
Anti-Suicidal Effects of Lithium, Ketamine, and Clozapine—A 10-Year Systematic Review



Abstract
1. Introduction
1.1. Lithium
1.2. Ketamine
1.3. Clozapine
2. Methods
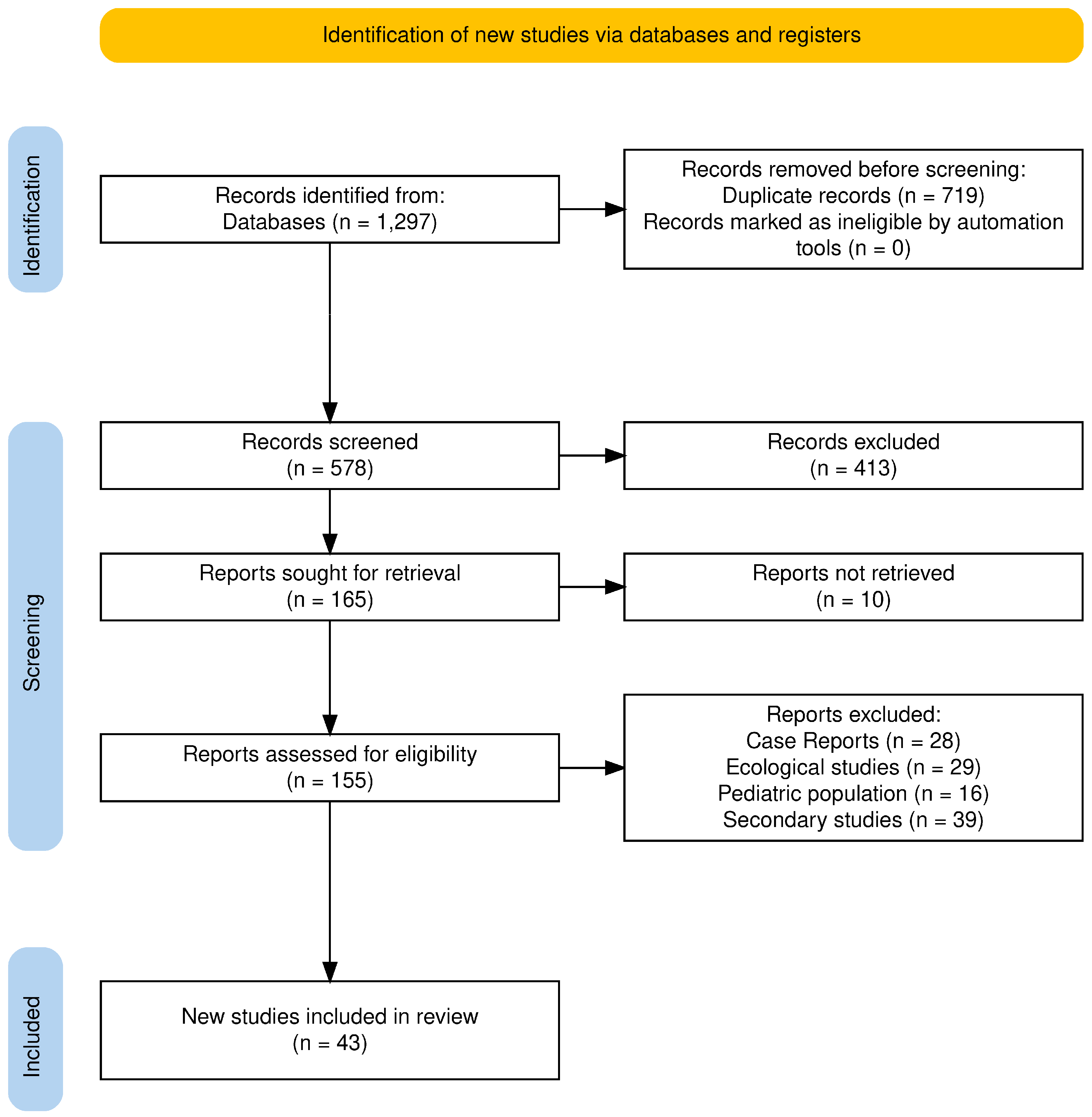
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Synthesis
3. Results
3.1. Lithium and Suicidality
3.1.1. Bipolar Patients
3.1.2. Anti-Suicidal Effect Studied in U.S. Veterans
3.1.3. Other Populations
3.2. Ketamine and Suicidality
3.3. Clozapine and Suicidality
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Suicide Worldwide in 2019. Available online: https://www.who.int/publications-detail-redirect/9789240026643 (accessed on 25 May 2023).
- World Health Organization. Live Life: An Implementation Guide for Suicide Prevention in Countries; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-002662-9. [Google Scholar]
- Song, Y.; Rhee, S.J.; Lee, H.; Kim, M.J.; Shin, D.; Ahn, Y.M. Comparison of Suicide Risk by Mental Illness: A Retrospective Review of 14-Year Electronic Medical Records. J. Korean Med. Sci. 2020, 35, e402. [Google Scholar] [CrossRef]
- Wilkinson, S.T.; Trujillo Diaz, D.; Rupp, Z.W.; Kidambi, A.; Ramirez, K.L.; Flores, J.M.; Avila-Quintero, V.J.; Rhee, T.G.; Olfson, M.; Bloch, M.H. Pharmacological and Somatic Treatment Effects on Suicide in Adults: A Systematic Review and Meta-Analysis. Focus 2023, 21, 197–208. [Google Scholar] [CrossRef]
- Ahmed, G.K.; Elserogy, Y.M.; Elfadl, G.M.A.; Ghada Abdelsalam, K.; Ali, M.A. Antidepressant and Anti-Suicidal Effects of Ketamine in Treatment-Resistant Depression Associated with Psychiatric and Personality Comorbidities: A Double-Blind Randomized Trial. J. Affect. Disord. 2023, 325, 127–134. [Google Scholar] [CrossRef]
- Chokhawala, K.; Lee, S.; Saadabadi, A. Lithium. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Tondo, L.; Alda, M.; Bauer, M.; Bergink, V.; Grof, P.; Hajek, T.; Lewitka, U.; Licht, R.W.; Manchia, M.; Müller-Oerlinghausen, B.; et al. Clinical Use of Lithium Salts: Guide for Users and Prescribers. Int. J. Bipolar Disord. 2019, 7, 16. [Google Scholar] [CrossRef]
- Malhi, G.S.; Tanious, M.; Das, P.; Coulston, C.M.; Berk, M. Potential Mechanisms of Action of Lithium in Bipolar Disorder. Current Understanding. CNS Drugs 2013, 27, 135–153. [Google Scholar] [CrossRef]
- Murphy, N.; Pham, G.; Weyland, A.; Engelhardt, J.; Kypriotakis, G.; Thomas, Y.T.; Kosten, T.R.; Moukaddam, N.; Mathew, S.J.; Swann, A.C. Lithium Reduces Impulsive Decision Making in Transdiagnostic Patients at High Risk for Suicide Attempt Recurrence: A Randomized, Double Blind, Placebo-Controlled, Crossover Study. J. Affect. Disord. Rep. 2024, 17, 100833. [Google Scholar] [CrossRef]
- Sinner, B.; Graf, B.M. Ketamine. In Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2008; pp. 313–333. [Google Scholar] [CrossRef]
- Das, J. Repurposing of Drugs-The Ketamine Story. J. Med. Chem. 2020, 63, 13514–13525. [Google Scholar] [CrossRef]
- Jelen, L.A.; Young, A.H.; Stone, J.M. Ketamine: A Tale of Two Enantiomers. J. Psychopharmacol. 2021, 35, 109–123. [Google Scholar] [CrossRef]
- Gao, M.; Rejaei, D.; Liu, H. Ketamine Use in Current Clinical Practice. Acta Pharmacol. Sin. 2016, 37, 865–872. [Google Scholar] [CrossRef]
- Berman, R.M.; Cappiello, A.; Anand, A.; Oren, D.A.; Heninger, G.R.; Charney, D.S.; Krystal, J.H. Antidepressant Effects of Ketamine in Depressed Patients. Biol. Psychiatry 2000, 47, 351–354. [Google Scholar] [CrossRef]
- Kang, M.J.Y.; Hawken, E.; Vazquez, G.H. The Mechanisms Behind Rapid Antidepressant Effects of Ketamine: A Systematic Review with a Focus on Molecular Neuroplasticity. Front. Psychiatry 2022, 13, 860882. [Google Scholar] [CrossRef]
- Zanos, P.; Gould, T.D. Mechanisms of Ketamine Action as an Antidepressant. Mol. Psychiatry 2018, 23, 801–811. [Google Scholar] [CrossRef]
- Sapkota, A.; Khurshid, H.; Qureshi, I.A.; Jahan, N.; Went, T.R.; Sultan, W.; Alfonso, M. Efficacy and Safety of Intranasal Esketamine in Treatment-Resistant Depression in Adults: A Systematic Review. Cureus 2021, 13, e17352. [Google Scholar] [CrossRef]
- Price, J.B.; Yates, C.G.; Morath, B.A.; Van De Wakker, S.K.; Yates, N.J.; Butters, K.; Frye, M.A.; McGee, S.L.; Tye, S.J. Lithium Augmentation of Ketamine Increases Insulin Signaling and Antidepressant-like Active Stress Coping in a Rodent Model of Treatment-Resistant Depression. Transl. Psychiatry 2021, 11, 598. [Google Scholar] [CrossRef]
- Costi, S.; Soleimani, L.; Glasgow, A.; Brallier, J.; Spivack, J.; Schwartz, J.; Levitch, C.F.; Richards, S.; Hoch, M.; Stade, E.C.; et al. Lithium Continuation Therapy Following Ketamine in Patients with Treatment Resistant Unipolar Depression: A Randomized Controlled Trial. Neuropsychopharmacology 2019, 44, 1812–1819. [Google Scholar] [CrossRef]
- Wilkowska, A.; Szałach, Ł.; Cubała, W.J. Ketamine in Bipolar Disorder: A Review. Neuropsychiatr. Dis. Treat. 2020, 16, 2707–2717. [Google Scholar] [CrossRef]
- Wagner, E.; Siafis, S.; Fernando, P.; Falkai, P.; Honer, W.G.; Röh, A.; Siskind, D.; Leucht, S.; Hasan, A. Efficacy and Safety of Clozapine in Psychotic Disorders—A Systematic Quantitative Meta-Review. Transl. Psychiatry 2021, 11, 487. [Google Scholar] [CrossRef]
- Haidary, H.A.; Padhy, R.K. Clozapine. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Kar, N.; Barreto, S.; Chandavarkar, R. Clozapine Monitoring in Clinical Practice: Beyond the Mandatory Requirement. Clin. Psychopharmacol. Neurosci. 2016, 14, 323–329. [Google Scholar] [CrossRef]
- Oloyede, E.; Dzahini, O.; Abolou, Z.; Gee, S.; Whiskey, E.; Malhotra, D.; Hussain, M.; Osborne, I.; Casetta, C.; McGuire, P.; et al. Clinical Impact of Reducing the Frequency of Clozapine Monitoring: Controlled Mirror-Image Cohort Study. Br. J. Psychiatry J. Ment. Sci. 2023, 223, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-Y.; Chen, P.-H.; Pan, C.-H.; Su, S.-S.; Tsai, S.-Y.; Chen, C.-C.; Kuo, C.-J. Clozapine and Its Protective Effect on All-Cause, Natural, and Suicide Mortality in Patients with Schizophrenia: A Nationwide Cohort Study in Taiwan. Schizophr. Res. 2024, 268, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, H.Y. Clozapine Treatment for Suicidality in SchizophreniaInternational Suicide Prevention Trial (InterSePT). Arch. Gen. Psychiatry 2003, 60, 82. [Google Scholar] [CrossRef]
- Vayalapalli, A.; McCall, W.V.; McEvoy, J.P.; Miller, B.J. Improved Insomnia Is One Pathway Underlying the Anti-suicidal Properties of Clozapine. Suicide Life. Threat. Behav. 2024, 54, 972–981. [Google Scholar] [CrossRef]
- Kerwin, R.W.; Bolonna, A.A. Is Clozapine Antisuicidal? Expert Rev. Neurother. 2004, 4, 187–190. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Dervic, K.; Sher, L.; Galfalvy, H.C.; Grunebaum, M.; Burke, A.K.; Sullivan, G.; Sublette, M.E.; Mann, J.J.; Oquendo, M.A. Antisuicidal Effect of Lithum in Bipolar Disorder: Is There an Age-Specific Effect? J. Affect. Disord. 2023, 341, 8–11. [Google Scholar] [CrossRef]
