
Molecular and Biologic Effects of Platelet-Rich Plasma (PRP) in Ligament and Tendon Healing and Regeneration: A Systematic Review


Abstract
1. Introduction
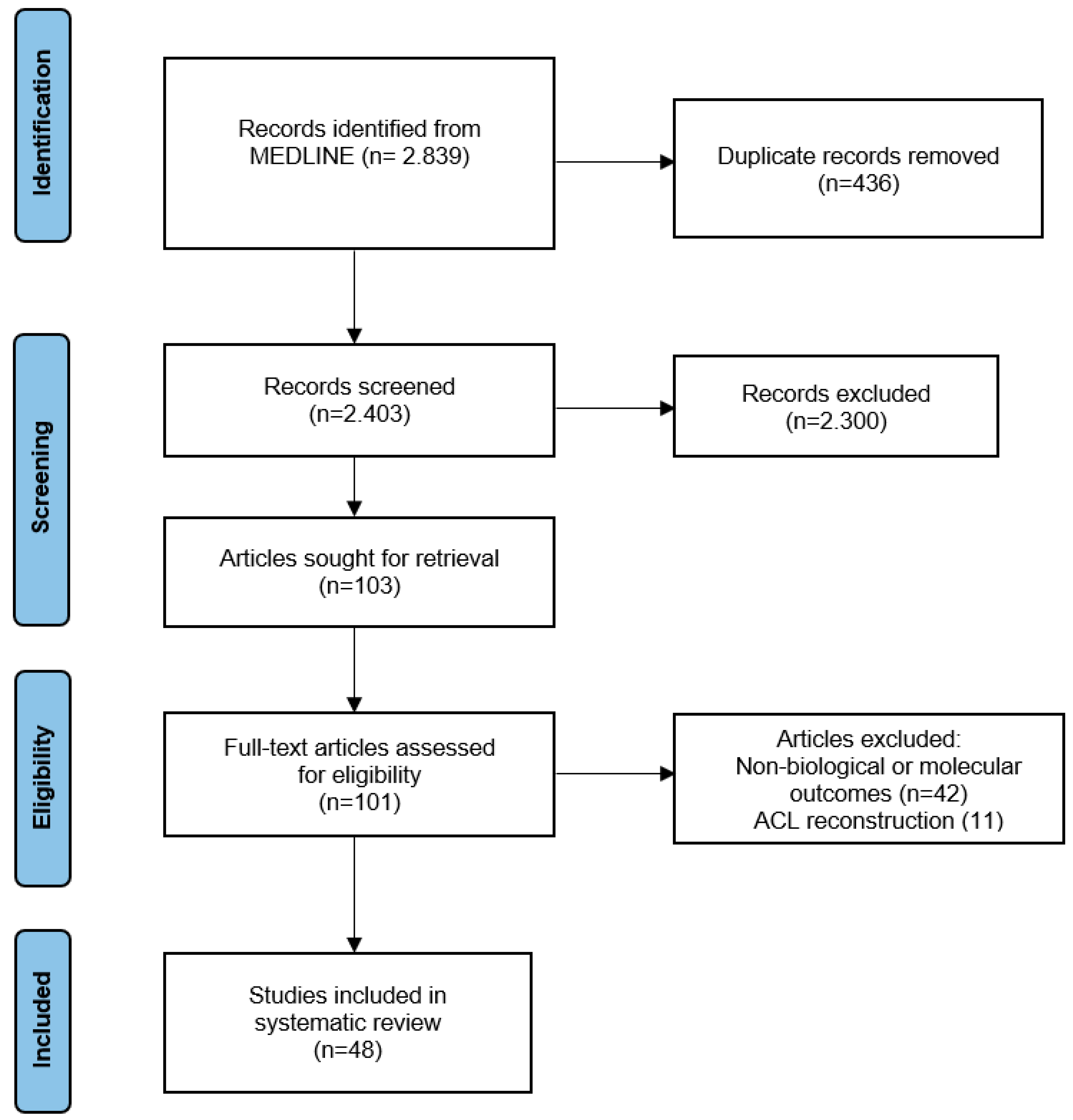
2. Materials and Methods
3. Results
3.1. Effect of PRP on Ligament Tissue
3.1.1. In Vitro Studies
Animal Studies
Human Studies
3.1.2. In Vivo Studies
Animal Studies
3.2. Effect of PRP on Tendon Structure
3.2.1. In Vitro Studies
Animal Studies
Human Studies
3.2.2. In Vivo Studies
Animal Studies
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACL | Anterior cruciate ligament |
| ARG | Arginase |
| BMA | Bone marrow aspirate |
| BMP | Bone morphogenetic protein |
| CCL | Chemokine (C-C motif) ligand |
| CD | Cluster of differentiation |
| COL | Collagen |
| COMP | Cartilage oligomeric matrix protein |
| Cox | Cyclooxygenase |
| CTGF | Connective tissue growth factor |
| ECM | Extracellular matrix |
| EGF | Epidermal growth factor |
| EGR | Early growth response protein |
| FGF | Fibroblast growth factor |
| HAS | Hyaluronan synthase |
| HGF | Hepatocyte growth factor |
| HMGB | High-mobility group box |
| IGF | Insulin-like growth factor |
| IL | Interleukin |
| LOX | Lipoxygenase |
| LP-PRP | Leukocyte poor platelet rich plasma |
| LR-PRP | Leukocyte rich platelet rich plasma |
| LTMI | Ligament tissue maturity index |
| MCL | Medial collateral ligament |
| MMP | Matrix metalloproteinase |
| PAR | Proteinase-activated receptor |
| PBMC | Peripheral blood mononuclear cells |
| PDGF | Platelet-derived growth factor |
| PPP | Platelet poor plasma |
| PRP | Platelet rich plasma |
| Runx2 | Runt-related transcription factor 2 |
| SCX | Scleraxis |
| SOD | Superoxide dismutase |
| TGF | Transforming growth factor |
| TIMP | Tissue inhibitor of metalloproteinases |
| TLR-4 | Toll-like receptor 4 |
| TNC | Tenascin C |
| TNMD | Tenomodulin |
| TSP-1 | Thrombospondin-1 |
| VEGF | Vascular endothelial growth factor |
| vWF | von Willebrand factor |
References
- Kjaer, M.; Langberg, H.; Heinemeier, K.; Bayer, M.L.; Hansen, M.; Holm, L.; Doessing, S.; Kongsgaard, M.; Krogsgaard, M.R.; Magnusson, S.P. From mechanical loading to collagen synthesis, structural changes and function in human tendon. Scand. J. Med. Sci. Sport 2009, 19, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Frank, C.B. Ligament structure, physiology and function. J. Musculoskelet. Neuronal Interact. 2004, 4, 199–201. [Google Scholar] [PubMed]
- Thorpe, C.T.; Screen, H.R. Tendon Structure and Composition. Adv. Exp. Med. Biol. 2016, 920, 3–10. [Google Scholar] [PubMed]
- Mienaltowski, M.J.; Birk, D.E. Structure, physiology, and biochemistry of collagens. Adv. Exp. Med. Biol. 2014, 802, 5–29. [Google Scholar] [PubMed]
- Wang, J.H.; Guo, Q.; Li, B. Tendon biomechanics and mechanobiology—A minireview of basic concepts and recent advancements. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 2012, 25, 133–141. [Google Scholar] [CrossRef]
- Yoon, J.H.; Halper, J. Tendon proteoglycans: Biochemistry and function. J. Musculoskelet. Neuronal Interact. 2005, 5, 22–34. [Google Scholar]
- Thorpe, C.T.; Birch, H.L.; Clegg, P.D.; Screen, H.R. The role of the non-collagenous matrix in tendon function. Int. J. Exp. Pathol. 2013, 94, 248–259. [Google Scholar] [CrossRef]
- Tang, Y.; Wang, Z.; Xiang, L.; Zhao, Z.; Cui, W. Functional biomaterials for tendon/ligament repair and regeneration. Regen. Biomater. 2022, 9, rbac062. [Google Scholar] [CrossRef]
- Voleti, P.B.; Buckley, M.R.; Soslowsky, L.J. Tendon healing: Repair and regeneration. Annu. Rev. Biomed. Eng. 2012, 14, 47–71. [Google Scholar] [CrossRef]
- Yang, G.; Rothrauff, B.B.; Tuan, R.S. Tendon and ligament regeneration and repair: Clinical relevance and developmental paradigm. Birth Defects Res. Part C Embryo Today Rev. 2013, 99, 203–222. [Google Scholar] [CrossRef]
- Walden, G.; Liao, X.; Donell, S.; Raxworthy, M.J.; Riley, G.P.; Saeed, A. A Clinical, Biological, and Biomaterials Perspective into Tendon Injuries and Regeneration. Tissue Eng. Part B Rev. 2017, 23, 44–58. [Google Scholar] [CrossRef] [PubMed]
- Riley, G. Tendinopathy—From basic science to treatment. Nat. Clin. Pract. Rheumatol. 2008, 4, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Kokubun, T.; Kanemura, N.; Murata, K.; Moriyama, H.; Morita, S.; Jinno, T.; Ihara, H.; Takayanagi, K. Effect of Changing the Joint Kinematics of Knees With a Ruptured Anterior Cruciate Ligament on the Molecular Biological Responses and Spontaneous Healing in a Rat Model. Am. J. Sport. Med. 2016, 44, 2900–2910. [Google Scholar] [CrossRef] [PubMed]
