
Multispectral, Fluorescent and Photoplethysmographic Imaging for Remote Skin Assessment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Prototype Devices for Multispectral Skin Imaging
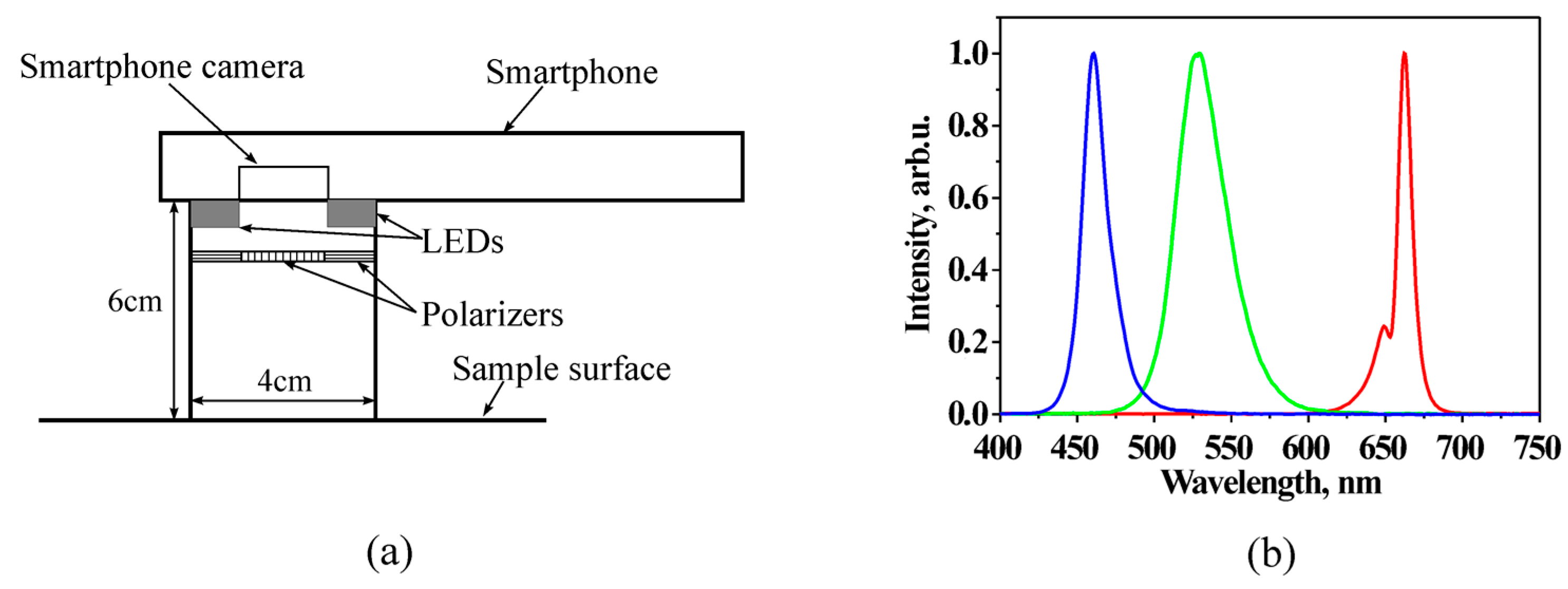
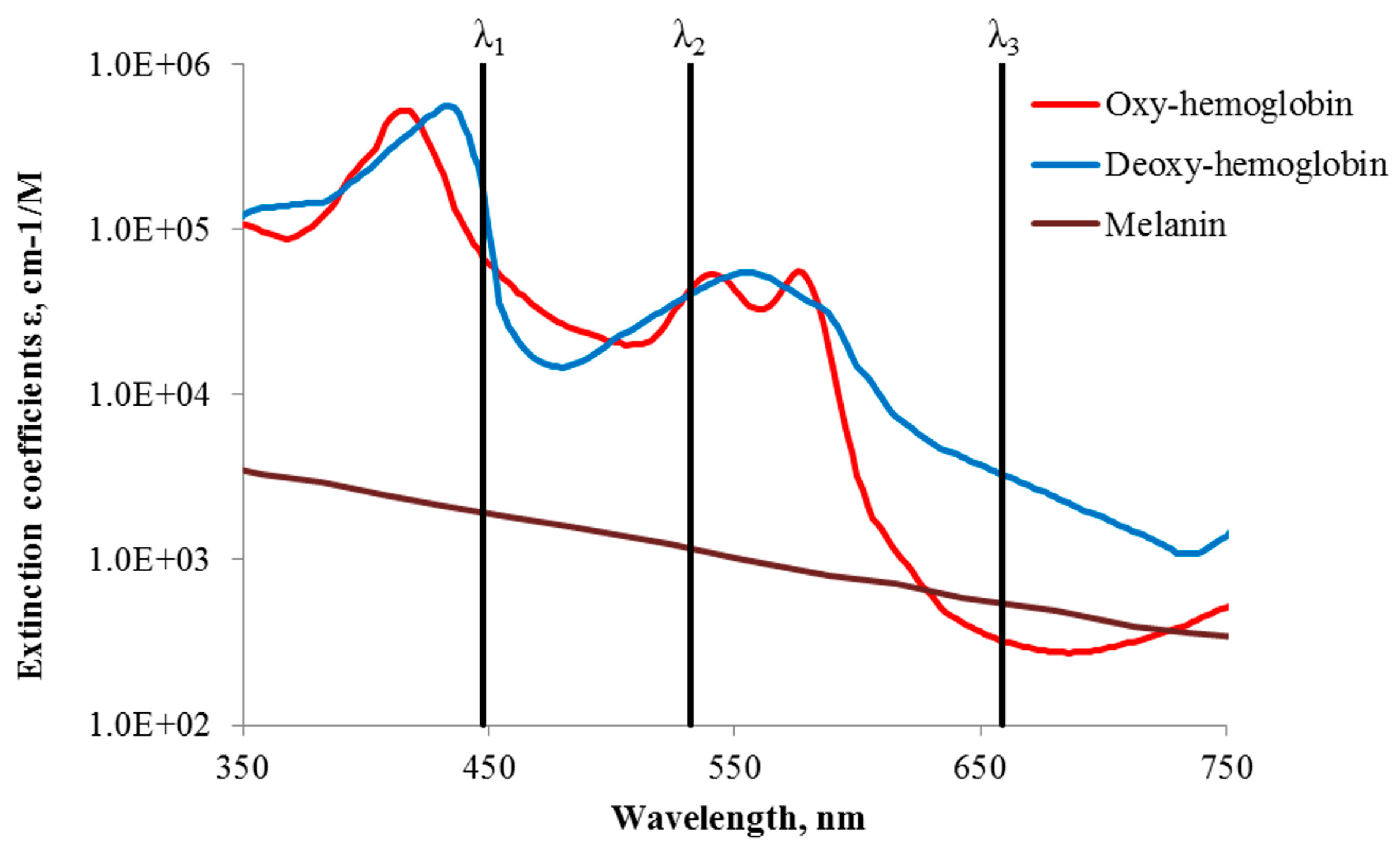
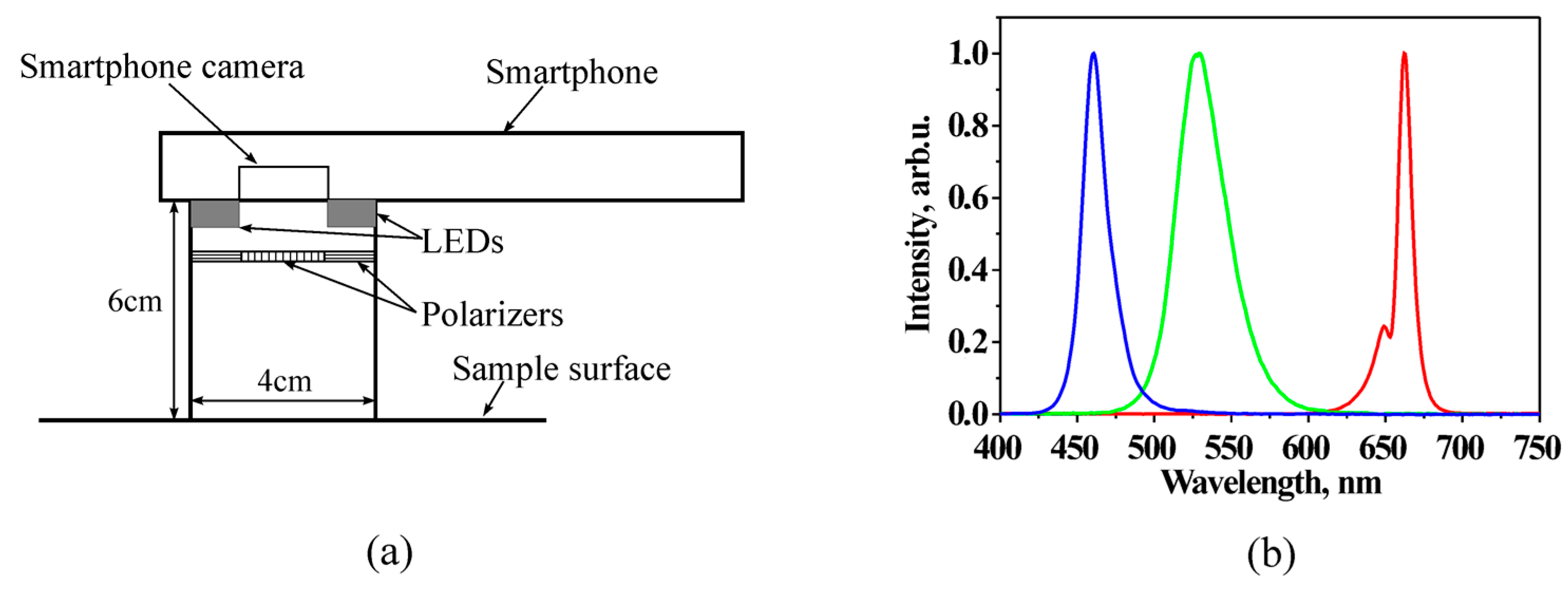
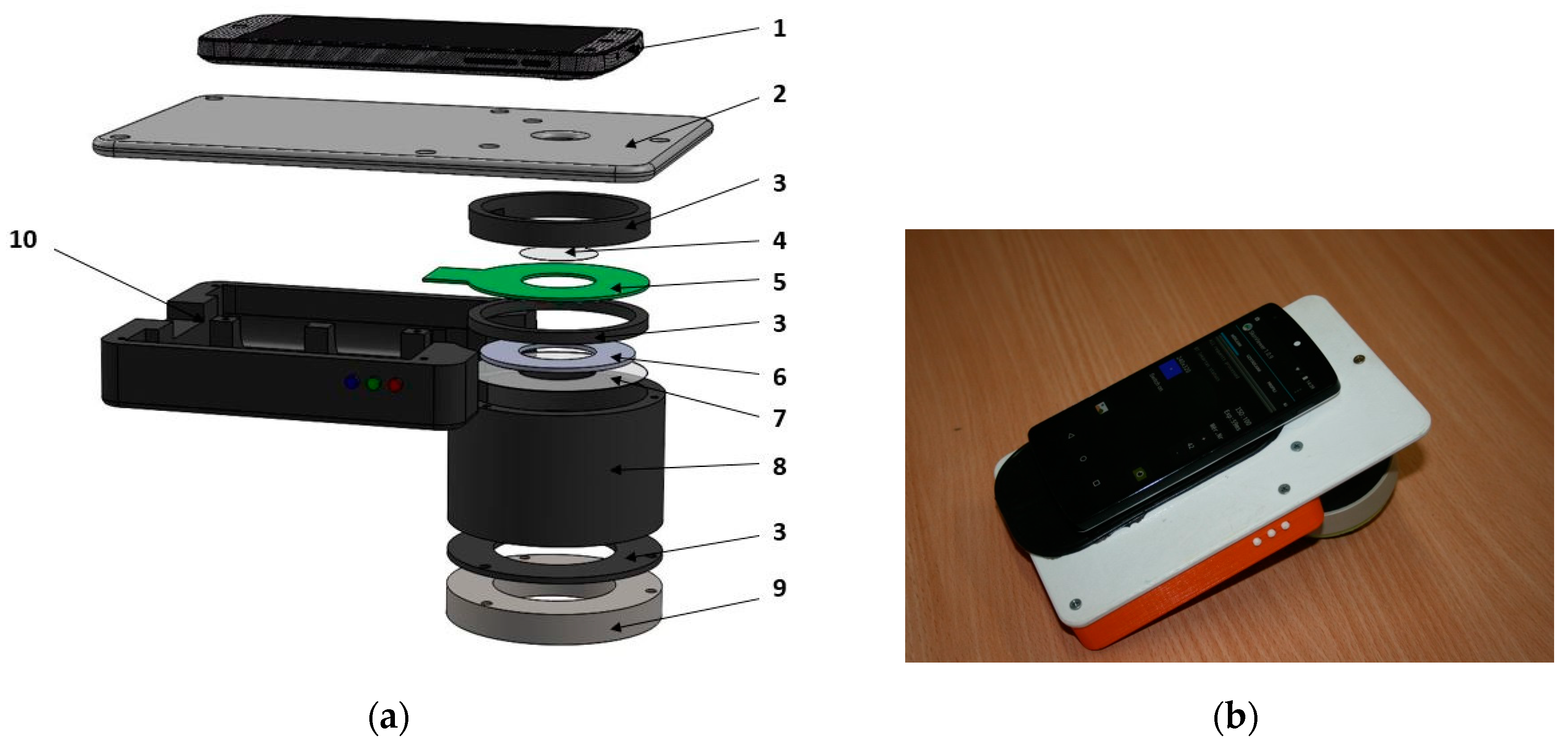
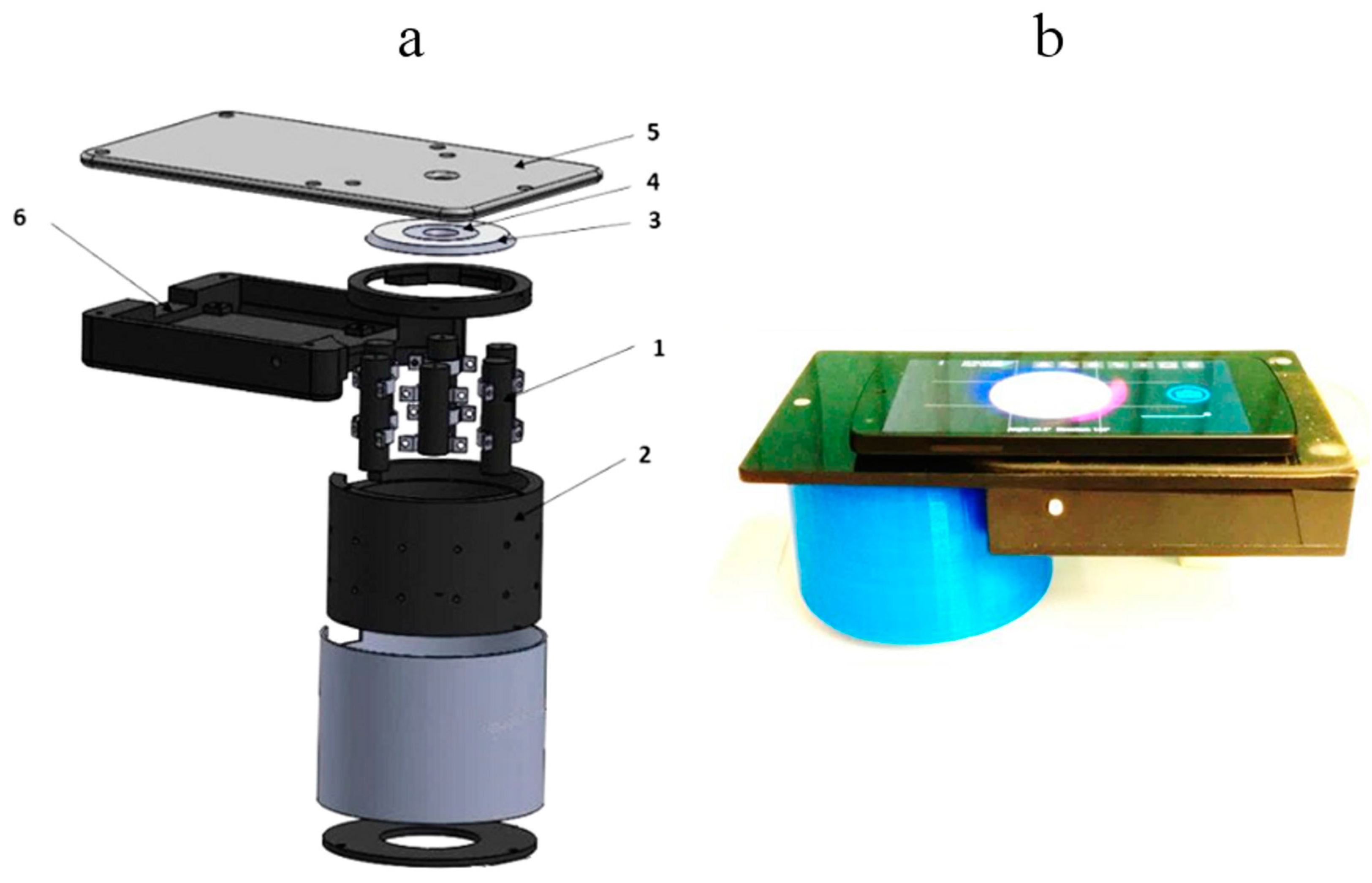
