
Functional and Molecular Markers for Hearing Loss and Vertigo Attacks in Meniere’s Disease


Abstract
1. Introduction
2. Functional Markers for MD
2.1. Pure Tone Audiometry (PTA)
2.2. Electrocochleography (ECochG)
2.3. Vestibular Evoked Myogenic Potential (VEMP)
2.4. Caloric Test/Video Head Impulse Test (vHIT)
2.5. MRI
2.6. The Problems and Future Directions of Functional Markers for MD
3. Molecular Markers for MD
3.1. Immunological/Autoimmunity Markers
3.2. Inflammatory Markers
3.3. Protein Signatures
3.4. Vasopressin
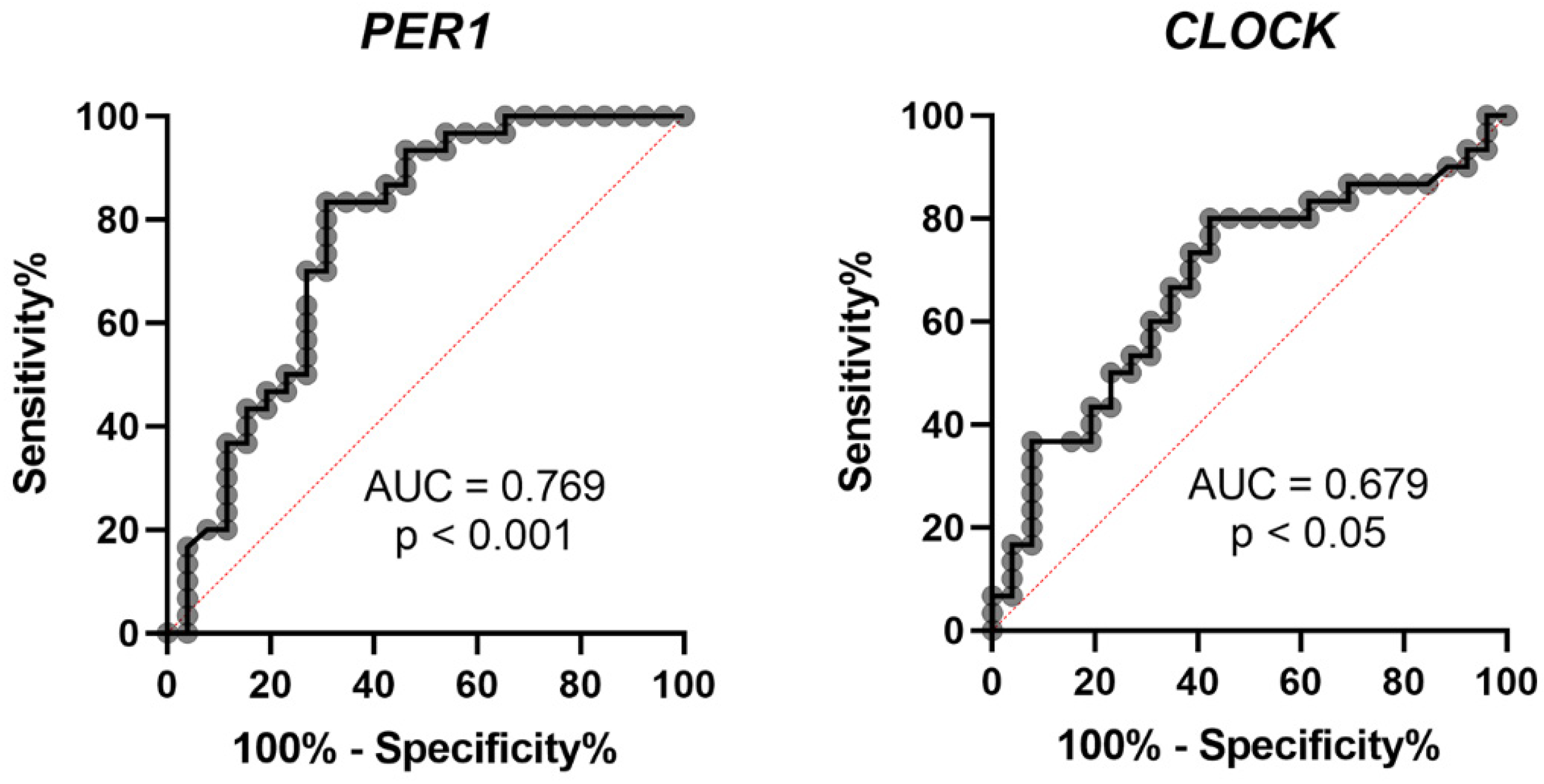
3.5. Circadian Clock Genes
3.6. The Problems and Future Directions of Molecular Markers for MD
4. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harris, J.P.; Alexander, T.H. Current-day prevalence of Ménière’s syndrome. Audiol. Neurootol. 2010, 15, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Paparella, M.M. Pathology of Meniere’s disease. Ann. Otol. Rhinol. Laryngol. Suppl. 1984, 112, 31–35. [Google Scholar] [CrossRef]
- Gluth, M.B. On the Relationship Between Menière’s Disease and Endolymphatic Hydrops. Otol. Neurotol. 2020, 41, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Merchant, S.N.; Adams, J.C.; Nadol, J.B., Jr. Pathophysiology of Meniere’s syndrome: Are symptoms caused by endolymphatic hydrops? Otol. Neurotol. 2005, 26, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.A.; Breeze, R.E. Endolymphatic hydrops in Ménière’s disease: Cause, consequence, or epiphenomenon? Otol. Neurotol. 2013, 34, 1210–1214. [Google Scholar] [CrossRef] [PubMed]
- Bächinger, D.; Luu, N.N.; Kempfle, J.S.; Barber, S.; Zürrer, D.; Lee, D.J.; Curtin, H.D.; Rauch, S.D.; Nadol, J.B., Jr.; Adams, J.C.; et al. Vestibular Aqueduct Morphology Correlates With Endolymphatic Sac Pathologies in Menière’s Disease-A Correlative Histology and Computed Tomography Study. Otol. Neurotol. 2019, 40, e548–e555. [Google Scholar] [CrossRef]
- Sando, I.; Ikeda, M. Pneumatization and thickness of the petrous bone in patients with Meniere’s disease. A histopathological study. Ann. Otol. Rhinol. Laryngol. Suppl. 1985, 118, 2–5. [Google Scholar] [CrossRef]
- Takeda, T.; Takeda, S.; Kakigi, A.; Okada, T.; Nishioka, R.; Taguchi, D.; Nishimura, M.; Nakatani, H. Hormonal aspects of Ménière’s disease on the basis of clinical and experimental studies. ORL J. Otorhinolaryngol Relat. Spec. 2010, 71 (Suppl. 1), 1–9. [Google Scholar] [CrossRef]
- Kakigi, A.; Takeda, T. Antidiuretic hormone and osmolality in patients with Ménière’s disease. ORL J. Otorhinolaryngol. Relat. Spec. 2009, 71, 11–13. [Google Scholar] [CrossRef]
- Gazquez, I.; Soto-Varela, A.; Aran, I.; Santos, S.; Batuecas, A.; Trinidad, G.; Perez-Garrigues, H.; Gonzalez-Oller, C.; Acosta, L.; Lopez-Escamez, J.A. High prevalence of systemic autoimmune diseases in patients with Menière’s disease. PLoS ONE 2011, 6, e26759. [Google Scholar] [CrossRef]
- Koo, J.W.; Oh, S.H.; Chang, S.O.; Park, M.H.; Lim, M.J.; Yoo, T.J.; Kim, C.S. Association of HLA-DR and type II collagen autoimmunity with Meniere’s disease. Tissue Antigens 2003, 61, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Sarna, B.; Abouzari, M.; Lin, H.W.; Djalilian, H.R. A hypothetical proposal for association between migraine and Meniere’s disease. Med. Hypotheses 2020, 134, 109430. [Google Scholar] [CrossRef] [PubMed]
- Ghavami, Y.; Mahboubi, H.; Yau, A.Y.; Maducdoc, M.; Djalilian, H.R. Migraine features in patients with Meniere’s disease. Laryngoscope 2016, 126, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Martinez, A.; Lopez-Escamez, J.A. Genetic architecture of Meniere’s disease. Hearth Res. 2020, 397, 107872. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Takeda, S.; Egami, N.; Kakigi, A.; Nishioka, R.; Yamasoba, T. Type 1 allergy-induced endolymphatic hydrops and the suppressive effect of leukotriene receptor antagonist. Otol. Neurotol. 2012, 33, 886–890. [Google Scholar] [CrossRef]
- Rizk, H.G.; Mehta, N.K.; Qureshi, U.; Yuen, E.; Zhang, K.; Nkrumah, Y.; Lambert, P.R.; Liu, Y.F.; McRackan, T.R.; Nguyen, S.A.; et al. Pathogenesis and Etiology of Meniere Disease: A Scoping Review of a Century of Evidence. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 360–368. [Google Scholar] [CrossRef]
- Goebel, J.A. 2015 Equilibrium Committee amendment to the 1995 AAO-HNS guidelines for the definition of Meniere’s disease. Otolaryngol. Head Neck Surg. 2016, 154, 403–404. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.-H.; Goebel, J.A.; Magnusson, M.; Mandalà, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F. Diagnostic criteria for Menière’s disease. J. Vestib. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef]
- Nakashima, T.; Pyykko, I.; Arroll, M.A.; Casselbrant, M.L.; Foster, C.A.; Manzoor, N.F.; Megerian, C.A.; Naganawa, S.; Young, Y.H. Meniere’s disease. Nat. Rev. Dis Prim. 2016, 2, 16028. [Google Scholar] [CrossRef] [PubMed]
- Committee on Hearing and Equilibrium. Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Menière’s disease. Otolaryngol. Head Neck Surg. 1995, 113, 181–185. [Google Scholar]
- Chen, H.L.; Tan, C.T.; Lai, J.T.; Liu, T.C. Long-term hearing progression of Ménière’s disease. Ear Nose Throat J. 2022, 1455613221074149. [Google Scholar] [CrossRef] [PubMed]