- Girlanda, F.; Cipriani, A.; Agrimi, E.; Appino, M.G.; Barichello, A.; Beneduce, R.; Bighelli, I.; Bisoffi, G.; Bisogno, A.; Bortolaso, P.; et al. Effectiveness of Lithium in Subjects with Treatment-Resistant Depression and Suicide Risk: Results and Lessons of an Underpowered Randomised Clinical Trial. BMC Res. Notes 2014, 7, 731. [Google Scholar] [CrossRef]
- Szmulewicz, A.; Madenci, A.; Ferguson, R.; Liang, M.H.; Lew, R.; Katz, I.R.; Hernán, M.A. Estimating the Per-Protocol Effect of Lithium on Suicidality in a Randomized Trial of Individuals with Depression or Bipolar Disorder. J. Psychopharmacol. 2023, 37, 539–544. [Google Scholar] [CrossRef]
- Stark, K. Impact of Lithium on Suicidality in the Veteran Population. Fed. Pract. 2022, 39, 130–135. [Google Scholar] [CrossRef]
- Brus, O.; Cao, Y.; Hammar, Å.; Landén, M.; Lundberg, J.; Nordanskog, P.; Nordenskjöld, A. Lithium for Suicide and Readmission Prevention after Electroconvulsive Therapy for Unipolar Depression: Population-Based Register Study. BJPsych Open 2019, 5, e46. [Google Scholar] [CrossRef] [PubMed]
- Toffol, E.; Hätönen, T.; Tanskanen, A.; Lönnqvist, J.; Wahlbeck, K.; Joffe, G.; Tiihonen, J.; Haukka, J.; Partonen, T. Lithium Is Associated with Decrease in All-Cause and Suicide Mortality in High-Risk Bipolar Patients: A Nationwide Registry-Based Prospective Cohort Study. J. Affect. Disord. 2015, 183, 159–165. [Google Scholar] [CrossRef]
- Katz, I.R.; Rogers, M.P.; Lew, R.; Thwin, S.S.; Doros, G.; Ahearn, E.; Ostacher, M.J.; DeLisi, L.E.; Smith, E.G.; Ringer, R.J.; et al. Lithium Treatment in the Prevention of Repeat Suicide-Related Outcomes in Veterans with Major Depression or Bipolar Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2022, 79, 24. [Google Scholar] [CrossRef]
- Chen, P.-H.; Tsai, S.-Y.; Chen, P.-Y.; Pan, C.-H.; Su, S.-S.; Chen, C.-C.; Kuo, C.-J. Mood Stabilizers and Risk of All-Cause, Natural, and Suicide Mortality in Bipolar Disorder: A Nationwide Cohort Study. Acta Psychiatr. Scand. 2023, 147, 234–247. [Google Scholar] [CrossRef]
- Smith, E.G.; Austin, K.L.; Kim, H.M.; Eisen, S.V.; Kilbourne, A.M.; Miller, D.R.; Zivin, K.; Hannemann, C.; Sauer, B.C.; Valenstein, M. Mortality Associated with Lithium and Valproate Treatment of US Veterans Health Administration Patients with Mental Disorders. Br. J. Psychiatry 2015, 207, 55–63. [Google Scholar] [CrossRef]
- Chan, J.K.N.; Wong, C.S.M.; Fang, C.Z.; Hung, S.C.; Lo, H.K.Y.; Chang, W.C. Mortality Risk and Mood Stabilizers in Bipolar Disorder: A Propensity-Score-Weighted Population-Based Cohort Study in 2002–2018. Epidemiol. Psychiatr. Sci. 2024, 33, e31. [Google Scholar] [CrossRef]
- Song, J.; Sjölander, A.; Joas, E.; Bergen, S.E.; Runeson, B.; Larsson, H.; Landén, M.; Lichtenstein, P. Suicidal Behavior During Lithium and Valproate Treatment: A Within-Individual 8-Year Prospective Study of 50,000 Patients with Bipolar Disorder. Am. J. Psychiatry 2017, 174, 795–802. [Google Scholar] [CrossRef]
- Smith, E.G.; Austin, K.L.; Kim, H.M.; Miller, D.R.; Sauer, B.C.; Valenstein, M. Suicide Death over the First Year of Lithium versus Valproate Treatment in Cohorts with and without Bipolar Disorder. J. Psychiatr. Res. 2022, 147, 349–356. [Google Scholar] [CrossRef]
- Smith, E.G.; Austin, K.L.; Kim, H.M.; Miller, D.R.; Eisen, S.V.; Christiansen, C.L.; Kilbourne, A.M.; Sauer, B.C.; McCarthy, J.F.; Valenstein, M. Suicide Risk in Veterans Health Administration Patients with Mental Health Diagnoses Initiating Lithium or Valproate: A Historical Prospective Cohort Study. BMC Psychiatry 2014, 14, 357. [Google Scholar] [CrossRef]
- Grunebaum, M.F.; Ellis, S.P.; Keilp, J.G.; Moitra, V.K.; Cooper, T.B.; Marver, J.E.; Burke, A.K.; Milak, M.S.; Sublette, M.E.; Oquendo, M.A.; et al. Ketamine versus Midazolam in Bipolar Depression with Suicidal Thoughts: A Pilot Midazolam-Controlled Randomized Clinical Trial. Bipolar Disord. 2017, 19, 176–183. [Google Scholar] [CrossRef]
- Fineberg, S.K.; Choi, E.Y.; Shapiro-Thompson, R.; Dhaliwal, K.; Neustadter, E.; Sakheim, M.; Null, K.; Trujillo-Diaz, D.; Rondeau, J.; Pittaro, G.F.; et al. A Pilot Randomized Controlled Trial of Ketamine in Borderline Personality Disorder. Neuropsychopharmacology 2023, 48, 991–999. [Google Scholar] [CrossRef]
- Phillips, J.L.; Norris, S.; Talbot, J.; Hatchard, T.; Ortiz, A.; Birmingham, M.; Owoeye, O.; Batten, L.A.; Blier, P. Single and Repeated Ketamine Infusions for Reduction of Suicidal Ideation in Treatment-Resistant Depression. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2020, 45, 606–612. [Google Scholar] [CrossRef]
- Abbar, M.; Demattei, C.; El-Hage, W.; Llorca, P.-M.; Samalin, L.; Demaricourt, P.; Gaillard, R.; Courtet, P.; Vaiva, G.; Gorwood, P.; et al. Ketamine for the Acute Treatment of Severe Suicidal Ideation: Double Blind, Randomised Placebo Controlled Trial. BMJ 2022, 376, e067194. [Google Scholar] [CrossRef]
- Canuso, C.M.; Singh, J.B.; Fedgchin, M.; Alphs, L.; Lane, R.; Lim, P.; Pinter, C.; Hough, D.; Sanacora, G.; Manji, H.; et al. Efficacy and Safety of Intranasal Esketamine for the Rapid Reduction of Symptoms of Depression and Suicidality in Patients at Imminent Risk for Suicide: Results of a Double-Blind, Randomized, Placebo-Controlled Study. Am. J. Psychiatry 2018, 175, 620–630. [Google Scholar] [CrossRef]
- Grunebaum, M.F.; Galfalvy, H.C.; Choo, T.-H.; Keilp, J.G.; Moitra, V.K.; Parris, M.S.; Marver, J.E.; Burke, A.K.; Milak, M.S.; Sublette, M.E.; et al. Ketamine for Rapid Reduction of Suicidal Thoughts in Major Depression: A Midazolam-Controlled Randomized Clinical Trial. Am. J. Psychiatry 2018, 175, 327–335. [Google Scholar] [CrossRef]
- Fu, D.-J.; Ionescu, D.F.; Li, X.; Lane, R.; Lim, P.; Sanacora, G.; Hough, D.; Manji, H.; Drevets, W.C.; Canuso, C.M. Esketamine Nasal Spray for Rapid Reduction of Major Depressive Disorder Symptoms in Patients Who Have Active Suicidal Ideation with Intent: Double-Blind, Randomized Study (ASPIRE I). J. Clin. Psychiatry 2020, 81, 19m13191. [Google Scholar] [CrossRef]
- Zolghadriha, A.; Anjomshoaa, A.; Jamshidi, M.R.; Taherkhani, F. Rapid and Sustained Antidepressant Effects of Intravenous Ketamine in Treatment-Resistant Major Depressive Disorder and Suicidal Ideation: A Randomized Clinical Trial. BMC Psychiatry 2024, 24, 341. [Google Scholar] [CrossRef]
- Ionescu, D.F.; Fu, D.-J.; Qiu, X.; Lane, R.; Lim, P.; Kasper, S.; Hough, D.; Drevets, W.C.; Manji, H.; Canuso, C.M. Esketamine Nasal Spray for Rapid Reduction of Depressive Symptoms in Patients with Major Depressive Disorder Who Have Active Suicide Ideation with Intent: Results of a Phase 3, Double-Blind, Randomized Study (ASPIRE II). Int. J. Neuropsychopharmacol. 2020, 24, 22–31. [Google Scholar] [CrossRef]