2.1.1. RGB-LED Add-On Illumination System for Smartphones
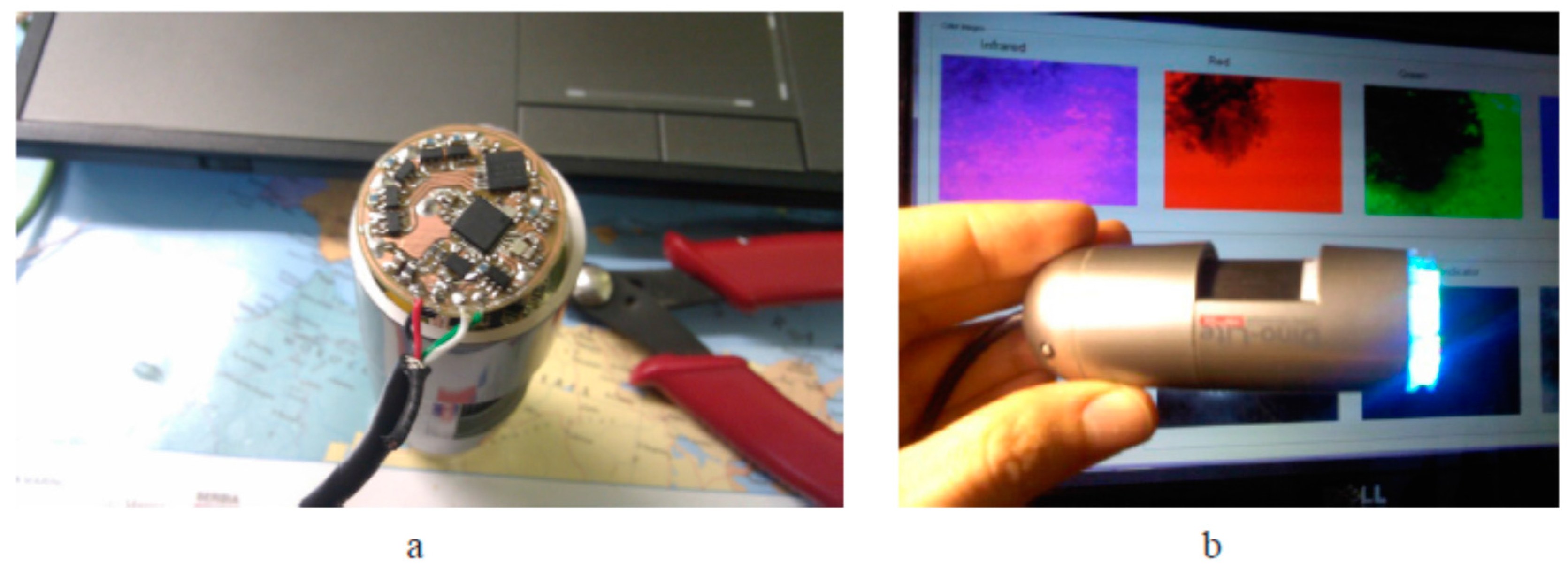
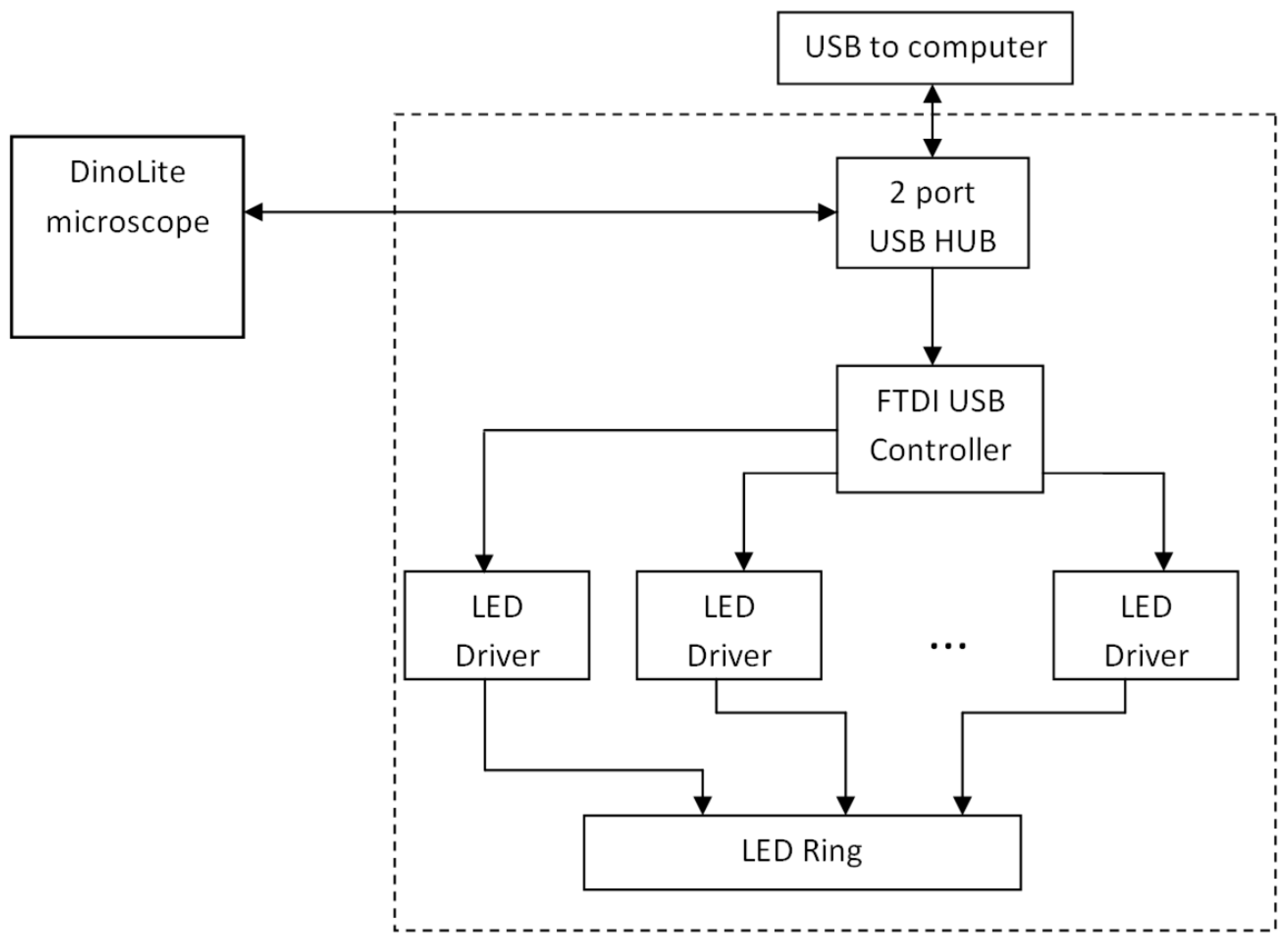
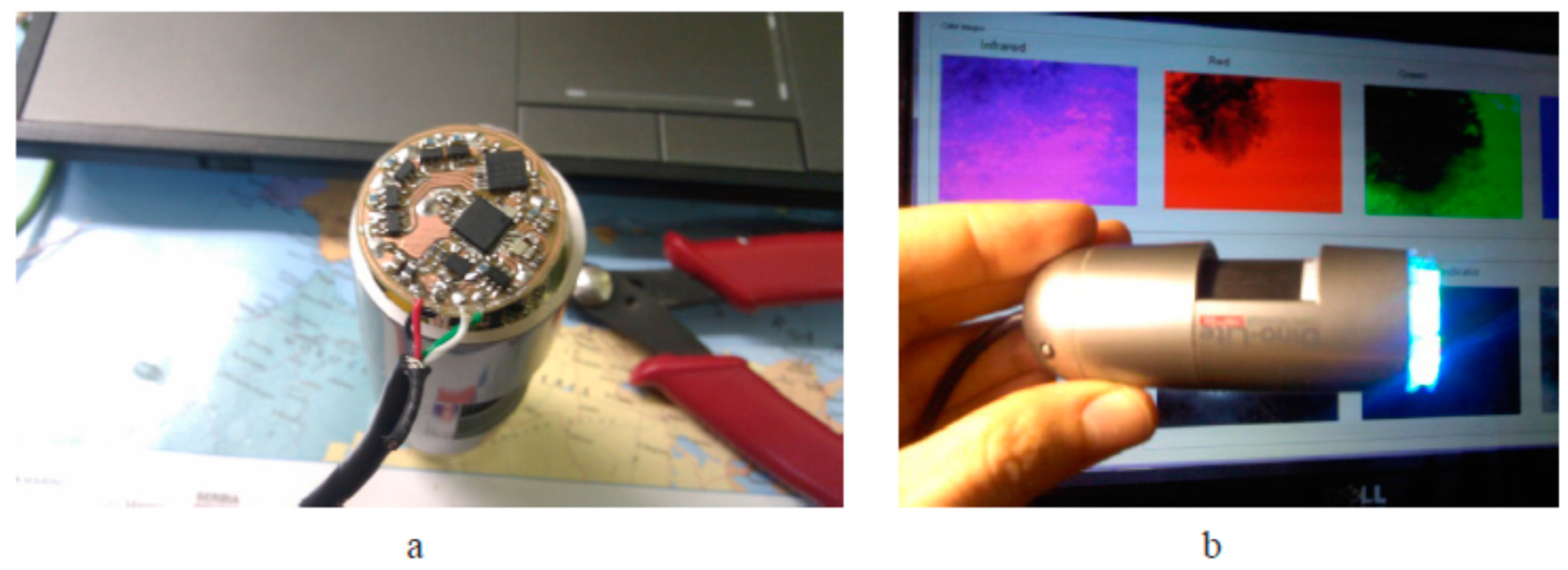
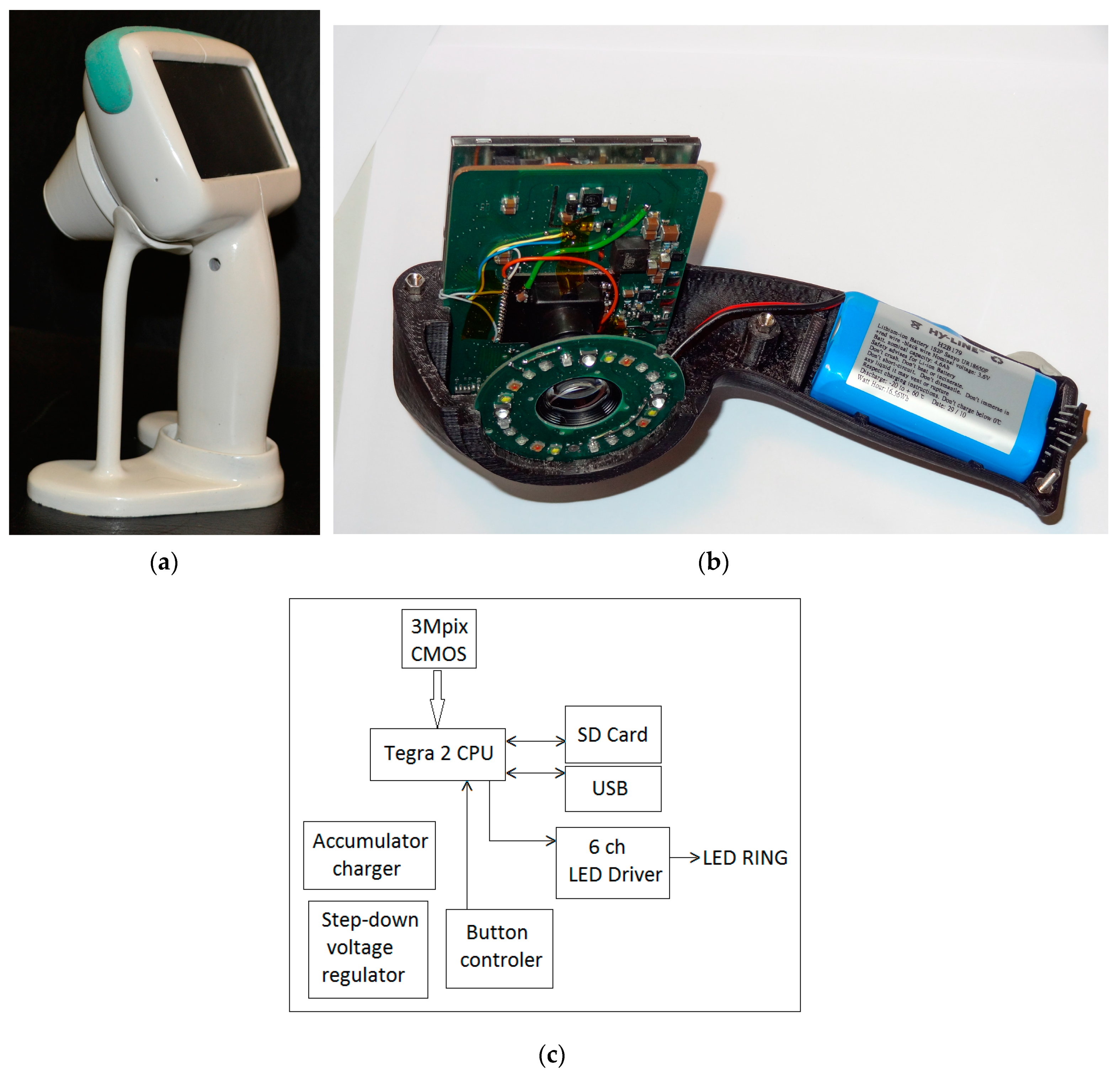
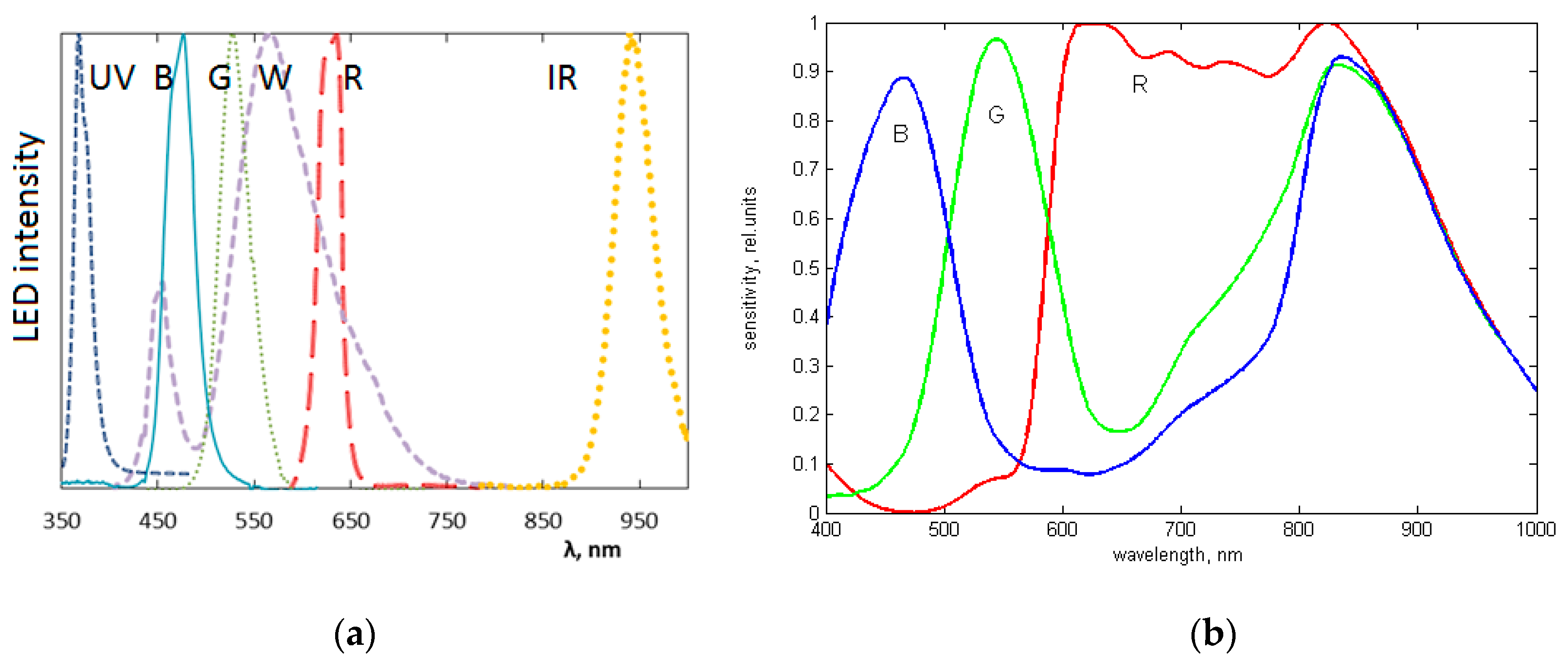
2.1.2. Modified Multispectral Video-Microscope
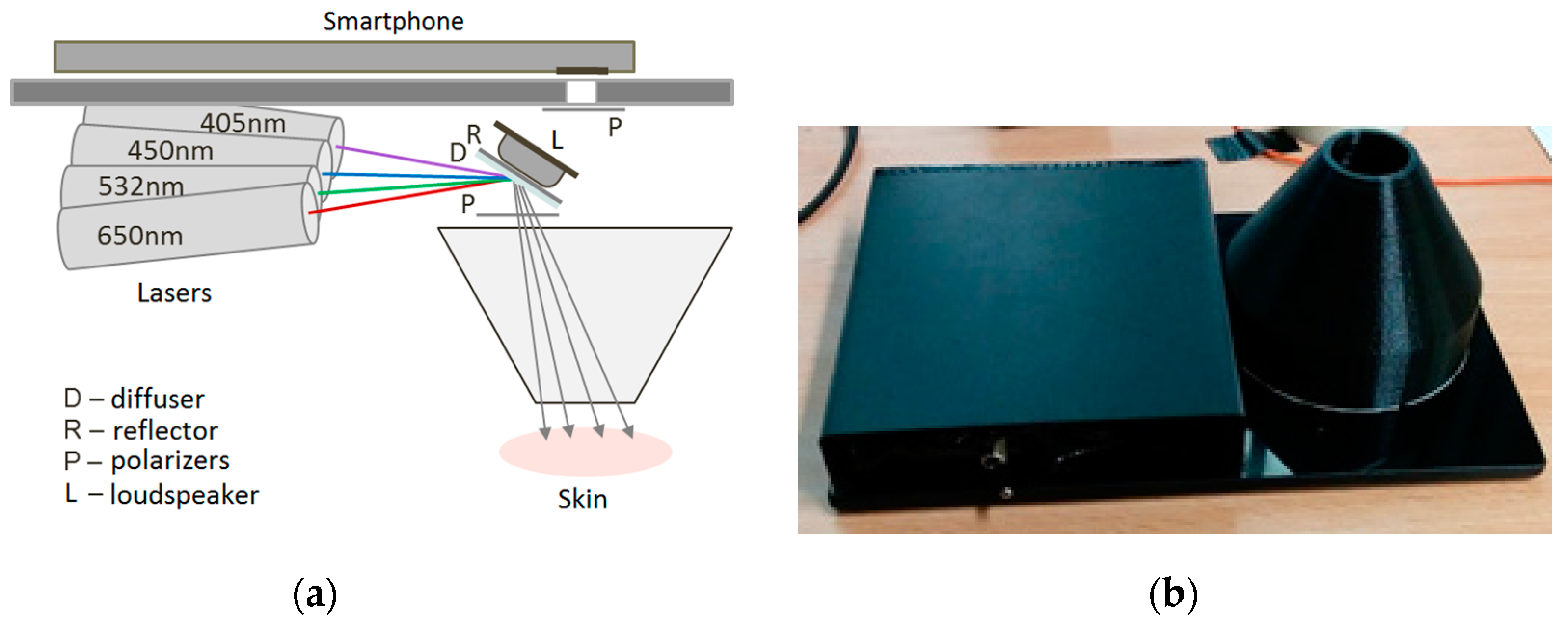
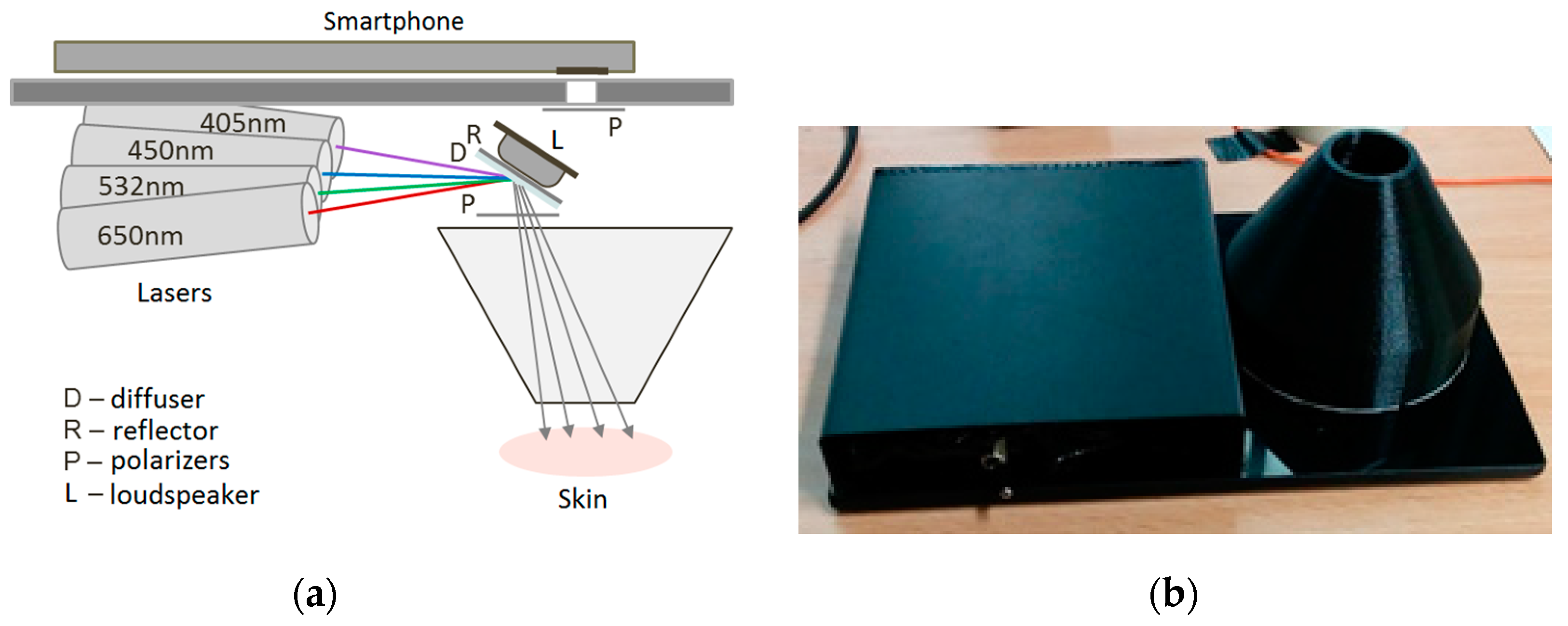
