The Effect of TBB, as an Initiator, on the Biological Compatibility of PMMA/MMA Bone Cement

 , ,
, , 
Abstract
1. Introduction
2. Results
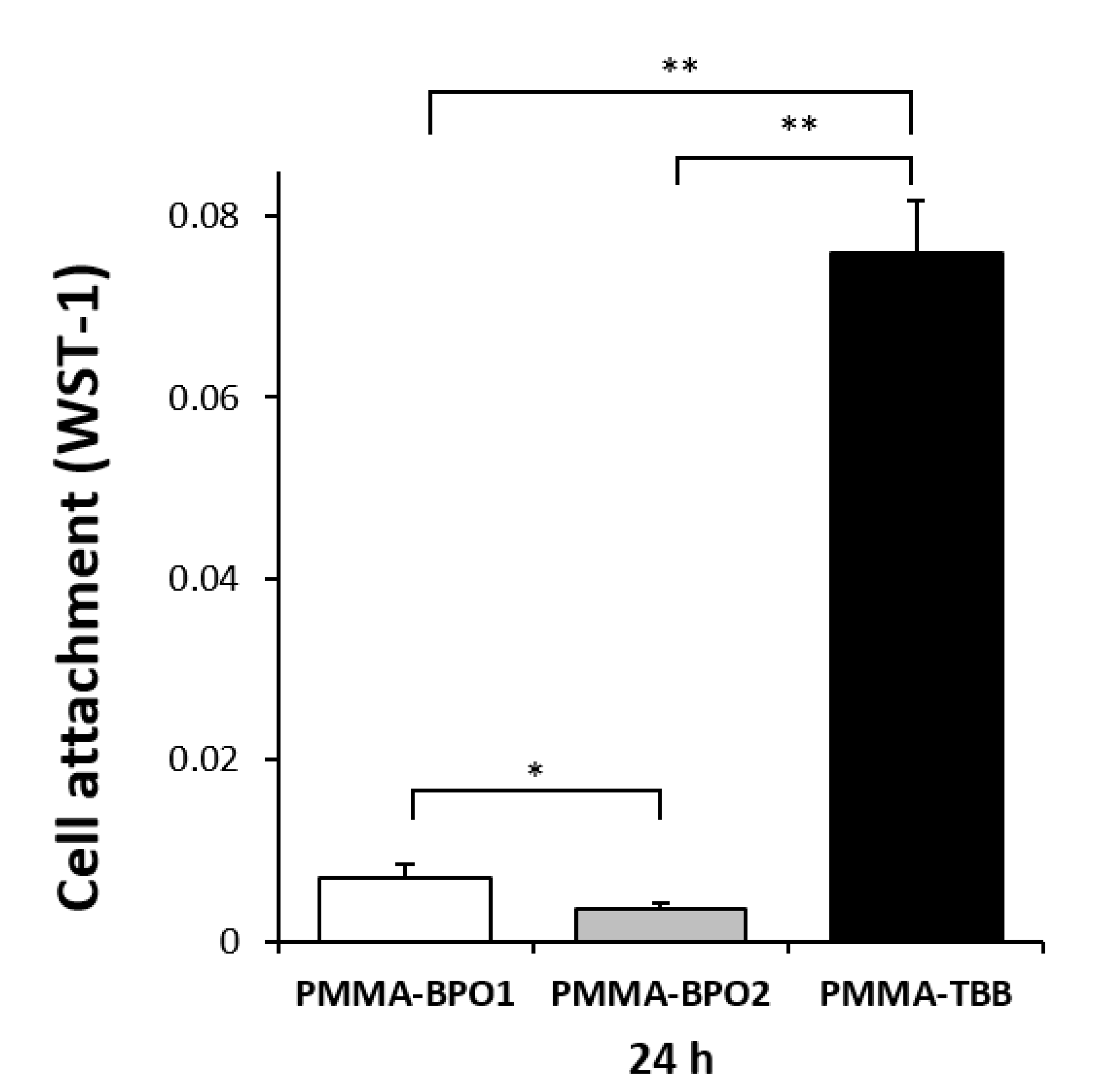
2.1. Improved Initial Attachment of Osteoblasts on PMMA-TBB
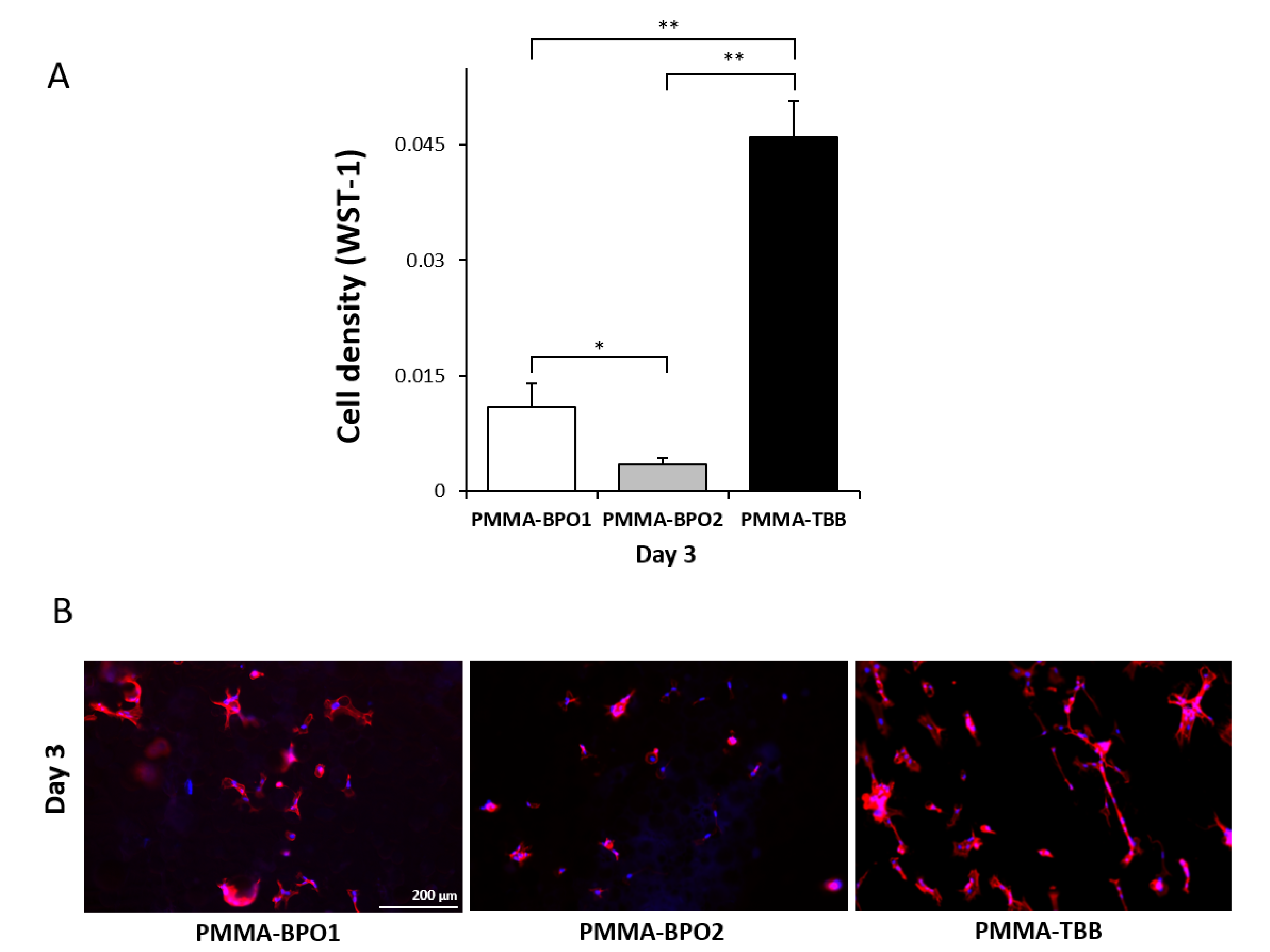
2.2. Improved Osteoblast Proliferation on PMMA-TBB
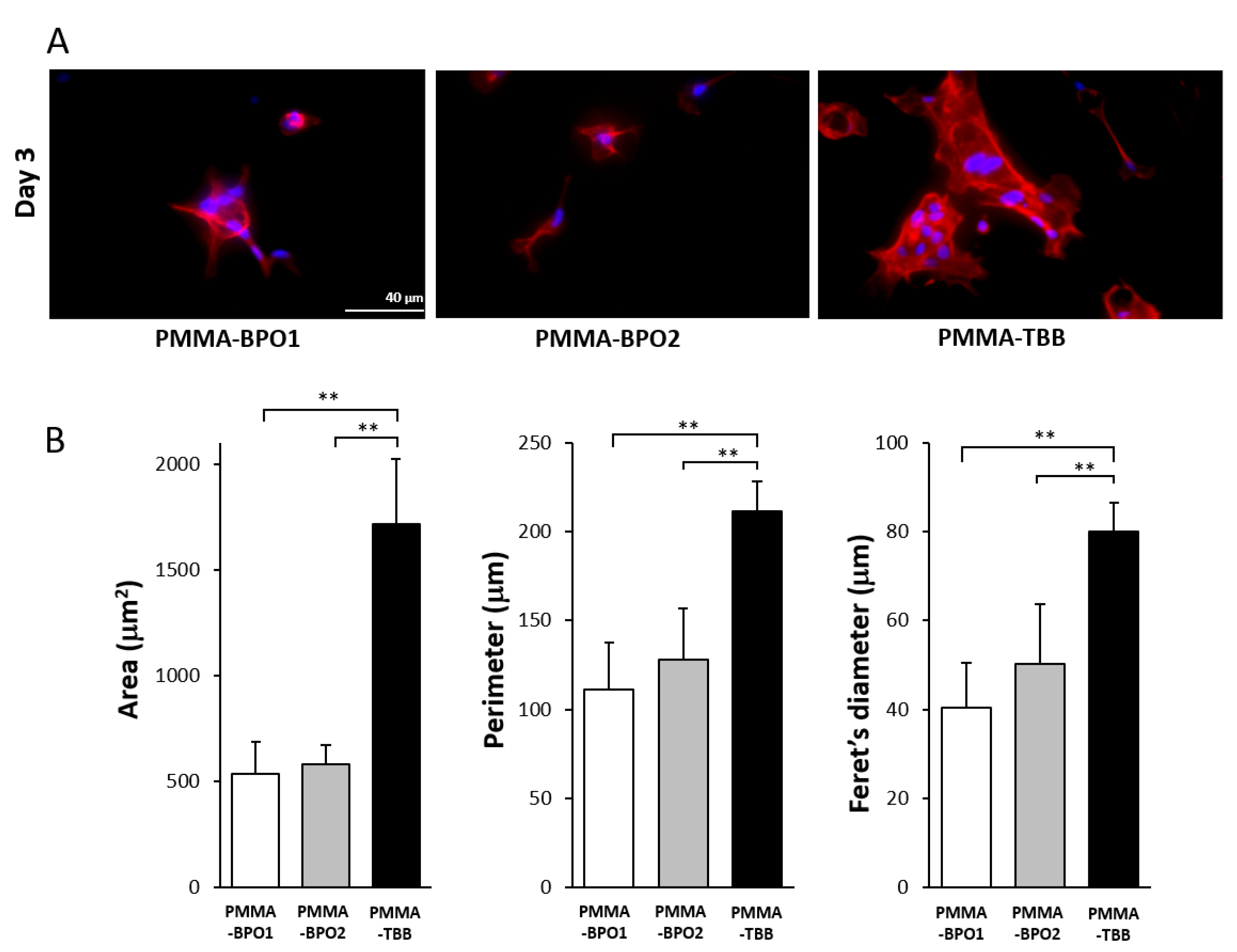
2.3. Enhanced Spreading Behavior of Osteoblasts on PMMA-TBB
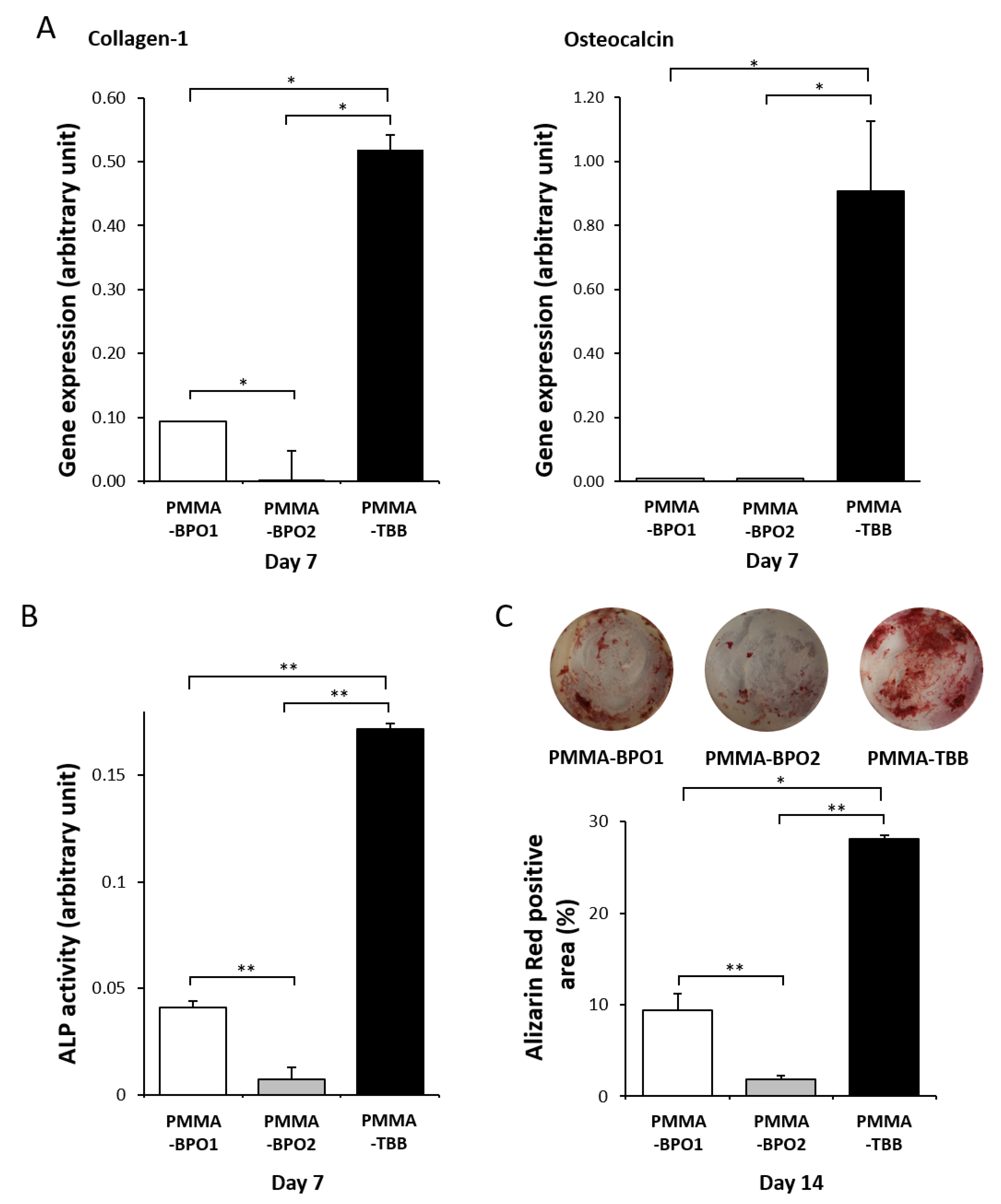
2.4. Improved Osteoblastic Functional Phenotype on PMMA-TBB
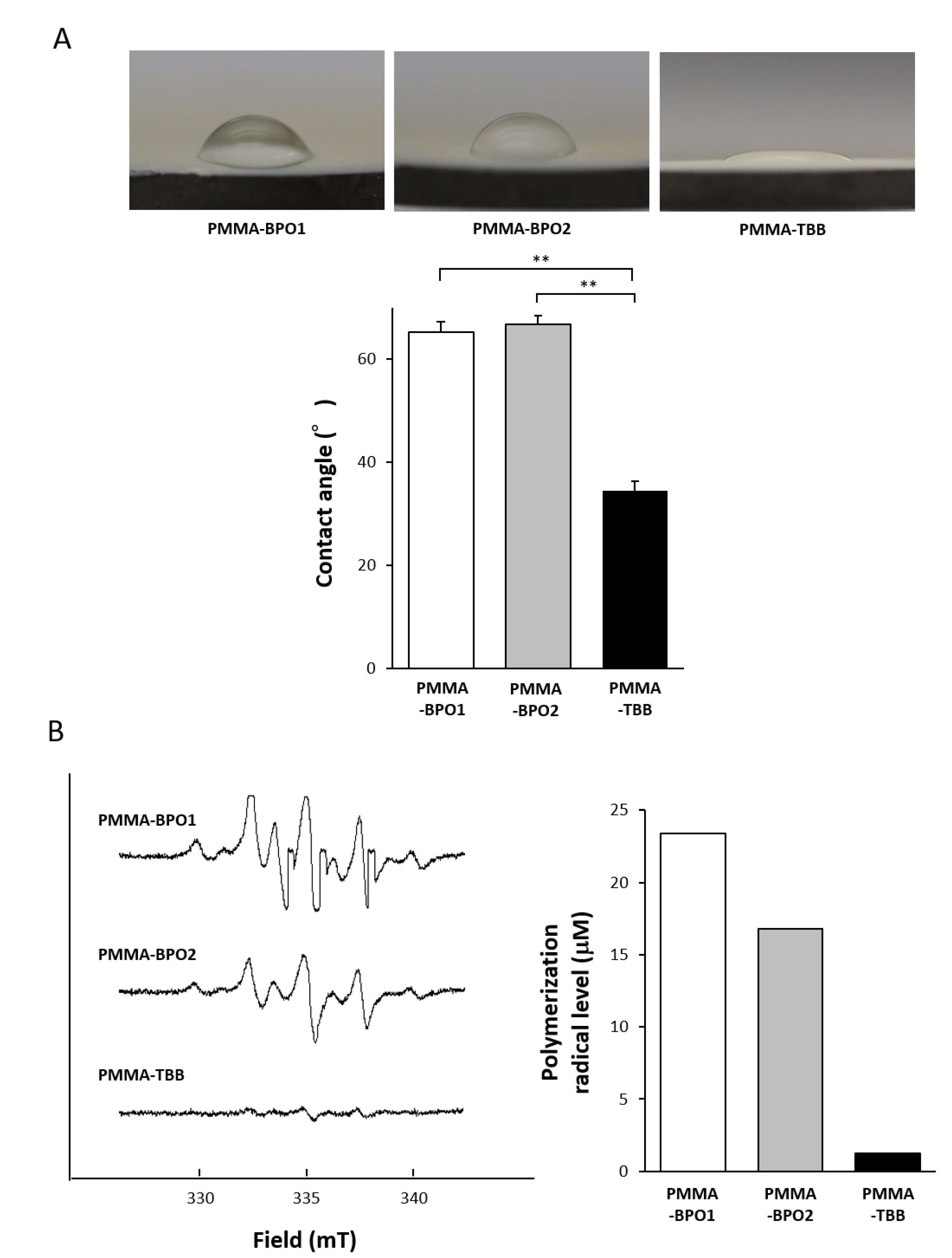
2.5. Physicochemical Properties of the PMMA-TBB Material
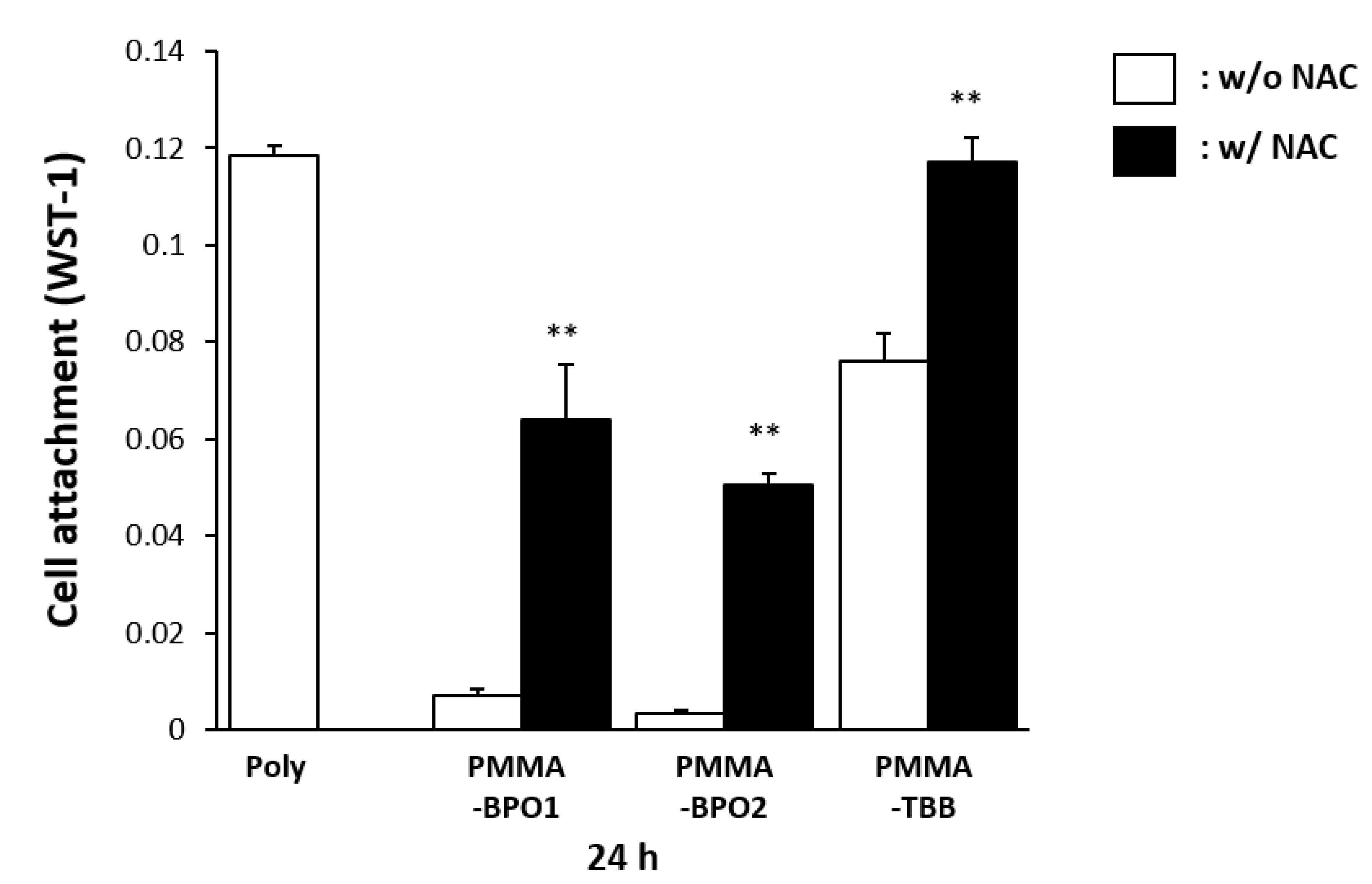
2.6. Mitigated Toxicity of Bone Cement Materials by Radical Scavenger
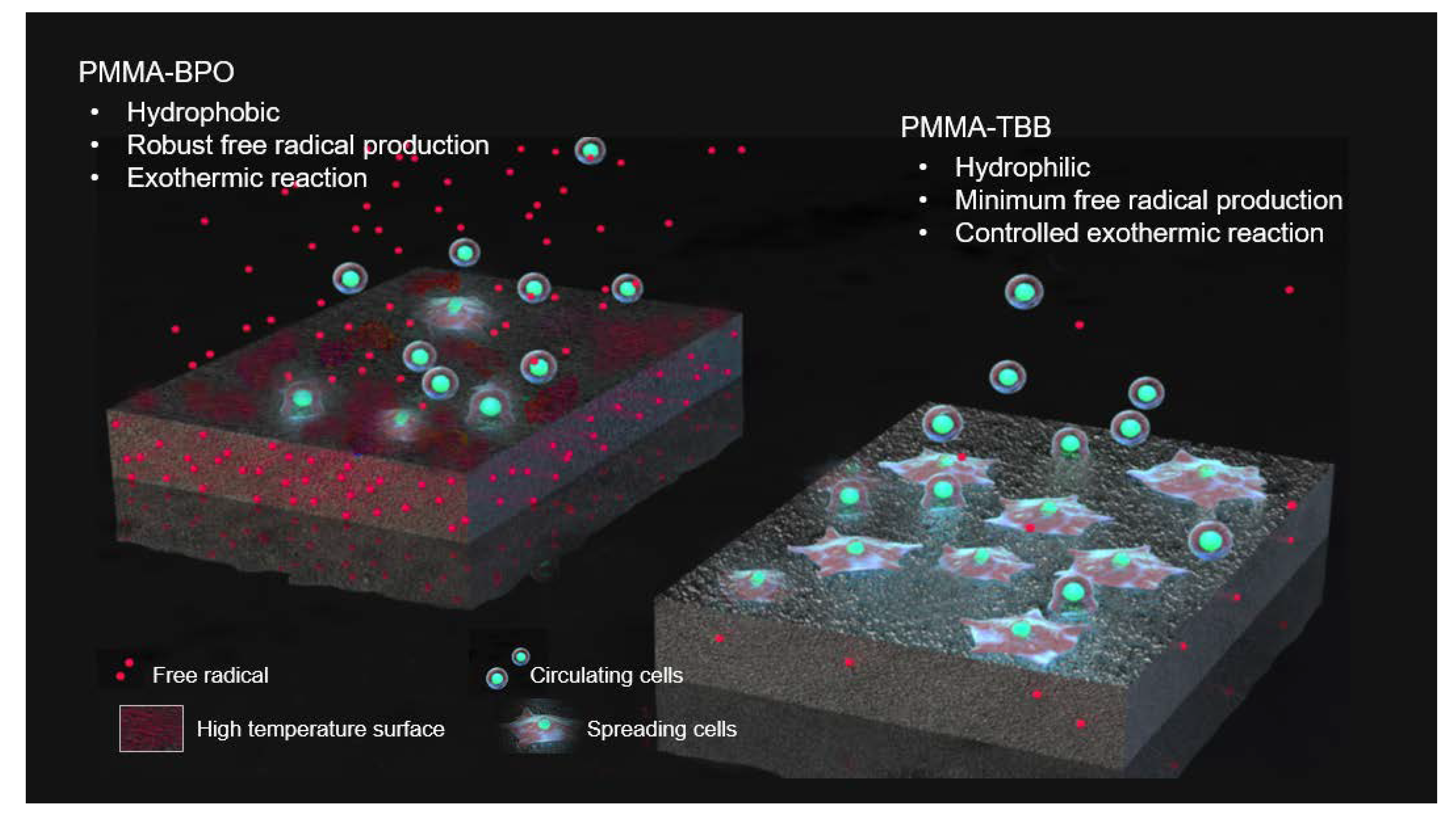
3. Discussion
4. Materials and Methods
4.1. Material Preparation and Characterization
4.2. Osteoblastic Cell Culture
4.3. Quantification of Cell Number
4.4. Morphology and Spreading Behavior of Osteoblasts
4.5. Alkaline Phosphatase (ALP) Activity
4.6. Real-Time Quantitative Polymerase Chain Reaction (qPCR)
4.7. Mineralizing Capability
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ALP | alkaline phosphatase |
| BCIS | bone cement implantation syndrome |
| BPO | benzoyl peroxide |
| cDNA | complementary DNA |
| DAPI | 4′,6-diamidino-2-phenylindole |
| ddH2O | double-distilled H2O |
| DmpT | N,N-dimethyl-p-toluidine |
| ELISA | enzyme-linked immunosorbent assay |
| ESR | electron spine resonance |
| MMA | methyl methacrylate |
| NAC | N-acetyl-cysteine |
| PCR | polymerase chain reaction |
| PMMA | polymethyl methacrylate |
| ROS | reactive oxygen species |
| TBB | tri-n-butyl borane |
| WST | water-soluble tetrazolium salts |
References
