
A Novel Blockchain-Based Healthcare System Design and Performance Benchmarking on a Multi-Hosted Testbed

 , , , , , , , and
, , , , , , , and (This article belongs to the Section Intelligent Sensors)
Abstract
:1. Introduction
- The Blockchain-enabled healthcare framework implementation and prototype design using on-chain and off-chain scheme is presented. Hyperledger Fabric is used for enacting smart contracts for client communications. A thorough performance evaluation of this prototype is presented herein.
- Performance analysis of the implemented healthcare prototype on a multi-hosted testbed by employing the Google Cloud Platform (GCP).
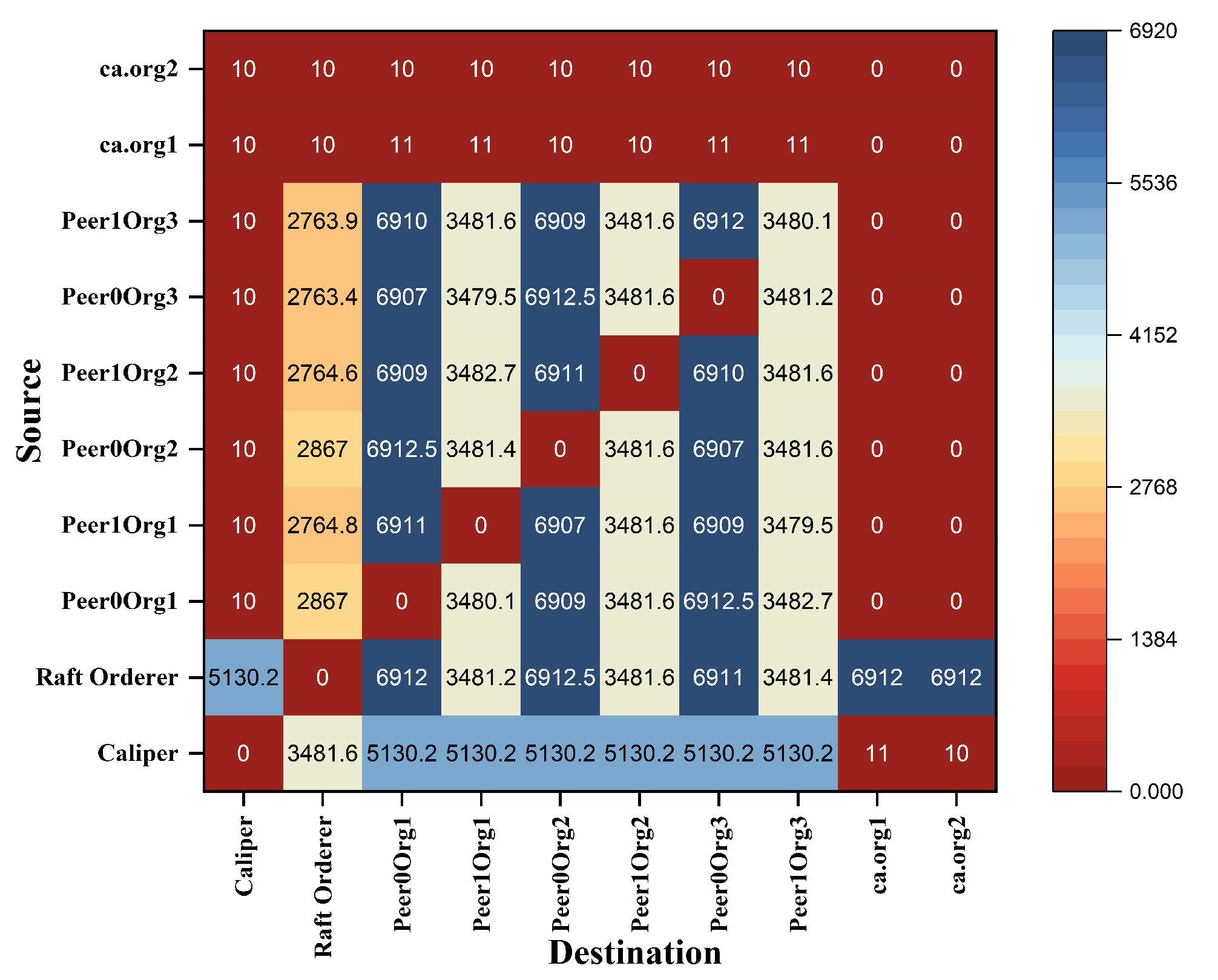
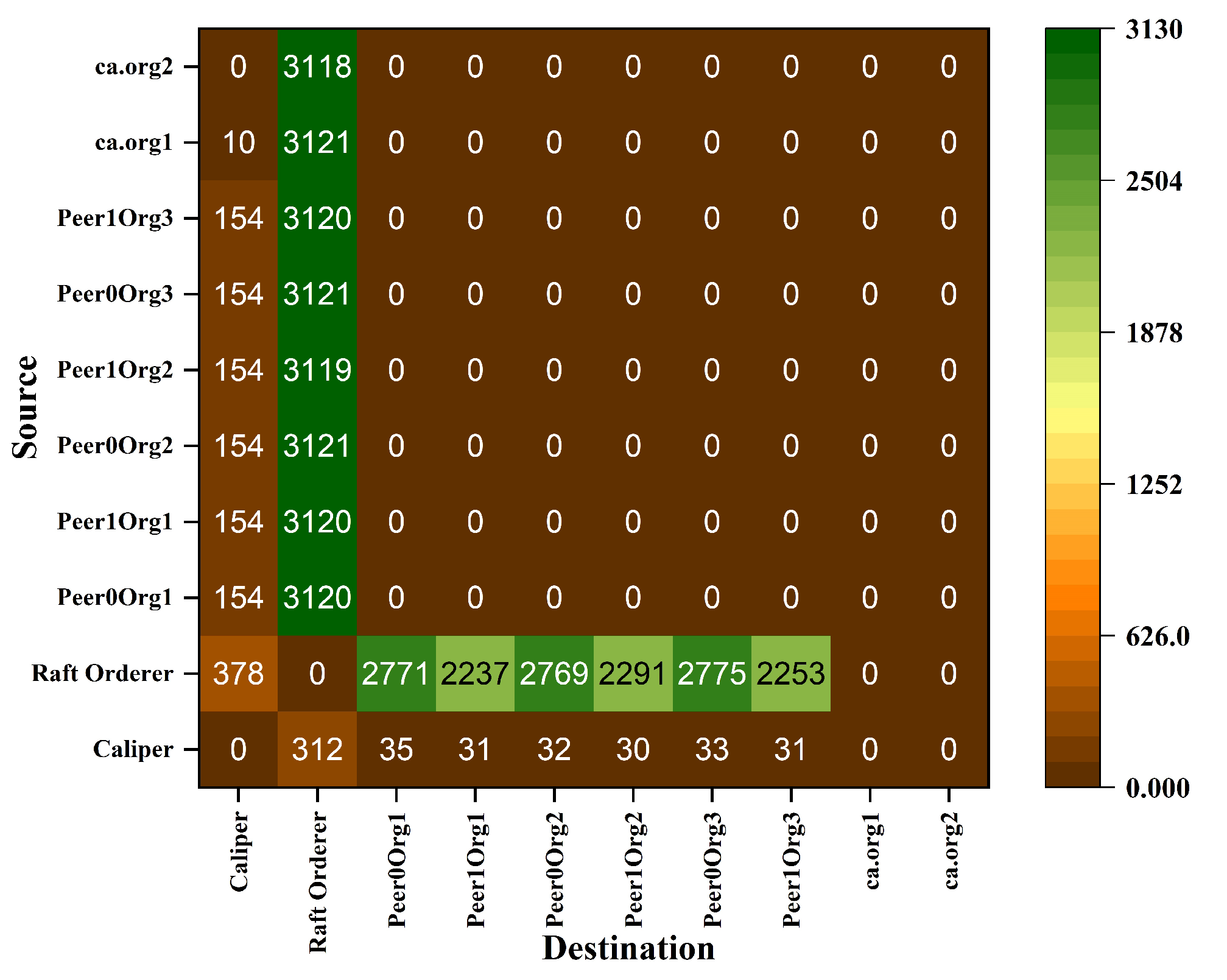
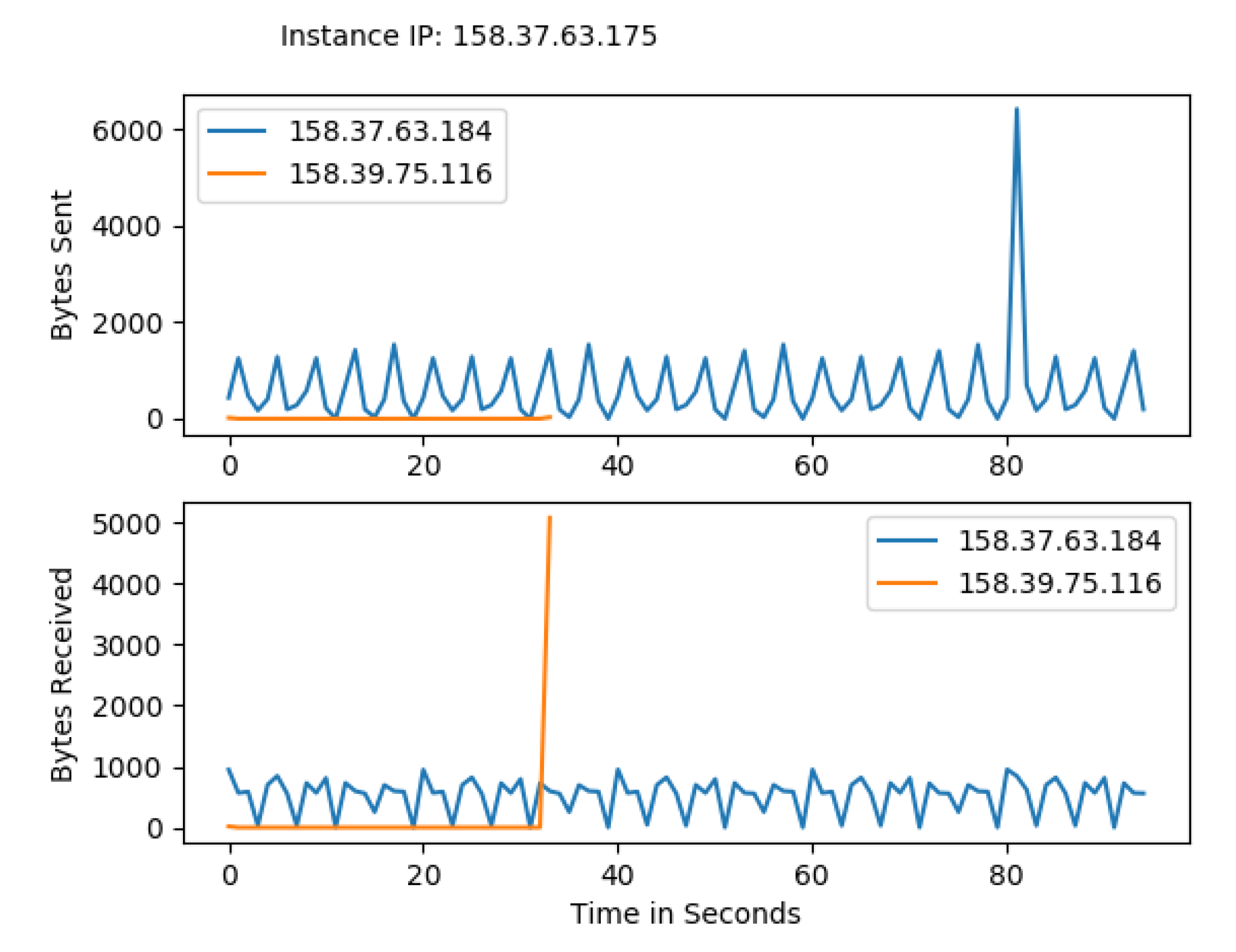
- Analysis of network transactions cost and fair optimized traffic owing to Gossip protocols resulting in a fair and efficient dissemination. Such an attempt is not yet studied for any Blockchain-based healthcare systems.
- The proposed framework enhances the propagation of blocks to all healthcare peers by 8 times faster than actual implementation while decreasing the network bandwidth and increasing throughput by more than 30%.
- Integrated use of the latest and far more reliable transaction orderer services such as Kafka and RAFT unlike SOLO [1].