- Sinyor, M.; Williams, M.; Belo, S.; Orser, B.; Vincent, M.; Mah, L.; Zarate, C.; Castel, S.; Levitt, A.J.; Schaffer, A. Ketamine Augmentation for Major Depressive Disorder and Suicidal Ideation: Preliminary Experience in an Inpatient Psychiatry Setting. J. Affect. Disord. 2018, 241, 103–109. [Google Scholar] [CrossRef]
- Su, T.-P.; Li, C.-T.; Lin, W.-C.; Wu, H.-J.; Tsai, S.-J.; Bai, Y.-M.; Mao, W.-C.; Tu, P.-C.; Chen, L.-F.; Li, W.-C.; et al. A Randomized, Double-Blind, Midazolam-Controlled Trial of Low-Dose Ketamine Infusion in Patients with Treatment-Resistant Depression and Prominent Suicidal Ideation. Int. J. Neuropsychopharmacol. 2023, 26, 331–339. [Google Scholar] [CrossRef]
- Price, R.B.; Iosifescu, D.V.; Murrough, J.W.; Chang, L.C.; Al Jurdi, R.K.; Iqbal, S.Z.; Soleimani, L.; Charney, D.S.; Foulkes, A.L.; Mathew, S.J. Effects of Ketamine on Explicit and Implicit Suicidal Cognition: A Randomized Controlled Trial in Treatment-Resistant Depression. Depress. Anxiety 2014, 31, 335–343. [Google Scholar] [CrossRef]
- Fan, W.; Yang, H.; Sun, Y.; Zhang, J.; Li, G.; Zheng, Y.; Liu, Y. Ketamine Rapidly Relieves Acute Suicidal Ideation in Cancer Patients: A Randomized Controlled Clinical Trial. Oncotarget 2016, 8, 2356. [Google Scholar] [CrossRef]
- Ionescu, D.F.; Bentley, K.H.; Eikermann, M.; Taylor, N.; Akeju, O.; Swee, M.B.; Pavone, K.J.; Petrie, S.R.; Dording, C.; Mischoulon, D.; et al. Repeat-Dose Ketamine Augmentation for Treatment-Resistant Depression with Chronic Suicidal Ideation: A Randomized, Double Blind, Placebo Controlled Trial. J. Affect. Disord. 2019, 243, 516–524. [Google Scholar] [CrossRef]
- Murrough, J.W.; Iosifescu, D.V.; Chang, L.C.; Al Jurdi, R.K.; Green, C.E.; Perez, A.M.; Iqbal, S.; Pillemer, S.; Foulkes, A.; Shah, A.; et al. Antidepressant Efficacy of Ketamine in Treatment-Resistant Major Depression: A Two-Site Randomized Controlled Trial. Am. J. Psychiatry 2013, 170, 1134–1142. [Google Scholar] [CrossRef]
- Feeney, A.; Hock, R.S.; Freeman, M.P.; Flynn, M.; Hoeppner, B.; Iosifescu, D.V.; Trivedi, M.H.; Sanacora, G.; Mathew, S.J.; Debattista, C.; et al. The Effect of Single Administration of Intravenous Ketamine Augmentation on Suicidal Ideation in Treatment-Resistant Unipolar Depression: Results from a Randomized Double-Blind Study. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2021, 49, 122–132. [Google Scholar] [CrossRef]
- Domany, Y.; Shelton, R.C.; McCullumsmith, C.B. Ketamine for Acute Suicidal Ideation. An Emergency Department Intervention: A Randomized, Double-blind, Placebo-controlled, Proof-of-concept Trial. Depress. Anxiety 2020, 37, 224–233. [Google Scholar] [CrossRef]
- Zeng, Q.-B.; Zou, D.-C.; Huang, X.-B.; Shang, D.-W.; Huang, X.; Yang, X.-H.; Ning, Y.-P.; Balbuena, L.; Xiang, Y.-T.; Zheng, W. Efficacy and Safety of Esketamine versus Propofol in Electroconvulsive Therapy for Treatment-Resistant Depression: A Randomized, Double-Blind, Controlled, Non-Inferiority Trial. J. Affect. Disord. 2025, 368, 320–328. [Google Scholar] [CrossRef]
- Hu, Y.-D.; Xiang, Y.-T.; Fang, J.-X.; Zu, S.; Sha, S.; Shi, H.; Ungvari, G.S.; Correll, C.U.; Chiu, H.F.K.; Xue, Y.; et al. Single i.v. Ketamine Augmentation of Newly Initiated Escitalopram for Major Depression: Results from a Randomized, Placebo-Controlled 4-Week Study. Psychol. Med. 2016, 46, 623–635. [Google Scholar] [CrossRef]
- Burger, J.; Capobianco, M.; Lovern, R.; Boche, B.; Ross, E.; Darracq, M.A.; McLay, R. A Double-Blinded, Randomized, Placebo-Controlled Sub-Dissociative Dose Ketamine Pilot Study in the Treatment of Acute Depression and Suicidality in a Military Emergency Department Setting. Mil. Med. 2016, 181, 1195–1199. [Google Scholar] [CrossRef]
- Jones, G.H.; Vecera, C.M.; Ruiz, A.C.; Wu, H.E.; McInturff, S.I.; Orejarena, M.J.; Smith, K.A.; Soares, J.C.; Zarate, C.A.; Lane, S.D.; et al. A Randomized, Double-Blind, Placebo-Controlled Pilot Trial of the Acute Antisuicidal and Antidepressant Effects of Intranasal (R,S)-Ketamine in Severe Unipolar and Bipolar Depression with and Without Comorbid Alcohol Use Disorder. J. Clin. Psychiatry 2024, 85, 23m14974. [Google Scholar] [CrossRef]
- Ringbäck Weitoft, G.; Berglund, M.; Lindström, E.A.; Nilsson, M.; Salmi, P.; Rosén, M. Mortality, Attempted Suicide, Re-hospitalisation and Prescription Refill for Clozapine and Other Antipsychotics in Sweden—A Register-based Study. Pharmacoepidemiol. Drug Saf. 2014, 23, 290–298. [Google Scholar] [CrossRef]
- Van Der Zalm, Y.; Foldager, L.; Termorshuizen, F.; Sommer, I.E.; Nielsen, J.; Selten, J. Clozapine and Mortality: A Comparison with Other Antipsychotics in a Nationwide Danish Cohort Study. Acta Psychiatr. Scand. 2021, 143, 216–226. [Google Scholar] [CrossRef]
- Taipale, H.; Lähteenvuo, M.; Tanskanen, A.; Mittendorfer-Rutz, E.; Tiihonen, J. Comparative Effectiveness of Antipsychotics for Risk of Attempted or Completed Suicide Among Persons with Schizophrenia. Schizophr. Bull. 2021, 47, 23–30. [Google Scholar] [CrossRef]
- Taipale, H.; Tanskanen, A.; Mehtälä, J.; Vattulainen, P.; Correll, C.U.; Tiihonen, J. 20-year Follow-up Study of Physical Morbidity and Mortality in Relationship to Antipsychotic Treatment in a Nationwide Cohort of 62,250 Patients with Schizophrenia (FIN20). World Psychiatry 2020, 19, 61–68. [Google Scholar] [CrossRef]
- Hassan, A.; De Luca, V.; Dai, N.; Asmundo, A.; Di Nunno, N.; Monda, M.; Villano, I. Effectiveness of Antipsychotics in Reducing Suicidal Ideation: Possible Physiologic Mechanisms. Healthcare 2021, 9, 389. [Google Scholar] [CrossRef]
- Gürcan, G.; Şenol, Ş.H.; Yağcıoğlu, A.E.A.; Ertuğrul, A. Effect of Clozapine on Suicidality in Patients with Schizophrenia at a University Hospital in Turkey. Schizophr. Res. 2024, 268, 161–164. [Google Scholar] [CrossRef]
- Miller, J.N.; Black, D.W. Bipolar Disorder and Suicide: A Review. Curr. Psychiatry Rep. 2020, 22, 6. [Google Scholar] [CrossRef]
- Chen, C.-C.; Zhou, N.; Hu, N.; Feng, J.-G.; Wang, X.-B. Acute Effects of Intravenous Sub-Anesthetic Doses of Ketamine and Intranasal Inhaled Esketamine on Suicidal Ideation: A Systematic Review and Meta-Analysis. Neuropsychiatr. Dis. Treat. 2023, 19, 587–599. [Google Scholar] [CrossRef]
- Feng, W.; Chen, C.; Zeng, Y.; Zhang, B. Efficacy of Single and Repeated Ketamine Administration for Suicidal Ideation in Adults with Psychiatric Disorders: A Meta-Analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2025, 136, 111152. [Google Scholar] [CrossRef]
- Shen, Z.; Gao, D.; Lv, X.; Wang, H.; Yue, W. A Meta-Analysis of the Effects of Ketamine on Suicidal Ideation in Depression Patients. Transl. Psychiatry 2024, 14, 248. [Google Scholar] [CrossRef]
- Masdrakis, V.G.; Baldwin, D.S. Prevention of Suicide by Clozapine in Mental Disorders: Systematic Review. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2023, 69, 4–23. [Google Scholar] [CrossRef]
- Yao, Z.; McCall, W.V. Designing Clinical Trials to Assess the Impact of Pharmacological Treatment for Suicidal Ideation/Behavior: Issues and Potential Solutions. Pharm. Med. 2023, 37, 221–232. [Google Scholar] [CrossRef]