- Hoskins, T.; Shah, J.K.; Patel, J.; Mazzei, C.; Goyette, D.; Poletick, E.; Colella, T., II; Wittig, J. The cost-effectiveness of antibiotic-loaded bone cement versus plain bone cement following total and partial knee and hip arthroplasty. J. Orthop. 2020, 20, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Saleh, K.J.; El Othmani, M.M.; Tzeng, T.H.; Mihalko, W.M.; Chambers, M.C.; Grupp, T.M. Acrylic bone cement in total joint arthroplasty: A review. J. Orthop. Res. 2016, 34, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhu, C.; Cheng, T.; Peng, X.; Zhang, W.; Qin, H.; Zhang, X. A systematic review and meta-analysis of antibiotic-impregnated bone cement use in primary total hip or knee arthroplasty. PLoS ONE 2013, 8, e82745. [Google Scholar] [CrossRef] [PubMed]
- Magnan, B.; Bondi, M.; Maluta, T.; Samaila, E.; Schirru, L.; Dall’Oca, C. Acrylic bone cement: Current concept review. Musculoskelet. Surg. 2013, 97, 93–100. [Google Scholar] [CrossRef] [PubMed]
- DiMaio, F.R. The science of bone cement: A historical review. Orthopedics 2002, 25, 1399–1407. [Google Scholar] [PubMed]
- Shridhar, P.; Chen, Y.; Khalil, R.; Plakseychuk, A.; Cho, S.K.; Tillman, B.; Kumta, P.N.; Chun, Y. A Review of PMMA Bone Cement and Intra-Cardiac Embolism. Materials 2016, 9, 821. [Google Scholar] [CrossRef]
- Tsukimura, N.; Yamada, M.; Aita, H.; Hori, N.; Yoshino, F.; Chang-Il Lee, M.; Kimoto, K.; Jewett, A.; Ogawa, T. N-acetyl cysteine (NAC)-mediated detoxification and functionalization of poly(methyl methacrylate) bone cement. Biomaterials 2009, 30, 3378–3389. [Google Scholar] [CrossRef]
- Stathopoulos, I.P.; Andrianopoulos, N.; Paschaloglou, D.; Tsarouchas, I. Revision total knee arthroplasty due to bone cement and metal hypersensitivity. Arch. Orthop. Trauma Surg. 2017, 137, 267–271. [Google Scholar] [CrossRef]
- Lee, A.J. Revision of total hips using bone cement: Improvement of materials and operative technique. Acta Orthop. Belg. 1986, 52, 263–270. [Google Scholar]
