
D-Chiro-Inositol in Endometrial Hyperplasia: A Pilot Study

 and
and
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Troìa, L.; Martone, S.; Morgante, G.; Luisi, S. Management of perimenopause disorders: Hormonal treatment. Gynecol. Endocrinol. 2021, 37, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.R.; Lumsden, M.A. Abnormal uterine bleeding in perimenopause. Climacteric 2017, 20, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Montanino Oliva, M.; Gambioli, R.; Forte, G.; Porcaro, G.; Aragona, C.; Unfer, V. Unopposed estrogens: Current and future perspectives. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2975–2989. [Google Scholar] [CrossRef]
- Patel, S.; Homaei, A.; Raju, A.B.; Meher, B.R. Estrogen: The necessary evil for human health, and ways to tame it. Biomed. Pharmacother. 2018, 102, 403–411. [Google Scholar] [CrossRef]
- Goad, J.; Ko, Y.A.; Kumar, M.; Jamaluddin, M.F.B.; Tanwar, P.S. Oestrogen fuels the growth of endometrial hyperplastic lesions initiated by overactive Wnt/β-catenin signalling. Carcinogenesis 2018, 39, 1105–1116. [Google Scholar] [CrossRef]
- Simpson, E.R. Aromatase: Biologic relevance of tissue-specific expression. Semin. Reprod. Med. 2004, 22, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Zahid, H.; Simpson, E.R.; Brown, K.A. Inflammation, dysregulated metabolism and aromatase in obesity and breast cancer. Curr. Opin. Pharmacol. 2016, 31, 90–96. [Google Scholar] [CrossRef]
- Nappi, R.E.; Albani, F.; Santamaria, V.; Tonani, S.; Magri, F.; Martini, E.; Chiovato, L.; Polatti, F. Hormonal and psycho-relational aspects of sexual function during menopausal transition and at early menopause. Maturitas 2010, 67, 78–83. [Google Scholar] [CrossRef]