2.1.3. Prototypes for Smartphone Monochromatic Spectral Imaging of Skin at Multi-Laser Illumination
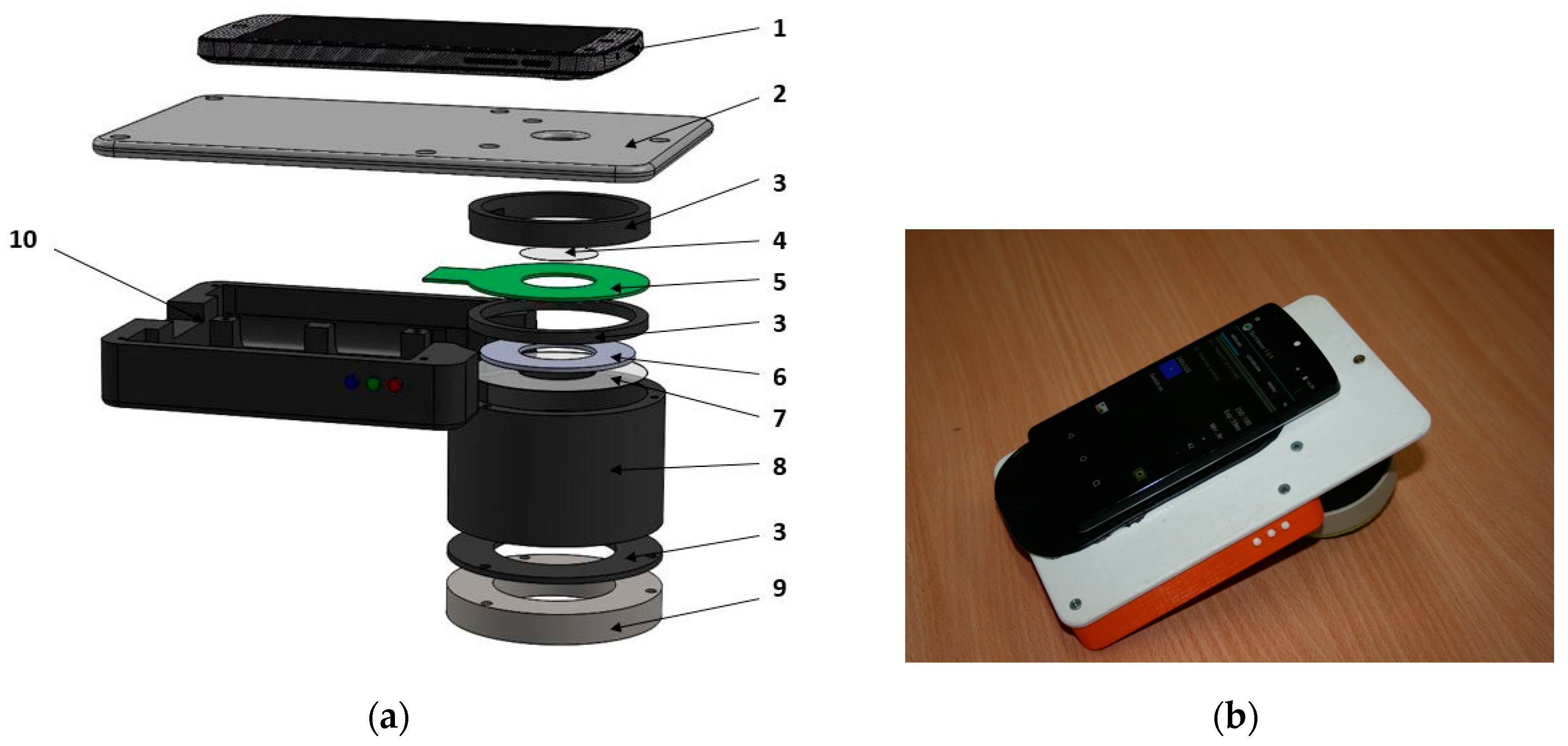
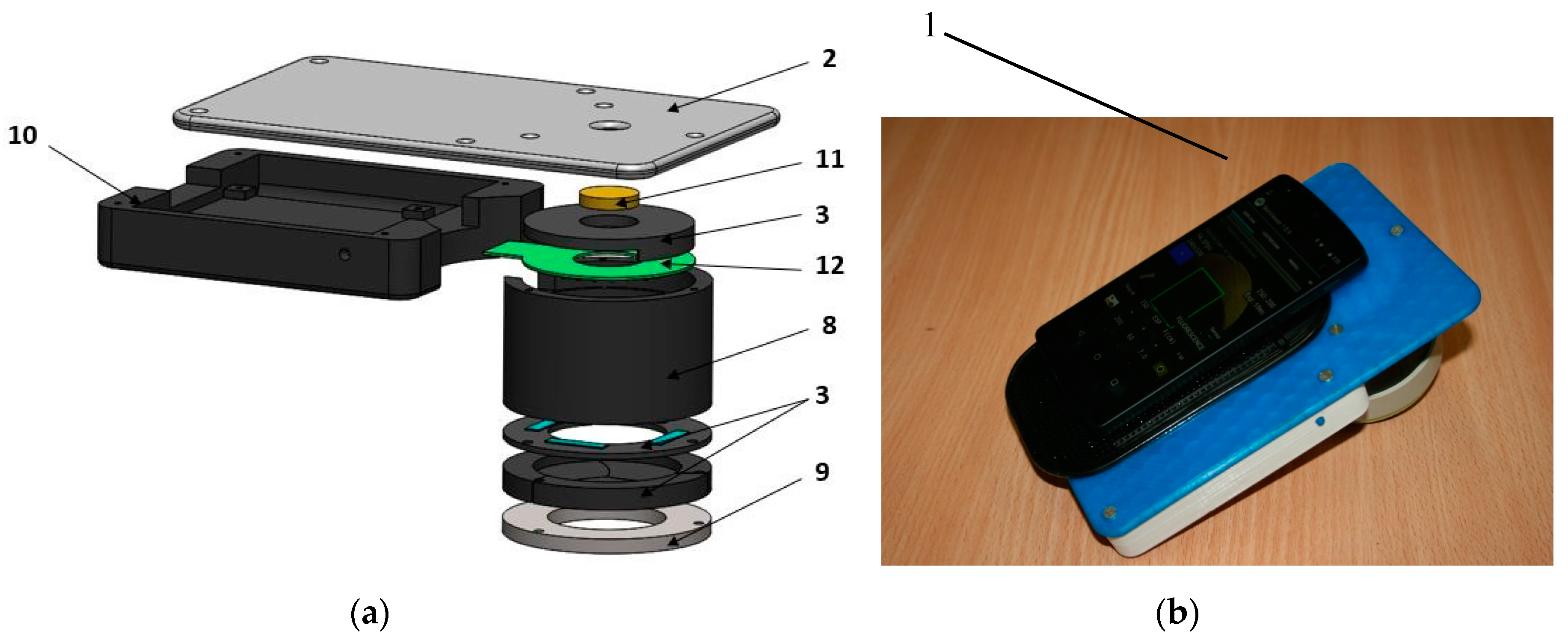
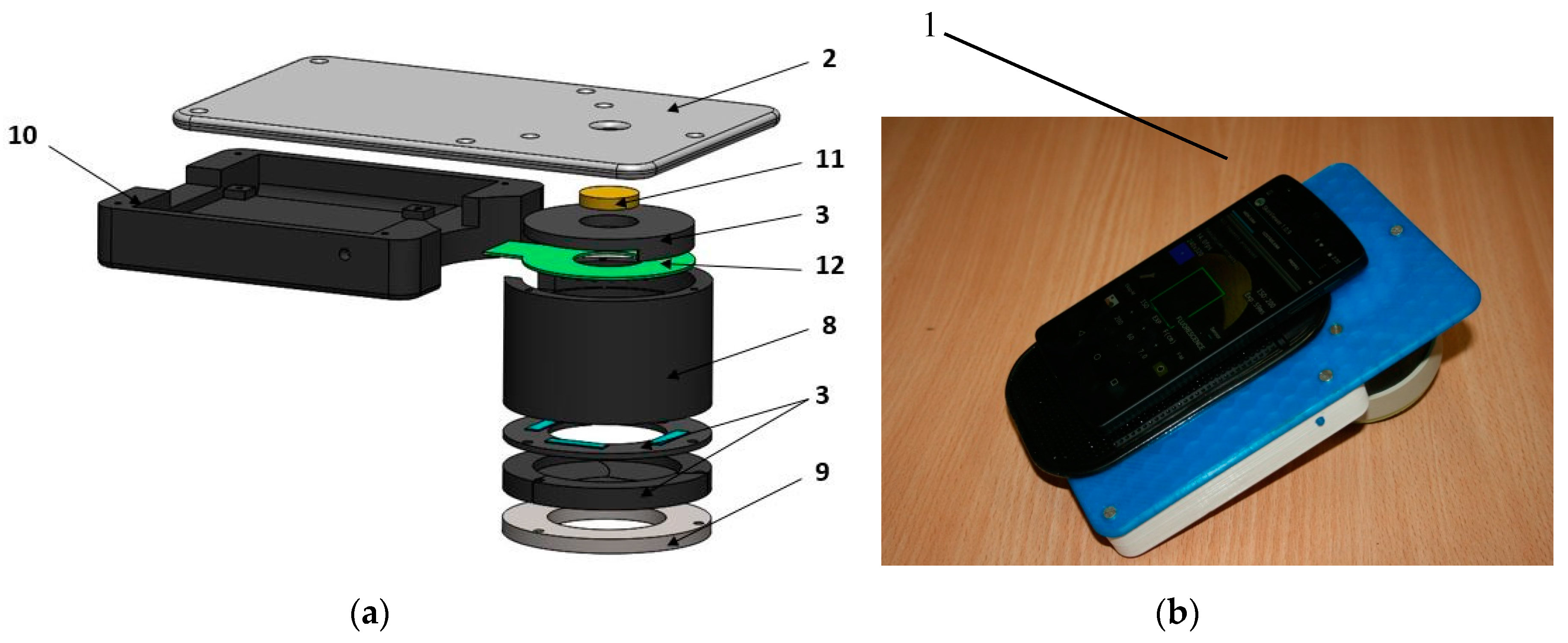
2.2. Prototype Device for Skin Fluorescence Imaging With a Smartphone
2.3. Photoplethysmography Video-Imaging Prototypes
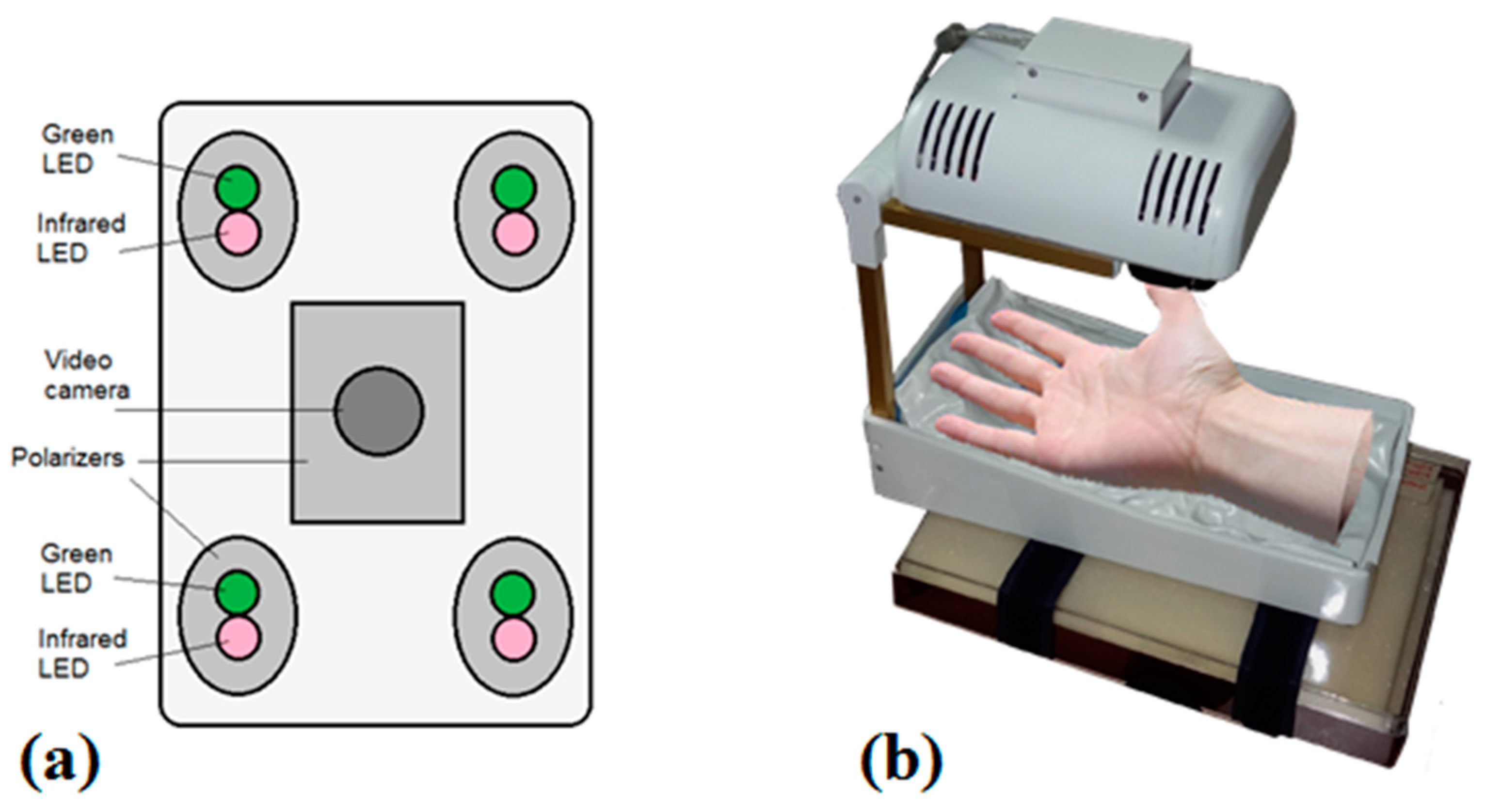
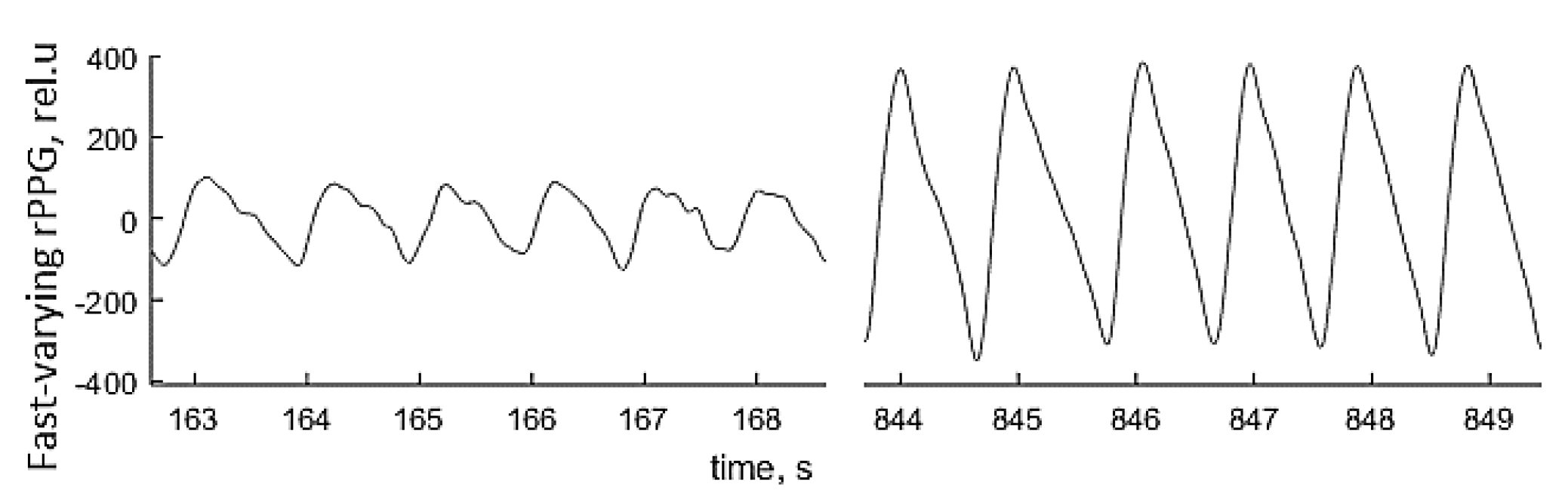
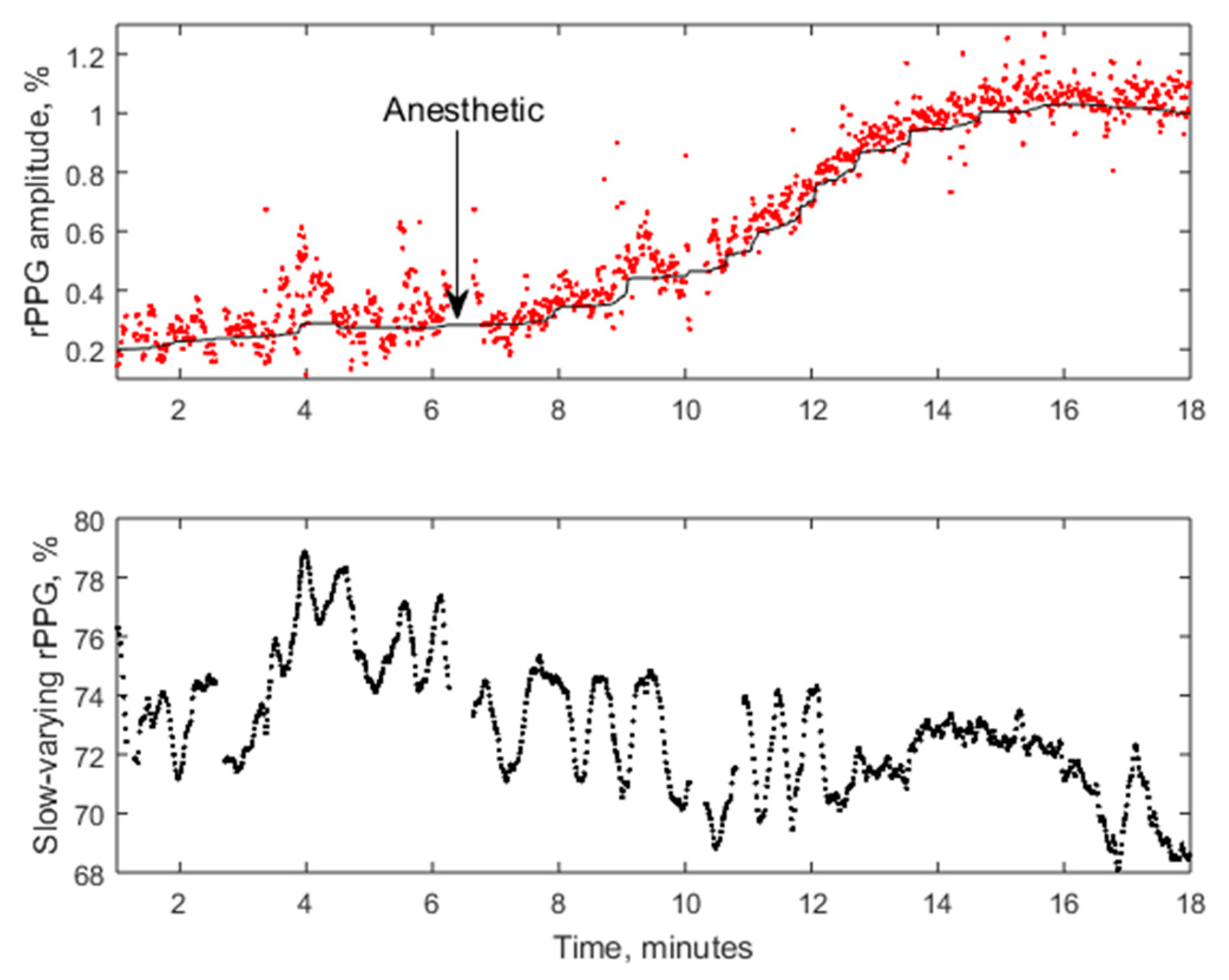
