
Improvement in Vascular Endothelial Function following Transcatheter Aortic Valve Implantation

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Data Collection
2.3. FMD Measurement
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Changes in Clinical Parameters following TAVI
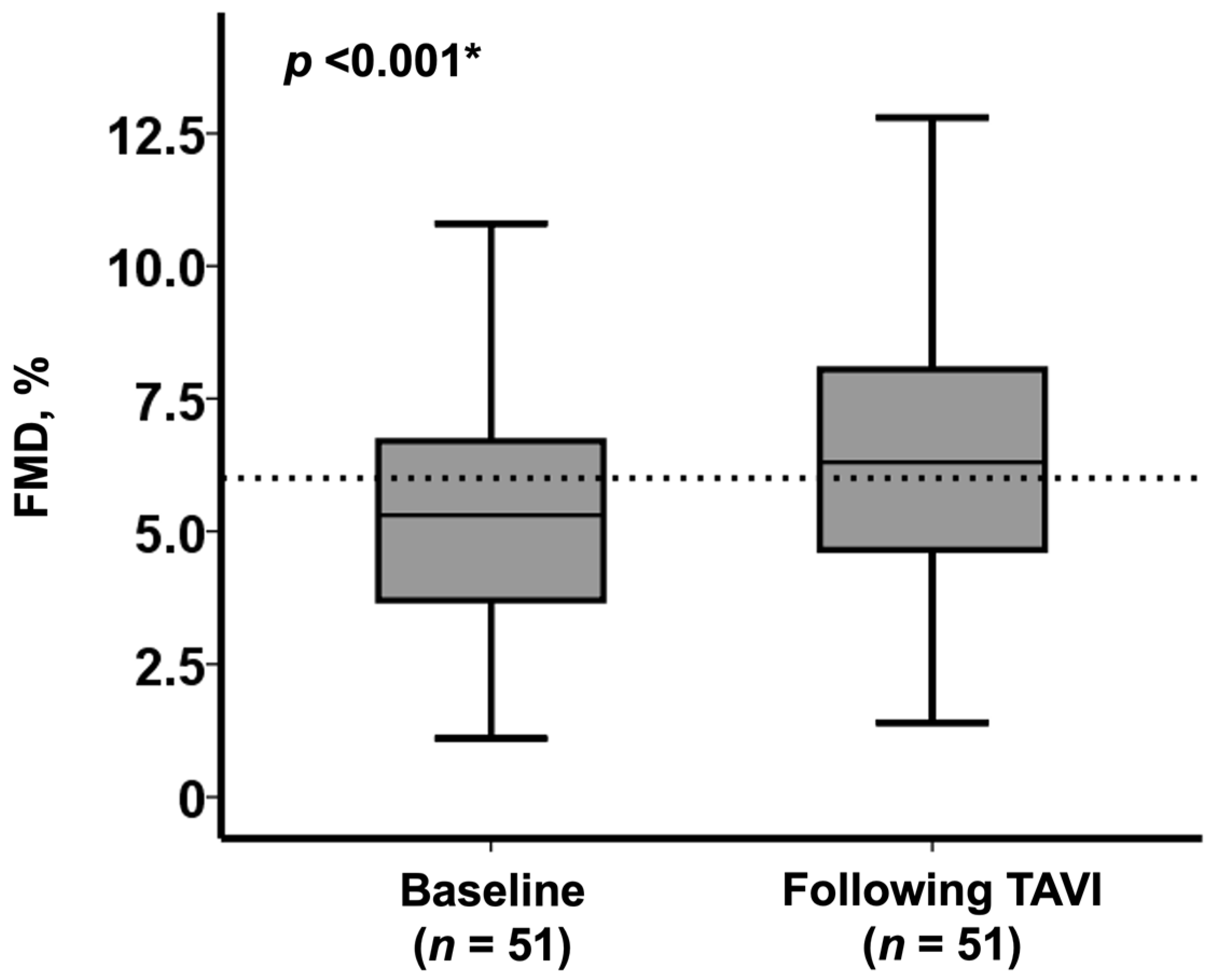
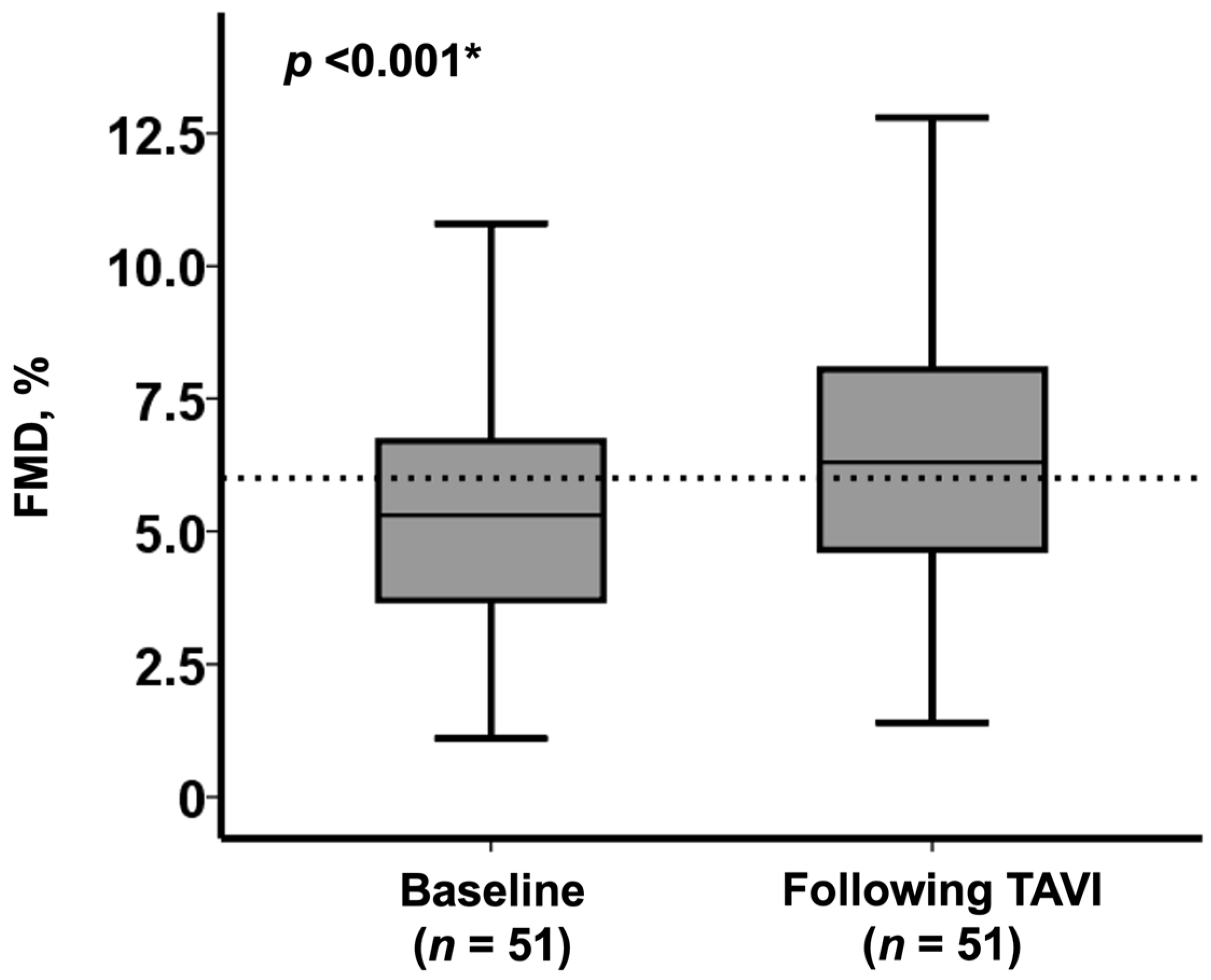
3.3. Changes in FMD Immediately after TAVI Procedure
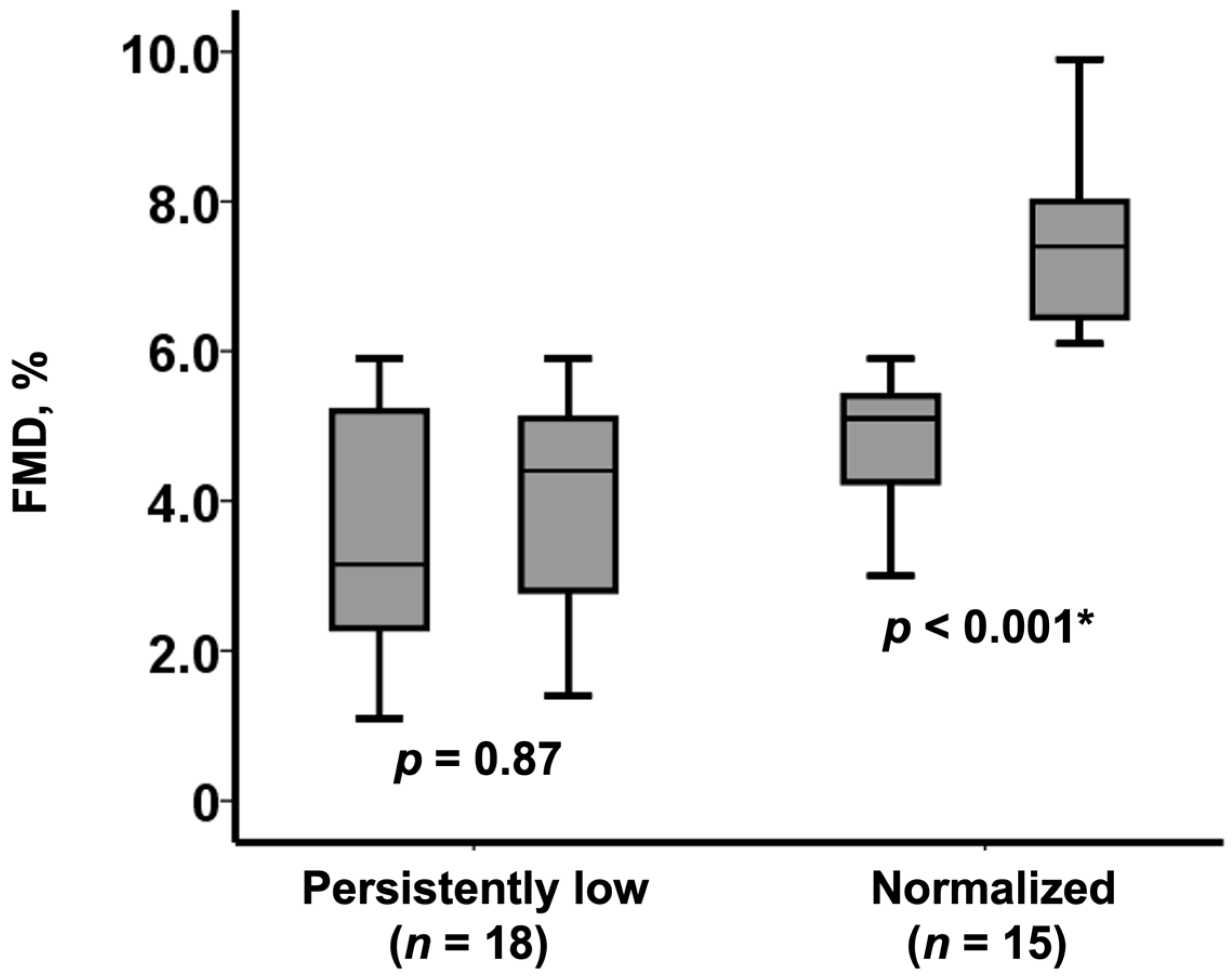
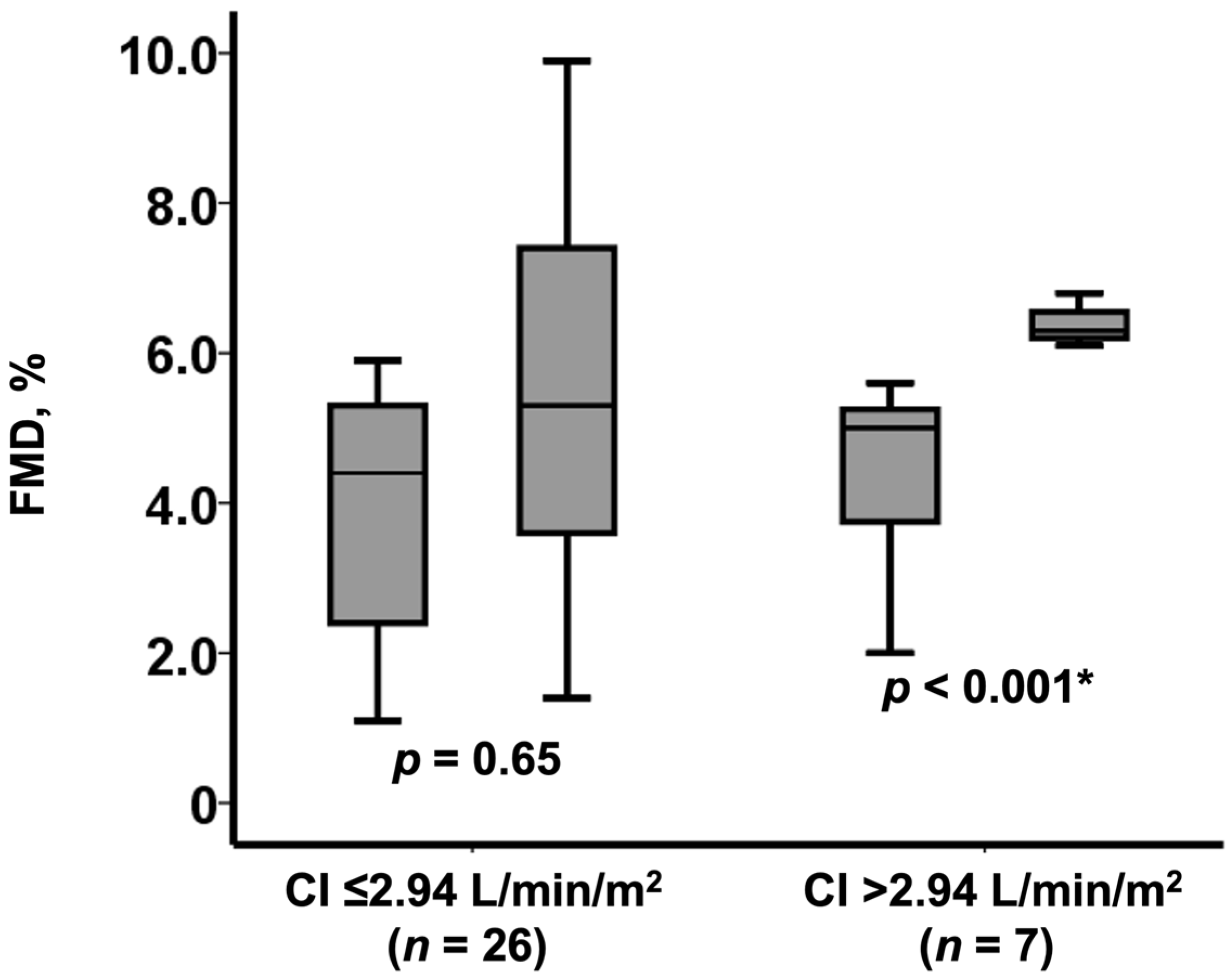
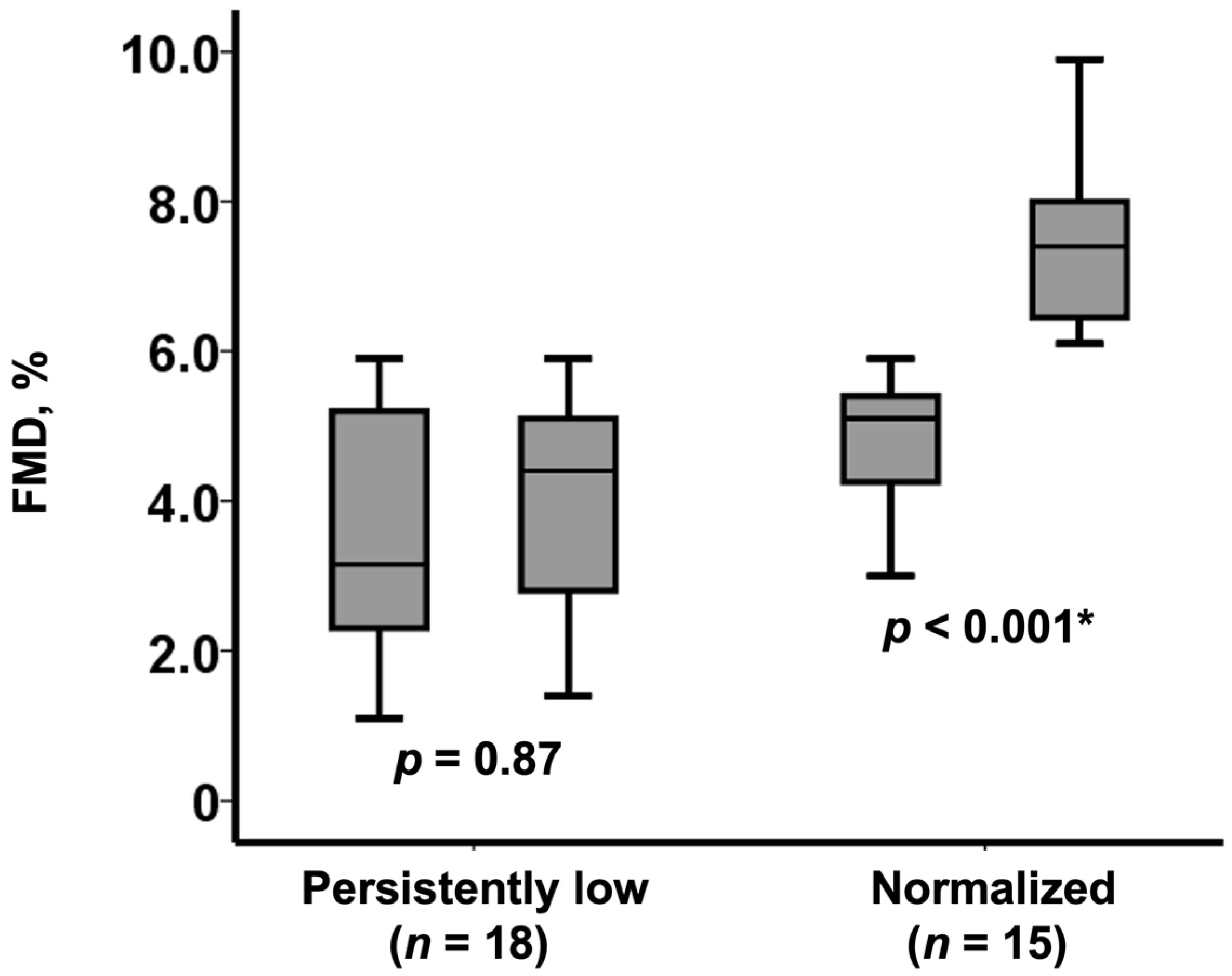
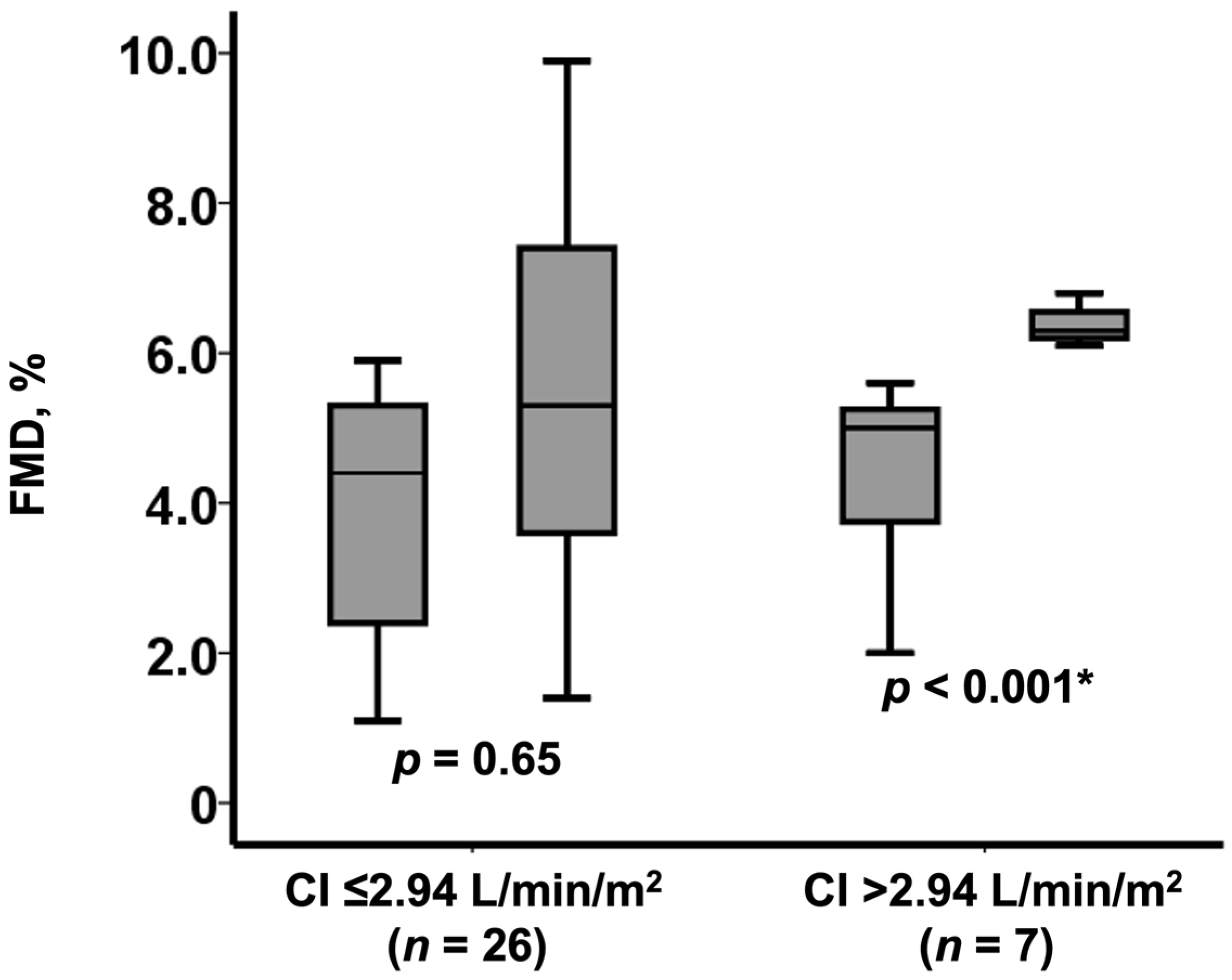
3.4. Normalization of FMD after TAVI
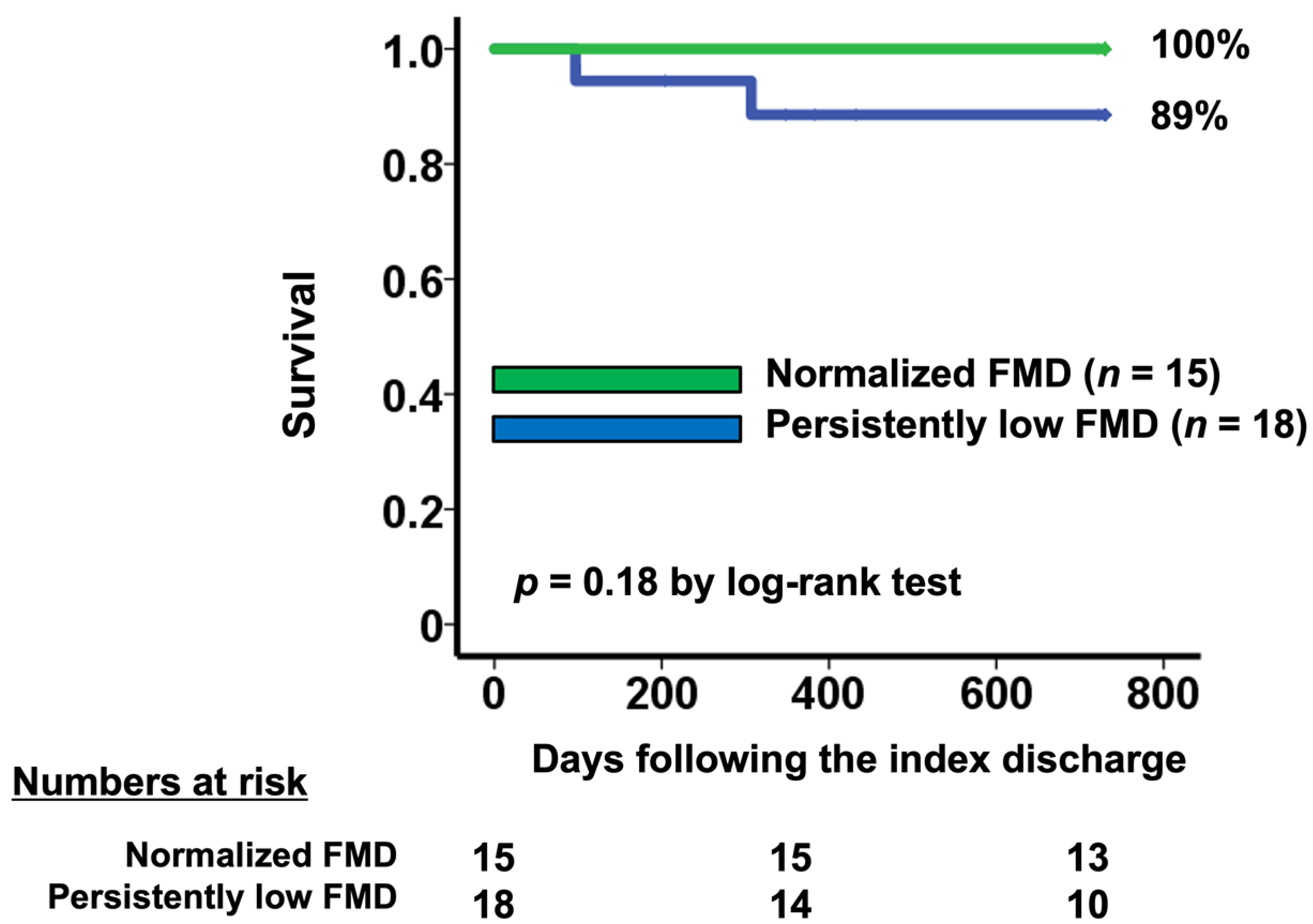
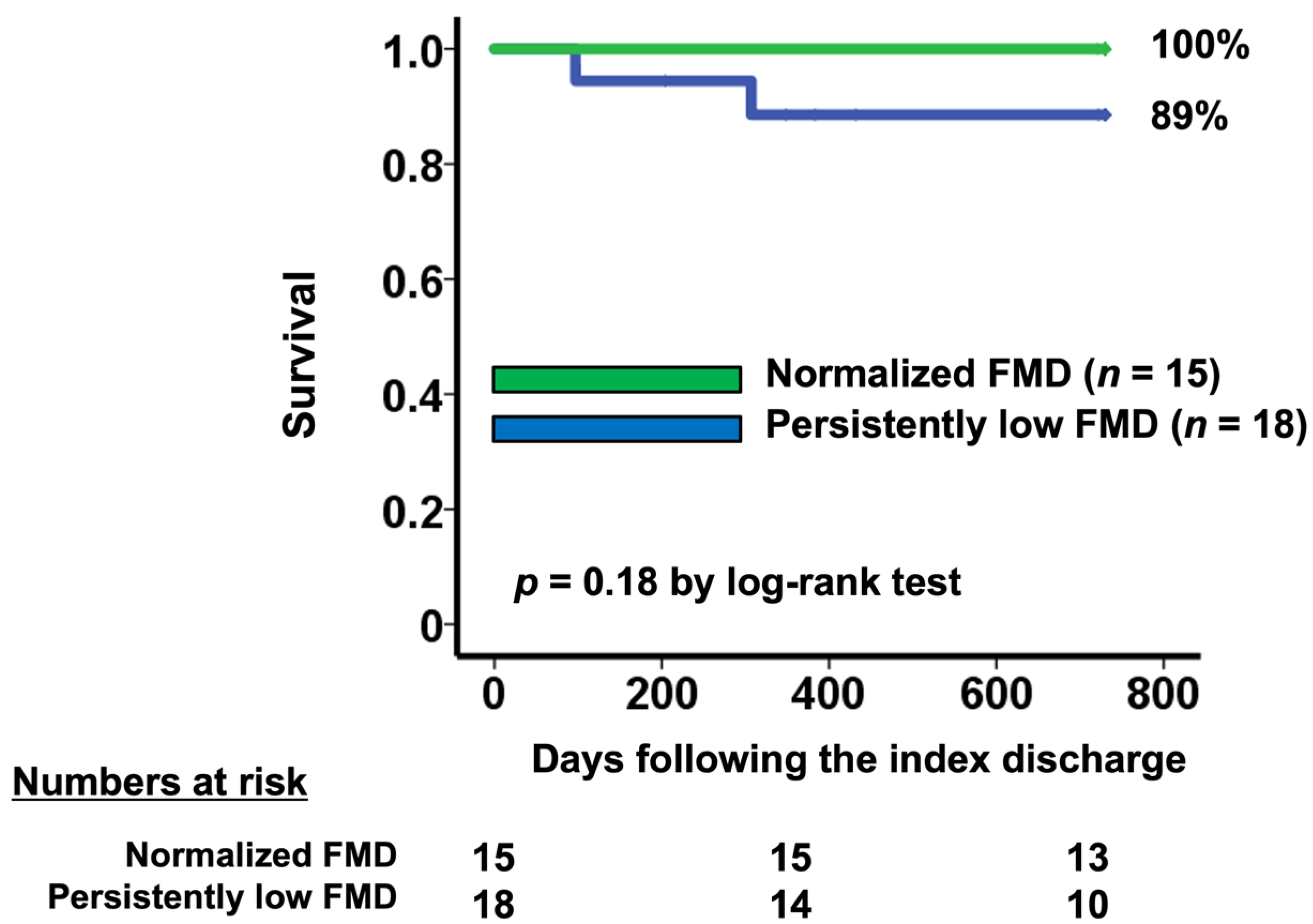
3.5. Normalization of FMD and Survival
4. Discussion
4.1. Endothelial Dysfunction and Severe AS
4.2. Change in FMD following TAVI
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Horstkotte, D.; Loogen, F. The natural history of aortic valve stenosis. Eur. Heart J. 1988, 9, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, D.H.J.; Black, M.A.; Pyke, K.E.; Padilla, J.; Atkinson, G.; Harris, R.A.; Parker, B.; Widlansky, M.E.; Tschakovsky, M.E.; Green, D.J. Assessment of flow-mediated dilation in humans: A methodological and physiological guideline. