Effects of Orally Administered Resveratrol on TNF, IL-1β, Leukocyte Phagocytic Activity and Oxidative Burst Function in Horses: A Prospective, Randomized, Double-Blinded, Placebo-Controlled Study


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. Patient Population
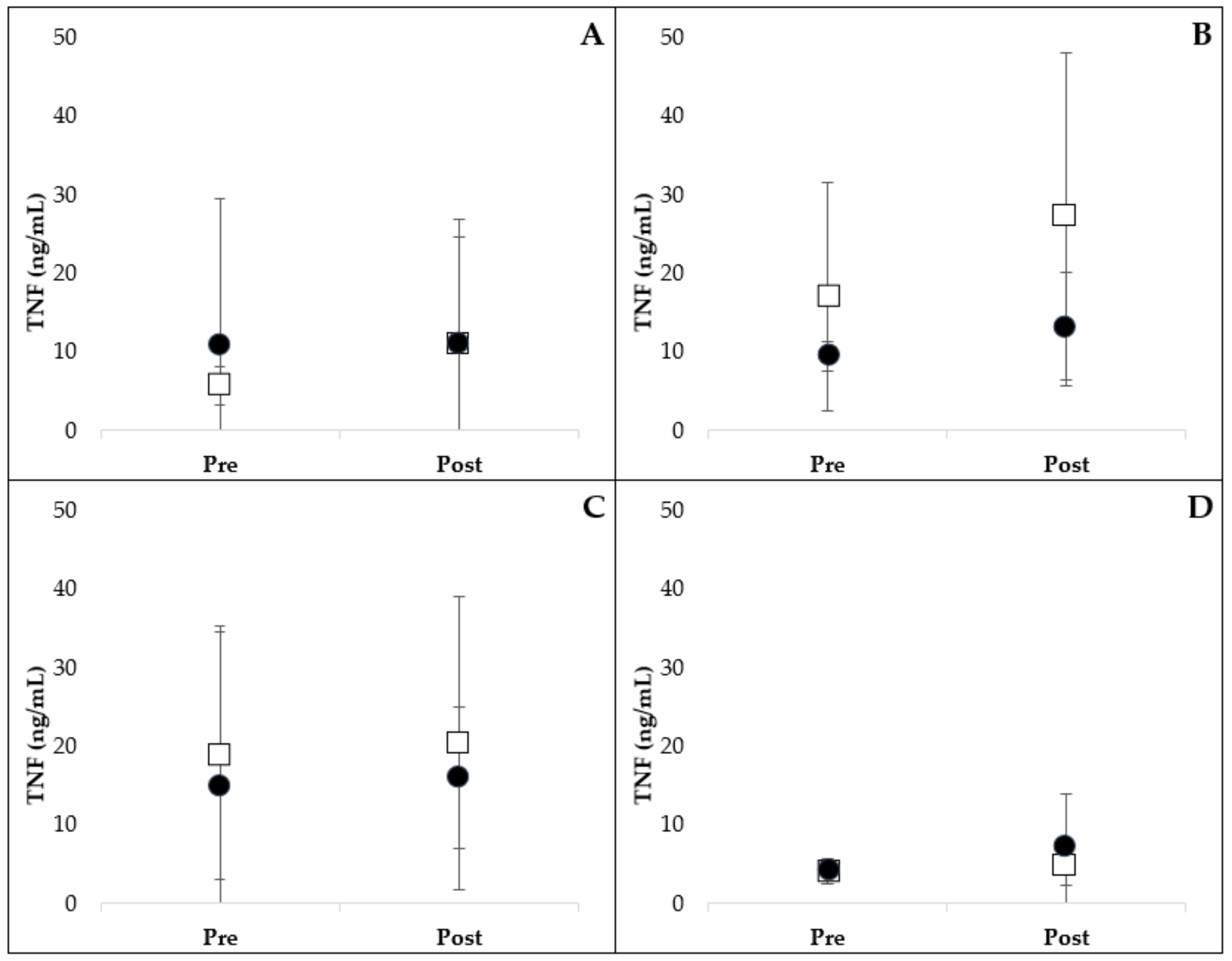
2.2. Leukocyte Cytokine Production
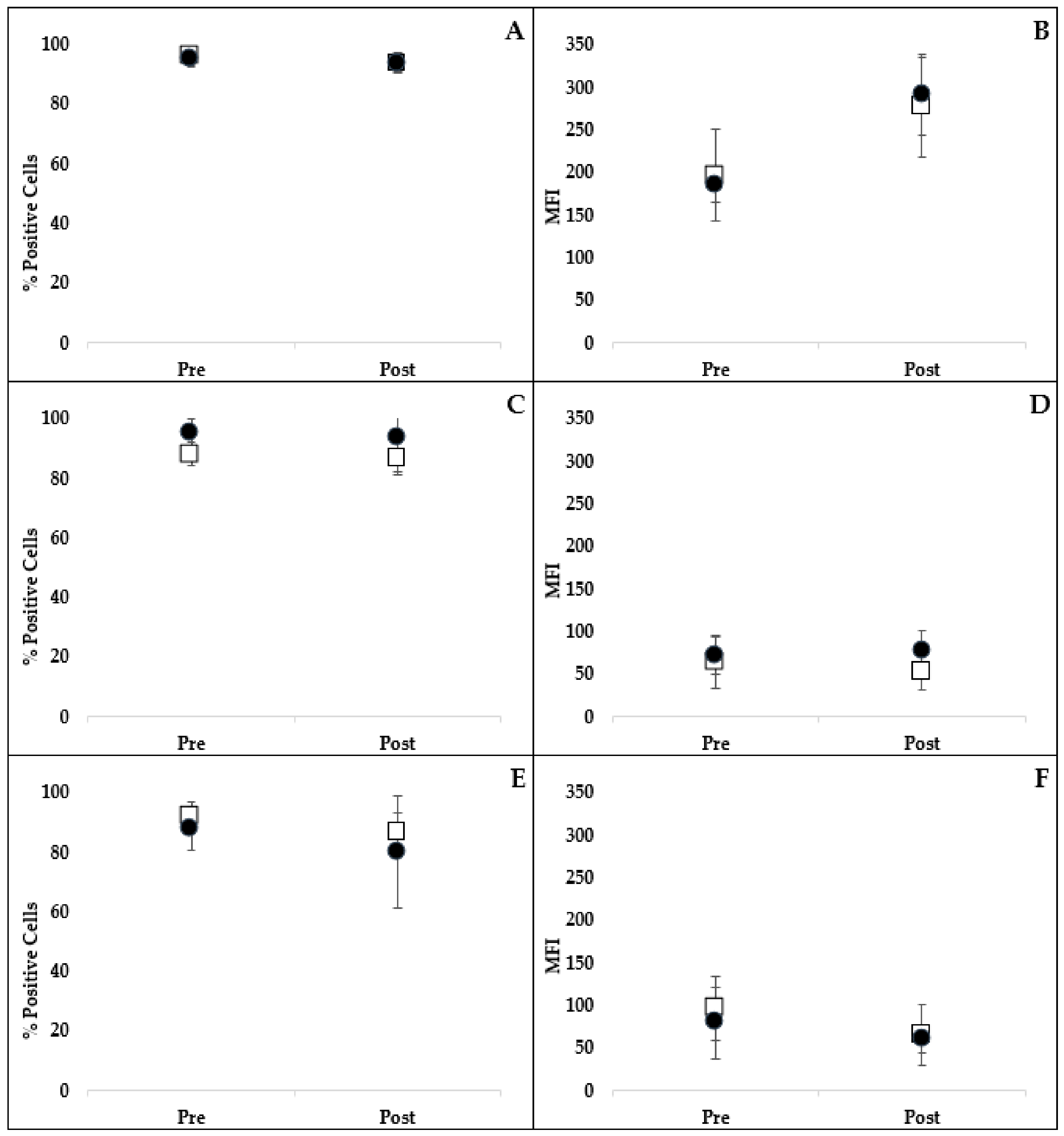
2.3. Phagocytosis and Oxidative Burst
3. Discussion
4. Materials and Methods
4.1. Resveratrol and Control
4.2. Animals and Monitoring
4.3. Sample Collection
4.4. Leukocyte Cytokine Production
4.5. TNF Assay
4.6. IL-1β Assay
4.7. Phagocytic and Oxidative Burst Function
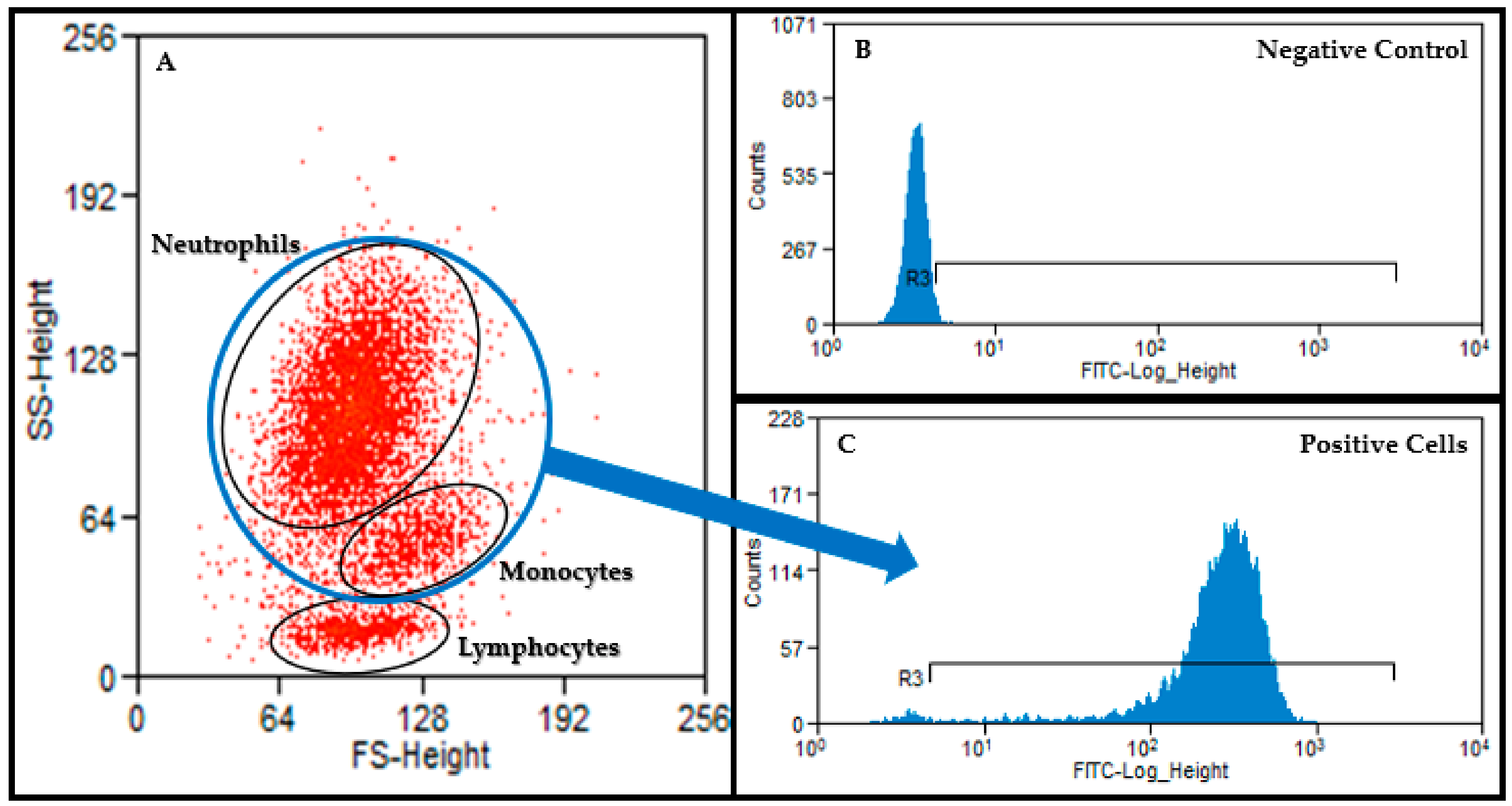
4.8. Flow Cytometry
4.9. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| COX | cyclo-oxygenase |
| E. coli | Escherichia coli |
| IL | interleukin |
| LPS | lipopolysaccharide |
| LTA | lipoteichoic acid |
| MFI | mean fluorescence intensity |
| NSAID | nonsteroidal anti-inflammatory drug |
| PAMP | pathogen-associated molecular pattern |
| PBMC | peripheral blood mononuclear cell |
| PBS | phosphate-buffered saline |
| PG | peptidoglycan |
| PMA | phorbol myristate acetate |
| PMN | polymorphonuclear leukocytes |
| RPMI | Roswell Park Memorial Institute |
| TNF | tumor necrosis factor |
References
- Doucet, M.Y.; Bertone, A.L.; Hendrickson, D.; Hughes, F.; MacAllister, C.; McClure, S.; Reinemeyer, C.; Rossier, Y.; Sifferman, R.; Vrins, A.A.; et al. Comparison of efficacy and safety of paste formulations of firocoxib and phenylbutazone in horses with naturally occurring osteoarthritis. J. Am. Veter. Med. Assoc. 2008, 232, 91–97. [Google Scholar] [CrossRef]
- Hu, H.H.; MacAllister, C.G.; Payton, M.E.; Erkert, R.S. Evaluation of the analgesic effects of phenylbutazone administered at a high or low dosage in horses with chronic lameness. J. Am. Veter. Med. Assoc. 2005, 226, 414–417. [Google Scholar] [CrossRef]
- Gambaro, G.; Perazella, M.A. Adverse renal effects of anti-inflammatory agents: Evaluation of selective and nonselective cyclooxygenase inhibitors. J. Intern. Med. 2003, 253, 643–652. [Google Scholar] [CrossRef]
- Nieto, J.E.; Aleman, M.; Anderson, J.D.; Fiack, C.; Snyder, J.R. Effects of phenylbutazone on gene expression of cyclooxygenase-1 and -2 in the oral, glandular gastric, and bladder mucosae of healthy horses. Am. J. Veter. Res. 2012, 73, 98–104. [Google Scholar] [CrossRef]
- Knych, H.K.; Corado, C.R.; McKemie, D.S.; Steffey, E.P. Pharmacokinetics and selected pharmacodynamic effects of tramadol following intravenous administration to the horse. Equine Vet. J. 2013, 45, 490–496. [Google Scholar] [CrossRef]
