
Beyond Visual Assessment of Basal Ganglia Uptake: Can Automated Method and Pineal Body Uptake Assessment Improve Identification of Nigrostriatal Dysfunction on 18F-DOPA PET/CT?


Abstract
1. Introduction
2. Results
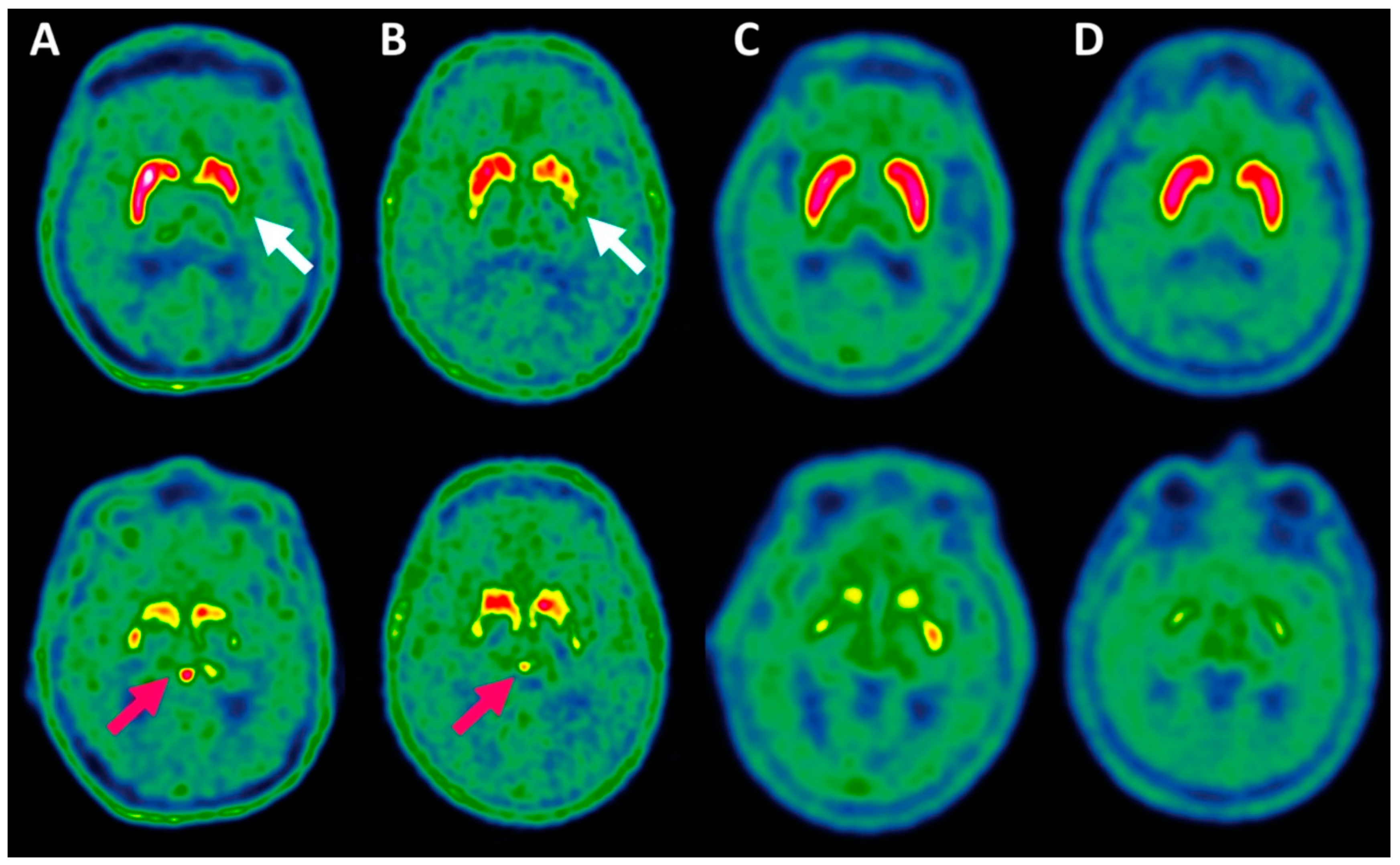
2.1. Evaluation of Basal Ganglia 18F-DOPA Uptake by Visual Assessment and Automated Method to Identify NSD
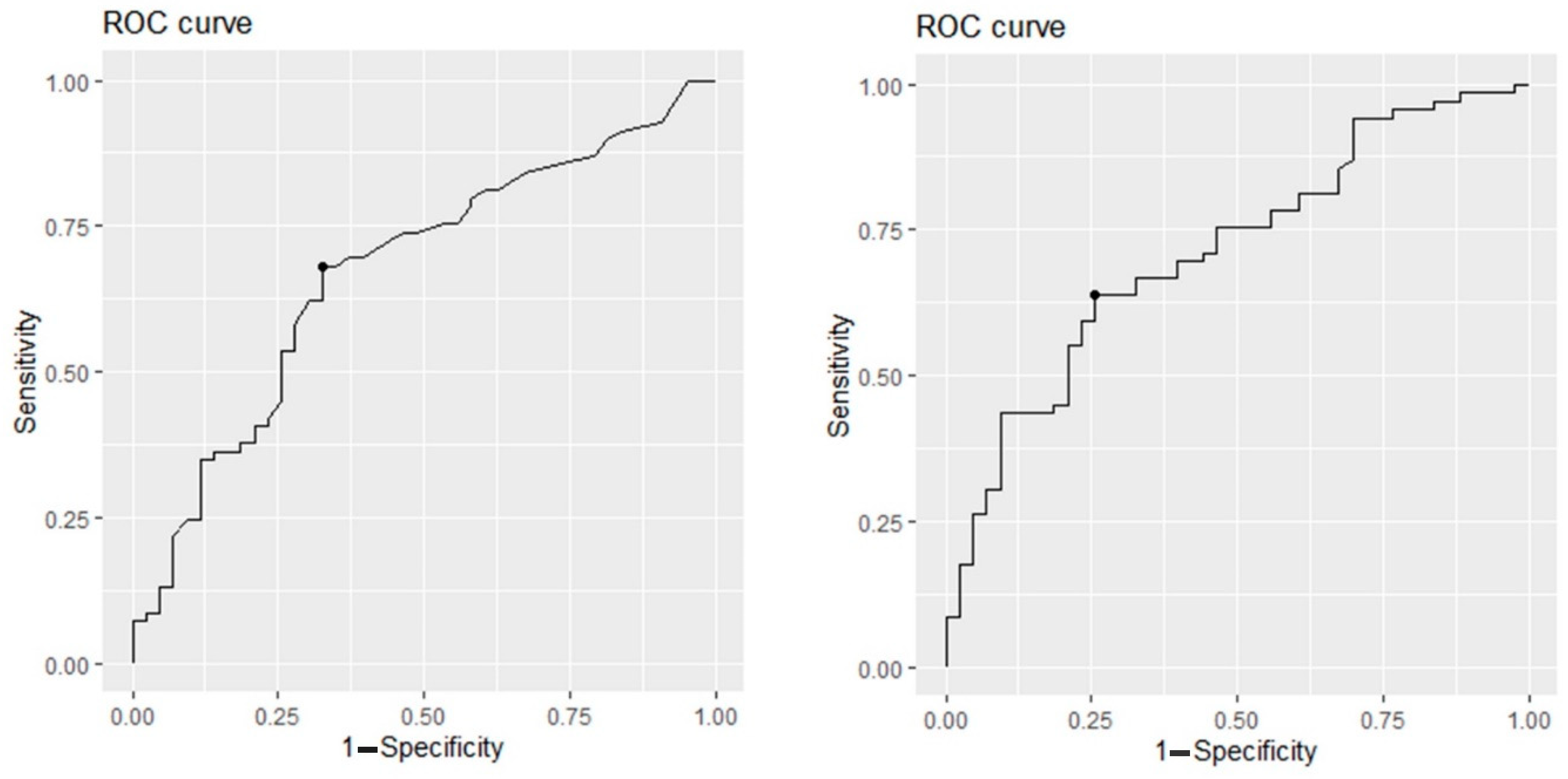
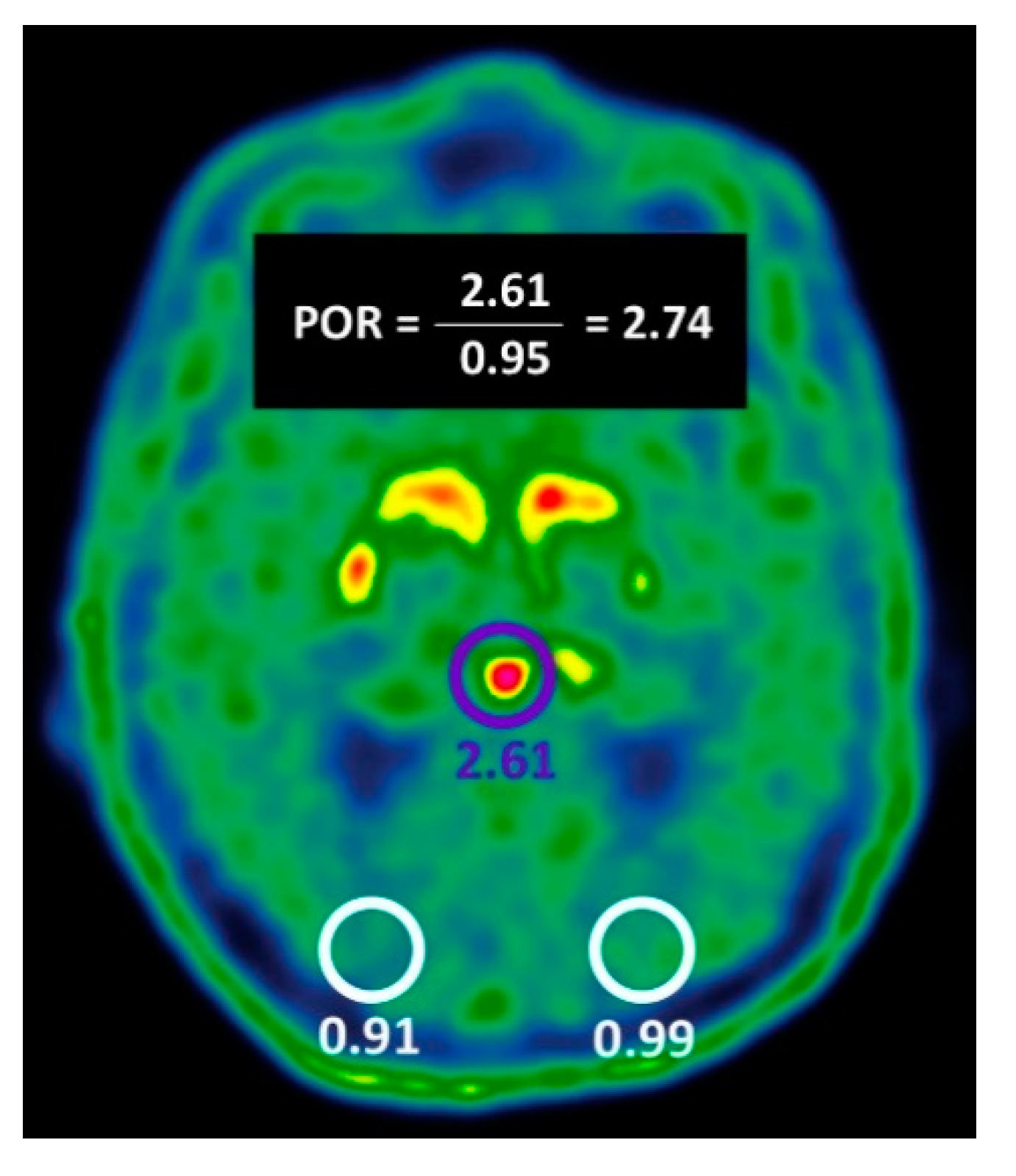
2.2. Evaluation of Pineal Body 18F-DOPA Uptake Parameters to Identify NSD
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. PET/CT Acquisition
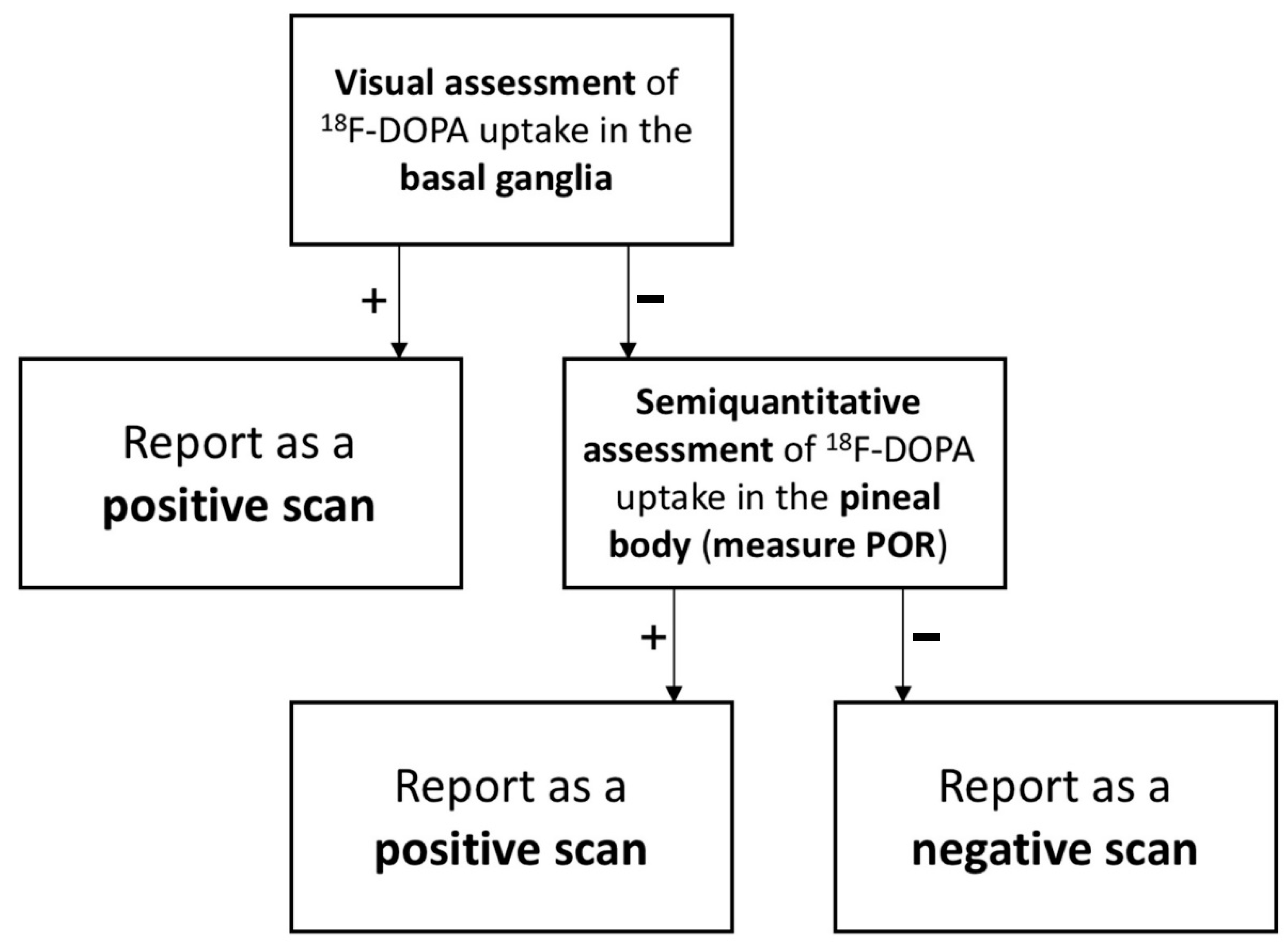
4.3. Investigated Imaging Criteria
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Rizzo, G.; Copetti, M.; Arcuti, S.; Martino, D.; Fontana, A.; Logroscino, G. Accuracy of clinical diagnosis of Parkinson disease: A systematic review and meta-analysis. Neurology 2016, 86, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Mitra, K.; Gangopadhaya, P.K.; Das, S.K. Parkinsonism plus syndrome—A review. Neurol. India 2003, 51, 183–188. [Google Scholar] [PubMed]
- O’Sullivan, S.S.; Williams, D.R.; Gallagher, D.A.; Massey, L.A.; Silveira-Moriyama, L.; Lees, A.J. Nonmotor symptoms as presenting complaints in Parkinson’s disease: A clinicopathological study. Mov. Disord. 