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H2–H12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, E.J.; Larson, M.; Keyes, M.J.; Mitchell, G.F.; Vasan, R.S.; Keaney, J.; Lehman, B.T.; Fan, S.; Osypiuk, E.; Vita, J. Clinical Correlates and Heritability of Flow-Mediated Dilation in the Community: The Framingham Heart Study. Circulation 2004, 109, 613–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitta, Y.; Obata, J.-E.; Nakamura, T.; Hirano, M.; Kodama, Y.; Fujioka, D.; Saito, Y.; Kawabata, K.-I.; Sano, K.; Kobayashi, T.; et al. Persistent Impairment of Endothelial Vasomotor Function Has a Negative Impact on Outcome in Patients With Coronary Artery Disease. J. Am. Coll. Cardiol. 2009, 53, 323–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modena, M.G.; Bonetti, L.; Coppi, F.; Bursi, F.; Rossi, R. Prognostic role of reversible endothelial dysfunction in hypertensive postmenopausal women. J. Am. Coll. Cardiol. 2002, 40, 505–510. [Google Scholar] [CrossRef]
- Briand, M.; Dumesnil, J.G.; Kadem, L.; Tongue, A.G.; Rieu, R.; Garcia, D.; Pibarot, P. Reduced Systemic Arterial Compliance Impacts Significantly on Left Ventricular Afterload and Function in Aortic Stenosis: Implications for Diagnosis and Treatment. J. Am. Coll. Cardiol. 2005, 46, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takata, M.; Amiya, E.; Watanabe, M.; Ozeki, A.; Watanabe, A.; Kawarasaki, S.; Nakao, T.; Hosoya, Y.; Uno, K.; Saito, A.; et al. Brachial artery diameter has a predictive value in the improvement of flow-mediated dilation after aortic valve replacement for aortic stenosis. Heart Vessel. 2014, 30, 218–226. [Google Scholar] [CrossRef]