- Strissel, P.L.; Ellmann, S.; Loprich, E.; Thiel, F.; Fasching, P.A.; Stiegler, E.; Hartmann, A.; Beckmann, M.W.; Strick, R. Early aberrant insulin-like growth factor signaling in the progression to endometrial carcinoma is augmented by tamoxifen. Int. J. Cancer 2008, 123, 2871–2879. [Google Scholar] [CrossRef]
- Unfer, V.; Simona, D.; Sara, R.; Sandro, G. Adjuvant treatment with D-chiro-inositol: A possible therapeutic strategy for insulin resistant and obese women with endometrial hyperplasia? Med. Hypotheses 2022, 164, 110860. [Google Scholar] [CrossRef]
- Guerin, J.; Engelmann, A.; Mattamana, M.; Borgelt, L.M. Use of hormonal contraceptives in perimenopause: A systematic review. Pharmacotherapy 2022, 42, 154–164. [Google Scholar] [CrossRef]
- Clement, N.S.; Oliver, T.R.; Shiwani, H.; Sanner, J.R.; Mulvaney, C.A.; Atiomo, W. Metformin for endometrial hyperplasia. Cochrane Database Syst. Rev. 2017, 10, Cd012214. [Google Scholar] [CrossRef]
- Yang, B.Y.; Gulinazi, Y.; Du, Y.; Ning, C.C.; Cheng, Y.L.; Shan, W.W.; Luo, X.Z.; Zhang, H.W.; Zhu, Q.; Ma, F.H.; et al. Metformin plus megestrol acetate compared with megestrol acetate alone as fertility-sparing treatment in patients with atypical endometrial hyperplasia and well-differentiated endometrial cancer: A randomised controlled trial. BJOG 2020, 127, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Barker, L.C.; Brand, I.R.; Crawford, S.M. Sustained effect of the aromatase inhibitors anastrozole and letrozole on endometrial thickness in patients with endometrial hyperplasia and endometrial carcinoma. Curr. Med. Res. Opin. 2009, 25, 1105–1109. [Google Scholar] [CrossRef] [PubMed]
- Straubhar, A.; Soisson, A.P.; Dodson, M.; Simons, E. Successful treatment of low-grade endometrial cancer in premenopausal women with an aromatase inhibitor after failure with oral or intrauterine progesterone. Gynecol. Oncol. Rep. 2017, 21, 10–12. [Google Scholar] [CrossRef]
