


Efficacy of Cold Atmospheric Plasma vs. Chemotherapy in Triple-Negative Breast Cancer: A Systematic Review
 , ,
, ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
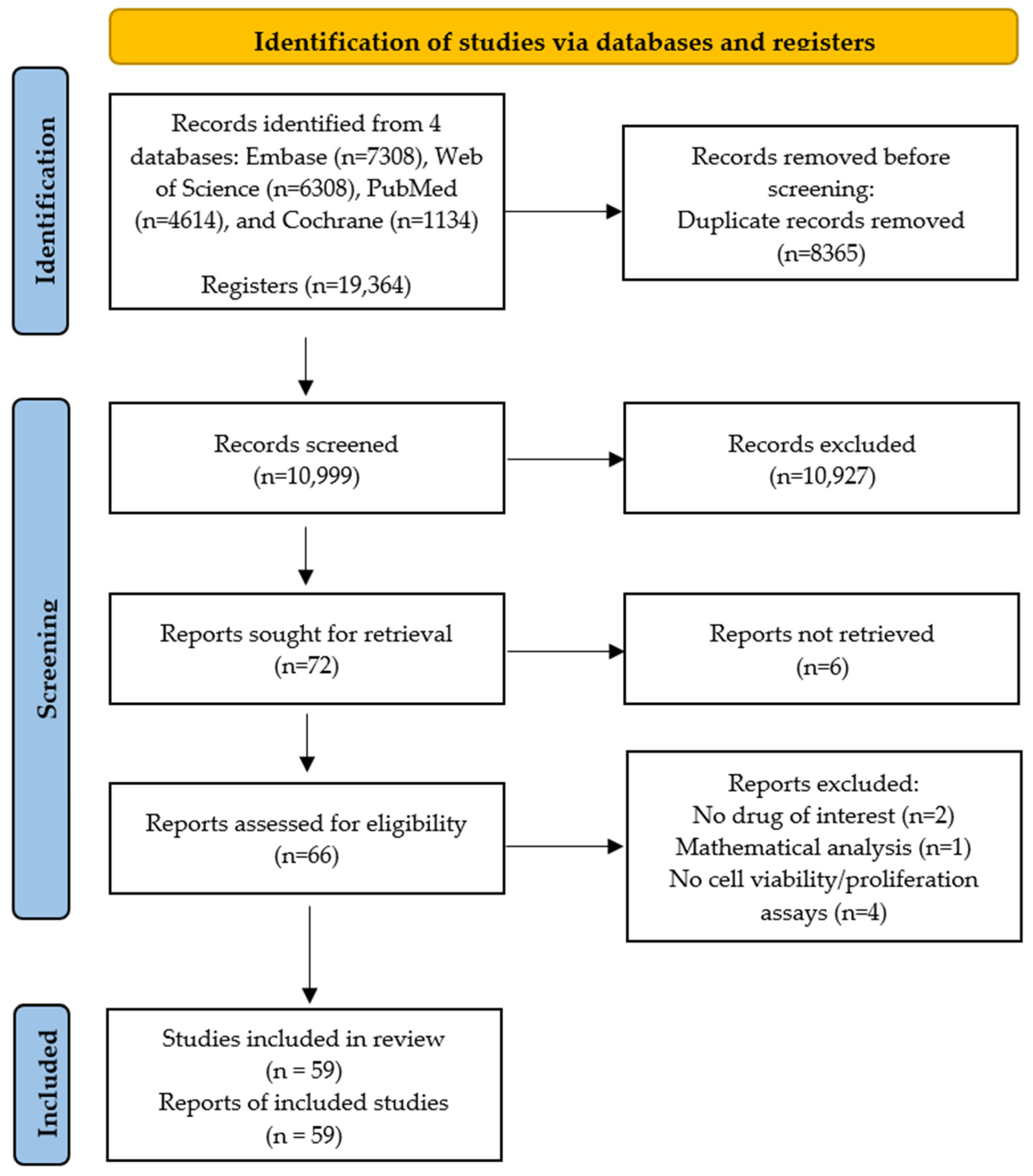
3.1. Study Selection
3.2. Studies’ Characteristics
3.2.1. In Vitro Studies
Chemotherapy
CAP Treatment
CAP Treatment and Chemotherapy
3.2.2. In Vivo Studies
Chemotherapy
CAP Treatment
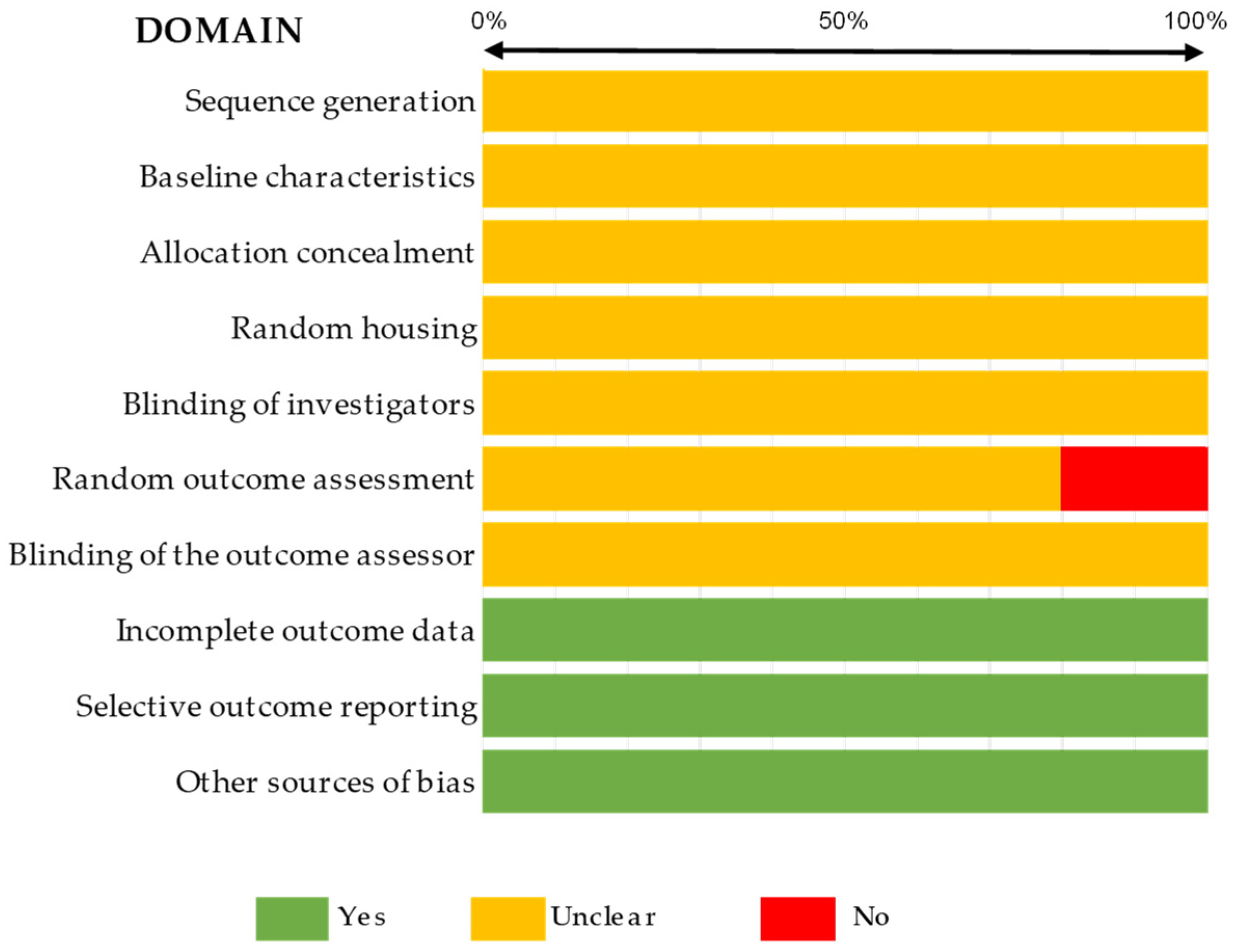
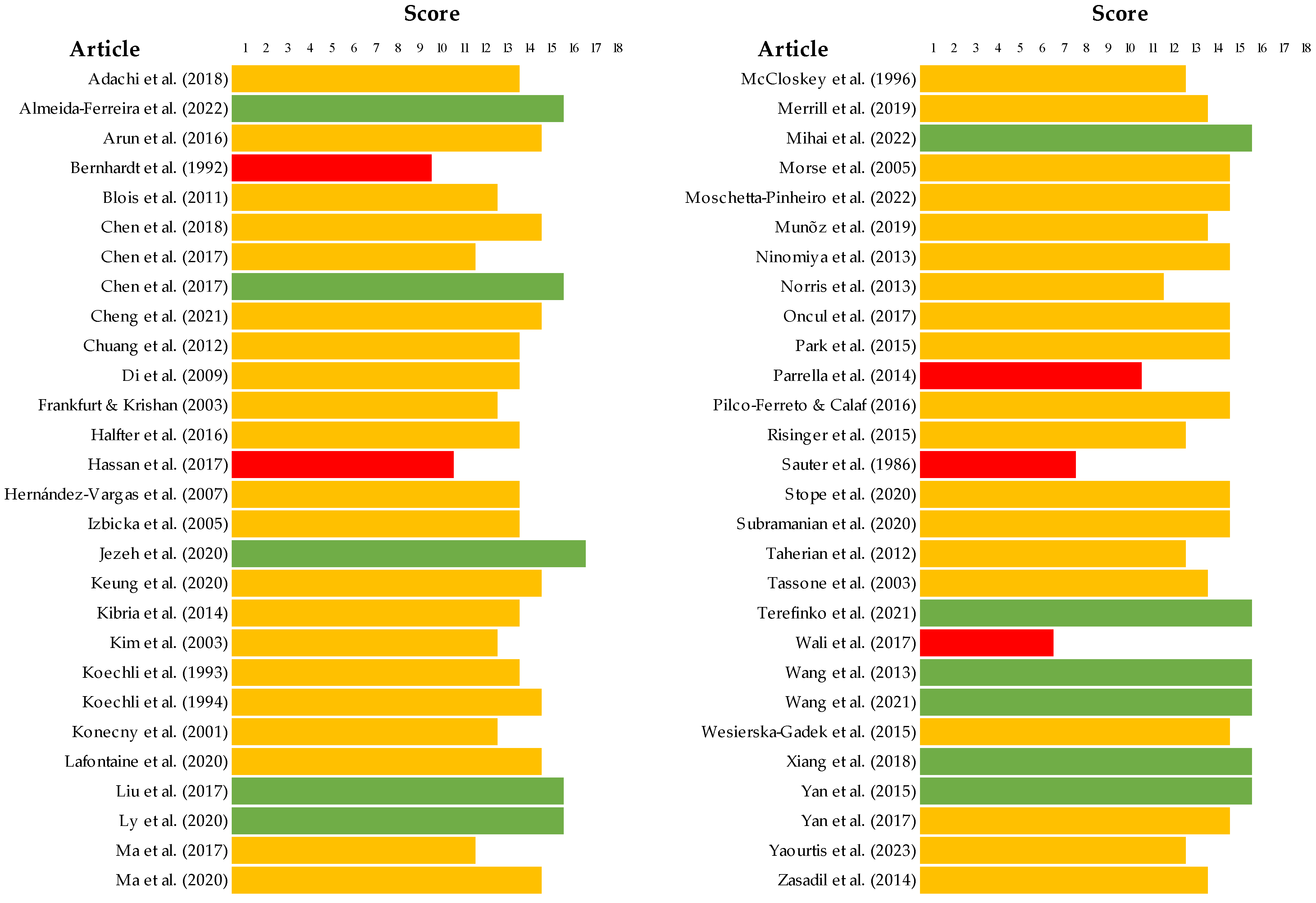
3.3. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Rakha, E.A.; Green, A.R. Molecular classification of breast cancer: What the pathologist needs to know. Pathology 2017, 49, 111–119. [Google Scholar] [CrossRef]
- Palomba, G.; Budroni, M.; Olmeo, N.; Atzori, F.; Ionta, M.T.; Pisano, M.; Tanda, F.; Cossu, A.; Palmieri, G. Triple-negative breast cancer frequency and type of BRCA mutation: Clues from Sardinia. Oncol. Lett. 2014, 7, 948–952. [Google Scholar] [CrossRef][Green Version]
- Provenzano, E.; Ulaner, G.A.; Chin, S.-F. Molecular Classification of Breast Cancer. PET Clin. 2018, 13, 325–338. [Google Scholar] [CrossRef]
- Cosar, R.; Sut, N.; Ozen, A.; Tastekin, E.; Topaloglu, S.; Cicin, I.; Nurlu, D.; Ozler, T.; Demir, S.; Yıldız, G.; et al. Breast Cancer Subtypes and Prognosis: Answers to Subgroup Classification Questions, Identifying the Worst Subgroup in Our Single-Center Series. Breast Cancer Targets Ther. 2022, 14, 259–280. [Google Scholar] [CrossRef]
- Lu, B.; Natarajan, E.; Balaji Raghavendran, H.R.; Markandan, U.D. Molecular Classification, Treatment, and Genetic Biomarkers in Triple-Negative Breast Cancer: A Review. Technol. Cancer Res. Treat. 2023, 22, 15330338221145246. [Google Scholar] [CrossRef]
- Sakach, E.; O’Regan, R.; Meisel, J.; Li, X. Molecular Classification of Triple Negative Breast Cancer and the Emergence of Targeted Therapies. Clin. Breast Cancer 2021, 21, 509–520. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Jovanović, B.; Chen, X.; Estrada, M.V.; Johnson, K.N.; Shyr, Y.; Moses, H.L.; Sanders, M.E.; Pietenpol, J.A. Refinement of Triple-Negative Breast Cancer Molecular Subtypes: Implications for Neoadjuvant Chemotherapy Selection. PLoS ONE 2016, 11, e0157368. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J. Clin. Investig. 2011, 121, 2750. [Google Scholar] [CrossRef]
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef]
- Gennari, A.; André, F.; Barrios, C.H.; Cortés, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 39, 1485–1505. [Google Scholar] [CrossRef]
- Lainetti, P.d.F.; Leis-Filho, A.F.; Laufer-Amorim, R.; Battazza, A.; Fonseca-Alves, C.E. Mechanisms of Resistance to Chemotherapy in Breast Cancer and Possible Targets in Drug Delivery Systems. Pharmaceutics 2020, 12, 1193. [Google Scholar] [CrossRef]
- Izadjoo, M.; Zack, S.; Kim, H.; Skiba, J. Medical applications of cold atmospheric plasma: State of the science. J. Wound. Care 2018, 27 (Suppl. S9), S4–S10. [Google Scholar] [CrossRef]
- Hoffmann, C.; Berganza, C.; Zhang, J. Cold Atmospheric Plasma: Methods of production and application in dentistry and oncology. Med. Gas Res. 2013, 3, 21. [Google Scholar] [CrossRef]
- Ikeda, J.; Tanaka, H.; Ishikawa, K.; Sakakita, H.; Ikehara, Y.; Hori, M. Plasma-activated medium (PAM) kills human cancer-initiating cells. Pathol. Int. 2018, 68, 23–30. [Google Scholar] [CrossRef]
- Yan, D.; Sherman, J.H.; Keidar, M. The Application of the Cold Atmospheric Plasma-Activated Solutions in Cancer Treatment. Anticancer Agents Med. Chem. 2018, 18, 769–775. [Google Scholar] [CrossRef]
- Ishaq, M.; Kumar, S.; Varinli, H.; Han, Z.J.; Rider, A.E.; Evans, M.D.M.; Murphy, A.B.; Ostrikov, K. Atmospheric gas plasma-induced ROS production activates TNF-ASK1 pathway for the induction of melanoma cancer cell apoptosis. Mol. Biol. Cell 2014, 25, 1523–1531. [Google Scholar] [CrossRef]
- Mihai, C.-T.; Mihaila, I.; Pasare, M.A.; Pintilie, R.M.; Ciorpac, M.; Topala, I. Cold Atmospheric Plasma-Activated Media Improve Paclitaxel Efficacy on Breast Cancer Cells in a Combined Treatment Model. Curr. Issues Mol. Biol. 2022, 44, 1995–2014. [Google Scholar] [CrossRef]
- Almeida-Ferreira, C.; Silva-Teixeira, R.; Gonçalves, A.C.; Marto, C.M.; Sarmento-Ribeiro, A.B.; Caramelo, F.; Botelho, M.F.; Laranjo, M. Cold Atmospheric Plasma Apoptotic and Oxidative Effects on MCF7 and HCC1806 Human Breast Cancer Cells. Int. J. Mol. Sci. 2022, 23, 1698. [Google Scholar] [CrossRef]
- Wang, M.; Holmes, B.; Cheng, X.; Zhu, W.; Keidar, M.; Zhang, L.G. Cold Atmospheric Plasma for Selectively Ablating Metastatic Breast Cancer Cells. PLoS ONE 2013, 8, e73741. [Google Scholar] [CrossRef]
- Silva-Teixeira, R.; Laranjo, M.; Lopes, B.; Almeida-Ferreira, C.; Gonçalves, A.C.; Rodrigues, T.; Matafome, P.; Sarmento-Ribeiro, A.B.; Caramelo, F.; Botelho, M.F. Plasma activated media and direct exposition can selectively ablate retinoblastoma cells. Free Radic. Biol. Med. 2021, 171, 302–313. [Google Scholar] [CrossRef]
- Guerrero-Preston, R.; Ogawa, T.; Uemura, M.; Shumulinsky, G.; Valle, B.L.; Pirini, F.; Ravi, R.; Sidransky, D.; Keidar, M.; Trink, B. Cold atmospheric plasma treatment selectively targets head and neck squamous cell carcinoma cells. Int. J. Mol. Med. 2014, 34, 941–946. [Google Scholar] [CrossRef]
- Keidar, M.; Shashurin, A.; Volotskova, O.; Ann Stepp, M.; Srinivasan, P.; Sandler, A.; Trink, B. Cold atmospheric plasma in cancer therapy. Phys. Plasmas 2013, 20, 057101. [Google Scholar] [CrossRef]
- Schneider, C.; Gebhardt, L.; Arndt, S.; Karrer, S.; Zimmermann, J.L.; Fischer, M.J.M.; Bosserhoff, A.-K. Cold atmospheric plasma causes a calcium influx in melanoma cells triggering CAP-induced senescence. Sci. Rep. 2018, 8, 10048. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Schneider, K.; Schwarz, M.; Burkholder, I.; Kopp-Schneider, A.; Edler, L.; Kinsner-Ovaskainen, A.; Hartung, T.; Hoffmann, S. “ToxRTool”, a new tool to assess the reliability of toxicological data. Toxicol. Lett. 2009, 189, 138–144. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Adachi, Y.; Yoshimura, M.; Nishida, K.; Usuki, H.; Shibata, K.; Hattori, M.; Kondo, N.; Yatabe, Y.; Iwata, H.; Kikumori, T.; et al. Acute phase dynamics of circulating tumor cells after paclitaxel and doxorubicin chemotherapy in breast cancer mouse models. Breast Cancer Res. Treat. 2018, 167, 439–450. [Google Scholar] [CrossRef]
- Arun, R.; Dhivya, S.; Abraham, S.K.; Premkumar, K. Low-dose chemotherapeutic drugs induce reactive oxygen species and initiate apoptosis-mediated genomic instability. Toxicol. Res. 2016, 5, 547–556. [Google Scholar] [CrossRef]
- Bernhardt, G.; Reile, H.; Birnbiick, H.; Sprufl, T.; Schiinenberger, H. Standardized kinetic microassay to quantify differential chemosensitivity on the basis of proliferative activity. J. Cancer Res. Clin. Oncol. 1992, 118, 35–43. [Google Scholar] [CrossRef]
- Blois, J.; Smith, A.; Josephson, L. The slow cell death response when screening chemotherapeutic agents. Cancer Chemother. Pharmacol. 2011, 68, 795–803. [Google Scholar] [CrossRef]