- Shilo, Y.; Britzi, M.; Eytan, B.; Lifschitz, T.; Soback, S.; Steinman, A. Pharmacokinetics of tramadol in horses after intravenous, intramuscular and oral administration. J. Vet. Pharmacol. Ther. 2008, 31, 60–65. [Google Scholar] [CrossRef]
- Rauf, A.; Imran, M.; Butt, M.S.; Nadeem, M.; Peters, D.G.; Mubarak, M.S. Resveratrol as an anti-cancer agent: A review. Crit. Rev. Food Sci. Nutr. 2018, 58, 1428–1447. [Google Scholar] [CrossRef]
- Singh, A.P.; Singh, R.; Verma, S.S.; Rai, V.; Kaschula, C.H.; Maiti, P.; Gupta, S.C. Health benefits of resveratrol: Evidence from clinical studies. Med. Res. Rev. 2019, 39, 1851–1891. [Google Scholar] [CrossRef]
- Baur, J.A.; Sinclair, D.A. Therapeutic potential of resveratrol: The in vivo evidence. Nat. Rev. Drug Discov. 2006, 5, 493–506. [Google Scholar] [CrossRef]
- Cianciulli, A.; Dragone, T.; Calvello, R.; Porro, C.; Trotta, T.; Lofrumento, D.D.; Panaro, M.A. IL-10 plays a pivotal role in anti-inflammatory effects of resveratrol in activated microglia cells. Int. Immunopharmacol. 2015, 24, 369–376. [Google Scholar] [CrossRef]
- Diaz-Gerevini, G.T.; Repossi, G.; Dain, A.; Tarres, M.C.; Das, U.N.; Eynard, A.R. Beneficial action of resveratrol: How and why? Nutrition 2016, 32, 174–178. [Google Scholar] [CrossRef]
- Park, E.; Pezzuto, J.M. The pharmacology of resveratrol in animals and humans. Biochim. Biophys. Acta Mol. Basis Dis. 2015, 1852, 1071–1113. [Google Scholar] [CrossRef]
- Smoliga, J.; Baur, J.A.; Hausenblas, H.A. Resveratrol and health—A comprehensive review of human clinical trials. Mol. Nutr. Food Res. 2011, 55, 1129–1141. [Google Scholar] [CrossRef]
- Vang, O.; Ahmad, N.; Baile, C.A.; Baur, J.A.; Brown, K.; Csiszar, A.; Das, D.K.; Delmas, M.; Gottfried, C.; Lin, H.-Y.; et al. What Is New for an Old Molecule? Systematic Review and Recommendations on the Use of Resveratrol. PLoS ONE 2011, 6, e19881. [Google Scholar] [CrossRef]
- Beijers, R.; Gosker, H.R.; Schols, A. Resveratrol for patients with chronic obstructive pulmonary disease: Hype or hope? Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 138–144. [Google Scholar] [CrossRef]
- Chen, S.; Zhao, X.; Ran, L.; Wan, J.; Wang, X.; Qin, Y.; Shu, F.; Gao, Y.; Yuan, L.; Zhang, Q.; et al. Resveratrol improves insulin resistance, glucose and lipid metabolism in patients with non-alcoholic fatty liver disease: A randomized controlled trial. Dig. Liver Dis. 2015, 47, 226–232. [Google Scholar] [CrossRef]
- Csiszar, A. Anti-inflammatory effects of resveratrol: Possible role in prevention of age-related cardiovascular disease. Ann. N. Y. Acad. Sci. 2011, 1215, 117–122. [Google Scholar] [CrossRef]
