
Characterization of Systemic and Culprit-Coronary Artery miR-483-5p Expression in Chronic CAD and Acute Myocardial Infarction Male Patients
 ,
,  and
and
Abstract
1. Introduction
2. Results
2.1. Patient Groups and Prevalence of Previous History
2.2. MiRNA Expression in Chronic CAD and Acute MI
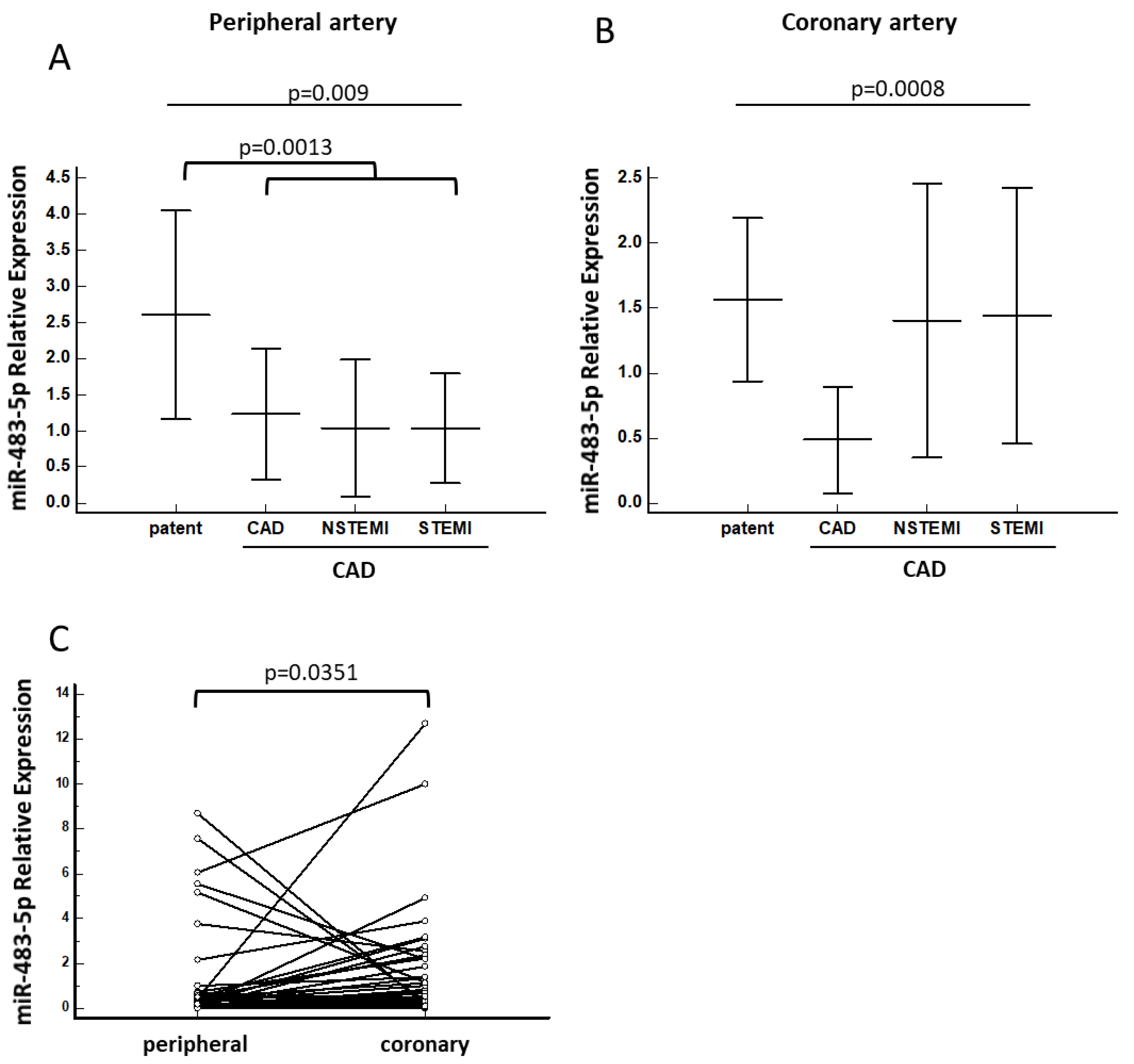
2.3. MiR-483-5p Regulation in Chronic CAD and Acute MI
2.4. Cardiovascular Disease-Related Medications and Their Association within the Study Groups
2.5. Predicted Gene Target for miR-483-5p
3. Discussion
4. Materials and Methods
4.1. Patient Recruitment and Sample Collection
4.2. RNA Extraction
4.3. Preparation of Libraries and miRNA Sequencing
4.4. Quantitative Real Time PCR (qPCR)
4.5. Bioinformatics and Statistical Analysis
4.6. Identification of Predicted Gene Targets for miR-483-5p
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADAMTS2 | ADAM metallopeptidase with thrombospondin type-1 motif -2 |
| ANOVA | One-way analysis of variance |
| CAD | Coronary artery disease |
| CRP | C-reactive protein |
| DNAAF10 | Dynein axonemal assembly factor 10 |
| dsDNA | Double-stranded Deoxyribonucleic Acid |
| GFR | Glomerular Filtration Rate |
| GRK2 | G protein-coupled receptor kinase 2 |
| HGSNAT | Heparan-alpha-glucosaminide N-acetyltransferase |
| IGF2 | Insulin-like growth factor-2 |
| IL-6 | Interleukin 6 |
| IL-10 | Interleukin 10 |
| IQSEC2 | IQ motif and Sec7 domain ArfGEF 2 |
| MDRD | Modification of diet in renal disease |
| MI | Myocardial infraction |
| MiRDB | An online database for prediction of functional miRNA targets |
| MiRNAs | Micro RiboNucleic Acids |
| MMP-9 | Matrix metallopeptidase-9 |
| MYOM2 | Myomesin 2 |
| NCBI | National center for biotechnology information |
| NGS | Next generation sequencing |
| NSTEMI | Non ST-segment elevation myocardial infraction |
| NUDT8 | Nudix hydrolase 8 |
| PCI | Percutaneous coronary intervention |
| PLA2G5 | Phospholipase A2 group V |
| qPCR | Quantitative polymerase chain reaction |
| ROC | Receiver operator curve analysis |
| RPKM | Reads Per Kilobase of transcript, per Million mapped reads |
| SMG6 | SMG6 Nonsense mediated mRNA decay factor |
| sPLA2 | Secretory phospholipase A2 |
| sPLA2-IIA | Secretory phospholipase A2-IIA |
| SRF | Serum response factor |
| STEMI | ST-segment elevation myocardial infraction |
| TIMP2 | TIMP metallopeptidase inhibitor 2 |
| TMM | Trimmed Mean of M |
| TNF-α | Tumor necrosis factor alpha |
| TRIM7 | Tripartite motif containing 7 |
| WBC | White blood cells |
| ZMYM6 | Zinc finger MYM-type containing 6 |
| ZNF417 | Zinc finger protein 417 |
| ZNF584 | Zinc finger protein 584 |
References
- Goren, Y.; Kushnir, M.; Zafrir, B.; Tabak, S.; Lewis, B.S.; Amir, O. Serum levels of microRNAs in patients with heart failure. Eur. J. Heart Fail. 2012, 14, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Clerk, A.; Cullingford, T.E.; Fuller, S.J.; Giraldo, A.; Markou, T.; Pikkarainen, S.; Sugden, P.H. Signaling pathways mediating cardiac myocyte gene expression in physiological and stress responses. J. Cell. Physiol. 