- Chen, Z.; Lin, L.; Zheng, Q.; Sherman, J.H.; Canady, J.; Trink, B.; Keidar, M. Micro-Sized Cold Atmospheric Plasma Source for Brain and Breast Cancer Treatment. Plasma Med. 2018, 8, 203–215. [Google Scholar] [CrossRef]
- Chen, Z.; Cheng, X.; Lin, L.; Keidar, M. Cold atmospheric plasma discharged in water and its potential use in cancer therapy. J. Phys. D Appl. Phys. 2017, 50, 015208. [Google Scholar] [CrossRef]
- Chen, Z.; Zhang, S.; Levchenko, I.; Beilis, I.I.; Keidar, M. In vitro Demonstration of Cancer Inhibiting Properties from Stratified Self-Organized Plasma-Liquid Interface. Sci. Rep. 2017, 7, 12163. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Murthy, S.R.K.; Zhuang, T.; Ly, L.; Jones, O.; Basadonna, G.; Keidar, M.; Kanaan, Y.; Canady, J. Canady helios cold plasma induces breast cancer cell death by oxidation of histone mRNA. Int. J. Mol. Sci. 2021, 22, 9578. [Google Scholar] [CrossRef]
- Chuang, H.C.; Kapuriya, N.; Kulp, S.K.; Chen, C.S.; Shapiro, C.L. Differential anti-proliferative activities of poly(ADP-ribose) polymerase (PARP) inhibitors in triple-negative breast cancer cells. Breast Cancer Res. Treat. 2012, 134, 649–659. [Google Scholar] [CrossRef]
- Di, X.; Shiu, R.P.; Newsham, I.F.; Gewirtz, D.A. Apoptosis, autophagy, accelerated senescence and reactive oxygen in the response of human breast tumor cells to Adriamycin. Biochem. Pharmacol. 2009, 77, 1139–1150. [Google Scholar] [CrossRef]
- Frankfurt, O.S.; Krishan, A. Apoptosis-based drug screening and detection of selective toxicity to cancer cells. Anti-Cancer Drugs 2003, 14, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Halfter, K.; Hoffmann, O.; Ditsch, N.; Ahne, M.; Arnold, F.; Paepke, S.; Grab, D.; Bauerfeind, I.; Mayer, B. Testing chemotherapy efficacy in HER2 negative breast cancer using patient-derived spheroids. J. Transl. Med. 2016, 14, 112. [Google Scholar] [CrossRef]
- Hassan, S.; Esch, A.; Liby, T.; Gray, J.W.; Heiser, L.M. Pathway-enriched gene signature associated with 53BP1 response to PARP inhibition in triple-negative breast cancer. Mol. Cancer Ther. 2017, 16, 2892–2901. [Google Scholar] [CrossRef]
- Hernández-Vargas, H.; Palacios, J.; Moreno-Bueno, G. Molecular profiling of docetaxel cytotoxicity in breast cancer cells: Uncoupling of aberrant mitosis and apoptosis. Oncogene 2007, 26, 2902–2913. [Google Scholar] [CrossRef]
- Izbicka, E.; Campos, D.; Carrizales, G.; Tolcher, A. Biomarkers for sensitivity to docetaxel and paclitaxel in human tumor cell lines in vitro. Cancer Genom. Proteom. 2005, 2, 219–226. [Google Scholar]
- Jezeh, M.A.; Tayebi, T.; Khani, M.R.; Niknejad, H.; Shokri, B. Direct cold atmospheric plasma and plasma-activated medium effects on breast and cervix cancer cells. Plasma Process. Polym. 2020, 17, 1900241. [Google Scholar] [CrossRef]
- Keung, M.Y.; Wu, Y.; Badar, F.; Vadgama, J.V. Response of breast cancer cells to PARP inhibitors is independent of BRCA status. J. Clin. Med. 2020, 9, 940. [Google Scholar] [CrossRef] [PubMed]
- Kibria, G.; Hatakeyama, H.; Akiyama, K.; Hida, K.; Harashima, H. Comparative Study of the Sensitivities of Cancer Cells to Doxorubicin, and Relationships between the Effect of the Drug-Efflux Pump P-gp. Biol. Pharm. Bull. 2014, 37, 1926–1935. [Google Scholar] [CrossRef]
- Kim, R.; Tanabe, K.; Emi, M.; Uchida, Y.; Toge, T. Death receptor-dependent and -independent pathways in anticancer drug-induced apoptosis of breast cancer cells. Oncol. Rep. 2003, 10, 1925–1930. [Google Scholar] [CrossRef]
- Koechli, O.R.; Sevin, B.-U.; Perras, J.R.; Chao Chou, T.; Angioli, R.; Steren, A.; Untch, M.; Averette, H.E. Characteristics of the combination paclitaxel plus doxorubicin in breast cancer cell lines analyzed with the ATP-Cell Viability Assay. Breast Cancer Res. Treat. 1993, 28, 21–27. [Google Scholar] [CrossRef]
- Koechli, O.R.; Sevin, B.-U.; Perras, J.P.; Angioli, R.; Untch, M.; Steren, A.; Ramachandran, C.; Averette, H.E. Comparative chemosensitivity profiles in three human breast cancer cell lines with the ATP-cell viability assay. Oncology 1994, 51, 552–558. [Google Scholar] [CrossRef]
- Konecny, G.; Untch, M.; Slamon, D.; Beryt, M.; Kahlert, S.; Felber, M.; Langer, E.; Lude, S.; Hepp, H.; Pegram, M. Drug interactions and cytotoxic effects of paclitaxel in combination with carboplatin, epirubicin, gemcitabine or vinorelbine in breast cancer cell lines and tumor samples. Breast Cancer Res. Treat. 2001, 67, 223–233. [Google Scholar] [CrossRef]
- Lafontaine, J.; Boisvert, J.-S.; Glory, A.; Coulombe, S.; Wong, P. Synergy between non-thermal plasma with radiation therapy and olaparib in a panel of breast cancer cell lines. Cancers 2020, 12, 348. [Google Scholar] [CrossRef]
- Liu, Y.; Tan, S.; Zhang, H.; Kong, X.; Ding, L.; Shen, J.; Lan, Y.; Cheng, C.; Zhu, T.; Xia, W. Selective effects of non-thermal atmospheric plasma on triple-negative breast normal and carcinoma cells through different cell signaling pathways. Sci. Rep. 2017, 7, 7980. [Google Scholar] [CrossRef]
- Ly, L.; Cheng, X.; Murthy, S.R.K.; Zhuang, T.; Jones, O.Z.; Basadonna, G.; Keidar, M.; Canady, J. Canady cold plasma conversion system treatment: An effective inhibitor of cell viability in breast cancer molecular subtypes. Clin. Plasma Med. 2020, 19–20, 100109. [Google Scholar] [CrossRef]
- Ma, J.; Zhang, Q.; Huang, Y.; Xu, Z. Study on inhibitory effect of paclitaxel on MEK and ERK protein overexpression and activation in different breast cancer cell lines. Int. J. Clin. Exp. Med. 2017, 10, 2986–2991. [Google Scholar]
- Ma, J.; Yu, K.N.; Zhang, H.; Nie, L.; Cheng, C.; Cui, S.; Chen, G.; Han, W. Non-Thermal Plasma Induces Apoptosis Accompanied by Protective Autophagy via Activating JNK/Sestrin2 Pathway. J. Phys. D Appl. Phys. 2020, 53, 465201. [Google Scholar] [CrossRef]
- Man, S.; Bocci, G.; Francia, G.; Green, S.; Jothy, S.; Hanahan, D.; Bohlen, P.; Hicklin, D.J.; Bergers, G.; Kerbel, R.S. Antitumor effects in mice of low-dose (metronomic) cyclophosphamide administered continuously through the drinking water. Cancer Res. 2002, 62, 2731–2735. [Google Scholar] [PubMed]
- Mccloskey, D.E.; Kaufmann, S.H.; Prestigiacomo, L.J.; Davidson, N.E. Paclitaxel Induces Programmed Cell Death in MDAMB-468 Human Breast Cancer Cells. Clin. Cancer Res. 1996, 2, 847–854. [Google Scholar] [PubMed]
- Merrill, N.M.; Lachacz, E.J.; Vandecan, N.M.; Ulintz, P.J.; Bao, L.; Lloyd, J.P.; Yates, J.A.; Morikawa, A.; Merajver, S.D.; Soellner, M.B. Molecular determinants of drug response in TNBC cell lines. Breast Cancer Res. Treat. 2020, 179, 337–347. [Google Scholar] [CrossRef]
- Morse, D.L.; Gray, H.; Payne, C.M.; Gillies, R.J. Docetaxel induces cell death through mitotic catastrophe in human breast cancer cells. Mol. Cancer Ther. 2005, 4, 1495–1504. [Google Scholar] [CrossRef]
