levels predict long-term all-cause mortality among adults. A historical prospective cohort study. Eur. J. Intern. Med. 2014, 25, 919–921. [Google Scholar] [CrossRef] [PubMed]
- Ruhl, C.E.; Everhart, J.E. The Association of Low Serum Alanine Aminotransferase Activity with Mortality in the US Population. Am. J. Epidemiol. 2013, 178, 1702–1711. [Google Scholar] [CrossRef] [PubMed]
- Portal, D.; Hofstetter, L.; Eshed, I.; Dan Lantsman, C.; Sella, T.; Urban, D.; Onn, A.; Bar, J.; Segal, G. L3 skeletal muscle index (L3SMI) is a surrogate marker of sarcopenia and frailty in non-small cell lung cancer patients. Cancer Manag. Res. 2019, 11, 2579–2588. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Count or Median (Range) |
|---|---|
| Age (years) | 59 (42–79) |
| Gender, male/female | 20/32 |
| Body mass index (kg/m2) | 26.94 (19.27–38.67) |
| Skeletal muscle index (cm2/m2), male | 50.37 (29.96–73.30) |
| Skeletal muscle index (cm2/m2), female | 37.00 (21.74 -60.52) |
| Total bilirubin (mg/dL) | 1.09 (0.43–2.47) |
| Serum albumin (g/dL) | 3.91 (2.28–5.25) |
| Platelets ×10^4/mm3 | 10.9 (3.7–29.3) |
| Total cholesterol (mg/dL) | 151.5 (80–221) |
| INR | 1.14 (0.95–2.27) |
| Alpha-fetoprotein (ng/mL) | 12.92 (2.14–131) |
| Serum creatinine (mg/dL) | 0.72 (0.4–1.06) |
| AST (IU/L) | 79 (28–224) |
| ALT (IU/L) | 72 (15–264) |
| Normal L3-SMI (n = 19) | Low L3-SMI (n = 33) | Mann-Whitney | ||||
|---|---|---|---|---|---|---|
| Median (Range) | Mean Rank | Median (Range) | Mean Rank | U | p | |
| Age (years) | 55.6 (42–73) | 22.58 | 60 (42–79) | 28.76 | 239.000 | 0.156 |
| BMI | 28.32 (20.2–34.42) | 30.16 | 26.82 (19.27–38.67) | 24.39 | 244.000 | 0.187 |
| Total bilirubin | 0.99 (0.6 -2.3) | 24.29 | 1.16 (0.43–2.47) | 27.77 | 271.500 | 0.425 |
| Serum albumin | 3.9 (2.49–5.25) | 26.79 | 3.94 (2.28–4.75) | 26.33 | 308.000 | 0.917 |
| Platelets | 10.6 (5.6–29.3) | 26.76 | 10.9 (3.7–26.10) | 26.35 | 308.500 | 0.924 |
| Total cholesterol | 148 (98–221) | 23.61 | 158 (80–212) | 28.17 | 258.500 | 0.296 |
| INR | 1.2 (0.95–1.55) | 29.71 | 1.12 (0.97–2.27) | 24.65 | 252.500 | 0.246 |
| Alpha-fetoprotein | 10.15 (3.82–131) | 25.71 | 13.06 (2.14–110) | 26.95 | 298.500 | 0.776 |
| Serum creatinine | 0.73 (0.53–1.06) | 29.94 | 0.68 (0.4–0.92) | 20.53 | 200.000 | 0.031 * |
| AST | 84 (28–197) | 25.34 | 78 (35–224) | 27.17 | 291.500 | 0.676 |
| ALT | 68 (33–264) | 27.74 | 75 (15–229) | 25.79 | 290.000 | 0.655 |
| Decreased (n = 38) | Increased (n = 14) | Mann-Whitney | ||||
|---|---|---|---|---|---|---|
| Median (Range) | Mean Rank | Median (Range) | Mean Rank | U | p | |
| Age (years) | 59.5 (42–79) | 27.04 | 57.07 (45–69) | 25.04 | 245.500 | 0.672 |
| BMI | 26.17 (19.27–36) | 23.55 | 28.84 (23.94–38.67) | 34.50 | 154.000 | 0.021 * |