- Zitnay, J.L.; Weiss, J.A. Load transfer, damage, and failure in ligaments and tendons. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2018, 36, 3093–3104. [Google Scholar] [CrossRef] [PubMed]
- Andia, I.; Martin, J.I.; Maffulli, N. Advances with platelet rich plasma therapies for tendon regeneration. Expert Opin. Biol. Ther. 2018, 18, 389–398. [Google Scholar] [CrossRef]
- Menter, D.G.; Tucker, S.C.; Kopetz, S.; Sood, A.K.; Crissman, J.D.; Honn, K.V. Platelets and cancer: A casual or causal relationship: Revisited. Cancer Metastasis Rev. 2014, 33, 231–269. [Google Scholar] [CrossRef]
- Eisinger, F.; Patzelt, J.; Langer, H.F. The Platelet Response to Tissue Injury. Front. Med. 2018, 5, 317. [Google Scholar] [CrossRef]
- Kaux, J.F.; Libertiaux, V.; Dupont, L.; Colige, A.; Denoël, V.; Lecut, C.; Hego, A.; Gustin, M.; Duwez, L.; Oury, C.; et al. Platelet-rich plasma (PRP) and tendon healing: Comparison between fresh and frozen-thawed PRP. Platelets 2020, 31, 221–225. [Google Scholar]
- Vander Doelen, T.; Jelley, W. Non-surgical treatment of patellar tendinopathy: A systematic review of randomized controlled trials. J. Sci. Med. Sport 2020, 23, 118–124. [Google Scholar] [CrossRef]
- Arumugam, S.; Prakash, A.; Janani, G.; Vignesh, M.; Anjanavannan, M.M.; Perumal, S.; Alwar, T. Platelet-Rich Plasma (PRP) Injection in Sports Injuries. Indian J. Orthop. 2021, 55, 484–491. [Google Scholar] [CrossRef]
- Tarpada, S.P.; Morris, M.T.; Lian, J.; Rashidi, S. Current advances in the treatment of medial and lateral epicondylitis. J. Orthop. 2018, 15, 107–110. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, R.; Zhu, B.; Li, Y.; Liu, X.; Guo, S.; Wang, C.; Wang, D.; Li, S. Effects of leukocyte- and platelet-rich plasma on tendon disorders based on in vitro and in vivo studies (Review). Exp. Ther. Med. 2021, 21, 639. [Google Scholar] [CrossRef] [PubMed]
- Kia, C.; Baldino, J.; Bell, R.; Ramji, A.; Uyeki, C.; Mazzocca, A. Platelet-Rich Plasma: Review of Current Literature on its Use for Tendon and Ligament Pathology. Curr. Rev. Musculoskelet. Med. 2018, 11, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Molloy, T.; Wang, Y.; Murrell, G. The roles of growth factors in tendon and ligament healing. Sport. Med. (Auckl. N.Z.) 2003, 33, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Madhi, M.I.; Yausep, O.E.; Khamdan, K.; Trigkilidas, D. The use of PRP in treatment of Achilles Tendinopathy: A systematic review of literature. Study design: Systematic review of literature. Ann. Med. Surg. 2020, 55, 320–326. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Saita, Y.; Takaku, T.; Yokomizo, T.; Nishio, H.; Ikeda, H.; Takazawa, Y.; Nagao, M.; Kaneko, K.; Komatsu, N. Platelet-rich plasma (PRP) accelerates murine patellar tendon healing through enhancement of angiogenesis and collagen synthesis. J. Exp. Orthop. 2020, 7, 49. [Google Scholar] [CrossRef]
- Yu, T.Y.; Pang, J.S.; Lin, L.P.; Cheng, J.W.; Liu, S.J.; Tsai, W.C. Platelet-Rich Plasma Releasate Promotes Early Healing in Tendon After Acute Injury. Orthop J Sport. Med. 2021, 9, 2325967121990377. [Google Scholar] [CrossRef]
- Padilla, S.; Sánchez, M.; Vaquerizo, V.; Malanga, G.A.; Fiz, N.; Azofra, J.; Rogers, C.J.; Samitier, G.; Sampson, S.; Seijas, R.; et al. Platelet-Rich Plasma Applications for Achilles Tendon Repair: A Bridge between Biology and Surgery. Int. J. Mol. Sci. 2021, 22, 824. [Google Scholar] [CrossRef]
- Liu, W.; Xie, X.; Wu, J. Platelet-Rich Plasma Promotes Spinal Ligament Healing after Injury. Clin. Lab. 2020, 66, 1–3. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, J.H. Platelet-rich plasma releasate promotes differentiation of tendon stem cells into active tenocytes. Am. J. Sport. Med. 2010, 38, 2477–2486. [Google Scholar] [CrossRef]