- Moschetta-Pinheiro, M.G.; Colombo, J.; Tuckumantel, M.S.; Rebolho, G.K.; Zuccari, D.A.P.C. Treatment of Triple Negative Cell Lines with Olaparib to Block DNA Repair. Anticancer Agents Med. Chem. 2022, 22, 2036–2045. [Google Scholar] [CrossRef]
- Muñoz, R.; Hileeto, D.; Cruz-Muñoz, W.; Wood, G.A.; Xu, P.; Man, S.; Viloria-Petit, A.; Kerbel, R.S. Suppressive impact of metronomic chemotherapy using UFT and/or cyclophosphamide on mediators of breast cancer dissemination and invasion. PLoS ONE 2019, 14, e0222580. [Google Scholar] [CrossRef]
- Ninomiya, K.; Ishijima, T.; Imamura, M.; Yamahara, T.; Enomoto, H.; Takahashi, K.; Tanaka, Y.; Uesugi, Y.; Shimizu, N. Evaluation of extra- and intracellular OH radical generation, cancer cell injury, and apoptosis induced by a non-thermal atmospheric-pressure plasma jet. J. Phys. D Appl. Phys. 2013, 46, 425401. [Google Scholar] [CrossRef]
- Norris, R.E.; Adamson, P.C.; Nguyen, V.T.; Fox, E. Preclinical evaluation of the PARP inhibitor, olaparib, in combination with cytotoxic chemotherapy in pediatric solid tumors. Pediatr. Blood Cancer 2014, 61, 145–150. [Google Scholar] [CrossRef]
- Oncul, S.; Ercan, A. Discrimination of the Effects of Doxorubicin on Two Different Breast Cancer Cell Lines on Account of Multidrug Resistance and Apoptosis. Indian J. Pharm. Sci. 2017, 79, 599–607. [Google Scholar] [CrossRef]
- Park, S.B.; Kim, B.; Bae, H.; Lee, H.; Lee, S.; Choi, E.H.; Kim, S.J. Differential epigenetic effects of atmospheric cold plasma on MCF-7 and MDA-MB-231 breast cancer cells. PLoS ONE 2015, 10, e0129931. [Google Scholar] [CrossRef] [PubMed]
- Parrella, A.; Lavorgna, M.; Criscuolo, E.; Russo, C.; Isidori, M. Estrogenic activity and cytotoxicity of six anticancer drugs detected in water systems. Sci. Total Environ. 2014, 485–486, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Pilco-Ferreto, N.; Calaf, G.M. Influence of doxorubicin on apoptosis and oxidative stress in breast cancer cell lines. Int. J. Oncol. 2016, 49, 753–762. [Google Scholar] [CrossRef]
- Risinger, A.L.; Dybdal-Hargreaves, N.F.; Mooberry, S.L. Breast cancer cell lines exhibit differential sensitivities to microtubule-targeting drugs independent of doubling time. Anticancer Res. 2015, 35, 5845–5850. [Google Scholar] [PubMed]
- Sauter, C.; Cogoli, M.; Arrenbrecht, S. Interactions of Cytotoxic and Other Drugs: Rapid Cell Culture Assay. Oncology 1986, 43, 46–49. [Google Scholar] [CrossRef]
- Shaked, Y.; Pham, E.; Hariharan, S.; Magidey, K.; Beyar-Katz, O.; Xu, P.; Man, S.; Wu, F.T.H.; Miller, V.; Andrews, D.; et al. Evidence implicating immunological host effects in the efficacy of metronomic low-dose chemotherapy. Cancer Res. 2016, 76, 5983–5993. [Google Scholar] [CrossRef]
- Stope, M.B.; Benouahi, R.; Sander, C.; Haralambiev, L.; Nitsch, A.; Egger, E.; Mustea, A. Protherapeutic effects and inactivation of mammary carcinoma cells by a medical argon plasma device. Anticancer Res. 2020, 40, 6205–6212. [Google Scholar] [CrossRef]
- Subramanian, P.S.G.; Jain, A.; Shivapuji, A.M.; Sundaresan, N.R.; Dasappa, S.; Rao, L. Plasma-activated water from a dielectric barrier discharge plasma source for the selective treatment of cancer cells. Plasma Process. Polym. 2020, 17, 1900260. [Google Scholar] [CrossRef]
- Taherian, A.; Mazoochi, T. Different expression of extracellular signal-regulated kinases (ERK) 1/2 and phospho-Erk proteins in MBA-MB-231 and MCF-7 cells after chemotherapy with doxorubicin or docetaxel. Iran. J. Basic Med. Sci. 2012, 15, 669–677. [Google Scholar] [PubMed]
- Tassone, P.; Tagliaferri, P.; Perricelli, A.; Blotta, S.; Quaresima, B.; Martelli, M.L.; Goel, A.; Barbieri, V.; Costanzo, F.; Boland, C.R.; et al. BRCA1 expression modulates chemosensitivity of BRCA1-defective HCC1937 human breast cancer cells. Br. J. Cancer 2003, 88, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Terefinko, D.; Dzimitrowicz, A.; Bielawska-Pohl, A.; Klimczak, A.; Pohl, P.; Jamroz, P. The influence of cold atmospheric pressure plasma-treated media on the cell viability, motility, and induction of apoptosis in human non-metastatic (Mcf7) and metastatic (mda-mb-231) breast cancer cell lines. Int. J. Mol. Sci. 2021, 22, 3855. [Google Scholar] [CrossRef]
- Wali, V.B.; Langdon, C.G.; Held, M.A.; Platt, J.T.; Patwardhan, G.A.; Safonov, A.; Aktas, B.; Pusztai, L.; Stern, D.F.; Hatzis, C. Systematic drug screening identifies tractable targeted combination therapies in triple-negative breast cancer. Cancer Res. 2017, 77, 566–578. [Google Scholar] [CrossRef]
- Wang, P.; Zhou, R.; Thomas, P.; Zhao, L.; Zhou, R.; Mandal, S.; Jolly, M.K.; Richard, D.J.; Rehm, B.H.A.; Ostrikov, K.; et al. Epithelial-to-mesenchymal transition enhances cancer cell sensitivity to cytotoxic effects of zcold atmospheric plasmas in breast and bladder cancer systems. Cancers 2021, 13, 2889. [Google Scholar] [CrossRef]
- Węsierska-Gądek, J.; Mauritz, M.; Mitulovic, G.; Cupo, M. Differential Potential of Pharmacological PARP Inhibitors for Inhibiting Cell Proliferation and Inducing Apoptosis in Human Breast Cancer Cells. J. Cell Biochem. 2015, 116, 2824–2839. [Google Scholar] [CrossRef]
- Xiang, L.; Xu, X.; Zhang, S.; Cai, D.; Dai, X. Cold atmospheric plasma conveys selectivity on triple negative breast cancer cells both in vitro and in vivo. Free Radic. Biol. Med. 2018, 124, 205–213. [Google Scholar] [CrossRef]
- Yan, D.; Talbot, A.; Nourmohammadi, N.; Cheng, X.; Canady, J.; Sherman, J.; Keidar, M. Principles of using Cold Atmospheric Plasma Stimulated Media for Cancer Treatment. Sci. Rep. 2015, 5, 18339. [Google Scholar] [CrossRef]
- Yan, D.; Cui, H.; Zhu, W.; Nourmohammadi, N.; Milberg, J.; Zhang, L.G.; Sherman, J.H.; Keidar, M. The Specific Vulnerabilities of Cancer Cells to the Cold Atmospheric Plasma-Stimulated Solutions. Sci. Rep. 2017, 7, 4479. [Google Scholar] [CrossRef] [PubMed]
- Yaourtis, A.M.; Levina, A.; Lay, P.A. Tumour cell heterogeneity in triple-negative breast cancer cells affects response to cisplatin, but not doxorubicin. J. Inorg. Biochem. 2023, 239, 112082. [Google Scholar] [CrossRef] [PubMed]
- Zasadil, L.M.; Andersen, K.A.; Yeum, D.; Rocque, G.B.; Wilke, L.G.; Tevaarwerk, A.J.; Raines, R.T.; Burkard, M.E.; Weaver, B.A. Cytotoxicity of Paclitaxel in Breast Cancer Is due to Chromosome Missegregation on Multipolar Spindles. Sci. Transl. Med. 2014, 6, 229ra43. [Google Scholar] [CrossRef]
- Zhou, X.; Cai, D.; Xiao, S.; Ning, M.; Zhou, R.; Zhang, S.; Chen, X.; Ostrikov, K.; Dai, X. Invivopen: A novel plasma source for in vivo cancer treatment. J. Cancer 2020, 11, 2273–2282. [Google Scholar] [CrossRef] [PubMed]
- Bosch, A.; Eroles, P.; Zaragoza, R.; Viña, J.R.; Lluch, A. Triple-negative breast cancer: Molecular features, pathogenesis, treatment and current lines of research. Cancer Treat. Rev. 2010, 36, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Gregório, A.C.; Lacerda, M.; Figueiredo, P.; Simões, S.; Dias, S.; Moreira, J.N. Therapeutic Implications of the Molecular and Immune Landscape of Triple-Negative Breast Cancer. Pathol. Oncol. Res. 2017, 24, 701–716. [Google Scholar] [CrossRef]