- Zarejavid, A.; Hormoznejad, R.; Yousefimanesh, H.A.; Haghighi-Zadeh, M.H.; Zakerkish, M. Impact of resveratrol supplementation on inflammatory, antioxidant, and periodontal markers in type 2 diabetic patients with chronic periodontitis. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2769–2774. [Google Scholar]
- Samsami-Kor, M.; Daryani, N.E.; Asl, P.R.; Hekmatdoost, A. Anti-Inflammatory Effects of Resveratrol in Patients with Ulcerative Colitis: A Randomized, Double-Blind, Placebo-controlled Pilot Study. Arch. Med. Res. 2015, 46, 280–285. [Google Scholar] [CrossRef]
- Bo, S.; Ciccone, G.; Castiglione, A.; Gambino, R.; De Michieli, F.; Villois, P.; Durazzo, M.; Cavallo-Perin, P.; Cassader, M. Anti-inflammatory and antioxidant effects of resveratrol in healthy smokers a randomized, double-blind, placebo-controlled, cross-over trial. Curr. Med. Chem. 2013, 20, 1323–1331. [Google Scholar] [CrossRef]
- Silva, A.M.; Oliveira, M.I.; Sette, L.; Almeida, C.R.; Oliveira, M.J.; Barbosa, M.A.; Santos, S.G. Resveratrol as a natural anti-tumor necrosis factor-alpha molecule: Implications to dendritic cells and their crosstalk with mesenchymal stromal cells. PLoS ONE 2014, 9, e91406. [Google Scholar]
- Kumar, A.; Sharma, S.S. NF-kappaB inhibitory action of resveratrol: A probable mechanism of neuroprotection in experimental diabetic neuropathy. Biochem. Biophys. Res. Commun. 2010, 394, 360–365. [Google Scholar] [CrossRef]
- Adams, A.; Siard, M.; Reedy, S.; Stewart, C.; Betancourt, A.; Sanz, M.; Horohov, D. Identifying the role of a “caloric restriction mimetic”, resveratrol, in Equine Metabolic Syndrome and its implications for targeted therapy. J. Equine Veter. Sci. 2013, 33, 346–347. [Google Scholar] [CrossRef]
- Ememe, M.U.; Mshelia, P.; Ayo, J.O. Ameliorative Effects of Resveratrol on Oxidative Stress Biomarkers in Horses. J. Equine Veter. Sci. 2015, 35, 518–523. [Google Scholar] [CrossRef]
- Ememe, M.U.; Abdullahi, U.S.; Sackey, A.K.B.; Ayo, J.O.; Mshelia, P.; Edeh, R.E. Effects of a joint supplement whose main components are resveratrol and hyaluronic acid on some biochemical parameters in aged lame horses. J. Equine Sci. 2016, 27, 19–22. [Google Scholar] [CrossRef]
- Ememe, M.; Edeh, E.; Abdullahi, U.S.; Sackey, A.K.B.; Ayo, J.O. Changes in hematological parameters and erythrocyte osmotic fragility in lame and aged horses administered with resveratrol supplement. Afr. J. Biomed. Res. 2016, 19, 37–43. [Google Scholar]