- Laganà, A.S.; Garzon, S.; Unfer, V. New clinical targets of d-chiro-inositol: Rationale and potential applications. Expert Opin. Drug Metab. Toxicol. 2020, 16, 703–710. [Google Scholar] [CrossRef]
- Gambioli, R.; Forte, G.; Aragona, C.; Bevilacqua, A.; Bizzarri, M.; Unfer, V. The use of D-chiro-Inositol in clinical practice. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 438–446. [Google Scholar] [CrossRef]
- Gambioli, R.; Montanino Oliva, M.; Nordio, M.; Chiefari, A.; Puliani, G.; Unfer, V. New Insights into the Activities of D-Chiro-Inositol: A Narrative Review. Biomedicines 2021, 9, 1378. [Google Scholar] [CrossRef]
- Dinicola, S.; Unfer, V.; Facchinetti, F.; Soulage, C.O.; Greene, N.D.; Bizzarri, M.; Laganà, A.S.; Chan, S.Y.; Bevilacqua, A.; Pkhaladze, L.; et al. Inositols: From Established Knowledge to Novel Approaches. Int. J. Mol. Sci. 2021, 22, 10575. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, A.; Dragotto, J.; Lucarelli, M.; Di Emidio, G.; Monastra, G.; Tatone, C. High Doses of D-Chiro-Inositol Alone Induce a PCO-Like Syndrome and Other Alterations in Mouse Ovaries. Int. J. Mol. Sci. 2021, 22, 5691. [Google Scholar] [CrossRef]
- Monastra, G.; Vucenik, I.; Harrath, A.H.; Alwasel, S.H.; Kamenov, Z.A.; Laganà, A.S.; Monti, N.; Fedeli, V.; Bizzarri, M. PCOS and Inositols: Controversial Results and Necessary Clarifications. Basic Differences Between D-Chiro and Myo-Inositol. Front. Endocrinol. 2021, 12, 660381. [Google Scholar] [CrossRef] [PubMed]
- Unfer, V.; Dinicola, S.; Russo, M. A PCOS Paradox: Does Inositol Therapy Find a Rationale in All the Different Phenotypes? Int. J. Mol. Sci. 2023, 24, 6213. [Google Scholar] [CrossRef]
