
Outdoor Air Pollution and Childhood Respiratory Disease: The Role of Oxidative Stress

 ,
,  , , ,
, , , 
Abstract
1. Introduction
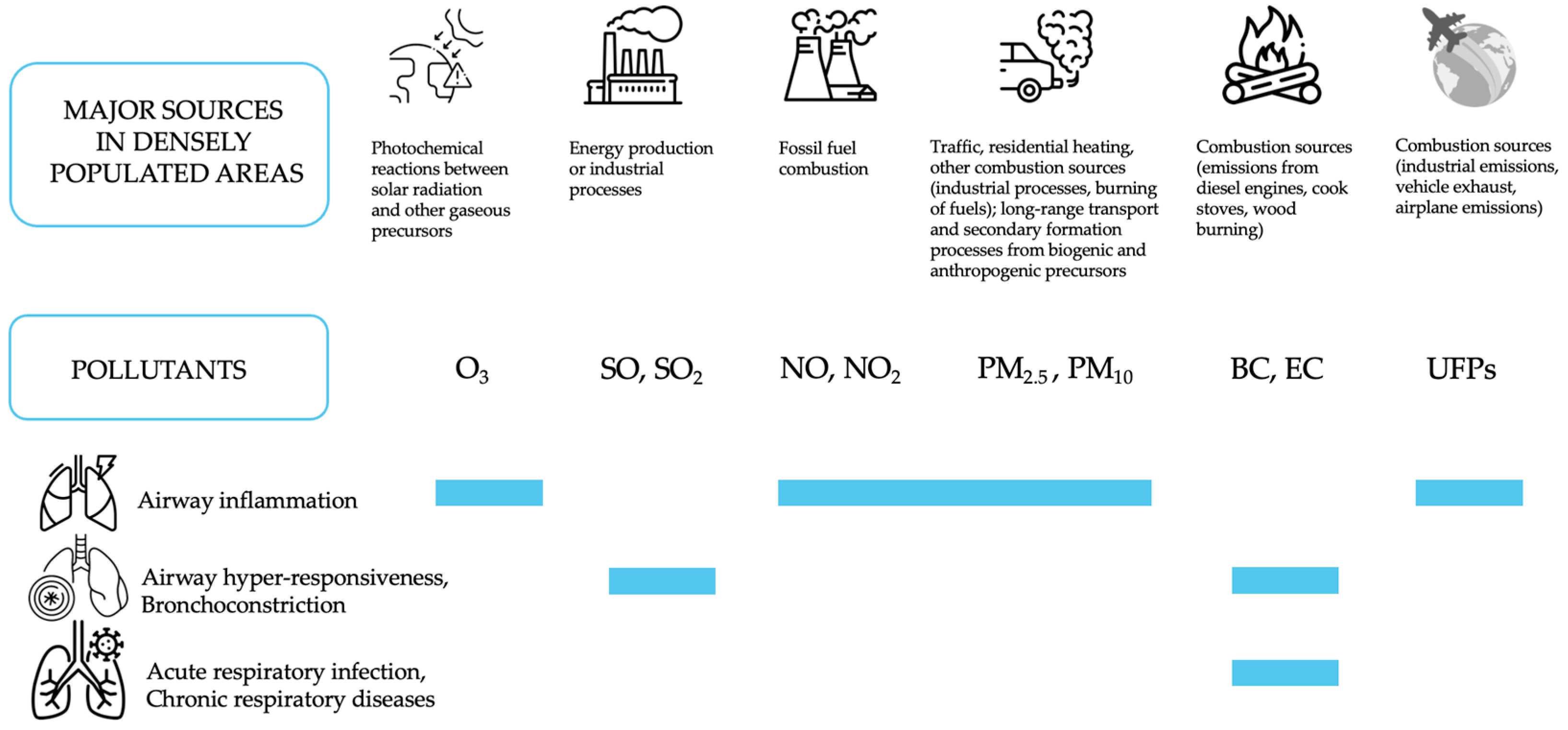
2. Main Outdoor Air Pollutants and Their Composition
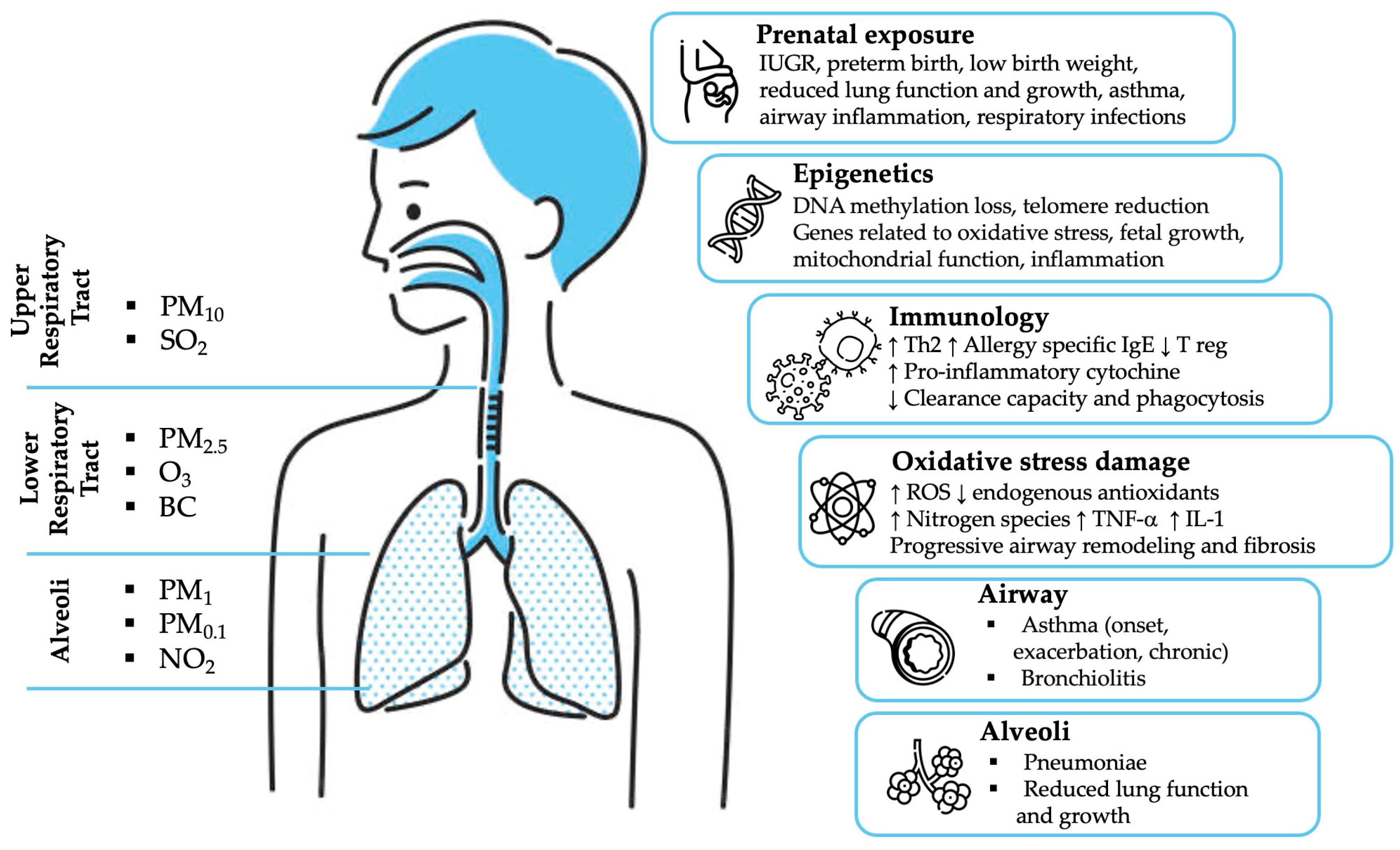
2.1. Air Pollution and Health Effects
2.2. Gases
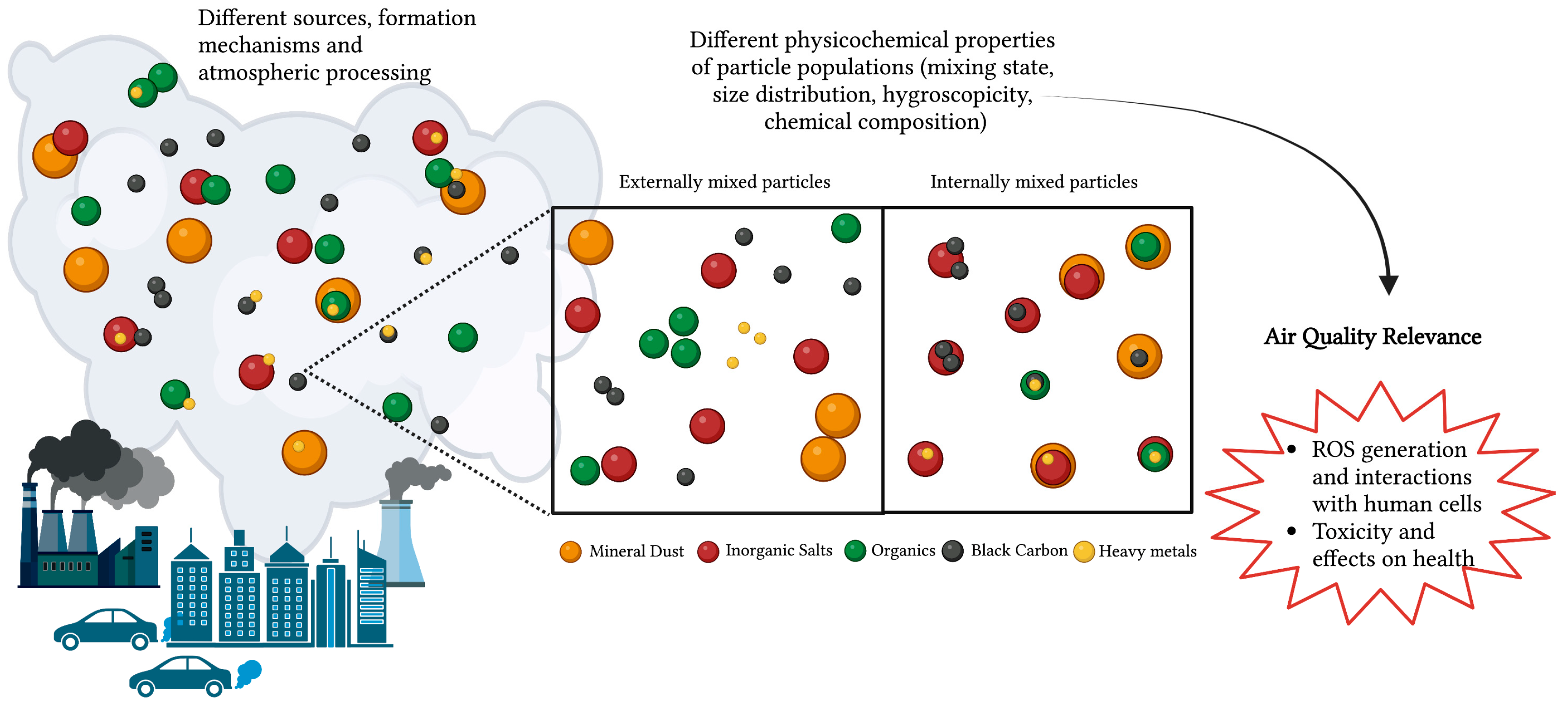
2.3. Particulate Matter (PM)
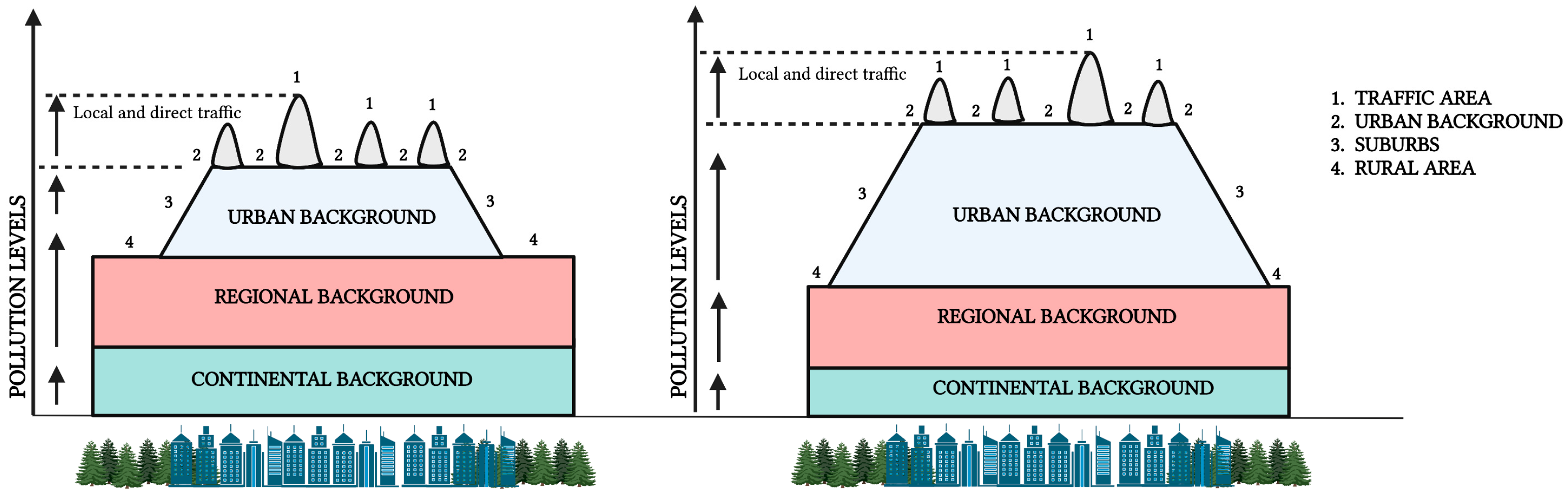
2.4. Traffic-Related Air Pollution (TRAP)
3. Health Outcomes: Effects on Childhood Respiratory Health
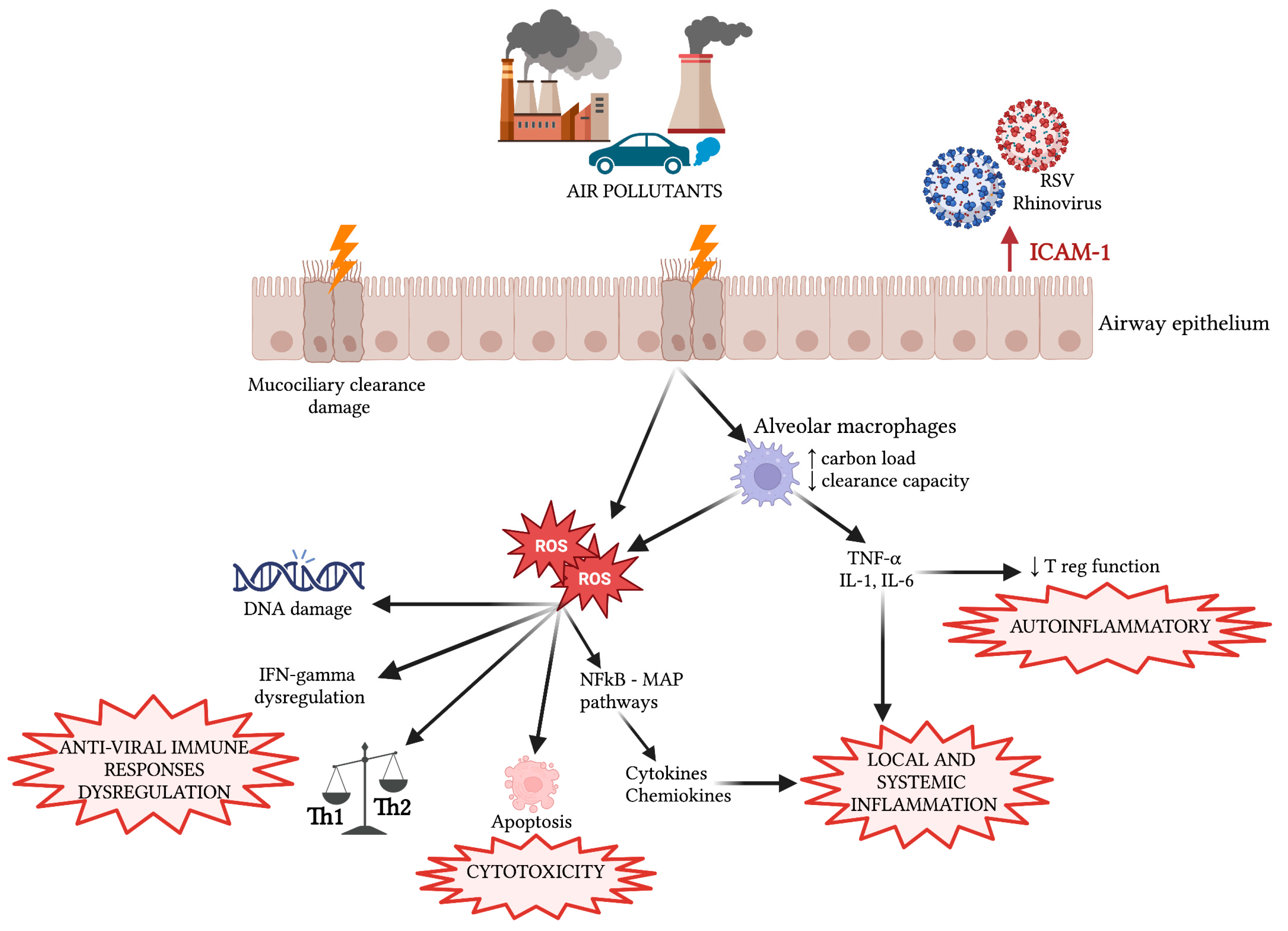
3.1. Local and Systemic Inflammation and Oxidative Stress Damage
3.2. Immune Response Modulation
3.3. Genetic and Epigenetic Changes
4. Focus on Respiratory Diseases
4.1. Asthma
4.2. Bronchiolitis
4.3. Respiratory Infections
4.4. Lifelong Effects on Respiratory Function
5. Prenatal Exposure
6. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| APCs | Antigen Presenting Cells |
| BED | Biologically Effective Dose |
| BC | Black Carbon |
| CO | Carbon Monoxide |
| COPD | Chronic Obstructive Pulmonary Disease |
| EC | Elemental Carbon |
| FEF25–75 | Forced Mid-Expiratory Flow |
| FEV1 | Forced Expiratory Volume in One Second |
| FVC | Forced Vital Capacity |
| GM-CSF | Granulocyte-Macrophage Colony-Stimulating Factor |
| ICAM-1 | Intercellular Adhesion Molecule-1 |
| IL | Interleukin |
| IQR | Interquartile Range |
| IUGR | Intrauterine Growth Restriction |
| MMEF | Maximum Mid-Expiratory Flow |
| NO, NO2 | Nitrogen Oxides |
| O3 | Ozone |
| OR | Odds Ratio |
| PAHs | Polycyclic Aromatic Hydrocarbons |
| PM | Particulate Matter |
| PM0.1 | Particulate Matter with an aerodynamic diameter of 0.1 μm |
| PM2.5 | Particulate matter with an aerodynamic diameter of 2.5 µm |
| PM10 | Particulate matter with an aerodynamic diameter of 10 µm |
| ROS | Reactive Oxygen Species |
| RR | Risk Ratio |
| RSV | Respiratory Syncytial Virus |
| SO, SO2 | Sulphur Oxides |
| TLRs | Toll-Like Receptors |
| TRAP | Traffic-Related Air Pollution |
| TNFα | Tumor Necrosis Factor Alfa |
| UFPs | Ultra Fine Particles |
| VOCs | Volatile Organic Compounds |
| WHO | World Health Organization |
References
- More than 90% of the World’s Children Breathe Toxic Air Every Day. Available online: https://www.who.int/news/item/29-10-2018-more-than-90-of-the-worlds-children-breathe-toxic-air-every-day (accessed on 14 September 2022).
- Johannson, K.A.; Balmes, J.R.; Collard, H.R. Air Pollution Exposure: A Novel Environmental Risk Factor for Interstitial Lung Disease? Chest 2015, 147, 1161–1167. [Google Scholar] [CrossRef]
- Bălă, G.-P.; Râjnoveanu, R.-M.; Tudorache, E.; Motișan, R.; Oancea, C. Air Pollution Exposure-the (in)Visible Risk Factor for Respiratory Diseases. Environ. Sci. Pollut. Res. Int. 2021, 28, 19615–19628. [Google Scholar] [CrossRef] [PubMed]
- Ayres, J.G.; Borm, P.; Cassee, F.R.; Castranova, V.; Donaldson, K.; Ghio, A.; Harrison, R.M.; Hider, R.; Kelly, F.; Kooter, I.M.; et al. Evaluating the Toxicity of Airborne Particulate Matter and Nanoparticles by Measuring Oxidative Stress Potential—A Workshop Report and Consensus Statement. Inhal. Toxicol. 2008, 20, 75–99. [Google Scholar] [CrossRef]
- WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide. Available online: https://www.who.int/publications-detail-redirect/9789240034228 (accessed on 11 April 2022).
- Chen, J.; Hoek, G. Long-Term Exposure to PM and All-Cause and Cause-Specific Mortality: A Systematic Review and Meta-Analysis. Environ. Int. 2020, 143, 105974. [Google Scholar] [CrossRef] [PubMed]
- Valavanidis, A.; Fiotakis, K.; Vlachogianni, T. Airborne Particulate Matter and Human Health: Toxicological Assessment and Importance of Size and Composition of Particles for Oxidative Damage and Carcinogenic Mechanisms. J. Environ. Sci. Health C Environ. Carcinog. Ecotoxicol. Rev. 2008, 26, 339–362. [Google Scholar] [CrossRef]
- Pope, C.A.; Dockery, D.W. Health Effects of Fine Particulate Air Pollution: Lines That Connect. J. Air Waste Manag. Assoc. 2006, 56, 709–742. [Google Scholar] [CrossRef]
- Ricciardelli, I.; Bacco, D.; Rinaldi, M.; Bonafè, G.; Scotto, F.; Trentini, A.; Bertacci, G.; Ugolini, P.; Zigola, C.; Rovere, F.; et al. A Three-Year Investigation of Daily PM2.5 Main Chemical Components in Four Sites: The Routine Measurement Program of the Supersito Project (Po Valley, Italy). Atmos. Environ. 2017, 152, 418–430. [Google Scholar] [CrossRef]
- Costabile, F.; Gualtieri, M.; Ancona, C.; Canepari, S.; Decesari, S. Ultrafine Particle Features Associated with Pro-Inflammatory and Oxidative Responses: Implications for Health Studies. Atmosphere 2020, 11, 414. [Google Scholar] [CrossRef]
- Donaldson, K.; Tran, L.; Jimenez, L.A.; Duffin, R.; Newby, D.E.; Mills, N.; MacNee, W.; Stone, V. Combustion-Derived Nanoparticles: A Review of Their Toxicology Following Inhalation Exposure. Part. Fibre Toxicol. 2005, 2, 10. [Google Scholar] [CrossRef]