- Dohmae, Y.; Bechtold, J.E.; Sherman, R.E.; Puno, R.M.; Gustilo, R.B. Reduction in cement-bone interface shear strength between primary and revision arthroplasty. Clin. Orthop. Relat. Res. 1988, 236, 214–220. [Google Scholar] [CrossRef]
- Vaishya, R.; Chauhan, M.; Vaish, A. Bone cement. J. Clin. Orthop. Trauma 2013, 4, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, A.J.; Thomson, H.E.; Harper, N.J.; Kenny, N.W. Bone cement implantation syndrome. Br. J. Anaesth. 2009, 102, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Johnston, R.C. Acrylic bone cement: Clinical development and current status in North America. Orthop. Clin. N. Am. 2005, 36, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Johanson, N.A.; Bullough, P.G.; Wilson, P.D., Jr.; Salvati, E.A.; Ranawat, C.S. The microscopic anatomy of the bone-cement interface in failed total hip arthroplasties. Clin. Orthop. Relat. Res. 1987, 218, 123–135. [Google Scholar] [CrossRef]
- Ciapetti, G.; Granchi, D.; Savarino, L.; Cenni, E.; Magrini, E.; Baldini, N.; Giunti, A. In vitro testing of the potential for orthopedic bone cements to cause apoptosis of osteoblast-like cells. Biomaterials 2002, 23, 617–627. [Google Scholar] [CrossRef]
- Ciapetti, G.; Granchi, D.; Cenni, E.; Savarino, L.; Cavedagna, D.; Pizzoferrato, A. Cytotoxic effect of bone cements in HL-60 cells: Distinction between apoptosis and necrosis. J. Biomed. Mater. Res. 2000, 52, 338–345. [Google Scholar] [CrossRef]
- Aita, H.; Tsukimura, N.; Yamada, M.; Hori, N.; Kubo, K.; Sato, N.; Maeda, H.; Kimoto, K.; Ogawa, T. N-acetyl cysteine prevents polymethyl methacrylate bone cement extract-induced cell death and functional suppression of rat primary osteoblasts. J. Biomed. Mater. Res. A 2010, 92, 285–296. [Google Scholar] [CrossRef]
- Bayliss, L.E.; Culliford, D.; Monk, A.P.; Glyn-Jones, S.; Prieto-Alhambra, D.; Judge, A.; Cooper, C.; Carr, A.J.; Arden, N.K.; Beard, D.J.; et al. The effect of patient age at intervention on risk of implant revision after total replacement of the hip or knee: A population-based cohort study. Lancet 2017, 389, 1424–1430. [Google Scholar] [CrossRef]
