
Phage Therapy in the Era of Multidrug Resistance in Bacteria: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
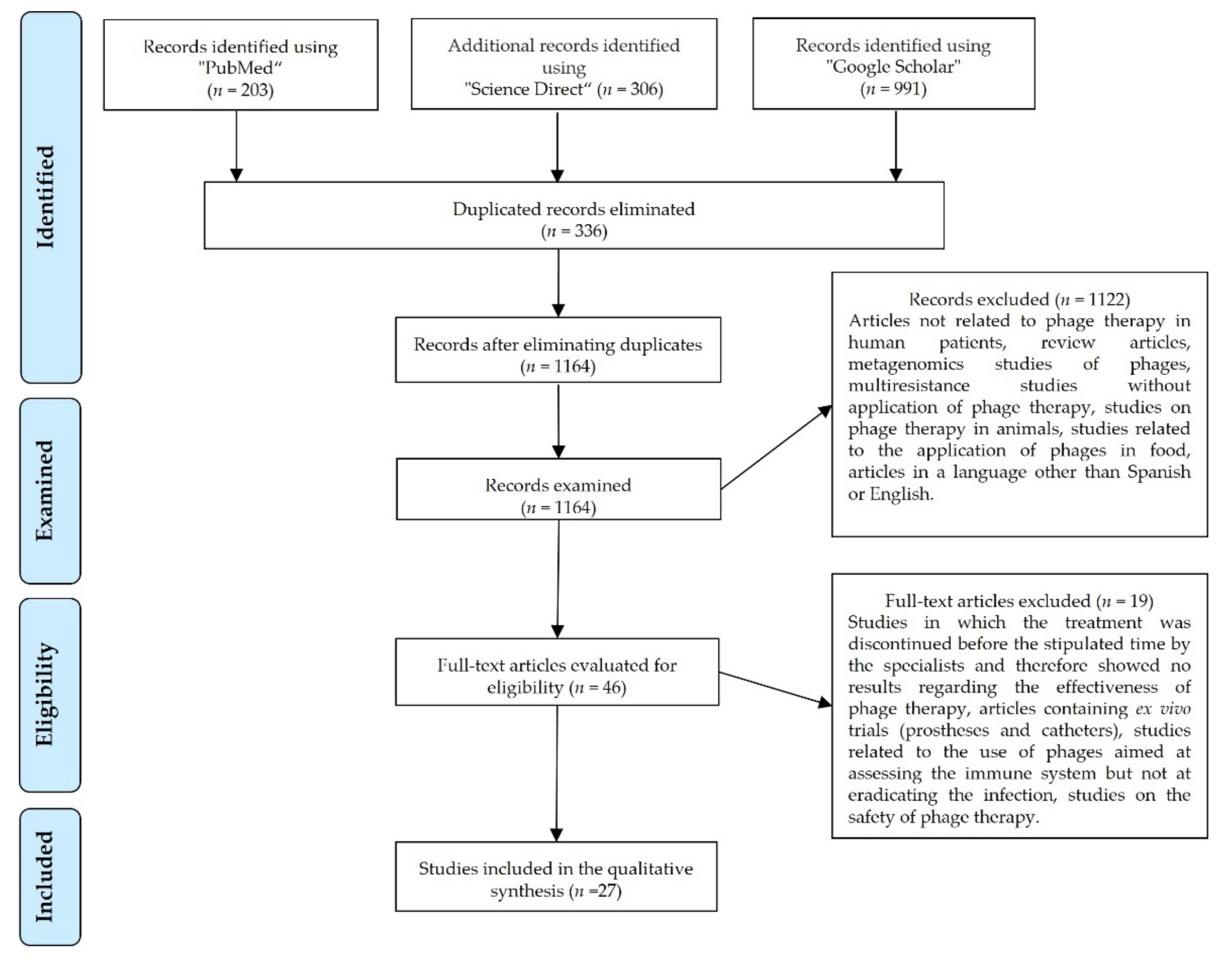
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Data Analysis
3. Results

{kind=link}
{kind=link}
| Author(s)/ Reference | Country | Year of Publication | Multidrug-Resistant Bacteria | Site or Type of Infection | Patients (Number/Gender/ Age) | Comorbidities/ Medical History | Adverse Effects | Effect of the Treatment |
|---|---|---|---|---|---|---|---|---|
| Ooi, M.L. et al. [37] | Australia | 2019 | Staphylococcus aureus | Recalcitrant chronic rhinosinusitis caused by a biofilm | 9/4 men, 5 women/ 18–70 years of age | Endoscopic sinus surgery | Diarrhea, epistaxis, oropharyngeal pain, cough, rhinalgia, and low blood bicarbonate level | Positive treatment effect: 2 patients were cured and the others showed reduced bacterial growth |
| Schooley, R.T. et al. [25] | U.S. | 2017 | Acinetobacter baumannii | Pancreatic pseudocyst infection | 1/male/68 years of age | Diabetic, necrotizing pancreatitis | Not reported | Positive treatment effect: patient showed continuous clinical improvement, woke up from coma, showed renal improvement, and was extubated |
| Jault, P. et al. [23] | France–Belgium | 2018 | Pseudomonas aeruginosa- Escherichia coli | Infection of wounds from burns on the skin | 12/men and women/ over 18 years of age | Hospitalized patients, treated for burns in a burn unit | No adverse effects related to PT were observed | No/insufficient treatment effect owing to the administration of a very low treatment dose |
| Law, N. et al. [34] | U.S. | 2019 | Pseudomonas aeruginosa | Respiratory tract infection | 1/woman/26 years of age | Patient with cystic fibrosis, persistent respiratory failure, and renal failure | No adverse effects related to PT were observed | Positive treatment effect: pneumonia clinically resolved, baseline renal function was restored, and fever disappeared |
| Aslam, S. et al. [19] | U.S. | 2019 | Pseudomonas aeruginosa-Burkholderia dolosa-Mycobacterium abscessus | Lower respiratory tract infections | 3/1 man, 2 women/ 67, 28, and 57 years of age | Lung transplantation and progressive kidney failure | Intravenous and nebulized formulations of bacteriophages were well tolerated without adverse effects attributed to bacteriophage administration | A positive effect of the treatment was observed in two of the three patients (one male and female, each aged 67 years) as they did not develop further infection with Pseudomonas aeruginosa, and their respiratory status markedly improved. The 28-year-old patient died. However, this was not attributed to PT, but rather to a sequence of events that led to multi-organ failure, most plausibly attributable to postsplenectomy complications and liver disease. Hence, a verdict on the treatment was not possible. |
| Nir-Paz, R. et al. [35] | U.S. | 2019 | Acinetobacter baumannii-Klebsiella pneumoniae | Left tibial infection following trauma | 1/male/42 years of age | Grade IIIA bilateral open fractures of the lower extremities: left bicondylar tibial plateau fracture with compartment syndrome and right distal femoral fracture | No adverse effects associated with PT were observed | Positive treatment effect, with healing of the graft and elimination of subtle chronic bone pain in the left leg. During a follow-up period of 8 months after treatment, no Ab- or Kp-positive cultures were obtained from any site. |
| Tkhilaisshvili, T. et al. [33] | Germany | 2019 | Pseudomonas aeruginosa- Staphylococcus epidermidis | Chronic recurrent periprosthetic infection of the knee and chronic osteomyelitis of the femur | 1/woman/ 80 years of age | Metabolic syndrome (type II diabetes mellitus and obesity) and chronic renal failure | No adverse effects related to PT were observed | Positive treatment effect. The patient did not report pain in the right knee; the soft tissue at the surgical site did not show complications; and mobility was satisfactory. All periprosthetic tissue samples collected intraoperatively resulted in negative cultures. |
| Corbellino, M. et al. [28] | Italy | 2019 | Klebsiella pneumoniae | Infections of the gastrointestinal and urinary tracts | 1/male/57 years of age | Crohn’s disease, obstructive nephrolithiasis, right nephrectomy and radical cystectomy, and stage III chronic renal failure | No adverse effects related to PT were observed | Positive treatment effect. Long-lasting multi-site colonization by an MDR Kp strain in a patient with a single kidney, a cutaneous ureterostomy, and an indwelling ureteral stent resolved after a 3-week course of PT. |