- Wu, I.-P.; Liao, S.-L.; Lai, S.-H.; Wong, K.-S. The Respiratory Impacts of Air Pollution in Children: Global and Domestic (Taiwan) Situation. Biomed. J. 2022, 45, 88–94. [Google Scholar] [CrossRef]
- Kim, J.J. American Academy of Pediatrics Committee on Environmental Health Ambient Air Pollution: Health Hazards to Children. Pediatrics 2004, 114, 1699–1707. [Google Scholar] [CrossRef]
- Bateson, T.F.; Schwartz, J. Children’s Response to Air Pollutants. J. Toxicol. Environ. Health A 2008, 71, 238–243. [Google Scholar] [CrossRef]
- Johnson, N.M.; Hoffmann, A.R.; Behlen, J.C.; Lau, C.; Pendleton, D.; Harvey, N.; Shore, R.; Li, Y.; Chen, J.; Tian, Y.; et al. Air Pollution and Children’s Health-a Review of Adverse Effects Associated with Prenatal Exposure from Fine to Ultrafine Particulate Matter. Environ. Health Prev. Med. 2021, 26, 72. [Google Scholar] [CrossRef]
- Garcia, E.; Rice, M.B.; Gold, D.R. Air Pollution and Lung Function in Children. J. Allergy Clin. Immunol 2021, 148, 1–14. [Google Scholar] [CrossRef]
- Schwartz, J. Air Pollution and Children’s Health. Pediatrics 2004, 113, 1037–1043. [Google Scholar] [CrossRef]
- Leung, S.Y.; Lau, S.Y.F.; Kwok, K.L.; Mohammad, K.N.; Chan, P.K.S.; Chong, K.C. Short-Term Association among Meteorological Variation, Outdoor Air Pollution and Acute Bronchiolitis in Children in a Subtropical Setting. Thorax 2021, 76, 360–369. [Google Scholar] [CrossRef]
- Andersen, Z.J.; Loft, S.; Ketzel, M.; Stage, M.; Scheike, T.; Hermansen, M.N.; Bisgaard, H. Ambient Air Pollution Triggers Wheezing Symptoms in Infants. Thorax 2008, 63, 710–716. [Google Scholar] [CrossRef]
- Johns, D.O.; Linn, W.S. A Review of Controlled Human SO₂ Exposure Studies Contributing to the US EPA Integrated Science Assessment for Sulfur Oxides. Inhal. Toxicol. 2011, 23, 33–43. [Google Scholar] [CrossRef]
- Lelieveld, J.; Evans, J.S.; Fnais, M.; Giannadaki, D.; Pozzer, A. The Contribution of Outdoor Air Pollution Sources to Premature Mortality on a Global Scale. Nature 2015, 525, 367–371. [Google Scholar] [CrossRef]
- Guarnieri, M.; Balmes, J.R. Outdoor Air Pollution and Asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef]
- Fuzzi, S.; Baltensperger, U.; Carslaw, K.; Decesari, S.; Denier van der Gon, H.; Facchini, M.C.; Fowler, D.; Koren, I.; Langford, B.; Lohmann, U.; et al. Particulate Matter, Air Quality and Climate: Lessons Learned and Future Needs. Atmos. Chem. Phys. 2015, 15, 8217–8299. [Google Scholar] [CrossRef]
- Mann, J.K.; Lutzker, L.; Holm, S.M.; Margolis, H.G.; Neophytou, A.M.; Eisen, E.A.; Costello, S.; Tyner, T.; Holland, N.; Tindula, G.; et al. Traffic-Related Air Pollution Is Associated with Glucose Dysregulation, Blood Pressure, and Oxidative Stress in Children. Environ. Res. 2021, 195, 110870. [Google Scholar] [CrossRef]
- Nel, A.; Xia, T.; Mädler, L.; Li, N. Toxic Potential of Materials at the Nanolevel. Science 2006, 311, 622–627. [Google Scholar] [CrossRef]
- Kelly, F.J. Oxidative Stress: Its Role in Air Pollution and Adverse Health Effects. Occup. Environ. Med. 2003, 60, 612–616. [Google Scholar] [CrossRef]
- Shiraiwa, M.; Ueda, K.; Pozzer, A.; Lammel, G.; Kampf, C.J.; Fushimi, A.; Enami, S.; Arangio, A.M.; Fröhlich-Nowoisky, J.; Fujitani, Y.; et al. Aerosol Health Effects from Molecular to Global Scales. Environ. Sci. Technol. 2017, 51, 13545–13567. [Google Scholar] [CrossRef]
- Kelly, F.J.; Fussell, J.C. Size, Source and Chemical Composition as Determinants of Toxicity Attributable to Ambient Particulate Matter. Atmos. Environ. 2012, 60, 504–526. [Google Scholar] [CrossRef]
- Carbone, C.; Decesari, S.; Mircea, M.; Giulianelli, L.; Finessi, E.; Rinaldi, M.; Fuzzi, S.; Marinoni, A.; Duchi, R.; Perrino, C.; et al. Size-Resolved Aerosol Chemical Composition over the Italian Peninsula during Typical Summer and Winter Conditions. Atmos. Environ. 2010, 44, 5269–5278. [Google Scholar] [CrossRef]
- Paglione, M.; Gilardoni, S.; Rinaldi, M.; Decesari, S.; Zanca, N.; Sandrini, S.; Giulianelli, L.; Bacco, D.; Ferrari, S.; Poluzzi, V.; et al. The Impact of Biomass Burning and Aqueous-Phase Processing on Air Quality: A Multi-Year Source Apportionment Study in the Po Valley, Italy. Atmos. Chem. Phys. 2020, 20, 1233–1254. [Google Scholar] [CrossRef]
- Janssen, N.A.H.; Hoek, G.; Simic-Lawson, M.; Fischer, P.; van Bree, L.; ten Brink, H.; Keuken, M.; Atkinson, R.W.; Anderson, H.R.; Brunekreef, B.; et al. Black Carbon as an Additional Indicator of the Adverse Health Effects of Airborne Particles Compared with PM10 and PM2.5. Environ. Health Perspect. 2011, 119, 1691–1699. [Google Scholar] [CrossRef]
- Künzi, L.; Krapf, M.; Daher, N.; Dommen, J.; Jeannet, N.; Schneider, S.; Platt, S.; Slowik, J.G.; Baumlin, N.; Salathe, M.; et al. Toxicity of Aged Gasoline Exhaust Particles to Normal and Diseased Airway Epithelia. Sci. Rep. 2015, 5, 11801. [Google Scholar] [CrossRef]
- Saffari, A.; Daher, N.; Shafer, M.M.; Schauer, J.J.; Sioutas, C. Global Perspective on the Oxidative Potential of Airborne Particulate Matter: A Synthesis of Research Findings. Environ. Sci. Technol. 2014, 48, 7576–7583. [Google Scholar] [CrossRef]
