
Pembrolizumab Plus Axitinib for Metastatic Papillary and Chromophobe Renal Cell Carcinoma: NEMESIA (Non Clear MEtaStatic Renal Cell Carcinoma Pembrolizumab Axitinib) Study, a Subgroup Analysis of I-RARE Observational Study (Meet-URO 23a)

 ,
,  ,
,  , , , , , , ,
, , , , , , , 
Abstract
1. Introduction
2. Results
2.1. Overall Population
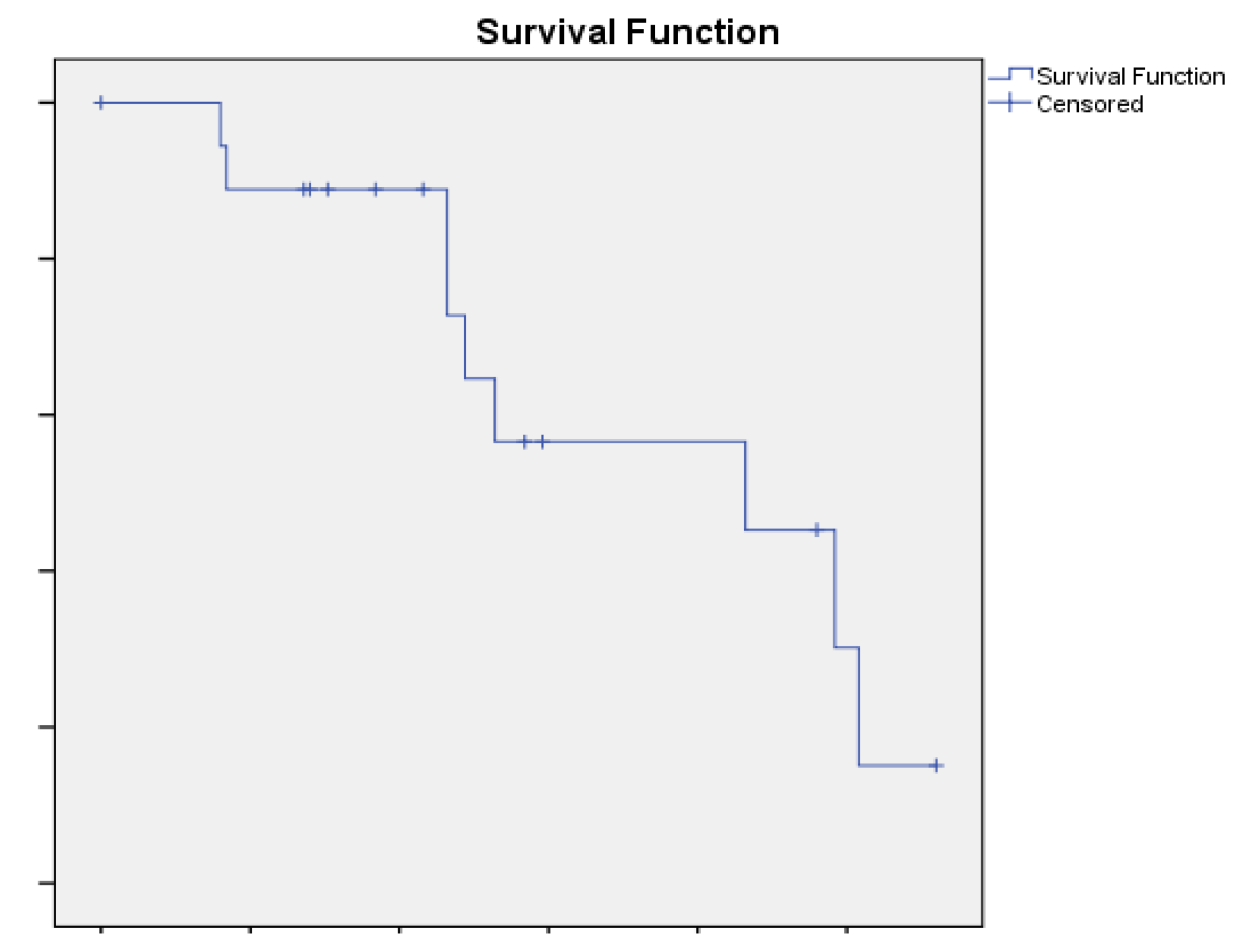
2.2. Chromophobe Renal Cell Carcinoma
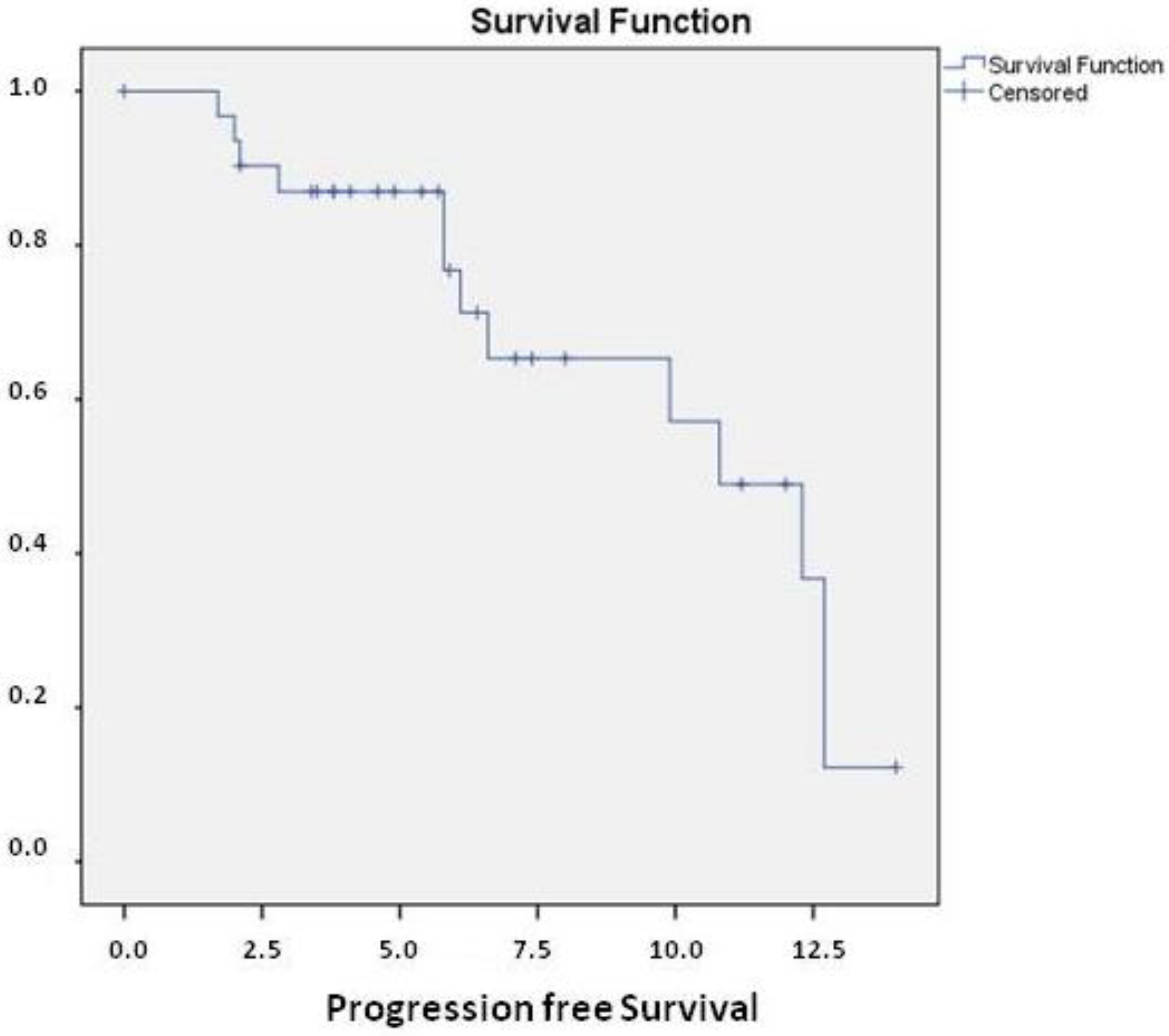
2.3. Papillary Renal Cell Carcinoma
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, J.J.; Purdue, M.P.; Signoretti, S.; Swanton, C.; Albiges, L.; Schmidinger, M.; Heng, D.Y.; Larkin, J.; Ficarra, V. Renal cell carcinoma. Nat. Rev. Dis. Prim. 2017, 3, 17009. [Google Scholar] [CrossRef]
- Linehan, W.M.; Spellman, P.T.; Ricketts, C.J.; Creighton, C.J.; Fei, S.S.; Davis, C.; Wheeler, D.A.; Murray, B.A.; Schmidt, L.; Vocke, C.D.; et al. Comprehensive Molecular Characterization of Papillary Renal-Cell Carcinoma. N. Engl. J. Med. 2016, 374, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.F.; Ricketts, C.J.; Wang, M.; Yang, L.; Cherniack, A.D.; Shen, H.; Buhay, C.; Kang, H.; Kim, S.C.; Fahey, C.C.; et al. The somatic genomic landscape of chromophobe renal cell carcinoma. Cancer Cell 2014, 26, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.J.; Halabi, S.; Eisen, T.; Broderick, S.; Stadler, W.M.; Jones, R.J.; Garcia, J.A.; Vaishampayan, U.N.; Picus, J.; Hawkins, R.E.; et al. Everolimus versus sunitinib for patients with metastatic non-clear cell renal cell carcinoma (ASPEN): A multicentre, open-label, randomised phase 2 trial. Lancet. Oncol. 2016, 17, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Tannir, N.M.; Jonasch, E.; Albiges, L.; Altinmakas, E.; Ng, C.S.; Matin, S.F.; Wang, X.; Qiao, W.; Dubauskas Lim, Z.; Tamboli, P.; et al. Everolimus Versus Sunitinib Prospective Evaluation in Metastatic Non-Clear Cell Renal Cell Carcinoma (ESPN): A Randomized Multicenter Phase 2 Trial. Eur. Urol. 2016, 69, 866–874. [Google Scholar] [CrossRef]
- Schöffski, P.; Wozniak, A.; Escudier, B.; Rutkowski, P.; Anthoney, A.; Bauer, S.; Sufliarsky, J.; van Herpen, C.; Lindner, L.H.; Grünwald, V.; et al. Crizotinib achieves long-lasting disease control in advanced papillary renal-cell carcinoma type 1 patients with MET mutations or amplification. EORTC 90101 CREATE trial. Eur. J. Cancer 2017, 87, 147–163. [Google Scholar] [CrossRef]
- Pal, S.K.; Tangen, C.; Thompson, I.M.J.; Balzer-Haas, N.; George, D.J.; Heng, D.Y.C.; Shuch, B.; Stein, M.; Tretiakova, M.; Humphrey, P.; et al. A comparison of sunitinib with cabozantinib, crizotinib, and savolitinib for treatment of advanced papillary renal cell carcinoma: A randomised, open-label, phase 2 trial. Lancet 2021, 397, 695–703. [Google Scholar] [CrossRef]