| Duplessis, C. et al. [36] | U.S. | 2017 | Pseudomonas aeruginosa | Recalcitrant infection after ASD/VSD closures | 1/male (child)/2 years of age | DiGeorge syndrome and complex congenital heart disease, including a type B interrupted aortic arch, posterior misalignment of a ventricular septal defect (VSD), sub-aortic stenosis, bicuspid aortic valve, and secundum atrial septal defect | Decompensation owing to anaphylaxis, which was subsequently attributed to progressive heart failure, although the release of endotoxins as a contributing factor could not be ruled out | Clinical improvement was seen after treatment for several days with PT; however, the patient decompensated and developed severe arrhythmias and cardiac and septic shocks. This turbulent worsening was attributed to the progressive accumulation of undrained fluids, a history of influenza infection, and end-stage heart failure. Finally, the child passed away. |
| Qin, J. et al. [24] | China | 2021 | Klebsiella pneumoniae | Multifocal urinary tract infections | 1/male/66 years of age | The patient’s cancerous bladder was partially resected | No adverse effects related to PT were observed | Negative treatment effect. The phage cocktail did not work. It is believed that the heterogeneous bacteria that colonized the renal pelvis could not be effectively eliminated because the phages could not reach them. |
| Tan, X. et al. [26] | China | 2021 | Acinetobacter baumannii | Lung infection | 1/male/86 years of age | Exacerbation of chronic obstructive pulmonary disease and type II diabetes | No adverse effects related to PT were observed | Positive treatment effect, with elimination of the pathogen and clinical improvement of the patient’s lung function |
| Hoyle, N. et al. [29] | Georgia | 2018 | Achromobacter xylosoxidans | Chronic lung infection | 1/female/ 17 years of age | Cystic fibrosis | No adverse effects related to PT were observed | Positive treatment effect; dyspnea resolved and cough was reduced. Lung function: FEV1 increased. |
| Leitner, L. et al. [38] | Georgia | 2018 | Enterococcus spp. Escherichia coli, Streptococcus spp. | Urinary tract infection | 28/men/ over 18 years of age | Transurethral resection of the prostate (TURP), with complicated or recurrent uncomplicated UTI without signs of systemic infection | No adverse effects related to PT were observed | Positive effect of treatment in 60% of patients, with normalization of urine cultures |
| Cano, E.J. et al. [30] | U.S. | 2020 | Klebsiella pneumoniae | Knee joint prosthesis infection | 1/male/62 years of age | Diabetes mellitus, obesity, total knee arthroplasty, multiple bacterial infections | No adverse effects related to PT were observed | Positive treatment effect. The patient showed improvement and remained asymptomatic 34 weeks after completing the treatment, in addition to showing improvement of erythema, swelling, pain, range of motion, and function of his right lower extremity. |
| Gupta, P. et al. [44] | Varanasi, India | 2019 | Escherichia coli, Staphylococcus aureus, and Pseudomonas aeruginosa | Infection of chronic wounds (ulcers) that do not heal | 20/12–60 years of age | Not reported | No adverse effects related to PT were observed | Positive treatment effect in 7 patients who completely healed; the others showed significant improvement in terms of wound healing |
| Lebeaux, D. et al. [45] | Paris, France | 2021 | Achromobacter xylosoxidans | Persistent lung infection | 1/male/12 years of age | Cystic fibrosis and double lung transplantation | No adverse effects related to PT were observed | Positive effect. Respiratory condition gradually improved, and the bacterial load decreased. |
| Nadareishvili, L. et al. [40] | Georgia | 2020 | Staphylococcus aureus | Osteomyelitis of the sternum and parasternal abscess | 1/male/74 years of age | Coronary artery graft, type II diabetes mellitus, high blood pressure | Not reported | Positive treatment effect. The diameter of the wound decreased and the purulent fistula closed. |
| Staphylococcus aureus | Chronic osteomyelitis of the right tibia | 1/female/ 60 years of age | Type II diabetes mellitus | Not reported | Positive treatment effect with complete wound closure | |||
| Burkholderia cepacia, S. aureus, and Enterococcus faecalis | Osteomyelitis with foot ulcer | 1/male/69 years of age | Type II diabetes mellitus | Not reported | Positive treatment effect. The patient improved and the ulcer healed. | |||
| Pseudomonas aeruginosa, then by Staphylococcus aureus and Serratia Marcescens | Laryngeal (post-surgical) infection | 1/male/68 years of age | Removal of the larynx due to carcinoma | Not reported | Positive treatment effect. The patient improved and infection was completely cured. | |||