- Ching, J.; Adachi, K.; Zaizen, Y.; Igarashi, Y.; Kajino, M. Aerosol Mixing State Revealed by Transmission Electron Microscopy Pertaining to Cloud Formation and Human Airway Deposition. npj Clim. Atmos. Sci. 2019, 2, 22. [Google Scholar] [CrossRef]
- Li, W.; Shao, L.; Zhang, D.; Ro, C.-U.; Hu, M.; Bi, X.; Geng, H.; Matsuki, A.; Niu, H.; Chen, J. A Review of Single Aerosol Particle Studies in the Atmosphere of East Asia: Morphology, Mixing State, Source, and Heterogeneous Reactions. J. Clean. Prod. 2016, 112, 1330–1349. [Google Scholar] [CrossRef]
- Riemer, N.; Ault, A.P.; West, M.; Craig, R.L.; Curtis, J.H. Aerosol Mixing State: Measurements, Modeling, and Impacts. Rev. Geophys. 2019, 57, 187–249. [Google Scholar] [CrossRef]
- Costabile, F.; Decesari, S.; Vecchi, R.; Lucarelli, F.; Curci, G.; Massabò, D.; Rinaldi, M.; Gualtieri, M.; Corsini, E.; Menegola, E.; et al. On the Redox-Activity and Health-Effects of Atmospheric Primary and Secondary Aerosol: Phenomenology. Atmosphere 2022, 13, 704. [Google Scholar] [CrossRef]
- Health Effects Institute. Systematic Review and Meta-Analysis of Selected Health Effects of Long-Term Exposure to Traffic-Related Air Pollution. Available online: https://www.healtheffects.org/publication/systematic-review-and-meta-analysis-selected-health-effects-long-term-exposure-traffic (accessed on 10 February 2023).
- Robinson, A.L.; Donahue, N.M.; Shrivastava, M.K.; Weitkamp, E.A.; Sage, A.M.; Grieshop, A.P.; Lane, T.E.; Pierce, J.R.; Pandis, S.N. Rethinking Organic Aerosols: Semivolatile Emissions and Photochemical Aging. Science 2007, 315, 1259–1262. [Google Scholar] [CrossRef]
- Daellenbach, K.R.; Uzu, G.; Jiang, J.; Cassagnes, L.-E.; Leni, Z.; Vlachou, A.; Stefenelli, G.; Canonaco, F.; Weber, S.; Segers, A.; et al. Sources of Particulate-Matter Air Pollution and Its Oxidative Potential in Europe. Nature 2020, 587, 414–419. [Google Scholar] [CrossRef]
- Boogaard, H.; Patton, A.P.; Atkinson, R.W.; Brook, J.R.; Chang, H.H.; Crouse, D.L.; Fussell, J.C.; Hoek, G.; Hoffmann, B.; Kappeler, R.; et al. Long-Term Exposure to Traffic-Related Air Pollution and Selected Health Outcomes: A Systematic Review and Meta-Analysis. Environ. Int. 2022, 164, 107262. [Google Scholar] [CrossRef]
- Farzan, S.F.; Habre, R.; Danza, P.; Lurmann, F.; Gauderman, W.J.; Avol, E.; Bastain, T.; Hodis, H.N.; Breton, C. Childhood Traffic-Related Air Pollution and Adverse Changes in Subclinical Atherosclerosis Measures from Childhood to Adulthood. Environ. Health 2021, 20, 44. [Google Scholar] [CrossRef]
- Havet, A.; Li, Z.; Zerimech, F.; Sanchez, M.; Siroux, V.; Le Moual, N.; Brunekreef, B.; Künzli, N.; Jacquemin, B.; Varraso, R.; et al. Does the Oxidative Stress Play a Role in the Associations between Outdoor Air Pollution and Persistent Asthma in Adults? Findings from the EGEA Study. Environ. Health 2019, 18, 90. [Google Scholar] [CrossRef]
- Oliveira, M.; Slezakova, K.; Delerue-Matos, C.; Pereira, M.C.; Morais, S. Children Environmental Exposure to Particulate Matter and Polycyclic Aromatic Hydrocarbons and Biomonitoring in School Environments: A Review on Indoor and Outdoor Exposure Levels, Major Sources and Health Impacts. Environ. Int. 2019, 124, 180–204. [Google Scholar] [CrossRef]
- Salvi, S. Health Effects of Ambient Air Pollution in Children. Paediatr. Respir. Rev. 2007, 8, 275–280. [Google Scholar] [CrossRef]
- Fanucchi, M.V.; Plopper, C.G.; Evans, M.J.; Hyde, D.M.; Van Winkle, L.S.; Gershwin, L.J.; Schelegle, E.S. Cyclic Exposure to Ozone Alters Distal Airway Development in Infant Rhesus Monkeys. Am. J. Physiol. Lung Cell Mol. Physiol. 2006, 291, L644–L650. [Google Scholar] [CrossRef]
- Anderson, J.O.; Thundiyil, J.G.; Stolbach, A. Clearing the Air: A Review of the Effects of Particulate Matter Air Pollution on Human Health. J. Med. Toxicol. 2012, 8, 166–175. [Google Scholar] [CrossRef]
- Lambert, A.L.; Mangum, J.B.; DeLorme, M.P.; Everitt, J.I. Ultrafine Carbon Black Particles Enhance Respiratory Syncytial Virus-Induced Airway Reactivity, Pulmonary Inflammation, and Chemokine Expression. Toxicol. Sci. 2003, 72, 339–346. [Google Scholar] [CrossRef]
- Gangwar, R.S.; Bevan, G.H.; Palanivel, R.; Das, L.; Rajagopalan, S. Oxidative Stress Pathways of Air Pollution Mediated Toxicity: Recent Insights. Redox Biol. 2020, 34, 101545. [Google Scholar] [CrossRef]
- Glencross, D.A.; Ho, T.-R.; Camiña, N.; Hawrylowicz, C.M.; Pfeffer, P.E. Air Pollution and Its Effects on the Immune System. Free Radic. Biol. Med. 2020, 151, 56–68. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; Valencia-Salazar, G.; Rodríguez-Alcaraz, A.; Gambling, T.M.; García, R.; Osnaya, N.; Villarreal-Calderón, A.; Devlin, R.B.; Carson, J.L. Ultrastructural Nasal Pathology in Children Chronically and Sequentially Exposed to Air Pollutants. Am. J. Respir. Cell Mol. Biol. 2001, 24, 132–138. [Google Scholar] [CrossRef]
- Sunil, V.R.; Vayas, K.N.; Massa, C.B.; Gow, A.J.; Laskin, J.D.; Laskin, D.L. Ozone-Induced Injury and Oxidative Stress in Bronchiolar Epithelium Are Associated with Altered Pulmonary Mechanics. Toxicol. Sci. 2013, 133, 309–319. [Google Scholar] [CrossRef]