- Horn, P.; Stern, D.; Veulemans, V.; Heiss, C.; Zeus, T.; Merx, M.W.; Kelm, M.; Westenfeld, R. Improved endothelial function and decreased levels of endothelium-derived microparticles after transcatheter aortic valve implantation. EuroIntervention 2015, 10, 1456–1463. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An Inflammatory Disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Poggianti, E.; Venneri, L.; Chubuchny, V.; Jambrik, Z.; Baroncini, L.A.; Picano, E. Aortic valve sclerosis is associatedwith systemic endothelial dysfunction. J. Am. Coll. Cardiol. 2003, 41, 136–141. [Google Scholar] [CrossRef] [Green Version]
- van Ooij, P.; Markl, M.; Collins, J.D.; Carr, J.C.; Rigsby, C.; Bonow, R.O.; Malaisrie, S.C.; McCarthy, P.M.; Fedak, P.W.; Barker, A.J. Aortic Valve Stenosis Alters Expression of Regional Aortic Wall Shear Stress: New Insights From a 4-Dimensional Flow Magnetic Resonance Imaging Study of 571 Subjects. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Ka, L.; Van Haperen, R.; De Waard, M.; Van Damme, L.C.A.; Tempel, D.; Hanemaaijer, L.; Van Cappellen, G.W.A.; Bos, J.; Slager, C.J.; et al. Shear stress affects the intracellular distribution of eNOS: Direct demonstration by a novel in vivo technique. Blood 2005, 106, 3691–3698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moscarelli, M.; Devito, F.; Fattouch, K.; Lancellotti, P.; Ciccone, M.M.; Rizzo, P.; Gaudino, M.; Marchese, A.; Angelini, G.; Speziale, G. The effect of surgical versus