| Patel, D.R. et al. [46] | India | 2019 | Escherichia coli, Pseudomonas aeruginosa, Staphylococcus aureus, Klebsiella pneumoniae, Proteus species, Citrobacter freundii, Morganella morganii, Acinetobacter baumannii | Chronic wound infection of the skin | 48/34 men, 14 women/12–70 years of age | 27 diabetics, 8 with high blood pressure, 2 with tuberculosis, and 10 with amputations | Not reported | Positive treatment effect in 39 patients who were completely cured; 2 patients died |
| Fadlallah, A. et al. [31] | Georgia | 2015 | Staphylococcus aureus | Eye infection/bacterial keratitis | 1/female/65 years of age | Postoperative corneal abscess of the left eye and interstitial keratitis after craniotomy for acoustic neurinoma | No adverse effects related to PT were observed | Positive treatment effects, with stabilization of ocular signs and negative eye and nasal cultures |
| Jennes, S. et al. [41] | Belgium | 2017 | Pseudomonas aeruginosa | Acute kidney infection after injury | 1/male/61 years of age | Peritonitis owing to Enterobacter cloacae and severe abdominal sepsis with disseminated intravascular coagulation secondary to strangulated diaphragmatic hernia. The patient had a prolonged hospital stay complicated by peripheral gangrene of his extremities, which resulted in the amputation of the lower limbs and the development of large necrotic pressure ulcers. | No adverse effects related to PT were observed | Positive treatment effects; blood cultures were negative, CRP levels decreased, and fever disappeared. Kidney function recovered within a few days. However, the patient died after 4 months from a sudden refractory cardiac arrest in the hospital due to Klebsiella pneumoniae. |
| Kuipers, S. et al. [42] | Holland | 2020 | Klebsiella pneumoniae | Recurrent urinary tract infection | 1/male/58 years of age | Kidney transplant | No adverse effects related to PT were observed | Positive treatment effects. The symptoms of urethritis quickly disappeared. |
| Onsea, S. et al. [43] | Belgium | 2019 | P. aeruginosa and S. epidermidis | Chronic osteomyelitis of the pelvis | Patient 1 | Isolated fibrous tumor in the left pelvic region | Not reported | Positive treatment effects. C-reactive protein and white blood cell levels returned to normal. |
| P. aeruginosa and S. epidermidis | Non-union of distal femur | Patient 2 | Polytrauma after aggression, with open segmental fractures of the right femur | Not reported | Positive treatment effects. The levels of C-reactive protein and white blood cells returned to normal. Infection-free. | |||
| S. agalactiae and S. aureus | Postoperative problems of the femur wound | Patient 3 | Polytrauma after the collapse of a building, with crush injuries of the upper right leg and complex fractures of the femur | Not reported | Positive treatment effects. C-reactive protein and white blood cell levels returned to normal. | |||
| E. faecalis | Infection of the surgical site with abscess formation and evolution to osteomyelitis of the femur | Patient 4 | Polytrauma after traffic accident, with fracture of the femur | Local redness and pain | Positive treatment effects. C-reactive protein and white blood cell levels returned to normal. | |||
| Wu, N. et al. [27] | Shanghai, China | 2021 | Acinetobacter baumannii | Respiratory tract infection acquired in the hospital | 1/male/62 years of age | Critical condition due to COVID-19 (RNA-negative) and co-infection with Candida albicans and Ralstonia mannitolilytica | Cytokine storm and fever 4 h after 1Ф phage administration | Positive treatment effects. Clinical improvement, discharged from the hospital on day 30. |
| Respiratory tract and intubation wound infections acquired in the hospital | 1/male/64 years of age | Critical condition due to COVID-19 (RNA-negative) | No adverse effects related to PT were observed | Positive treatment effects. Clinical improvement and discharge from the hospital on day 9. | ||||
| Respiratory tract infection acquired in the hospital | 1/male/81 years of age | Critical condition due to COVID-19 (RNA-negative) and co-infection with Candida albicans and Candida glabrata | No adverse effects related to PT were observed | Positive treatment effects. The infection was eliminated; however, patient died on day 10 owing to respiratory failure caused by infection with Klebsiella pneumoniae. | ||||
| Respiratory tract and bladder infections acquired in the hospital | 1/male/78 years of age | Critical status due to COVID-19 (RNA-negative) and co-infection with Candida albicans, Klebsiella pneumoniae resistant to carbapenems, and Sphingomonas paucimobilis | No adverse effects related to PT were observed | Positive treatment effect with improvement, patient was discharged from the ICU on day 7; however, he died on day 40 owing to respiratory failure | ||||
| Bao, J. et al. [22] | Shanghai, China | 2020 | Klebsiella pneumoniae | Recurrent urinary tract infection | 1/female/63 years of age | Type II diabetes and hypertension | No adverse effects related to PT were observed | Positive treatment effect. The infection was completely eradicated. |