- Moore, L.D.; Le, T.; Fan, G. DNA Methylation and Its Basic Function. Neuropsychopharmacology 2013, 38, 23–38. [Google Scholar] [CrossRef]
- Suhaimi, N.F.; Jalaludin, J.; Abu Bakar, S. Deoxyribonucleic Acid (DNA) Methylation in Children Exposed to Air Pollution: A Possible Mechanism Underlying Respiratory Health Effects Development. Rev. Environ. Health 2021, 36, 77–93. [Google Scholar] [CrossRef]
- Rider, C.F.; Carlsten, C. Air Pollution and DNA Methylation: Effects of Exposure in Humans. Clin. Epigenetics 2019, 11, 131. [Google Scholar] [CrossRef]
- Gruzieva, O.; Xu, C.-J.; Breton, C.V.; Annesi-Maesano, I.; Antó, J.M.; Auffray, C.; Ballereau, S.; Bellander, T.; Bousquet, J.; Bustamante, M.; et al. Epigenome-Wide Meta-Analysis of Methylation in Children Related to Prenatal NO2 Air Pollution Exposure. Environ. Health Perspect. 2017, 125, 104–110. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Hossein-Nezhad, A.; Adabi, E.; Asadollah-Pour, E.; Sadeghi, M.; Mohammad-Nabi, S.; Zakeri Rad, L.; Malek Hosseini, A.-A.; Radmehr, M.; Faghihi, F.; et al. Air Pollution during Pregnancy and Placental Adaptation in the Levels of Global DNA Methylation. PLoS ONE 2018, 13, e0199772. [Google Scholar] [CrossRef]
- Cai, J.; Zhao, Y.; Liu, P.; Xia, B.; Zhu, Q.; Wang, X.; Song, Q.; Kan, H.; Zhang, Y. Exposure to Particulate Air Pollution during Early Pregnancy Is Associated with Placental DNA Methylation. Sci. Total Environ. 2017, 607–608, 1103–1108. [Google Scholar] [CrossRef]
- Janssen, B.G.; Godderis, L.; Pieters, N.; Poels, K.; Kiciński, M.; Cuypers, A.; Fierens, F.; Penders, J.; Plusquin, M.; Gyselaers, W.; et al. Placental DNA Hypomethylation in Association with Particulate Air Pollution in Early Life. Part. Fibre Toxicol. 2013, 10, 22. [Google Scholar] [CrossRef]
- Isaevska, E.; Moccia, C.; Asta, F.; Cibella, F.; Gagliardi, L.; Ronfani, L.; Rusconi, F.; Stazi, M.A.; Richiardi, L. Exposure to Ambient Air Pollution in the First 1000 Days of Life and Alterations in the DNA Methylome and Telomere Length in Children: A Systematic Review. Environ. Res. 2021, 193, 110504. [Google Scholar] [CrossRef]
- Veras, M.M.; de Oliveira Alves, N.; Fajersztajn, L.; Saldiva, P. Before the First Breath: Prenatal Exposures to Air Pollution and Lung Development. Cell Tissue Res. 2017, 367, 445–455. [Google Scholar] [CrossRef]
- Liu, J.; Ballaney, M.; Al-alem, U.; Quan, C.; Jin, X.; Perera, F.; Chen, L.-C.; Miller, R.L. Combined Inhaled Diesel Exhaust Particles and Allergen Exposure Alter Methylation of T Helper Genes and IgE Production in Vivo. Toxicol. Sci. 2008, 102, 76–81. [Google Scholar] [CrossRef]
- Makrinioti, H.; Camargo, C.A.; Zhu, Z.; Freishtat, R.J.; Hasegawa, K. Air Pollution, Bronchiolitis, and Asthma: The Role of Nasal MicroRNAs. Lancet Respir. Med. 2022, 10, 733–734. [Google Scholar] [CrossRef]
- Ji, H.; Biagini Myers, J.M.; Brandt, E.B.; Brokamp, C.; Ryan, P.H.; Khurana Hershey, G.K. Air Pollution, Epigenetics, and Asthma. Allergy Asthma Clin. Immunol. 2016, 12, 51. [Google Scholar] [CrossRef]
- Lin, W.-W.; Chen, Z.-X.; Kong, M.-L.; Xie, Y.-Q.; Zeng, X.-W. Air Pollution and Children’s Health in Chinese. Adv. Exp. Med. Biol. 2017, 1017, 153–180. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for Europe & European Centre for Environment and Health. Effects of Air Pollution on Children’s Health and Development: A Review of the Evidence; WHO Regional Office for Europe: Copenhagen, Denmark, 2005. [Google Scholar]
- Morales, E.; Garcia-Esteban, R.; de la Cruz, O.A.; Basterrechea, M.; Lertxundi, A.; de Dicastillo, M.D.M.L.; Zabaleta, C.; Sunyer, J. Intrauterine and Early Postnatal Exposure to Outdoor Air Pollution and Lung Function at Preschool Age. Thorax 2015, 70, 64–73. [Google Scholar] [CrossRef]
- Evangelisti, M.; Cangiano, G.; Nenna, R.; Nicolai, A.; Frassanito, A.; Papasso, S.; Alessandroni, C.; Mario, C.D.; Zambonini, V.; Mattia, G.D.; et al. Air Pollution and Bronchiolitis from 2004 to 2014 in Rome. Eur. Respir. J. 2015, 46, PA4505. [Google Scholar] [CrossRef]
- Loaiza-Ceballos, M.C.; Marin-Palma, D.; Zapata, W.; Hernandez, J.C. Viral Respiratory Infections and Air Pollutants. Air Qual. Atmos. Health 2022, 15, 105–114. [Google Scholar] [CrossRef]
- Milani, G.P.; Cafora, M.; Favero, C.; Luganini, A.; Carugno, M.; Lenzi, E.; Pistocchi, A.; Pinatel, E.; Pariota, L.; Ferrari, L.; et al. PM2.5, PM10 and Bronchiolitis Severity: A Cohort Study. Pediatr. Allergy Immunol. 2022, 33, e13853. [Google Scholar] [CrossRef]
- Nenna, R.; Evangelisti, M.; Frassanito, A.; Scagnolari, C.; Pierangeli, A.; Antonelli, G.; Nicolai, A.; Arima, S.; Moretti, C.; Papoff, P.; et al. Respiratory Syncytial Virus Bronchiolitis, Weather Conditions and Air Pollution in an Italian Urban Area: An Observational Study. Environ. Res. 2017, 158, 188–193. [Google Scholar] [CrossRef]