- Stone, M.; Laughren, T.; Jones, M.L.; Levenson, M.; Holland, P.C.; Hughes, A.; Hammad, T.A.; Temple, R.; Rochester, G. Risk of Suicidality in Clinical Trials of Antidepressants in Adults: Analysis of Proprietary Data Submitted to US Food and Drug Administration. BMJ 2009, 339, b2880. [Google Scholar] [CrossRef] [PubMed]
- Lenze, E.J.; Mulsant, B.H.; Blumberger, D.M.; Karp, J.F.; Newcomer, J.W.; Anderson, S.J.; Dew, M.A.; Butters, M.A.; Stack, J.A.; Begley, A.E.; et al. Efficacy, Safety, and Tolerability of Augmentation Pharmacotherapy with Aripiprazole for Treatment-Resistant Depression in Late Life: A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2015, 386, 2404–2412. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Reference Number | Main Author | Study Design | Sample Size | Lithium (Serum Level) | Control (Dose) | Inclusion Criteria | Exclusion Criteria | Main Findings |
|---|---|---|---|---|---|---|---|---|
| [30] | Kanita Dervic 2023 | 2.5 year randomized, double-blind trial | 94 | 0.6–1.0 [mEq/dL] | valproate; 45–125 µg/mL serum level | BD patients (DSM-IV) with at least one past suicide attempt; in depressive or mixed episode; aged 18–75 years | lack of capacity to provide informed consent; pregnancy or lactation; active medical problems, including substance abuse problems requiring detoxification; contraindication to use of lithium or valproate; a history of nonresponse to adequate dosages of either lithium and valproate in the past 2 years; contraindication to the use of adjunctive antidepressants if in a depressed state or adjunctive antipsychotics if in a mixed or psychotic depressed state. | significant antisuicidal effect of lihium in BD patients > 42 yo, independent of clinicals and sociodemographic characteristics, effect not observed for younger patients group |
| [31] | Francesca Girlanda 2014 | underpowered RCT | 58 | 0.57 [mEq/dL] (mean) | usual care | diagnosis of unipolar major depression (DSM-IV); an episode of Deliberate Self-Harm in the previous 12 months; inadequate response to at least two antidepressants given for the current depressive episode; uncertainty about which treatment arm would be best for the participant; age 18 or above; informed consent | a primary diagnosis of any concurrent Axis I disorder (DSM-IV) other than major depression; previous exposure to lithium associated with lack of efficacy or adverse reactions; clinical conditions contraindicating lithium; pregnant/lactating women and women of childbearing potential not practicing a reliable method of contraception. | study failed to achieve, minimum sample size needed to detect clinically meaningful difference, source for further meta-analyses |
| [32] | Szmulewicz A. 2023 | double-blind, placabo controlled, randomized trial | 486 | 0.6–0.8 [mEq/dL] | placebo | U.S. Veterans with a diagnosis of major depressive disorder or bipolar disorder with a suicidal event in the prior 6 months | clinical conditions that justify stopping the study drug; use of medications that justify stopping the study drug; frequency of measurement of lithium levels both during the titration phase and after the titration phase; minimum number of pills of the study drug that participants must use if they had no justified reason to stop treatment; maximum time without a clinical visit. | protective effect of lithium cannot be ruled out, need for further studies |
| [33] | Kelsie M. Stark 2022 | retrospective review | 98 | 0.6–1.2 [mEq/dL] | no control–tracking suicidal behavior in time | U.S. Veterans; aged ≥18 years; had an active lithium prescription on the date of data extraction; had an active lithium prescription for at least 6 months | had <3 months of data before and/or after lithium was used for 6 months; if they were initiated on lithium outside particular healthcare institution | significant antisuicidal effect, but point to a need of prospective placebo-controlled studies due to limitations (sample size, unknown serum levels, etc.), study should be considered as hypothesis-generating |
| [34] | Ole Brus 2019 | register-based cohort study | 7350 | not measured | standard care | all patients in the Swedish National Quality Register for ECT (electroconvulsive therapy) who had received index ECT for unipolar depression between 2011 and 2016, and were registered as in-patients in the Swedish National Patient Register at the start of the treatment series. | age under 18 years of age; readmission on the same day as discharge; death registered before or on the day of discharge; incomplete data on marital status. | Patients treated with lithium after ECT for unipolar depression were less likely to die by suicide or be readmitted |
| [35] | Elena Toffol 2015 | nationwide registry-based prospective cohort study | 826 | not measured | standard care | all the individuals who were hospitalized in Finland because of a suicide attempt between 1 January 1996 and 31 December 2003, and in prospective screening had been hospitalized due to bipolar disorder before the index attempt | lithium non-significantly lowers risk of suicide attempt, is assosiated with decreased suicide mortality and all-cause mortality (by 49%), recommendationf for lithium usage in suicidal BP patients | |
| [36] | Ira R. Katz 2022 | randomized clinical trial | 519 | 0.6–0.8 [mEq/dL] | placebo + usual care | U.S. Veterans with a diagnosis of major depressive disorder or bipolar disorder with a suicidal event in the prior 6 months | schizophrenia; 6 or more previous lifetime suicide attempts; use of lithium within the past 6 months; history of significant adverse effects of lithium; unstable substance use or medical conditions; pregnancy, lactation, or not using birth control; participating in another randomized intervention trial; current use of clozapine, haloperidol, or diuretics except amiloride. | adding lithium to existing treatment is unlikely to be effective for preventing a broad range of suicide-related events |
| [37] | Pao-Huan Chen 2023 | nationwide cohort study | 25,787 | not measured | valproate, lamotrigine, carbamazepine | all from patients with BD diagnosis from Taiwan’s insurance registry (1 February 2001–31 December 2016) | at least one psychiatric diagnosis of schizophrenia | longer duration of lithium use and higher cumulative doses are associated with lower risk of all-cause mortality (both suicidal and natural). much greater then other medications. evidence-based support for lithium as the treatment of choice for patients with bipolar disorder at high risk of suicide |