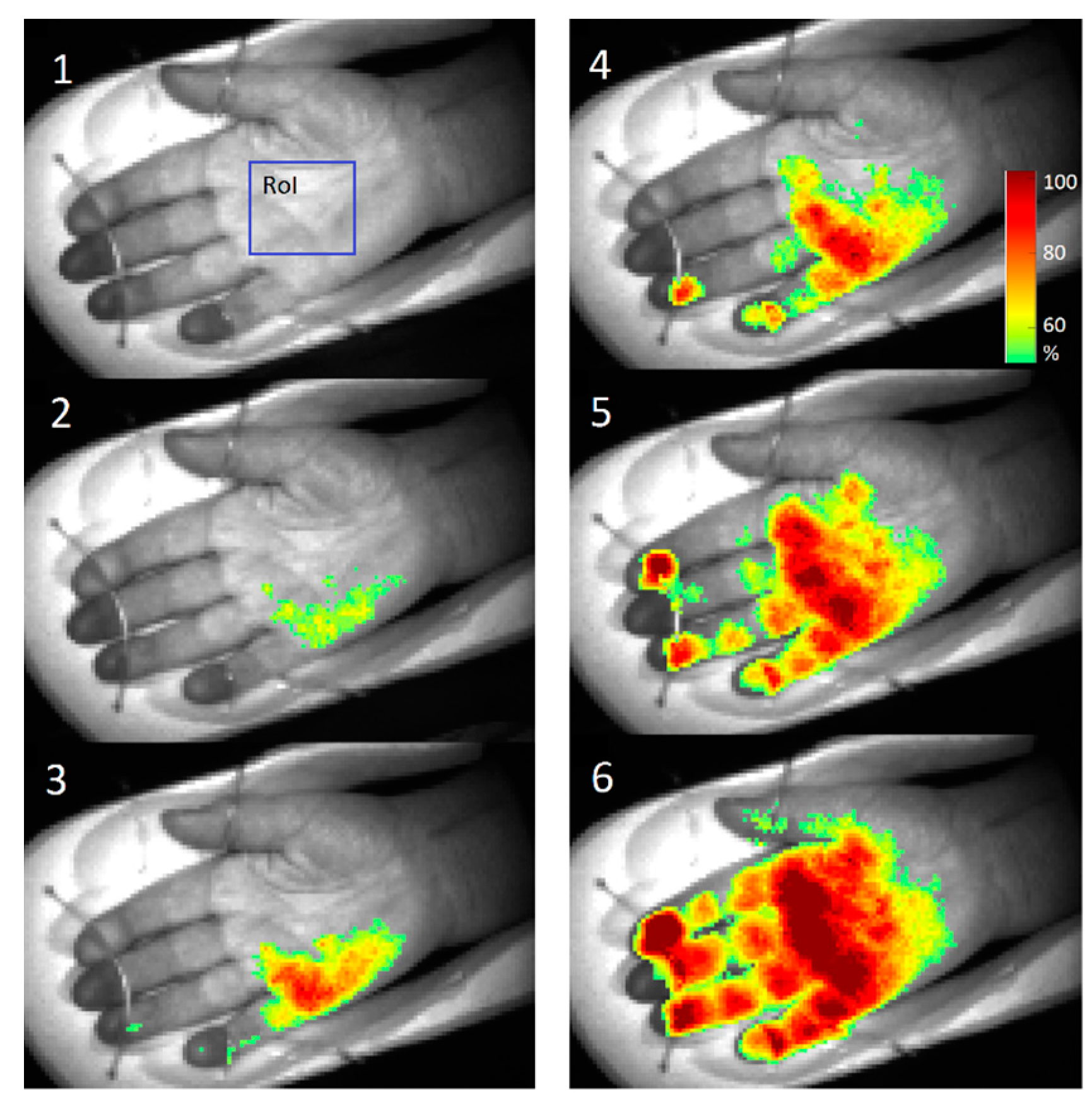
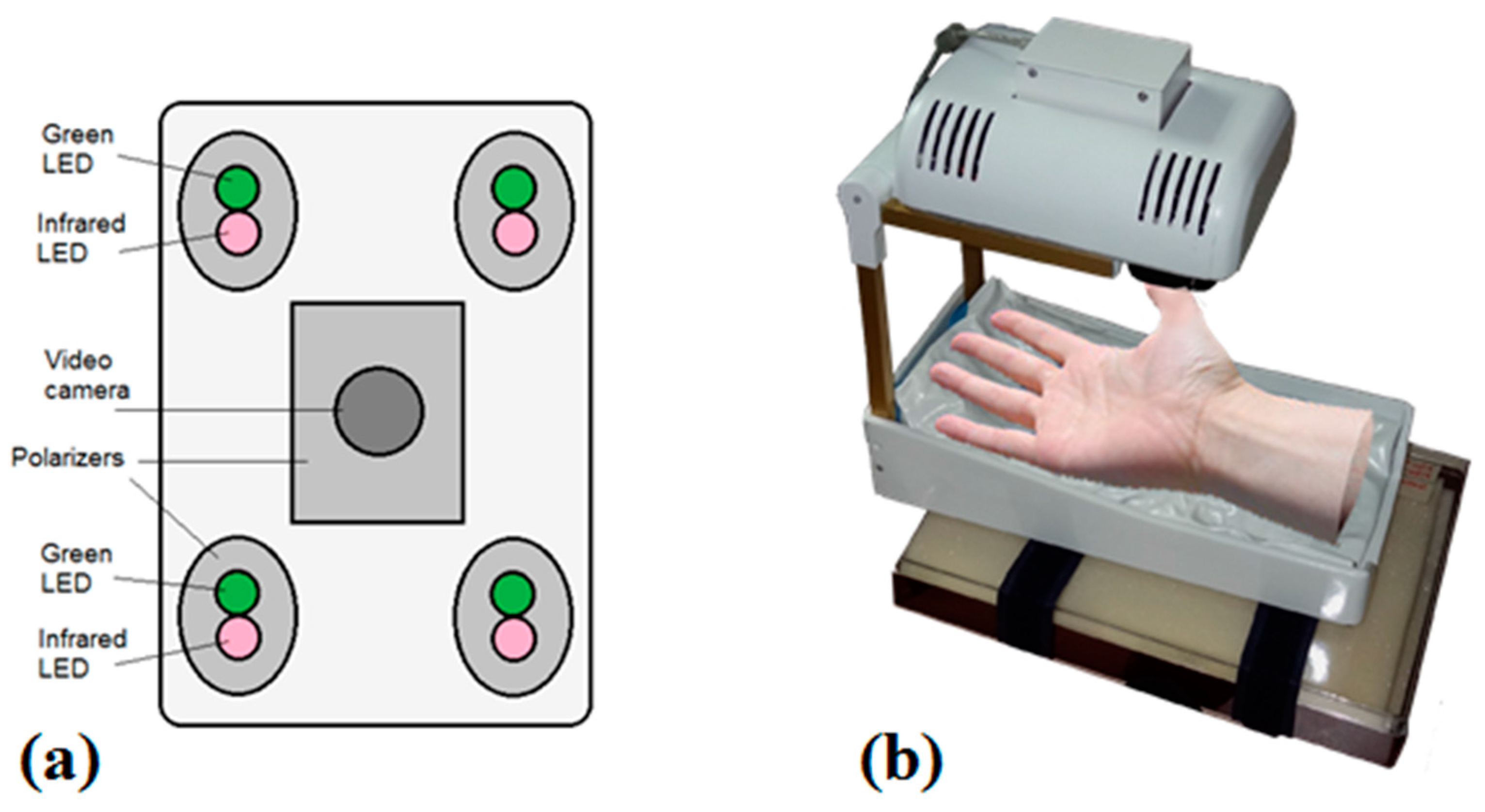
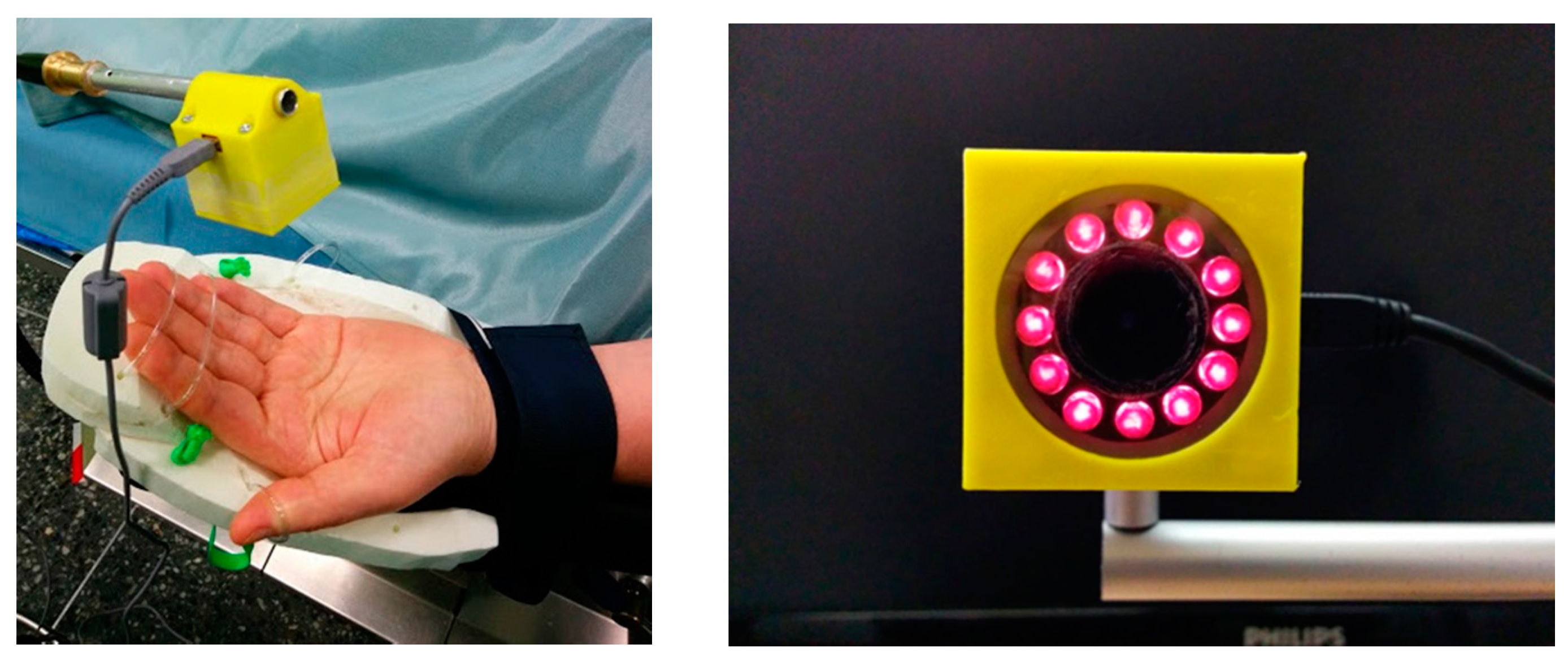
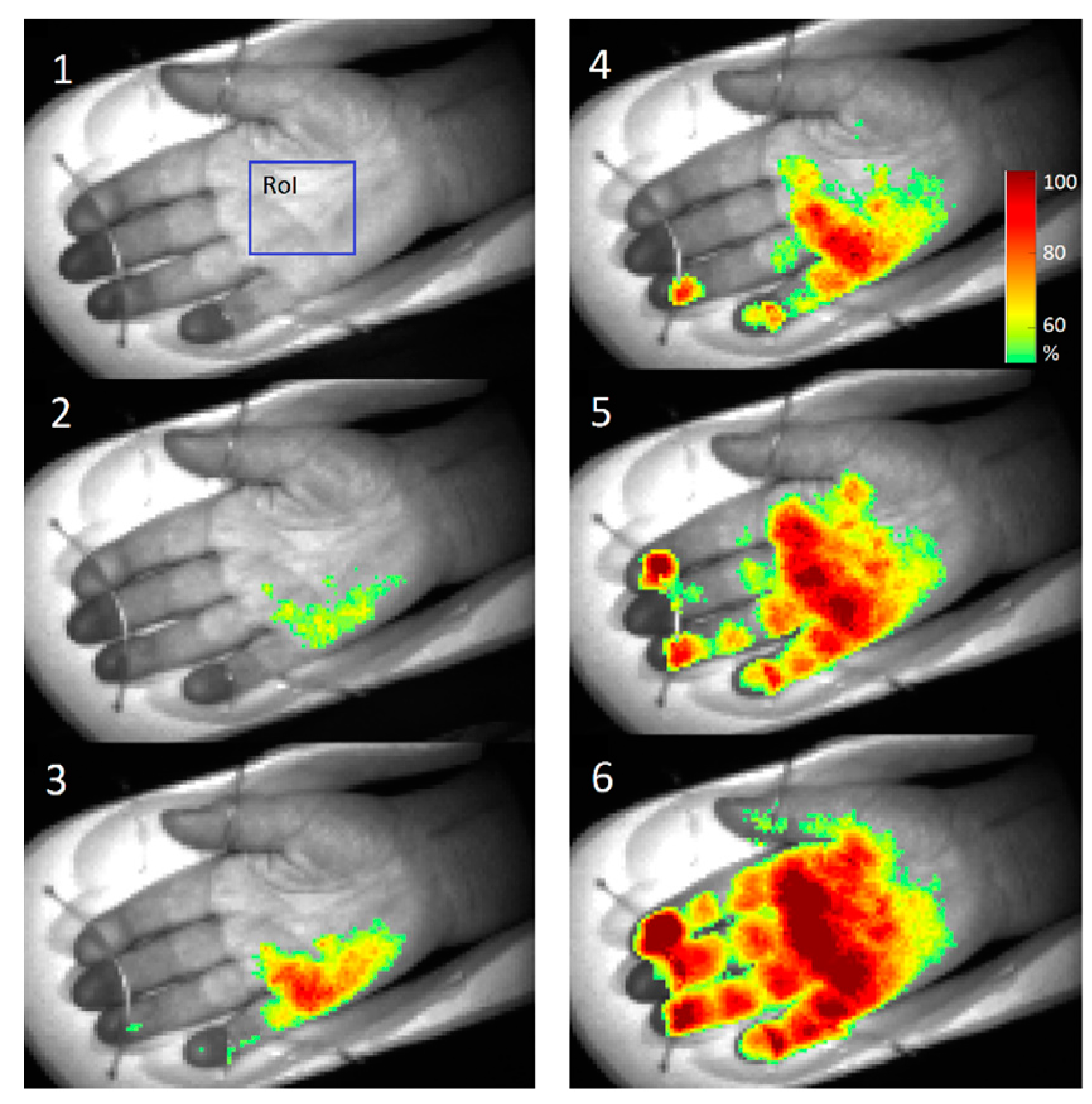
2.3.1. PPGI Prototype for Palm Anesthesia Monitoring
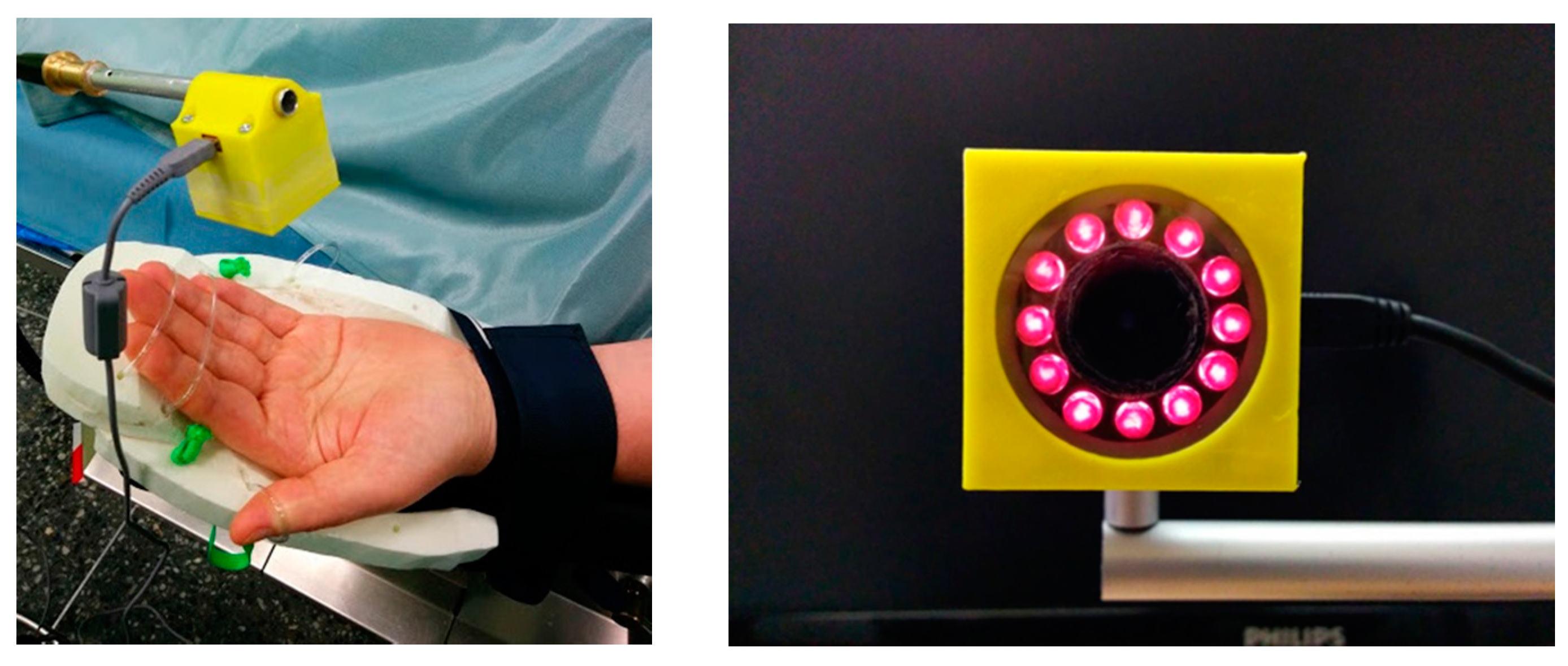
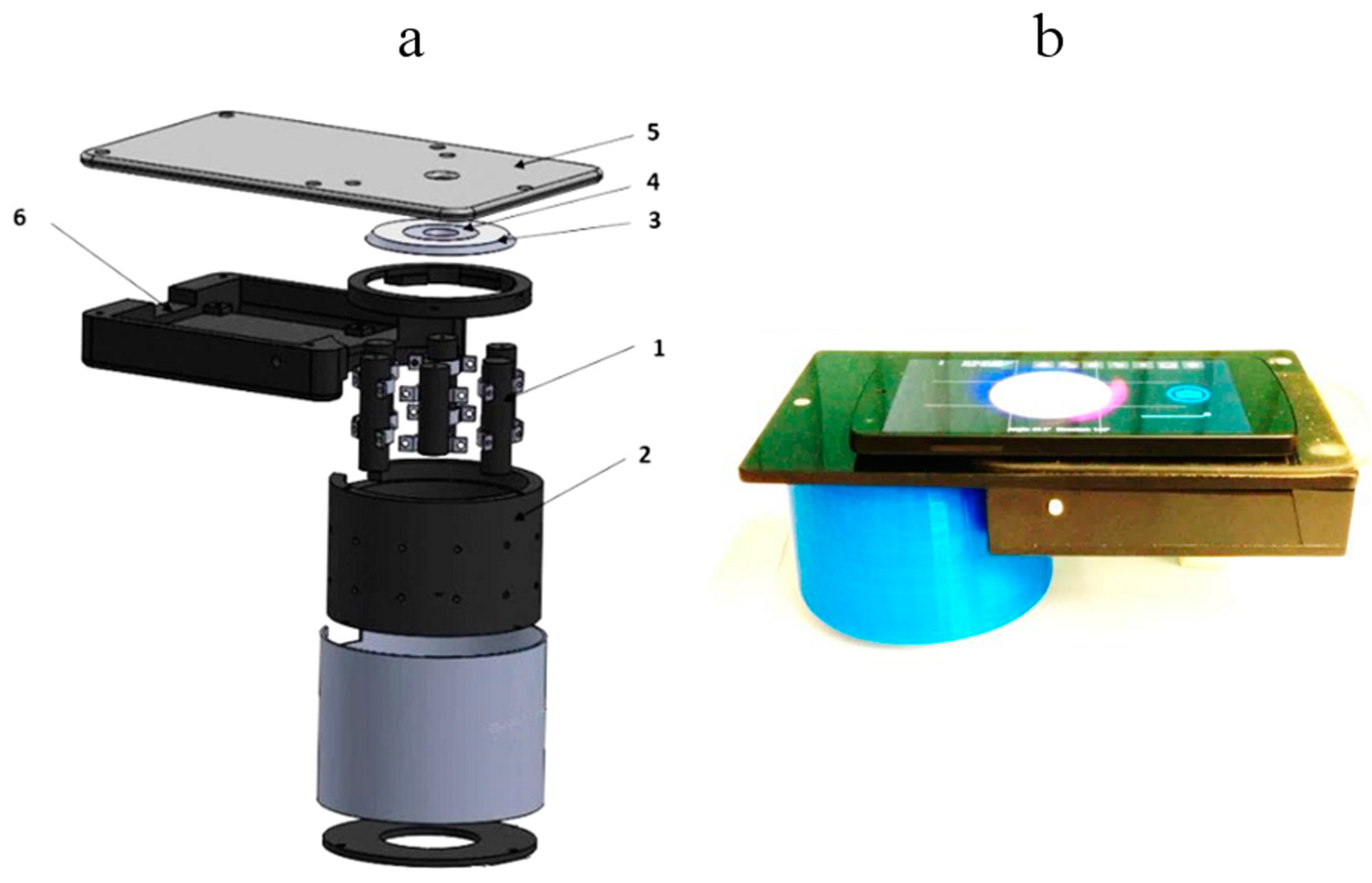
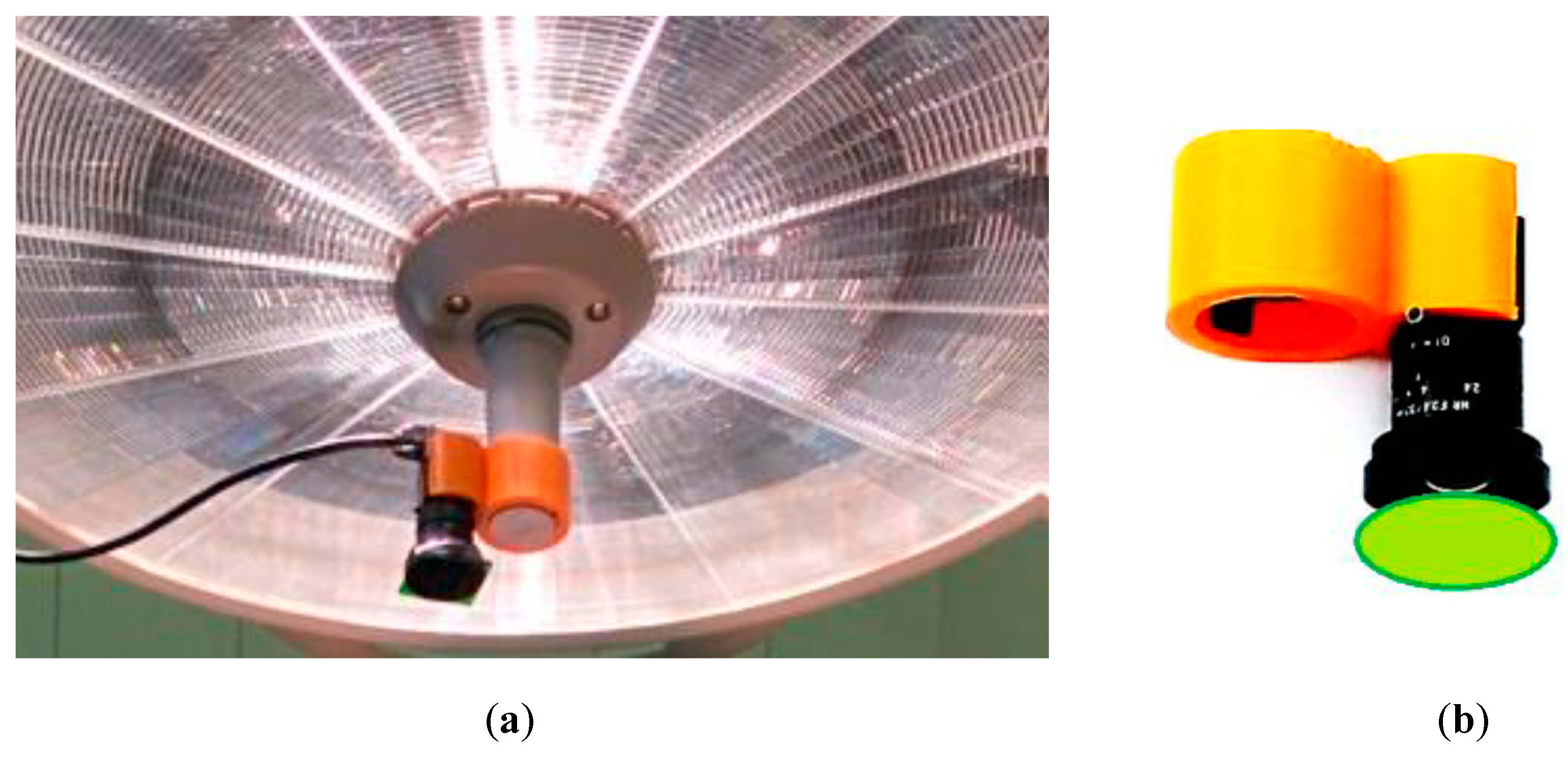
2.3.2. Universal Compact PPPGI Prototypes
2.4. Multimodal Skin Imagers