- Kohlhaas, K.S. Effects of Resveratrol Supplementation on Metabolic Health and Reproductive Performance in Obese Mares on Pasture. Master’s Thesis, Virginia Polytechnic Institute and State University, Blacksburg, VA, USA, 26 April 2013. [Google Scholar]
- Watts, A.E.; Dabareiner, R.; Marsh, C.; Carter, G.K.; Cummings, K.J. A randomized, controlled trial of the effects of resveratrol administration in performance horses with lameness localized to the distal tarsal joints. J. Am. Veter. Med. Assoc. 2016, 249, 650–659. [Google Scholar] [CrossRef]
- Zambito, J.L. Effects of Resveratrol Supplementation on Glycemic Response and Oxidant Status in Moderately Exercised Mature Quarter Horse Geldings. Master’s Thesis, West Virginia University, Morgantown, WV, USA, 2011. [Google Scholar]
- Frank, N.; Geor, R.J.; Bailey, S.R.; Durham, A.E.; Johnson, P.J. ACVIM consensus statement on equine metabolic syndrome. J. Vet. Intern. Med. 2010, 24, 467–475. [Google Scholar] [CrossRef]
- Durham, A.E.; Frank, N.; McGowan, C.; Menzies-Gow, N.J.; Roelfsema, E.; Vervuert, I.; Feige, K.; Fey, K. ECEIM consensus statement on equine metabolic syndrome. J. Veter. Intern. Med. 2019, 33, 335–349. [Google Scholar] [CrossRef]
- Martin, L.; Johnson, P.J.; Amorim, J.R.; Honaker, A.R.; Donaldson, R.S.; DeClue, A.E. Investigation of the potential immunomodulatory effects of resveratrol on equine whole blood: An in vitro investigation. Res. Veter. Sci. 2016, 106, 97–99. [Google Scholar] [CrossRef]
- Siard, M.H.; McMurry, K.E.; Adams, A.A. Effects of polyphenols including curcuminoids, resveratrol, quercetin, pterostilbene, and hydroxypterostilbene on lymphocyte pro-inflammatory cytokine production of senior horses in vitro. Veter. Immunol. Immunopathol. 2016, 173, 50–59. [Google Scholar] [CrossRef]
- Mathew, L.M.; Woode, R.A.; Axiak-Bechtel, S.M.; Amorim, J.R.; DeClue, A.E. Resveratrol administration increases phagocytosis, decreases oxidative burst, and promotes pro-inflammatory cytokine production in healthy dogs. Veter. Immunol. Immunopathol. 2018, 203, 21–29. [Google Scholar] [CrossRef]
- Sheats, M. A Comparative Review of Equine SIRS, Sepsis, and Neutrophils. Front. Veter. Sci. 2019, 6, 69. [Google Scholar] [CrossRef]
- Salehi, B.; Mishra, A.P.; Nigam, M.; Sener, B.; Kilic, M.; Sharifi-Rad, J.; Fokou, P.V.T.; Martins, N.; Sharifi-Rad, J. Resveratrol: A Double-Edged Sword in Health Benefits. Biomedicines 2018, 6, 91. [Google Scholar] [CrossRef]
- Walle, T. Bioavailability of resveratrol. Ann. N. Y. Acad. Sci. 2011, 1215, 9–15. [Google Scholar] [CrossRef]
- Bode, L.M.; Bunzel, D.; Huch, M.; Cho, G.-S.; Ruhland, D.; Bunzel, M.; Bub, A.; Franz, C.M.; Kulling, S.E.; Kesse-Guyot, E.; et al. In vivo and in vitro metabolism of trans-resveratrol by human gut microbiota. Am. J. Clin. Nutr. 2013, 97, 295–309. [Google Scholar] [CrossRef]