| Total bilirubin | 1.1 (0.48–2.47) | 26.71 | 1.0 (0.43–2.4) | 25.93 | 258.000 | 0.869 |
| Serum albumin | 4.04 (2.28–5.25) | 28.79 | 3.69 (2.44–4.5) | 20.29 | 179.000 | 0.073 |
| Platelets | 11.6 (5.6–29.3) | 27.20 | 10.25 (3.7–17.5) | 24.61 | 239.500 | 0.584 |
| Total cholesterol | 150.5 (80–221) | 26.51 | 157.5 (102–198) | 25.93 | 265.500 | 0.992 |
| INR | 1.14 (0.95–1.98) | 26.13 | 1.14 (0.97–2.27) | 27.50 | 252.000 | 0.772 |
| Alpha-fetoprotein | 11.2 (2.14–131) | 24.26 | 26.15 (3.07–110) | 32.57 | 181.000 | 0.080 |
| Serum creatinine | 0.71 (0.4–0.95) | 26.39 | 0.7 (0.52–1.06) | 26.79 | 262.000 | 0.934 |
| AST | 69 (28–224) | 24.05 | 107.5 (38–146) | 33.14 | 173.000 | 0.055 |
| ALT | 66.5 (15–264) | 23.95 | 88 (38–229) | 33.43 | 169.000 | 0.045 * |
| Normal L3-SMI (n = 19) | Low L3-SMI (n = 33) | Mann-Whitney | ||||
|---|---|---|---|---|---|---|
| Median (Range) | Mean Rank | Median (Range) | Mean Rank | U | p | |
| L3-SMI difference (numeric) | −3.98 (−16.94 to 23.81) | 20.16 | −1.3 (−6.94 to 17.34) | 30.15 | 193.000 | 0.022 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihai, F.; Trifan, A.; Stanciu, C.; Huiban, L.; Muzîca, C.; Lupașcu-Ursulescu, C.; Negru, D.; Savin, M.L.; Gîrleanu, I.; Cuciureanu, T.; et al. L3 Skeletal Muscle Index Dynamics in Patients with HCV-Related Compensated Cirrhosis Following Sustained Virological Response after Direct Acting Antiviral Treatment. Medicina 2021, 57, 1226. https://doi.org/10.3390/medicina57111226
Mihai F, Trifan A, Stanciu C, Huiban L, Muzîca C, Lupașcu-Ursulescu C, Negru D, Savin ML, Gîrleanu I, Cuciureanu T, et al. L3 Skeletal Muscle Index Dynamics in Patients with HCV-Related Compensated Cirrhosis Following Sustained Virological Response after Direct Acting Antiviral Treatment. Medicina. 2021; 57(11):1226. https://doi.org/10.3390/medicina57111226
Chicago/Turabian StyleMihai, Florin, Anca Trifan, Carol Stanciu, Laura Huiban, Cristina Muzîca, Corina Lupașcu-Ursulescu, Dragoș Negru, Marius Lucian Savin, Irina Gîrleanu, Tudor Cuciureanu, and et al. 2021. "L3 Skeletal Muscle Index Dynamics in Patients with HCV-Related Compensated Cirrhosis Following Sustained Virological Response after Direct Acting Antiviral Treatment" Medicina 57, no. 11: 1226. https://doi.org/10.3390/medicina57111226
APA StyleMihai, F., Trifan, A., Stanciu, C., Huiban, L., Muzîca, C., Lupașcu-Ursulescu, C., Negru, D., Savin, M. L., Gîrleanu, I., Cuciureanu, T., & Sîngeap, A. M. (2021). L3 Skeletal Muscle Index Dynamics in Patients with HCV-Related Compensated Cirrhosis Following Sustained Virological Response after Direct Acting Antiviral Treatment. Medicina, 57(11), 1226. https://doi.org/10.3390/medicina57111226