- Zhang, J.; Nie, D.; Williamson, K.; Rocha, J.L.; Hogan, M.V.; Wang, J.H. Selectively activated PRP exerts differential effects on tendon stem/progenitor cells and tendon healing. J. Tissue Eng. 2019, 10, 2041731418820034. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Troya, M.; Orive, G. An autologous platelet-rich plasma stimulates periodontal ligament regeneration. J. Periodontol. 2013, 84, 1556–1566. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.; Johnson, V.M.; Murray, M.M. Effects of age and platelet-rich plasma on ACL cell viability and collagen gene expression. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2012, 30, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.; Wang, H.; Yoshida, R.; Murray, M.M. Platelets and plasma proteins are both required to stimulate collagen gene expression by anterior cruciate ligament cells in three-dimensional culture. Tissue Eng. Part A 2010, 16, 1479–1489. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, M.S.; Karna, S.K.; Dhatt, S.S.; Behera, P.; Bhatia, A. Can Platelet rich plasma stimulate human ACL growth in culture? A preliminary experience. Muscles Ligaments Tendons J. 2015, 5, 156–161. [Google Scholar]
- Fallouh, L.; Nakagawa, K.; Sasho, T.; Arai, M.; Kitahara, S.; Wada, Y.; Moriya, H.; Takahashi, K. Effects of autologous platelet-rich plasma on cell viability and collagen synthesis in injured human anterior cruciate ligament. J. Bone Jt. Surg. Am. Vol. 2010, 92, 2909–2916. [Google Scholar] [CrossRef]
- Krismer, A.M.; Cabra, R.S.; May, R.D.; Frauchiger, D.A.; Kohl, S.; Ahmad, S.S.; Gantenbein, B. Biologic response of human anterior cruciate ligamentocytes on collagen-patches to platelet-rich plasma formulations with and without leucocytes. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2017, 35, 2733–2739. [Google Scholar] [CrossRef]
- McCarrel, T.; Fortier, L. Temporal growth factor release from platelet-rich plasma, trehalose lyophilized platelets, and bone marrow aspirate and their effect on tendon and ligament gene expression. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2009, 27, 1033–1042. [Google Scholar] [CrossRef]
- Rattanasuwan, K.; Rassameemasmaung, S.; Kiattavorncharoen, S.; Sirikulsathean, A.; Thorsuwan, J.; Wongsankakorn, W. Platelet-rich plasma stimulated proliferation, migration, and attachment of cultured periodontal ligament cells. Eur. J. Dent. 2018, 12, 469–474. [Google Scholar] [CrossRef]
- Schnabel, L.V.; Sonea, H.O.; Jacobson, M.S.; Fortier, L.A. Effects of platelet rich plasma and acellular bone marrow on gene expression patterns and DNA content of equine suspensory ligament explant cultures. Equine Vet. J. 2008, 40, 260–265. [Google Scholar] [CrossRef]
- Smith, J.J.; Ross, M.W.; Smith, R.K. Anabolic effects of acellular bone marrow, platelet rich plasma, and serum on equine suspensory ligament fibroblasts in vitro. Vet. Comp. Orthop. Traumatol. V.C.O.T 2006, 19, 43–47. [Google Scholar] [PubMed]
- Yoshida, R.; Cheng, M.; Murray, M.M. Increasing platelet concentration in platelet-rich plasma inhibits anterior cruciate ligament cell function in three-dimensional culture. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2014, 32, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Huang, W.; He, B.; Tan, H.; Lin, P.; Zha, Z. Positive effects of platelet-rich plasma (PRP) and a Sanguisorba officinalis polysaccharide on the proliferation and differentiation of anterior cruciate ligament (ACL) fibroblasts in vitro. Pharm. Biol. 2020, 58, 297–305. [Google Scholar] [CrossRef]
- Yoshida, R.; Murray, M.M. Peripheral blood mononuclear cells enhance the anabolic effects of platelet-rich plasma on anterior cruciate ligament fibroblasts. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2013, 31, 29–34. [Google Scholar] [CrossRef]
- Amar, E.; Snir, N.; Sher, O.; Brosh, T.; Khashan, M.; Salai, M.; Dolkart, O. Platelet-rich plasma did not improve early healing of medial collateral ligament in rats. Arch. Orthop. Trauma Surg. 2015, 135, 1571–1577. [Google Scholar] [CrossRef]
- Bozynski, C.C.; Stannard, J.P.; Smith, P.; Hanypsiak, B.T.; Kuroki, K.; Stoker, A.; Cook, C.; Cook, J.L. Acute Management of Anterior Cruciate Ligament Injuries Using Novel Canine Models. J. Knee Surg. 2016, 29, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.L.; Smith, P.A.; Bozynski, C.C.; Kuroki, K.; Cook, C.R.; Stoker, A.M.; Pfeiffer, F.M. Multiple injections of leukoreduced platelet rich plasma reduce pain and functional impairment in a canine model of ACL and meniscal deficiency. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2016, 34, 607–615. [Google Scholar] [CrossRef]
- Harris, N.L.; Huffer, W.E.; von Stade, E.; Larson, A.I.; Phinney, S.; Purnell, M.L. The effect of platelet-rich plasma on normal soft tissues in the rabbit. J. Bone Jt. Surg. Am. Vol. 2012, 94, 786–793. [Google Scholar] [CrossRef]