- Parsons, H.A.; Beaver, J.A.; Cimino-Mathews, A.; Ali, S.M.; Axilbund, J.; Chu, D.; Connolly, R.M.; Cochran, R.L.; Croessmann, S.; Clark, T.A.; et al. Individualized Molecular Analyses Guide Efforts (IMAGE): A prospective study of molecular profiling of tissue and blood in metastatic triple-negative breast cancer. Clin. Cancer Res. 2017, 23, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Braný, D.; Dvorská, D.; Halašová, E.; Škovierová, H. Molecular Sciences Cold Atmospheric Plasma: A Powerful Tool for Modern Medicine. Int. J. Mol. Sci. 2020, 21, 2932. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hou, H.; Zhang, P.; Zhang, Z. Co-delivery of doxorubicin and paclitaxel by reduction/pH dual responsive nanocarriers for osteosarcoma therapy. Drug Deliv. 2020, 27, 1044–1053. [Google Scholar] [CrossRef]
- Li, H.; Xu, W.; Li, F.; Zeng, R.; Zhang, X.; Wang, X.; Zhao, S.; Weng, J.; Li, Z.; Sun, L. Amplification of anticancer efficacy by co-delivery of doxorubicin and lonidamine with extracellular vesicles. Drug Deliv. 2022, 29, 192–202. [Google Scholar] [CrossRef]
- Pazdur, R.; Kudelka, A.P.; Kavanagh, J.J.; Cohen, P.R.; Raber, M.N. The taxoids: Paclitaxel (Taxol®) and docetaxel (Taxotere®). Cancer Treat. Rev. 1993, 19, 351–386. [Google Scholar] [CrossRef]
- Goulooze, S.C.; Cohen, A.F.; Rissmann, R. Olaparib. Br. J. Clin. Pharmacol. 2016, 81, 171–173. [Google Scholar] [CrossRef]
- de Sousa, G.F.; Wlodarczyk, S.R.; Monteiro, G. Carboplatin: Molecular mechanisms of action associated with chemoresistance. Braz. J. Pharm. Sci. 2014, 50, 693–701. [Google Scholar] [CrossRef]
- Mills, K.A.; Chess-Williams, R.; McDermott, C. Novel insights into the mechanism of cyclophosphamide-induced bladder toxicity: Chloroacetaldehyde’s contribution to urothelial dysfunction in vitro. Arch. Toxicol. 2019, 93, 3291–3303. [Google Scholar] [CrossRef]
- Walko, C.M.; Lindley, C. Capecitabine: A review. Clin. Ther. 2005, 27, 23–44. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Xiong, Z.; Zou, F.; Zhao, S.; Lu, X.; Yang, G.; He, G.; Ostrikov, K.K. Plasma-Induced Death of HepG2 Cancer Cells: Intracellular Effects of Reactive Species. In Plasma Processes and Polymers; Wiley: New York, NY, USA, 2012; Volume 9, pp. 59–66. [Google Scholar]
- Kumara, M.H.S.R.; Piao, M.J.; Kang, K.A.; Ryu, Y.S.; Park, J.E.; Shilnikova, K.; Jo, J.O.; Mok, Y.S.; Shin, J.H.; Park, Y.; et al. Non-thermal gas plasma-induced endoplasmic reticulum stress mediates apoptosis in human colon cancer cells. Oncol. Rep. 2016, 36, 2268–2274. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, N.; Nakamura, K.; Kajiyama, H. Current understanding of plasma-activated solutions for potential cancer therapy. Free Radic. Res. 2023, 57, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.J.; Kim, K.I.; Hoan, N.N.; Kim, C.H.; Moon, E.; Choi, K.S.; Yang, S.S.; Lee, J.S. Targeting cancer cells with reactive oxygen and nitrogen species generated by atmospheric-pressure air plasma. PLoS ONE 2014, 9, e86173. [Google Scholar] [CrossRef]
- Almeida-Ferreira, C.; Silva-Teixeira, R.; Laranjo, M.; Almeida, N.; Brites, G.; Dias-Ferreira, J.; Marques, I.; Neves, R.; Serambeque, B.; Teixo, R.; et al. Open-Air Cold Plasma Device Leads to Selective Tumor Cell Cytotoxicity. Appl. Sci. 2021, 11, 4171. [Google Scholar] [CrossRef]
- Tavares-da-Silva, E.; Pereira, E.; Pires, A.S.; Neves, A.R.; Braz-Guilherme, C.; Marques, I.A.; Abrantes, A.M.; Gonçalves, A.C.; Caramelo, F.; Silva-Teixeira, R.; et al. Cold Atmospheric Plasma, a Novel Approach against Bladder Cancer, with Higher Sensitivity for the High-Grade Cell Line. Biology 2021, 10, 41. [Google Scholar] [CrossRef]
- Hamouda, I.; Labay, C.; Cvelbar, U.; Ginebra, M.-P.; Canal, C. Selectivity of direct plasma treatment and plasma-conditioned media in bone cancer cell lines. Sci. Rep. 2021, 11, 17521. [Google Scholar] [CrossRef] [PubMed]
- Canal, C.; Fontelo, R.; Hamouda, I.; Guillem-Marti, J.; Cvelbar, U.; Ginebra, M.-P. Plasma-induced selectivity in bone cancer cells death. Free Radic. Biol. Med. 2017, 110, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Vaquero, J.; Judée, F.; Vallette, M.; Decauchy, H.; Arbelaiz, A.; Aoudjehane, L.; Scatton, O.; Gonzalez-Sanchez, E.; Merabtene, F.; Augustin, J.; et al. Cold-atmospheric plasma induces tumor cell death in preclinical in vivo and in vitro models of human cholangiocarcinoma. Cancers 2020, 12, 1280. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.M.; Yoon, H.K.; Kim, S.Y.; Yun, M.R.; Kim, G.H.; Lee, W.J.; Lee, M.W.; Chang, S.E.; Won, C.H. Anticancer Effect of Cold Atmospheric Plasma in Syngeneic Mouse Models of Melanoma and Colon Cancer. Molecules 2023, 28, 4171. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Description |
|---|---|
| Population (P) | Triple-negative breast cancer cell lines and animal models |
| Intervention (I) | Cold atmospheric plasma |
| Comparison (C) | Doxorubicin or epirubicin or cyclophosphamide or paclitaxel or docetaxel or carboplatin or capecitabine or olaparib |
| Outcome (O) | In vitro studies: cell viability/proliferation In vivo studies: tumor volume and histopathological changes |
| Author (Year) | Type of Study | Experimental Model | Treatment Characteristics | Methods | Main Results |
|---|---|---|---|---|---|
| Adachi et al. (2018) [29] | In vitro | MDA-MB-231 | PTX (1, 10, 100 nM, and 1 µM) Incubation: 48 h PTX (100 nM) or DOX (10 µg/mL) for FC Incubation: 24 h | Viable cells counted with a hemocytometer; Annexin V/PI (FC) | The growth of cells in vitro was significantly inhibited by increasing doses of PTX (p < 0.01). Cells treated with PTX (100 nM) for 24 h showed a slight increase in early apoptotic cells. DOX markedly inhibited cells in a dose-dependent manner (p < 0.01). Apoptosis analysis confirmed an apparent increase in early plus late apoptotic cells 24 h after DOX3 treatment. |
| Almeida-Ferreira et al. (2022) [20] | In vitro | HCC1806 | CAP. Plasma device: 4 kV, pulses of 1 kHz through a sterilized needle 0.9 mm in radius and 40 mm in length Exposure time: 60 and 120 s Incubation: 24 h | Annexin V/PI (FC) | The proportion of viable cells significantly decreased from 80.50 ± 1.59% to 64.67 ± 2.16% (p = 0.0008) after 60 s of exposure and to 65.00 ± 3.39% (p = 0.01) after 120 s. |
| Arun et al. (2016) [30] | In vitro | MDA-MB-231 | DOX (1, 2, 3, 4, 5, and 6 µM) Incubation: 12 and 24 h | MTT assay | DOX (1 μM) resulted in 90% of cell viability, and DOX (6 μM) resulted in 80% at 12 h. Cell viability was 65% after 24 h when low doses were used. |
| Bernhardt et al. (1992) [31] | In vitro | MDA-MB-231 | DOX (1 µM) Incubation: 0–333 h | Crystal violet assay | The drug was cytotoxic (data were not shown). |
| Blois et al. (2011) [32] | In vitro | MDA-MB-231 | PTX (100 mM) Incubation: 48 h | SRB assay | IC50 (nM): 0.07 |