- Geraci, G.; Lo Iacono, G.; Lo Nigro, C.; Cannizzaro, F.; Cajozzo, M.; Modica, G. Asymptomatic bone cement pulmonary embolism after vertebroplasty: Case report and literature review. Case Rep. Surg. 2013, 2013, 591432. [Google Scholar] [CrossRef]
- Olsen, F.; Kotyra, M.; Houltz, E.; Ricksten, S.E. Bone cement implantation syndrome in cemented hemiarthroplasty for femoral neck fracture: Incidence, risk factors, and effect on outcome. Br. J. Anaesth. 2014, 113, 800–806. [Google Scholar] [CrossRef]
- Hines, C.B. Understanding Bone Cement Implantation Syndrome. AANA J. 2018, 86, 433–441. [Google Scholar] [PubMed]
- Kojima, N.; Yamada, M.; Paranjpe, A.; Tsukimura, N.; Kubo, K.; Jewett, A.; Ogawa, T. Restored viability and function of dental pulp cells on poly-methylmethacrylate (PMMA)-based dental resin supplemented with N-acetyl cysteine (NAC). Dent. Mater. 2008, 24, 1686–1693. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Kojima, N.; Paranjpe, A.; Att, W.; Aita, H.; Jewett, A.; Ogawa, T. N-acetyl cysteine (NAC)-assisted detoxification of PMMA resin. J. Dent. Res. 2008, 87, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Georgieva, E.; Ivanova, D.; Zhelev, Z.; Bakalova, R.; Gulubova, M.; Aoki, I. Mitochondrial Dysfunction and Redox Imbalance as a Diagnostic Marker of “Free Radical Diseases”. Anticancer Res. 2017, 37, 5373–5381. [Google Scholar] [PubMed]
- Choppadandi, M.; More, N.; Kapusetti, G. Detoxification of poly(methyl methacrylate) bone cement by natural antioxidant intervention. J. Biomed. Mater. Res. A 2019, 107, 2835–2847. [Google Scholar] [CrossRef]
- Granchi, D.; Cenni, E.; Savarino, L.; Ciapetti, G.; Forbicini, G.; Vancini, M.; Maini, C.; Baldini, N.; Giunti, A. Bone cement extracts modulate the osteoprotegerin/osteoprotegerin-ligand expression in MG63 osteoblast-like cells. Biomaterials 2002, 23, 2359–2365. [Google Scholar] [CrossRef]