| [38] | Eric G Smith 2015 | cohort study | 93,162 | not measured | valproate | U.S. Veterans; at least one psychotic or depresive disorder; incident users receiving at least one out-patient prescription for lithium or valproate from April 1999 to December 2008; broad cohort of patients with mood or psychotic diagnoses in the 30 days prior to medication initiation was examined since the limited prior literature concerning lithium and mortality is not restricted to bipolar disorder | patients with possible non-psychiatric indications for valproate or lithium; initiated lithium or valproate on an ‘as needed’ basis or both medications simultaneously, or resided outside the USA. | lithium lowered suicide rates in general, but in intent-to-treat method effect is visible 0–90 days but not later, majorly due to disontinuation and connected increased risk (as shown in as-treated aproach) |
| [39] | Joe Kwun Nam Chan 2024 | cohort study | 8137 | not measured | valproate, quetiapine, risperidone, olanzapine | all individuals aged ≥15 years who received a first-recorded diagnosis of BD for public psychiatric inpatient or outpatient treatment in Hong Kong between 1 January 2002 and 31 December 2018. | individuals with their diagnosis changed to schizophrenia or schizoaffective disorder; BD patients who had not been exposed to any of the five studied mood stabilizers | supports usage of lithium as first-line mood stabilizer for BD. lithium, quetiapine and valproate are associated with lower risk of all-cause death compared to risperidone and olanzapine. doesnt differenciate risks betwen lithium, quatiepine and valproate. |
| [40] | Jie Song 2017 | prospective study | 51,535 | not measured | valproate and without mood stabilizer | BD patients followed from 1 October 2005, or age 15, or date of first diagnosis if later than 1 October 2005, until emigration, death, or 31 December 2013, whichever occurred first; data acquired from drifferent Swedish National Registries | lithium decreased suicide rate by 14% compared to valproate. lithium should by considerd for patients with BD with suicidal intentions. estimation that more than 10% of all suicide-related events could be prevented if all patients had been treated with lithium. points to risk of discontinuation | |
| [41] | Eric G Smith 2022 | cohort study | 23,298 | not measured | valproate | Veterans Health Administration (VHA) patients with mental health diagnoses initiating lithium or valproate from April 1999 to December 2008; all individuals with recent VHA utilization were identified among all individuals with a mood or psychotic diagnosis in the past 30 days who received at least one outpatient prescription of lithium or valproate; incident recipients within this cohort were identified as individuals with ≥6 months of no lithium or valproate use prior to initiation | individuals with potentially nonpsychiatric indications for lithium or valproate treatment; individuals starting both lithium and valproate simultaneously | decreased one-year suicide risk, but also increased (14/20-fold) suicidal behaviour after discontinouation, decreased suicide risk for not bipolar patients. |
| [42] | Eric G Smith 2014 | historical prospective cohort study | 93,335 | not measured | valproate | U.S. Veterans; at least one psychotic or depresive disorder; incident users receiving at least one out-patient prescription for lithium or valproate from April 1999 to December 2008; broad cohort of patients with mood or psychotic diagnoses in the 30 days prior to medication initiation was examined since the limited prior literature concerning lithium and mortality is not restricted to bipolar disorder | patients with possible non-psychiatric indications for valproate or lithium; initiated lithium or valproate on an ‘as needed’ basis or both medications simultaneously, or resided outside the USA. | no significant change in suicidal behaviour on lithium, but increased risk of suicide death after discountinuation of lithium |
| Reference Number | Main Author | Study Design | Sample Size | Ketamine (Dose) | Control (Dose) | Inclusion Criteria | Exclusion Criteria | SI-Scale | Main Findings |
|---|---|---|---|---|---|---|---|---|---|
| [43] | Grunebaum et al., 2017 | Double-blind randomised trial | N = 16 K = 7 C = 9 | 0.5 mg/kg infusion + current psychotropics except for benzodiazepines | Midazolam 0.02 mg/kg + current psychotropics | Age 18–65 DSM IV BD and MDE scoring HDRS-17 ≥ 16 and SSI ≥ 4 | unstable medical or neurological illness, significant (ECG) abnormality, pregnancy or lactation, current psychosis, history of ketamine abuse or dependence, other drug or alcohol dependence within 6 months, suicidality due to binge substance use or withdrawal, prior ineffective trial of or adverse reaction to ketamine or midazolam, daily opiate use > 20 mg oxycodone or equivalent during the 3 days pre-infusion, score < 25 on the Mini Mental State Exam18 (for subjects > 60 years old) | SSI assessed at screening, baseline (day before infusion), 230 min post-infusion, day 1, and weeks 1–6 of follow-up. | Mean reduction of SSI 24 h after ketamine infusion was almost 6 points greater than after midazolam, although this was not statistically significant. |
| [44] | Fineberg et al., 2023 | RCT | N = 22 K = 10 M = 12 | 0.5 mg/kg | Midazolam 0.04 mg/kg | 21–60 yrs current suicidal ideation borderline personality disorder | Current acute risk of suicide Psychotic disorder Substance abuse Current intake of topiramate, lithium, lamotrigine Exposure to ketamine in the past year | BSS | Ketamine did not lead to a significant decrease in suicidal ideation compared to midazolam |
| [45] | Phillips et al., 2020 | Double-blind randomised cross-over comparison | N = 37 | 0.5 mg/kg | Midazolam 0.03 mg/kg | Age 18–65 MDD DSM-IV TRD MADRS ≥ 25 Item 10 MADRS-SI ≥ 2 | history of substance use disorder, body mass index ≥ 35 and unstable medical conditions. | MADRS-SI | Greater reduction of SI 2 h and 7 days post infusion, with greatest effect at 7 days. SI scored did not differ at 24 h Scores were not assessed 24 h–7 days. |
| [46] | Abbar et al., 2022 | Double-blind randomised placebo controlled trial | N = 156 K = 73 C = 83 | Two 0.5 mg/kg infusions, 24 h apart | Two placebo 0.9% saline infusions 24 h apart | Age ≥ 18 SSI > 3 | Psychotic disorders schizoid or schizotypic personality disorders; presence of psychotic symptoms at initial interview; substance dependence; positive urine screening for illicit substances; pregnancy or breastfeeding; unstable somatic condition; known or suspected contraindication for ketamine; clinically important anomalies found during clinical examination, biological tests or electrocardiogram; non-stabilised hypertension or hypertension > 180/100; concomitant electroconvulsive therapy; current participation or participation within the past three months in another interventional study; patients under judicial protection or guardianship. | Clinician rated SSI score Full suicidal remission assessed as SSI < 3 | 63.0% reached full remission) three days after two infusions in the ketamine group in comparison with 31.6% in the placebo group. This effect was rapid, with 43.8% remission only two hours after the first infusion versus 7.3% in the placebo group. Until week 6, the ketamine arm continued to have better full suicidal remission than the placebo arm although this was not significant at week 6 owing to reduced suicidality in the placebo group over time |