transcatheter aortic valve replacement on endothelial function. An observational study. Int. J. Surg. 2019, 63, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezoagli, E.; Ichinose, F.; Strelow, S.; Roy, N.; Shelton, K.; Matsumine, R.; Chen, L.; Bittner, E.A.; Bloch, D.; Zapol, W.M.; et al. Pulmonary and Systemic Vascular Resistances After Cardiopulmonary Bypass: Role of Hemolysis. J. Cardiothorac. Vasc. Anesthesia 2017, 31, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Comella, A.; Michail, M.; Chan, J.; Cameron, J.D.; Gooley, R.; Mathur, A.; Hughes, A.D.; Brown, A.J. Patients with aortic stenosis exhibit early improved endothelial function following transcatheter aortic valve replacement: The eFAST study. Int. J. Cardiol. 2021, 332, 143–147. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 51) | Baseline Normal FMD (>6%) (n = 18) | Baseline Low FMD (≤6%) (n = 33) | p Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 86 (81, 89) | 85 (82, 89) | 87 (82, 89) | 0.95 |
| Men | 12 (24%) | 1 (6%) | 11 (33%) | 0.024 * |
| Body surface area, m2 | 1.39 (1.34, 1.51) | 1.37 (1.30, 1.44) | 1.43 (1.36, 1.56) | 0.083 |
| Comorbidity | ||||
| Diabetes mellitus (%) | 8 (16%) | 2 (11%) | 6 (18%) | 0.41 |
| Dyslipidemia (%) | 29 (57%) | 10 (56%) | 19 (58%) | 0.56 |
| Current smoker (%) | 10 (20%) | 1 (6%) | 9 (27%) | 0.062 |
| Chronic obstructive pulmonary disease (%) | 5 (10%) | 1 (6%) | 4 (12%) | 0.42 |
| History of stroke (%) | 6 (12%) | 2 (11%) | 4 (12%) | 0.65 |