- Sugita, Y.; Okubo, T.; Saita, M.; Ishijima, M.; Torii, Y.; Tanaka, M.; Iwasaki, C.; Sekiya, T.; Tabuchi, M.; Mohammadzadeh Rezaei, N.; et al. Novel Osteogenic Behaviors around Hydrophilic and Radical-Free 4-META/MMA-TBB: Implications of an Osseointegrating Bone Cement. Int. J. Mol. Sci. 2020, 21, 2405. [Google Scholar] [CrossRef]
- Dulany, K.; Hepburn, K.; Goins, A.; Allen, J.B. In vitro and in vivo biocompatibility assessment of free radical scavenging nanocomposite scaffolds for bone tissue regeneration. J. Biomed. Mater. Res. A 2020, 108, 301–315. [Google Scholar] [CrossRef]
- Kennedy, J.G.; O’Grady, P.; McCarthy, D.R.; Johnson, S.J.; Hynes, D.; Walsh, M.; McManus, F.M.; Salih, E.; Gouverneur, M.; Fitzpatrick, J. An investigation into the role of oxygen free radical scavengers in preventing polymethylmethacrylate-induced necrosis in an osteoblast cell culture. Orthopedics 2000, 23, 481–485. [Google Scholar]
- Cenni, E.; Granchi, D.; Ciapetti, G.; Savarino, L.; Corradini, A.; Vancini, M.; Giunti, A. Gene expression of bone-associated cytokines in MG63 osteoblast-like cells incubated with acrylic bone cement extracts in minimum essential medium. J. Biomater. Sci. Polym. Ed. 2002, 13, 1283–1294. [Google Scholar] [CrossRef]
- Anselmetti, G.C.; Manca, A.; Kanika, K.; Murphy, K.; Eminefendic, H.; Masala, S.; Regge, D. Temperature measurement during polymerization of bone cement in percutaneous vertebroplasty: An in vivo study in humans. Cardiovasc. Intervent. Radiol. 2009, 32, 491–498. [Google Scholar] [CrossRef]
- Lai, P.L.; Chen, L.H.; Chen, W.J.; Chu, I.M. Chemical and physical properties of bone cement for vertebroplasty. Biomed. J. 2013, 36, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Harving, S.; Soballe, K.; Bunger, C. A method for bone-cement interface thermometry. An in vitro comparison between low temperature curing cement Palavit, and Surgical Simplex P. Acta Orthop. Scand. 1991, 62, 546–548. [Google Scholar] [CrossRef] [PubMed]