- Carugno, M.; Dentali, F.; Mathieu, G.; Fontanella, A.; Mariani, J.; Bordini, L.; Milani, G.P.; Consonni, D.; Bonzini, M.; Bollati, V.; et al. PM10 Exposure Is Associated with Increased Hospitalizations for Respiratory Syncytial Virus Bronchiolitis among Infants in Lombardy, Italy. Environ. Res. 2018, 166, 452–457. [Google Scholar] [CrossRef]
- Aguilera, I.; Pedersen, M.; Garcia-Esteban, R.; Ballester, F.; Basterrechea, M.; Esplugues, A.; Fernández-Somoano, A.; Lertxundi, A.; Tardón, A.; Sunyer, J. Early-Life Exposure to Outdoor Air Pollution and Respiratory Health, Ear Infections, and Eczema in Infants from the INMA Study. Environ. Health Perspect. 2013, 121, 387–392. [Google Scholar] [CrossRef]
- Li, H.; Li, X.; Zheng, H.; Liu, L.; Wu, Y.; Zhou, Y.; Meng, X.; Hong, J.; Cao, L.; Lu, Y.; et al. Ultrafine Particulate Air Pollution and Pediatric Emergency-Department Visits for Main Respiratory Diseases in Shanghai, China. Sci. Total Environ. 2021, 775, 145777. [Google Scholar] [CrossRef]
- White, M.C.; Etzel, R.A.; Wilcox, W.D.; Lloyd, C. Exacerbations of Childhood Asthma and Ozone Pollution in Atlanta. Environ. Res. 1994, 65, 56–68. [Google Scholar] [CrossRef]
- Smargiassi, A.; Kosatsky, T.; Hicks, J.; Plante, C.; Armstrong, B.; Villeneuve, P.J.; Goudreau, S. Risk of Asthmatic Episodes in Children Exposed to Sulfur Dioxide Stack Emissions from a Refinery Point Source in Montreal, Canada. Environ. Health Perspect. 2009, 117, 653–659. [Google Scholar] [CrossRef]
- Gaffin, J.M.; Hauptman, M.; Petty, C.R.; Sheehan, W.J.; Lai, P.S.; Wolfson, J.M.; Gold, D.R.; Coull, B.A.; Koutrakis, P.; Phipatanakul, W. Nitrogen Dioxide Exposure in School Classrooms of Inner-City Children with Asthma. J. Allergy Clin. Immunol. 2018, 141, 2249–2255.e2. [Google Scholar] [CrossRef]
- Bowatte, G.; Lodge, C.; Lowe, A.J.; Erbas, B.; Perret, J.; Abramson, M.J.; Matheson, M.; Dharmage, S.C. The Influence of Childhood Traffic-Related Air Pollution Exposure on Asthma, Allergy and Sensitization: A Systematic Review and a Meta-Analysis of Birth Cohort Studies. Allergy 2015, 70, 245–256. [Google Scholar] [CrossRef]
- Mölter, A.; Agius, R.M.; de Vocht, F.; Lindley, S.; Gerrard, W.; Lowe, L.; Belgrave, D.; Custovic, A.; Simpson, A. Long-Term Exposure to PM10 and NO2 in Association with Lung Volume and Airway Resistance in the MAAS Birth Cohort. Environ. Health Perspect. 2013, 121, 1232–1238. [Google Scholar] [CrossRef]
- EPA. Integrated Science Assessment (ISA) for Particulate Matter. Available online: https://www.epa.gov/isa/integrated-science-assessment-isa-particulate-matter (accessed on 5 January 2023).
- Latzin, P.; Röösli, M.; Huss, A.; Kuehni, C.E.; Frey, U. Air Pollution during Pregnancy and Lung Function in Newborns: A Birth Cohort Study. Eur. Respir. J. 2009, 33, 594–603. [Google Scholar] [CrossRef]
- Darrow, L.A.; Klein, M.; Flanders, W.D.; Mulholland, J.A.; Tolbert, P.E.; Strickland, M.J. Air Pollution and Acute Respiratory Infections among Children 0–4 Years of Age: An 18-Year Time-Series Study. Am. J. Epidemiol. 2014, 180, 968–977. [Google Scholar] [CrossRef]
- Glick, A.F.; Tomopoulos, S.; Fierman, A.H.; Elixhauser, A.; Trasande, L. Association Between Outdoor Air Pollution Levels and Inpatient Outcomes in Pediatric Pneumonia Hospitalizations, 2007 to 2008. Acad. Pediatr. 2019, 19, 414–420. [Google Scholar] [CrossRef]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R.; Lucas, K.; Nieuwenhuijsen, M. Exposure to Traffic-Related Air Pollution and Risk of Development of Childhood Asthma: A Systematic Review and Meta-Analysis. Environ. Int. 2017, 100, 1–31. [Google Scholar] [CrossRef]
- Lavigne, E.; Donelle, J.; Hatzopoulou, M.; Van Ryswyk, K.; van Donkelaar, A.; Martin, R.V.; Chen, H.; Stieb, D.M.; Gasparrini, A.; Crighton, E.; et al. Spatiotemporal Variations in Ambient Ultrafine Particles and the Incidence of Childhood Asthma. Am. J. Respir. Crit. Care Med. 2019, 199, 1487–1495. [Google Scholar] [CrossRef]
- Wang, P.; You, D.; Saravia, J.; Shen, H.; Cormier, S.A. Maternal Exposure to Combustion Generated PM Inhibits Pulmonary Th1 Maturation and Concomitantly Enhances Postnatal Asthma Development in Offspring. Part. Fibre Toxicol. 2013, 10, 29. [Google Scholar] [CrossRef]
- Zhang, Y.; Wei, J.; Shi, Y.; Quan, C.; Ho, H.C.; Song, Y.; Zhang, L. Early-Life Exposure to Submicron Particulate Air Pollution in Relation to Asthma Development in Chinese Preschool Children. J. Allergy Clin. Immunol. 2021, 148, 771–782.e12. [Google Scholar] [CrossRef]
- Peden, D.B. Prenatal Exposure to Particulate Matter Air Pollution: A Preventable Risk for Childhood Asthma. J. Allergy Clin. Immunol. 2021, 148, 716–718. [Google Scholar] [CrossRef]
- Liu, F.; Zhang, Z.; Chen, H.; Nie, S. Associations of Ambient Air Pollutants with Regional Pulmonary Tuberculosis Incidence in the Central Chinese Province of Hubei: A Bayesian Spatial-Temporal Analysis. Environ. Health 2020, 19, 51. [Google Scholar] [CrossRef]