- Chow, H.-H.; Garland, L.L.; Hsu, C.-H.; Vining, D.R.; Chew, W.M.; Miller, J.A.; Perloff, M.; Crowell, J.A.; Alberts, D.S. Resveratrol modulates drug- and carcinogen-metabolizing enzymes in a healthy volunteer study. Cancer Prev. Res. 2010, 3, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, A.C.; Johnson, P.J.; Lopes, M.A.; Perry, S.C.; Lanter, H.R. A Microbiological Map of the Healthy Equine Gastrointestinal Tract. PLoS ONE 2016, 11, e0166523. [Google Scholar] [CrossRef]
- Muzzio, M.; Huang, Z.; Hu, S.C.; Johnson, W.D.; McCormick, D.L.; Kapetanovic, I.M. Determination of resveratrol and its sulfate and glucuronide metabolites in plasma by LC-MS/MS and their pharmacokinetics in dogs. J. Pharm. Biomed. Anal. 2012, 59, 201–208. [Google Scholar] [CrossRef]
- Boocock, D.J.; Faust, G.E.; Patel, K.R.; Schinas, A.M.; Brown, V.A.; Ducharme, M.P.; Booth, T.D.; Crowell, J.A.; Perloff, M.; Gescher, A.J.; et al. Phase I Dose Escalation Pharmacokinetic Study in Healthy Volunteers of Resveratrol, a Potential Cancer Chemopreventive Agent. Cancer Epidemiol. Biomark. Prev. 2007, 16, 1246–1252. [Google Scholar] [CrossRef]
- Brown, V.A.; Patel, K.R.; Viskaduraki, M.; Crowell, J.A.; Perloff, M.; Booth, T.D.; Vasilinin, G.; Sen, A.; Schinas, A.M.; Piccirilli, G.; et al. Repeat dose study of the cancer chemopreventive agent resveratrol in healthy volunteers: Safety, pharmacokinetics, and effect on the insulin-like growth factor axis. Cancer Res. 2010, 70, 9003–9011. [Google Scholar] [CrossRef]
- Crowell, J.A.; Korytko, P.J.; Morrissey, R.L.; Booth, T.D.; Levine, B.S. Resveratrol-Associated Renal Toxicity. Toxicol. Sci. 2004, 82, 614–619. [Google Scholar] [CrossRef]
- Pearson, K.J.; Baur, J.A.; Lewis, K.N.; Peshkin, L.; Price, N.L.; Labinskyy, N.; Swindell, W.R.; Kamara, D.; Minor, R.K.; Perez, E.; et al. Resveratrol Delays Age-Related Deterioration and Mimics Transcriptional Aspects of Dietary Restriction without Extending Life Span. Cell Metab. 2008, 8, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Swirsley, N.; Spooner, H.S.; Hoffman, R.M. Supplement Use and Perceptions: A Study of US Horse Owners. J. Equine Veter. Sci. 2017, 59, 34–39. [Google Scholar] [CrossRef]
- Asensi, M.; Medina, I.; Ortega, A.; Carretero, J.; Bañó, C.; Obrador, E.; Estrela, J.M. Inhibition of cancer growth by resveratrol is related to its low bioavailability. Free. Radic. Boil. Med. 2002, 33, 387–398. [Google Scholar] [CrossRef]