| Rose, T. et al. [39] | Brussels, Belgium | 2014 | Pseudomonas aeruginosa and Staphylococcus aureus | Burn infection | 9/4 men, 5 women/ 27–88 years of age | Not reported | No adverse effects related to PT were observed | Negative treatment effect. Low bacterial load, almost unchanged. |
| Rubalskii, E. et al. [32] | Germany | 2020 | Staphylococcus aureus, Enterococcus faecium, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Escherichia coli | Patients had infections associated with immunosuppression after organ transplantation or had infections of vascular grafts, implanted medical devices, and surgical wounds | 8/7 men, 1 woman | Not reported | No adverse effects related to PT were observed | Positive effect of treatment in 7 patients who are completely cured; the other showed a significant improvement in terms of decreased bacterial load |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pires, D.P.; Cleto, S.; Sillankorva, S.; Azeredo, J.; Lu, T.K. Genetically Engineered Phages: A Review of Advances over the Last Decade. Microbiol. Mol. Biol. Rev. 2016, 80, 523–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payaslian, F.; Gradaschi, V.; Piuri, M. Genetic Manipulation of Phages for Therapy Using BRED. Curr. Opin. Biotechnol. 2021, 68, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Henry, M.; O’Sullivan, O.; Sleator, R.D.; Coffey, A.; Ross, R.P.; McAuliffe, O.; O’Mahony, J.M. In Silico Analysis of Ardmore, a Novel Mycobacteriophage Isolated from Soil. Gene 2010, 453, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Kilcher, S.; Loessner, M.J. Engineering Bacteriophages as Versatile Biologics. Trends Microbiol. 2019, 27, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Martínez, D.A.; Puente-Muñoz, A.I. Bacterias, Endotoxinas Y Neuroinflamación Crónica: ¿Una Etiopatogenia Para Las Enfermedad De Alzheimer? Rev. Ecuatoriana Neurol. 2020, 29, 137–144. [Google Scholar] [CrossRef]
- Vispo, N.S.; Puchades, Y. Bacteriófagos: De La Terapia Con Fagos a La Biología Combinatoria. Biotecnol. Apl. 2001, 18, 135–147. [Google Scholar]
- Ukuhor, H.O. The Interrelationships between Antimicrobial Resistance, COVID-19, Past, and Future Pandemics. J. Infect. Public Health 2021, 14, 53–60. [Google Scholar] [CrossRef]
- World Health Organization New Report Calls for Urgent Action to Avert Antimicrobial Resistance Crisis. Available online: https://www.who.int/news/item/29-04-2019-new-report-calls-for-urgent-action-to-avert-antimicrobial-resistance-crisis (accessed on 31 March 2022).
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, Research, and Development of New Antibiotics: The WHO Priority List of Antibiotic-Resistant Bacteria and Tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Cecchini, M. Stemming the Superbug Tide Just a Few Dollars More; Organisation for Economic Co-Operation and Development: Paris, France, 2018; pp. 1–10. [Google Scholar]
- Suzuki, Y.; Ishimoto, T.; Fujita, S.; Kiryu, S.; Wada, M.; Akatsuka, T.; Saito, M.; Kawano, M. Antimicrobial Antisense RNA Delivery to F-Pili Producing Multidrug-Resistant Bacteria via a Genetically Engineered Bacteriophage. Biochem. Biophys. Res. Commun. 2020, 530, 533–540. [Google Scholar] [CrossRef]
- Tinoco, J.M.; Liss, N.; Zhang, H.; Nissan, R.; Gordon, W.; Tinoco, E.; Sassone, L.; Stevens, R. Antibacterial Effect of Genetically-Engineered Bacteriophage ΦEf11/ΦFL1C(Δ36)PnisA on Dentin Infected with Antibiotic-Resistant Enterococcus Faecalis. Arch. Oral Biol. 2017, 82, 166–170. [Google Scholar] [CrossRef]
- García, I.; Porras, M. Aislamiento de Bacteriófagos de Pseudomonas Aeruginosa Multidrogo–Resistente En Aguas de Tres Ríos de la Provincia de Lima-Perú; Universidad Nacional Mayor de San Marcos: Lima, Peru, 2018. [Google Scholar]
- Sinha, A.; Eniyan, K.; Manohar, P.; Ramesh, N.; Bajpai, U. Characterization and Genome Analysis of B1 Sub-Cluster Mycobacteriophage PDRPxv. Virus Res. 2020, 279, 197884. [Google Scholar] [CrossRef] [PubMed]
- Romero, J.; Feijoo, C.G.; Navarrete, P. Antibiotics in Aquaculture–Use, Abuse and Alternatives. Heal. Environ. Aquac. 2012, 159, 198. [Google Scholar] [CrossRef] [Green Version]
- Cebriá-Mendoza, M.; Sanjuán, R.; Domingo-Calap, P. Directed Evolution of a Mycobacteriophage. Antibiotics 2019, 8, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajpai, U.; Mehta, A.K.; Eniyan, K.; Sinha, A.; Ray, A.; Virdi, S.; Ahmad, S.; Shah, A.; Arora, D.; Marwaha, D.; et al. Isolation and Characterization of Bacteriophages from India, with Lytic Activity against Mycobacterium Tuberculosis. Can. J. Microbiol. 2018, 64, 483–491. [Google Scholar] [CrossRef] [Green Version]