| Chen et al. (2018) [33] | In vitro | MDA-MB-231 | CAP. Plasma device: 8 kV, 16 kHz. He gas was injected into the quartz tube with a 0.2 L/min flow rate. Micro-sized CAP with stainless-steel tubes 20 mm and 60 mm in length. Exposure time: 5, 10, 30, 60, and 120 s Incubation: 24 and 48 h | MTT assay | The cell viability dropped with increasing treatment time for both 20 mm and 60 mm µCAP treatment. For each exposure time, the cell viability of breast cancer cells was lower for the 20 mm CAP length than for the 60 mm CAP length. |
| Chen et al. (2017) [34] | In vitro | MDA-MB-231 | PAM. Plasma device: immersed in DI water. The electrodes were connected to a secondary high-voltage transformer (2–5 kV, 30 kHz). Ar, He, and N2 were used, and the flow rate was maintained at about 0.3 min−1. Exposure gas: Ar, He, and N2 Solutions: DI water and DMEM Incubation: 24 and 48 h | MTT assay | After 24 h, cell viability decreased by approximately 27.4% and 14.7% when treated with Ar and He plasma, respectively. Only a slight decrease in cell viability was observed in the case of DI water and N2 plasma solution. After 48 h, viability decreased approximately 73.1%, 22.8%, 14.1%, and 13.5% when cells were treated with Ar plasma solution, He plasma solution, N2 plasma solution, and DI water, respectively. Thus, the most potent effect was observed in the case of Ar plasma, while the smallest was in N2 plasma. |
| Chen et al. (2017) [35] | In vitro | MDA-MB-231 | PAM. Plasma device: 1–3012 V, 40 mA activated with low or high current Solutions: DI water and DMEM Exposure time: 12, 24, 36, 48, and 60 s Incubation: 24 and 48 h | MTT assay | The viability of cells incubated in low-current PAM was generally lower than that of cells incubated in high = current PAM. This was observed both after 24 h (36 s, p > 0.05; 48 s, p < 0.05; 60 s, p < 0.001) and 48 h (36 s, p < 0.01; 48 s, p > 0.05; 60 s, p < 0.05). The cell viability of cells incubated for 48 h at low current steadily decreased with treatment duration, while the cell viability at high current initially decreased and then increased slightly. |
| Cheng et al. (2021) [36] | In vitro | MDA-MB-231 | CAP. Plasma device: Canady Helios Cold Plasma™. He flow rate at 3 L/min; 4 kV, 300 kHz, and 40 W Power settings: 80P (15.7 W), 100P (22.3 W) and 120P (28.7 W) Exposure time: 3, 5, and 6 min Incubation: 6, 24, and 48 h | Annexin V/PI (FC) | Exposure for 3, 5, or 6 min at 80P or 120P reduced the live cells after 24 and 48 h of incubation. |
| Chuang et al. (2012) [37] | In vitro | MDA-MB-231, MDA-MB-468, CAL51 | Olaparib (20, 40, 60, 80, or 100 µM) Incubation: 72 h | MTT assay; Clonogenic assay (14–21 days) | IC50 (µM) by MTT MDA-MB-231: >100; MDA-MB-468: 18; CAL51: 9.5 IC50 (µM) by clonogenic assay MDA-MB-231: 4.5; MDA-MB-468: 0.2; CAL51: 0.4 |
| Di et al. (2009) [38] | In vitro | MDA-MB-231 | DOX | Clonogenic assay (14 days) | The mean number of colonies was 2.7 ± 0.9% compared to the control. |
| Frankfurt & Krishan (2003) [39] | In vitro | MDA-MB-468 | DOX or PTX Incubation: 48 h | MTT assay SRB assay | IC50 (µM) by MTT and SRB assays, respectively. DOX: 0.05; 0.1 PTX: 0.01; 0.01 |
| Halfter et al. (2016) [40] | In vitro | HCC1143 and HCC1937 spheroids | Single or combined regimens of CAR, CCP, DOC, EPI, and PTX Incubation: 96 h | ATP assay | Metabolic activity (HCC1143 and HCC1937, respectively) CAR: 104.71 ± 26.68; 80.95 ± 0.67 DOC: 121.36 ± 45.60; 101.38 ± 2.69 PTX: 81.97 ± 42.22; 93.37 ± 1.71 EPI and CCP: 86.07 ± 24.99; 85.12 ± 5.26 EPI and CCP and DOC: 117.00 ± 23.75; 87.57 ± 5.03 EPI and CCP and PTX: 91.59 ± 33.35; 83.74 ± 10.44 DOC and DOX and CCP: 97.56 ± 6.57; 75.06 ± 2.80 |
| Hassan et al. (2017) [41] | In vitro | MDA-MB-436, MDA-MB-231, MDA-MB-453, MDA-MB-468, HCC1143, HCC1937, HCC1806, HCC1395 | Olaparib (0.25 nmol/L to 100 mmol/L) Incubation: 9 days, drugs plus media changed after 4–5 days | Chemosensitivity assay | IC50 differed in all cell lines, ranging from 0.003 to 3.8 mmol/L. |
| Hernández-Vargas et al. (2007) [42] | In vitro | MDA-MB-231 | DOC (from 0 to 500 nM) Incubation: 24–96 h | Crystal violet assay; Annexin-V-FITC Apoptosis detection kit (FC) | Cells were sensitive to nM concentrations of DOC. There was a growth inhibition at concentrations lower than 10 nM. IC75 (nM): 2 nM |
| Izbicka et al. (2005) [43] | In vitro | MDA-MB-231 | DOC (0.1, 0.5, or 5 nM) or PTX (0.1, 1, or 5 nM) Incubation: 72 and 120 h | MTS assay | IC50 (pM) DOC: 499 (72 h); 35 (120 h) PTX: 933 (72 h) PTX toxicity at day five increased about twofold in comparison with day three. |
| Jezeh et al. (2020) [44] | In vitro | MDA-MB-231 | CAP or PAM. Plasma device: 20–70 kHz and 5 kV. Gas flow: He or He + 0.5% O2 Exposure time: 1, 2, 3, 4, and 5 min Incubation: 48 h PAM: 200 µL of medium | MTT assay | CAP: Cell viability was reduced in almost all CAP exposure. Generally, better results were obtained using He + 0.5% O2 than pure gas. The viability of MDA-MB-231 cells decreased by more than 60% after 5 min of treatment. PAM: Similar results were observed despite no significant differences between He + 0.5% O2 and He. Cell viability decreased to about 50% after 5 min. |
| Keung et al. (2020) [45] | In vitro | MDA-MB-231, MDA-MB-436, MDA-MB-468, HCC1143, HCC1937, BT-549, HCC70, HCC1806 | Olaparib (from 0.001 to 200 μM) Incubation: 7 days | MTT assay | IC50 (µM) MDA-MB-231: 13.5; MDA-MB-436: 4.7; MDA-MB-468: 5.2; HCC1143: 14; HCC1937: 96; BT-549: 81; HCC70: 11; HCC1806: 1.2 |
| Kibria et al. (2014) [46] | In vitro | MDA-MB-231 | DOX (several concentrations) Incubation: 24 h with medium changed after 8 h | WST-8 assay | EC50: 25.72 ± 20.27 μg/mL |
| Kim et al. (2003) [47] | In vitro | MDA-MB-231 | DOX or PTX Incubation: 48 h | MTT assay | IC50 (µM) DOX: 0.3 PTXl: 0.03 |
| Koechli et al. (1993) [48] | In vitro | BT-20 | PTX (0.001; 0.002; 0.005; 0.01 PPCs) or DOX (0.1; 0.2; 0.5; 1.0 PPCs) or PTX and DOX (1:1000) | ATP cell viability assay | IC50 (PPCs): PTX: 0.00163; DOX: 0.319; PTX and DOX: 0.2277. The CI values ranged from 5.4 to 0.9. At a ratio of 1:10 (PPC), the CI values ranged from 0.4 to 0.5, indicating synergism over the whole range. |
| Koechli et al. (1994) [49] | In vitro | BT-20 | DOX or PTX or CCP (0.01, 0.02, 0.05, 0.1, and 0.5 PPC | ATP cell viability assay | IC50 (µM) DOX: 0.32; PTX: 0.007; CCP: 5.53 |
| Konecny et al. (2001) [50] | In vitro | MDA-MB-231 | PTX (0.9, 1.8, 3.6, 7.2, 14.5, 29, 58, 116 nM) and CAR (3.1, 6.2, 12.5, 25, 50, 100, 200, 400 µM) or PTX (0.4, 0.9, 1.8, 3.6, 7.2, 14.5, 29, 58, 116 nM and EPI (1.7, 3.3, 6.7, 13.4, 26.8, 53.7, 107, 215, 430 nM) | Crystal violet assay | CAR doses (<10 μM) showed additive interactions in combination with PTX. However, EPI and PTX demonstrated an antagonistic effect. |