2. Related Work
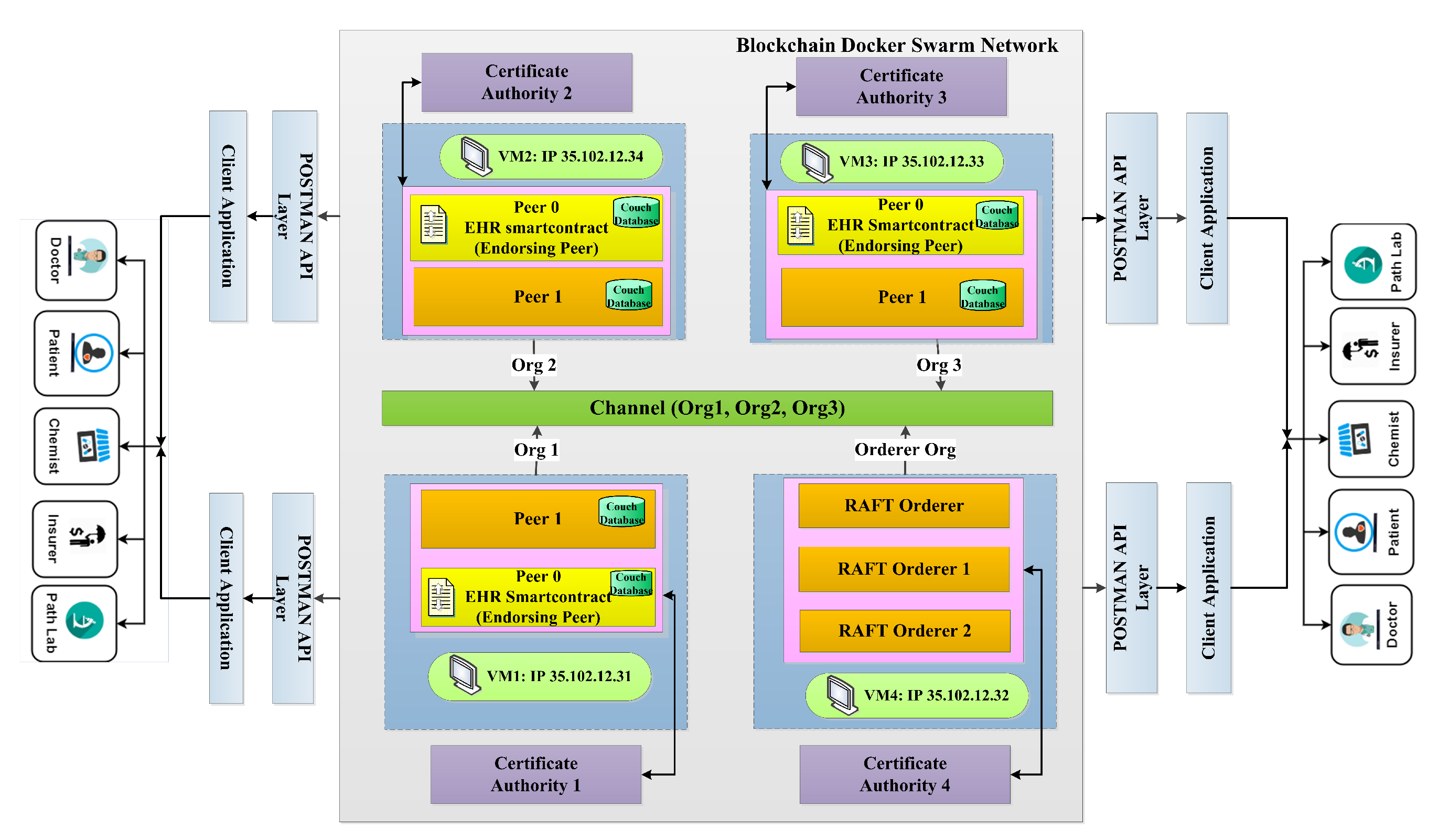
3. System Architecture for the Proposed Framework
3.1. Proposed Network Model
3.2. Proposed Transactions
| Algorithm 1: Algorithm for participant creating, initializing and querying healthcare records (buying, selling medicine and appointment status matching) |
 |
3.3. Proposed Participants, and Assets
- Participants: The individual entities in healthcare organizations such as doctors, patients, chemists, insurers, and path lab are called participants.
- Assets: Doctors as a participant create a prescription asset for the patients. The patient as a participant pays a cash or coin asset for buying medicine, consulting doctors fees, and collecting path lab testing reports. The chemist, as a participant, generates a receipt for the sold drugs. Similarly, the path lab as a participant generates lab test reports as an asset for patients. Assets are tangible or intangible.
- Transactions: A transaction in a healthcare system is a read, write, or update operation that follows the sequence such as instantiated, invoked, endorsed, validated, ordered, committed, and finally broadcasted to the intended users. In our proposed work, three transactions are considered as creating an EHR, initializing the ledger, and querying a healthcare system.