- Kapetanovic, I.M.; Muzzio, M.; Huang, Z.; Thompson, T.N.; McCormick, D.L. Pharmacokinetics, oral bioavailability, and metabolic profile of resveratrol and its dimethylether analog, pterostilbene, in rats. Cancer Chemother Pharmacol. 2011, 68, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Masterson, G.R.; Hunter, J.M. Does anaesthesia have long-term consequences? Br. J. Anaesth. 1996, 77, 569–571. [Google Scholar] [CrossRef] [PubMed]
- Roth-Isigkeit, A.; Hasselbach, L.; Ocklitz, E.; Bruckner, S.; Ros, A.; Gehring, H.; Schmucker, P.; Rink, L.; Seyfarth, M. Inter-individual differences in cytokine release in patients undergoing cardiac surgery with cardiopulmonary bypass. Clin. Exp. Immunol. 2001, 125, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Schraut, W.; Wendelgass, P.; Calzada, J.; Frankenberger, M.; Ziegler-Heitbrock, H. Tnf gene expression in monocytes of low and high responder individuals. Cytokine 1997, 9, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Gurgul, A.; Jasielczuk, I.; Semik-Gurgul, E.; Pawlina-Tyszko, K.; Stefaniuk, M.; Szmatoła, T.; Polak, G.; Tomczyk-Wrona, I.; Bugno-Poniewierska, M. A genome-wide scan for diversifying selection signatures in selected horse breeds. PLoS ONE 2019, 14, e0210751. [Google Scholar] [CrossRef] [PubMed]
- Fredman, N.J.; Duque, G.; Duckham, R.L.; Green, D.; Brennan-Olsen, S.L. Associations between socioeconomic factors and proinflammatory cytokines in children, adolescents and young adults: A systematic review protocol. BMJ Open 2018, e019381. [Google Scholar] [CrossRef]
- Li, Y.; Oosting, M.; Smeekens, S.P.; Jaeger, M.; Aguirre-Gamboa, R.; Le, K.T.T.; Deelen, P.; Ricano-Ponce, I.; Schoffelen, T.; Jansen, A.F.M.; et al. A Functional Genomics Approach to Understand Variation in Cytokine Production in Humans. Cell 2016, 167, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Makki, K.; Froguel, P.; Wolowczuk, I. Adipose Tissue in Obesity-Related Inflammation and Insulin Resistance: Cells, Cytokines, and Chemokines. ISRN Inflamm. 2013, 2013, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Moldoveanu, A.I.; Shephard, R.J.; Shek, P.N. The cytokine response to physical activity and training. Sports Med. 2001, 31, 115–144. [Google Scholar] [CrossRef]
- Schirmer, M.; Kumar, V.; Netea, M.G.; Xavier, R.J. The causes and consequences of variation in human cytokine production in health. Curr. Opin. Immunol. 2018, 54, 50–58. [Google Scholar] [CrossRef]
- Ter Horst, R.; Jaeger, M.; Smeekens, S.P.; Oosting, M.; Swertz, M.A.; Li, Y.; Kumar, V.; Diavatopoulos, D.A.; Jansen, A.F.M.; Lemmers, H.; et al. Host and Environmental Factors Influencing Individual Human Cytokine Responses. Cell 2016, 167, 1111–1124. [Google Scholar] [CrossRef] [PubMed]