2008, 23, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Arena, J.E.; Stoessl, A.J. Optimizing diagnosis in Parkinson’s disease: Radionuclide imaging. Parkinsonism Relat. Disord. 2016, 22 (Suppl. S1), S47–S51. [Google Scholar] [CrossRef]
- Garnett, E.S.; Firnau, G.; Nahmias, C. Dopamine visualized in the basal ganglia of living man. Nature 1983, 305, 137–138. [Google Scholar] [CrossRef]
- Eshuis, S.A.; Jager, P.L.; Maguire, R.P.; Jonkman, S.; Dierckx, R.A.; Leenders, K.L. Direct comparison of FP-CIT SPECT and F-DOPA PET in patients with Parkinson’s disease and healthy controls. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 454–462. [Google Scholar] [CrossRef]
- Ishikawa, T.; Dhawan, V.; Kazumata, K.; Chaly, T.; Mandel, F.; Neumeyer, J.; Margouleff, C.; Babchyck, B.; Zanzi, I.; Eidelberg, D. Comparative nigrostriatal dopaminergic imaging with iodine-123-beta CIT-FP/SPECT and fluorine-18-FDOPA/PET. J. Nucl. Med. 1996, 37, 1760–1765. [Google Scholar]
- Dhawan, V.; Niethammer, M.H.; Lesser, M.L.; Pappas, K.N.; Hellman, M.; Fitzpatrick, T.M.; Bjelke, D.; Singh, J.; Quatarolo, L.M.; Choi, Y.Y.; et al. Prospective F-18 FDOPA PET Imaging Study in Human PD. Nucl. Med. Mol. Imaging 2022, 56, 147–157. [Google Scholar] [CrossRef]