- Belkoff, S.M.; Molloy, S. Temperature measurement during polymerization of polymethylmethacrylate cement used for vertebroplasty. Spine 2003, 28, 1555–1559. [Google Scholar] [CrossRef] [PubMed]
- Urrutia, J.; Bono, C.M.; Mery, P.; Rojas, C. Early histologic changes following polymethylmethacrylate injection (vertebroplasty) in rabbit lumbar vertebrae. Spine 2008, 33, 877–882. [Google Scholar] [CrossRef]
- Mjoberg, B.; Pettersson, H.; Rosenqvist, R.; Rydholm, A. Bone cement, thermal injury and the radiolucent zone. Acta Orthop. Scand. 1984, 55, 597–600. [Google Scholar] [CrossRef]
- Tavakoli, M.; Bakhtiari, S.S.E.; Karbasi, S. Incorporation of chitosan/graphene oxide nanocomposite in to the PMMA bone cement: Physical, mechanical and biological evaluation. Int. J. Biol. Macromol. 2020, 149, 783–793. [Google Scholar] [CrossRef]
- Yamada, M.; Ogawa, T. Chemodynamics underlying N-acetyl cysteine-mediated bone cement monomer detoxification. Acta Biomater. 2009, 5, 2963–2973. [Google Scholar] [CrossRef]
- Hasenwinkel, J.M.; Lautenschlager, E.P.; Wixson, R.L.; Gilbert, J.L. Effect of initiation chemistry on the fracture toughness, fatigue strength, and residual monomer content of a novel high-viscosity, two-solution acrylic bone cement. J. Biomed. Mater. Res. 2002, 59, 411–421. [Google Scholar] [CrossRef]
- Tanzi, M.C.; Sket, I.; Gatti, A.M.; Monari, E. Physical characterization of acrylic bone cement cured with new accelerator systems. Clin. Mater. 1991, 8, 131–136. [Google Scholar] [CrossRef]