4. Implementation
4.1. Experimental Setup
4.2. Deployment of Virtual Machines and Other Prerequisites
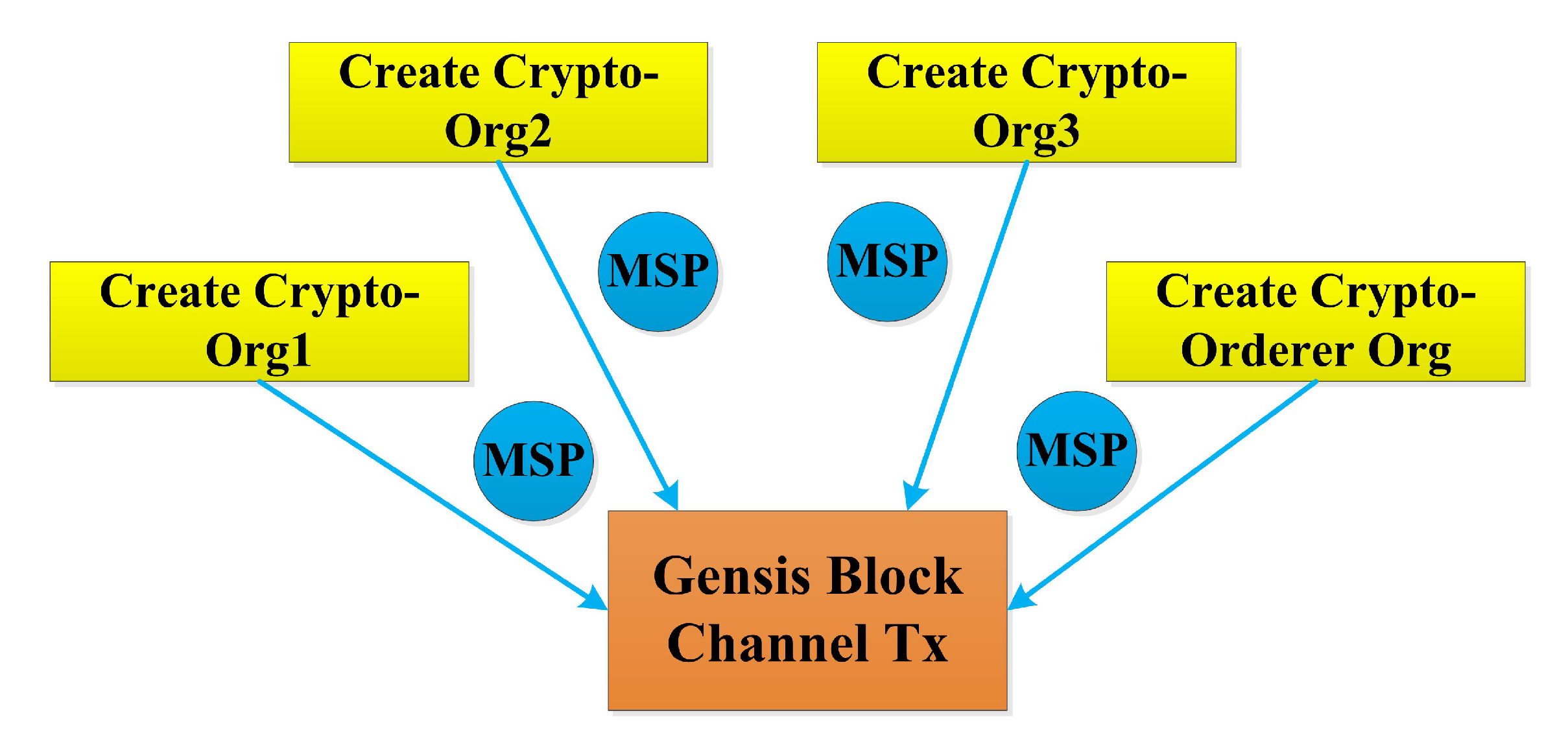
4.3. Crypto Materials for Org 1, Org 2, Org 3 and RAFT Orderer
4.4. Creating Docker Swarm Network

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 |
4.5. Creating Channel Artifacts
 |
4.6. Creating and Joining Channel
4.7. EHR Chaincode Deployment
4.8. Install, Approve, Commit, and Invoke EHR Chain Code
4.9. Commit Chain Code and Invoke Transaction
 |
 |
5. Performance Analysis and Discussion
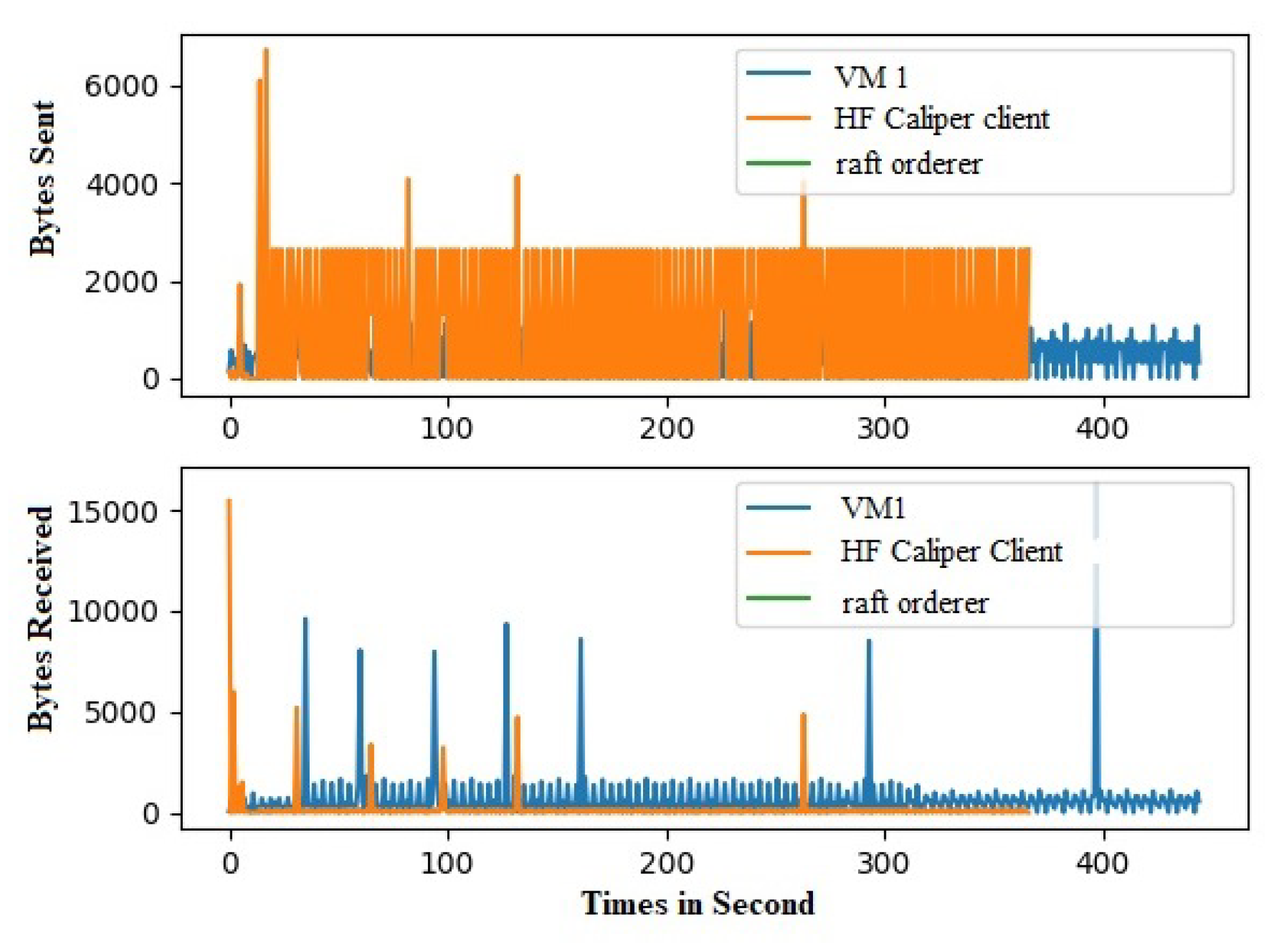
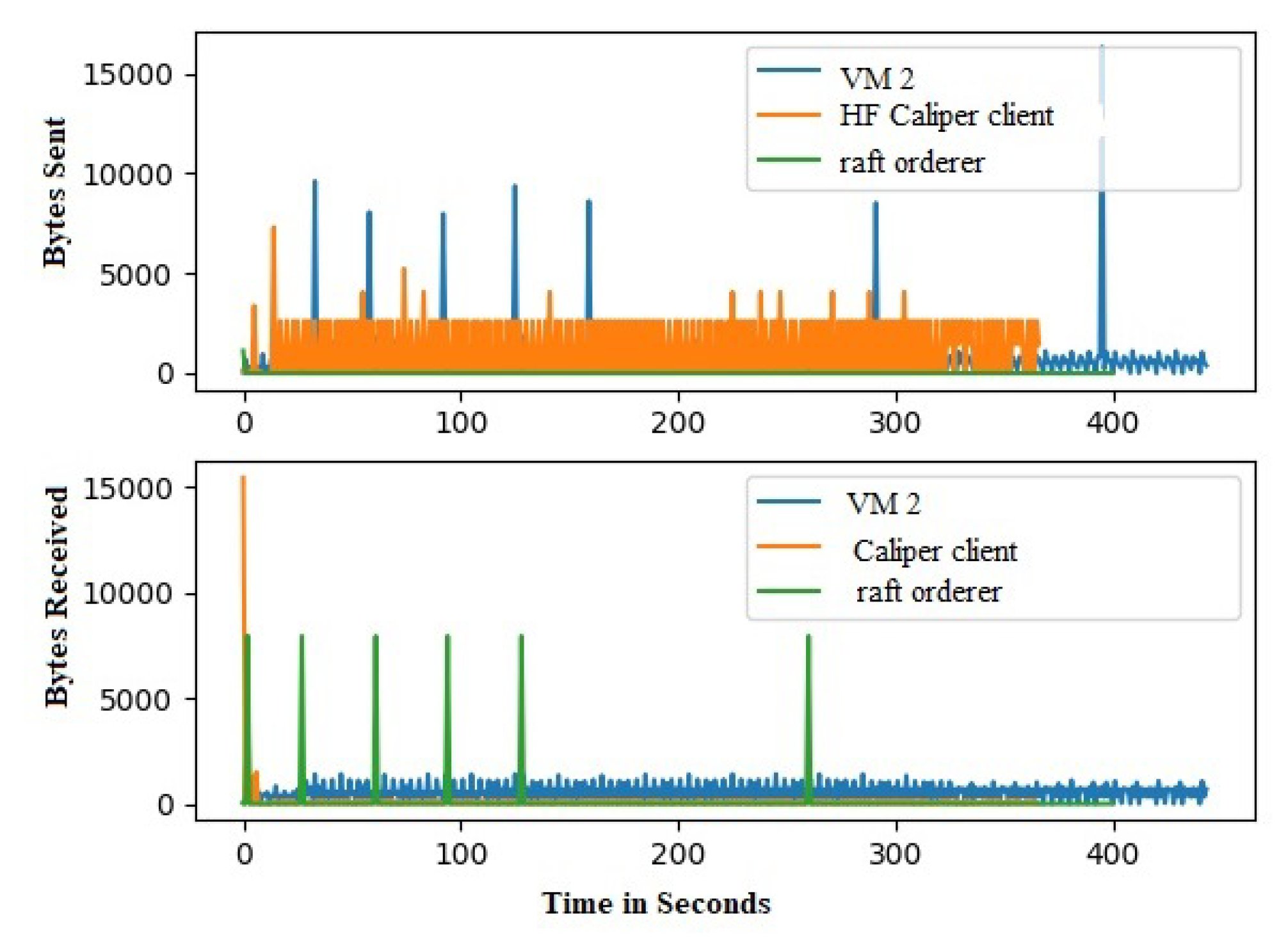
5.1. Measurement of GOSSIP Traffic
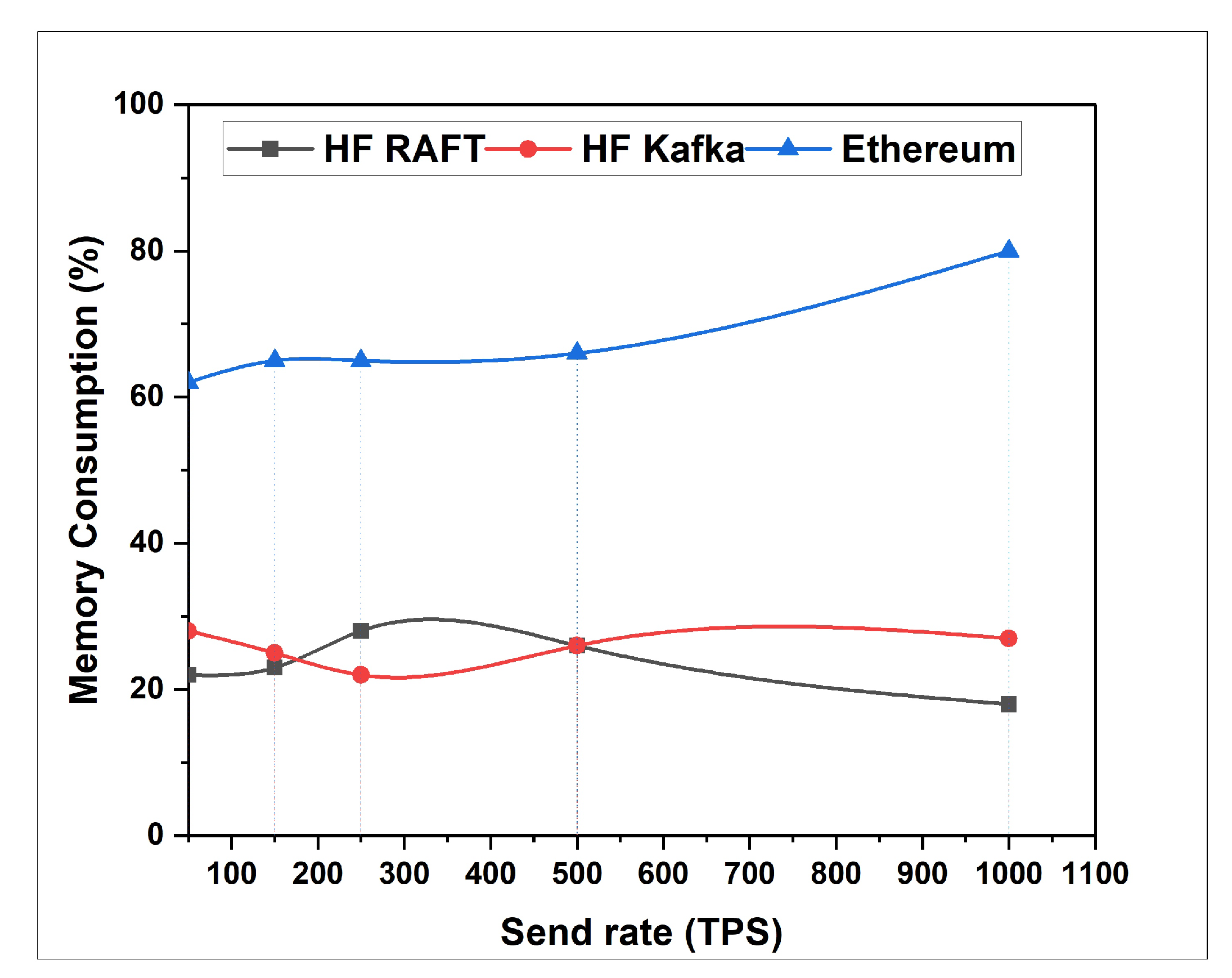
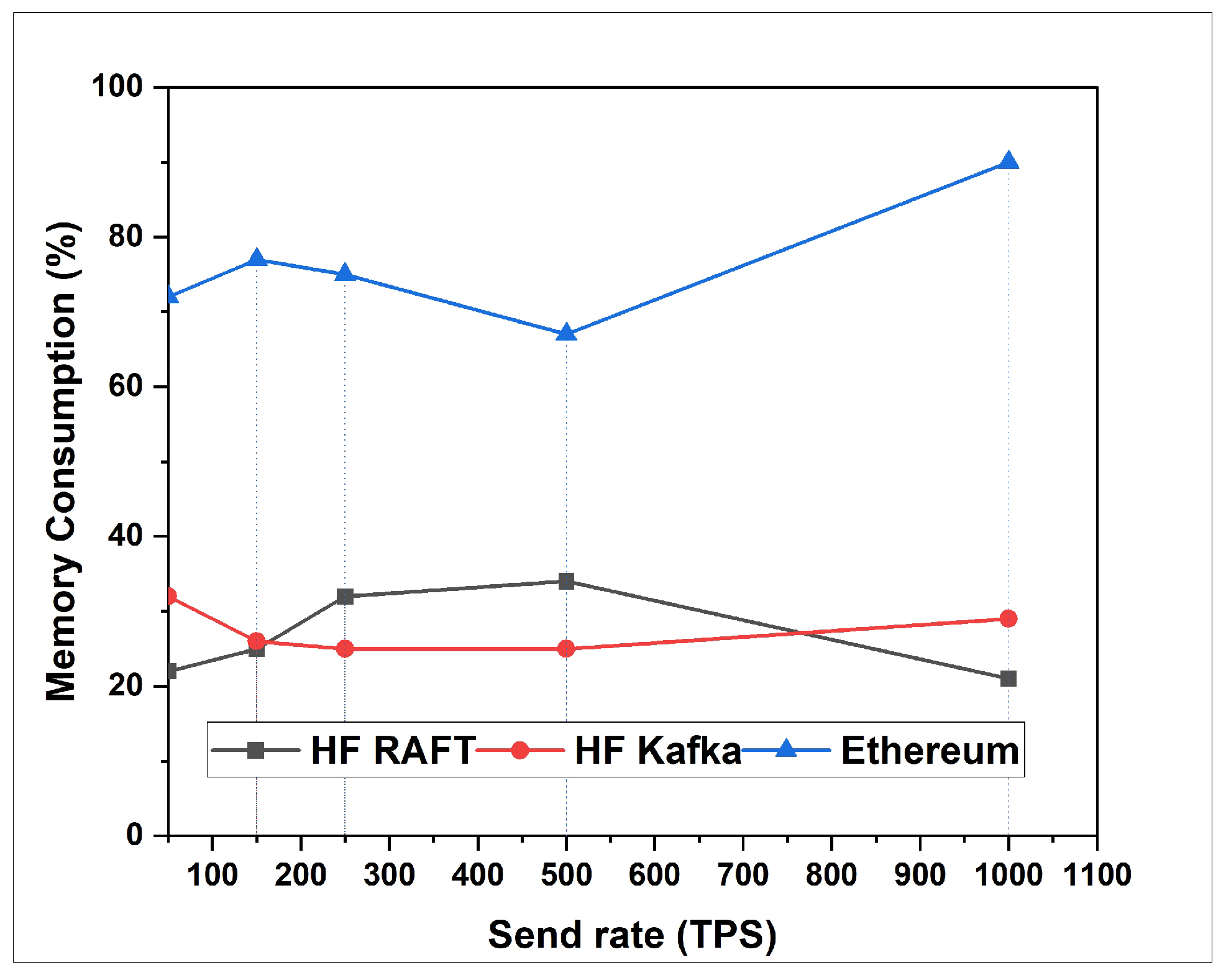
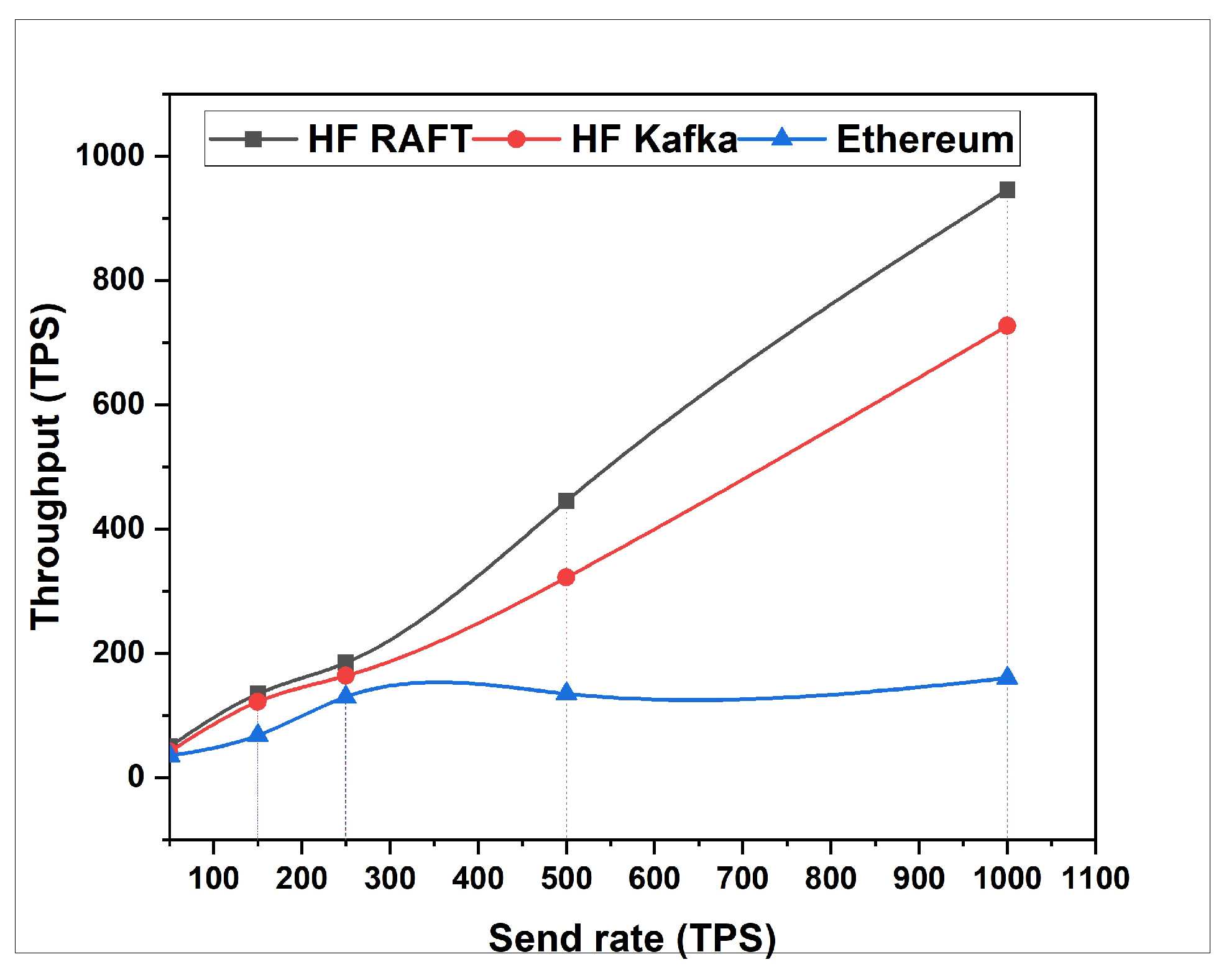
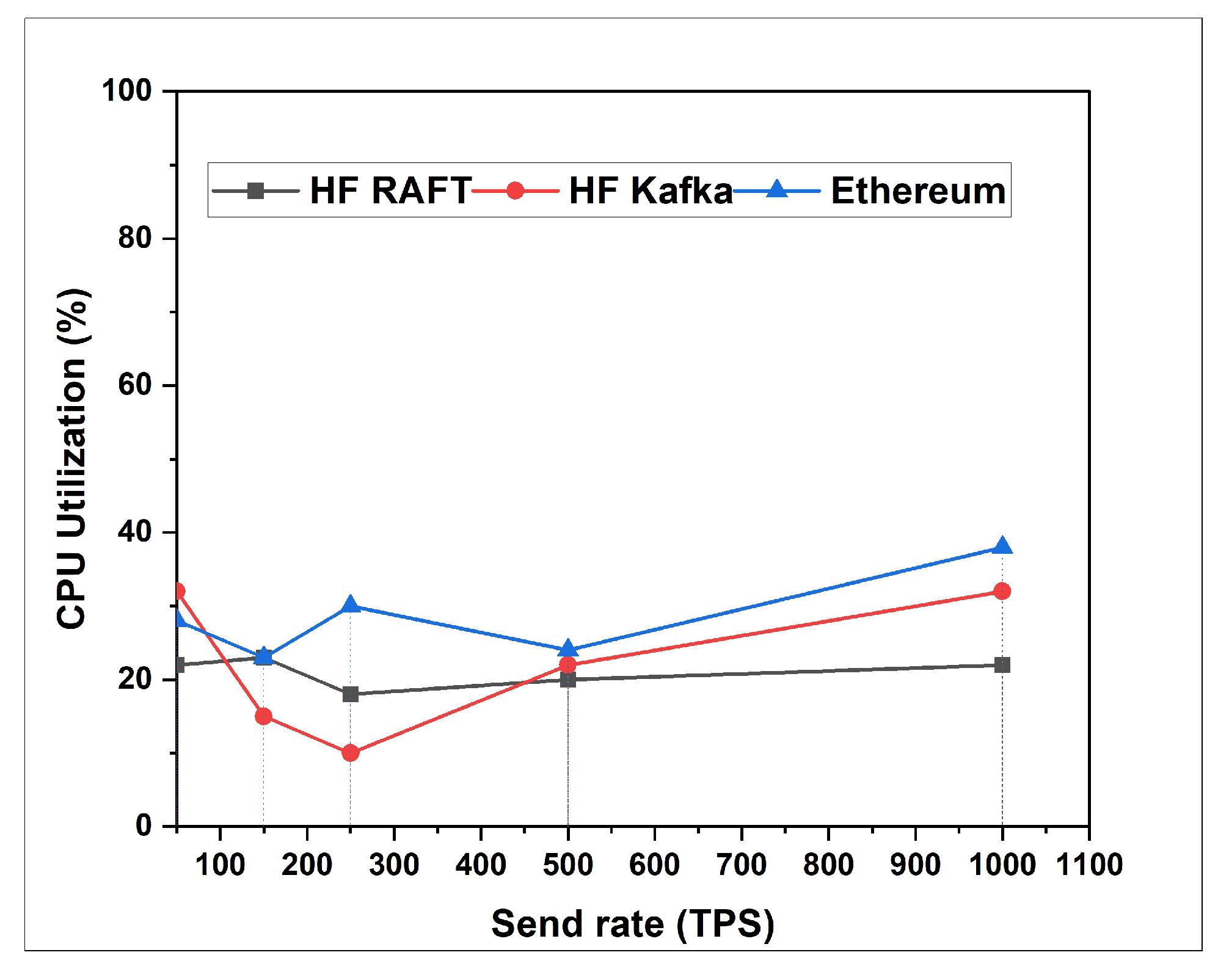
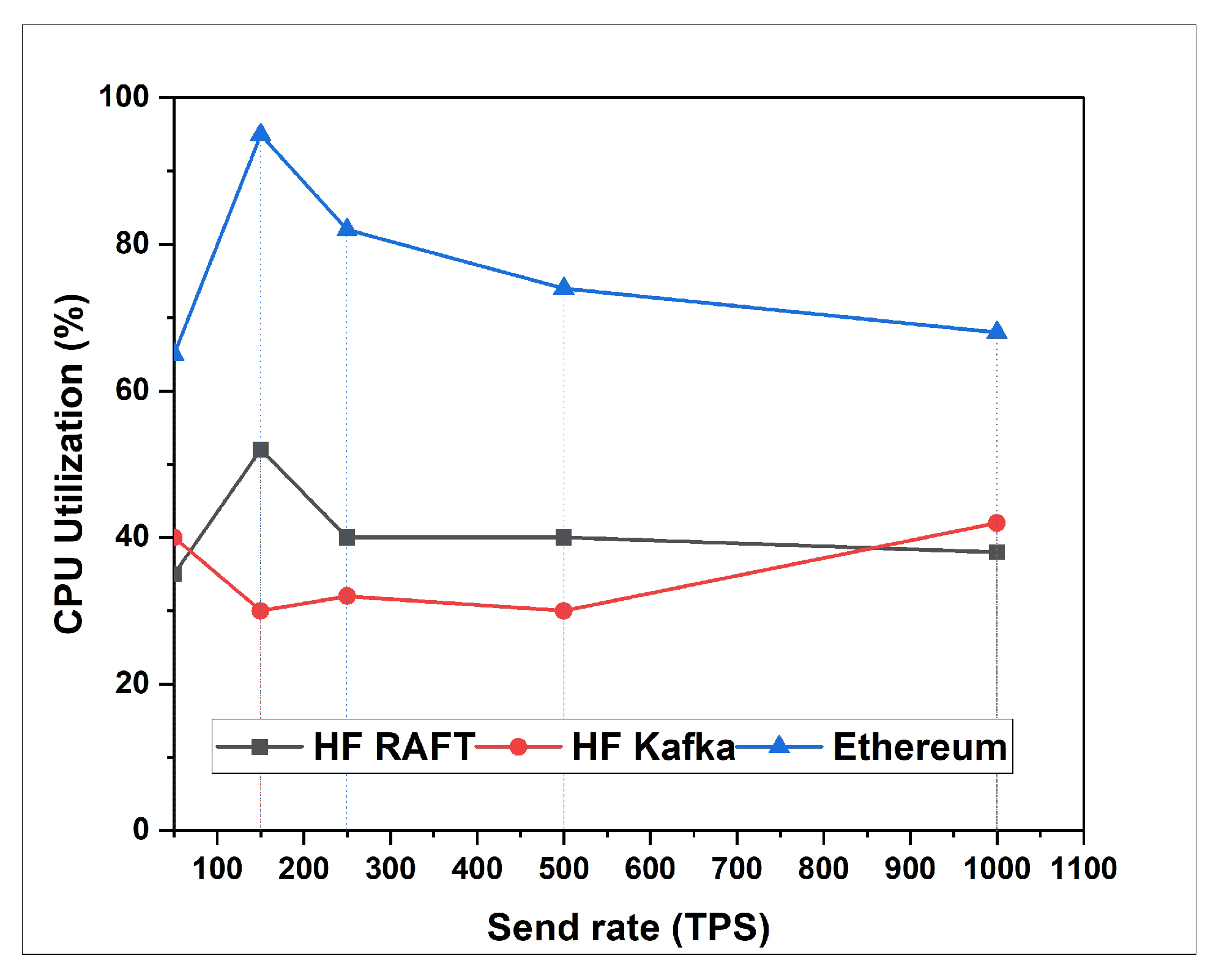
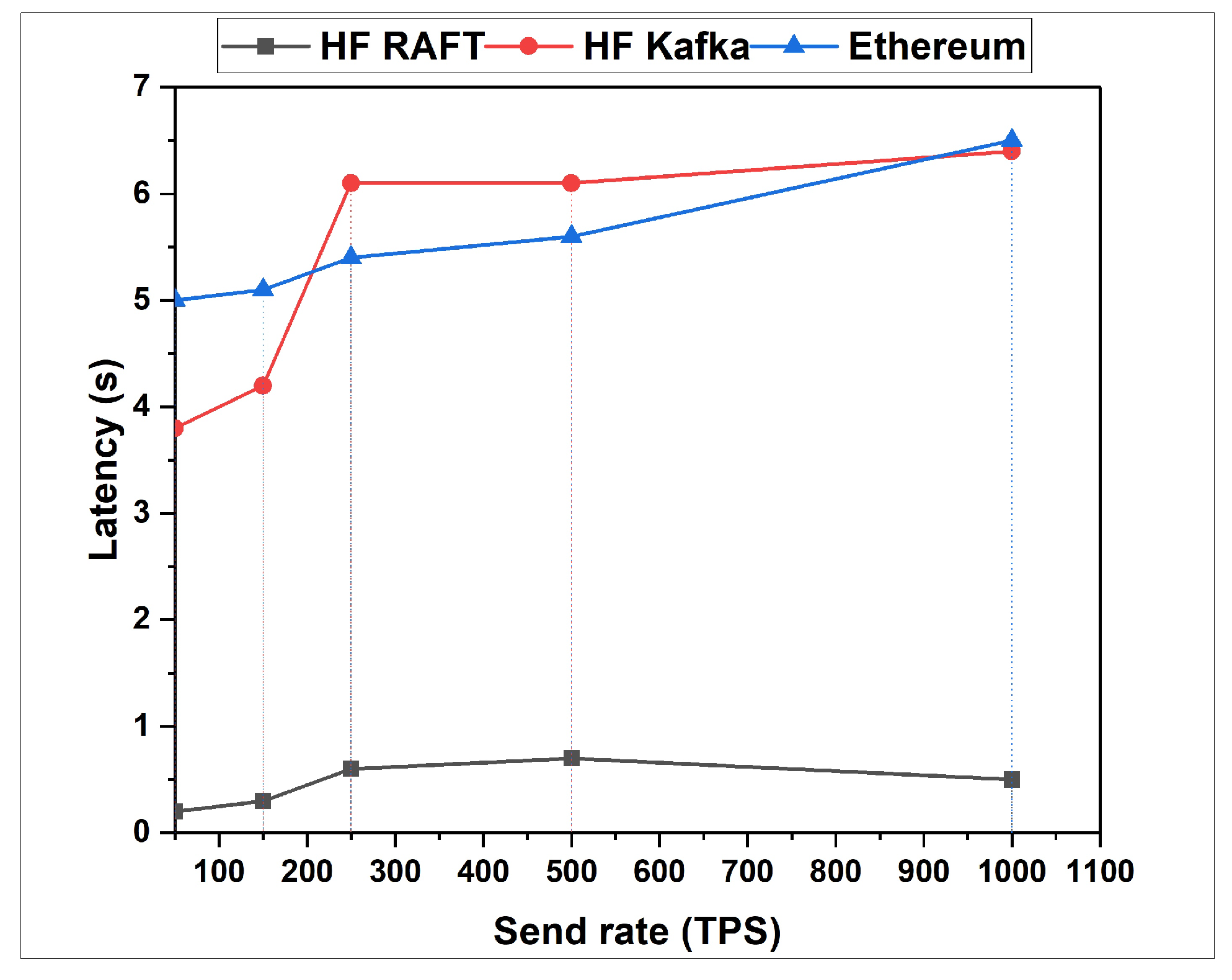
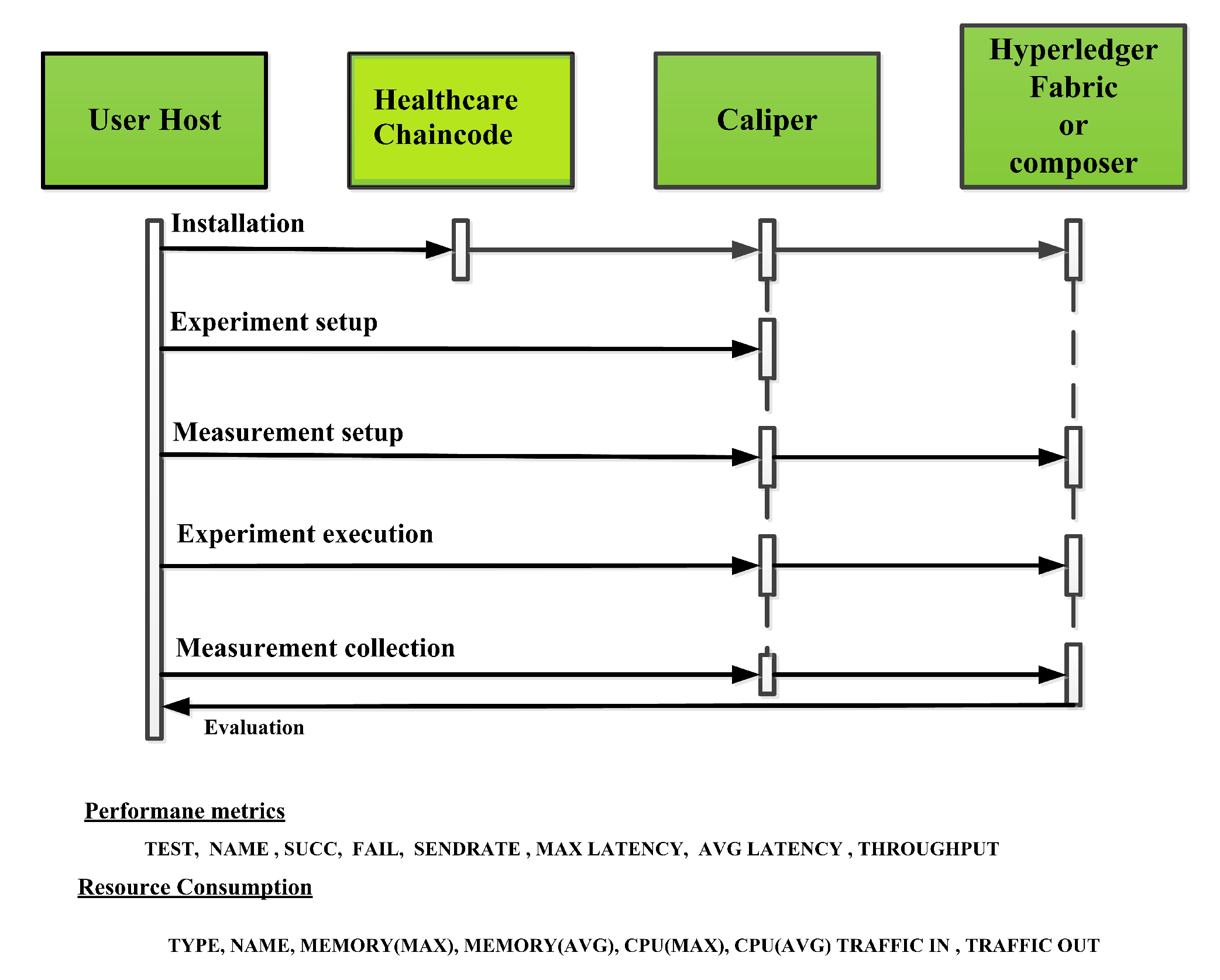
5.2. Performance Measurement Using Caliper
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, A.P.; Pradhan, N.R.; Luhach, A.K.; Agnihotri, S.; Jhanjhi, N.Z.; Verma, S.; Ghosh, U.; Roy, D.S. A Novel Patient-Centric Architectural Framework for Blockchain-Enabled Healthcare Applications. IEEE Trans. Ind. Informa. 2021, 17, 5779–5789. [Google Scholar] [CrossRef]
- Yazdinejad, A.; Srivastava, G.; Parizi, R.M.; Dehghantanha, A.; Choo, K.-K.R.; Aledhari, M. Decentralized Authentication of Distributed Patients in Hospital Networks Using Blockchain. IEEE J. Biomed. Health Inform. 2020, 24, 2146–2156. [Google Scholar] [CrossRef] [PubMed]
- Geneiatakis, D.; Soupionis, Y.; Steri, G.; Kounelis, I.; Neisse, R.; Nai-Fovino, I. Blockchain Performance Analysis for Supporting Cross-Border E-Government Services. IEEE Trans. Eng. Manag. 2020, 67, 1310–1322. [Google Scholar] [CrossRef]
- Dwivedi, A.D.; Srivastava, G.; Dhar, S.; Singh, R. A decentralized privacy-preserving healthcare blockchain for IoT. Sensors 2019, 19, 326. [Google Scholar] [CrossRef] [Green Version]
- Ismail, L.; Materwala, H. Blockchain Paradigm for Healthcare: Performance Evaluation. Symmetry 2020, 12, 1200. [Google Scholar] [CrossRef]
- Bhavin, M.; Tanwar, S.; Sharma, N.; Tyagi, S.; Kumar, N. Blockchain and quantum blind signature-based hybrid scheme for healthcare 5.0 applications. J. Inf. Secur. Appl. 2021, 56, 102673. [Google Scholar] [CrossRef]