- Watanabe, H.; Okada, M.; Kaji, Y.; Satouchi, M.; Sato, Y.; Yamabe, Y.; Onaya, H.; Endo, M.; Sone, M.; Arai, Y. New response evaluation criteria in solid tumours-Revised RECIST Guideline (version 1.1). Jpn. J. Cancer Chemother. 2009, 36, 2495–2501. [Google Scholar]
- Mendhiratta, N.; Muraki, P.; Sisk, A.E.J.; Shuch, B. Papillary renal cell carcinoma: Review. Urol. Oncol. 2021, 39, 327–337. [Google Scholar] [CrossRef]
- Garje, R.; Elhag, D.; Yasin, H.A.; Acharya, L.; Vaena, D.; Dahmoush, L. Comprehensive review of chromophobe renal cell carcinoma. Crit. Rev. Oncol. Hematol. 2021, 160, 103287. [Google Scholar] [CrossRef]
- Cheville, J.C.; Lohse, C.M.; Zincke, H.; Weaver, A.L.; Blute, M.L. Comparisons of outcome and prognostic features among histologic subtypes of renal cell carcinoma. Am. J. Surg. Pathol. 2003, 27, 612–624. [Google Scholar] [CrossRef]
- Pignot, G.; Elie, C.; Conquy, S.; Vieillefond, A.; Flam, T.; Zerbib, M.; Debré, B.; Amsellem-Ouazana, D. Survival analysis of 130 patients with papillary renal cell carcinoma: Prognostic utility of type 1 and type 2 subclassification. Urology 2007, 69, 230–235. [Google Scholar] [CrossRef]