- Sato, G.; Sekine, K.; Matsuda, K.; Ueeda, H.; Horii, A.; Nishiike, S.; Kitahara, T.; Uno, A.; Imai, T.; Inohara, H.; et al. Long-term prognosis of hearing loss in patients with unilateral Ménière’s disease. Acta Otolaryngol. 2014, 134, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Huppert, D.; Strupp, M.; Brandt, T. Long-term course of Menière’s disease revisited. Acta Otolaryngol. 2010, 130, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Wang, D.; Ren, T.; Wang, W. Auditory Manifestations of Vestibular Migraine. Front. Neurol. 2022, 13, 944001. [Google Scholar] [CrossRef] [PubMed]
- Fushiki, H.; Junicho, M.; Kanazawa, Y.; Aso, S.; Watanabe, Y. Prognosis of sudden low-tone loss other than acute low-tone sensorineural hearing loss. Acta Otolaryngol. 2010, 130, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Committee on Hearing and Equilibrium. Report of Subcommittee on Equilibrium and its Measurement. Meniere’s disease: Criteria for diagnosis and evaluation of therapy for reporting. Trans. Am. Acad. Ophthalmol. Otolaryngol. 1972, 76, 1462–1464. [Google Scholar]
- Yamasoba, T.; Kikuchi, S.; Sugasawa, M.; Yagi, M.; Harada, T. Acute low-tone sensorineural hearing loss without vertigo. Arch. Otolaryngol. Head Neck Surg. 1994, 120, 532–535. [Google Scholar] [CrossRef]
- Junicho, M.; Aso, S.; Fujisaka, M.; Watanabe, Y. Prognosis of low-tone sudden deafness—Does it inevitably progress to Meniere’s disease? Acta Otolaryngol. 2008, 128, 304–308. [Google Scholar] [CrossRef]
- Xue, J.; Ma, X.; Lin, Y.; Shan, H.; Yu, L. Audiological Findings in Patients with Vestibular Migraine and Migraine: History of Migraine May Be a Cause of Low-Tone Sudden Sensorineural Hearing Loss. Audiol. Neuro-Otol. 2020, 25, 209–214. [Google Scholar] [CrossRef]
- Lai, J.T.; Liu, T.C. Proposal for a New Diagnosis for Cochlear Migraine. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 185–186. [Google Scholar] [CrossRef]
- Pyykkö, I.; Nakashima, T.; Yoshida, T.; Zou, J.; Naganawa, S. Meniere’s disease: A reappraisal supported by a variable latency of symptoms and the MRI visualisation of endolymphatic hydrops. BMJ Open 2013, 3, e001555. [Google Scholar] [CrossRef] [PubMed]
- Perez-Garrigues, H.; Lopez-Escamez, J.A.; Perez, P.; Sanz, R.; Orts, M.; Marco, J.; Barona, R.; Tapia, M.C.; Aran, I.; Cenjor, C.; et al. Time course of episodes of definitive vertigo in Meniere’s disease. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Green, J.D., Jr.; Blum, D.J.; Harner, S.G. Longitudinal followup of patients with Menière’s disease. Otolaryngol. Head Neck Surg. 1991, 104, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Havia, M.; Kentala, E. Progression of symptoms of dizziness in Ménière’s disease. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Gibson, W.P.; Moffat, D.A.; Ramsden, R.T. Clinical electrocochleography in the diagnosis and management of Meneère’s disorder. Audiology 1977, 16, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Ziylan, F.; Smeeing, D.P.; Stegeman, I.; Thomeer, H.G. Click Stimulus Electrocochleography Versus MRI With Intratympanic Contrast in Ménière’s Disease: A Systematic Review. Otol. Neurotol. 2016, 37, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.H.; Kim, K.W.; Chang, J.; Jun, H.S.; Kwon, E.H.; Choi, J.Y.; Im, G.J.; Chae, S.W.; Jung, H.H.; Choi, J. Can we use electrocochleography as a clinical tool in the diagnosis of Meniere’s disease during the early symptomatic period? Acta Otolaryngol. 2014, 134, 771–775. [Google Scholar] [CrossRef]
- Orchik, D.J.; Shea, J.J., Jr.; Ge, N.N. Summating potential and action potential ratio in Meniere’s disease before and after treatment. Am. J. Otol. 1998, 19, 478–482. [Google Scholar]
- Kim, H.H.; Kumar, A.; Battista, R.A.; Wiet, R.J. Electrocochleography in patients with Meniere’s disease. Am. J. Otolaryngol. 2005, 26, 128–131. [Google Scholar] [CrossRef]
- Pappas, D.G., Jr.; Pappas, D.G., Sr.; Carmichael, L.; Hyatt, D.P.; Toohey, L.M. Extratympanic electrocochleography: Diagnostic and predictive value. Am. J. Otol. 2000, 21, 81–87. [Google Scholar] [CrossRef]
- Ghosh, S.; Gupta, A.K.; Mann, S.S. Can electrocochleography in Meniere’s disease be noninvasive? J. Otolaryngol. 2002, 31, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Hornibrook, J.; Kalin, C.; Lin, E.; O’Beirne, G.A.; Gourley, J. Transtympanic Electrocochleography for the Diagnosis of Ménière’s Disease. Int. J. Otolaryngol. 2012, 2012, 852714. [Google Scholar] [CrossRef] [PubMed]
- Gibson, W.P. A comparison of two methods of using transtympanic electrocochleography for the diagnosis of Meniere’s disease: Click summating potential/action potential ratio measurements and tone burst summating potential measurements. Acta Otolaryngol. Suppl. 2009, 129, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Hornibrook, J.; Flook, E.; Greig, S.; Babbage, M.; Goh, T.; Coates, M.; Care, R.; Bird, P. MRI Inner Ear Imaging and Tone Burst Electrocochleography in the Diagnosis of Ménière’s Disease. Otol. Neurotol. 2015, 36, 1109–1114. [Google Scholar] [CrossRef]
- Al-momani, M.O.; Ferraro, J.A.; Gajewski, B.J.; Ator, G. Improved sensitivity of electrocochleography in the diagnosis of Meniere’s disease. Int. J. Audiol. 2009, 48, 811–819. [Google Scholar] [CrossRef]