| Lafontaine et al. (2020) [51] | In vitro | BT549, Hs578T, MDA-MB-157, MDA-MB-231, MDA-MB-468 | CAP. Plasma device: 10 or 35 W, He and O2 gas flow Exposure time: 10 to 120 s Olaparib Concentration: 2 µM Incubation: 2 h before CAP | Crystal violet assay | CAP: Only 30 s of CAP treatment reached a more intense effect than did other application modes. The efficacy increased with treatment time. Olaparib: Affected cell growth, especially for MDA-MB-468 (more than 60% of inhibition, p < 0.001). CAP + olaparib: The combination improved the cytotoxic effect of CAP in all cell lines. |
| Liu et al. (2017) [52] | In vitro | MDA-MB-231, MDA-MB-453 | CAP. Plasma device: 10 kV and 5 mA Exposure time: 60, 90, and 120 s Incubation: 48 h | Trypan blue | There was significant reduction of cell viability after 60 s in MDA-MB-231, while MDA-MB-453 did not show significant reduction. After 120 s, CAP treatment decreased the viability to <80% MDA-MB-453 and <50% MDA-MB-231. |
| Ly et al. (2020) [53] | In vitro | MDA-MB-231, Hs578T, HCC1806 | CAP. Plasma device: Canady Helios Cold Plasma™ Scalpel, 4 kV, He flow rate at 3 L/min and power set to 80, 100, and 120 P. Exposure time: 1, 2, 3, 4, 5, and 6 min Incubation: 48 h | MTT assay | Increasing power and treatment duration from 80 to 120 P for 1–6 min yielded a greater viability reduction in MDA-MB-231. A 92–99% decrease in cell viability was achievable after 120 P at 5 or 6 min (p ≤ 0.05). HCC1806 showed the greatest overall CAP resistance. |
| Ma et al. (2017) [54] | In vitro | HCC1937, BT-549, HCC38 | PTX | Annexin V/PI (FC) and 7AAD kit (BD559763) | PTX increased the number of apoptotic cells. |
| Ma et al. (2020) [55] | In vitro | MDA-MB-231 | CAP. Plasma device: 12 kV, 24 kHz. Power density: 0.9 W/cm2. Gas flow: He at 120 L/h Exposure time: 30, 60, 90, and 120 s Incubation: 24 h | Cell counting kit-8 kit and Annexin V-FITC/PI (FC) | CAP significantly decreased the cell viability in a dose-dependent manner and induced apoptotic cell death. |
| Man et al. (2002) [56] | In vivo | MDA-MB-231; Female CB-17 SCID mice; Orthotopically implanted into the mammary fat pad | CCP (25 mg/kg of continuous low doses via drinking water; 450 mg/kg/cycle: 150 mg/kg/injection every other day over six days) | Tumor and weight monitoring | Six-day therapy cycles were similar to low-dose administration for tumor size reduction. However, the former was extremely toxic to SCID mice, resulting in severe weight loss and death of mice after the first week. No weight loss or other signs of toxicity were observed in the group of SCID mice treated via drinking water. |
| McCloskey et al. (1996) [57] | In vitro | MDA-MB-468 | PTX Incubation: 3, 24, and 120 h | Trypan blue | Cells exposed for 3 h demonstrated concentration-dependent growth inhibition at ≥10 nM PTX (IC50 = 17 nM). At 24 h, growth inhibition was at 1 nM (IC50 = 2.6 nM). At 120 h, the IC50 was 1.8 nM. |
| Merrill et al. (2019) [58] | In vitro | MUM51, BT-20, BT-549, CAL148, CAL51, DU4475, HCC1806, HCC1937, HCC38, HCC70, Hs578T, MDA-MB-157, MDA-MB-231, MDA-MB-436, MDA-MB-453, MDA-MB-468, MFM223, SUM52, SUM102, SUM149, SUM159, SUM185 | PTX (from 0.6 to 10,000 nM) or DOC (from 0.1 to 1000 nM) Incubation: 72 h | WTS-1 followed by CellTiter-Glo® assay | IC50 (nM) PTX: 110 (MUM51); 159 (BT-20); 110 (BT-549); 4 (CAL148); 310 (CAL51); 19 (DU4475); 77 (HCC1806); 130 (HCC1937); 1700 (HCC38); 3 (HCC70); 150 (Hs578T); 190 (MDA-MB-157); 200 (MDA-MB-231); 110 (MDA-MB-436); 2 (MDA-MB-453); 89 (MDA-MB-468); 4 (MFM223); 9 (SUM102); 13 (SUM149); 2 (SUM159); 10 (SUM185); 3 (SUM52). DOC: 2 (MUM51); 2 (BT20); 1 (BT549); 2 (CAL148); 4 (CAL51); 5 (DU4475); 4 (HCC1806); 1 (HCC1937); 1 (HCC38); 1 (HCC70); 1 (Hs578T); 1 (MDA-MB-157); 2 (MDA-MB-231); 1 (MDA-MB-436); 1 (MDA-MB-453); 1 (MDA-MB-468); 740 (MFM223); 1 (SUM102); 5 (SUM149); 140 (SUM159); 2 (SUM185); 2 (SUM52). |
| Mihai et al. (2022) [19] | In vitro | MDA-MB-231 and MDA-MB-231 spheroids | PAM. Plasma device: 10 kV and 28 kHz Solution: DMEM without FBS (160 µL) Exposure time: 30 and 60 s Incubation: 20 min and medium changed to 10% FBS DMEM PTX (0.1 μM, 0.01 μM, and 0.001 μM) after PAM Incubation: 24 and 48 h | MTT assay; Clonogenic assay; Spheroid area | PTX: Cell viability was reduced to 63.05% and 28.31% (0.1 μM PTX) after 24 and 48 h, respectively. PAM: At 48 h, cell viability reduced to approximately 25%. PTX + PAM: Cell line showed values between 33.77% and 36.28% at 24 h and 18.80% and 19.95% at 48 h. After 15 s of PAM, the total area of spheroids significantly decreased to 23.81% compared to control (p < 0.05) and 20.95% compared to PTX treatment. Cells were susceptible to PAM and combined treatment. PAM could induce a stable cytotoxic effect and improve PTX chemosensitivity. |
| Morse et al. (2005) [59] | In vitro | MDA-MB-231 | DOC (10 nmol/L) (1) Incubation: 48 h (2) Incubation: 24 or 48 h or 48 h followed by 24 h in drug-free medium (3) Incubation: 0, 2, 4, 8, 16, 24, and 48 h | (1) Trypan blue (2) Crystal violet assay (3) Annexin V/PI (FC) | (1) Cells had 10% lower viability. (2) IC50 (24 h): 9.28 × 10−8 (1.63 × 10−9 to 5.28 × 10−6); IC50 (48 h): 5.12 × 10−8 (3.25 × 10−8 to 8.07 × 10−8); IC50 (48 + 24 h): 5.00 × 10−8 (3.43 × 10−8 to 7.29 × 10−8). (3) The maximal increase of apoptosis was 0.97% (p = 0.39) at 8 h. |
| Moschetta-Pinheiro et al. (2022) [60] | In vitro | MDA-MB-468 | CAR (1, 2, 4, 8, 10, and 20 µM) Incubation: 24 h | MTT assay | IC50 (µM): 10 Results showed that within 24 h, all CAR concentrations, except for 2 μM, were able to significantly reduce cell viability when compared to control (p < 0.05). |
| Munõz et al. (2019) [61] | In vitro and in vivo | (1) MDA-MB-231/LM2-4 (metastatic variant) (2) Female CB-17 SCID mice; 2 × 106 cells orthotopically implanted into the right inguinal mammary fat pad | CCP (1) 0.01, 0.05, 0.1, and 1 μM Incubation: 6 days (2) 20 mg/Kg/day through the drinking water, initiated on day 14 | (1) MTS assay (2) Tumor growth and volume (mm3) and H&E | (1) 1 μM showed a marked decrease in cell proliferation. (2) Tumor volume was reduced. The median of necrosis was 78% (70–80% range) for the control group and 85% (80–90% range) for the treated group. In the invasive tumor border, the percentage of necrosis was 16% (0–40% range) for untreated tumors and 40% (20–80% range) for the CCP group. No weight loss or other signs of toxicity were observed. |
| Ninomiya et al. (2013) [62] | In vitro | MDA-MB-231 | CAP. Plasma device: 9 kHz, He gas flow Exposure conditions: 4, 8, 12, 16, or 18 kV for 600 s Incubation: 24 h | Trypan blue | The half-maximal effective peak-to-peak voltage was 16.7 ± 0.3 kV. Cell viability reduced with the increase in voltage. |
| Norris et al. (2013) [63] | In vitro | HCC1937 | Olaparib (0.02–100 μM) Incubation: 120 h | SRB assay | IC50 (μM): ≈100 |
| Oncul et al. (2017) [64] | In vitro | MDA-MB-231 | DOX (50, 100, 200, 400, 800, 1000, 1500, 2000, 3000, 4000, 8000 nM) Incubation: 48 h | SRB assay; Annexin V/PI (FC) | IC50 (nM): 6602 Cells underwent apoptosis in proportions of 6.75, 15, and 8.25% when treated with 50, 200, and 800 nM of the drug, respectively. Necrotic cells increased by 29% as a response to treatment of 800 nM. |