- Jokinen, P.; Helenius, H.; Rauhala, E.; Brück, A.; Eskola, O.; Rinne, J.O. Simple ratio analysis of 18F-fluorodopa uptake in striatal subregions separates patients with early Parkinson disease from healthy controls. J. Nucl. Med. 2009, 50, 893–899. [Google Scholar] [CrossRef]
- Takikawa, S.; Dhawan, V.; Chaly, T.; Robeson, W.; Dahl, R.; Zanzi, I.; Mandel, F.; Spetsieris, P.; Eidelberg, D. Input functions for 6-[fluorine-18]fluorodopa quantitation in parkinsonism: Comparative studies and clinical correlations. J. Nucl. Med. 1994, 35, 955–963. [Google Scholar]
- Dhawan, V.; Ma, Y.; Pillai, V.; Spetsieris, P.; Chaly, T.; Belakhlef, A.; Margouleff, C.; Eidelberg, D. Comparative analysis of striatal FDOPA uptake in Parkinson’s disease: Ratio method versus graphical approach. J. Nucl. Med. 2002, 43, 1324–1330. [Google Scholar] [PubMed]
- Chang, I.C.; Lue, K.H.; Hsieh, H.J.; Liu, S.H.; Kao, C.H. Automated striatal uptake analysis of ¹⁸F-FDOPA PET images applied to Parkinson’s disease patients. Ann. Nucl. Med. 2011, 25, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, M.; Rudolf, J.; Hilker, R.; Herholz, K.; Heiss, W.D. Increased pineal Fdopa uptake is related to severity of Parkinson’s disease—A PET study. J. Pineal. Res. 2001, 30, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.Y.; Whone, A.L.; Brooks, D.J. Extrastriatal monoamine neuron function in Parkinson’s disease: An 18F-dopa PET study. Neurobiol. Dis. 2008, 29, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Rakshi, J.S.; Uema, T.; Ito, K.; Bailey, D.L.; Morrish, P.K.; Ashburner, J.; Dagher, A.; Jenkins, I.H.; Friston, K.J.; Brooks, D.J. Frontal, midbrain and striatal dopaminergic function in early and advanced Parkinson’s disease A 3D [(18)F]dopa-PET study. Brain 1999, 122 Pt 9, 1637–1650. [Google Scholar] [CrossRef]
- Tolosa, E.; Wenning, G.; Poewe, W. The diagnosis of Parkinson’s disease. Lancet Neurol. 2006, 5, 75–86. [Google Scholar] [CrossRef]
- Wallert, E.D.; van de Giessen, E.; Knol, R.J.J.; Beudel, M.; de Bie, R.M.A.; Booij, J. Imaging Dopaminergic Neurotransmission in Neurodegenerative Disorders. J. Nucl. Med. 2022, 63 (Suppl. S1), 27S–32S. [Google Scholar] [CrossRef]
- Calabria, F.F.; Calabria, E.; Gangemi, V.; Cascini, G.L. Current status and future challenges of brain imaging with (18)F-DOPA PET for movement disorders. Hell. J. Nucl. Med. 2016, 19, 33–41. [Google Scholar] [CrossRef]
- Morbelli, S.; Esposito, G.; Arbizu, J.; Barthel, H.; Boellaard, R.; Bohnen, N.I.; Brooks, D.; Darcourt, J.; Dickson, J.; Douglas, D.; et al. EANM practice guideline/SNMMI procedure standard for dopaminergic imaging in Parkinsonian syndromes 1.0. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1885–1912. [Google Scholar] [CrossRef]