- Zhuang, Y.; Sheets, L.R.; Chen, Y.-W.; Shae, Z.-Y.; Tsai, J.J.P.; Shyu, C.-R. A Patient-Centric Health Information Exchange Framework Using Blockchain Technology. IEEE J. Biomed. Health Inform. 2020, 24, 2169–2176. [Google Scholar] [CrossRef]
- Ismail, L.; Materwala, H.; Zeadally, S. Lightweight Blockchain for Healthcare. IEEE Access 2019, 7, 149935–149951. [Google Scholar] [CrossRef]
- Mazumdar, S.; Ruj, S. Design of Anonymous Endorsement System in Hyperledger Fabric. IEEE Trans. Emerg. Top. Comput. 2019, 9, 1780–1791. [Google Scholar] [CrossRef] [Green Version]
- Pongnumkul, S.; Siripanpornchana, C.; Thajchayapong, S. Performance Analysis of Private Blockchain Platforms in Varying Workloads. In Proceedings of the 2017 26th International Conference on Computer Communication and Networks (ICCCN), Vancouver, BC, Canada, 31 July–3 August 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Thakkar, P.; Nathan, S.; Viswanathan, B. Performance Benchmarking and Optimizing Hyperledger Fabric Blockchain Platform. In Proceedings of the 2018 IEEE 26th International Symposium on Modeling, Analysis, and Simulation of Computer and Telecommunication Systems (MASCOTS), Milwaukee, WI, USA, 25–28 September 2018; pp. 264–276. [Google Scholar] [CrossRef] [Green Version]
- Androulaki, E.; Artem, B.; Vita, B.; Christian, C.; Konstantinos, C.; Angelo, C.D.; David, E.; Ferris, C.; Laventman, G.; Manevich, Y.; et al. Hyperledger fabric: A distributed operating system for permissioned blockchains. In Proceedings of the Thirteenth EuroSys Conference, Porto, Portugal, 23–26 April 2018; pp. 1–15. [Google Scholar]
- Stamatellis, C.; Papadopoulos, P.; Pitropakis, N.; Katsikas, S.; Buchanan, W.J. A Privacy-Preserving Healthcare Framework Using Hyperledger Fabric. Sensors 2020, 20, 6587. [Google Scholar] [CrossRef]
- Tanwar, S.; Karan, P.; Richard, E. Blockchain-based electronic healthcare record system for healthcare 4.0 applications. J. Inf. Secur. Appl. 2020, 50, 102407. [Google Scholar] [CrossRef]
- Houtan, B.; Hafid, A.S.; Makrakis, D. A Survey on Blockchain-Based Self-Sovereign Patient Identity in Healthcare. IEEE Access 2020, 8, 90478–90494. [Google Scholar] [CrossRef]
- Lakhan, A.; Mohammed, M.A.; Kozlov, S.; Rodrigues, J.J. Mobile-fog-cloud assisted deep reinforcement learning and blockchain-enable IoMT system for healthcare workflows. Trans. Emerg. Telecommun. Technol. 2021, e4363. [Google Scholar] [CrossRef]