| Ischemic heart disease (%) | 10 (20%) | 3 (17%) | 7 (21%) | 0.5 |
| Peripheral artery disease (%) | 17 (33%) | 7 (39%) | 10 (30%) | 0.38 |
| Hemodynamics | ||||
| Systolic blood pressure, mmHg | 109 (100, 118) | 109 (101, 116) | 110 (101, 122) | 0.82 |
| Heart rate, bpm | 72 (63, 79) | 72 (61, 75) | 73 (64, 81) | 0.36 |
| Mean right atrial pressure, mmHg | 6 (3, 8) | 4 (2, 7) | 6 (3, 8) | 0.22 |
| Pulmonary capillary wedge pressure, mmHg | 12 (8, 16) | 12 (7, 17) | 13 (9, 16) | 0.87 |
| Cardiac index, L/min/m2 | 2.64 (2.28, 2.96) | 2.61 (2.38, 2.91) | 2.63 (2.25, 2.85) | 0.4 |
| Laboratory | ||||
| Hemoglobin, g/dL | 11.0 (10.0, 12.2) | 11.2 (10.2, 12.1) | 11.0 (9.2, 11.9) | 0.9 |
| Serum albumin, mg/dL | 3.9 (3.6, 4.0) | 3.9 (3.8, 4.2) | 3.8 (3.6, 4.0) | 0.37 |
| Serum sodium, mEq/L | 140 (139, 142) | 140 (140, 141) | 141 (139, 142) | 0.59 |
| eGFR, mL/min/1.73 m2 | 47.4 (38.0, 64.4) | 49.6 (40.8, 64.2) | 46.1 (30.8, 60.1) | 0.23 |
| Serum C-reactive protein, mg/dL | 0.06 (0.03, 0.22) | 0.08 (0.04, 0.15) | 0.09 (0.03, 0.26) | 0.63 |
| Plasma B-type natriuretic peptide, pg/mL | 297 (114, 620) | 443 (190, 667) | 292 (109, 586) | 0.32 |
| Echocardiography | ||||
| Maximum velocity at aortic valve, m/s | 4.7 (4.0, 5.4) | 5.1 (4.3, 6.0) | 4.5 (4.0, 5.0) | 0.038 * |
| Left ventricular end-diastolic diameter, mm | 45 (41, 49) | 45 (42, 50) | 45 (39, 49) | 0.51 |
| Left ventricular ejection fraction, % | 65 (57, 72) | 65 (53, 68) | 64 (59, 72) | 0.7 |