- Bizzarri, M.; Monti, N.; Piombarolo, A.; Angeloni, A.; Verna, R. Myo-Inositol and D-Chiro-Inositol as Modulators of Ovary Steroidogenesis: A Narrative Review. Nutrients 2023, 15, 1875. [Google Scholar] [CrossRef] [PubMed]
- MacLean, J.A., 2nd; Hayashi, K. Progesterone Actions and Resistance in Gynecological Disorders. Cells 2022, 11, 647. [Google Scholar] [CrossRef]
- Park, Y.R.; Lee, S.W.; Kim, Y.; Bae, I.Y.; Kim, H.K.; Choe, J.; Kim, Y.M. Endometrial thickness cut-off value by transvaginal ultrasonography for screening of endometrial pathology in premenopausal and postmenopausal women. Obstet. Gynecol. Sci. 2019, 62, 445–453. [Google Scholar] [CrossRef]
- Tsuda, H.; Ito, Y.M.; Todo, Y.; Iba, T.; Tasaka, K.; Sutou, Y.; Hirai, K.; Dozono, K.; Dobashi, Y.; Manabe, M.; et al. Measurement of endometrial thickness in premenopausal women in office gynecology. Reprod. Med. Biol. 2018, 17, 29–35. [Google Scholar] [CrossRef]
- Geirsson, R.T.; Gemzell-Danielsson, K. Heavy menstrual bleeding and quality of life. Acta Obstet. Gynecol. Scand. 2014, 93, 617–618. [Google Scholar] [CrossRef]
- Auclair, M.H.; Yong, P.J.; Salvador, S.; Thurston, J.; Colgan, T.T.J.; Sebastianelli, A. Guideline No. 390-Classification and Management of Endometrial Hyperplasia. J. Obstet. Gynaecol. Can. 2019, 41, 1789–1800. [Google Scholar] [CrossRef] [PubMed]
- Bofill Rodriguez, M.; Lethaby, A.; Jordan, V. Progestogen-releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2020, 6, Cd002126. [Google Scholar] [CrossRef]
- Joo, J.K.; Shin, J.H.; Lee, J.R.; Kim, M.R. Levonorgestrel-Releasing Intrauterine System Use in Perimenopausal Women. J. Menopausal Med. 2021, 27, 49–57. [Google Scholar] [CrossRef]
- Kamenov, Z.; Gateva, A. Inositols in PCOS. Molecules 2020, 25, 5566. [Google Scholar] [CrossRef]