- Stellato, M.; Santini, D. ImmuneOncology-tyrosine kinase inhibitors combination, sometimes less is more. Int. Immunopharmacol. 2021, 98, 107673. [Google Scholar] [CrossRef]
- Sepe, P.; Ottini, A.; Pircher, C.C.; Franza, A.; Claps, M.; Guadalupi, V.; Verzoni, E.; Procopio, G. Characteristics and Treatment Challenges of Non-Clear Cell Renal Cell Carcinoma. Cancers 2021, 13, 3807. [Google Scholar] [CrossRef]
- Graham, J.; Wells, J.C.; Dudani, S.; Gan, C.L.; Donskov, F.; Lee, J.-L.; Kollmannsberger, C.K.; Meza, L.; Beuselinck, B.; Hansen, A.; et al. Outcomes of patients with advanced non-clear cell renal cell carcinoma treated with first-line immune checkpoint inhibitor therapy. Eur. J. Cancer 2022, 171, 124–132. [Google Scholar] [CrossRef]
- Procopio, G.; Sepe, P.; Claps, M.; Buti, S.; Colecchia, M.; Giannatempo, P.; Guadalupi, V.; Mariani, L.; Lalli, L.; Fucà, G.; et al. Cabozantinib as First-line Treatment in Patients With Metastatic Collecting Duct Renal Cell Carcinoma: Results of the BONSAI Trial for the Italian Network for Research in Urologic-Oncology (Meet-URO 2 Study). JAMA Oncol. 2022, 8, 910–913. [Google Scholar] [CrossRef]
- Escudier, B.; Porta, C.; Schmidinger, M.; Rioux-Leclercq, N.; Bex, A.; Khoo, V.; Grünwald, V.; Gillessen, S.; Horwich, A. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 706–720. [Google Scholar] [CrossRef]