- Haus, B.M.; Mastrangelo, A.N.; Murray, M.M. Effect of anterior cruciate healing on the uninjured ligament insertion site. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2012, 30, 86–94. [Google Scholar] [CrossRef]
- Joshi, S.M.; Mastrangelo, A.N.; Magarian, E.M.; Fleming, B.C.; Murray, M.M. Collagen-platelet composite enhances biomechanical and histologic healing of the porcine anterior cruciate ligament. Am. J. Sport. Med. 2009, 37, 2401–2410. [Google Scholar] [CrossRef]
- LaPrade, R.F.; Goodrich, L.R.; Phillips, J.; Dornan, G.J.; Turnbull, T.L.; Hawes, M.L.; Dahl, K.D.; Coggins, A.N.; Kisiday, J.; Frisbie, D.; et al. Use of Platelet-Rich Plasma Immediately After an Injury Did Not Improve Ligament Healing, and Increasing Platelet Concentrations Was Detrimental in an In Vivo Animal Model. Am. J. Sport. Med. 2018, 46, 702–712. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, A.N.; Vavken, P.; Fleming, B.C.; Harrison, S.L.; Murray, M.M. Reduced platelet concentration does not harm PRP effectiveness for ACL repair in a porcine in vivo model. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2011, 29, 1002–1007. [Google Scholar] [CrossRef]
- Matsunaga, D.; Akizuki, S.; Takizawa, T.; Omae, S.; Kato, H. Compact platelet-rich fibrin scaffold to improve healing of patellar tendon defects and for medial collateral ligament reconstruction. Knee 2013, 20, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.M.; Spindler, K.P.; Abreu, E.; Muller, J.A.; Nedder, A.; Kelly, M.; Frino, J.; Zurakowski, D.; Valenza, M.; Snyder, B.D.; et al. Collagen-platelet rich plasma hydrogel enhances primary repair of the porcine anterior cruciate ligament. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2007, 25, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.M.; Spindler, K.P.; Ballard, P.; Welch, T.P.; Zurakowski, D.; Nanney, L.B. Enhanced histologic repair in a central wound in the anterior cruciate ligament with a collagen-platelet-rich plasma scaffold. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2007, 25, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.M.; Spindler, K.P.; Devin, C.; Snyder, B.S.; Muller, J.; Takahashi, M.; Ballard, P.; Nanney, L.B.; Zurakowski, D. Use of a collagen-platelet rich plasma scaffold to stimulate healing of a central defect in the canine ACL. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2006, 24, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, T.; Kanamori, A.; Washio, T.; Aoto, K.; Uemura, K.; Sakane, M.; Ochiai, N. The effects of plasma rich in growth factors (PRGF-Endoret) on healing of medial collateral ligament of the knee. Knee Surg. Sport. Traumatol. Arthrosc. Off. J. ESSKA 2013, 21, 1763–1769. [Google Scholar] [CrossRef]
- Anitua, E.; Sanchez, M.; Nurden, A.T.; Zalduendo, M.; de la Fuente, M.; Azofra, J.; Andia, I. Reciprocal actions of platelet-secreted TGF-beta1 on the production of VEGF and HGF by human tendon cells. Plast. Reconstr. Surg. 2007, 119, 950–959. [Google Scholar] [CrossRef]
- Anitua, E.; Sanchez, M.; Nurden, A.T.; Zalduendo, M.; de la Fuente, M.; Orive, G.; Azofra, J.; Andia, I. Autologous fibrin matrices: A potential source of biological mediators that modulate tendon cell activities. J. Biomed. Mater. Res. Part A 2006, 77, 285–293. [Google Scholar] [CrossRef]
- de Mos, M.; van der Windt, A.E.; Jahr, H.; van Schie, H.T.; Weinans, H.; Verhaar, J.A.; van Osch, G.J. Can platelet-rich plasma enhance tendon repair? A cell culture study. Am. J. Sport. Med. 2008, 36, 1171–1178. [Google Scholar] [CrossRef]
- Hudgens, J.L.; Sugg, K.B.; Grekin, J.A.; Gumucio, J.P.; Bedi, A.; Mendias, C.L. Platelet-Rich Plasma Activates Proinflammatory Signaling Pathways and Induces Oxidative Stress in Tendon Fibroblasts. Am. J. Sport. Med. 2016, 44, 1931–1940. [Google Scholar] [CrossRef] [PubMed]
- Jo, C.H.; Kim, J.E.; Yoon, K.S.; Shin, S. Platelet-rich plasma stimulates cell proliferation and enhances matrix gene expression and synthesis in tenocytes from human rotator cuff tendons with degenerative tears. Am. J. Sport. Med. 2012, 40, 1035–1045. [Google Scholar] [CrossRef]