- Davidsson, A.; Georgiopoulos, C.; Dizdar, N.; Granerus, G.; Zachrisson, H. Comparison between visual assessment of dopaminergic degeneration pattern and semi-quantitative ratio calculations in patients with Parkinson’s disease and Atypical Parkinsonian syndromes using DaTSCAN® SPECT. Ann. Nucl. Med. 2014, 28, 851–859. [Google Scholar] [CrossRef]
- Adler, C.H.; Beach, T.G.; Hentz, J.G.; Shill, H.A.; Caviness, J.N.; Driver-Dunckley, E.; Sabbagh, M.N.; Sue, L.I.; Jacobson, S.A.; Belden, C.M.; et al. Low clinical diagnostic accuracy of early vs advanced Parkinson disease: Clinicopathologic study. Neurology 2014, 83, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Arena, J.E.; Urrutia, L.; Falasco, G.; de Leon, M.P.; Vazquez, S. Quantification methods comparison in brain 18F-FDOPA PET. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 274–281. [Google Scholar] [PubMed]
- Bernheimer, H.; Birkmayer, W.; Hornykiewicz, O.; Jellinger, K.; Seitelberger, F. Brain dopamine and the syndromes of Parkinson and Huntington. Clinical, morphological and neurochemical correlations. J. Neurol. Sci. 1973, 20, 415–455. [Google Scholar] [CrossRef] [PubMed]