- Powles, T.; Albiges, L.; Bex, A.; Grünwald, V.; Porta, C.; Procopio, G.; Schmidinger, M.; Suárez, C.; de Velasco, G. ESMO Clinical Practice Guideline update on the use of immunotherapy in early stage and advanced renal cell carcinoma. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1511–1519. [Google Scholar] [CrossRef]
- McDermott, D.F.; Lee, J.-L.; Ziobro, M.; Suarez, C.; Langiewicz, P.; Matveev, V.B.; Wiechno, P.; Gafanov, R.A.; Tomczak, P.; Pouliot, F.; et al. Open-Label, Single-Arm, Phase II Study of Pembrolizumab Monotherapy as First-Line Therapy in Patients With Advanced Non-Clear Cell Renal Cell Carcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 1029–1039. [Google Scholar] [CrossRef]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (%) | |
|---|---|
| Median Age | 68 yrs |
| M | 23/32 (72) |
| F | 9/32 (28) |
| Chromophobe RCC | 13/32 (40) |
| Papillary RCC | 19/32 (60) |
| Sarcomatoid features | 3/32 (9) |
| IMDC score | |
| good | 4/32 (12) |
| intermediate | 20/32 (62) |
| Poor | 8/32 (25) |
| Previous Nephrectomy | 23/32 (72) |
| Cytoreductive Nephrectomy | 17/32 (53) |
| ECOG PS | |
| 0 | 21/32 (65) |
| 1 | 7/32 (22) |
| 2 | 5/32 (13) |
| Synchronous metastatic disease | 13/32 (40) |
| Bone met | 4/32 (12) |
| Liver met | 13/32 (40) |