2007, 212, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Creemers, E.E.; Tijsen, A.J.; Pinto, Y.M. Circulating microRNAs: Novel biomarkers and extracellular communicators in cardiovascular disease? Circ. Res. 2012, 110, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Khera, A.V.; Kathiresan, S. Genetics of coronary artery disease: Discovery, biology and clinical translation. Nat. Rev. Genet. 2017, 18, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Liu, C.; Hu, J.; Liu, Y.; Wang, J.; Chen, G.; Li, Z.; Chen, H. Epigenetic mechanisms in coronary artery disease: The current state and prospects. Trends Cardiovasc. Med. 2018, 28, 311–319. [Google Scholar] [CrossRef]
- Oikonomou, E.; Siasos, G.; Tsigkou, V.; Bletsa, E.; Panoilia, M.-E.; Oikonomou, I.N.; Simanidis, I.; Spinou, M.; Papastavrou, A.; Kokosias, G.; et al. Coronary Artery Disease and Endothelial Dysfunction: Novel Diagnostic and Therapeutic Approaches. Curr. Med. Chem. 2020, 27, 1052–1080. [Google Scholar] [CrossRef]
- Chintalgattu, V.; Rees, M.L.; Culver, J.C.; Goel, A.; Jiffar, T.; Zhang, J.; Dunner, K., Jr.; Pati, S.; Bankson, J.A.; Pasqualini, R.; et al. Coronary microvascular pericytes are the cellular target of sunitinib malate induced cardiotoxicity. Sci. Transl. Med. 2013, 5, 187ra69. [Google Scholar] [CrossRef]
- Monteleone, I.; Muscoli, S.; Terribili, N.; Zorzi, F.; Mariano, E.; Mehta, J.L.; Pallone, F.; Monteleone, G.; Romeo, F. Local immune activity in acute coronary syndrome: oxLDL abrogates LPS-tolerance in mononuclear cells isolated from culprit lesion. Int. J. Cardiol. 2013, 169, 44–51. [Google Scholar] [CrossRef]
- Leoni, G.; Soehnlein, O. (Re) Solving Repair After Myocardial Infarction. Front. Pharmacol. 2018, 9, 1342. [Google Scholar] [CrossRef]
- Robertson, L.; Grip, L.; Mattsson Hultén, L.; Hulthe, J.; Wiklund, O. Release of protein as well as activity of MMP-9 from unstable atherosclerotic plaques during percutaneous coronary intervention. J. Intern. Med. 2007, 262, 659–667. [Google Scholar] [CrossRef]
- Duan, L.; Xiong, X.; Liu, Y.; Wang, J. miRNA-1: Functional roles and dysregulation in heart disease. Mol. Biosyst. 2014, 10, 2775–2782. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.L.; Fang, H.C.; Zhao, H.L.; Li, X.-L.; Luo, Y.; Wu, B.-Q.; Fu, M.-J.; Liu, W.; Liang, J.-J.; Chen, X.-H. The role of microRNA-1 targeting of MAPK3 in myocardial ischemia-reperfusion injury in rats undergoing sevoflurane preconditioning via the PI3K/Akt pathway. Am. J. Physiol. Cell Physiol. 2018, 315, C380–C388. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Zhang, S.; Huo, Z. Serum Circulating miR-150 is a Predictor of Post-Acute Myocardial Infarction Heart Failure. Int. Heart J. 2019, 60, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Fan, Z.; Zhao, T.; Cao, W.; Zhang, L.; Li, H.; Xie, Q.; Tian, Y.; Wang, B. Plasma miR-1, miR-208, miR-499 as potential predictive biomarkers for acute myocardial infarction: An independent study of Han population. Exp. Gerontol. 2015, 72, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Grabmaier, U.; Clauss, S.; Gross, L.; Klier, I.; Franz, W.; Steinbeck, G.; Wakili, R.; Theiss, H.; Brenner, C. Diagnostic and prognostic value of miR-1 and miR-29b on adverse ventricular remodeling after acute myocardial infarction—The SITAGRAMI-miR analysis. Int. J. Cardiol. 2017, 244, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Lan, C.; Pei, H.; Duan, G.; Huang, L.; Li, L. Expression of circulating miR-486 and miR-150 in patients with acute myocardial infarction. BMC Cardiovasc. Disord. 2015, 15, 51. [Google Scholar] [CrossRef] [PubMed]