| Scoring | ||||
| STS score for SAVR, % | 5.1 (3.5, 7.9) | 4.9 (3.6, 5.9) | 5.1 (3.6, 8.4) | 0.31 |
| EURO II score, % | 3.3 (2.2, 4.3) | 3.4 (2.5, 4.1) | 3.2 (2.2, 4.6) | 0.91 |
| Medication | ||||
| Beta-blocker (%) | 16 (31%) | 5 (28%) | 11 (33%) | 0.47 |
| Angiotensin converting enzyme II inhibitor (%) | 7 (14%) | 1 (6%) | 6 (18%) | 0.21 |
| Renin-angiotensin system inhibitor (%) | 37 (73%) | 12 (67%) | 25 (76%) | 0.49 |
| FMD, % | 5.3 (3.2, 6.7) | 7.5 (6.7, 10.2) | 4.5 (2.6, 5.2) | <0.00 * |
| Baseline (n = 51) | After TAVI (n = 51) | p Value | |
|---|---|---|---|
| Systolic BP, mmHg | 110 (100, 118) | 117 (104, 131) | 0.036 * |
| Diastolic BP, mmHg | 58 (49, 65) | 56 (50, 62) | 0.307 |
| Pulse pressure, mmHg | 52 (143, 60) | 61 (46, 74) | 0.003 * |
| Pulse Rate, bpm | 72 (63, 79) | 71 (63, 78) | 0.386 |
| sCr, mg/dl | 1.00 (0.70, 1.18) | 0.95 (0.67, 1.13) | 0.274 |
| BNP, pg/ml | 368 (114, 620) | 138 (41, 178) | <0.001 * |
| 6min. walking distance, m | 219 (162, 280) | 235 (169, 297) | 0.023 * |
| Echocardiography | |||
| Left ventricular end-diastolic dimension, mm | 45 (41, 49) | 44 (41, 48) | 0.746 |
| Left ventricular ejection fraction, % | 65 (57, 72) | 67 (59, 70) | 0.450 |
| Aortic valve indices | |||
| Peak velocity of aortic valve flow, m/s | 4.7 (4.0, 5.4) | 2.3 (2.1, 2.6) | <0.001 * |
| Aortic valve area, cm2 | 0.57 (0.43, 0.69) | 1.47 (1.20, 1.70) | <0.001 * |
| FMD, % | 5.3 (3.2, 6.7) | 6.3 (4.7, 8.1) | <0.001 * |