- Iseli, C.; Gibson, W. A comparison of three methods of using transtympanic electrocochleography for the diagnosis of Meniere’s disease: Click summating potential measurements, tone burst summating potential amplitude measurements, and biasing of the summating potential using a low frequency tone. Acta Otolaryngol. 2010, 130, 95–101. [Google Scholar]
- Lopes Kde, C.; Munhoz, M.S.; Santos, M.A.; Moraes, M.F.; Chaves, A.G. Graphic angle measure as an electrocochleography evaluation parameter. Braz. J. Otorhinolaryngol. 2011, 77, 214–220. [Google Scholar] [CrossRef]
- Ge, X.; Shea, J.J., Jr. Transtympanic electrocochleography: A 10-year experience. Otol. Neurotol. 2002, 23, 799–805. [Google Scholar] [CrossRef]
- Takeda, T.; Kakigi, A. The clinical value of extratympanic electrocochleography in the diagnosis of Ménière’s disease. ORL J. Otorhinolaryngol. Relat. Spec. 2010, 72, 196–204. [Google Scholar] [CrossRef]
- Martines, F.; Dispenza, F.; Montalbano, C.; Priola, R.; Torrente, A.; La Gumina, R.; Brighina, F.; Galletti, F.; Salvago, P. Comparison of Electrocochleography and Video Head Impulse Test findings in Vestibular Migraine and Ménière Disease: A Preliminary Study. J. Int Adv. Otol. 2020, 16, 183–189. [Google Scholar] [CrossRef]
- Yollu, U.; Uluduz, D.U.; Yilmaz, M.; Yener, H.M.; Akil, F.; Kuzu, B.; Kara, E.; Hayir, D.; Ceylan, D.; Korkut, N. Vestibular migraine screening in a migraine-diagnosed patient population, and assessment of vestibulocochlear function. Clin. Otolaryngol. 2017, 42, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Curthoys, I.S. A critical review of the neurophysiological evidence underlying clinical vestibular testing using sound, vibration and galvanic stimuli. Clin. Neurophysiol. 2010, 121, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Maheu, M.; Alvarado-Umanzor, J.M.; Delcenserie, A.; Champoux, F. The Clinical Utility of Vestibular-Evoked Myogenic Potentials in the Diagnosis of Ménière’s Disease. Front. Neurol. 2017, 8, 415. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Weng, W.J.; Jaw, F.S.; Young, Y.H. Ocular and cervical vestibular-evoked myogenic potentials: A study to determine whether air- or bone-conducted stimuli are optimal. Ear Hearth 2010, 31, 283–288. [Google Scholar] [CrossRef]
- Taylor, R.L.; Wijewardene, A.A.; Gibson, W.P.; Black, D.A.; Halmagyi, G.M.; Welgampola, M.S. The vestibular evoked-potential profile of Ménière’s disease. Clin. Neurophysiol. 2011, 122, 1256–1263. [Google Scholar] [CrossRef]
- Huang, C.H.; Wang, S.J.; Young, Y.H. Localization and prevalence of hydrops formation in Ménière’s disease using a test battery. Audiol. Neuro-Otol. 2011, 16, 41–48. [Google Scholar] [CrossRef]
- Young, Y.H.; Huang, T.W.; Cheng, P.W. Assessing the stage of Meniere’s disease using vestibular evoked myogenic potentials. Arch. Otolaryngol. Head Neck Surg. 2003, 129, 815–818. [Google Scholar] [CrossRef]
- Zhang, S.; Leng, Y.; Liu, B.; Shi, H.; Lu, M.; Kong, W. Diagnostic Value of Vestibular Evoked Myogenic Potentials in Endolymphatic Hydrops: A Meta-Analysis. Sci Rep. 2015, 5, 14951. [Google Scholar] [CrossRef]
- Fife, T.D.; Colebatch, J.G.; Kerber, K.A.; Brantberg, K.; Strupp, M.; Lee, H.; Walker, M.F.; Ashman, E.; Fletcher, J.; Callaghan, B.; et al. Practice guideline: Cervical and ocular vestibular evoked myogenic potential testing: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2017, 89, 2288–2296. [Google Scholar] [CrossRef]
- Wu, C.L.; Young, Y.H. Vestibular evoked myogenic potentials in acute low-tone sensorineural hearing loss. Laryngoscope 2004, 114, 2172–2175. [Google Scholar] [CrossRef]
- Young, Y.H.; Wu, C.C.; Wu, C.H. Augmentation of vestibular evoked myogenic potentials: An indication for distended saccular hydrops. Laryngoscope 2002, 112, 509–512. [Google Scholar] [CrossRef]
- Wu, P.H.; Chang, C.M.; Lo, W.C.; Wang, C.T.; Wen, M.H.; Huang, T.W.; Young, Y.H.; Cheng, P.W. Prediction of Unilateral Meniere’s Disease Attack Using Inner Ear Test Battery. Ear Hearth 2020, 41, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.Y.; Timmer, F.C.; Oriel, B.S.; Zhou, G.; Guinan, J.J.; Kujawa, S.G.; Herrmann, B.S.; Merchant, S.N.; Rauch, S.D. Vestibular evoked myogenic potentials (VEMP) can detect asymptomatic saccular hydrops. Laryngoscope 2006, 116, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Manzari, L.; Tedesco, A.R.; Burgess, A.M.; Curthoys, I.S. Ocular and cervical vestibular-evoked myogenic potentials to bone conducted vibration in Ménière’s disease during quiescence vs during acute attacks. Clin. Neurophysiol. 2010, 121, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Zuniga, M.G.; Janky, K.L.; Schubert, M.C.; Carey, J.P. Can vestibular-evoked myogenic potentials help differentiate Ménière disease from vestibular migraine? Otolaryngol. Head Neck Surg. 2012, 146, 788–796. [Google Scholar] [CrossRef] [PubMed]
- Inoue, A.; Egami, N.; Fujimoto, C.; Kinoshita, M.; Yamasoba, T.; Iwasaki, S. Vestibular Evoked Myogenic Potentials in Vestibular Migraine: Do They Help Differentiating From Menière’s Disease? Ann. Otol. Rhinol. Laryngol. 2016, 125, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Rizk, H.G.; Liu, Y.F.; Strange, C.C.; Van Ausdal, C.H.; English, R.C.; McRackan, T.R.; Meyer, T.A. Predictive Value of Vestibular Evoked Myogenic Potentials in the Diagnosis of Menière’s Disease and Vestibular Migraine. Otol. Neurotol. 2020, 41, 828–835. [Google Scholar] [CrossRef]