- Ralapanawa, U.; Sivakanesan, R. Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome: A Narrative Review. J. Epidemiol. Glob. Health. 2021, 11, 169–177. [Google Scholar] [CrossRef]
- Nagelschmitz, J.; Blunck, M.; Kraetzschmar, J.; Ludwig, M.; Wensing, G.; Hohlfeld, T. Pharmacokinetics and pharmacodynamics of acetylsalicylic acid after intravenous and oral administration to healthy volunteers. Clin. Pharmacol. 2014, 6, 51–59. [Google Scholar] [CrossRef]
- Olsen, M.B.; Gregersen, I.; Sandanger, Ø.; Yang, K.; Sokolova, M.; Halvorsen, B.E.; Gullestad, L.; Broch, K.; Aukrust, P.; Louwe, M.C. Targeting the Inflammasome in Cardiovascular Disease. JACC Basic Transl. Sci. 2022, 7, 84–98. [Google Scholar] [CrossRef]
- Zhang, J.; He, Y.; Yan, X.; Chen, S.; He, M.; Lei, Y.; Zhang, J.; Gongol, B.; Gu, M.; Miao, Y.; et al. MicroRNA-483 amelioration of experimental pulmonary hypertension. EMBO Mol. Med. 2020, 12, e11303. [Google Scholar] [CrossRef]
- Chouri, E.; Servaas, N.H.; Bekker, C.P.J.; Affandi, A.J.; Cossu, M.; Hillen, M.R.; Angiolilli, C.; Mertens, J.S.; van den Hoogen, L.L.; Silva-Cardoso, S.; et al. Serum microRNA screening and functional studies reveal miR-483-5p as a potential driver of fibrosis in systemic sclerosis. J. Autoimmun. 2018, 89, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Warnecke-Eberz, U.; Chon, S.H.; Hölscher, A.H.; Drebber, U.; Bollschweiler, E. Exosomal onco-miRs from serum of patients with adenocarcinoma of the esophagus: Comparison of miRNA profiles of exosomes and matching tumor. Tumour Biol. 2015, 36, 4643–4653. [Google Scholar] [CrossRef] [PubMed]
- Szilágyi, M.; Pös, O.; Márton, É.; Buglyó, G.; Soltész, B.; Keserű, J.; Penyige, A.; Szemes, T.; Nagy, B. Circulating Cell-Free Nucleic Acids: Main Characteristics and Clinical Application. Int. J. Mol. Sci. 2020, 21, 6827. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Yuan, H.; Yu, H. Downregulation of miR-483-5p decreases hypoxia-induced injury in human cardiomyocytes by targeting MAPK3. Cell. Mol. Biol. Lett. 2020, 25, 20. [Google Scholar] [CrossRef]
- Qiao, Y.; Ma, N.; Wang, X.; Hui, Y.; Li, F.; Xiang, Y.; Zhou, J.; Zou, C.; Jin, J.; Lv, G.; et al. MiR-483-5p controls angiogenesis in vitro and targets serum response factor. FEBS Lett. 2011, 585, 3095–3100. [Google Scholar] [CrossRef]
- Wootton, P.T.E.; Arora, N.L.; Drenos, F.; Thompson, S.R.; Cooper, J.A.; Stephens, J.W.; Hurel, S.J.; Hurt-Camejo, E.; Wiklund, O.; Humphries, S.E.; et al. Tagging SNP haplotype analysis of the secretory PLA2-V gene, PLA2G5, shows strong association with LDL and oxLDL levels, suggesting functional distinction from sPLA2-IIA: Results from the UDACS study. Human Mol. Genet. 2007, 16, 1437–1444. [Google Scholar] [CrossRef]
- Cannavo, A.; Komici, K.; Bencivenga, L.; D’Amico, M.L.; Gambino, G.; Liccardo, D.; Ferrara, N.; Rengo, G. GRK2 as a therapeutic target for heart failure. Expert Opin. Ther. Targets 2018, 22, 75–83. [Google Scholar] [CrossRef]