| Univariate Analyses | Multivariate Analyses | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Age, years | 1.01 (0.87–1.16) | 0.95 | ||
| Men | 0.57 (0.13–2.53) | 0.46 | ||
| Body surface area, m2 | 0.12 (0.01–5.73) | 0.28 | ||
| Diabetes mellitus | 1.86 (0.29–11.9) | 0.51 | ||
| Dyslipidemia | 0.83 (0.21–3.35) | 0.8 | ||
| Current smoker | 4.14 (0.71–24.2) | 0.21 | ||
| Chronic obstructive pulmonary disease | 2.80 (0.26–30.2) | 0.40 | ||
| History of stroke | 2.80 (0.26–30.2) | 0.40 | ||
| Ischemic heart disease | 7.00 (0.74–66.6) | 0.21 | ||
| Peripheral artery disease | 1.38 (0.31–6.20) | 0.68 | ||
| Systolic blood pressure, mmHg | 0.97 (0.92–1.02) | 0.27 | ||
| Heart rate, bpm | 1.01 (0.96–1.08) | 0.64 | ||
| Mean right atrial pressure, mmHg | 1.00 (0.81–1.23) | 0.97 | ||
| Pulmonary capillary wedge pressure, mmHg | 1.07 (0.93–1.24) | 0.36 | ||
| Cariac index, L/min/m2 | 3.26 (0.56–19.0) | 0.19 | 11.8 (1.12–124) | 0.040 * |
| Hemoglobin, g/dL | 0.90 (0.61–1.34) | 0.61 | ||
| Serum albumin, mg/dL | 1.21 (0.19–7.55) | 0.84 | ||
| Serum sodium, m Eq/L | 0.97 (0.85–1.27) | 0.85 | ||
| eGFR, mL/min/1.73 m2 | 1.00 (0.97–1.05) | 0.83 | ||
| Serum C-reactive protein, mg/dL | 0.50 (0.08–3.26) | 0.47 | ||
| Plasma B-type natriuretic peptide, pg/mL | 1.00 (1.00–1.01) | 0.095 | 1.00 (1.00–1.01) | 0.060 |
| Maximum velocity at aortic valve, m/s | 2.00 (0.75–5.39) | 0.17 | 1.15 (0.34–3.90) | 0.83 |
| Left ventricular end-diastolic diameter, mm | 0.95 (0.85–1.06) | 0.37 | ||