- Chan, B.K.; Abedon, S.T.; Loc-Carrillo, C. Phage Cocktails and the Future of Phage Therapy. Future Microbiol. 2013, 8, 769–783. [Google Scholar] [CrossRef]
- Aslam, S.; Courtwright, A.M.; Koval, C.; Lehman, S.M.; Morales, S.; Furr, C.L.L.; Rosas, F.; Brownstein, M.J.; Fackler, J.R.; Sisson, B.M.; et al. Early Clinical Experience of Bacteriophage Therapy in 3 Lung Transplant Recipients. Am. J. Transplant 2019, 19, 2631–2639. [Google Scholar] [CrossRef]
- De Oliveira, A.; Souza, R.; Piscoya, M.E.; Iquiapaza, R.A. Resistencia Bacteriana y Mortalidad En Un Centro de Terapia Intensiva. Rev. Latino-Am. Enferm. 2010, 18, 6–10. [Google Scholar]
- Harper, D.R.; Parracho, H.M.R.T.; Walker, J.; Sharp, R.; Hughes, G.; Werthén, M.; Lehman, S.; Morales, S. Bacteriophages and Biofilms. Antibiotics 2014, 3, 270. [Google Scholar] [CrossRef]
- Bao, J.; Wu, N.; Zeng, Y.; Chen, L.; Li, L.; Yang, L.; Zhang, Y.; Guo, M.; Li, L.; Li, J.; et al. Non-Active Antibiotic and Bacteriophage Synergism to Successfully Treat Recurrent Urinary Tract Infection Caused by Extensively Drug-Resistant Klebsiella Pneumoniae. Emerg. Microbes Infect. 2020, 9, 771–774. [Google Scholar] [CrossRef] [Green Version]
- Jault, P.; Leclerc, T.; Jennes, S.; Pirnay, J.P.; Que, Y.A.; Resch, G.; Rousseau, A.F.; Ravat, F.; Carsin, H.; Le Floch, R.; et al. Efficacy and Tolerability of a Cocktail of Bacteriophages to Treat Burn Wounds Infected by Pseudomonas Aeruginosa (PhagoBurn): A Randomised, Controlled, Double-Blind Phase 1/2 Trial. Lancet. Infect. Dis. 2019, 19, 35–45. [Google Scholar] [CrossRef]
- Qin, J.; Wu, N.; Bao, J.; Shi, X.; Ou, H.; Ye, S.; Zhao, W.; Wei, Z.; Cai, J.; Li, L.; et al. Heterogeneous Klebsiella Pneumoniae Co-Infections Complicate Personalized Bacteriophage Therapy. Front. Cell. Infect. Microbiol. 2021, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schooley, R.T.; Biswas, B.; Gill, J.J.; Hernandez-Morales, A.; Lancaster, J.; Lessor, L.; Barr, J.J.; Reed, S.L.; Rohwer, F.; Benler, S.; et al. Development and Use of Personalized Bacteriophage-Based Therapeutic Cocktails To Treat a Patient with a Disseminated Resistant Acinetobacter Baumannii Infection. Antimicrob. Agents Chemother. 2017, 61, e00954-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, X.; Chen, H.; Zhang, M.; Zhao, Y.; Jiang, Y.; Liu, X.; Huang, W.; Ma, Y. Clinical Experience of Personalized Phage Therapy Against Carbapenem-Resistant Acinetobacter Baumannii Lung Infection in a Patient With Chronic Obstructive Pulmonary Disease. Front. Cell. Infect. Microbiol. 2021, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Dai, J.; Guo, M.; Li, J.; Zhou, X.; Li, F.; Gao, Y.; Qu, H.; Lu, H.; Jin, J.; et al. Pre-Optimized Phage Therapy on Secondary Acinetobacter Baumannii Infection in Four Critical COVID-19 Patients. Emerg. Microbes Infect. 2021, 10, 612–618. [Google Scholar] [CrossRef]
- Corbellino, M.; Kieffer, N.; Kutateladze, M.; Balarjishvili, N.; Leshkasheli, L.; Askilashvili, L.; Tsertsvadze, G.; Rimoldi, S.G.; Nizharadze, D.; Hoyle, N.; et al. Eradication of a Multidrug-Resistant, Carbapenemase-Producing Klebsiella Pneumoniae Isolate Following Oral and Intra-Rectal Therapy With a Custom Made, Lytic Bacteriophage Preparation. Clin. Infect. Dis. 2020, 70, 1998–2001. [Google Scholar] [CrossRef]
- Hoyle, N.; Zhvaniya, P.; Balarjishvili, N.; Bolkvadze, D.; Nadareishvili, L.; Nizharadze, D.; Wittmann, J.; Rohde, C.; Kutateladze, M. Phage Therapy against Achromobacter Xylosoxidans Lung Infection in a Patient with Cystic Fibrosis: A Case Report. Res. Microbiol. 2018, 169, 540–542. [Google Scholar] [CrossRef]
- Cano, E.J.; Caflisch, K.M.; Bollyky, P.L.; Van Belleghem, J.D.; Patel, R.; Fackler, J.; Brownstein, M.J.; Horne, B.; Biswas, B.; Henry, M.; et al. Phage Therapy for Limb-Threatening Prosthetic Knee Klebsiella Pneumoniae Infection: Case Report and In Vitro Characterization of Anti-Biofilm Activity. Clin. Infect. Dis. 2021, 73, E144–E151. [Google Scholar] [CrossRef]
- Fadlallah, A.; Chelala, E.; Legeais, J.-M. Corneal Infection Therapy with Topical Bacteriophage Administration. Open Ophthalmol. J. 2015, 9, 167–168. [Google Scholar] [CrossRef] [Green Version]
- Rubalskii, E.; Ruemke, S.; Salmoukas, C.; Boyle, E.C.; Warnecke, G.; Tudorache, I.; Shrestha, M.; Schmitto, J.D.; Martens, A.; Rojas, S.V.; et al. Bacteriophage Therapy for Critical Infections Related to Cardiothoracic Surgery. Antibiotics 2020, 9, 232. [Google Scholar] [CrossRef]
- Tkhilaishvili, T.; Winkler, T.; Müller, M.; Perka, C.; Trampuz, A. Bacteriophages as Adjuvant to Antibiotics for the Treatment of Periprosthetic Joint Infection Caused by Multidrug-Resistant Pseudomonas Aeruginosa. Antimicrob. Agents Chemother. 2019, 64, e00924-19. [Google Scholar] [CrossRef] [Green Version]