- Auxerre-Plantié, E.; Nielsen, T.; Grunert, M.; Olejniczak, O.; Perrot, A.; Özcelik, C.; Harries, D.; Matinmehr, F.; Dos Remedios, C.; Mühlfeld, C.; et al. Identification of MYOM2 as a candidate gene in hypertrophic cardiomyopathy and Tetralogy of Fallot, and its functional evaluation in the Drosophila heart. Dis. Model Mech. 2020, 13, dmm045377. [Google Scholar] [CrossRef]
- Liu, X.; Xu, H.; Xu, H.; Geng, Q.; Mak, W.-H.; Ling, F.; Su, Z.; Yang, F.; Zhang, T.; Chen, J.; et al. New genetic variants associated with major adverse cardiovascular events in patients with acute coronary syndromes and treated with clopidogrel and aspirin. Pharmacogenom. J. 2021, 21, 664–672. [Google Scholar] [CrossRef]
- Kandalam, V.; Basu, R.; Abraham, T.; Wang, X.; Soloway, P.D.; Jaworski, D.M.; Oudit, G.Y.; Kassiri, Z. TIMP2 Deficiency Accelerates Adverse Post–Myocardial Infarction Remodeling Because of Enhanced MT1-MMP Activity Despite Lack of MMP2 Activation. Circ. Res. 2010, 106, 796–808. [Google Scholar] [CrossRef]
- Wang, X.; Chen, W.; Zhang, J.; Khan, A.; Li, L.; Huang, F.; Qiu, Z.; Wang, L.; Chen, X. Critical Role of ADAMTS2 (A Disintegrin and Metalloproteinase with Thrombospondin Motifs 2) in Cardiac Hypertrophy Induced by Pressure Overload. Hypertension 2017, 69, 1060–1069. [Google Scholar] [CrossRef] [PubMed]
- Korf-Klingebiel, M.; Reboll, M.R.; Grote, K.; Schleiner, H.; Wang, Y.; Wu, X.; Klede, S.; Mikhed, Y.; Nobre, A.; Bauersachs, J.; et al. Heparan Sulfate–Editing Extracellular Sulfatases Enhance VEGF Bioavailability for Ischemic Heart Repair. Circ. Res. 2019, 125, 787–801. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.J.; Yu, S.L.; Su, T.C.; Hsu, H.-C.; Chen, M.-F.; Lee, Y.-T.; Chien, K.-L.; Lu, T.-P. Statin-induced microRNAome alterations modulating inflammation pathways of peripheral blood mononuclear cells in patients with hypercholesterolemia. Biosci. Rep. 2020, 40, BSR20201885. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Hu, D.; Song, J.; Lee, C.; Chen, H. Early diagnostic value of circulating microRNAs in patients with suspected acute myocardial infarction. J. Cell. Physiol. 2019, 234, 13649–13658. [Google Scholar] [CrossRef]
- Li, F.; Ma, N.; Zhao, R.; Wu, G.; Zhang, Y.; Qiao, Y.; Han, D.; Xu, Y.; Xiang, Y.; Yan, B.; et al. Overexpression of miR-483-5p/3p cooperate to inhibit mouse liver fibrosis by suppressing the TGF-β stimulated HSCs in transgenic mice. J. Cell. Mol. Med. 2014, 18, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Tang, W.; Guo, J.; Sun, S. miR-483-5p plays a protective role in chronic obstructive pulmonary disease. Int. J. Mol. Med. 2017, 40, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Mohan, R.; Mao, Y.; Zhang, S.; Zhang, Y.-W.; Xu, C.-R.; Gradwohl, G.; Tang, X. Differentially Expressed MicroRNA-483 Confers Distinct Functions in Pancreatic β- and α-Cells. J. Biol. Chem. 2015, 290, 19955–19966. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Qiu, F.; Cao, H.; Li, H.; Dai, G.; Ma, T.; Gong, Y.; Luo, W.; Zhu, D.; Qiu, Z.; et al. Therapeutic delivery of microRNA-125a-5p oligonucleotides improves recovery from myocardial ischemia/reperfusion injury in mice and swine. Theranostics 2023, 13, 685–703. [Google Scholar] [CrossRef]