- Jabarulla, M.Y.; Lee, H.N. Blockchain-based distributed patient-centric image management system. Appl. Sci. 2020, 11, 196. [Google Scholar] [CrossRef]
- Garg, N.; Wazid, M.; Das, A.K.; Singh, D.P.; Rodrigues, J.J.P.C.; Park, Y. BAKMP-IoMT: Design of Blockchain Enabled Authenticated Key Management Protocol for Internet of Medical Things Deployment. IEEE Access 2020, 8, 95956–95977. [Google Scholar] [CrossRef]
- Pradhan, N.R.; Singh, A.P.; Kumar, V. Blockchain-Enabled Traceable, Transparent Transportation System for Blood Bank. In Advances in VLSI, Communication, and Signal Processing; Harvey, D., Kar, H., Verma, S., Bhadauria, V., Eds.; Lecture Notes in Electrical Engineering; Springer: Singapore, 2021; Volume 683. [Google Scholar]
- Pradhan, N.R.; Rout, S.S.; Singh, A.P. Blockchain Based Smart Healthcare System for Chronic—Illness Patient Monitoring. In Proceedings of the 2020 3rd International Conference on Energy, Power and Environment: Towards Clean Energy Technologies, Shillong, India, 5–7 March 2021; pp. 1–6. [Google Scholar]
- Wu, H.; Dwivedi, A.D.; Srivastava, G. Security and privacy of patient information in medical systems based on blockchain technology. ACM Trans. Multimed. Comput. Commun. Appl. (TOMM) 2021, 17, 1–17. [Google Scholar] [CrossRef]
- Kaushik, K.; Dahiya, S.; Singh, R.; Dwivedi, A.D. Role of Blockchain in Forestalling Pandemics. In Proceedings of the 2020 IEEE 17th International Conference on Mobile Ad Hoc and Sensor Systems (MASS), Delhi, India, 10–13 December 2020; pp. 32–37. [Google Scholar] [CrossRef]
- Singh, R.; Dwivedi, A.D.; Srivastava, G. Internet of things based blockchain for temperature monitoring and counterfeit pharmaceutical prevention. Sensors 2020, 20, 3951. [Google Scholar] [CrossRef]
- Dwivedi, A.D.; Singh, R.; Kaushik, K.; Mukkamala, R.R.; Alnumay, W.S. Blockchain and artificial intelligence for 5G-enabled Internet of Things: Challenges, opportunities, and solutions. Trans. Emerg. Telecommun. Technol. 2021, e4329. [Google Scholar] [CrossRef]
- Meng, T.; Zhao, Y.; Wolter, K.; Xu, C.-Z. On Consortium Blockchain Consistency: A Queueing Network Model Approach. IEEE Trans. Parallel Distrib. Syst. 2021, 32, 1369–1382. [Google Scholar] [CrossRef]
- Azaria, A.; Ekblaw, A.; Vieira, T.; Lippman, A. Medrec: Using blockchain for medical data access and permission management. In Proceedings of the 2016 2nd International Conference on Open and Big Data (OBD), Vienna, Austria, 22–24 August 2016; pp. 25–30. [Google Scholar]