- Madigan, S.; Towler, M.R.; Lewis, G. Optimisation of the composition of an acrylic bone cement: Application to relative amounts of the initiator and the activator/co-initiator in Surgical Simplex P. J. Mater. Sci. Mater. Med. 2006, 17, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Milner, R. The development of theoretical relationships between some handling parameters (setting time and setting temperature), composition (relative amounts of initiator and activator) and ambient temperature for acrylic bone cement. J. Biomed. Mater. Res. B Appl. Biomater. 2004, 68, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Brauer, G.M.; Steinberger, D.R.; Stansbury, J.W. Dependence of curing time, peak temperature, and mechanical properties on the composition of bone cement. J. Biomed. Mater. Res. 1986, 20, 839–852. [Google Scholar] [CrossRef] [PubMed]
- Kalra, A.; Sharma, A.; Palaniswamy, C.; El-Oshar, S.; Desai, P.; Yazbeck, M.; Zanotti-Cavazzoni, S.L. Diagnosis and management of bone cement implantation syndrome: Case report and brief review. Am. J. Ther. 2013, 20, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Olsen, F.; Hard Af Segerstad, M.; Nellgard, B.; Houltz, E.; Ricksten, S.E. The role of bone cement for the development of intraoperative hypotension and hypoxia and its impact on mortality in hemiarthroplasty for femoral neck fractures. Acta Orthop. 2020. [Google Scholar] [CrossRef]
- Zhang, S.; Wang, G.J.; Wang, Q.; Yang, J.; Xu, S.; Yang, C.H. A mysterious risk factor for bone cement leakage into the spinal canal through the Batson vein during percutaneous kyphoplasty: A case control study. BMC Musculoskelet. Disord. 2019, 20, 423. [Google Scholar] [CrossRef]
- Stea, S.; Granchi, D.; Zolezzi, C.; Ciapetti, G.; Visentin, M.; Cavedagna, D.; Pizzoferrato, A. High-performance liquid chromatography assay of N,N-dimethyl-p-toluidine released from bone cements: Evidence for toxicity. Biomaterials 1997, 18, 243–246. [Google Scholar] [CrossRef]
- Hirabayashi, C.; Imai, Y. Studies on MMA-tBB resin. I. Comparison of TBB and other initiators in the polymerization of PMMA/MMA resin. Dent. Mater. J. 2002, 21, 314–321. [Google Scholar] [CrossRef]