- Xu, M.; Liu, D.; Gao, X.; Wang, Z.; Zhang, L.; Fan, H. MiR-423-5p Inhibition Exerts Protective Effects on Angiotensin II-Induced Cardiomyocyte Hypertrophy. Tohoku J. Exp. Med. 2023, 259, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Shang, F.; Guo, X.; Chen, Y.; Wang, C.; Gao, J.; Wen, E.; Lai, B.; Bai, L. Endothelial MicroRNA-483-3p Is Hypertension-Protective. Oxid. Med. Cell. Longev. 2022, 2022, 3698219. [Google Scholar] [CrossRef]
- Lamon, S.; Le Carré, J.; Petito, G.; Duong, H.P.; Luthi, F.; Hiam, D.; Léger, B. The effect of the menstrual cycle on the circulating microRNA pool in human plasma: A pilot study. Hum. Reprod. 2023, 38, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Lu, J.; Luo, Y.; Li, S.; Chen, M. High association between human circulating microRNA-497 and acute myocardial infarction. Sci. World J. 2014, 2014, 931845. [Google Scholar] [CrossRef] [PubMed]
- Kok, M.G.M.; Halliani, A.; Moerland, P.D.; Meijers, J.C.M.; Creemers, E.E.; Pinto-Sietsma, S.J. Normalization panels for the reliable quantification of circulating microRNAs by RT-qPCR. FASEB J. 2015, 29, 3853–3862. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, X. Prediction of functional microRNA targets by integrative modeling of microRNA binding and target expression data. Genome Biol. 2019, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, X. miRDB: An online database for prediction of functional microRNA targets. Nucleic Acids Res. 2020, 48, D127–D131. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No CAD n = 23 | CAD (PCI) n = 28 | STEMI n = 22 | NSTEMI n = 26 | ANOVA p Value | |
|---|---|---|---|---|---|
| Age | 62 ± 10 | 63 ± 9 | 60 ± 8 | 62 ± 9 | 0.632 |
| Hypertension | 14 (61%) | 21 (78%) | 11 (50%) | 18 (69%) | 0.188 |
| Diabetes mellitus | 10 (43%) | 15 (56%) | 9 (41%) | 8 (31%) | 0.280 |
| Hyperlipidemia | 16 (70%) | 17 (63%) | 12 (54%) | 17 (65%) | 0.767 |
| Family History of CAD | 8 (35%) | 3 (11%) | 6 (27%) | 9 (35%) | 0.154 |
| Smoking | 4 (17%) † | 11 (41%) | 16 (72%) *,‡ | 9 (36%)† | 0.002 |
| Renal failure | 0 (0%) | 0 (0%) | 0 (0%) | 2 (8%) | 0.127 |
| Previous MI | 0 (0%) | 4 (16) | 0 (0%) | 6 (24%) | 0.011 |
| Previous PCI | 0 (0%) **,‡ | 19 (70%) *,†,‡ | 2 (9%) ** | 9 (35%) *,** | <0.0001 |
| Atrial fibrillation | 2 (9%) | 0 (0%) | 1 (5%) | 1 (4%) | 0.489 |
| Hemoglobin (gr/dL) | 14 ± 2 | 14 ± 2 | 15 ± 1 | 14 ± 2 | 0.328 |
| WBC (×1000/dL) | 8.8 ± 2.7 | 9.3 ± 2.1 | 10.8 ± 2.8 | 8.9 ± 3.4 | 0.101 |
| Creatinine (mg/dL) | 0.86 ± 0.19 | 0.98 ± 0.32 | 0.98 ± 0.23 | 1.01 ± 0.27 | 0.318 |
| GFR (MDRD, ml/min) | 95 ± 25 | 85 ± 24 | 84 ± 22 | 81 ± 21 | 0.251 |
| All Patients n = 99 | Odds Ratio | Confidence Interval | Odds Ratio | Confidence Interval | p Value |
|---|---|---|---|---|---|
| Univariable | Multivariable, stepwise | ||||
| Age | 1.001 | 0.94 to 1.07 | |||
| Smoking | 12.20 | 2.47 to 60.03 | 4.36 | 1.32 to 14.37 | 0.0155 |
| Coronary miRNA483 | 1.01 | 0.783 to 1.30 | |||
| Peripheral miRNA483 | 0.77 | 0.59 to 0.98 | 0.83 | 0.69 to 0.99 | 0.0402 |
| Patients without previous PCI, n = 68 | |||||
| Univariable | Multivariable, stepwise | ||||
| Age | 1.04 | 0.97 to 1.12 | |||