- Brooks, D.; Salmon, E.; Mathias, C.J.; Quinn, N.; Leenders, K.L.; Bannister, R.; Marsden, C.D.; Frackowiak, R. The relationship between locomotor disability, autonomic dysfunction, and the integrity of the striatal dopaminergic system in patients with multiple system atrophy, pure autonomic failure, and Parkinson’s disease, studied with PET. Brain 1990, 113 Pt 5, 1539–1552. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Rahmani, B.; Gandhi, J.; Seyam, O.; Joshi, G.; Reid, I.; Smith, N.L.; Waltzer, W.C.; Khan, S.A. Revisiting the pineal gland: A review of calcification, masses, precocious puberty, and melatonin functions. Int. J. Neurosci. 2020, 130, 464–475. [Google Scholar] [CrossRef]
- Kish, S.J.; Zhong, X.H.; Hornykiewicz, O.; Haycock, J.W. Striatal 3,4-dihydroxyphenylalanine decarboxylase in aging: Disparity between postmortem and positron emission tomography studies? Ann. Neurol. 1995, 38, 260–264. [Google Scholar] [CrossRef]
- Kaasinen, V.; Vahlberg, T. Striatal dopamine in Parkinson disease: A meta-analysis of imaging studies. Ann. Neurol. 2017, 82, 873–882. [Google Scholar] [CrossRef]
- Morrish, P.K.; Sawle, G.V.; Brooks, D.J. Regional changes in [18F]dopa metabolism in the striatum in Parkinson’s disease. Brain 1996, 119 Pt 6, 2097–2103. [Google Scholar] [CrossRef]
- DaTQUANTTM. GE Healthcare Website. Available online: https://www.gehealthcare.com/products/nuclearimaging-agents/datquant (accessed on 10 January 2023).