| Park et al. (2015) [65] | In vitro | MDA-MB-231 | CAP Exposure time: 30 s, 10 times | Cell counting kit-8 and clonogenic assay; Annexin V/PI (FC) | Six days after the treatment, CAP reduced the growth rate compared to control. Apoptosis increased from 7.67 to 13.8%. |
| Parrella et al. (2014) [66] | In vitro | MDA-MB-231 | CAB or DOX Incubation: 48 and 72 h | MTT assay | IC50 (µM) CAB: 5150 (24 h) and 2790 (72 h) DOX: 19 (24 h) and 4 (72 h) |
| Pilco-Ferreto & Calaf (2016) [67] | In vitro | MDA-MB-231 | DOX (1, 2, 4, and 8 μM) Incubation: 24 and 48 h | MTT assay | IC50 (μM): 1 The increase in DOX concentration decreased the viability in a time- and dose-dependent manner. |
| Risinger et al. (2015) [68] | In vitro | MDA-MB-231, MDA-MB-468, BT-549, Hs578T, HCC1937 | PTX or DOC | SRB assay | MDA-MB-468 was the most sensitive, and BT-549 and HCC1937 were the most resistant. |
| Sauter et al. (1986) [69] | In vitro | BT-20 | CCP or DOX | Phase-contrast microscopy | Cytotoxicity effect was measured by cytopathogenic effect, with no results from CCP. It was 1.7 μM regarding DOX. |
| Shaked et al. (2016) [70] | In vivo | MDA-MB-231/LM2–4 (metastatic variant); Female CB-17 SCID mice; 2 × 106 cells were orthotopically implanted in the mammary fat pad of 6-week-old females | CAB (LDM: 100 mg/kg; MTD: 400 mg/kg/day for 4 days followed by a 17-day drug-free break period) or CCP (20 mg/kg/day through the drinking water) | Survival | There were no significant differences in the mortality between CAB LDM, CAB MTD, and control. Adding CCP to the LDM of CAB significantly increased the survival percentage compared to the control (p = 0.006). |
| Stope et al. (2020) [71] | In vitro | MDA-MB-231 | CAP Exposure time: 5, 20, and 60 s PAM Exposure time: 20 and 60 s Incubation: 4, 24, 48, 72, 96, and 120 h | Cell counting | CAP: Effects were seen after 20 s of treatment and 72 h of incubation. More pronounced effects were seen after 60 s. After 60 s, a 4.5-fold growth reduction occurred from 4 to 120 h of incubation. PAM: The results showed a slightly lower anti-proliferative potential for PAM than for CAP. From 4 to 120 h, cell growth was reduced threefold. At 48 h of incubation, the cell growth reduced significantly from the control at two conditions. |
| Subramanian et al. (2020) [72] | In vitro | MDA-MB-231 | PAM. Plasma device: 5 kV, 15 kHz, 6.8 ± 0.6 W Solution: UP water Exposure time: 6, 12, and 18 min Volume: 60, 80, 100, 150, and 200 µL for 6 min | MTT assay | Cell viability was 81% (p < 0.001), 55% (p < 0.001), and 24% (p < 0.001) after 6, 12, and 18 min, respectively, under a volume of 200 μL. A significant reduction of cell viability was observed only at higher volumes (>100 μL), with 66% (p < 0.01) and 20% (p < 0.001) at 150 and 200 μL, respectively. |
| Taherian et al. (2012) [73] | In vitro | MDA-MB-231 | DOX or DOC; Incubation: 48 h | MTT assay | IC50 (nM) DOX: 887.75 ± 65.26; DOC: 634.58 ± 92.4 |
| Tassone et al. (2003) [74] | In vitro | MDA-MB-231, HCC1937 | DOX (from 0.1 to 100 µM) or PTX (from 0.01 to 2 µM); Incubation: 48 h | MTT assay; Annexin V/PI (FC) | IC50 (µM) DOX: 45–50 (HCC1937); 5–10 (MDA-MB-231) PTX: 2 (HCC1937); 0.01–0.02 (MDA-MB-231) An apoptotic effect was seen in HCC1937 cells exposed to PTX IC50. |
| Terefinko et al. (2021) [75] | In vitro | MDA-MB-231 | PAM. Plasma device: 6 kV, 66.45 kHz, He gas flow rate at 10.6 L/min Solution: DMEM or Opti-MEM media with or without 3% FBS; Incubation: 24 and 48 h Exposure time: 150, 180, 210, and 240 s Volume: 1.5 or 3 mL | MTT assay; Annexin V/PI (FC) | Without FBS: No significant results in cells incubated with DMEM-activated media. However, after 48 h, Opti-MEM-activated media exhibited a great impact on the decrease in cell viability, especially in the treatment times of 180 and 240 s (** p < 0.001, *** p < 0.0004, respectively). With FBS: DMEM-activated media did not affect cell viability. On the other hand, Opti-MEM-activated media affected cell viability after 180 and 240 s (** p < 0.0014; *** p < 0.0002, respectively) at 24 h. At 48 h, cell viability was reduced in all exposure times (* p < 0.013; ** p < 0.0014; *** p < 0.0002). Opti-MEM-activated media exhibited the most prominent reduction of the live cell population after the one-day experiment (day 1—from 84.00% to 68.12%, **** p < 0.0001; day 2—from 84.00% to 67.86%, ** p < 0.0015). |
| Wali et al. (2017) [76] | In vitro | BT-20, MDA-MB-231, MDA-MB-468, BT-549, MDA-MB-436, HCC38 | PTX (0.03, 0.01, 0.03, 0.1, 1 µM) Incubation: 72 h | ATP-based CellTiter-Glo® luminescent; Cell viability assay | PTX reduced cell viability with increased concentrations in most cell lines. MDA-MB-231 was the less sensitive cell line. The highest concentration ≤ IC50 was 3 nM. |
| Wang et al. (2013) [21] | In vitro | MDA-MB-231 BRCA | CAP. Plasma device: 60 V/6 A, He gas flow rate of 4.6 L/min Incubation: 24, 48, and 120 h Exposure time: 30, 60, and 90 s | MTS assay | All CAP-treated groups showed significantly inhibited cell proliferation after 3 and 5 days (p < 0.01). |
| Wang et al. (2021) [77] | In vitro | MDA-MB-231, MDA-MB-468 | PAM. Plasma device: Ar jet, model kINPen 09, gas flow rate of 5.0 L/m Exposure time: 10 min PAM was diluted to different concentrations as designated by the percent remaining (e.g., 70% 10PAM refers to 70% concentration at use) Incubation: 24 h | Cell viability assay | The cell viability of MDA-MB-468 and MDA-MB-231 cells subjected to 100% PAM was 40.29 ± 6% and 16.02 ± 5.02%, respectively. Treatment did not influence the attached cell numbers of MDA-MB-468 cells but did inhibit the MDA-MB-231 cell line, which indicated MDA-MB-231 cells were more sensitive than were the other cancer lines. |
| Wesierska-Gadek et al. (2015) [78] | In vitro | BT-20 | Olaparib (from 1 to 10 µM) Incubation: 24, 48, and 72 h | CellTiter-Glo® cell viability assay (correlated with ATP levels) | There were no significant variations in the number of viable cells or increase of apoptosis. |
| Xiang et al. (2018) [79] | In vitro and in vivo | (1) MDA-MB-231, MDA-MB-468 (2) Female BALB/c mice; 1 × 106 MDA-MB-231 cells were injected subcutaneously | PAM. Plasma device: 1.0 to 1.4 kV, 8.8 kHz, He gas flow was 1 L/min Solution: 2 mL of medium; Exposure time: 1, 2, 3, 4, and 5 min Incubation: 24 h | (1) Cell counting kit-8; Annexin V/PI (FC) (2) Tumor growth and weight | (1) Five-minute PAM reduced the viability to 0.41 and 0.46, respectively, for MDA-MB-231 and MDA-MB-468 cells. The relative apoptosis increased on both cell lines compared to healthy cells. (2) Tumor growth was inhibited, and tumor weight dropped considerably after PAM treatment (from 4.053 g to 0.787 g, p = 4.69 × 10−4). No visible side effects were observed. |