- Schnabel, L.V.; Mohammed, H.O.; Miller, B.J.; McDermott, W.G.; Jacobson, M.S.; Santangelo, K.S.; Fortier, L.A. Platelet rich plasma (PRP) enhances anabolic gene expression patterns in flexor digitorum superficialis tendons. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2007, 25, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Al-Ani, M.K.; Sun, Y.; Xu, W.; Pan, L.; Song, Y.; Xu, Z.; Pan, X.; Yang, L. Platelet-rich plasma activates tendon-derived stem cells to promote regeneration of Achilles tendon rupture in rats. J. Tissue Eng. Regen. Med. 2017, 11, 1173–1184. [Google Scholar] [CrossRef] [PubMed]
- Cross, J.A.; Cole, B.J.; Spatny, K.P.; Sundman, E.; Romeo, A.A.; Nicholson, G.P.; Wagner, B.; Fortier, L.A. Leukocyte-Reduced Platelet-Rich Plasma Normalizes Matrix Metabolism in Torn Human Rotator Cuff Tendons. Am. J. Sport. Med. 2015, 43, 2898–2906. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, J.; Wu, H.; Hogan, M.V.; Wang, J.H. The differential effects of leukocyte-containing and pure platelet-rich plasma (PRP) on tendon stem/progenitor cells—Implications of PRP application for the clinical treatment of tendon injuries. Stem Cell Res. Ther. 2015, 6, 173. [Google Scholar] [CrossRef] [PubMed]
- Aspenberg, P.; Virchenko, O. Platelet concentrate injection improves Achilles tendon repair in rats. Acta Orthop. Scand. 2004, 75, 93–99. [Google Scholar] [CrossRef]
- Bosch, G.; René van Weeren, P.; Barneveld, A.; van Schie, H.T. Computerised analysis of standardised ultrasonographic images to monitor the repair of surgically created core lesions in equine superficial digital flexor tendons following treatment with intratendinous platelet rich plasma or placebo. Vet. J. 2011, 187, 92–98. [Google Scholar] [CrossRef]
- Han, L.; Fang, W.L.; Jin, B.; Xu, S.C.; Zheng, X.; Hu, Y.G. Enhancement of tendon-bone healing after rotator cuff injuries using combined therapy with mesenchymal stem cells and platelet rich plasma. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 9075–9084. [Google Scholar]
- Li, S.; Wu, Y.; Jiang, G.; Tian, X.; Hong, J.; Chen, S.; Yan, R.; Feng, G.; Cheng, Z. Intratendon delivery of leukocyte-rich platelet-rich plasma at early stage promotes tendon repair in a rabbit Achilles tendinopathy model. J. Tissue Eng. Regen. Med. 2020, 14, 452–463. [Google Scholar] [CrossRef]
- Lyras, D.N.; Kazakos, K.; Georgiadis, G.; Mazis, G.; Middleton, R.; Richards, S.; O’Connor, D.; Agrogiannis, G. Does a single application of PRP alter the expression of IGF-I in the early phase of tendon healing? J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2011, 50, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Lyras, D.N.; Kazakos, K.; Verettas, D.; Polychronidis, A.; Tryfonidis, M.; Botaitis, S.; Agrogiannis, G.; Simopoulos, C.; Kokka, A.; Patsouris, E. The influence of platelet-rich plasma on angiogenesis during the early phase of tendon healing. Foot Ankle Int. 2009, 30, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, F.; Augi, T.; Williamson, K.M.; Onishi, K.; Hogan, M.V.; Neal, M.D.; Wang, J.H. Platelet HMGB1 in Platelet-Rich Plasma (PRP) promotes tendon wound healing. PLoS ONE 2021, 16, e0251166. [Google Scholar] [CrossRef] [PubMed]
- Jiang, G.; Wu, Y.; Meng, J.; Wu, F.; Li, S.; Lin, M.; Gao, X.; Hong, J.; Chen, W.; Yan, S.; et al. Comparison of Leukocyte-Rich Platelet-Rich Plasma and Leukocyte-Poor Platelet-Rich Plasma on Achilles Tendinopathy at an Early Stage in a Rabbit Model. Am. J. Sport. Med. 2020, 48, 1189–1199. [Google Scholar] [CrossRef]
- Yan, R.; Gu, Y.; Ran, J.; Hu, Y.; Zheng, Z.; Zeng, M.; Heng, B.C.; Chen, X.; Yin, Z.; Chen, W.; et al. Intratendon Delivery of Leukocyte-Poor Platelet-Rich Plasma Improves Healing Compared With Leukocyte-Rich Platelet-Rich Plasma in a Rabbit Achilles Tendinopathy Model. Am. J. Sport. Med. 2017, 45, 1909–1920. [Google Scholar] [CrossRef]


{kind=link}
| Article | Year | Animal (Species)/Human | Number of Animals or Participants | Ligaments | Solutions Compared | Duration of Culture | Histology and Cellular Activity | Molecular Effect |
|---|---|---|---|---|---|---|---|---|
| Smith et al. [41] | 2006 | Animal (horse) | 5 | Suspensory ligament | control, equine serum, foetal bovine serum, ABM (5%, 10%), PRP (5%, 10%) | 48 h | ↑ COMP, 3H-Leucine incorporation | |
| Schnabel et al. [40] | 2008 | Animal (horse) | 6 | Suspensory ligament | control, whole blood, BMA, PPP, PRP (10%, 50% or 100%) | 3 days | ↑ COMP, MMP3 ↓ COL3A1, MMP13 ≈ COL1A1, COL1A1:COL3A1, Decorin | |
| McCarrel et al. [38] | 2009 | Animal (horse) | 5 | Suspensory ligament | control, PPP, PRP, BMA | 96 h | ↑ COL1A1, COMP, Decorin, MMP3, COL1A1:COL3A1 ↓ COL3A1, MMP13 | |