| Smoking | 11.80 | 2.52 to 55.40 | 6.67 | 1.79 to 24.81 | 0.0046 |
| Coronary miRNA483 | 0.98 | 0.76 to 1.25 | |||
| Peripheral miRNA483 | 0.73 | 0.55 to 0.96 | 0.78 | 0.61 to 0.99 | 0.0465 |
| No CAD n = 23 | CAD (PCI) n = 28 | STEMI n = 22 | NSTEMI n = 26 | ANOVA p Value | |
|---|---|---|---|---|---|
| Beta blockers | 6 (26%) ** | 16 (57%) *,† | 2 (9%) ** | 5 (19%) | 0.006 |
| Angiotensin receptor blockers (ARBs) | 1 (4%) | 1 (4%) | 0 (0%) | 0 (0%) | 0.722 |
| Calcium channel blockers (CCBs) | 2 (9%) | 4 (14%) | 2 (9%) | 5 (19%) | 0.340 |
| Angiotensin-converting enzyme (ACE) inhibitors | 10 (43%) | 14 (50%) ‡ | 6 (li%) | 2 (8%) ** | 0.044 |
| Anticoagulants | 2 (9%) | 1 (4%) | 1 (9%) | 0 (0%) | 0.616 |
| Aspirin | 15 (65%) † | 22 (79%) †, ‡ | 4 (18%) *, ** | 7 (26%) ** | <0.001 |
| Statins | 14 (61%) | 16 (57%) | 6 (27%) | 9 (35%) | 0.355 |
| Gene | Gene Name | Function | Expression |
|---|---|---|---|
| PLA2G5 | phospholipase A2 group V | Encoded enzyme catalyzes the hydrolysis of membrane phospholipids to generate lysophospholipids and free fatty acids including arachidonic acid. It preferentially hydrolyzes linoleoyl-containing phosphatidylcholine substrates. Secretion of this enzyme is thought to induce inflammatory responses in neighboring cells. | Biased expression in heart (RPKM 14.5), |
| NUDT8 | nudix hydrolase 8 | Encoded enzyme predicted to enable magnesium ion binding activity. Predicted to be involved in purine nucleoside bisphosphate catabolic process. Predicted to be located in mitochondria. | Broad expression in heart (RPKM 4.8) |
| MYOM2 | myomesin 2 | The giant protein titin, together with its associated proteins, interconnects the major structure of sarcomeres, the M bands and Z discs. The C-terminal end of the titin string extends into the M line, where it binds tightly to M-band constituents of apparent molecular masses of 190 kD and 165 kD. The predicted MYOM2 protein contains 1465 amino acids. Like MYOM1, MYOM2 has a unique N-terminal domain followed by 12 repeat domains with strong homology to either fibronectin type III or immunoglobulin C2 domains. Protein sequence comparisons suggested that the MYOM2 protein and bovine M protein are identical. | Biased expression in heart (RPKM 193.6) |
| GRK2 | G protein-coupled receptor kinase 2 | This gene encodes a member of the G protein-coupled receptor kinase family of proteins. The encoded protein phosphorylates the beta-adrenergic receptor as well as a wide range of other substrates including non-GPCR cell surface receptors, and cytoskeletal, mitochondrial and transcription factor proteins. Data from rodent models support a role for this gene in embryonic development, heart function and metabolism. Elevated expression of this gene observed in human patients with heart failure and Alzheimer’s disease. | Broad expression in bone marrow (RPKM 91.8), and other tissues including the heart average expression (10.2 RPKM) |