- O’Neill, G. The caloric stimulus: Mechanisms of heat transfer. Br. J. Audiol. 1995, 29, 87–94. [Google Scholar] [CrossRef]
- Valli, P.; Buizza, A.; Botta, L.; Zucca, G.; Ghezzi, L.; Valli, S. Convection, buoyancy or endolymph expansion: What is the actual mechanism responsible for the caloric response of semicircular canals? J. Vestib Res. 2002, 12, 155–165. [Google Scholar] [CrossRef]
- Cordero-Yanza, J.A.; Arrieta Vázquez, E.V.; Hernaiz Leonardo, J.C.; Mancera Sánchez, J.; Hernández Palestina, M.S.; Pérez-Fernández, N. Comparative study between the caloric vestibular and the video-head impulse tests in unilateral Menière’s disease. Acta Otolaryngol. 2017, 137, 1178–1182. [Google Scholar] [CrossRef]
- Shin, J.E.; Kim, C.H.; Park, H.J. Vestibular abnormality in patients with Meniere’s disease and migrainous vertigo. Acta Otolaryngol. 2013, 133, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.U.; Kim, H.J.; Koo, J.W.; Kim, J.S. Comparison of caloric and head-impulse tests during the attacks of Meniere’s disease. Laryngoscope 2017, 127, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Limviriyakul, S.; Luangsawang, C.; Suvansit, K.; Prakairungthong, S.; Thongyai, K.; Atipas, S. Video head impulse test and caloric test in definite Ménière’s disease. Eur. Arch. Otorhinolaryngol. 2020, 277, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Kaci, B.; Nooristani, M.; Mijovic, T.; Maheu, M. Usefulness of Video Head Impulse Test Results in the Identification of Meniere’s Disease. Front. Neurol. 2020, 11, 581527. [Google Scholar] [CrossRef]
- Mahringer, A.; Rambold, H.A. Caloric test and video-head-impulse: A study of vertigo/dizziness patients in a community hospital. Eur. Arch. Otorhinolaryngol. 2014, 271, 463–472. [Google Scholar] [CrossRef]
- van Esch, B.F.; Abolhosseini, K.; Masius-Olthof, S.; van der Zaag-Loonen, H.J.; van Benthem, P.P.G.; Bruintjes, T.D. Video-head impulse test results in patients with Menière’s disease related to duration and stage of disease. J. Vestib Res. 2018, 28, 401–407. [Google Scholar] [CrossRef]
- Hannigan, I.P.; Welgampola, M.S.; Watson, S.R.D. Dissociation of caloric and head impulse tests: A marker of Meniere’s disease. J. Neurol. 2021, 268, 431–439. [Google Scholar] [CrossRef]
- Blödow, A.; Heinze, M.; Bloching, M.B.; von Brevern, M.; Radtke, A.; Lempert, T. Caloric stimulation and video-head impulse testing in Ménière’s disease and vestibular migraine. Acta Otolaryngol. 2014, 134, 1239–1244. [Google Scholar] [CrossRef]
- Yilmaz, M.S.; Egilmez, O.K.; Kara, A.; Guven, M.; Demir, D.; Genc Elden, S. Comparison of the results of caloric and video head impulse tests in patients with Meniere’s disease and vestibular migraine. Eur. Arch. Otorhinolaryngol. 2021, 278, 1829–1834. [Google Scholar] [CrossRef]
- Nakashima, T.; Naganawa, S.; Sugiura, M.; Teranishi, M.; Sone, M.; Hayashi, H.; Nakata, S.; Katayama, N.; Ishida, I.M. Visualization of endolymphatic hydrops in patients with Meniere’s disease. Laryngoscope 2007, 117, 415–420. [Google Scholar] [CrossRef]
- Naganawa, S.; Yamazaki, M.; Kawai, H.; Bokura, K.; Sone, M.; Nakashima, T. Imaging of Ménière’s disease after intravenous administration of single-dose gadodiamide: Utility of subtraction images with different inversion time. Magn. Reson. Med. Sci. 2012, 11, 213–219. [Google Scholar] [CrossRef]
- Naganawa, S.; Suzuki, K.; Nakamichi, R.; Bokura, K.; Yoshida, T.; Sone, M.; Homann, G.; Nakashima, T.; Ikeda, M. Semi-quantification of endolymphatic size on MR imaging after intravenous injection of single-dose gadodiamide: Comparison between two types of processing strategies. Magn. Reson. Med. Sci. 2013, 12, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, T.; Naganawa, S.; Teranishi, M.; Tagaya, M.; Nakata, S.; Sone, M.; Otake, H.; Kato, K.; Iwata, T.; Nishio, N. Endolymphatic hydrops revealed by intravenous gadolinium injection in patients with Ménière’s disease. Acta Otolaryngol. 2010, 130, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Naganawa, S.; Kawai, H.; Taoka, T.; Sone, M. Improved HYDROPS: Imaging of Endolymphatic Hydrops after Intravenous Administration of Gadolinium. Magn. Reson. Med. Sci. 2017, 16, 357–361. [Google Scholar] [CrossRef]
- Bernaerts, A.; Vanspauwen, R.; Blaivie, C.; van Dinther, J.; Zarowski, A.; Wuyts, F.L.; Vanden Bossche, S.; Offeciers, E.; Casselman, J.W.; De Foer, B. The value of four stage vestibular hydrops grading and asymmetric perilymphatic enhancement in the diagnosis of Menière’s disease on MRI. Neuroradiology 2019, 61, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Baráth, K.; Schuknecht, B.; Naldi, A.M.; Schrepfer, T.; Bockisch, C.J.; Hegemann, S.C. Detection and grading of endolymphatic hydrops in Menière disease using MR imaging. AJNR Am. J. Neuroradiol. 2014, 35, 1387–1392. [Google Scholar] [CrossRef] [PubMed]
- Jasińska, A.; Lachowska, M.; Wnuk, E.; Pierchała, K.; Rowiński, O.; Niemczyk, K. Correlation between magnetic resonance imaging classification of endolymphatic hydrops and clinical manifestations and audiovestibular test results in patients with definite Ménière’s disease. Auris Nasus Larynx 2022, 49, 34–45. [Google Scholar] [CrossRef]