| Lung met | 8/32 (25) |
| Nodes met | 24/32 (75) |
| Overall Population (n = 32) | Chromophobe Histology (n = 13) | Papillary Histology (n = 19) | |
|---|---|---|---|
| CR | 0 | 0 | 0 |
| PR | 14 (43.8) | 5 (16.1) | 9 (19.3) |
| SD | 11 (34.3) | 5 (19.3) | 6 (16.1) |
| PD | 6 (18.8) | 2 (12.9) | 4 (6.4) |
| NE | 1 (3.1) | 1 (3.1) | |
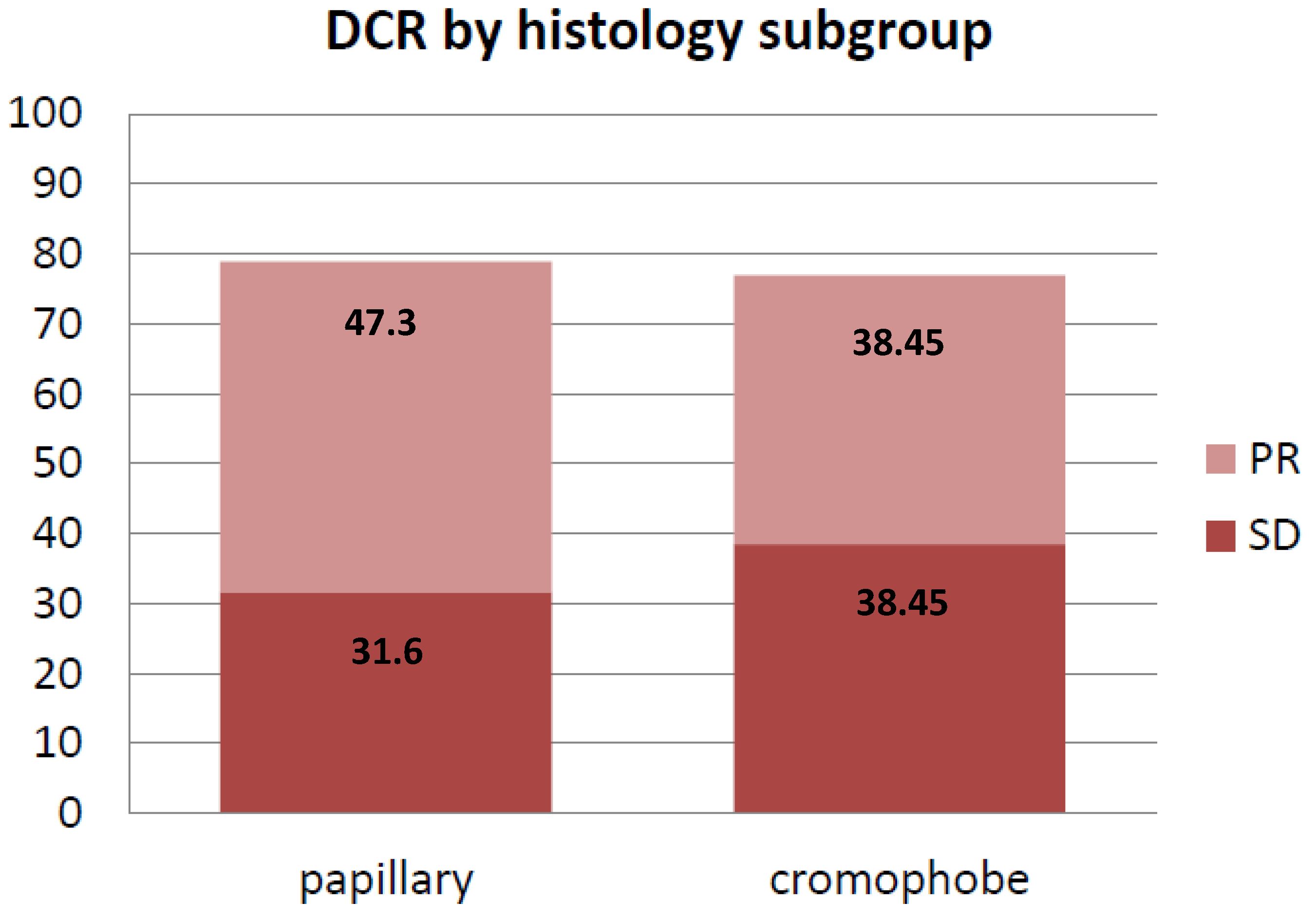
| DCR | 78.1% | 78.9% | 76.9% |
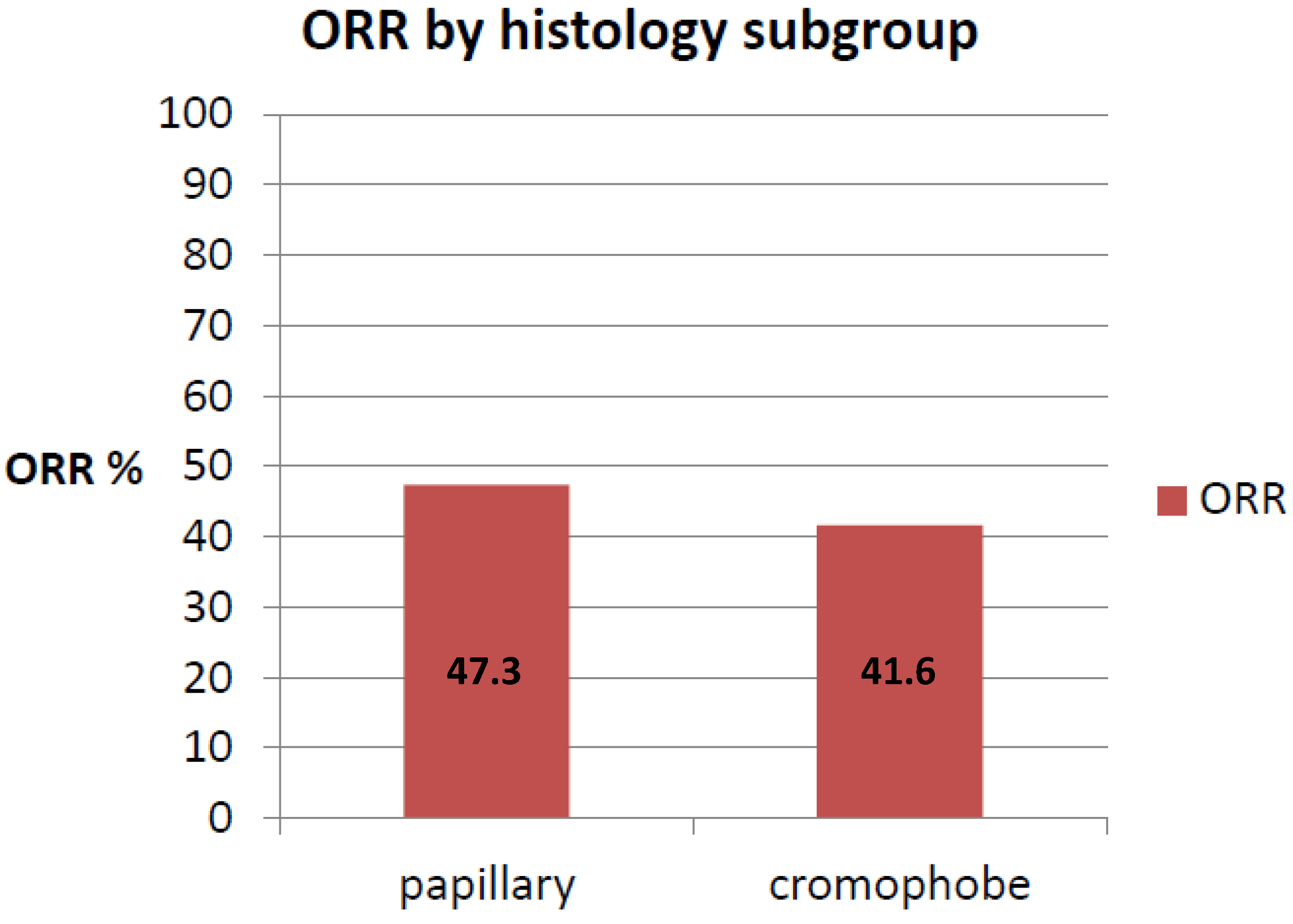
| ORR | 43.7% | 41.6% | 47.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stellato, M.; Buti, S.; Maruzzo, M.; Bersanelli, M.; Pierantoni, F.; De Giorgi, U.; Di Napoli, M.; Iacovelli, R.; Vitale, M.G.; Ermacora, P.; et al. Pembrolizumab Plus Axitinib for Metastatic Papillary and Chromophobe Renal Cell Carcinoma: NEMESIA (Non Clear MEtaStatic Renal Cell Carcinoma Pembrolizumab Axitinib) Study, a Subgroup Analysis of I-RARE Observational Study (Meet-URO 23a). Int. J. Mol. Sci. 2023, 24, 1096. https://doi.org/10.3390/ijms24021096
Stellato M, Buti S, Maruzzo M, Bersanelli M, Pierantoni F, De Giorgi U, Di Napoli M, Iacovelli R, Vitale MG, Ermacora P, et al. Pembrolizumab Plus Axitinib for Metastatic Papillary and Chromophobe Renal Cell Carcinoma: NEMESIA (Non Clear MEtaStatic Renal Cell Carcinoma Pembrolizumab Axitinib) Study, a Subgroup Analysis of I-RARE Observational Study (Meet-URO 23a). International Journal of Molecular Sciences. 2023; 24(2):1096. https://doi.org/10.3390/ijms24021096