- Bui, D.S.; Burgess, J.A.; Lowe, A.J.; Perret, J.L.; Lodge, C.J.; Bui, M.; Morrison, S.; Thompson, B.R.; Thomas, P.S.; Giles, G.G.; et al. Childhood Lung Function Predicts Adult Chronic Obstructive Pulmonary Disease and Asthma-Chronic Obstructive Pulmonary Disease Overlap Syndrome. Am. J. Respir. Crit. Care Med. 2017, 196, 39–46. [Google Scholar] [CrossRef]
- Stocks, J.; Hislop, A.; Sonnappa, S. Early Lung Development: Lifelong Effect on Respiratory Health and Disease. Lancet Respir. Med. 2013, 1, 728–742. [Google Scholar] [CrossRef]
- Soriano, J.B.; Polverino, F.; Cosio, B.G. What Is Early COPD and Why Is It Important? Eur. Respir. J. 2018, 52, 1801448. [Google Scholar] [CrossRef]
- Deng, Q.; Lu, C.; Yu, Y.; Li, Y.; Sundell, J.; Norbäck, D. Early Life Exposure to Traffic-Related Air Pollution and Allergic Rhinitis in Preschool Children. Respir. Med. 2016, 121, 67–73. [Google Scholar] [CrossRef]
- Li, C.H.; Sayeau, K.; Ellis, A.K. Air Pollution and Allergic Rhinitis: Role in Symptom Exacerbation and Strategies for Management. J. Asthma Allergy 2020, 13, 285–292. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Y.; Dong, J.; Wang, J.; Bao, H.; Zhai, G. Association between Air Pollution and Emergency Department Visits for Upper Respiratory Tract Infection in Lanzhou, China. Environ. Sci. Pollut. Res. Int. 2022, 29, 28816–28828. [Google Scholar] [CrossRef]
- Toskala, E.; Kennedy, D.W. Asthma Risk Factors. Int. Forum Allergy Rhinol. 2015, 5 (Suppl. S1), S11–S16. [Google Scholar] [CrossRef]
- Jung, K.H.; Hsu, S.-I.; Yan, B.; Moors, K.; Chillrud, S.N.; Ross, J.; Wang, S.; Perzanowski, M.S.; Kinney, P.L.; Whyatt, R.M.; et al. Childhood Exposure to Fine Particulate Matter and Black Carbon and the Development of New Wheeze Between Ages 5 and 7 In an Urban Prospective Cohort. Environ. Int. 2012, 45, 44–50. [Google Scholar] [CrossRef]
- Liu, L.; Poon, R.; Chen, L.; Frescura, A.-M.; Montuschi, P.; Ciabattoni, G.; Wheeler, A.; Dales, R. Acute Effects of Air Pollution on Pulmonary Function, Airway Inflammation, and Oxidative Stress in Asthmatic Children. Environ. Health Perspect. 2009, 117, 668–674. [Google Scholar] [CrossRef]
- Fuertes, E.; Heinrich, J. The Influence of Childhood Traffic-Related Air Pollution Exposure on Asthma, Allergy and Sensitization. Allergy 2015, 70, 1350–1352. [Google Scholar] [CrossRef]
- Brumberg, H.L.; Karr, C.J. Council on Environmental Health Ambient Air Pollution: Health Hazards to Children. Pediatrics 2021, 147, e2021051484. [Google Scholar] [CrossRef]
- Dondi, A.; Betti, L.; Carbone, C.; Dormi, A.; Paglione, M.; Rinaldi, M.; Gualtieri, M.; Scotto, F.; Poluzzi, V.; Fabi, M.; et al. Understanding the Environmental Factors Related to the Decrease in Pediatric Emergency Department Referrals for Acute Asthma during the SARS-CoV-2 Pandemic. Pediatr. Pulmonol. 2022, 57, 66–74. [Google Scholar] [CrossRef]
- Li, Y.; Wang, W.; Wang, J.; Zhang, X.; Lin, W.; Yang, Y. Impact of Air Pollution Control Measures and Weather Conditions on Asthma during the 2008 Summer Olympic Games in Beijing. Int. J. Biometeorol. 2011, 55, 547–554. [Google Scholar] [CrossRef]
- Baraldi, E.; Lanari, M.; Manzoni, P.; Rossi, G.A.; Vandini, S.; Rimini, A.; Romagnoli, C.; Colonna, P.; Biondi, A.; Biban, P.; et al. Inter-Society Consensus Document on Treatment and Prevention of Bronchiolitis in Newborns and Infants. Ital. J. Pediatr. 2014, 40, 65. [Google Scholar] [CrossRef]
- Silver, A.H.; Nazif, J.M. Bronchiolitis. Pediatr. Rev. 2019, 40, 568–576. [Google Scholar] [CrossRef]
- Karr, C.; Lumley, T.; Schreuder, A.; Davis, R.; Larson, T.; Ritz, B.; Kaufman, J. Effects of Subchronic and Chronic Exposure to Ambient Air Pollutants on Infant Bronchiolitis. Am. J. Epidemiol. 2007, 165, 553–560. [Google Scholar] [CrossRef]
- Jedrychowski, W.A.; Perera, F.P.; Spengler, J.D.; Mroz, E.; Stigter, L.; Flak, E.; Majewska, R.; Klimaszewska-Rembiasz, M.; Jacek, R. Intrauterine Exposure to Fine Particulate Matter as a Risk Factor for Increased Susceptibility to Acute Broncho-Pulmonary Infections in Early Childhood. Int. J. Hyg. Environ. Health 2013, 216, 395–401. [Google Scholar] [CrossRef]
- Gouveia, N.; Fletcher, T. Respiratory Diseases in Children and Outdoor Air Pollution in São Paulo, Brazil: A Time Series Analysis. Occup. Environ. Med. 2000, 57, 477–483. [Google Scholar] [CrossRef]
- Brugha, R.; Grigg, J. Urban Air Pollution and Respiratory Infections. Paediatr. Respir. Rev. 2014, 15, 194–199. [Google Scholar] [CrossRef]
- Esplugues, A.; Ballester, F.; Estarlich, M.; Llop, S.; Fuentes-Leonarte, V.; Mantilla, E.; Vioque, J.; Iñiguez, C. Outdoor, but Not Indoor, Nitrogen Dioxide Exposure Is Associated with Persistent Cough during the First Year of Life. Sci. Total Environ. 2011, 409, 4667–4673. [Google Scholar] [CrossRef]
- Gehring, U.; Gruzieva, O.; Agius, R.M.; Beelen, R.; Custovic, A.; Cyrys, J.; Eeftens, M.; Flexeder, C.; Fuertes, E.; Heinrich, J.; et al. Air Pollution Exposure and Lung Function in Children: The ESCAPE Project. Environ. Health Perspect. 2013, 121, 1357–1364. [Google Scholar] [CrossRef]