| [47] | Canuso et al., 2018 | Double-blind randomised placebo controlled study | N = 86 K = 36 C = 32 | Esketamine 84 mg twice weekly for 4 weeks + standard of care medication | Placebo Twice weekly for 4 weeks + standard of care medication | Age 19–64 MDD-DSM IV without psychotic features Affirmative response to MINI question B5 and B9 MADRS ≥ 22 | current diagnosis of bipolar disorder, moderate to severe substance use disorder, intellectual disability, antisocial personality disorder, borderline personality disorder, or a current or past diagnosis of a psychotic disorder. | MADRS-SI Clinician global judgement of suicide risk | Esketamine group had significantly greater improvement in score on the MADRS suicidal thoughts item 4 h after first dose but not at 24 h or at double-blind end point-day 25. Analysis of the clinician global judgment of suicide risk showed numerically greater, but not statistically significant, decreases in ratings 4 and 24 h after the first dose. |
| [48] | Grunebaum et al., 2017 | RCT | N = 80 K = 40 C = 40 | 0.5 mg/kg + current psychiatric medication except benzodiazepines | Midazolam 0.02 mg/kg + current psychiatric medication except benzodiazepines | 18–65 yrs MDD HDRS-17 ≥ 16 and SSI ≥ 4 | unstable medical or neurological illness, significant ECG abnormality, pregnancy or lactation, current psychosis, history of ketamine abuse or dependence, other drug or alcohol dependence within six months, suicidal ideation due to binge substance use or withdrawal, prior ineffective trial of or adverse reaction to ketamine or midazolam, daily opiate use greater than 20 mg oxycodone or equivalent during the three days pre-infusion, score < 25 on the Mini Mental State Exam (25) for persons > 60 years old, lack of capacity to consent or inadequate understanding of English. | Clinician rated SSI | A single ketamine infusion was associated with greater reduction in suicidal thoughts at 230 min and 24 h post infusion, compared to midazolam control |
| [49] | Fu et al., 2020 | Double-blind placebo controlled randomised study | N = 226 K = 114 C = 112 | 84 mg esketamine nasal spray twice weekly for 4 weeks + standard of care | Placebo spray twice weekly for 4 weeks + standard of care | 18–64 MDD-DSM V with MADRS > 28 and in need of acute psychiatric hospitalization due to imminent suicide risk | bipolar disorder, obsessive-compulsive disorder, antisocial personality disorder, borderline personality disorder, substance or alcohol use disorder within 6 months prior to screening, diagnosis of psychotic disorder | SIBAT | At the 24-h endpoint, patients in both treatment groups experienced improvement in the severity of their suicidality as measured by CGI-SS-r, though there was no statistically significant difference between treatment groups Improvement in severity of suicidality was also observed in both treatment groups at the end of double-blind treatment. |
| [50] | Zolghadriha et al., 2024 | RCT | N = 64 K = 32 C = 32 | 0.5 mg/kg | Saline | 25–60 yrs old MDD-DSM 5 MARDS > 25 TRD | uncontrolled hypertension, active substance abuse, or a history of psychosis | BSI | Decrease in suicidal ideation was observed specifically in the group that received ketamine treatment |
| [51] | Ionescu et al., 2020 | RCT | N = 227 K = 114 C = 113 | 84 mg of esketamine twice weekly for four weeks+ standard of care | Placebo + standard of care | 18–64 MDD-DSM V MADRS > 28 Suicidal ideation with intent | bipolar disorder, obsessive-compulsive disorder, antisocial personality disorder, borderline personality disorder, substance or alcohol use disorder within 6 months prior to screening, diagnosis of psychotic disorder | SIBAT | Patients in both treatment groups experienced rapid reduction in the severity of their suicidality, the between-group difference was not statistically significant |
| [5] | Ahmed et al., 2023 | RCT | N = 36 K = 18 C = 18 | Two infusions of 0.5 mg/kg ketamine one week apart | Two infusions of saline one week apart | 18–65 TRD MDD-EMA Current suicidal risk | major unstable medical condition or neurological illness, the presence of perceptual disturbance, a history of sensitivity to ketamine, a history or present substance use, and an ECT treatment in the previous 3 weeks | Suicide probability scale | Significant reduction in SPS in ketamine group, no change in placebo group 1 week after finishing 2 infusions. |
| [52] | Sinyor et al., 2018 | Randomised controlled trial | N = 9 K = 5 C = 4 | 0.5 mg/kg 6 infusions over 12 days Adjunct to treatment | Midazolam 0.045 mg/kg 6 infusions over 12 days | 18–65 MDD SSI or CSSRS > 0 MDD did not have to be treatment resistant No minimum required depression score | (1) current or past manic symptoms; (2) current or past psychotic symptoms; (3) current substance or alcohol dependence or substance abuse within the past month; (4) pervasive developmental disorder or dementia; (5) unstable medical illness; (6) medical condition that would contraindicate the use of ketamine/midazolam or affect their metabolism; (7) current treatment with ketamine; (8) any treatment that might contraindicate the use of study medications (9) concomitant electroconvulsive therapy; and (10) pregnancy. | SSI | Subjects in both the ketamine and midazolam groups experienced a rapid reduction in SI, the reduction in the ketamine group appeared to be somewhat larger, more robust, and longer-lasting (up to 42 days) with SSI scores increasing in the midazolam group after the second infusion. |
| [53] | TP Su 2023 | RCT | N = 84 K = 42 C = 42 | 0.5 mg/kg Single infusion | 0.045 mg/kg Midazolam | 20–64 MDD-DSM V TRD MADRS item 10 ≥ 4 | major medical or neurological diseases or a history of alcohol or substance use disorders in current study | CSSRS-ISS MADRS item 10 PANSI | More patients receiving ketamine reached full remission of suicidal ideation from day 2 to day 5 compared with those receiving midazolam. Significant antisuicidal effects of low-dose ketamine infusion at least up to day 5. |
| [54] | Price 2014 | RCT | N = 57 K = 36 C = 21 | 0.5 mg/kg Single infusion | Midazolam 0.045 mg/kg | MDD TRD Moderate-severe depression Psychotropic medication free | Serious and imminent suicidal or homicidal risk Psychotic disorder Bipolar disorder Substance abuse | Explicit SI composite score (BSS, MARDS-S, QIDS-SI) | Tweny-four hours postinfusion, ketamine-treated patients exhibited large, rapid reductions in explicit suicidal cognition, which were significantly greater than reductions observed in midazolam-treated patients. Ketamine eradicated all self-report and clinician-rated indications of suicidal ideation in 53% of patients, compared to 24% of patients receiving midazolam |