- Shen, B.; Guo, J.; Yang, Y. MedChain: Efficient healthcare data sharing via blockchain. Appl. Sci. 2019, 9, 1207. [Google Scholar] [CrossRef] [Green Version]
- Gorenflo, C.; Lee, S.; Golab, L.; Keshav, S. FastFabric: Scaling Hyperledger Fabric to 20,000 Transactions per Second. Int. J. Netw. Manag. 2020, 30, e2099. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Zhang, R.; Wang, X.; Gao, K.; Liu, L. A decentralizing attribute-based signature for healthcare blockchain. In Proceedings of the 2018 27th International Conference on Computer Communication and Networks (ICCCN), Hangzhou, China, 30 July–2 August 2018; pp. 1–9. [Google Scholar]
- Chen, L.; Lee, W.K.; Chang, C.H.; Choo, K.K.R.; Zhang, N. Blockchain based searchable encryption for electronic health record sharing. Fut. Gener. Comput. Syst. 2019, 95, 420–429. [Google Scholar] [CrossRef]


| References | Year | Objective | Performance | Limitation | Performance Evaluation |
|---|---|---|---|---|---|
| Azaria et al. [26] | 2016 | MedRec: Ethereum based permission less mode of operation | It slows down network computing over the time and makes the network less transparent | Full transparency | No |
| Shen et al. [27] | 2019 | MedChain: patient centric healthcare by providing the privacy preserving mechanism for healthcare data | Only calculated average response time, throughput and average message time based on Ethereum | Full transparency | Partially |
| Gorenflo et al. [28] | 2018 | To scale a blockchain network using Hyperledger Fabric | Demonstrable capability of blockchain network | Increased computing power needed | No |
| Sun et al. [29] | 2018 | To propose a decentralizing attribute based signature using blockchain | Verifiable secure sharing of large-scale and distributed EHR | Attribute certificates, storage capacity | Partially |
| Chen et al. [30] | 2019 | To design a searchable encryption for EHR using blockchain | Security analysis with searchable encryption algorithm | Scalability | No |
| Singh et al. [1] | 2020 | To design and propose an efficient blockchain based EHR system using HF and SOLO ordering services | EHR with smart contract, achieves performance optimization using Caliper | No fault tolerance capacity of the network | Yes |