- Law, N.; Logan, C.; Yung, G.; Furr, C.L.L.; Lehman, S.M.; Morales, S.; Rosas, F.; Gaidamaka, A.; Bilinsky, I.; Grint, P.; et al. Successful Adjunctive Use of Bacteriophage Therapy for Treatment of Multidrug-Resistant Pseudomonas Aeruginosa Infection in a Cystic Fibrosis Patient. Infection 2019, 47, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Nir-Paz, R.; Gelman, D.; Khouri, A.; Sisson, B.M.; Fackler, J.; Alkalay-Oren, S.; Khalifa, L.; Rimon, A.; Yerushalmy, O.; Bader, R.; et al. Successful Treatment of Antibiotic-Resistant, Poly-Microbial Bone Infection With Bacteriophages and Antibiotics Combination. Clin. Infect. Dis. 2019, 69, 2015–2018. [Google Scholar] [CrossRef] [PubMed]
- Duplessis, C.; Biswas, B.; Hanisch, B.; Perkins, M.; Henry, M.; Quinones, J.; Wolfe, D.; Estrella, L.; Hamilton, T. Refractory Pseudomonas Bacteremia in a 2-Year-Old Sterilized by Bacteriophage Therapy. J. Pediatric Infect. Dis. Soc. 2018, 7, 253–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ooi, M.L.; Drilling, A.J.; Morales, S.; Fong, S.; Moraitis, S.; MacIas-Valle, L.; Vreugde, S.; Psaltis, A.J.; Wormald, P.J. Safety and Tolerability of Bacteriophage Therapy for Chronic Rhinosinusitis Due to Staphylococcus Aureus. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 723–729. [Google Scholar] [CrossRef]
- Leitner, L.; Ujmajuridze, A.; Chanishvili, N.; Goderdzishvili, M.; Chkonia, I.; Rigvava, S.; Chkhotua, A.; Changashvili, G.; McCallin, S.; Schneider, M.P.; et al. Intravesical Bacteriophages for Treating Urinary Tract Infections in Patients Undergoing Transurethral Resection of the Prostate: A Randomised, Placebo-Controlled, Double-Blind Clinical Trial. Lancet. Infect. Dis. 2021, 21, 427–436. [Google Scholar] [CrossRef]
- Rose, T.; Verbeken, G.; De Vos, D.; Merabishvili, M.; Vaneechoutte, M.; Lavigne, R.; Jennes, S.; Zizi, M.; Pirnay, J.-P. Experimental Phage Therapy of Burn Wound Infection: Difficult First Steps. Int. J. Burns Trauma 2014, 4, 66. [Google Scholar]
- Nadareishvili, L.; Hoyle, N.; Nakaidze, N.; Nizharadze, D.; Kutateladze, M.; Balarjishvili, N.; Kutter, E.; Pruidze, N. Bacteriophage Therapy as a Potential Management Option for Surgical Wound Infections. Phage 2020, 1, 158–165. [Google Scholar] [CrossRef]
- Jennes, S.; Merabishvili, M.; Soentjens, P.; Pang, K.W.; Rose, T.; Keersebilck, E.; Soete, O.; François, P.M.; Teodorescu, S.; Verween, G.; et al. Use of Bacteriophages in the Treatment of Colistin-Only-Sensitive Pseudomonas Aeruginosa Septicaemia in a Patient with Acute Kidney Injury-a Case Report. Crit. Care 2017, 21, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Kuipers, S.; Ruth, M.M.; Mientjes, M.; de Sévaux, R.G.L.; van Ingen, J. A Dutch Case Report of Successful Treatment of Chronic Relapsing Urinary Tract Infection with Bacteriophages in a Renal Transplant Patient. Antimicrob. Agents Chemother. 2019, 64, e01281-19. [Google Scholar] [CrossRef] [Green Version]
- Onsea, J.; Soentjens, P.; Djebara, S.; Merabishvili, M.; Depypere, M.; Spriet, I.; De Munter, P.; Debaveye, Y.; Nijs, S.; Vanderschot, P.; et al. Bacteriophage Application for Difficult-to-Treat Musculoskeletal Infections: Development of a Standardized Multidisciplinary Treatment Protocol. Viruses 2019, 11, 891. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.; Singh, H.S.; Shukla, V.K.; Nath, G.; Bhartiya, S.K. Bacteriophage Therapy of Chronic Nonhealing Wound: Clinical Study. Int. J. Low. Extrem. Wounds 2019, 18, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Lebeaux, D.; Merabishvili, M.; Caudron, E.; Lannoy, D.; Van Simaey, L.; Duyvejonck, H.; Guillemain, R.; Thumerelle, C.; Podglajen, I.; Compain, F.; et al. A Case of Phage Therapy against Pandrug-Resistant Achromobacter Xylosoxidans in a 12-Year-Old Lung-Transplanted Cystic Fibrosis Patient. Viruses 2021, 13, 60. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.R.; Bhartiya, S.K.; Kumar, R.; Shukla, V.K.; Nath, G. Use of Customized Bacteriophages in the Treatment of Chronic Nonhealing Wounds: A Prospective Study. Int. J. Low. Extrem. Wounds 2021, 20, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Oechslin, F.; Piccardi, P.; Mancini, S.; Gabard, J.; Moreillon, P.; Entenza, J.M.; Resch, G.; Que, Y.A. Synergistic Interaction Between Phage Therapy and Antibiotics Clears Pseudomonas Aeruginosa Infection in Endocarditis and Reduces Virulence. J. Infect. Dis. 2017, 215, 703–712. [Google Scholar] [CrossRef] [Green Version]
- Chan, B.K.; Turner, P.E.; Kim, S.; Mojibian, H.R.; Elefteriades, J.A.; Narayan, D. Phage Treatment of an Aortic Graft Infected with Pseudomonas Aeruginosa. Evol. Med. Public Heal. 2018, 2018, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Hernando, M.; Barrero, L.; Villalobos, A. Resistencia Bacteriana a Los Antimicrobianos en el Ambito Hospitalario; Universidad Nacional Mayor de San Marcos: Lima, Peru, 2018; pp. 1–17. [Google Scholar]