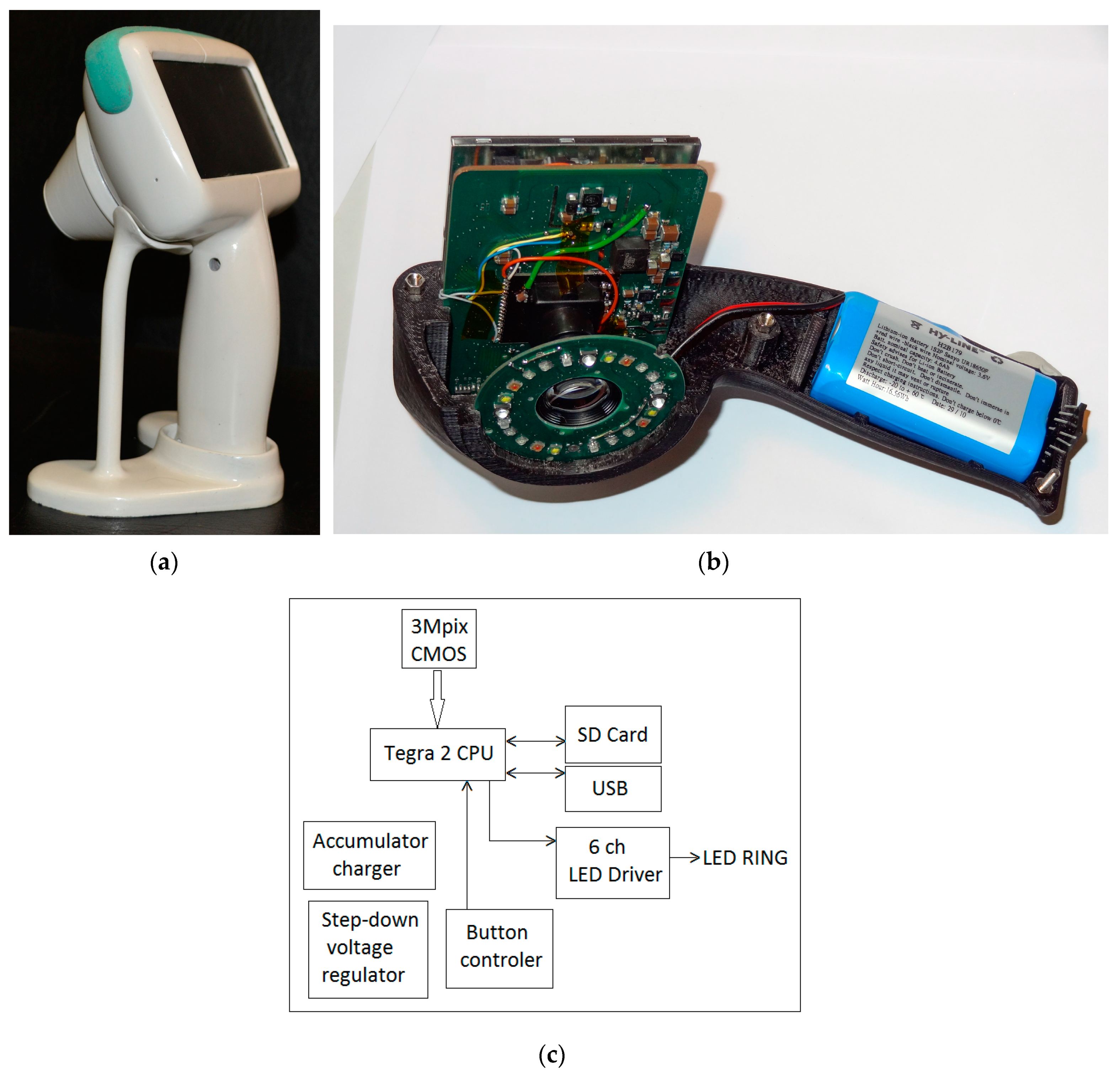
2.4.1. SkImager—A Concept Device for Multimodal Skin Imaging
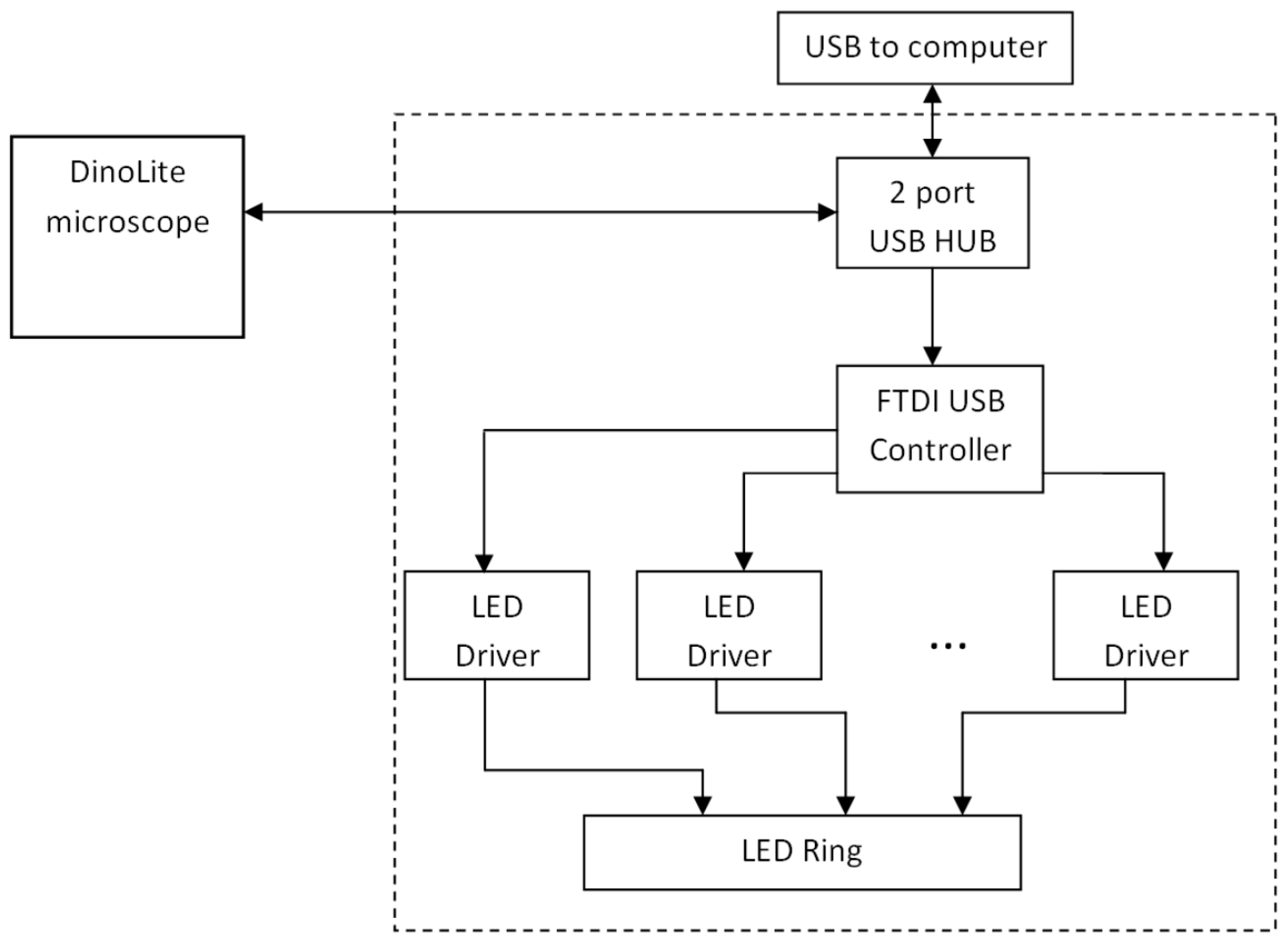
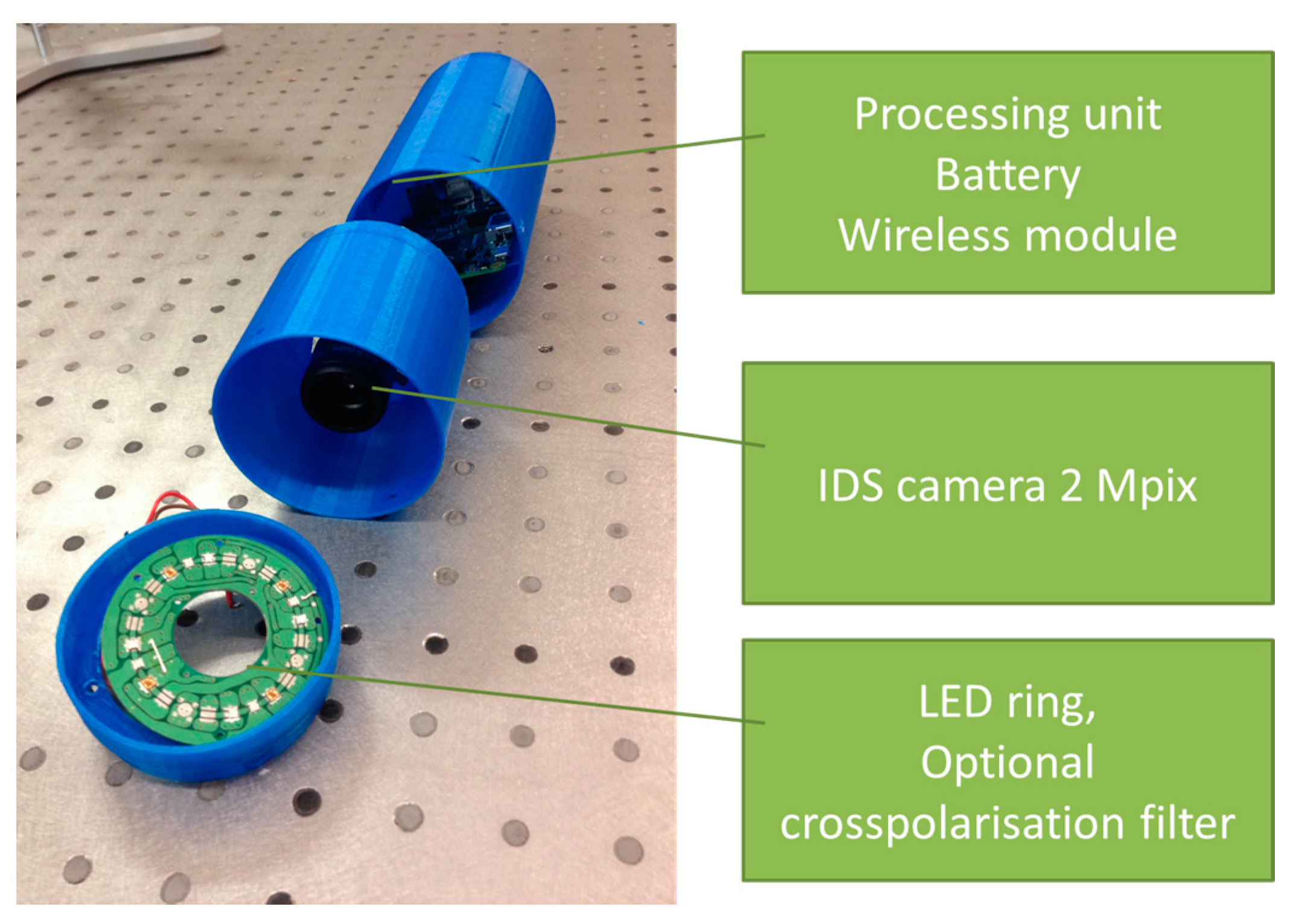
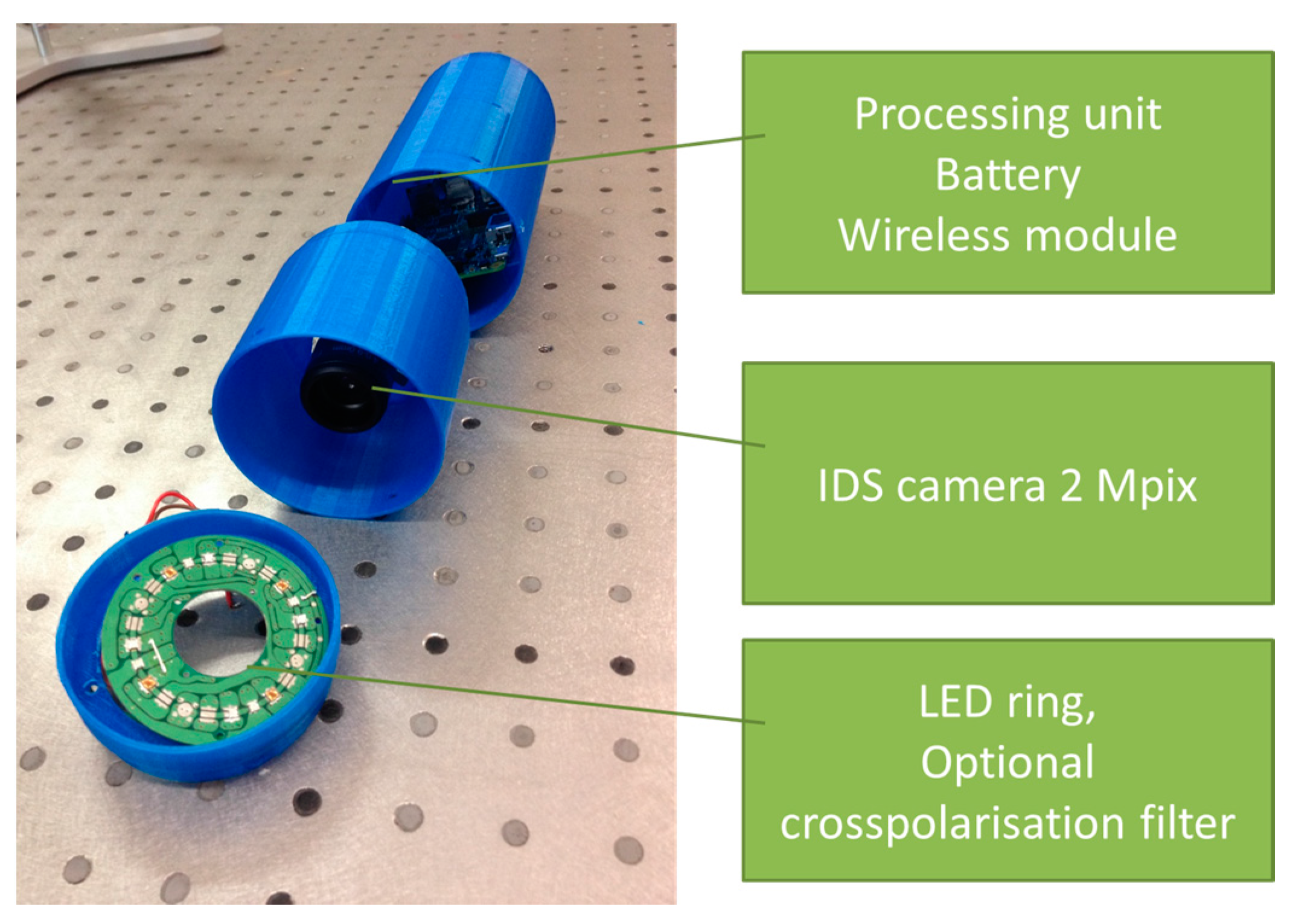
2.4.2. The Modular Multimodal Skin Imager
- Processing, wireless transmission and power block,
- Camera and lens block,
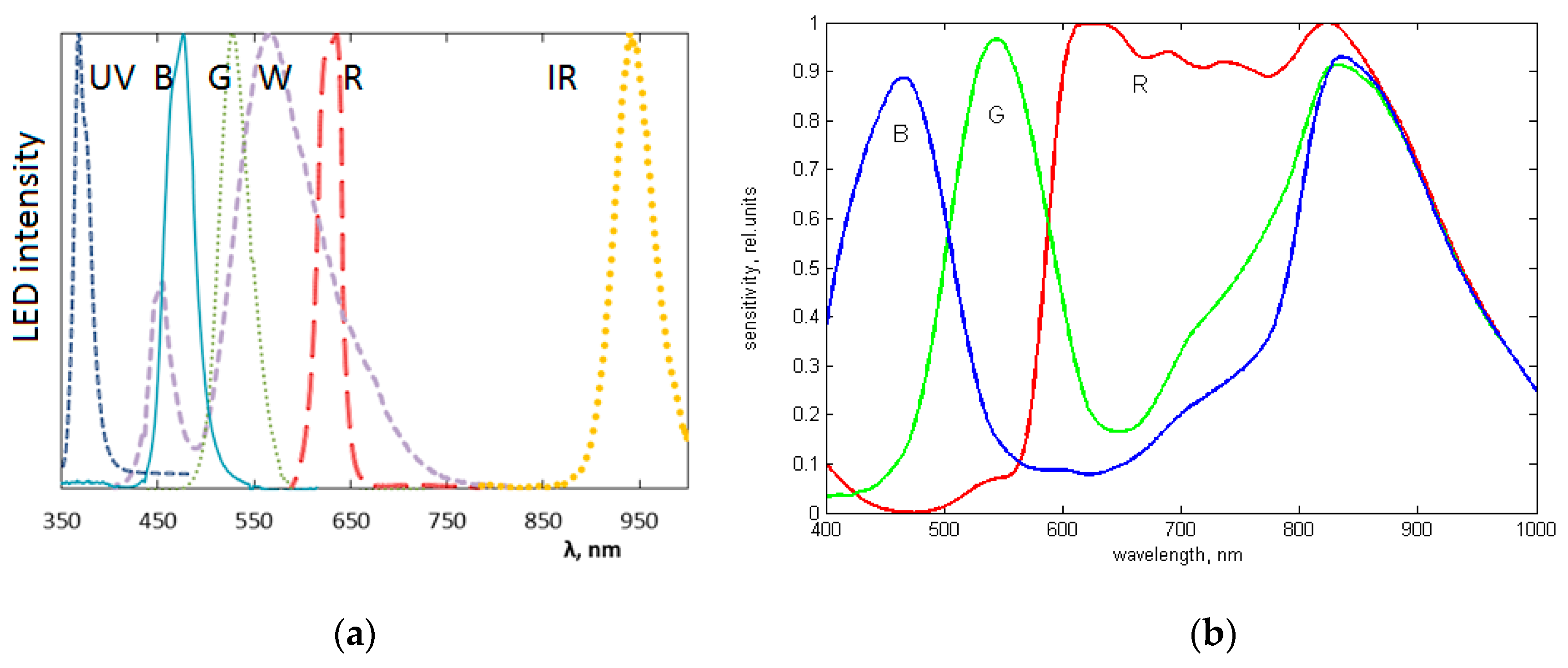
- Illumination block.