| Left ventricular ejection fraction, % | 0.97 (0.90–1.04) | 0.40 | ||
| STS score | 0.98 (0.81–1.18) | 0.83 | ||
| EURO II score | 1.08 (0.86–1.35) | 0.53 | ||
| Beta blocker | 1.00 (0.23–4.28) | 1.0 | ||
| Angiotensin converting enzyme II inhibitor | 5.39 (0.55–52.4) | 0.15 | 7.19 (0.49–106) | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, S.; Imamura, T.; Ushijima, R.; Sobajima, M.; Fukuda, N.; Ueno, H.; Hirai, T.; Kinugawa, K. Improvement in Vascular Endothelial Function following Transcatheter Aortic Valve Implantation. Medicina 2021, 57, 1008. https://doi.org/10.3390/medicina57101008
Tanaka S, Imamura T, Ushijima R, Sobajima M, Fukuda N, Ueno H, Hirai T, Kinugawa K. Improvement in Vascular Endothelial Function following Transcatheter Aortic Valve Implantation. Medicina. 2021; 57(10):1008. https://doi.org/10.3390/medicina57101008
Chicago/Turabian StyleTanaka, Shuhei, Teruhiko Imamura, Ryuichi Ushijima, Mitsuo Sobajima, Nobuyuki Fukuda, Hiroshi Ueno, Tadakazu Hirai, and Koichiro Kinugawa. 2021. "Improvement in Vascular Endothelial Function following Transcatheter Aortic Valve Implantation" Medicina 57, no. 10: 1008. https://doi.org/10.3390/medicina57101008
APA StyleTanaka, S., Imamura, T., Ushijima, R., Sobajima, M., Fukuda, N., Ueno, H., Hirai, T., & Kinugawa, K. (2021). Improvement in Vascular Endothelial Function following Transcatheter Aortic Valve Implantation. Medicina, 57(10), 1008. https://doi.org/10.3390/medicina57101008