| Author(s)/ Reference | Phage/Cocktail Identification | Number of Phages in the Cocktail | Phage Order or Family | Route of Administration | Concentration Per Unit Dose/Duration of Treatment | Antibiotics |
|---|---|---|---|---|---|---|
| Ooi, M.L. et al. [37] | Cocktail AB-SA01 | 3 | Myoviridae | Nasal irrigation | 3 × 108–109 PFU, for 14 days | NA |
| Schooley, R.T. et al. [25] | AB-Navy1-AB-Navy4-AB-Navy71-AB-Navy97-AbTP3Φ1-AC4-C1P12-C2P21-C2P24, cocktails ΦPC-ΦIV-ΦIVB | 8 | Myoviridae-Podoviridae (AbTP3Φ1) | Intravenous-Intracavitary | 5 × 109 PFU, for 2 to 16 weeks | Meropenem, fluconazole, and minocycline |
| Jault, P. et al. [23] | Cocktail PP1131 | 12 | Not reported | Topical | 1 × 106 PFU, for 7 days | NA |
| Law, N. et al. [34] | Cocktail ABPA01 | 4 | Not reported | Intravenous | 4 × 109 PFU, for 8 weeks | Ciprofloxacin, piperacillin–tazobactam, doripenem |
| Aslam, S. et al. [19] | Cocktails AB-PA01, AB-PA01-m1, Navy 1, Navy 2 | 4, 5, 2, 3 | Not reported | Intravenous | Between 5.3 × 106 PFU and 5 × 109 PFU for 3 to 5 weeks | Piperacillin-tazobactam and colistin |
| Cocktail AB-PA01 | 4 | Piperacillin-tazobactam, tobramycin, and inhaled colistin | ||||
| BdPF16phi4281 | 1 | Meropenem, ceftazidime-avibactam, minocycline, and tobramycin | ||||
| Nir-Paz, R. et al. [35] | ФAbKT21phi3 and ФKpKT21phi1 | 2 | Not reported | Intravenous | 5 × 107 PFU for 5 days | Colistin and meropenem |
| Tkhilaisshvili, T. et al. [33] | Local phage adjuvants | Not reported | Not reported | Intravenous (local administration system) | 108 PFU for 5 days | Colistin, meropenem, and ceftazidime |
| Corbellino, M. et al. [28] | vB_KpnM_GF | Not reported | Not reported | Oral and intrarectal | Did not report concentration, for 3 weeks | NA |
| Duplessis, C. et al. [36] | Phage cocktail | 2 | Not reported | Intravenous | 3.5 × 105 PFU, did not specify duration of treatment | NA |
| Qin, J. et al. [24] | Phage cocktails Ф902, ФJD905, ФJD907, ФJD908, JD910 | 5 | Podoviridae, Myoviridae (ФJD905) | Irrigations | 5 × 108 PFU for 4 weeks | piperacillin– tazobactam, imipenem, amikacin |
| Tan, X. et al. [26] | Unique Ab_SZ3 phage | 1 | Siphoviridae | Airway (vibrating mesh nebulizer) | Increasing concentrations: 5 × 106 on day 1 to 2.5 × 107 PFU, day 2 with 108 PFU, day 4 with 109 PFU, and day 13 with 5 × 1010 PFU for 16 days | Tigecycline and polymyxin E |
| Hoyle, N. et al. [29] | Phage cocktail | 2 | Siphoviridae | Inhalation (compressor nebulizer) | 3 × 108 PFU for 20 days | Piperacillin- tazobactam |
| Leiter, L. et al. [38] | PYO cocktail | Not reported | Not reported | Intravesical instillation | 104 to 105 PFU for 7 days | NA |
| Cano, E.J. et al. [30] | Phage KpJH46Φ2 | 1 | Not reported | Peripheral intravenous | 40 doses of 6.3 × 1010 PFU/mL for 30 min plus minocycline | Minocycline |
| Gupta, P. et al. [44] | Phage cocktail | 3 | Not reported | Topical | 0.1 mL/cm2 (a concentration of 109 PFU/mL from 9 to 13 days) | NA |
| Lebeaux, D. et al. [45] | JW Delta, JWT, and 2-1 cocktails (APC 1.1) | 3 | Not reported | Inhalation (vibrating mesh nebulizer) | 4 × 1010 PFU (3 nebulizations/day of 5 mL of solution). Did not specify the duration of treatment. | Imipenem |
| Cocktail 2, plus phage JW alpha (APC 2.1) | 4 | Not reported | Administered to the lungs using a fibroscope and through nebulization | 5 × 109 PFU/mL. Did not specify the duration of treatment. | NA | |
| Nadareishvili, L. et al. [40] | Staphylococcal bacteriophage, PYO bacteriophage, and SES bacteriophage | 3 | Not reported | Topical and oral | Did not specify the concentration; 10 mL once a day for 20 days and then for 2 weeks | NA |
| Staphylococcus bacteriophage and Intesti bacteriophage | 2 | Not reported | Topical and oral | Did not specify the concentration; 10 mL once a day for 20 days initially and then for 15 days | NA | |
| Staphylococcus bacteriophage and Intesti bacteriophage | 2 | Not reported | Topical and oral | Did not specify the concentration; 10 mL once a day for 20 days initially and then for 20 days | NA | |
| Pyo bacteriophage and Intesti bacteriophage | 2 | Not reported | Topical and oral | Did not specify the concentration; 10 mL once a day for 20 days initially and then for 20 days. Solcoseryl (epithelial regenerator) was also used. | NA | |
| Patel, D.R. et al. [46] | Phage cocktail | Not reported | Not reported | Topical | Did not specify the concentration or the duration of treatment; 500 μL/cm2, 5–7 applications | NA |
| Fadlallah, A. et al. [31] | Phage SATA-8505 (ATCC PTA-9476) | 1 | Not reported | Topical (eye drops and nasal spray) and general (intravenous) | Did not specify the concentration, for 4 weeks | NA |
| Jennes, S. et al. [41] | BFC1 Cocktail | 2 | Not reported | 50 microliters administered through intravenous infusion for 6 h over 10 days. Wounds were irrigated with 50 mL of BFC1 every 8 h for 10 days. | Did not specify the concentration, for 10 days | NA |