| [55] | Fan et al., 2016 | RCT | N = 39 K = 20 C = 19 | 0.5 mg/kg | Midazolam 0.05 mg/kg | 18–70 First diagnosed with cancer 3 months | cardiorespiratory diseases; drug addiction history or sedative–hypnotic drug(s) use; neuropsychiatric or cognitive diseases or a related treatment history; suicidal attempts or ideation before cancer diagnosis; and family history of psychiatric history. | BSS MARDS-SI | Suicidal ideation significantly lower in ketamine group at day 1 and day 3 post infusion |
| [56] | Ionescu et al., 2019 | RCT | N = 26 K = 13 C = 13 | 0.5 mg/kg Six infusions over three weeks | Saline Six infusions over three weeks | 18–65 MDD-DSM IV HDRS ≥ 20 C-SSRS > 1 for 3 months + HDRSi12 ≥ 4 | (1) pregnancy; (2) unstable medical illness; (3) bipolar disorder; (4) past multiple adverse drug reactions; (5) psychotic illness; (6) substance use disorder within the past year; (7) positive urine toxicology; (8) past history of ketamine abuse; (9) SI requiring immediate hospitalization or indicating immediate | C-SSRS | Ketamine treatment did not have a significant advantage in terms of reducing SI. |
| [57] | Murrough et al., 2015 | RCT | N = 24 K = 12 C = 12 | 0.5 mg/kg Single infusion | Midazolam 0.045 mg/kg Single infusion | 18–80 MADRS-SI ≥ 4 Range of psychiatric diagnoses | C-SSRS 4 or 5 Schizophrenia or other primary psychotic disorder, current psychotic or manic symptoms, substance use disorder within 1 month of screening, | BSS MADRS-SI | BSS score was not significantly different between the treatment groups 24 h post treatment A significant effect of treatment on BSI score emerged at 48 h following intervention. 24 h following treatment, MADRS-SI score was significantly lower in the ketamine group compared to midazolam group |
| [58] | Feeney et al., 2021 | RCT | N = 56 K = 40 C = 16 | 0.1 mg/kg 0.5 mg/kg 1.0 mg/kg | Midazolam 0.045 mg/kg | 18–70 MDD of at least 8 weeks prior to screening TRD MADRS > 20 MADRS-SI ≥ 2 | Imminent risk of suicide More than seven adequate antidepressant trials in current episode | MADRS-SI | Those who had received IV ketamine had a significant reduction in suicidal ideation compared to those who had received IV midazolam. However, when participants with an apparent early anti-suicidal response to the infusion were analyzed, treatment and placebo groups did not differ significantly at days 5, 7, 14 or 30 post infusion. |
| [59] | Domany et al., 2020 | RCT | N = 18 K = 9 C = 9 | 0.2 mg/kg over 5 min Single infusion | Saline Single infusion | 18–65 MDD Clinically significant suicidal ideation | Psychotic disorder Anorexia nervosa Substance abuse Pregnancy, post-partum | BSS MARDS-SI | A reduction in suicidal ideation was noted at 90–180 min Ninety minutes after infusion, 88% of the ketamine group had achieved remission of suicidal ideation compared with 33% in the placebo group |
| [60] | Zeng et al., 2025 | RCT | N = 40 K = 20 C = 20 | Esketamine 0.5 mg/kg + ECT | Propofol 1.5–2.5 mg/kg + ECT | 18 and 65 years TRD MDD (DSM-IV) HAMD-17 scores ≥ 17. | (1) Other psychiatric disorders, However, individuals with comorbid anxiety disorder, obsessive-compulsive disorder, or eating disorder were allowed provided that these conditions were not the primary presenting issue; (2) severe physical disease; (3) pregnancy, planning to get pregnant, or breastfeeding; (4) having received ECT or repetitive transcranial magnetic stimulation within the previous three months; and (5) having allergies to the anesthetic agents. | SSI-part1 | Antisuicidal effects in SSI-part 1 scores did not differ significantly between the two groups |
| [61] | Hu et al., 2016 | RCT | N = 30 | Four weeks escitalopram 10 mg/day + single infusion 0.5 mg/kg ketamine | Four weeks escitalopram 10 mg/day + single saline infusion | Outpatients with non-psychotic MDD HAMD ≥ 24 ≥1 item 3 HAMD 18–60 | Psychotic, bipolar, OCD disorders Substance abuse Suicide attempt in the current episode | QIDRS-SR item 12 | Escitalopram+ketamine was associated with significantly lower QIDRS-SR suicidality item scores from 2 to 72 h |
| [62] | Burger et al., 2016 | RCT | N = 10 K = 3 C = 7 | 0.2 mg/kg single ketamine infusion over 2 min | Saline over 2 min | Patients presenting to military ED with depression and suicidal thinking BSS > 4 BHS > 8 | Psychotic disorder Bipolar disorder Substance abuse | BSS | 67% of subjects who received ketamine presented significant improvement in suicidal ideation in the emergency department (4 h) |
| [63] | Jones et al., 2024 | RCT | N = 28 K = 17 C = 11 | 50 mg IN ketamine | Saline | 21–60 Current SI Past suicide attempt MDD | Psychotic disorders Substance abuse-excluding alcohol | SSI MARDS-SI | No significant improvement was observed in SSI Significant response observed in MARDS-SI |
| [59] | Domany et al., 2021 | RCT | N = 30 K = 15 C = 15 | 40 mg IN ketamine | Saline | Required psychiatric hospitalisation due to suicidal risk | Schizophrenia spectrum disorders Dissociative disorders Cognitive disorders Substance abuse | BSS MARDS-SI | A significant reduction in suicidal ideation was observed 4 h after administration 80% achieved suicidal remission compared to 33% in placebo group |
| Reference Number | Main Author | Study Design | Sample Size | Control | FOLLOW UP | Inclusion Criteria | Exclusion Criteria | Main Findings |
|---|---|---|---|---|---|---|---|---|
| [64] | Gunilla Ringbäck Weitoft 2014 | A population-based cohort study (Sweden) | Total sample = (n = 26,046) 2138 (8.2%) 13 suicide deaths 42 suicide attempts | Those who did not die specifically from suicide and those who did not have a hospital-stay because of suicide attempt. | For prescription refill analysis, patients were followed for 12 three-month periods (quarters 1, 3, 5, 7, 9, and 11). For re-hospitalisation analysis, the follow-up period started from day 183 after the index care event and lasted until day 365. | Adults (18–79 years old) Patients diagnosed with schizophrenia (ICD-10: F20) or schizoaffective syndromes (F25) Patients who received hospital or specialized outpatient care for schizophrenia in Sweden between 2006 and 2009 | Patients who died from other causes before the fictitious date were excluded. | Clozapine users had a lower odds ratio (OR) for death by suicide (OR = 0.45, 95% CI: 0.20–0.98) and for attempted suicide (OR = 0.44, 95% CI: 0.28–0.70) compared to haloperidol users. Clozapine users also had a lower risk of re-hospitalization and higher prescription refill rates. A calculation suggests that using clozapine instead of first-generation antipsychotics could have prevented 95 suicide attempts during the study period. |