3. Results
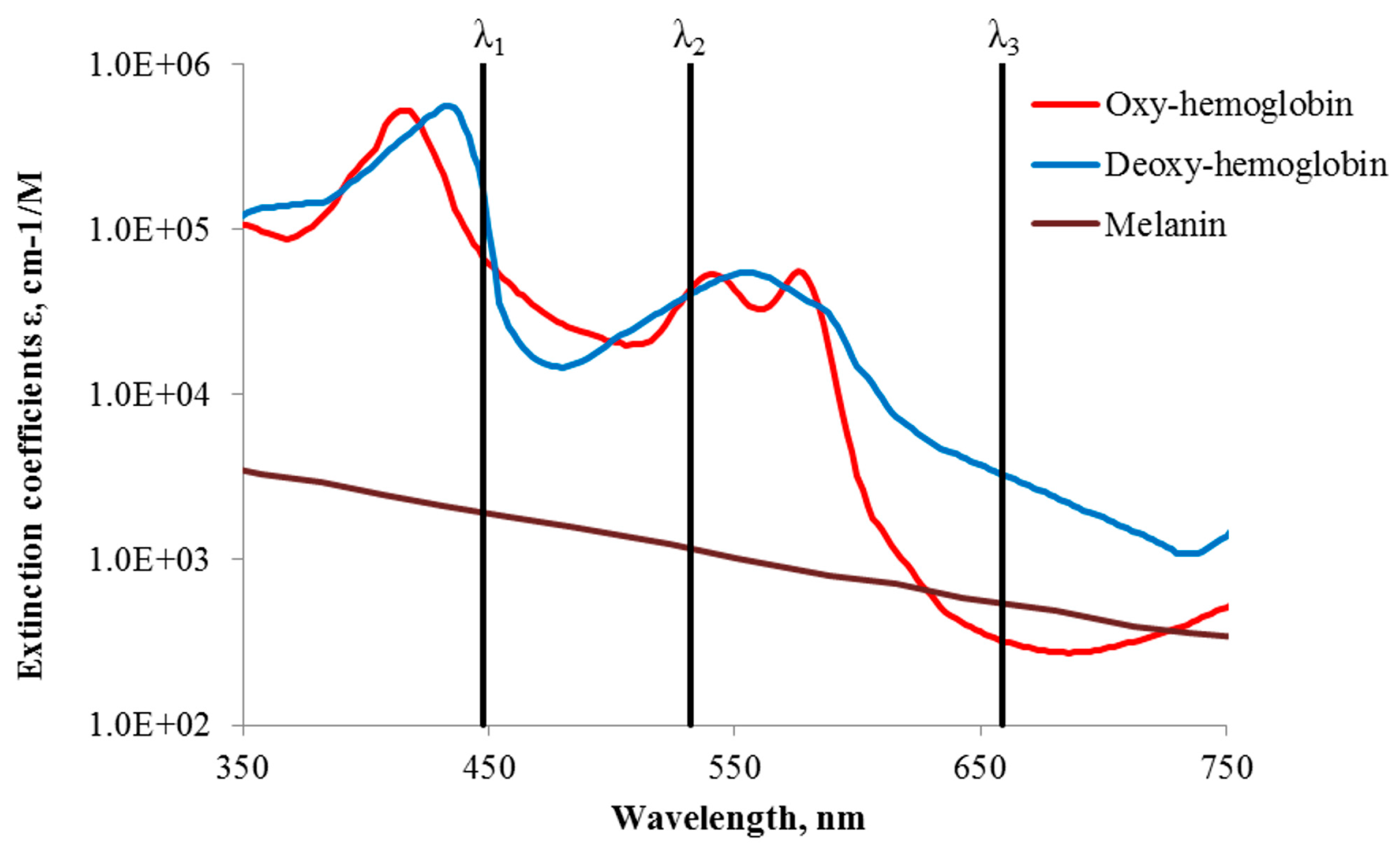
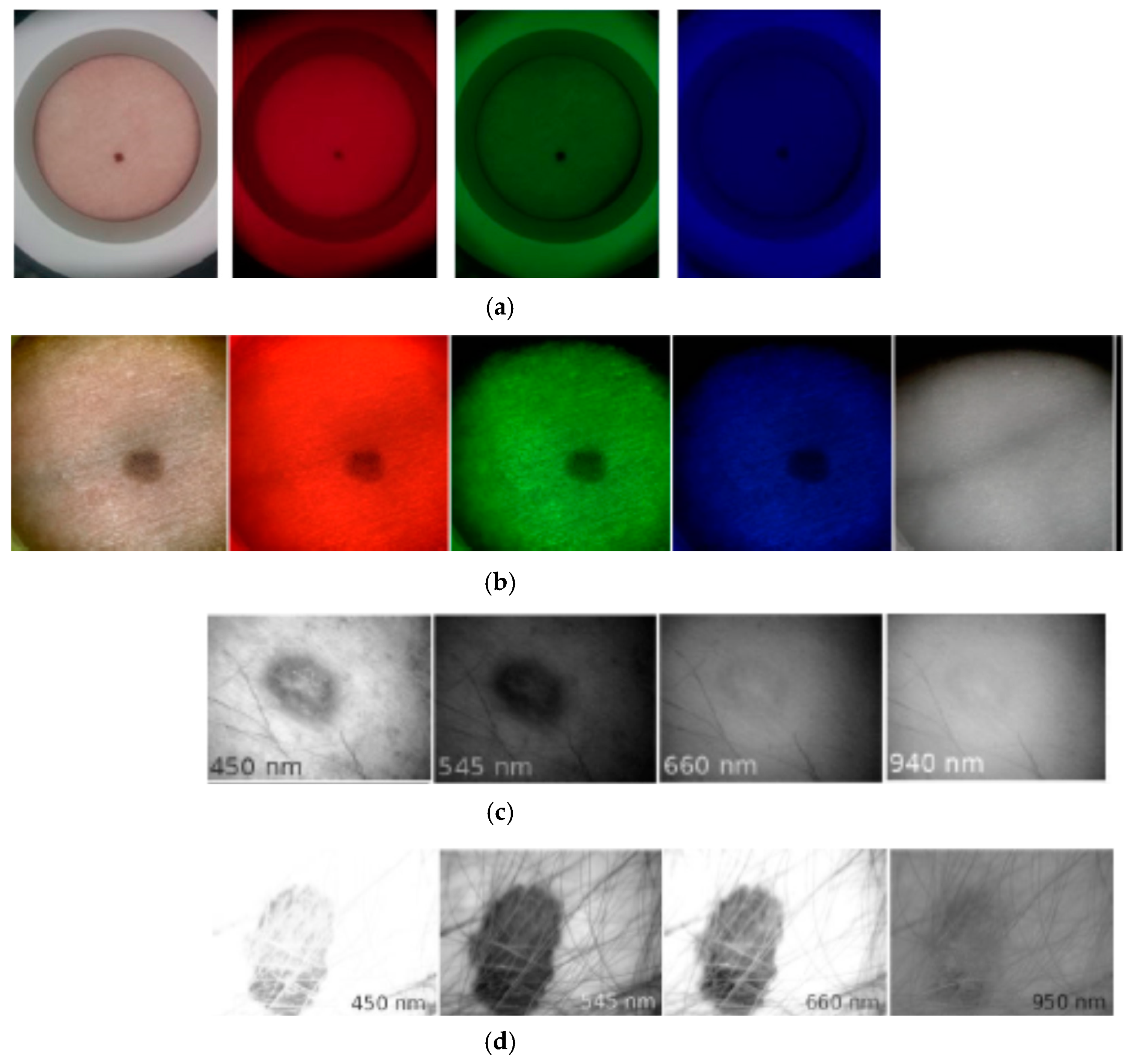
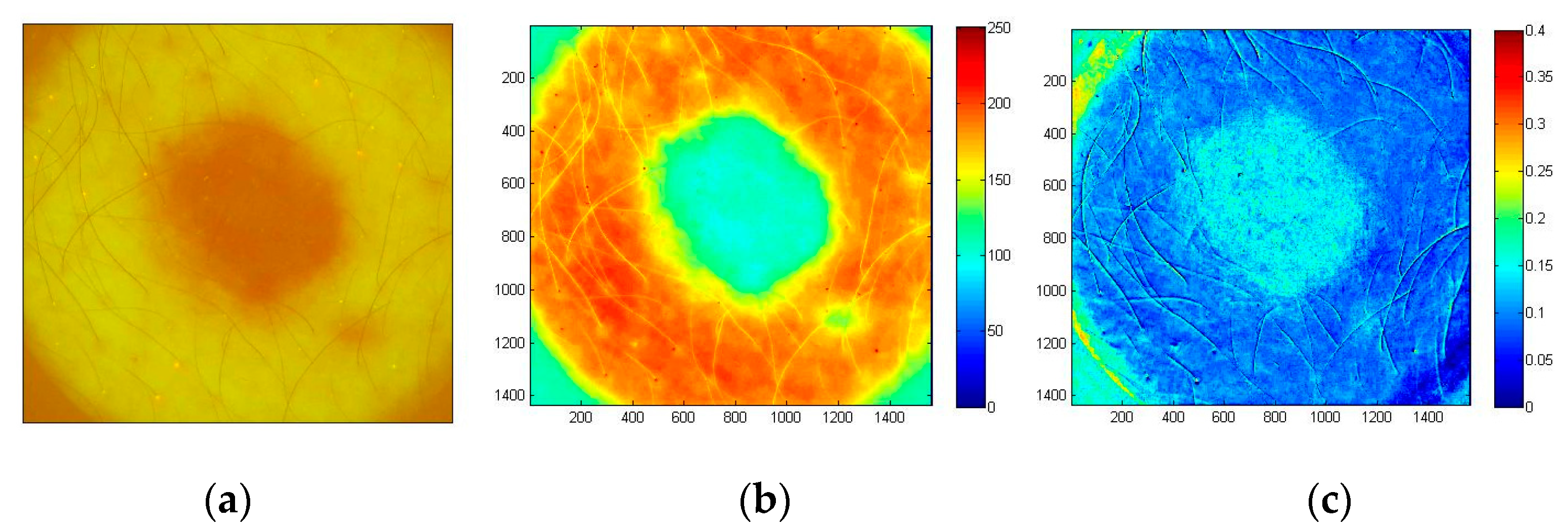
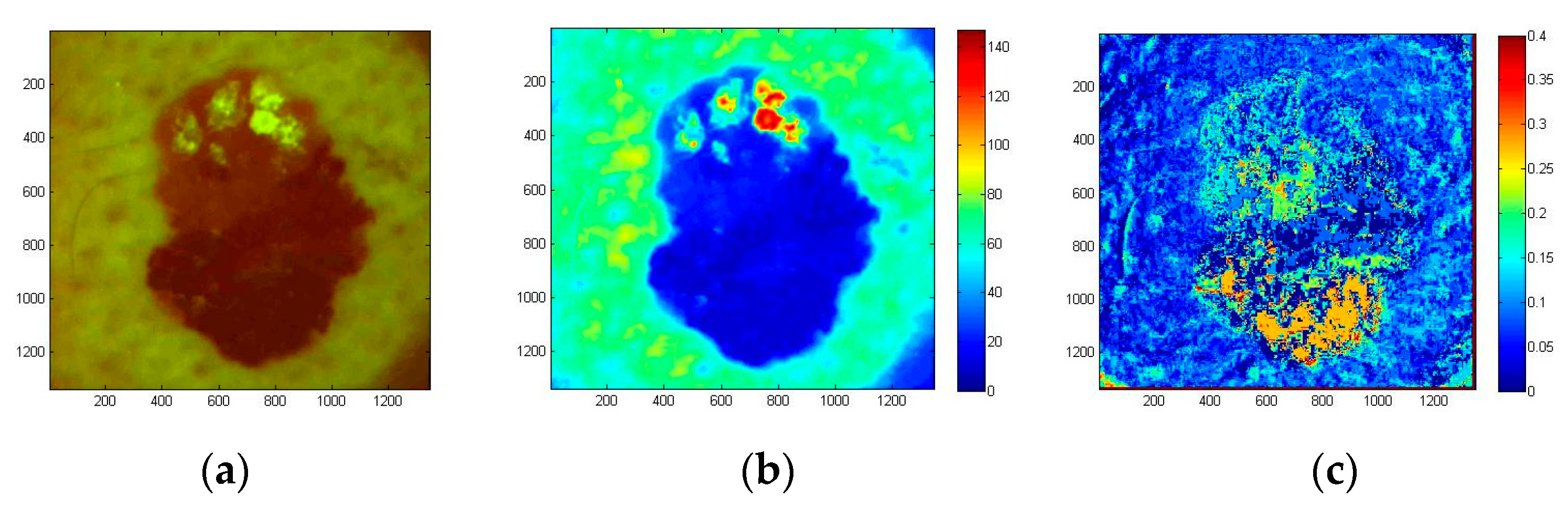
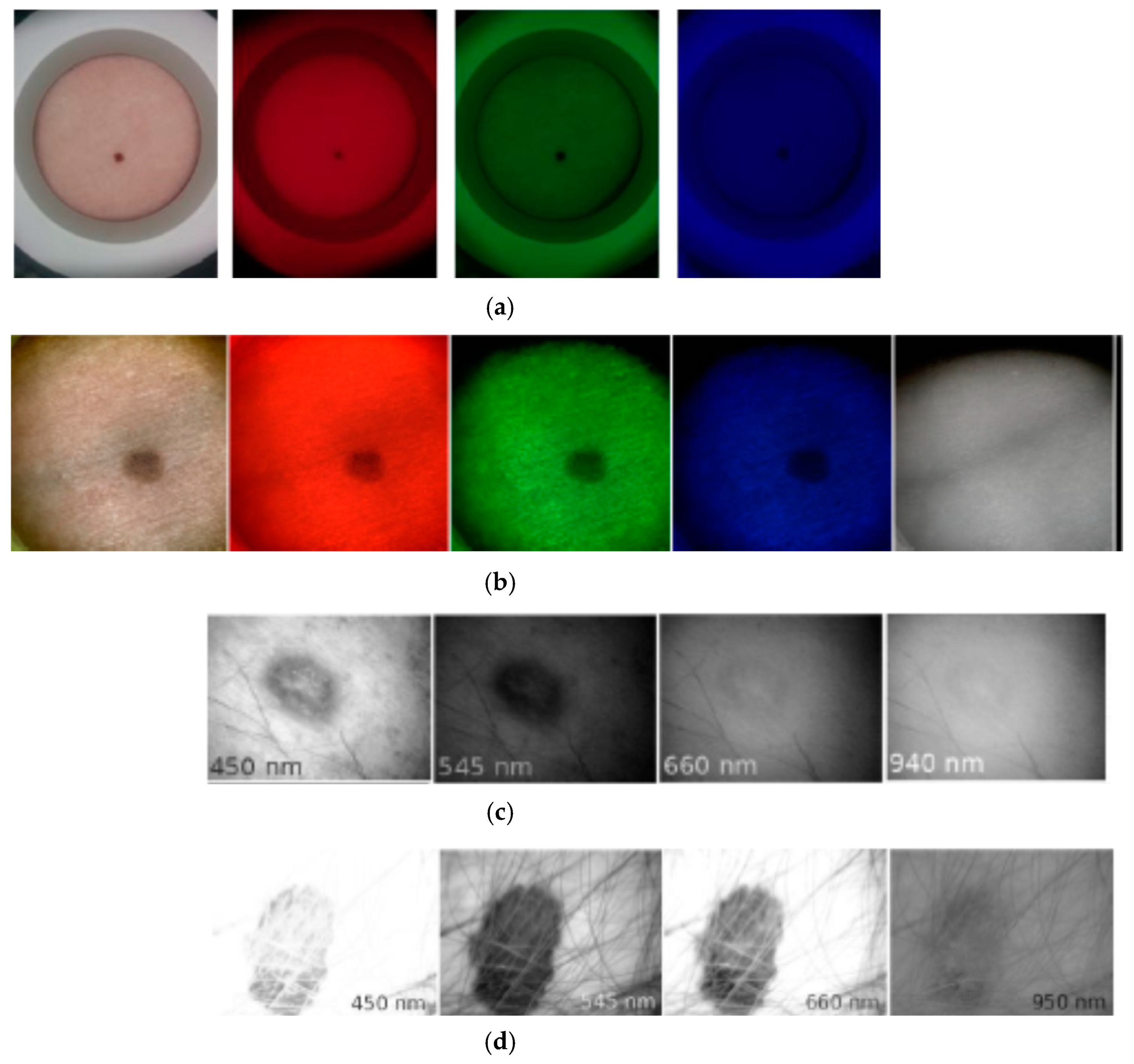
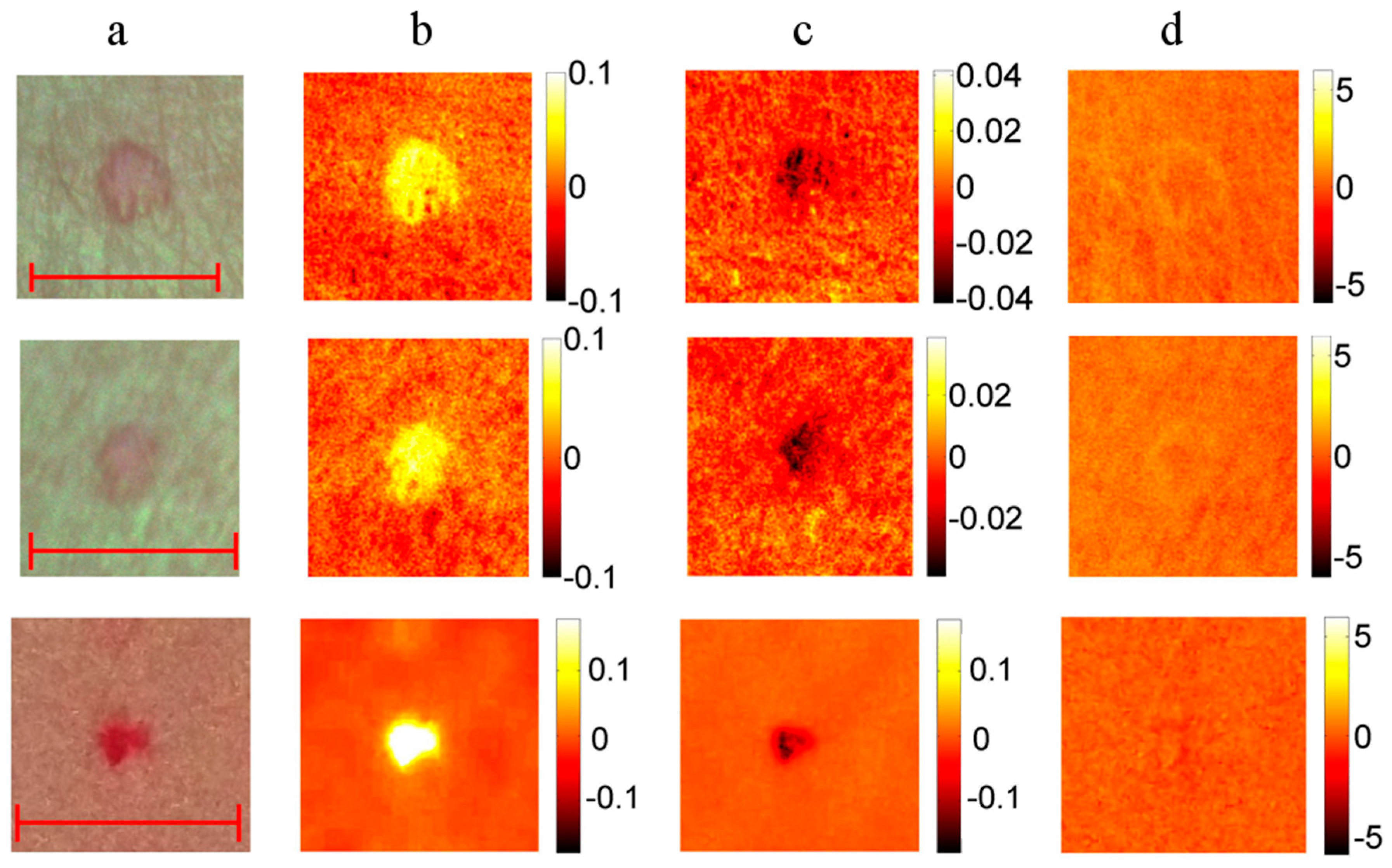
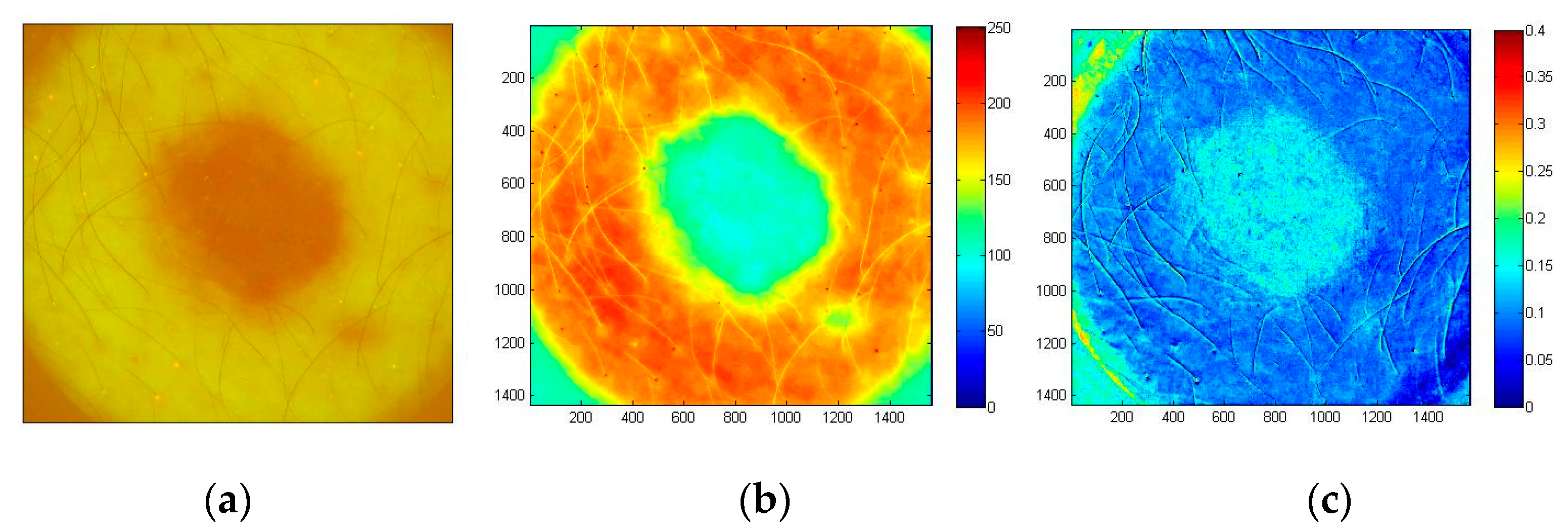
3.1. Clinical Spectral Images and Chromophore Maps of Skin
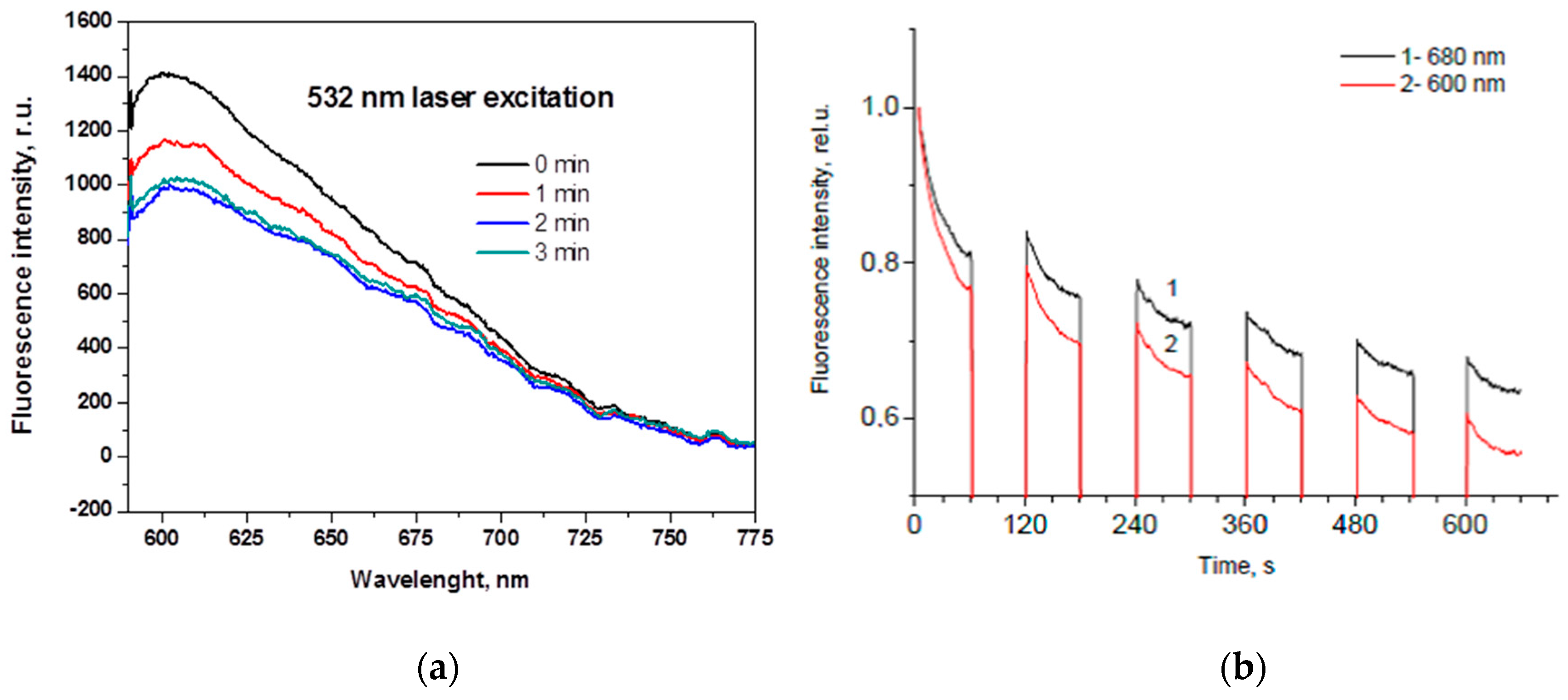
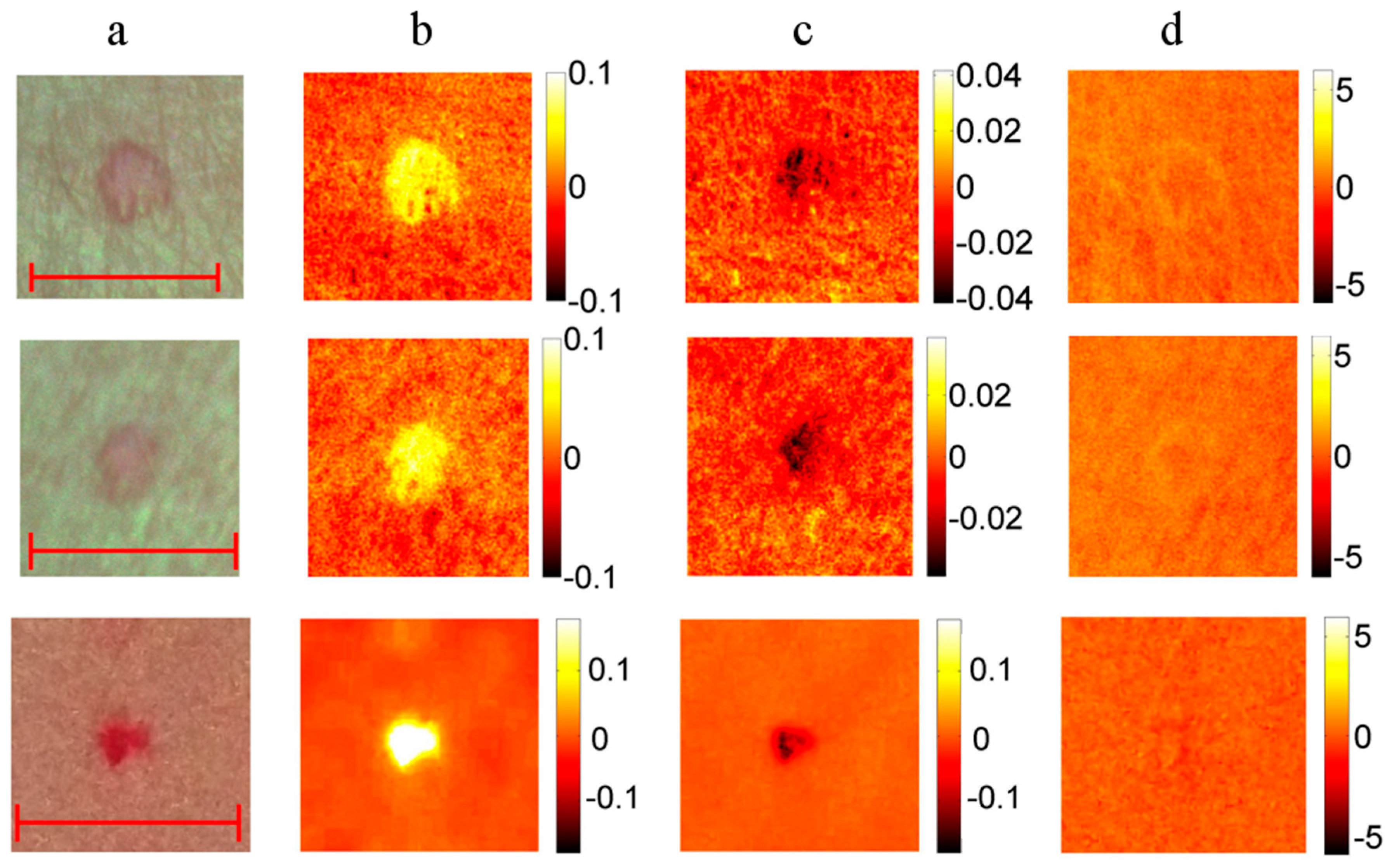
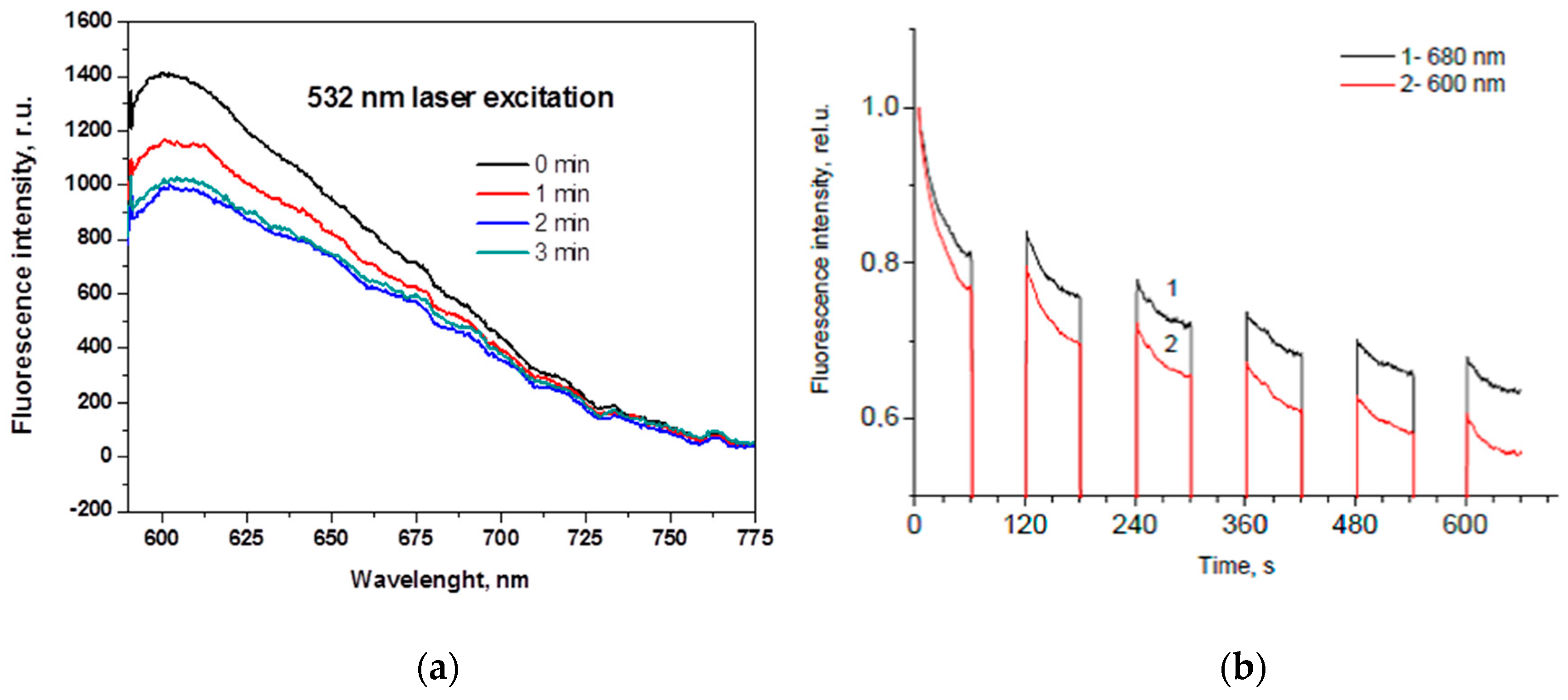
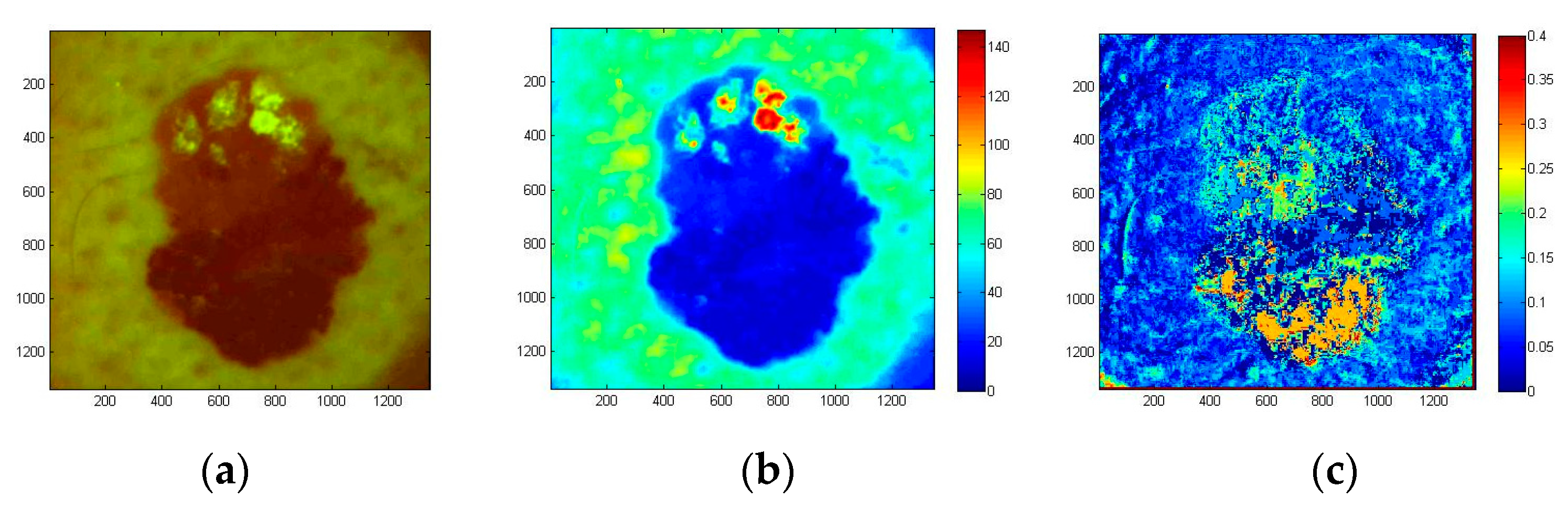
3.2. Fluorescent and Photo-Bleaching Rate Images of Skin Tumors
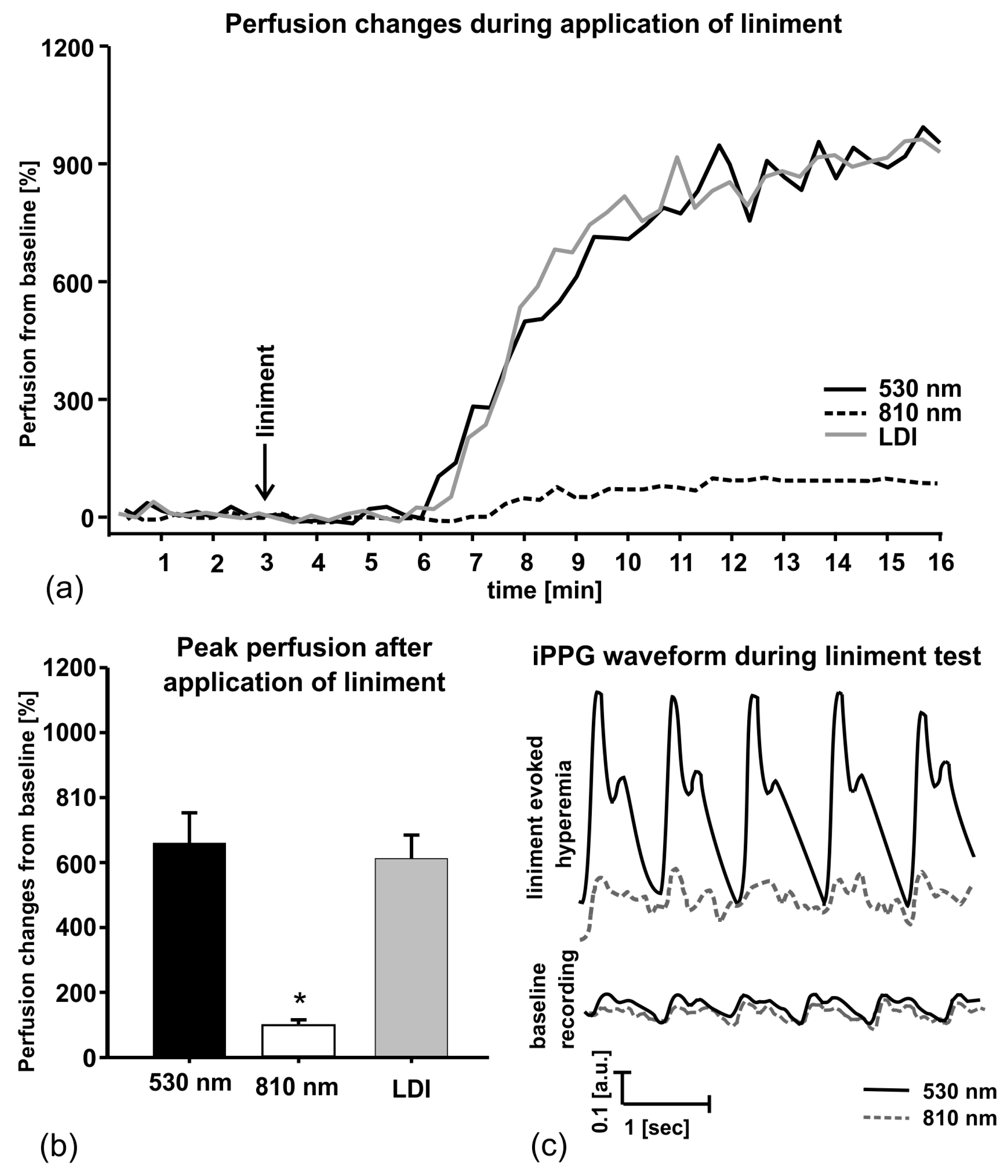
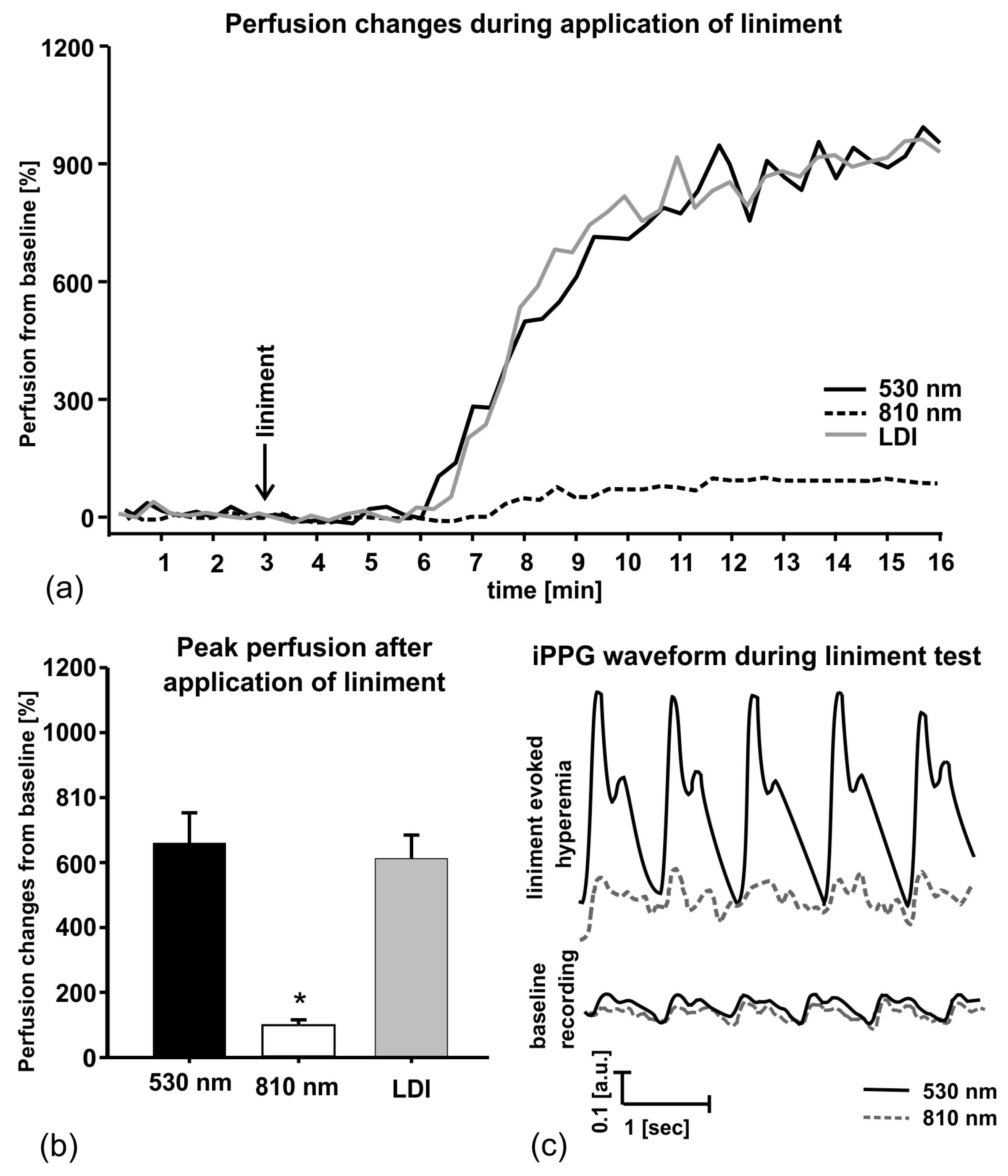
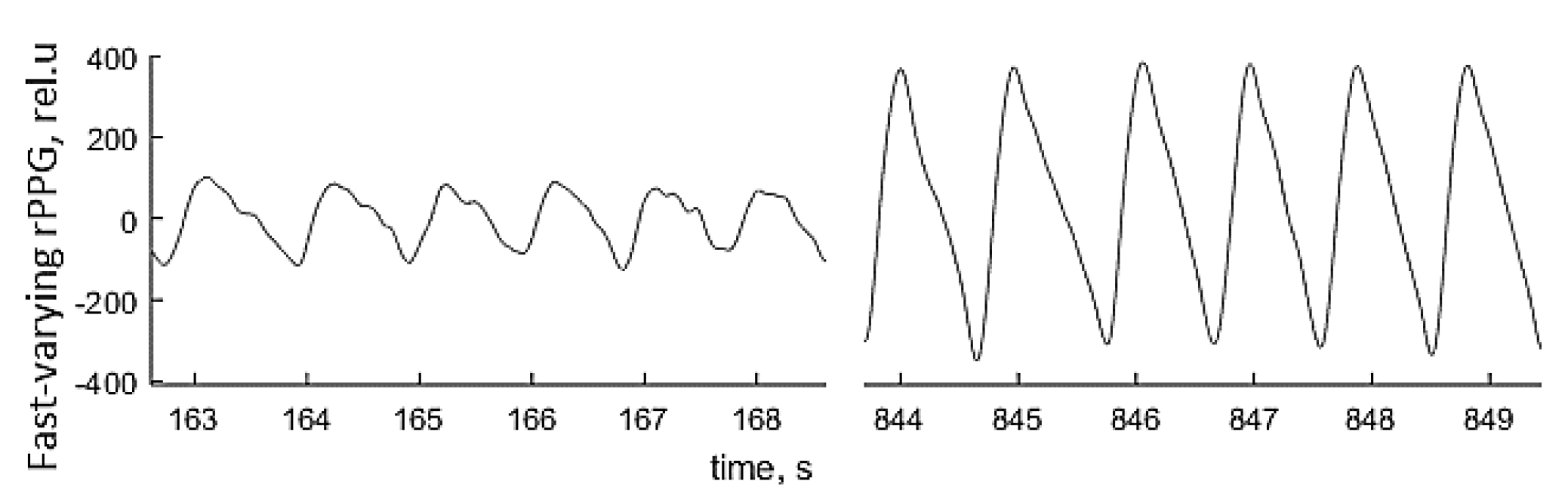
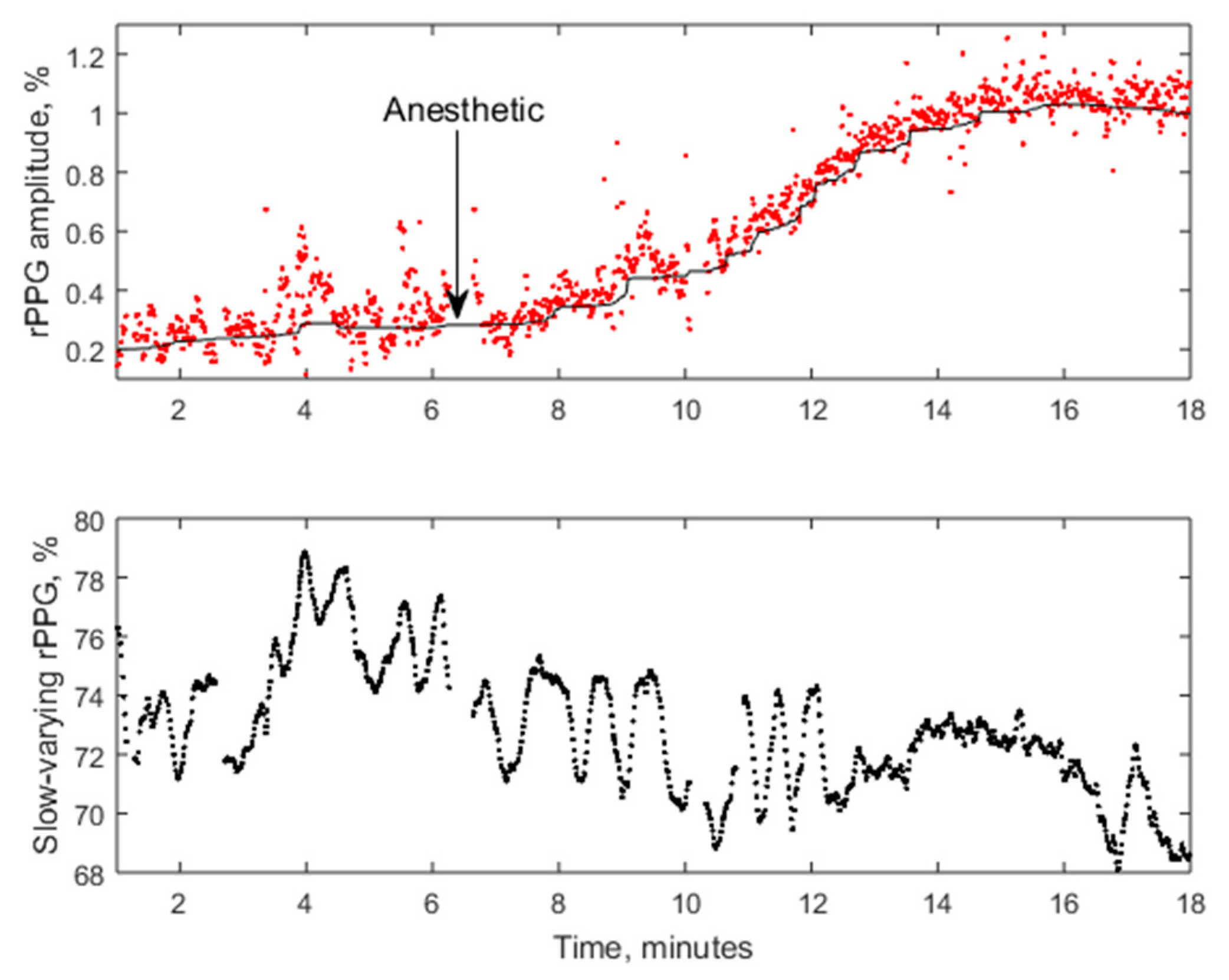
3.3. Skin Blood Perfusion Measurements With the PPGI Prototypes
4. Discussion
Acknowledgments
Conflicts of Interest
References
- MoleMate Siascope Handheld Melanoma Screening System. Available online: http://www.wms.co.uk/Dermatology/Dermatoscopes,Lights_and_Magnifiers/MoleMate_Siascope_Handheld_Melanoma_Screening_System (accessed on 9 April 2017).
- MelaFind. Available online: http://www.melafind.com/melafind/ (accessed on 9 April 2017).
- Que, S.K.T.; Grant-Kels, J.M.; Rabinovitz, H.S.; Oliveiro, M.; Scope, A. Application of handheld confocal microscopy for skin cancer diagnosis. Dermatol. Clin. 2016, 34, 469–475. [Google Scholar] [CrossRef] [PubMed]
- DermaInspect. Available online: http://www.jenlab.de/DermaInspect.29.0.html?&L=en%3E%22 (accessed on 9 April 2017).
- Dermlight. Available online: https://dermlite.com/ (accessed on 9 April 2017).
- Dlite Microscope. Available online: http://skinandhairscope.com/Products/Dlite/Dlite.php (accessed on 9 April 2017).
- Skinvision. Available online: https://www.skinvision.com/technology-skin-cancer-melanoma-mobile-app (accessed on 12 March 2017).
- Vidovič, L.; Milanič, M.; Randeberg, L.L.; Majaron, B. Quantitative characterization of traumatic bruises by combined pulsed photothermal radiometry and diffuse reflectance spectroscopy. Proc. SPIE 2015, 9303, 930307. [Google Scholar] [CrossRef]
- Spigulis, J. Biophotonic technologies for noninvasive assessment of skin condition and blood microcirculation. Latv. J. Phys. Techn. Sci. 2012, 49, 63–80. [Google Scholar]
- Multispectral Imaging. Available online: http://www.imaging.org/site/PDFS/Reporter/Articles/REP27_4_CIC20_TOMINAGA_p177.pdf (accessed on 12 March 2017).
- Jakovels, D.; Spigulis, J.; Rogule, L. RGB mapping of hemoglobin distribution in skin. Proc. SPIE 2011, 8087, 80872B. [Google Scholar]
- Jakovels, D.; Kuzmina, I.; Berzina, A.; Valeine, L.; Spigulis, J. Noncontact monitoring of vascular lesion phototherapy efficiency by RGB multispectral imaging. J. Biomed. Opt. 2013, 18, 126019. [Google Scholar] [CrossRef] [PubMed]
- Jakovels, D.; Spigulis, J. 2-D mapping of skin chromophores in the spectral range 500–700 nm. J. Biophoton. 2010, 3, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Jakovels, D.; Spigulis, J. RGB imaging device for mapping and monitoring of hemoglobin distribution in skin. Lith. J. Phys. 2012, 52, 50–54. [Google Scholar] [CrossRef]
- Philips Vital Signs Camera. Available online: http://www.vitalsignscamera.com/ (accessed on 12 March 2017).
- The Best Heart Disease iPhone & Android Apps of the Year. Available online: http://www.healthline.com/health-slideshow/top-heart-disease-iphone-android-apps#5 (accessed on 12 March 2017).
- Spigulis, J.; Lacis, M.; Kuzmina, I.; Lihacovs, A.; Upmalis, V.; Rupenheits, Z. Method and Device for Smartphone Mapping of Tissue Compounds. Lv. Patent WO 2017012675 A1, 26 January 2017. [Google Scholar]
- Kuzmina, I.; Lacis, M.; Spigulis, J.; Berzina, A.; Valaine, L. Study of smartphone suitability for mapping of skin chromophores. J. Biomed. Opt. 2015, 20, 090503. [Google Scholar] [CrossRef] [PubMed]