- Suryadhi, M.A.H.; Abudureyimu, K.; Kashima, S.; Yorifuji, T. Nitrogen Dioxide and Acute Respiratory Tract Infections in Children in Indonesia. Arch. Environ. Occup. Health 2020, 75, 274–280. [Google Scholar] [CrossRef]
- Grigg, J. Air Pollution and Children’s Respiratory Health—Gaps in the Global Evidence. Clin. Exp. Allergy 2011, 41, 1072–1075. [Google Scholar] [CrossRef]
- Mishra, R.; Krishnamoorthy, P.; Gangamma, S.; Raut, A.A.; Kumar, H. Particulate Matter (PM10) Enhances RNA Virus Infection through Modulation of Innate Immune Responses. Environ. Pollut. 2020, 266, 115148. [Google Scholar] [CrossRef]
- Cole, M.A.; Ozgen, C.; Strobl, E. Air Pollution Exposure and COVID-19 in Dutch Municipalities. Environ. Resour. Econ. 2020, 76, 581–610. [Google Scholar] [CrossRef]
- Wu, X.; Nethery, R.C.; Sabath, B.M.; Braun, D.; Dominici, F. Exposure to Air Pollution and COVID-19 Mortality in the United States: A Nationwide Cross-Sectional Study. medRxiv 2020. [Google Scholar] [CrossRef]
- Travaglio, M.; Yu, Y.; Popovic, R.; Selley, L.; Leal, N.S.; Martins, L.M. Links between Air Pollution and COVID-19 in England. Environ. Pollut. 2021, 268, 115859. [Google Scholar] [CrossRef]
- Contini, D.; Costabile, F. Does Air Pollution Influence COVID-19 Outbreaks? Atmosphere 2020, 11, 377. [Google Scholar] [CrossRef]
- McGeachie, M.J.; Yates, K.P.; Zhou, X.; Guo, F.; Sternberg, A.L.; Van Natta, M.L.; Wise, R.A.; Szefler, S.J.; Sharma, S.; Kho, A.T.; et al. Patterns of Growth and Decline in Lung Function in Persistent Childhood Asthma. N. Engl. J. Med. 2016, 374, 1842–1852. [Google Scholar] [CrossRef]
- Gauderman, W.J.; Avol, E.; Gilliland, F.; Vora, H.; Thomas, D.; Berhane, K.; McConnell, R.; Kuenzli, N.; Lurmann, F.; Rappaport, E.; et al. The Effect of Air Pollution on Lung Development from 10 to 18 Years of Age. N. Engl. J. Med. 2004, 351, 1057–1067. [Google Scholar] [CrossRef]
- de Barros Mendes Lopes, T.; Groth, E.E.; Veras, M.; Furuya, T.K.; de Souza Xavier Costa, N.; Ribeiro Júnior, G.; Lopes, F.D.; de Almeida, F.M.; Cardoso, W.V.; Saldiva, P.H.N.; et al. Pre- and Postnatal Exposure of Mice to Concentrated Urban PM2.5 Decreases the Number of Alveoli and Leads to Altered Lung Function at an Early Stage of Life. Environ. Pollut. 2018, 241, 511–520. [Google Scholar] [CrossRef]
- Cai, Y.; Hansell, A.L.; Granell, R.; Blangiardo, M.; Zottoli, M.; Fecht, D.; Gulliver, J.; Henderson, A.J.; Elliott, P. Prenatal, Early-Life, and Childhood Exposure to Air Pollution and Lung Function: The ALSPAC Cohort. Am. J. Respir. Crit. Care Med. 2020, 202, 112–123. [Google Scholar] [CrossRef]
- Schultz, E.S.; Hallberg, J.; Bellander, T.; Bergström, A.; Bottai, M.; Chiesa, F.; Gustafsson, P.M.; Gruzieva, O.; Thunqvist, P.; Pershagen, G.; et al. Early-Life Exposure to Traffic-Related Air Pollution and Lung Function in Adolescence. Am. J. Respir. Crit. Care Med. 2016, 193, 171–177. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Maugeri, U.; Jedrychowska-Bianchi, I. Body Growth Rate in Preadolescent Children and Outdoor Air Quality. Environ. Res. 2002, 90, 12–20. [Google Scholar] [CrossRef]
- Lu, C.; Peng, W.; Kuang, J.; Wu, M.; Wu, H.; Murithi, R.G.; Johnson, M.B.; Zheng, X. Preconceptional and Prenatal Exposure to Air Pollution Increases Incidence of Childhood Pneumonia: A Hypothesis of the (Pre-)Fetal Origin of Childhood Pneumonia. Ecotoxicol. Environ. Saf. 2021, 210, 111860. [Google Scholar] [CrossRef]
- Usemann, J.; Decrue, F.; Korten, I.; Proietti, E.; Gorlanova, O.; Vienneau, D.; Fuchs, O.; Latzin, P.; Röösli, M.; Frey, U.; et al. Exposure to Moderate Air Pollution and Associations with Lung Function at School-Age: A Birth Cohort Study. Environ. Int. 2019, 126, 682–689. [Google Scholar] [CrossRef]
- He, B.; Huang, J.V.; Kwok, M.K.; Au Yeung, S.L.; Hui, L.L.; Li, A.M.; Leung, G.M.; Schooling, C.M. The Association of Early-Life Exposure to Air Pollution with Lung Function at ~17.5 years in the “Children of 1997” Hong Kong Chinese Birth Cohort. Environ. Int. 2019, 123, 444–450. [Google Scholar] [CrossRef]
- Agusti, A.; Faner, R. Lung Function Trajectories in Health and Disease. Lancet Respir. Med. 2019, 7, 358–364. [Google Scholar] [CrossRef]
- Parker, J.D.; Rich, D.Q.; Glinianaia, S.V.; Leem, J.H.; Wartenberg, D.; Bell, M.L.; Bonzini, M.; Brauer, M.; Darrow, L.; Gehring, U.; et al. The International Collaboration on Air Pollution and Pregnancy Outcomes: Initial Results. Environ. Health Perspect. 2011, 119, 1023–1028. [Google Scholar] [CrossRef]
- Li, C.; Yang, M.; Zhu, Z.; Sun, S.; Zhang, Q.; Cao, J.; Ding, R. Maternal Exposure to Air Pollution and the Risk of Low Birth Weight: A Meta-Analysis of Cohort Studies. Environ. Res. 2020, 190, 109970. [Google Scholar] [CrossRef]
- Liu, Y.; Xu, J.; Chen, D.; Sun, P.; Ma, X. The Association between Air Pollution and Preterm Birth and Low Birth Weight in Guangdong, China. BMC Public Health 2019, 19, 3. [Google Scholar] [CrossRef]
- Chen, Q.; Ren, Z.; Liu, Y.; Qiu, Y.; Yang, H.; Zhou, Y.; Wang, X.; Jiao, K.; Liao, J.; Ma, L. The Association between Preterm Birth and Ambient Air Pollution Exposure in Shiyan, China, 2015–2017. Int. J. Environ. Res. Public Health 2021, 18, 4326. [Google Scholar] [CrossRef]