| Yan et al. (2015) [80] | In vitro | MDA-MB-231 | PAM. Plasma device: 3.16 kV, 5 W, He gas flow rate was 4.7 L/min (1) Cell concentrations: 20,000, 40,000, and 80,000 cells/mL Exposure time: 30, 60, 90, and 120 s (2) Well number on a plate: 6, 12, 24, and 48 (3) Volume media: 1, 2, 3, and 4 mL Exposure time: 60 s Incubation: 72 h | MTT assay | (1) The anti-tumor capacity increased as the treatment time exposure increased and decreased as the cell seeding confluence decreased. (2) One minute after PAM, proliferation decreased as the size of the wells decreased. The effect of treatment was reduced 2/3 in the 48-well plate compared to the 6-well plate. (3) Relative viability significantly increased as the volume of media increased from 1 to 4 mL. |
| Yan et al. (2017) [81] | In vitro | MDA-MB-231 | PAM. Plasma device: 3.16 kV, 30 kHz, He gas flow rate was 4.7 L/min Solution: Ringer’s solution mixed with DMEM or only medium; Exposure time: 60 s Incubation: 20 min, 1, 2, 3, and 4 h | MTT assay | Removing PAM 2, 3, or 4 h after the treatment did not change the effect of PAM on cell viability. When PAM was removed 1 h after treatment, the cytotoxicity was not as severe. The dilution remarkably impacted the anti-cancer capacity of the PAM solutions. |
| Yaourtis et al. (2023) [82] | In vitro | MDA-MB-231 (spindle and stellar phenotype) | DOX (Serial dilutions, from 0 to 10 µM) Incubation: 72 h | MTT assay | Spindle phenotype: IC50 = 0.31 ± 0.05 µM, p > 0.05 Stellar phenotype: IC50 = 0.25 ± 0.05 µM, p > 0.05 |
| Zasadil et al. (2014) [83] | In vitro | MDA-MB-231; CAL51 | PTX (5, 10, 20, 50, or 100 nM) Incubation: 24,72 and 120 h | Trypan blue; Clonogenic assay | Low nanomolar concentrations of PTX caused a decrease in live cell numbers over 120 h. Colony formation was substantially inhibited at concentrations ≥5 nM after 14 days. |
| Zhou et al. (2020) [84] | In vivo | Female BALB/c mice; 3 × 106 MDA-MB-231 cells were injected subcutaneously in the right forelimbs | CAP or PAM. Plasma device: 5 kV, 8.8 kHz; He gas flow was 0.2 L/min CAP Exposure time: 5 min PAM injection treatment Solution: 2 mL of PBS Exposure time: 10 min It was subcutaneously administered into two slots of the tumor in each mouse at 100 µL/slot. Treatments were repeated every 72 h until death or the end of study (30 days). | Tumor monitoring | All mice in the control group died within 27 days, and all mice from the CAP direct group survived to the last day. The 30-day survival of mice in the CAP group was significantly higher than that of the PAM group (p = 4.9 × 10−4). Both treatments significantly inhibited tumor growth (CAP: p = 0.044 for CAP; PAM: p = 0.017). However, the growth of the tumors in the PAM group was more suppressed than that in the CAP group. |
| Key Aspect | Highlights |
|---|---|
| TNBC | (1) Due to its aggressive nature and poor prognosis compared to other molecular subtypes, TNBC requires a broader range of treatment options. (2) Chemotherapy is a well-established treatment for TNBC, but it comes with associated adverse effects. The selection of chemotherapy drugs, particularly paclitaxel, docetaxel, cyclophosphamide, doxorubicin, olaparib, carboplatin, and capecitabine, was based on ESMO and ASCO guidelines. |
| Plasma treatment | Cold plasma, investigated across various medical fields, including tumor therapy, shows promise in cancer treatment, including TNBC, with results indicating cell death. |
| Search | (1) Initial retrieval of 19,364 studies from four databases. (2) After screening, 59 articles were included in the systematic review. Articles were published between 1986 and 2023, with focus on the efficacy of chemotherapy drugs and CAP treatment. |
| In vitro studies | (1) In vitro studies demonstrated a reduction in cell proliferation with various chemotherapy concentrations tested, and additive interactions were observed between paclitaxel and carboplatin. (2) Different strategies, including CAP and PAM, exhibited a time-dependent reduction in TNBC cell viability, with apoptosis being the predominant type of cell death. (3) Combination therapies involving cold plasma and chemotherapy drugs tended to improve cytotoxicity in TNBC cell lines. |
| In vivo studies | Animal models are crucial for assessing therapy efficacy. Studies demonstrated inhibition of tumor growth with no noticeable adverse effects in animal models regarding CAP treatment. |
| Limitations | Heterogeneity between studies, including methodological approaches and lack of detailed information, poses limitations to meta-analysis studies and conclusive interpretations. This emphasizes the need for standardized methodologies. |
| Future directions | (1) This systematic review underscores the need for further research using standardized methodologies to address current limitations and advance clinical translation. (2) Studies directly comparing CAP, PAM, and standard chemotherapy regimens should be performed, including the evaluation of cell death and associated mechanisms of action. (3) Conducting studies to unravel specific protein alterations after CAP and PAM treatment might be a strategy for establishing combinations with drugs used in clinical practice. (4) Future studies should consider other animal models and explore combination therapies. Cold plasma therapy could potentially reduce chemotherapy-associated side effects by lowering drug concentrations, necessitating further investigation in this field. (5) The use of patient-derived xenografts must be considered as a key approach to verifying the effects of CAP. The findings should be correlated with patients’ clinical data. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida-Ferreira, C.; Marto, C.M.; Carmo, C.; Almeida-Ferreira, J.; Frutuoso, C.; Carvalho, M.J.; Botelho, M.F.; Laranjo, M. Efficacy of Cold Atmospheric Plasma vs. Chemotherapy in Triple-Negative Breast Cancer: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 3254. https://doi.org/10.3390/ijms25063254
Almeida-Ferreira C, Marto CM, Carmo C, Almeida-Ferreira J, Frutuoso C, Carvalho MJ, Botelho MF, Laranjo M. Efficacy of Cold Atmospheric Plasma vs. Chemotherapy in Triple-Negative Breast Cancer: A Systematic Review. International Journal of Molecular Sciences. 2024; 25(6):3254. https://doi.org/10.3390/ijms25063254
Chicago/Turabian StyleAlmeida-Ferreira, Catarina, Carlos Miguel Marto, Chrislaura Carmo, Joana Almeida-Ferreira, Cristina Frutuoso, Maria João Carvalho, Maria Filomena Botelho, and Mafalda Laranjo. 2024. "Efficacy of Cold Atmospheric Plasma vs. Chemotherapy in Triple-Negative Breast Cancer: A Systematic Review" International Journal of Molecular Sciences 25, no. 6: 3254. https://doi.org/10.3390/ijms25063254
APA StyleAlmeida-Ferreira, C., Marto, C. M., Carmo, C., Almeida-Ferreira, J., Frutuoso, C., Carvalho, M. J., Botelho, M. F., & Laranjo, M. (2024). Efficacy of Cold Atmospheric Plasma vs. Chemotherapy in Triple-Negative Breast Cancer: A Systematic Review. International Journal of Molecular Sciences, 25(6), 3254. https://doi.org/10.3390/ijms25063254