| Cheng et al. [34] | 2010 | Animal (pig) | Nm | ACL | control, platelet, PPP, PRP | 14 days | ↑ metabolic activity, collagen organization ↓ apoptotic rate Centrally positioned elongated nuclei, oriented along the longitudinal axis; highest average nuclear aspect ratio; wave fiber-like structure of collagenous ECM aligned with the longitudinal axis of the constructs; prevalence of collagen fibrils, mostly aligned with the cells and packed into collagen fibers | ↑ COL1A1, COL3A1 |
| Cheng et al. [33] | 2012 | Animal (pig) | 15 | ACL | control, PRP | 14 days | ↑ metabolic activity, collagen organization ↓apoptotic rate (more in immature and adolescent animals) | ↑ COL1A1, COL3A1 (more in immature and adolescent animals) |
| Yoshida et al. [44] | 2013 | Animal (pig) | Nm | ACL | control, PPP, PRP, PBMC, PPP + PBMC, PRP + PBMC | 14 days | PRP + PBMC ↑ metabolic activity, collagen | PRP + PBMC ↑ procollagen type I and type III genes, IL-6 |
| Yoshida et al. [42] | 2014 | Animal (pig) | 5 | ACL | control, PPP, PRP, PRPx3, PRPx5 | 14 days | ↑ metabolic activity, viability | ↑ COL1A1, COL3A1 |
| Zheng et al. [43] | 2020 | Animal (rabbit) | 4 | ACL | control, Sanguisorba officinalis L. polysaccharide + PRP, PRP | 72 h | ↑ viability, migration ↓ apoptotic rate | ↑ Runx2, ALP, BMP2, COL1, OPG ↓ TLR-4, p65 phosphorylation |
| Fallouh et al. [36] | 2010 | Human | 4 | ACL | control, PRP, PPP 5%, PRP 10% | 7 days | ↑ viability | ↑ total collagen, COL3 ≈ COL1, collagen/μg DNA |
| Anitua et al. [32] | 2013 | Human | 3 | Periodontal ligament | control, PRP | 24, 48, 72 h | ↑ proliferation, migration, attachment to COL1 | ↑ VEGF, TSP-1, HGF, Procollagen I, CTGF ↓ α2-Integrin |
| Dhillon et al. [35] | 2015 | Human | 11 | ACL | control, 5% PPP, 5% PRP, 10% PRP | 2 days | ↑ viability, proliferation ≈ apoptosis | |
| Krismer et al. [37] | 2017 | Human | 5 | ACL | controls, 2.5% LR-PRP, 2.5% PRP, 20% LR-PRP | 7, 14, 21 days | ↑ proliferation ≈ extracellular matrix production | ↑ COL1A2, COL2A1, TNC, SCXA, TNMD, ACAN, MKX, MMP13 ↓ COL3A1, MMP3 |
| Rattanasuwan et al. [39] | 2018 | Human | 3 | Periodontal ligament | control, 5% PRP, 10% PRP | 6 h | ↑ proliferation, migration, attachment to COL1 PRP (5% and 10%) Increased periodontal ligament fibroblasts cells with spindle shape and positive stain for toluidine blue O |
| Article | Year | Animal Species | Number of Animals | Ligaments (Pathology) | Comparison Modalities | Time from PRP Application | Histology and Cellular Activity |
|---|---|---|---|---|---|---|---|
| Murray et al. [56] | 2006 | Dog | 12 | ACL (tear) | control, collagen-PRP composite | 3,6 weeks | ↑ defect filling |
| Murray et al. [54] | 2007 | Pig | 5 | ACL (tear) | control, collagen-PRP composite | 4 weeks | ↑ cellularity, vascularity ↓ inflammation |
| Murray et al. [55] | 2007 | Dog | 17 | ACL, MCL, Patellar tendon (full thickness tear) | extraarticular ligament, collagen-PRP hydrogel at ACL | 3, 6 weeks | ≈ modified LTMI to extraarticular ligaments |
| Joshi et al. [50] | 2009 | Pig | 27 | ACL (full thickness tear) | control, collagen-PRP matrix | 4,6 weeks, 3 months | ↑ cellularity ≈ vascularity Increased number of fusiform-shaped cells |
| Mastrangelo et al. [52] | 2011 | Pig | 8 | ACL (full thickness tear) | collagen-3xPRP matrix, collagen-5xPRP matrix | 13 weeks | 5xPRP ↑ modified LTMI Similar cell orientation and shape in both groups |
| Harris et al. [48] | 2012 | Rabbit | 18 | MCL (full thickness tear) | control, PRP | 2,6 weeks, 12 weeks (reinjection at 6 weeks) | ↓ prominent inflammation at 6 and 12 weeks |
| Haus et al. [49] | 2012 | Pig | 24 | ACL (full thickness tear) | control, collagen-PRP composite | 15 weeks | ↑ remodeling at the insertion site, cellularity, collagen organization (less in older age animals) Increased collagen organization at fibrous zone with relatively large proportion of collagen oriented perpendicular to the insertion site in a densely packed arrangement; relatively good organization of collagen perpendicular to the subchondral plate at fibrocartilage zone; distinct fibrocartilage layer |
| Matsunaga et al. [53] | 2013 | Rabbit | 20 | MCL (full thickness tear) | control, PRP-fibrin scaffold | 4, 8, 12 weeks | ↑ mature neo-ligament at 12 weeks Neo-ligament of dense and longitudinally aligned collagen bundles and direct fibrocartilage insertions |