- Funk, R.A.; Stewart, A.J.; Wooldridge, A.A.; Kwessi, E.; Kemppainen, R.J.; Behrend, E.N.; Zhong, Q.; Johnson, A.K. Seasonal changes in plasma adrenocorticotropic hormone and alpha-melanocyte-stimulating hormone in response to thyrotropin-releasing hormone in normal, aged horses. J. Vet. Intern. Med. 2011, 25, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Borer-Weir, K.E.; Menzies-Gow, N.J.; Bailey, S.; Harris, P.A.; Elliott, J. Seasonal and annual influence on insulin and cortisol results from overnight dexamethasone suppression tests in normal ponies and ponies predisposed to laminitis. Equine Veter J. 2013, 45, 688–693. [Google Scholar] [CrossRef]
- Benbarek, H.; Deby-Dupont, G.; Caudron, I.; Grulke, S.; Deby, C.; Lamy, M.; Serteyn, D. Interactions between lipopolysaccharides and blood factors on the stimulation of equine polymorphonuclear neutrophils. Veter. Immunol. Immunopathol. 1998, 64, 313–322. [Google Scholar] [CrossRef]
- Damsgaard, C.T.; Lauritzen, L.; Calder, P.C.; Kjær, T.M.; Frøkiær, H. Whole-blood culture is a valid low-cost method to measure monocytic cytokines—A comparison of cytokine production in cultures of human whole-blood, mononuclear cells and monocytes. J. Immunol. Methods 2009, 340, 95–101. [Google Scholar] [CrossRef]
- De Groote, D.; Zangerle, P.F.; Gevaert, Y.; Fassotte, M.F.; Beguin, Y.; Noizat-Pirenne, F.; Pirenne, J.; Gathy, R.; Lopez, M.; Dehart, I.; et al. Direct stimulation of cytokines (IL-1 beta, TNF-alpha, IL-6, IL-2, IFN-gamma and GM-CSF) in whole blood. I. Comparison with isolated PBMC stimulation. Cytokine 1992, 4, 239–248. [Google Scholar] [CrossRef]
- DeClue, A.E.; Johnson, P.J.; Day, J.L.; Amorim, J.R.; Honaker, A.R. Pathogen associated molecular pattern motifs from Gram-positive and Gram-negative bacteria induce different inflammatory mediator profiles in equine blood. Vet. J. 2012, 192, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Baarsch, M.J.; Wannemuehler, M.J.; Molitor, T.W.; Murtaugh, M.P. Detection of tumor necrosis factor alpha from porcine alveolar macrophages using an L929 fibroblast bioassay. J. Immunol. Methods 1991, 140, 15–22. [Google Scholar] [CrossRef]
- DeClue, A.E.; Cohn, L.A.; Lechner, E.S.; Bryan, M.E.; Dodam, J. Effects of subanesthetic doses of ketamine on hemodynamic and immunologic variables in dogs with experimentally induced endotoxemia. Am. J. Veter. Res. 2008, 69, 228–232. [Google Scholar] [CrossRef]