| TIMP2 | TIMP metallopeptidase inhibitor 2 | This gene is a member of the TIMP gene family, a family of natural inhibitors of the matrix metalloproteinases, a group of peptidases involved in degradation of the extracellular matrix. In addition to an inhibitory role against metalloproteinases, the encoded protein has a unique role among TIMP family members in its ability to directly suppress the proliferation of endothelial cells. As a result, the encoded protein may be critical to the maintenance of tissue homeostasis by suppressing the proliferation of quiescent tissues in response to angiogenic factors, and by inhibiting protease activity in tissues undergoing remodelling of the extracellular matrix. | Ubiquitous expression in many tissues including the heart (68.2 RPKM) |
| DNAAF10 | dynein axonemal assembly factor 10 | This gene encodes a protein with two WD40 repeat domains thought to be involved in apoptosis via activation of caspase-3. Multiple transcript variants encoding different isoforms have been found for this gene. | Ubiquitous expression in many tissues including the heart average tissue expression (2.3 RPKM) |
| TRIM7 | tripartite motif containing 7 | The protein encoded by this gene is a member of the tripartite motif (TRIM) family. The TRIM motif includes three zinc-binding domains, a RING, a B-box type 1, a B-box type 2 and a coiled-coil region. The protein localizes to both the nucleus and the cytoplasm, and may represent a participant in the initiation of glycogen synthesis. | Biased expression in 10 tissues including the heart (0.43 RPKM) |
| ZNF584 | zinc finger protein 584 | Predicted to enable DNA-binding transcription factor activity, RNA polymerase II-specific and RNA polymerase II cis-regulatory region sequence-specific DNA binding activity. Predicted to be involved in regulation of transcription by RNA polymerase II. | Biased expression in many tissues amongst them higher expression in the heart (1.4 RPKM) |
| ADAMTS2 | ADAM metallopeptidase with thrombospondin type-1 motif -2 | This gene encodes a member of the ADAMTS (a disintegrin and metalloproteinase with thrombospondin motifs) protein family. Members of the family share several distinct protein modules, including a propeptide region, a metalloproteinase domain, a disintegrin-like domain, and a thrombospondin type 1 (TS) motif. Individual members of this family differ in the number of C-terminal TS motifs, and some have unique C-terminal domains. The encoded preproprotein is proteolytically processed to generate the mature procollagen N-proteinase. This proteinase excises the N-propeptide of the fibrillar procollagens types I-III and type V. Mutations in this gene cause Ehlers-Danlos syndrome type VIIC, a recessively inherited connective-tissue disorder. | Broad expression in many tissues including the heart average tissue expression (2.1 RPKM) |
| HGSNAT | heparan-alpha-glucosaminide N-acetyltransferase | This gene encodes a lysosomal acetyltransferase, which is one of several enzymes involved in the lysosomal degradation of heparin sulfate. Mutations in this gene are associated with Sanfilippo syndrome C, one type of the lysosomal storage disease mucopolysaccaridosis III, which results from impaired degradation of heparan sulfate. | Ubiquitous expression in many tissues including the heart low-average tissue expression (5.9 RPKM) |