| [65] | van der Zalm 2021 | cohort study (Denmark) | The incidence cohort included 22,110 The prevalence cohort included 50,881 Clozapine patients 1677 | No control group | The study followed the cohort over a long-term period, taking data from 1995 (when the Danish National Prescription Registry started) up to 2015 (the last available data in the Causes of Death Register). | Patients had to have a diagnosis of schizophrenia or a related psychotic disorder: Patients aged 15 to 100 Patients had to be inhabitants of Denmark with a first diagnosis between 1 January 1995, and 30 June 2013 (incidence cohort). A prevalence cohort included all individuals ever diagnosed with up to 30 June 2013. | Migrants to Denmark were excluded | Current use of clozapine was associated with a lower risk of suicide compared to other antipsychotics. In the prevalence cohort, users of other antipsychotics had a significantly higher risk of suicide compared to clozapine users (HR_adj = 2.20; 95% CI 1.35–3.59). Increased Suicide Risk After Clozapine Discontinuation Cumulative use of clozapine for up to 1 year was associated with a higher risk of suicide compared to other antipsychotics (HR_adj = 0.65; 95% CI 0.46–0.91). |
| [66] | Taipale 2020 | cohort study—(Sweden and Finland) | Finnish cohort: 61,889 individuals with schizophrenia. Swedish cohort: 29,823 individuals with schizophrenia. | No control group | follow-up periods of up to 22 years (Finland) and 11 years (Sweden). | ICD-10 codes (F20, F25) and older equivalents Finland: All individuals treated for schizophrenia in inpatient care from 1972 to 2014. Sweden: All individuals aged 16–64 with a recorded schizophrenia diagnosis between 2006 and 2013. Participants were not institutionalized for long-term care. | Delusional disorder (F22) and nonspecific psychosis (F29) were excluded to maintain a homogeneous cohort. In the incident cohort, individuals were excluded if they had used antipsychotics in the year before their first schizophrenia diagnosis. | Clozapine was the only antipsychotic consistently associated with a decreased risk of suicidal outcomes: Finnish cohort: Hazard Ratio (HR) = 0.64 (95% CI: 0.49–0.84). Swedish cohort: HR = 0.66 (95% CI: 0.43–0.99). No other antipsychotic showed a statistically significant reduction in suicide risk. |
| [67] | Taipale 2021 | register-based cohort study | Finland cohort: 62,250 individuals with schizophrenia) | No control group | Follow-up duration: Up to 20 years (median: 14.1 years | Diagnosis of Schizophrenia Defined using ICD-10 codes F20 (schizophrenia) and F25 (schizoaffective disorder) Older ICD versions (ICD-9 & ICD-8: code 295) were also used to identify cases in earlier years Nationwide Cohort in Finland Included all individuals hospitalized for schizophrenia in Finland between 1972 and 2014 | Psychotic disorders other than schizophrenia In the incident cohort (first-episode patients), individuals were excluded if they had used antipsychotics in the year before their first schizophrenia-related hospitalization. | The adjusted hazard ratio (aHR) for suicide mortality was 0.21 (95% CI: 0.15–0.29) for clozapine, indicating a 79% reduction in suicide risk compared to non-use. |
| [68] | Hassan 2021 | Prospective cohort study (Canada) | 103 participants | No control group | average follow-up duration of 17.4 ± 7.4 months | Participants were included if they: Were older than 18 years. Had a diagnosis of schizophrenia or schizoaffective disorder. Were fluent in English. Were being treated as outpatients at the Centre for Addiction and Mental Health (CAMH), Toronto. | Participants were excluded if they had psychosis due to traumatic brain injury or a general medical condition and/or were not fluent in English. | The study found that clozapine did not show a significant difference in reducing suicidal ideation compared to other antipsychotics. Here are the exact results: Mean Beck Scale for Suicidal Ideation (BSS) score at follow-up: Clozapine group: 1.93 ± 4.63 Non-clozapine group: 1.67 ± 4.3 Reduction in BSS score: Clozapine group: −0.93 Non-clozapine group: −0.8 p = 0.847 (not statistically significant) |
| [25] | Chen 2024 | Cohort study (Taiwan) | Study population = 43,025 Of them, we selected those who received clozapine (clozapine cohort, n = 5800). | For each patient in the clozapine cohort, authors selected two individuals from inpatients with schizophrenia who had never used clozapine after matching them by age, sex, and the year of the index date at a ratio of 1:2 | The study followed up patients from 1 January 2001, to 31 December 2019 (18 years). The mean follow-up period for the study cohort was 7.9 years. | Population: 43,025 inpatients with schizophrenia from Taiwan’s National Health Insurance Research Database (2001–2019). Clozapine group: 5800 patients. Control group: 11,583 non-clozapine users, matched 1:2 by age, sex, and year of index date. Total cohort: 17,383 patients. | Diagnosis of affective psychosis from 2001 to 2019. Missing information on sex and birth date | Clozapine users had a 63% lower risk of suicide mortality compared to non-users (adjusted hazard ratio (aHR) = 0.37, 95% CI: 0.20–0.67, p = 0.001). Dose-dependent effect: Each 10-day increase in clozapine use lowered suicide risk by 26% (aHR = 0.74, p = 0.004). Each 10 defined daily doses (DDDs) of clozapine lowered suicide risk by 31% (aHR = 0.69, p = 0.010). |
| [69] | Gürcan 2024 | Cross sectional study (Turkey) | 122 outpatients with schizophrenia | No control group | No follow up | Single center, diagnosis of schizophrenia (DSM-IV criteria) and who had been receiving clozapine treatment for at least 6 weeks | Not mentioned | Before clozapine: 39.3% of patients had attempted suicide. After clozapine: Only 7.4% attempted suicide (p < 0.001). A total of 32% (39 patients) with prior suicide attempts had no further attempts after clozapine. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waszak, P.M.; Opalko, J.; Olszańska, N.; Zagożdżon, P. Anti-Suicidal Effects of Lithium, Ketamine, and Clozapine—A 10-Year Systematic Review. Pharmaceuticals 2025, 18, 742. https://doi.org/10.3390/ph18050742
Waszak PM, Opalko J, Olszańska N, Zagożdżon P. Anti-Suicidal Effects of Lithium, Ketamine, and Clozapine—A 10-Year Systematic Review. Pharmaceuticals. 2025; 18(5):742. https://doi.org/10.3390/ph18050742
Chicago/Turabian StyleWaszak, Przemyslaw M., Jan Opalko, Natalia Olszańska, and Paweł Zagożdżon. 2025. "Anti-Suicidal Effects of Lithium, Ketamine, and Clozapine—A 10-Year Systematic Review" Pharmaceuticals 18, no. 5: 742. https://doi.org/10.3390/ph18050742
APA StyleWaszak, P. M., Opalko, J., Olszańska, N., & Zagożdżon, P. (2025). Anti-Suicidal Effects of Lithium, Ketamine, and Clozapine—A 10-Year Systematic Review. Pharmaceuticals, 18(5), 742. https://doi.org/10.3390/ph18050742