| Yoshika et al. [57] | 2013 | Rabbit | 31 | MCL (full thickness tear) | control, clot of PRP | 3, 6 weeks | ↑ collagen organization ≈ cellular size, cellularity |
| Amar et al. [45] | 2015 | Rat | 32 | MCL (full thickness tear) | control, PRP | 3 weeks | cellularity, collagen organization, vascularityFat cells; inflammatory foci; loose and disorganized collagen |
| Bozynski et al. [46] | 2016 | Dog | 12 | ACL (partial tear) | standard care, washout, LP-PRP | ≈ myxoid/mucinous degeneration, collagen fiber orientation | |
| Cook et al. [47] | 2016 | Dog | 12 | ACL (partial tear) | control, LP-PRP (inj. at 1, 2, 3, 6 and 8 weeks) | 24 weeks | ↓ severe pathology |
| LaPrade et al. [51] | 2018 | Rabbit | 80 | MCL (full thickness tear) | control, PPP, 2xPRP, 4xPRP, intact | 6 weeks | ≈ LTMI to controls ↓ LTMI than intact ligament Negative effect of 4xPRP |
| Article | Year | Animal (Species)/Human | Number of Animals or Participants | Tendon | Solutions Compared | Duration of Culture | Histology and Cellular Activity | Molecular Effect |
|---|---|---|---|---|---|---|---|---|
| Schnabel et al. [63] | 2007 | Animal (horse) | 6 | Flexor digitorum superficialis | control, whole blood, BMA, PPP, PRP (10%, 50% or 100%) | 3 days | ↑ COL1A1, COL3A1, COL1A1:COL3A1, COMP ↓ MMP13 ≈ MMP3, Decorin | |
| McCarrel et al. [38] | 2009 | Animal (horse) | 5 | Flexor digitorum superficialis | control, 100% BMA, 100% PRP, lyophilized platelet product | 96 h | ↑ COL1A1, COL1A1:COL3A1, COMP, MMP3 ↓ COL3A1, Decorin, MMP13 | |
| Zhou et al. [66] | 2015 | Animal (rabbit) | 2 | Patellar | control, 10% LR-PRP, 10% PRP | 14 days | LR-PRP ↑ cell proliferation | PRP ↑ COL1, COL3, α-SMA LR-PRP ↑ MMP1, MMP13, IL-6, IL-1β, TNF-α, PGE2 |
| Hudgens et al. [61] | 2016 | Animal (rat) | Nm | Tail tendon | control, PPP, PRP | 5 days | ↑ BMP7, CCL2, CCL7, IL-1a, IL-6, IL-10, TNFa, LOX, COL8, Lubricin, MMP3, MMP9, MMP10, MMP13, Ki67, Fosb, Fosl1, c-Jun, PLD1, PTGES, Cox1, Cox2, SOD1, SOD2, NFE2L2, Prdx1 ↓ CTGF, IGF1, IL-15, Elastin, COL1, COL3, CILP, Fibromodulin, COL12, COL14, EGR1, EGR2, SCX, TNMD ≈ TGFβ, IL-1b, VEGF, HAS1, HAS2, MMP8, MMP2, TIMP1, TIMP2, Atg10, Bnip1, GABARAPL2, beclin 1, Trim13, SIRT1, iNOS, 5-LOX | |
| Xu et al. [64] | 2017 | Animal (rat) | Nm | Achilles | control, 10% PRP | 3 weeks | ↑ viability, migration, proliferation at 3 days | COL1, COL3, SCX, Tenascin-C |
| Anitua et al. [59] | 2006 | Human | 6 | Semitendinosus | control, PPP, PRP | 6 days | ↑ proliferation | ↑ VEGF, TGF-β1, HGF, human Procollagen I C-peptide |
| Anitua et al. [58] | 2007 | Human | 4 | Semitendinosus | control, PPP or PRP with or without PDGF or TGF-β1 | 4 days | PDGF ↑ proliferation TGF-β1 ↑ collagen synthesis | TGF-β1 group ↑ VEGF, HGF |
| de Mos et al. [60] | 2008 | Human | 3 | Hamstring | control, PRP or PPP (10% or 20%) | 4, 7, 14 days | ↑ proliferation, collagen production Changes in cells appearance: from spindle-shaped, fibroblast-like cells to stretched, oblong shaped cells | ↑ MMP3, MMP13, VEGF-A, TGF-β1 ↓ COL1, COL3, MMP1. ≈ COL3:COL1 |
| Jo et al. [62] | 2012 | Human | 9 | Rotator cuff | control, PPP, PRP, PRP + thrombin | 14 days | ↑ proliferation, total collagen, glycosaminoglycans | Day 7 ↑ COL1, COL3, Tenascin-C ≈ COL3:COL1 Day 14 ↑ COL3, Decorin, SCX, Tenascin-C ≈ COL3:COL1 |
| Cross et al. [65] | 2015 | Human | 20 | Supraspinatous | control, LP-PRP, LR-PRP | ↑ COL1:COL3, MMP9, IL-1b ≈ COMP, MMP13 | ||
| Zhang et al. [31] | 2019 | Human | 7 | Patellar | control, PRP + thrombin, PRP + PAR1, PRP + PAR4 | 5 days | ↑ proliferation PRP + thrombin Elongated tenocyte-like cells PRP + PAR1 Tenocyte-like cells, “vessel-like” cellular pattern PRP + PAR4 More organized cells than PRP + PAR1 group | ↑ COL1, MMP1, MMP2 ≈ COL2, Runx-2, LPL |
| Article | Year | Animal Species | Number of Animals | Tendons | Comparison Modalities | Time from PRP Application | Histology and Cellular Activity | Molecular Effect |
|---|---|---|---|---|---|---|---|---|
| Aspenberg and Virchenko [67] | 2004 | Rat | 80 | Achilles (full thickness tear) | control, PPP, PRP | 11, 21 days | 21 days ↓ time to healing | |
| Anitua et al. [59] | 2006 | Sheep | 6 | Achilles (intact) | control, PPP or PRP (4 inj/1 per week) | 7 days after last injection | ↑ cell density, vascularity | |
| Lyras et al. [72] | 2009 | Rabbit | 48 | Achilles (full thickness tear) | control, PRP | 1, 2, 3, 4 weeks | ↓ time to healing | Week 1,2 ↑ CD31 Week 3,4 ↓ CD31 |