- Sacchi, S.; Marinaro, F.; Tondelli, D.; Lui, J.; Xella, S.; Marsella, T.; Tagliasacchi, D.; Argento, C.; Tirelli, A.; Giulini, S.; et al. Modulation of gonadotrophin induced steroidogenic enzymes in granulosa cells by d-chiroinositol. Reprod. Biol. Endocrinol. 2016, 14, 52. [Google Scholar] [CrossRef] [PubMed]
- Nestler, J.E.; Jakubowicz, D.J.; Reamer, P.; Gunn, R.D.; Allan, G. Ovulatory and metabolic effects of D-chiro-inositol in the polycystic ovary syndrome. N. Engl. J. Med. 1999, 340, 1314–1320. [Google Scholar] [CrossRef] [PubMed]
- Cheang, K.I.; Baillargeon, J.P.; Essah, P.A.; Ostlund, R.E., Jr.; Apridonize, T.; Islam, L.; Nestler, J.E. Insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator correlates with insulin sensitivity in women with polycystic ovary syndrome. Metabolism 2008, 57, 1390–1397. [Google Scholar] [CrossRef]
- Nestler, J.E. Regulation of the aromatase activity of human placental cytotrophoblasts by insulin, insulin-like growth factor-I, and -II. J. Steroid Biochem. Mol. Biol. 1993, 44, 449–457. [Google Scholar] [CrossRef]
- Nordio, M.; Bezerra Espinola, M.S.; Bilotta, G.; Capoccia, E.; Montanino Oliva, M. Long-Lasting Therapies with High Doses of D-chiro-inositol: The Downside. J. Clin. Med. 2023, 12, 390. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Baseline | End of Study | p-Values |
|---|---|---|---|
| Height (m) | 1.65 ± 0.07 | 1.65 ± 0.07 | 1 |
| Weight (kg) | 64.08 ± 5.35 | 63.77 ± 4.76 | 0.17 |
| BMI (kg/m2) | 23.63 ± 1.53 | 23.52 ± 1.39 | 0.18 |
| Outcome | p-Value | Adjusted p-Value | Adjusted Significance |
|---|---|---|---|
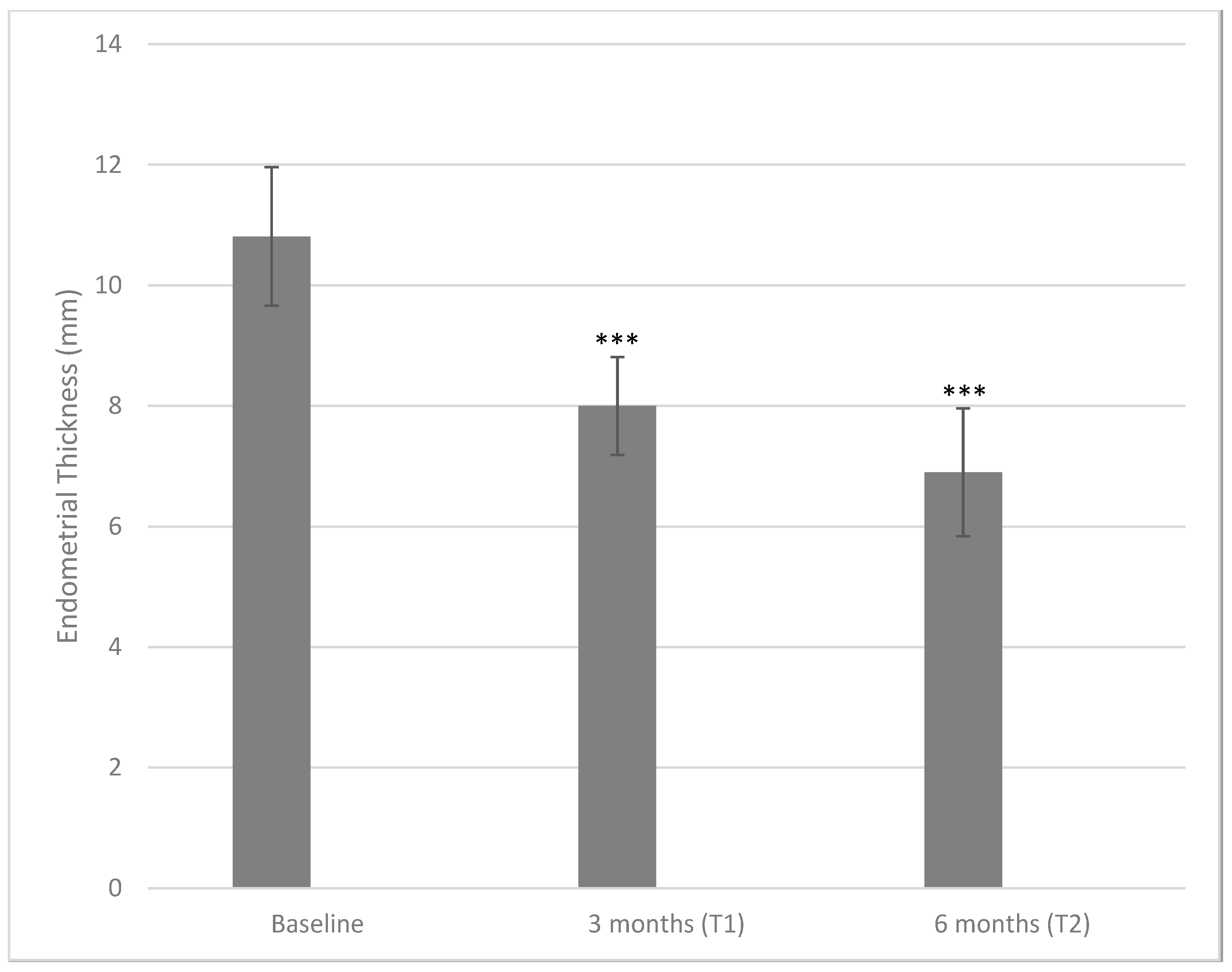
| Endometrial thickness T0 versus T1 | <0.001 | 0.006 | ** |
| Endometrial thickness T0 versus T2 | <0.001 | 0.006 | ** |
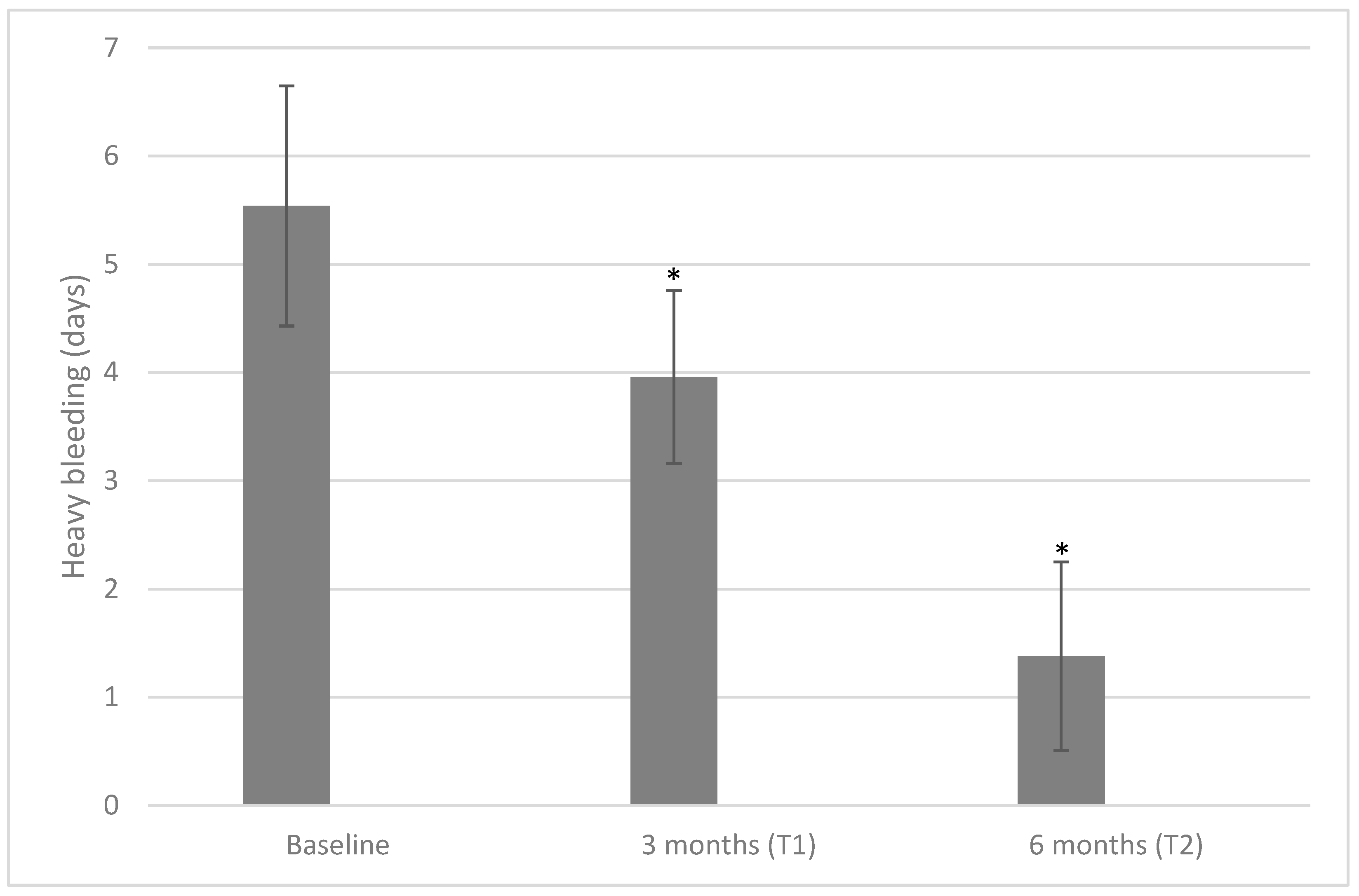