| Proposed Approach | 2022 | To design and propose an efficient blockchain based EHR sharing with HF and RAFT ordering services with on-chain and off-chain storing scheme | Transaction traffic analysis and performance optimization using Caliper | Fault tolerance | Yes |
| Requirements | Specification |
|---|---|
| Operating System | Ubuntu Linux 18.04 (8 GB RAM)(64 bit) |
| Virtual machine 1 (35.102.12 .31) | Ubuntu Linux 18.04 (2core, 8 GB RAM, 30 GB memory, 64 bit) |
| Virtual machine 2 (35.102.12 .34) | Ubuntu Linux 18.04 (2core, 4 GB RAM, 30 GB memory, 64 bit) |
| Virtual machine 3 (35.102.12 .33) | Ubuntu Linux 18.04 (2core, 4 GB RAM, 30 GB memory, 64 bit) |
| Virtual machine 4 (35.102.12 .32) | Ubuntu Linux 18.04 (2core, 4 GB RAM, 30 GB memory, 64 bit) |
| cURL Tool | Version 7.74.0 |
| Docker engine | Version 17.06.2 |
| Docker Composer | Version 1.14 |
| Javascript | 1.8.5 |
| Node JS | Version 10.21 |
| NPM | Version 6.14.4 |
| Hyperledger Fabric | 2.0.1 |
| VS Code | 1.49.1 |
| Docker Swarm Network | 12.06 |
| Postman API | v7.333.0 |
| Hyperledger Caliper | v0.4.2 |
| Fauxton Apache couch DB | version 6.1 |
| Name | No. of TXs | Succ | Send Rate (TPS) | Avg Latency (s) | Throughput |
|---|---|---|---|---|---|
| RAFT (Open) | 1000 | 946 | 50, 150, 250 | 0.2, 0.3, 0.5 | 50, 135, 185 |
| Kafka (Open) | 1000 | 727 | 50, 150, 250 | 3.8, 4.2, 6.1 | 42, 122, 164 |
| RAFT (Query) | 1000 | 1000 | 50, 150, 250 | 0.12, 3.63, 7.62 | 66, 77, 87 |
| Kafka (Query) | 1000 | 1000 | 50, 150, 250 | 4.12, 5.86, 8.11 | 67, 84, 105 |
| RAFT (Transfer) | 1000 | 1000 | 50, 150, 250 | 0.2, 0.3, 1.3 | 45, 61, 92 |
| Kafka (Transfer) | 1000 | 1000 | 50, 150, 250 | 3.2, 3.3, 4.6 | 32, 53, 84 |
| Type | Name | Memory (Max MB) | Memory (Avg MB) | CPU (Max) | CPU (Avg) | Traffic In | Traffic Out | Disc Write |
|---|---|---|---|---|---|---|---|---|
| Docker | peer 0.org 1.35.102.12.31 | 403.8 | 389.3 | 5.23% | 3.13% | 3.3 | 1.9 | 18.3 |
| Docker | peer 1.org 1.35.102.12.31 | 512.9 | 406.4 | 4.52% | 3.7 % | 3.3 | 1.86 | 18.3 |
| Docker | peer 0.org 2.35.102.12.34 | 205.3 | 200.3 | 5.16% | 3.03% | 3.3 | 1.7 | 17.3 |
| Docker | peer1.org2.35.102.12.34 | 201.3 | 200.3 | 4.57% | 3.23% | 3.3 | 1.77 | 17.3 |
| Docker | peer 0.org 3.35.102.12.33 | 203.9 | 200.3 | 5.64% | 3.01% | 3.3 | 1.81 | 16.3 |
| Docker | peer 1.org 3.35.102.12.33 | 146.6 | 119.3 | 4.28% | 3.04% | 3.3 | 2.0 | 16.3 |
| Docker | RAFTorderer.35.102.12.32 | 19.6 | 18.0 | 1.01% | 0.26% | 2.3 | 4.5 | 8.0 |