- Han, S.C.; Kim, Y.S.; Kim, Y.; Lee, S.-Y.; Song, J.-J.; Choi, B.Y.; Kim, J.-S.; Bae, Y.J.; Koo, J.-W. Correlation of clinical parameters with endolymphatic hydrops on MRI in Meniere’s disease. Front. Neurol. 2022, 13, 937703. [Google Scholar] [CrossRef]
- Shi, S.; Guo, P.; Li, W.; Wang, W. Clinical Features and Endolymphatic Hydrops in Patients With MRI Evidence of Hydrops. Ann. Otol. Rhinol. Laryngol. 2019, 128, 286–292. [Google Scholar] [CrossRef]
- Zhang, W.; Hui, L.; Zhang, B.; Ren, L.; Zhu, J.; Wang, F.; Li, S. The Correlation Between Endolymphatic Hydrops and Clinical Features of Meniere Disease. Laryngoscope 2021, 131, E144–E150. [Google Scholar] [CrossRef]
- Nakada, T.; Teranishi, M.; Sugiura, S.; Uchida, Y.; Naganawa, S.; Sone, M. Imaging of endolymphatic hydrops on a vertigo attack of Meniere’s disease. Nagoya J. Med. Sci. 2021, 83, 209–216. [Google Scholar]
- Chen, W.; Geng, Y.; Niu, Y.; Lin, M.; Lin, N.; Sha, Y. Endolymphatic Hydrops Magnetic Resonance Imaging in Menire’s Disease Patients on a Vertigo Attack. Otol. Neurotol. 2022, 43, 489–493. [Google Scholar] [CrossRef]
- Fukushima, M.; Akahani, S.; Inohara, H.; Takeda, N. Stability of Endolymphatic Hydrops in Ménière Disease Shown by 3-Tesla Magnetic Resonance Imaging During and After Vertigo Attacks. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 583–585. [Google Scholar] [CrossRef]
- Zhang, D.G.; Shi, H.L.; Fan, Z.M.; Wang, G.B.; Han, Y.C.; Li, Y.W.; Wang, H.B. Visualization of endolymphatic hydrops in 3D-FLAIR MRI after intratympanic Gd-DTPA administration in Meniere’s disease patients. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2013, 48, 628–633. [Google Scholar] [PubMed]
- Lin, K.T.; Lu, C.J.; Young, Y.H. Predicting positive cochlear endolymphatic hydrops on magnetic resonance images. Laryngoscope Investig. Otolaryngol. 2022, 7, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Zhang, F.; Zheng, H.; Sun, X.; Chen, J.; Chen, J.; Liu, Y.; Wang, L.; Wang, W.; Li, S.; et al. The Correlation of a 2D Volume-Referencing Endolymphatic-Hydrops Grading System With Extra-Tympanic Electrocochleography in Patients With Definite Ménière’s Disease. Front. Neurol. 2020, 11, 595038. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.T.; Lu, C.J.; Young, Y.H. Magnetic resonance imaging: Role on diagnosing all types of endolymphatic hydrops. J. Med. Assoc. 2022, 121, 1325–1333. [Google Scholar] [CrossRef]
- Kazemi, M.A.; Ghasemi, A.; Casselman, J.W.; Shafiei, M.; Zarandy, M.M.; Sharifian, H.; Hashemi, H.; Firouznia, K.; Moradi, B.; Kasani, K.; et al. Correlation of semi-quantitative findings of endolymphatic hydrops in MRI with the audiometric findings in patients with Meniere’s disease. J. Otol. 2022, 17, 123–129. [Google Scholar] [CrossRef]
- Kirsch, V.; Becker-Bense, S.; Berman, A.; Kierig, E.; Ertl-Wagner, B.; Dieterich, M. Transient endolymphatic hydrops after an attack of vestibular migraine: A longitudinal single case study. J. Neurol. 2018, 265, 51–53. [Google Scholar] [CrossRef]
- Gürkov, R.; Kantner, C.; Strupp, M.; Flatz, W.; Krause, E.; Ertl-Wagner, B. Endolymphatic hydrops in patients with vestibular migraine and auditory symptoms. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 2661–2667. [Google Scholar] [CrossRef]
- Lee, B.N.; Hwang, S.-B.; Kang, J.-J.; Oh, S.-Y. Endolymphatic Hydrops in Vestibular Migraine Associated with Menière’s Disease: A Report of Two Cases. Res. Vestib. Sci. 2021, 20, 156–160. [Google Scholar] [CrossRef]
- Oh, S.Y.; Dieterich, M.; Lee, B.N.; Boegle, R.; Kang, J.J.; Lee, N.R.; Gerb, J.; Hwang, S.B.; Kirsch, V. Endolymphatic Hydrops in Patients With Vestibular Migraine and Concurrent Meniere’s Disease. Front. Neurol. 2021, 12, 594481. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Guo, P.; Ren, T.; Wang, W. Magnetic resonance imaging of intratympanic gadolinium helps differentiate vestibular migraine from Ménière disease. Laryngoscope 2017, 127, 2382–2388. [Google Scholar] [CrossRef] [PubMed]
- Leng, Y.; Lei, P.; Chen, C.; Liu, Y.; Xia, K.; Liu, B. Non-contrast MRI of Inner Ear Detected Differences of Endolymphatic Drainage System Between Vestibular Migraine and Unilateral Ménière’s Disease. Front. Neurol. 2022, 13, 814518. [Google Scholar] [CrossRef] [PubMed]
- Basura, G.J.; Adams, M.E.; Monfared, A.; Schwartz, S.R.; Antonelli, P.J.; Burkard, R.; Bush, M.L.; Bykowski, J.; Colandrea, M.; Derebery, J. Clinical practice guideline: Ménière’s disease. Otolaryngol. Head Neck Surg. 2020, 162, S1–S55. [Google Scholar] [CrossRef]
- Caulley, L.; Quimby, A.; Karsh, J.; Ahrari, A.; Tse, D.; Kontorinis, G. Autoimmune arthritis in Ménière’s disease: A systematic review of the literature. Semin. Arthritis Rheum. 2018, 48, 141–147. [Google Scholar] [CrossRef]
- Greco, A.; Gallo, A.; Fusconi, M.; Marinelli, C.; Macri, G.F.; de Vincentiis, M. Meniere’s disease might be an autoimmune condition? Autoimmun. Rev. 2012, 11, 731–738. [Google Scholar] [CrossRef]
- De Maio, A. Extracellular Hsp70: Export and function. Curr. Protein Pept. Sci. 2014, 15, 225–231. [Google Scholar] [CrossRef]