- Dino-Lite for Healthcare. Available online: http://www.dino-lite.com/applications_list.php?index_id=8 (accessed on 12 March 2017).
- Dino-Lite AM4115-FUT. Available online: http://www.dino-lite.com/products_detail.php?index_m1_id=0&index_m2_id=0&index_id=61 (accessed on 12 March 2017).
- Rubins, U.; Zaharans, J.; Lihacova, I.; Spigulis, J. Multispectral video-microscope modified for skin diagnostics. Latv. J. Phys. Techn. Sci. 2014, 51, 65–70. [Google Scholar] [CrossRef]
- Diebele, I.; Kuzmina, I.; Lihachev, A.; Spigulis, J.; Kapostinsh, J.; Derjabo, A.; Valaine, L. Clinical evaluation of melanomas and common nevi by spectral imaging. Biomed. Opt. Express 2012, 3, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Bekina, A.; Diebele, I.; Rubins, U.; Zaharans, J.; Derjabo, A.; Spigulis, J. Multispectral assessment of skin malformations by modified video-microscope. Latv. J. Phys. Techn. Sci. 2012, 49, 4–8. [Google Scholar]
- Bekina, A.; Rubins, U.; Lihachova, I.; Zaharans, J.; Spigulis, J. Skin chromophore mapping by means of a modified video-microscope for skin malformation diagnosis. Proc. SPIE 2013, 8856, 88562G. [Google Scholar]
- Spigulis, J.; Elste, L. Method and Device for Imaging of Spectral Reflectance at Several Wavelength Bands. Lv. Patent WO2013135311 A1, 19 September 2013. [Google Scholar]
- Spigulis, J.; Jakovels, D.; Rubins, U. Multi-spectral skin imaging by a consumer photo-camera. Proc. SPIE 2010, 7557, 75570M. [Google Scholar]
- Spigulis, J.; Oshina, I. Snapshot RGB mapping of skin melanin and hemoglobin. J. Biomed. Opt. 2015, 20, 050503. [Google Scholar] [CrossRef] [PubMed]
- Spigulis, J.; Oshina, I.; Berzina, A.; Bykov, A. Smartphone snapshot mapping of skin chromophores under triple-wavelength laser illumination. J. Biomed. Opt. 2017, 22, 091508. [Google Scholar] [CrossRef] [PubMed]
- Prahl, S. Tabulated Molar Extinction Coefficient for Hemoglobin in Water. Available online: http://omlc.ogi.edu/spectra/hemoglobin/summary.html (accessed on 30 November 2016).
- Sarna, T.; Swartz, H.M. The Physical Properties of Melanin. Available online: http://omlc.ogi.edu/spectra/melanin/eumelanin.html (accessed on 30 November 2016).
- Spigulis, J.; Elste, L. Single-snapshot RGB multispectral imaging at fixed wavelengths: proof of concept. Proc. SPIE 2014, 8937, 89370L. [Google Scholar]
- Spigulis, J.; Oshina, I. Method and Device for Chromophore Mapping under Illumination by Several Spectral Lines. Lv. Patent 15106 B, 20 March 2016. [Google Scholar]
- Rubins, U.; Kviesis-Kipge, E.; Spigulis, J. Device for Obtaining Speckle-Free Images at Illumination by Scattered Laser Beams. Lv. Patent P-17-17, 10 May 2017. [Google Scholar]
- Oshina, I.; Spigulis, J.; Rubins, U.; Kviesis-Kipge, E.; Lauberts, K. Express RGB mapping of three to five skin chromophores. OSA Tech. Dig. 2017, in press. [Google Scholar]
- Lihachev, A.; Lesins, J.; Jakovels, D.; Spigulis, J. Low power cw-laser signatures on human skin. Quant. Electron. 2010, 40, 1077–1080. [Google Scholar] [CrossRef]
- Lihachev, A. Kinetics of Laser-Excited In-Vivo Skin Autofluorescence and Remission. Ph.D. Thesis, University of Latvia, Riga, Latvia, 2010. [Google Scholar]
- Lesinsh, J.; Lihachev, A.; Rudys, R.; Bagdonas, S.; Spigulis, J. Skin autofluorescence photobleaching and photo-memory. Proc. SPIE 2011, 8092, 80920N. [Google Scholar]
- Spigulis, J.; Lihachev, A.; Erts, R. Imaging of laser-excited tissue autofluorescence bleaching rates. Appl. Opt. 2009, 48, D163–D168. [Google Scholar] [CrossRef] [PubMed]
- Lihachev, A.; Derjabo, A.; Ferulova, I.; Lange, M.; Lihacova, I.; Spigulis, J. Autofluorescence imaging of Basal Cell Carcinoma by smartphone RGB camera. J. Biomed. Opt. 2015, 20, 120502. [Google Scholar] [CrossRef] [PubMed]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1. [Google Scholar] [CrossRef] [PubMed]