| ZNF417 | zinc finger protein 417 | Predicted to enable DNA-binding transcription factor activity, RNA polymerase II-specific and RNA polymerase II cis-regulatory region sequence-specific DNA binding activity. Predicted to be involved in regulation of transcription by RNA polymerase II. Predicted to be active in nucleus. | Ubiquitous expression in many tissues including the heart low-average tissue expression (1.4 RPKM) |
| IQSEC2 | IQ motif and Sec7 domain ArfGEF 2 | This gene encodes a guanine nucleotide exchange factor for the ARF family of small GTP-binding proteins. The encoded protein is a component of the postsynaptic density at excitatory synapses, and may play a critical role in cytoskeletal and synaptic organization through the activation of selected ARF substrates including ARF1 and ARF6. Mutations in this gene have been implicated in nonsyndromic X-linked cognitive disability. | Ubiquitous expression in many tissues including the heart low-average tissue expression (0.4 RPKM) |
| SMG6 | SMG6 nonsense mediated mRNA decay factor | This gene encodes a component of the telomerase ribonucleoprotein complex responsible for the replication and maintenance of chromosome ends. The encoded protein also plays a role in the nonsense-mediated mRNA decay (NMD) pathway, providing the endonuclease activity near the premature translation termination codon that is needed to initiate NMD. | Ubiquitous expression in many tissues including the heart average tissue expression (2.2 RPKM) |
| ZMYM6 | zinc finger MYM-type containing 6 | Predicted to enable DNA binding activity. Involved in cytoskeleton organization and regulation of cell morphogenesis. Predicted to be located in nucleus. | Ubiquitous expression in many tissues including the heart average tissue expression (2.7 RPKM) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volodko, O.; Volinsky, N.; Yarkoni, M.; Margalit, N.; Kusniec, F.; Sudarsky, D.; Elbaz-Greener, G.; Carasso, S.; Amir, O. Characterization of Systemic and Culprit-Coronary Artery miR-483-5p Expression in Chronic CAD and Acute Myocardial Infarction Male Patients. Int. J. Mol. Sci. 2023, 24, 8551. https://doi.org/10.3390/ijms24108551
Volodko O, Volinsky N, Yarkoni M, Margalit N, Kusniec F, Sudarsky D, Elbaz-Greener G, Carasso S, Amir O. Characterization of Systemic and Culprit-Coronary Artery miR-483-5p Expression in Chronic CAD and Acute Myocardial Infarction Male Patients. International Journal of Molecular Sciences. 2023; 24(10):8551. https://doi.org/10.3390/ijms24108551
Chicago/Turabian StyleVolodko, Olga, Natalia Volinsky, Merav Yarkoni, Nufar Margalit, Fabio Kusniec, Doron Sudarsky, Gabby Elbaz-Greener, Shemy Carasso, and Offer Amir. 2023. "Characterization of Systemic and Culprit-Coronary Artery miR-483-5p Expression in Chronic CAD and Acute Myocardial Infarction Male Patients" International Journal of Molecular Sciences 24, no. 10: 8551. https://doi.org/10.3390/ijms24108551
APA StyleVolodko, O., Volinsky, N., Yarkoni, M., Margalit, N., Kusniec, F., Sudarsky, D., Elbaz-Greener, G., Carasso, S., & Amir, O. (2023). Characterization of Systemic and Culprit-Coronary Artery miR-483-5p Expression in Chronic CAD and Acute Myocardial Infarction Male Patients. International Journal of Molecular Sciences, 24(10), 8551. https://doi.org/10.3390/ijms24108551