- Gottschlich, S.; Billings, P.B.; Keithley, E.M.; Weisman, M.H.; Harris, J.P. Assessment of serum antibodies in patients with rapidly progressive sensorineural hearing loss and Menière’s disease. Laryngoscope 1995, 105, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- DiBerardino, F.; Cesarani, A.; Hahn, A.; Alpini, D. Viral infection and serum antibodies to heat shock protein 70 in the acute phase of Ménière’s disease. Int. Tinnitus J. 2007, 13, 90–93. [Google Scholar]
- Ruckenstein, M.J.; Prasthoffer, A.; Bigelow, D.C.; Von Feldt, J.M.; Kolasinski, S.L. Immunologic and serologic testing in patients with Ménière’s disease. Otol. Neurotol. 2002, 23, 517–520. [Google Scholar] [CrossRef] [PubMed]
- Rauch, S.D.; Zurakowski, D.; Bloch, D.B.; Bloch, K.J. Anti-heat shock protein 70 antibodies in Meniere’s disease. Laryngoscope 2000, 110, 1516–1521. [Google Scholar] [CrossRef] [PubMed]
- Brookes, G.B. Circulating immune complexes in Meniere’s disease. Arch. Otolaryngol. Head Neck Surg. 1986, 112, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, K.; Ohashi, T.; Urushibata, T.; Kenmochi, M.; Akagi, M. Antibodies of type II collagen and immune complexes in Menière’s disease. Acta Otolaryngol. Suppl. 1996, 522, 79–85. [Google Scholar] [PubMed]
- Derebery, M.J.; Rao, V.S.; Siglock, T.J.; Linthicum, F.H.; Nelson, R.A. Menière’s disease: An immune complex-mediated illness? Laryngoscope 1991, 101, 225–229. [Google Scholar]
- Hsu, L.; Zhu, X.N.; Zhao, Y.S. Immunoglobulin E and circulating immune complexes in endolymphatic hydrops. Ann. Otol. Rhinol. Laryngol. 1990, 99, 535–538. [Google Scholar] [CrossRef]
- Savastano, M.; Giacomelli, L.; Marioni, G. Non-specific immunological determinations in Meniere’s disease: Any role in clinical practice? Eur. Arch. Otorhinolaryngol. 2007, 264, 15–19. [Google Scholar] [CrossRef]
- Perez Garrigues, H.; Carmona, E.; Morera, C.; Sanchez-Cuenca, J.M. Circulating auto-antibodies in Ménière’s disease. Ann. Otolaryngol. Chir. Cervicofac. 1995, 112, 225–228. [Google Scholar]
- Muiño, J.C.; Carreras, R.; Ocampo, M.A.; Ferrero, M.; Romero Piffiguer, M.D.; Landa, C.; Beltramo, D. The importance of IgG auto-antibodies, anti-collagen type II specific in Menière’s disease and progressive hearing loss. Rev. Fac. Cien Med. Univ. Nac. Cordoba 1999, 56, 71–80. [Google Scholar]
- Derebery, M.J. Allergic and immunologic features of Ménière’s disease. Otolaryngol. Clin. North. Am. 2011, 44, 655–666. [Google Scholar] [CrossRef]
- Keles, E.; Gödekmerdan, A.; Kalidağ, T.; Kaygusuz, I.; Yalçin, S.; Cengiz Alpay, H.; Aral, M. Meniere’s disease and allergy: Allergens and cytokines. J. Laryngol. Otol. 2004, 118, 688–693. [Google Scholar] [CrossRef]
- Ma, Y.; Sun, Q.; Zhang, K.; Bai, L.; Du, L. High level of IgE in acute low-tone sensorineural hearing loss: A predictor for recurrence and Meniere Disease transformation. Am. J. Otolaryngol. 2021, 42, 102856. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Lyu, Y.; Guo, J.; Liu, J.; Song, Y.; Fan, Z.; Li, X.; Li, N.; Zhang, D.; Wang, H. Bidirectional Transport of IgE by CD23 in the Inner Ear of Patients with Meniere’s Disease. J. Immunol. 2022, 208, 827–838. [Google Scholar] [CrossRef] [PubMed]
- Frejo, L.; Lopez-Escamez, J.A. Cytokines and Inflammation in Meniere Disease. Clin. Exp. Otorhinolaryngol. 2022, 15, 49–59. [Google Scholar] [CrossRef]
- Frejo, L.; Gallego-Martinez, A.; Requena, T.; Martin-Sanz, E.; Amor-Dorado, J.C.; Soto-Varela, A.; Santos-Perez, S.; Espinosa-Sanchez, J.M.; Batuecas-Caletrio, A.; Aran, I.; et al. Proinflammatory cytokines and response to molds in mononuclear cells of patients with Meniere disease. Sci. Rep. 2018, 8, 5974. [Google Scholar] [CrossRef] [PubMed]
- Flook, M.; Frejo, L.; Gallego-Martinez, A.; Martin-Sanz, E.; Rossi-Izquierdo, M.; Amor-Dorado, J.C.; Soto-Varela, A.; Santos-Perez, S.; Batuecas-Caletrio, A.; Espinosa-Sanchez, J.M.; et al. Differential Proinflammatory Signature in Vestibular Migraine and Meniere Disease. Front. Immunol 2019, 10, 1229. [Google Scholar] [CrossRef]
- Zhang, S.; Gong, Y.; Liang, Y.; Wang, B.; Gao, W.; Xu, Q. Cyclophosphamide inhibits the progression of Meniere’s disease by reducing the generation of circulating immune complex. Exp. Med. 2021, 22, 1177. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, J.Y.; Lee, H.J.; Gi, M.; Kim, B.G.; Choi, J.Y. Autoimmunity as a candidate for the etiopathogenesis of Meniere’s disease: Detection of autoimmune reactions and diagnostic biomarker candidate. PLoS ONE 2014, 9, e111039. [Google Scholar] [CrossRef] [PubMed]
- Chiarella, G.; Saccomanno, M.; Scumaci, D.; Gaspari, M.; Faniello, M.C.; Quaresima, B.; Di Domenico, M.; Ricciardi, C.; Petrolo, C.; Cassandro, C.; et al. Proteomics in Ménière disease. J. Cell Physiol. 2012, 227, 308–312. [Google Scholar] [CrossRef]