| Kuipers, S. et al. [42] | Anti-Klebsiella pneumoniae phages | Not reported | Not reported | Oral and bladder irrigation/ intravesical | Did not report the concentration, for 8 weeks | NA |
| Onsea, S. et al. [43] | COCKTAIL BCF1 | 3 | Not reported | Topical and in marrow | 107 PFU/mL for 7 days | Vancomycin, rifampicin, moxifloxacin |
| COCKTAIL BCF1 | 3 | Not reported | Topical | 107 PFU/mL for 10 days | Vancomycin, colistin, fosfomycin | |
| COCKTAIL BCF1 | 3 | Not reported | Topical | 107 PFU/mL for 9 days | Vancomycin, clindamycin, moxifloxacin | |
| PYO phage | Not reported | Not reported | Topical | 107 PFU/mL for 7 days | Amoxicillin | |
| Wu, N. et al. [27] | Phage 1Ф (ФAb124) | 1 | Podoviridae | Respiratory by inhalation | 108 PFU/mL for 20 min, two doses with 1 h interval | NA |
| Cocktail 2Ф (ФAb124 and ФAb121) | 2 | Podoviridae and Myoviridae | Respiratory by inhalation | 1 × 1010 PFU, did not specify concentration | NA | |
| Cocktail 2Ф (ФAb124 and ФAb121) | 2 | Podoviridae and Myoviridae | Respiratory by inhalation and topical with a wet compress | 1 × 1010 PFU, did not specify concentration | NA | |
| Cocktail 2Ф (ФAb124 and ФAb121) | 2 | Podoviridae and Myoviridae | Respiratory by inhalation | 1 × 1010 PFU, did not specify concentration | NA | |
| Cocktail 2Ф (ФAb124 and ФAb121) | 2 | Podoviridae and Myoviridae | Respiratory by inhalation | 1 × 1010 PFU, did not specify concentration | NA | |
| Bao, J. et al. [22] | Cocktail I (SZ-1, SZ-2, SZ-3, SZ-6) against the CX7224 strain | 5 | Not reported | Bladder irrigation | 5 × 108 PFU per mL of each phage for 5 days | NA |
| Cocktail II (Kp165, Kp166, Kp167, Kp158, and Kp169) for the CX8070 strain | 5 | Not reported | Bladder irrigation | Did not specify the concentration, for 5 days | NA | |
| Cocktail III (Kp152, Kp154, Kp155, Kp164, Kp6377, and HD001) | 6 | Not reported | Bladder irrigation | SMZ-TMP administered orally (800–160 mg) twice daily, plus the cocktail for 5 days | NA | |
| Rose, T. et al. [39] | BFC-1 cocktail (P. aeruginosa phage 14/1, S. aureus phages ISP and PNM) | 3 | Podoviridae and Myoviridae | Topical | 109 PFU/mL, did not specify the duration of treatment | Ceftazidime or meropenem in combination with amikacin. Vancomycin or linezolid. |
| Rubalskii, E. et al. [32] | Staphylococcus phage CH1, Enterococcus phage Enf1, Pseudomonas phage PA5, Pseudomonas phage PA10 | 4 | Myoviridae, Siphoviridae, Myoviridae, Myoviridae | Local | 1 × 108 PFU/ml | Cefepime, daptomycin, linezolid, tobramycin |
| Klebsiella phage KPV811, Klebsiella phage KPV15 | 2 | Podoviridae, Myoviridae | Respiratory by inhalation, via nasogastric tube | 1 × 108 PFU/ml | Ceftazidime, linezolid, avibactam, colistin, meropenem, cotrimoxazole, tobramycin | |
| Staphylococcus phage CH1 | 1 | Myoviridae | local application via drainage | 1 × 109 PFU/ml | Rifampicin, flucloxacillin | |
| Staphylococcus phage CH1 | 1 | Myoviridae | local application via drainage | 1 × 109 PFU/ml | Daptomycin | |
| Staphylococcus phage Sa30, Staphylococcus phage CH1, Staphylococcus phage SCH1, Staphylococcus phage SCH111 | 4 | Myoviridae, Myoviridae, Podoviridae, Podoviridae | Local application via drainage, intranasal | 1 ×109 PFU/ml | Daptomycin | |
| Staphylococcus phage Sa30 | 1 | Myoviridae | Locally, intraoperatively mixed with fibrin glue | 4 × 1010 PFU/ml | Sultamicillin | |
| Escherichia phage ECD7, Escherichia phage V18 | 2 | Myoviridae | Locally, intraoperatively mixed with fibrin glue | 4 × 1010 PFU/ml | Clindamycin | |
| Pseudomonas phage PA5, Pseudomonas phage PA10 | 2 | Myoviridae | Locally, intraoperatively mixed with fibrin glue | 4 ×1010 PFU/ml | Colistin, ceftazidime, avibactam |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aranaga, C.; Pantoja, L.D.; Martínez, E.A.; Falco, A. Phage Therapy in the Era of Multidrug Resistance in Bacteria: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 4577. https://doi.org/10.3390/ijms23094577
Aranaga C, Pantoja LD, Martínez EA, Falco A. Phage Therapy in the Era of Multidrug Resistance in Bacteria: A Systematic Review. International Journal of Molecular Sciences. 2022; 23(9):4577. https://doi.org/10.3390/ijms23094577
Chicago/Turabian StyleAranaga, Carlos, Lady Daniela Pantoja, Edgar Andrés Martínez, and Aura Falco. 2022. "Phage Therapy in the Era of Multidrug Resistance in Bacteria: A Systematic Review" International Journal of Molecular Sciences 23, no. 9: 4577. https://doi.org/10.3390/ijms23094577
APA StyleAranaga, C., Pantoja, L. D., Martínez, E. A., & Falco, A. (2022). Phage Therapy in the Era of Multidrug Resistance in Bacteria: A Systematic Review. International Journal of Molecular Sciences, 23(9), 4577. https://doi.org/10.3390/ijms23094577