- MacIntyre, E.A.; Gehring, U.; Mölter, A.; Fuertes, E.; Klümper, C.; Krämer, U.; Quass, U.; Hoffmann, B.; Gascon, M.; Brunekreef, B.; et al. Air Pollution and Respiratory Infections during Early Childhood: An Analysis of 10 European Birth Cohorts within the ESCAPE Project. Environ. Health Perspect. 2014, 122, 107–113. [Google Scholar] [CrossRef]
- Gauderman, W.J.; Urman, R.; Avol, E.; Berhane, K.; McConnell, R.; Rappaport, E.; Chang, R.; Lurmann, F.; Gilliland, F. Association of Improved Air Quality with Lung Development in Children. N. Engl. J. Med. 2015, 372, 905–913. [Google Scholar] [CrossRef]
- Huang, Y.-C.T. Outdoor Air Pollution: A Global Perspective. J. Occup. Environ. Med. 2014, 56, S3. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Fuller, R. Environmental Pollution: An Enormous and Invisible Burden on Health Systems in Low- and Middle-Income Counties. World Hosp. Health Serv. 2014, 50, 35–40. [Google Scholar]
- Carlsten, C.; Salvi, S.; Wong, G.W.K.; Chung, K.F. Personal Strategies to Minimise Effects of Air Pollution on Respiratory Health: Advice for Providers, Patients and the Public. Eur. Respir. J. 2020, 55, 1902056. [Google Scholar] [CrossRef] [PubMed]
- Csavina, J.; Field, J.; Félix, O.; Corral-Avitia, A.Y.; Sáez, A.E.; Betterton, E.A. Effect of Wind Speed and Relative Humidity on Atmospheric Dust Concentrations in Semi-Arid Climates. Sci. Total Environ. 2014, 487, 82–90. [Google Scholar] [CrossRef]
- Tian, G.; Qiao, Z.; Xu, X. Characteristics of Particulate Matter (PM10) and Its Relationship with Meteorological Factors during 2001–2012 in Beijing. Environ. Pollut. 2014, 192, 266–274. [Google Scholar] [CrossRef]
- Li, L.; Qian, J.; Ou, C.-Q.; Zhou, Y.-X.; Guo, C.; Guo, Y. Spatial and Temporal Analysis of Air Pollution Index and Its Timescale-Dependent Relationship with Meteorological Factors in Guangzhou, China, 2001–2011. Environ. Pollut. 2014, 190, 75–81. [Google Scholar] [CrossRef]
- Zanobetti, A.; Peters, A. Disentangling Interactions between Atmospheric Pollution and Weather. J. Epidemiol. Community Health 2015, 69, 613–615. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Innate Immune System | Epithelial cells | ↑ Pro-inflammatory cytokines: IL-1, IL-6, TNFα, GMCSF (O3, NO2, PM) ↑ ICAM-1 expression (NO2) ↑ Leukotriene C4 (NO2) |
| Monocytes/Macrophages | ↑ Carbon loading; ↓ Clearance capacity and phagocytosis; ↑ Pro-inflammatory cytokine (PM) | |
| Neutrophils | ↑ Migration and activation (PM, O3, NO2) | |
| Eosinophils | ↑ Migration and activation (SO2, PM2.5) | |
| Adaptive Immune System | Immune tolerance | ↓ T reg function; neo-antigens (ROS); ↑ antigens immunogenicity (PM); ↑ immunogenicity of antigens (PM) |
| B cells | ↓ IgA and ↑ IgE (PM2.5) | |
| T cells | ↓ Th1 and ↑ Th2 (NO2, PM); ↑ Th17 response (PM); Dysregulated IFN-gamma and IL-17A production (PM) |
| Prenatal Exposure | Short Term Exposure | Long Term Exposure |
|---|---|---|
| Reduced lung function and growth (TRAP, NO2, PM10, PM2.5) [61,67] |
PM2.5 [68,71], PM10 [69,72] | Reduced lung function (NO2, O3) [16] |
| Increased risk of Respiratory Tract Infection (NO2) [73] | Asthma exacerbation (UFPs [74], O3 [75], SO2 [76], NO2 [77], TRAP [78], BC [78], PM2.5 [78]) | Reduced lung growth (PM2.5, PM10, NO2) [79,80] |
| Airway inflammation (NO2) [81] Higher ventilatory demand (PM10) [81] |
| Chronic Asthma (PM2.5, TRAP) [78,84] |
| Increased incidence of asthma (UFPs [85], PM0.1, PM1, PM2.5) [86,87,88] | Tuberculosis (PM10, SO2, NO2) [89] | COPD [90,91,92] |
| Allergic rhinitis (TRAP [93], NO2 [94]) | Upper Respiratory Tract Infection (UFPs [74], PM2.5 [95], PM10 [95], SO2 [95], NO2 [95], CO [95]) | Allergic rhinitis (TRAP [93], PM10 [93], SO2 [94], NO2 [93]) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dondi, A.; Carbone, C.; Manieri, E.; Zama, D.; Del Bono, C.; Betti, L.; Biagi, C.; Lanari, M. Outdoor Air Pollution and Childhood Respiratory Disease: The Role of Oxidative Stress. Int. J. Mol. Sci. 2023, 24, 4345. https://doi.org/10.3390/ijms24054345
Dondi A, Carbone C, Manieri E, Zama D, Del Bono C, Betti L, Biagi C, Lanari M. Outdoor Air Pollution and Childhood Respiratory Disease: The Role of Oxidative Stress. International Journal of Molecular Sciences. 2023; 24(5):4345. https://doi.org/10.3390/ijms24054345
Chicago/Turabian StyleDondi, Arianna, Claudio Carbone, Elisa Manieri, Daniele Zama, Chiara Del Bono, Ludovica Betti, Carlotta Biagi, and Marcello Lanari. 2023. "Outdoor Air Pollution and Childhood Respiratory Disease: The Role of Oxidative Stress" International Journal of Molecular Sciences 24, no. 5: 4345. https://doi.org/10.3390/ijms24054345
APA StyleDondi, A., Carbone, C., Manieri, E., Zama, D., Del Bono, C., Betti, L., Biagi, C., & Lanari, M. (2023). Outdoor Air Pollution and Childhood Respiratory Disease: The Role of Oxidative Stress. International Journal of Molecular Sciences, 24(5), 4345. https://doi.org/10.3390/ijms24054345