- Chiarella, G.; Di Domenico, M.; Petrolo, C.; Saccomanno, M.; Rothenberger, R.; Giordano, A.; Costanzo, F.; Cassandro, E.; Cuda, G. A proteomics-driven assay defines specific plasma protein signatures in different stages of Ménière’s disease. J. Cell Biochem. 2014, 115, 1097–1100. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, T.; Okayasu, T.; Ito, T.; Fujita, H.; Ueda, K. Endolymphatic Sac Drainage Surgery and Plasma Stress Hormone Vasopressin Levels in Meniere’s Disease. Front. Neurol. 2021, 12, 722217. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Kakigi, A.; Saito, H. Antidiuretic hormone (ADH) and endolymphatic hydrops. Acta Otolaryngol. Suppl. 1995, 519, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Aoki, M.; Ando, K.; Kuze, B.; Mizuta, K.; Hayashi, T.; Ito, Y. The association of antidiuretic hormone levels with an attack of Meniere’s disease. Clin. Otolaryngol. 2005, 30, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Aoki, M.; Asai, M.; Nishihori, T.; Mizuta, K.; Ito, Y.; Ando, K. The relevance of an elevation in the plasma vasopressin levels to the pathogenesis of Meniere’s attack. J. Neuroendocr. 2007, 19, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Aoki, M.; Hayashi, H.; Kuze, B.; Mizuta, K.; Ito, Y. The association of the plasma vasopressin level during attacks with a prognosis of Meniere’s disease. Int. J. Audiol. 2010, 49, 1–6. [Google Scholar] [CrossRef]
- Lim, J.S.; Lange, M.E.; Megerian, C.A. Serum antidiuretic hormone levels in patients with unilateral Meniere’s disease. Laryngoscope 2003, 113, 1321–1326. [Google Scholar] [CrossRef]
- Hornibrook, J.; George, P.; Gourley, J. Vasopressin in definite Meniere’s disease with positive electrocochleographic findings. Acta Otolaryngol. 2011, 131, 613–617. [Google Scholar] [CrossRef]
- Wu, J.; Zhou, J.; Dong, L.; Fan, W.; Zhang, J.; Wu, C. A Mysterious Role of Arginine Vasopressin Levels in Ménière’s Disease-Meta-analysis of Clinical Studies. Otol. Neurotol. 2017, 38, 161–167. [Google Scholar] [CrossRef]
- Kitahara, T.; Doi, K.; Maekawa, C.; Kizawa, K.; Horii, A.; Kubo, T.; Kiyama, H. Meniere’s attacks occur in the inner ear with excessive vasopressin type-2 receptors. J. Neuroendocr. 2008, 20, 1295–1300. [Google Scholar] [CrossRef]
- Kitahara, T.; Okamoto, H.; Fukushima, M.; Sakagami, M.; Ito, T.; Yamashita, A.; Ota, I.; Yamanaka, T. A Two-Year Randomized Trial of Interventions to Decrease Stress Hormone Vasopressin Production in Patients with Meniere’s Disease-A Pilot Study. PLoS ONE 2016, 11, e0158309. [Google Scholar] [CrossRef]
- Yang, C.-H.; Hwang, C.-F.; Chuang, J.-H.; Lian, W.-S.; Wang, F.-S.; Huang, E.I.; Yang, M.-Y. Constant Light Dysregulates Cochlear Circadian Clock and Exacerbates Noise-Induced Hearing Loss. Int. J. Mol. Sci. 2020, 21, 7535. [Google Scholar] [PubMed]
- Yang, M.-Y.; Yang, W.-C.; Lin, P.-M.; Hsu, J.-F.; Hsiao, H.-H.; Liu, Y.-C.; Tsai, H.-J.; Chang, C.-S.; Lin, S.-F. Altered expression of circadian clock genes in human chronic myeloid leukemia. J. Biol. Rhythm. 2011, 26, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.; Hwang, C.F.; Lin, P.M.; Chuang, J.H.; Hsu, C.M.; Lin, S.F.; Yang, M.Y. Sleep Disturbance and Altered Expression of Circadian Clock Genes in Patients With Sudden Sensorineural Hearing Loss. Medicine 2015, 94, e978. [Google Scholar] [CrossRef]
- Fukuya, H.; Emoto, N.; Nonaka, H.; Yagita, K.; Okamura, H.; Yokoyama, M. Circadian expression of clock genes in human peripheral leukocytes. Biochem. Biophys. Res. Commun. 2007, 354, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Rauch, S.D. Clinical hints and precipitating factors in patients suffering from Meniere’s disease. Otolaryngol. Clin. North. Am. 2010, 43, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.; Hwang, C.F.; Tsai, N.W.; Yang, M.Y. Expression of circadian clock genes in leukocytes of patients with Meniere’s disease. Laryngoscope Investig. Otolaryngol. 2022, 7, 584–591. [Google Scholar] [CrossRef]
- Sun, Q.; Yang, Y.; Wang, Z.; Yang, X.; Gao, Y.; Zhao, Y.; Ge, W.; Liu, J.; Xu, X.; Guan, W. PER1 interaction with GPX1 regulates metabolic homeostasis under oxidative stress. Redox Biol. 2020, 37, 101694. [Google Scholar] [PubMed]
- Alicandri-Ciufelli, M.; Aggazzotti-Cavazza, E.; Cunsolo, E.; Marchioni, D.; Monzani, D.; Genovese, E.; Presutti, L. Is Ménière’s disease the ‘inner ear migraine’? A neurovascular region-based hypothesis supported by epidemiological appraisal and pathophysiological considerations. Hearth Balance Commun. 2016, 14, 63–69. [Google Scholar] [CrossRef]
- Martami, F.; Razeghi Jahromi, S.; Togha, M.; Ghorbani, Z.; Seifishahpar, M.; Saidpour, A. The serum level of inflammatory markers in chronic and episodic migraine: A case-control study. Neurol. Sci 2018, 39, 1741–1749. [Google Scholar] [CrossRef]
- Togha, M.; Razeghi Jahromi, S.; Ghorbani, Z.; Ghaemi, A.; Rafiee, P. Evaluation of Inflammatory State in Migraineurs: A Case-control Study. Iran. J. Allergy Asthma Immunol. 2020, 19, 83–90. [Google Scholar] [CrossRef]
- Hampton, K.K.; Esack, A.; Peatfield, R.C.; Grant, P.J. Elevation of plasma vasopressin in spontaneous migraine. Cephalalgia 1991, 11, 249–250. [Google Scholar] [CrossRef] [PubMed]
- Hasselblatt, M.; Köhler, J.; Volles, E.; Ehrenreich, H. Simultaneous monitoring of endothelin-1 and vasopressin plasma levels in migraine. Neuroreport 1999, 10, 423–425. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, K.S.; Dhillon, H.; Velly, A.M. The role of a potential biomarker in patients with migraine: Review and new insights. Expert Rev. Neurother. 2021, 21, 817–831. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Definite MD: |
| 1. Two or more spontaneous attacks of vertigo, each lasting 20 min to 12 h |
| 2. Audiometrically documented fluctuating low- to midfrequency sensorineural hearing loss in the affected ear on at least 1 occasion before, during, or after 1 of the episodes of vertigo |