- DeClue, A.E.; Williams, K.J.; Sharp, C.; Haak, C.; Lechner, E.; Reinero, C.R. Systemic response to low-dose endotoxin infusion in cats. Veter. Immunol. Immunopathol. 2009, 132, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Nafe, L.A.; DeClue, A.E.; Lee-Fowler, T.M.; Eberhardt, J.M.; Reinero, C.R. Evaluation of biomarkers in bronchoalveolar lavage fluid for discrimination between asthma and chronic bronchitis in cats. Am. J. Veter. Res. 2010, 71, 583–591. [Google Scholar] [CrossRef]
- Suagee, J.K.; Corl, B.A.; Crisman, M.V.; Pleasant, R.S.; Thatcher, C.D.; Geor, R.J. Relationships between Body Condition Score and Plasma Inflammatory Cytokines, Insulin, and Lipids in a Mixed Population of Light-Breed Horses. J. Vet. Intern. Med. 2013, 27, 157–163. [Google Scholar] [CrossRef]
- Mateus, L.; Lopes-Da-Costa, L.; Carvalho, H.; Serra, P.; Silva, J.R. Blood and intrauterine leukocyte profile and function in dairy cows that spontaneously recovered from postpartum endometritis. Reprod. Domest. Anim. 2002, 37, 176–180. [Google Scholar] [CrossRef]
- Da Costa, R.P.R.; Carvalho, H.; Agrícola, R.; Alpoim-Moreira, J.; Martins, C.; Dias, G.M.L.F. Peripheral blood neutrophil function and lymphocyte subpopulations in cycling mares. Reprod. Domest. Anim. 2003, 38, 464–469. [Google Scholar] [CrossRef]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, L.M.; Johnson, P.J.; Amorim, J.R.; DeClue, A.E. Effects of Orally Administered Resveratrol on TNF, IL-1β, Leukocyte Phagocytic Activity and Oxidative Burst Function in Horses: A Prospective, Randomized, Double-Blinded, Placebo-Controlled Study. Int. J. Mol. Sci. 2020, 21, 1453. https://doi.org/10.3390/ijms21041453
Martin LM, Johnson PJ, Amorim JR, DeClue AE. Effects of Orally Administered Resveratrol on TNF, IL-1β, Leukocyte Phagocytic Activity and Oxidative Burst Function in Horses: A Prospective, Randomized, Double-Blinded, Placebo-Controlled Study. International Journal of Molecular Sciences. 2020; 21(4):1453. https://doi.org/10.3390/ijms21041453
Chicago/Turabian StyleMartin, Lynn M., Philip J. Johnson, Juliana R. Amorim, and Amy E. DeClue. 2020. "Effects of Orally Administered Resveratrol on TNF, IL-1β, Leukocyte Phagocytic Activity and Oxidative Burst Function in Horses: A Prospective, Randomized, Double-Blinded, Placebo-Controlled Study" International Journal of Molecular Sciences 21, no. 4: 1453. https://doi.org/10.3390/ijms21041453
APA StyleMartin, L. M., Johnson, P. J., Amorim, J. R., & DeClue, A. E. (2020). Effects of Orally Administered Resveratrol on TNF, IL-1β, Leukocyte Phagocytic Activity and Oxidative Burst Function in Horses: A Prospective, Randomized, Double-Blinded, Placebo-Controlled Study. International Journal of Molecular Sciences, 21(4), 1453. https://doi.org/10.3390/ijms21041453