- Spigulis, J. Optical non-invasive monitoring of skin blood pulsations. Appl. Opt. 2005, 44, 1850–1857. [Google Scholar] [CrossRef] [PubMed]
- Rubins, U.; Upmalis, V.; Rubenis, O.; Jakovels, D.; Spigulis, J. Real-time photoplethysmography imaging system. Proc. IFMBE 2011, 34, 183–186. [Google Scholar]
- Rubins, U.; Spigulis, J.; Miscuks, A. Photoplethysmography imaging algorithm for continuous monitoring of regional anesthesia. In Proceedings of the 2016 ACM/IEEE 14th Symposium on Embedded Systems for Real-Time Multimedia, Pittsburgh, PA, USA, 6–7 October 2016. [Google Scholar] [CrossRef]
- Rubins, U.; Spigulis, J.; Miscuks, A. Application of color magnification technique for revealing skin microcircuration changes under regional anaesthetic input. Proc. SPIE 2013, 9032, 903203. [Google Scholar]
- Spigulis, J.; Gailite, L.; Lihachev, A.; Erts, R. Simultaneous recording of skin blood pulsations at different vascular depths by multi-wavelength photoplethysmography. Appl. Opt. 2007, 46, 1754–1759. [Google Scholar] [CrossRef] [PubMed]
- Marcinkevics, Z.; Rubins, U.; Zaharans, J.; Miscuks, A.; Urtane, E.; Ozolina-Moll, L. Imaging photoplethysmography for clinical assessment of cutaneous microcirculation at two different depths. J. Biomed. Opt. 2016, 21, 35005. [Google Scholar] [CrossRef] [PubMed]
- Rubins, U.; Miscuks, A.; Lange, M. Simple and convenient remote photoplethysmography system for monitoring regional anesthesia effectiveness. In Proceedings of the EMBEC-NBC2017, Tampere, Finland, 12–15 June 2017. in press. [Google Scholar]
- Spigulis, J.; Garancis, V.; Rubins, U.; Zaharans, E.; Zaharans, J.; Elste, L. A device for multimodal imaging of skin. Proc. SPIE 2013, 8574, 85740J. [Google Scholar]
- Spigulis, J.; Rubins, U.; Kviesis-Kipge, E.; Rubenis, O. SkImager: A concept device for in-vivo skin assessment by multimodal imaging. Proc. Est. Acad. Sci. 2014, 63, 213–220. [Google Scholar] [CrossRef]
- Spigulis, J.; Rubins, U.; Kviesis-Kipge, E. Multimodal Imaging Device for Non-Contact Skin Diagnostics. Lv. Patent 14749 B, 20 November 2013. [Google Scholar]
- Embedded Linux on Board Computer Description. Available online: https://www.raspberrypi.org/ (accessed on 12 March 2017).
- Industrial USB Cameras Description. Available online: https://en.ids-imaging.com/ (accessed on 12 March 2017).
- Bliznuks, D.; Jakovels, D.; Saknite, I.; Spigulis, J. Mobile platform for online processing of multimodal skin optical images: Using online Matlab server for processing remission, fluorescence and laser speckle images, obtained by using novel handheld device. In Proceedings of the 2015 International Conference on BioPhotonics (BioPhotonics), Florence, Italy, 20–22 May 2015. [Google Scholar] [CrossRef]
- Anderson, R.R.; Parrish, J.A. The optics of human skin. J. Invest. Dermatol. 1981, 77, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Rigel, S.D.; Robinson, K.J.; Ross, I.M.; Friedman, R. Cancer of the Skin: Expert Consult, 2nd ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2011; pp. 99–123. [Google Scholar]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spigulis, J. Multispectral, Fluorescent and Photoplethysmographic Imaging for Remote Skin Assessment. Sensors 2017, 17, 1165. https://doi.org/10.3390/s17051165
Spigulis J. Multispectral, Fluorescent and Photoplethysmographic Imaging for Remote Skin Assessment. Sensors. 2017; 17(5):1165. https://doi.org/10.3390/s17051165
Chicago/Turabian StyleSpigulis, Janis. 2017. "Multispectral, Fluorescent and Photoplethysmographic Imaging for Remote Skin Assessment" Sensors 17, no. 5: 1165. https://doi.org/10.3390/s17051165
APA StyleSpigulis, J. (2017). Multispectral, Fluorescent and Photoplethysmographic Imaging for Remote Skin Assessment. Sensors, 17(5), 1165. https://doi.org/10.3390/s17051165