| 3. Fluctuating aural symptoms (hearing loss, tinnitus, or fullness) in the affected ear |
| 4. Other causes excluded by other tests |
| Probable MD: |
| 1. At least 2 episodes of vertigo or dizziness lasting 20 min to 24 h |
| 2. Fluctuating aural symptoms (hearing loss, tinnitus, or fullness) in the affected ear |
| 3. Other causes excluded by other tests |
| Differentiate MD From Healthy Controls | Differentiate Hearing Levels and Stages of MD | Differentiate Vertigo Attacks with Remission in MD | Differentiate MD from VM | |
|---|---|---|---|---|
| Functional markers | ||||
| PTA | Documented audiometry is mandatory to diagnose definite MD | Stages of MD are defined by the hearing levels of the affected ear | The fluctuated hearing loss is not always related to vertigo attacks [31] | Typical MD exhibits low-tone hearing loss with progression. VM usually could recover from low-tone hearing loss [22,25]. |
| ECochG | Sensitivity: 66.7–85.7% Specificity: 80–100% [36] | Increased SP/AP ratio in patients with higher levels of hearing loss [42,48,49] and longer duration of the disease [38] | SP/AP ratio does not recover even if vertigo attacks disappear [38] | A higher proportion of abnormal ECochG in MD than VM [50] |
| VEMP | Sensitivity: 49% Specificity: 95% [58] | IAD ratio of VEMP increased in the advanced stage of MD [57] | Differ between quiescence and acute attack status [64] | MD group showed a reduction in tone-evoked amplitudes for oVEMP [65] and the prevalence of a higher IAD ratio compared to the VM group [66] |
| Caloric test/vHIT | 47–67% of patients with MD have unilateral canal weakness [70,71]. The incidence of vHIT abnormality is lower than the caloric test [78] | The incidence of canal paresis in the caloric test is higher in the advanced stage of MD [73]. No differences in abnormal vHIT results between different stages of MD [73,76]. | Caloric responses are usually diminished during the attacks of MD [72] vHIT results may differ during and between acute vertigo attacks [72,74,75] | Incidences of abnormal caloric test and vHIT are higher in MD than in VM [78] |
| MRI | sensitivity: 79.5–84.6% specificity: 92.3–93.6% [85] | MRI EH degree has a positive correlation between the hearing level and the vestibular EH degree [87,88,89,90] | The grade of EH is not correlated with the extent of vertigo [87,89]. EH is stable during and after vertigo attacks [93]. | A higher incidence of EH was observed in MD compared to VM [102,103] |
| Molecular markers | ||||
| Immunological/ autoimmunity markers | Increased HSP70 antibodies [109], CICs [117] and IgE [123] in MD | The phase of pure tone average was positively associated with HSP70 and CIC [127] IgE was correlated to the hearing stage [123] | Not determined | Not determined |
| Inflammatory markers | MD patients had higher basal level of IL-1β, IL-1RA, IL-6 and TNF-α compaed to healthy controls [125] | The phase of pure tone average was positively associated with TNF-α [127] | Not determined | Cytokine panel with IL- 1β, CCL3, CCL22, and CXCL1 levels may help to differentiate the MD from VM [126]. |
| Protein signatures | Higher several protein signatures in MD [128,129,130] | Increased fibrinogen α- and γ-chain expression in stage III and decreased β-2-glycoprotein expression in stage IV patients. Stage I individuals have a higher expression of complement factor H and B proteins [130] | Not determined | Not determined |
| Vasopressin | Vasopressin levels were higher in MD patients [132,133,134,135] or no difference between MD and controls [136,137] | Vasopressin levels did not correlate with the disease stage of MD [137] | Vasopressin levels were significantly higher in the acute phase than remission phase [132] | Not determined |
| Circadian clock genes | Decreased PER1 and increased CLOCK gene expression in the MD group compared to a healthy control group [146] | PER1 is significantly lower in patients with stage 3 and 4 compared to stage 1 and 2 [146] Down expression of PER1 was significantly correlated to the pure tone average and speech reception threshold of the affected ear [146] | Not determined | Not determined |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, C.-H.; Yang, M.-Y.; Hwang, C.-F.; Lien, K.-H. Functional and Molecular Markers for Hearing Loss and Vertigo Attacks in Meniere’s Disease. Int. J. Mol. Sci. 2023, 24, 2504. https://doi.org/10.3390/ijms24032504
Yang C-H, Yang M-Y, Hwang C-F, Lien K-H. Functional and Molecular Markers for Hearing Loss and Vertigo Attacks in Meniere’s Disease. International Journal of Molecular Sciences. 2023; 24(3):2504. https://doi.org/10.3390/ijms24032504
Chicago/Turabian StyleYang, Chao-Hui, Ming-Yu Yang, Chung-Feng Hwang, and Kuang-Hsu Lien. 2023. "Functional and Molecular Markers for Hearing Loss and Vertigo Attacks in Meniere’s Disease" International Journal of Molecular Sciences 24, no. 3: 2504. https://doi.org/10.3390/ijms24032504
APA StyleYang, C.-H., Yang, M.-Y., Hwang, C.-F., & Lien, K.-H. (2023). Functional and Molecular Markers for Hearing Loss and Vertigo Attacks in Meniere’s Disease. International Journal of Molecular Sciences, 24(3), 2504. https://doi.org/10.3390/ijms24032504