- Evans, A.C.; Collins, D.L.; Mills, S.R.; Brown, E.D.; Kelly, R.L.; Peters, T.M. 3D statistical neuroanatomical models from 305 MRI volumes. In Proceedings of the 1993 IEEE Conference Record Nuclear Science Symposium and Medical Imaging Conference, San Francisco, CA, USA, 31 October–6 November 1993; pp. 1813–1817. [Google Scholar]
- Booij, J.; Speelman, J.D.; Horstink, M.W.; Wolters, E.C. The clinical benefit of imaging striatal dopamine transporters with [123I]FP-CIT SPET in differentiating patients with presynaptic parkinsonism from those with other forms of parkinsonism. Eur. J. Nucl. Med. 2001, 28, 266–272. [Google Scholar] [CrossRef]
- Cutpointr: Determine and Evaluate Optimal Cutpoints in Binary Classification Tasks. Available online: https://cran.r-project.org/web/packages/cutpointr/index.html (accessed on 27 November 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Positivity among NSD Patients | Positivity among Non-NSD Patients | p Value | |
|---|---|---|---|
| VA-BG | 61/69 (88.4%) | 3/43 (7%) | <0.01 |
| AM-BG | 37/69 (53.6%) | 3/43 (7%) | <0.01 |
| Sensitivity | Specificity | Accuracy | PPV | NPV | |
|---|---|---|---|---|---|
| VA-BG | 61/69 (88.4%) | 40/43 (93.0%) | 101/112 (90.2%) | 61/64 (95.3%) | 40/48 (83.3%) |
| AM-BG | 37/69 (53.6%) | 40/43 (93.0%) | 77/112 (68.8%) | 37/40 (92.5%) | 40/72 (55.6%) |
| VA-BG OR AM-BG | 63/69 (91.3%) | 38/43 (88.4%) | 101/112 (90.2%) | 63/68 (92.6%) | 38/44 (86.4%) |
| VA-BG AND AM-BG | 35/69 (50.7%) | 42/43 (97.7%) | 77/112 (68.8%) | 35/36 (97.2%) | 42/76 (55.3%) |
| Positivity among NSD Patients | Positivity among Non-NSD Patients | p Value | |
|---|---|---|---|
| VA-PB | 48/69 (69.6%) | 17/43 (39.5%) | <0.01 |
| SUVmax ≥ 0.72 | 47/69 (68.1%) | 14/43 (32.6%) | <0.01 |
| POR ≥ 1.57 | 44/69 (63.8%) | 11/43 (25.6%) | <0.01 |
| Sensitivity | Specificity | Accuracy | PPV | NPV | |
|---|---|---|---|---|---|
| VA-BG | 61/69 (88.4%) | 40/43 (93.0%) | 101/112 (90.2%) | 61/64 (95.3%) | 40/48 (83.3%) |
| VA-PB | 48/69 (69%) | 26/43 (60%) | 74/112 (66%) | 48/65 (74%) | 26/47 (55%) |
| SUVmax ≥ 0.72 | 47/69 (68%) | 29/43 (67.4%) | 76/112 (67.8%) | 47/61 (77.0%) | 29/51 (56.8%) |
| POR ≥ 1.57 | 44/69 (63.7%) | 32/43 (74.4%) | 76/112 (67.8%) | 44/55 (80%) | 32/57 (56.1%) |
| VA-BG OR POR ≥ 1.57 | 68/69 (98.5%) | 29/43 (67.4%) | 97/112 (86.6%) | 68/82 (82.9%) | 29/30 (96.6%) |
| VA-BG AND POR ≥ 1.57 | 37/69 (53.6%) | 43/43 (100%) | 80/112 (71.4%) | 37/37 (100%) | 43/75 (57.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hazut Krauthammer, S.; Cohen, D.; Even-Sapir, E.; Lerman, H. Beyond Visual Assessment of Basal Ganglia Uptake: Can Automated Method and Pineal Body Uptake Assessment Improve Identification of Nigrostriatal Dysfunction on 18F-DOPA PET/CT? Int. J. Mol. Sci. 2023, 24, 5683. https://doi.org/10.3390/ijms24065683
Hazut Krauthammer S, Cohen D, Even-Sapir E, Lerman H. Beyond Visual Assessment of Basal Ganglia Uptake: Can Automated Method and Pineal Body Uptake Assessment Improve Identification of Nigrostriatal Dysfunction on 18F-DOPA PET/CT? International Journal of Molecular Sciences. 2023; 24(6):5683. https://doi.org/10.3390/ijms24065683
Chicago/Turabian StyleHazut Krauthammer, Shir, Dan Cohen, Einat Even-Sapir, and Hedva Lerman. 2023. "Beyond Visual Assessment of Basal Ganglia Uptake: Can Automated Method and Pineal Body Uptake Assessment Improve Identification of Nigrostriatal Dysfunction on 18F-DOPA PET/CT?" International Journal of Molecular Sciences 24, no. 6: 5683. https://doi.org/10.3390/ijms24065683
APA StyleHazut Krauthammer, S., Cohen, D., Even-Sapir, E., & Lerman, H. (2023). Beyond Visual Assessment of Basal Ganglia Uptake: Can Automated Method and Pineal Body Uptake Assessment Improve Identification of Nigrostriatal Dysfunction on 18F-DOPA PET/CT? International Journal of Molecular Sciences, 24(6), 5683. https://doi.org/10.3390/ijms24065683