Chicago/Turabian StyleStellato, Marco, Sebastiano Buti, Marco Maruzzo, Melissa Bersanelli, Francesco Pierantoni, Ugo De Giorgi, Marilena Di Napoli, Roberto Iacovelli, Maria Giuseppa Vitale, Paola Ermacora, and et al. 2023. "Pembrolizumab Plus Axitinib for Metastatic Papillary and Chromophobe Renal Cell Carcinoma: NEMESIA (Non Clear MEtaStatic Renal Cell Carcinoma Pembrolizumab Axitinib) Study, a Subgroup Analysis of I-RARE Observational Study (Meet-URO 23a)" International Journal of Molecular Sciences 24, no. 2: 1096. https://doi.org/10.3390/ijms24021096
APA StyleStellato, M., Buti, S., Maruzzo, M., Bersanelli, M., Pierantoni, F., De Giorgi, U., Di Napoli, M., Iacovelli, R., Vitale, M. G., Ermacora, P., Malgeri, A., Maiorano, B. A., Prati, V., Mennitto, A., Cavo, A., Santoni, M., Carella, C., Fratino, L., Procopio, G., ... Santini, D. (2023). Pembrolizumab Plus Axitinib for Metastatic Papillary and Chromophobe Renal Cell Carcinoma: NEMESIA (Non Clear MEtaStatic Renal Cell Carcinoma Pembrolizumab Axitinib) Study, a Subgroup Analysis of I-RARE Observational Study (Meet-URO 23a). International Journal of Molecular Sciences, 24(2), 1096. https://doi.org/10.3390/ijms24021096