| Docker | ca.org 1.35.102.12.31 | 8.3 | 7.6 | 0.13% | 0.00% | 1.5 | 0 | 0 |
| Docker | ca.org 2.35.102.12.34 | 8.3 | 7.6 | 0.13% | 0.00% | 1.5 | 0 B | 0 B |
| Docker | ca.org 3.35.102.12.33 | 8.6 | 7.8 | 0.29% | 0.00% | 1.4 | 0 | 0 |
| Type | Name | Memory (Max MB) | Memory (Avg MB) | CPU (Max) | CPU (Avg) | Traffic In | Traffic Out | Disc Write |
|---|---|---|---|---|---|---|---|---|
| Docker | peer 0.org 1.35.102.12.31 | 405.7 | 138.0 | 6.47% | 3.16% | 6.6 | 3.61 | 34.5 |
| Docker | peer 1.org 1.35.102.12.31 | 405.7 | 125.0 | 6.19% | 3.16% | 6.8 | 3.62 | 33.5 |
| Docker | peer 0.org 2.35.102.12.34 | 208.6 | 124.0 | 6.29% | 3.16% | 6.72 | 3.5 | 34.8 |
| Docker | peer 1.org 2.35.102.12.34 | 207.6 | 124.0 | 6.19% | 3.16% | 6.5 | 3.53 | 33.5 |
| Docker | peer 0.org 3.35.102.12.33 | 204.6 | 124.0 | 5.19% | 3.16% | 6.6 | 3.62 | 32.5 |
| Docker | peer 1.org 3.35.102.12.33 | 66.3 | 61.1 | 4.39% | 3.15% | 6.6 | 3.59 | 34.15 |
| Docker | RAFTorderer.35.102.12.32 | 34.5 | 24.1 | 1.51% | 0.26% | 4.5 | 9.0 | 16.1 |
| Docker | ca.org 1.35.102.12.31 | 6.5 | 5.8 | 0.20% | 0.00% | 729 | 0 | 0 |
| Docker | ca.org 2.35.102.12.34 | 6.5 | 5.8 | 0.20% | 0.00% | 729 | 0 | 0 |
| Docker | ca.org 3.35.102.12.33 | 5.9 | 5.9 | 0.29% | 0.00% | 729 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pradhan, N.R.; Singh, A.P.; Verma, S.; Kavita; Kaur, N.; Roy, D.S.; Shafi, J.; Wozniak, M.; Ijaz, M.F. A Novel Blockchain-Based Healthcare System Design and Performance Benchmarking on a Multi-Hosted Testbed. Sensors 2022, 22, 3449. https://doi.org/10.3390/s22093449
Pradhan NR, Singh AP, Verma S, Kavita, Kaur N, Roy DS, Shafi J, Wozniak M, Ijaz MF. A Novel Blockchain-Based Healthcare System Design and Performance Benchmarking on a Multi-Hosted Testbed. Sensors. 2022; 22(9):3449. https://doi.org/10.3390/s22093449
Chicago/Turabian StylePradhan, Nihar Ranjan, Akhilendra Pratap Singh, Sahil Verma, Kavita, Navneet Kaur, Diptendu Sinha Roy, Jana Shafi, Marcin Wozniak, and Muhammad Fazal Ijaz. 2022. "A Novel Blockchain-Based Healthcare System Design and Performance Benchmarking on a Multi-Hosted Testbed" Sensors 22, no. 9: 3449. https://doi.org/10.3390/s22093449
APA StylePradhan, N. R., Singh, A. P., Verma, S., Kavita, Kaur, N., Roy, D. S., Shafi, J., Wozniak, M., & Ijaz, M. F. (2022). A Novel Blockchain-Based Healthcare System Design and Performance Benchmarking on a Multi-Hosted Testbed. Sensors, 22(9), 3449. https://doi.org/10.3390/s22093449