| Lyras et al. [71] | 2011 | Rabbit | 48 | Achilles (full thickness tear) | control, PRP | 1, 2, 3, 4 weeks | ↓ time to healing | Until 3 weeks ↑ IGF-I in epitendon and endotendon Week 4 ↑ IGF-I in epitendon ↓ IGF-I in endotendon |
| Bosch et al. [68] | 2011 | Horse | 6 | Superficial digitorum flexor (full thickness tear) | control, PRP | 23 weeks | ↑ collagen organization | |
| Harris et al. [48] | 2012 | Rabbit | 18 | Achilles (intact) | control, PRP | 2, 6 weeks, 12 weeks (reinjection at 6 weeks) | ↓ inflammatory response | |
| Matsunaga et al. [53] | 2013 | Rabbit | 18 | Patellar (full thickness tear) | control, PRP-fibrin scaffold | 4 weeks | ↑ collagen organization | |
| Xu et al. [64] | 2017 | Rat | 45 | Achilles (full thickness tear) | control, collagen-matrix, PRP-collagen matrix | 1, 2, 3 weeks | ↑ cell maturation, collagen organization | |
| Yan et al. [75] | 2017 | Rabbit | 28 | Achilles (chronic tendinopathy) | control, LP-PRP, LR-PRP | 4 weeks | LR-PRP ↑ modified Movin score, mature collagen fibers | LR-PRP ↓ IL-6 ≈ IL-1β, TNF-α. LP-PRP ↑ COL1, TIMP-1, ↓ MMP-9. LR-PRP and LP-PRP ↑ COL1:COL3 ↓ MMP1, MMP3. ≈ COL 3 |
| Han et al. [69] | 2019 | Rat | Nm | Rotator cuff (full thickness tear) | control, MSC, PRP, PRP + MSC | 4 weeks | ↑ VEGF, PDGF, EGF, TGF-β, BMP2, BMP7, COL1, TNMD, SCX, p-ERK1/2, Osterix, Runx2, OCN | |
| Zhang et al. [31] | 2019 | Rat | 8 | Patellar (partial tear) | control, PRP + thrombin, PRP + PAR1, PRP + PAR4 | 8 weeks | ↓ time to healing (faster healing when thrombin-activated) | |
| Jiang et al. [74] | 2020 | Rabbit | 28 | Achilles (tendinopathy) | control, LP-PRP, LR-PRP | 3, 6 week | LR-PRP ↑ modified Movin score, mature collagen fibers | Week 3—LR-PRP ↑ COL1, VEGF, VEGF receptor, TNF-a, ARG2, IL-10, CD163 ↓ COL3 Week 6—LR-PRP ↑ COL1, CD163 ↓ COL3, VEGF, VEGF receptor, TNF-a, ARG2, IL-10 Week 6—LP-PRP ↑ ARG2, IL-10 |
| Kobayashi et al. [26] | 2020 | Rat | 40 | Patellar (full thickness tear)— | control, PRP gel | 2, 4, 6, 8, 10 weeks | ↓ time to healing ↑ collagen rearrangement, vascularity, tendon thickening Week 2,4 ↑ Bonar score, vascularity score Week 6,8 ↓ Bonar score, ground substance score, collagen arrangement PRP Earlier invasion of inflammatory cells; increase of blood capillaries; thickening of tendon during the early phase; collagen rearrangement | |
| Li et al. [70] | 2020 | Rabbit | 32 | Achilles (tendinopathy) | control, LR-PRP (at 1 or 4 week) | 6 weeks | ↑ collagen organization, vascularity, cell density | Week 1 ↑ IL-10, COL1, CD163+ M2 macrophages Week 4 ↑ IL-6, COL3, MMP1, MMP3 ≈ IL-1β, TNF-α |
| Yu et al. [27] | 2021 | Rat | 48 | Achilles (partial tear) | control, PRP | 5, 10 days | Days 5 ↑ fibroblast orientation, collagen matrix ↓ cell apoptosis Day 10 ↑ newly formed tendon fibers, collagen fibers | Days 5 ↑ Ki-67–positive cells ↓ ED1+ macrophages Day 10 ≈ Ki-67–positive cells, ED1+ macrophages |
| Zhang et al. [73] | 2021 | Mouse | 18 | Patellar (partial tear) | control, PRP with or without HMGB1 | 7 days | ↓ time to healing (faster healing when HMGB1 present) | ↑ CD146+ and CD73+ stem cells ↓ CD68+ M1 macrophages |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chalidis, B.; Givissis, P.; Papadopoulos, P.; Pitsilos, C. Molecular and Biologic Effects of Platelet-Rich Plasma (PRP) in Ligament and Tendon Healing and Regeneration: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 2744. https://doi.org/10.3390/ijms24032744
Chalidis B, Givissis P, Papadopoulos P, Pitsilos C. Molecular and Biologic Effects of Platelet-Rich Plasma (PRP) in Ligament and Tendon Healing and Regeneration: A Systematic Review. International Journal of Molecular Sciences. 2023; 24(3):2744. https://doi.org/10.3390/ijms24032744
Chicago/Turabian StyleChalidis, Byron, Panagiotis Givissis, Pericles Papadopoulos, and Charalampos Pitsilos. 2023. "Molecular and Biologic Effects of Platelet-Rich Plasma (PRP) in Ligament and Tendon Healing and Regeneration: A Systematic Review" International Journal of Molecular Sciences 24, no. 3: 2744. https://doi.org/10.3390/ijms24032744
APA StyleChalidis, B., Givissis, P., Papadopoulos, P., & Pitsilos, C. (2023). Molecular and Biologic Effects of Platelet-Rich Plasma (PRP) in Ligament and Tendon Healing and Regeneration: A Systematic Review. International Journal of Molecular Sciences, 24(3), 2744. https://doi.org/10.3390/ijms24032744