| Days of heavy bleeding T0 versus T2 | <0.001 | 0.007 | ** |
| Days of heavy bleeding T1 versus T2 | <0.001 | 0.008 | ** |
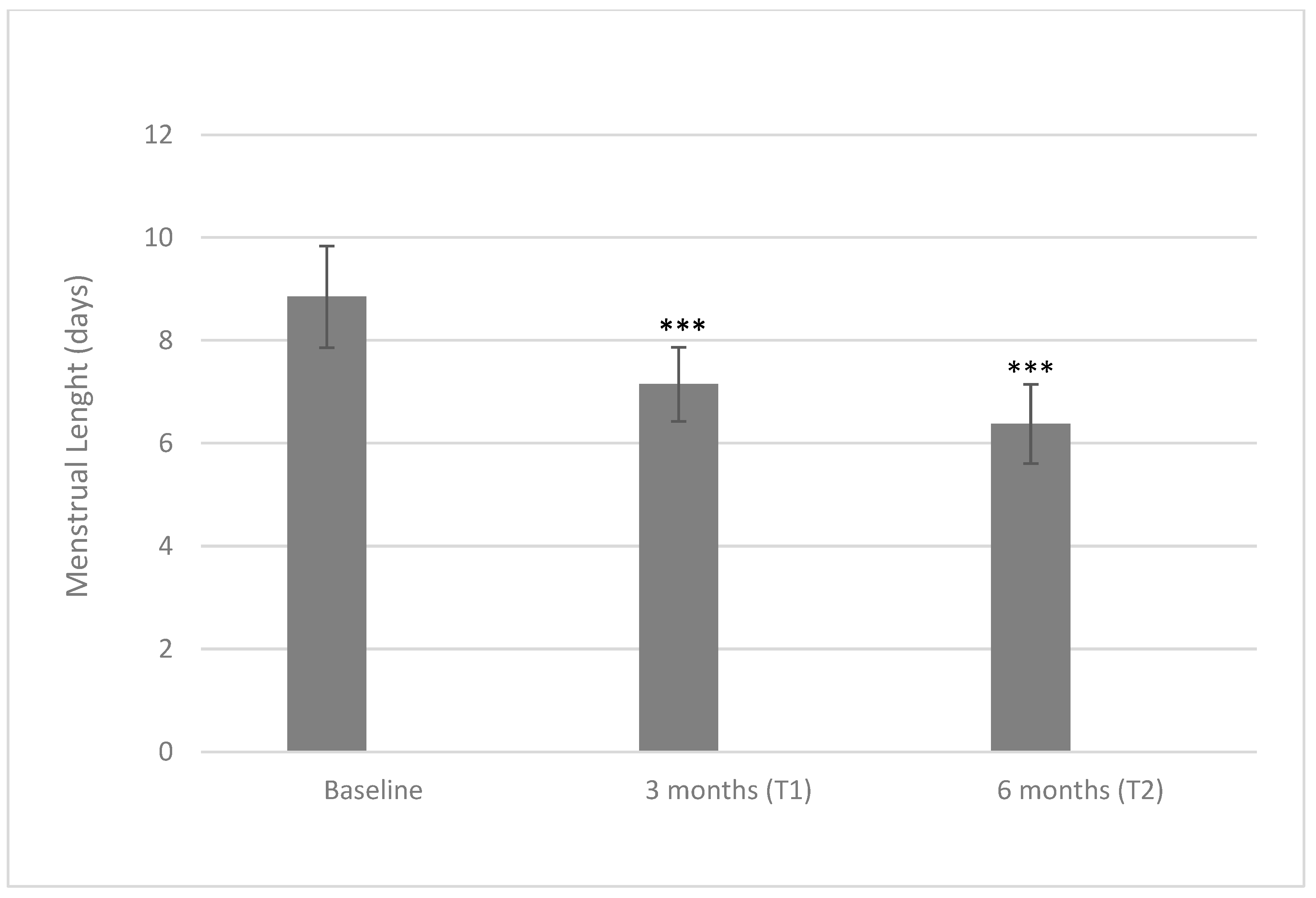
| Menstruation length T0 versus T2 | <0.001 | 0.010 | * |
| Menstruation length T0 versus T1 | <0.001 | 0.012 | * |
| Endometrial thickness T1 versus T2 | <0.001 | 0.016 | * |
| Days of heavy bleeding T0 versus T1 | <0.001 | 0.025 | * |
| Menstruation length T1 versus T2 | <0.001 | 0.049 | * |
| Hormone | Baseline | End of Study | p-Values |
|---|---|---|---|
| FSH (mUI/mL) | 7.97 ± 1.36 | 8.07 ± 1.14 | 0.70 |
| LH (mUI/mL) | 12.56 ± 0.83 | 12.63 ± 0.84 | 0.61 |
| FSH/LH | 0.63 ± 0.10 | 0.64 ± 0.09 | 0.72 |
| TSH (mcUI/mL) | 2.59 ± 0.54 | 2.58 ± 0.40 | 0.87 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porcaro, G.; Bilotta, G.; Capoccia, E.; Bezerra Espinola, M.S.; Aragona, C. D-Chiro-Inositol in Endometrial Hyperplasia: A Pilot Study. Int. J. Mol. Sci. 2023, 24, 10080. https://doi.org/10.3390/ijms241210080
Porcaro G, Bilotta G, Capoccia E, Bezerra Espinola MS, Aragona C. D-Chiro-Inositol in Endometrial Hyperplasia: A Pilot Study. International Journal of Molecular Sciences. 2023; 24(12):10080. https://doi.org/10.3390/ijms241210080
Chicago/Turabian StylePorcaro, Giuseppina, Gabriele Bilotta, Elena Capoccia, Maria Salomé Bezerra Espinola, and Cesare Aragona. 2023. "D-Chiro-Inositol in Endometrial Hyperplasia: A Pilot Study" International Journal of Molecular Sciences 24, no. 12: 10080. https://doi.org/10.3390/ijms241210080
APA StylePorcaro, G., Bilotta, G., Capoccia, E., Bezerra Espinola, M. S., & Aragona, C. (2023). D-Chiro-Inositol in Endometrial Hyperplasia: A Pilot Study. International Journal of Molecular Sciences, 24(12), 10080. https://doi.org/10.3390/ijms241210080