- Hirabayashi, C. Studies on MMA-TBB resin II. The effect of dual use of TBB and other initiators on polymerization of PMMA/MMA resin. Dent. Mater. J. 2003, 22, 48–55. [Google Scholar] [CrossRef]
- Davy, K.W.; Braden, M. Residual monomer in acrylic polymers. Biomaterials 1991, 12, 540–544. [Google Scholar] [CrossRef]
- Lewis, G.; Xu, J.; Madigan, S.; Towler, M.R. Influence of strontia on various properties of surgical simplex P acrylic bone cement and experimental variants. Acta Biomater. 2007, 3, 970–979. [Google Scholar] [CrossRef] [PubMed]
- Taningher, M.; Pasquini, R.; Bonatti, S. Genotoxicity analysis of N,N-dimethylaniline and N,N-dimethyl-p-toluidine. Environ. Mol. Mutagen. 1993, 21, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Inami, C.; Shimizu, H.; Suzuki, S.; Haraguchi, N.; Itsuno, S. Study on the performance of methyl methacrylate polymerization: Comparison of partially oxidized tri-n-butylborane and benzoyl peroxide with aromatic tertiary amines. Dent. Mater. J. 2019, 38, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, S.; Kadoma, Y. Tri-n-Butylborane/WaterComplex-Mediated Copolymerization of Methyl Methacrylate with Proteinaceous Materials and Proteins: A Review. Polymers 2010, 2, 575–595. [Google Scholar] [CrossRef]
- Eriksson, R.A.; Albrektsson, T.; Magnusson, B. Assessment of bone viability after heat trauma. A histological, histochemical and vital microscopic study in the rabbit. Scand. J. Plast. Reconstr. Surg. 1984, 18, 261–268. [Google Scholar] [CrossRef]
- Eriksson, A.; Albrektsson, T.; Grane, B.; McQueen, D. Thermal injury to bone. A vital-microscopic description of heat effects. Int. J. Oral Surg. 1982, 11, 115–121. [Google Scholar] [CrossRef]
- Field, S.B.; Morris, C.C. The relationship between heating time and temperature: Its relevance to clinical hyperthermia. Radiother. Oncol. 1983, 1, 179–186. [Google Scholar] [CrossRef]
- Dolan, E.B.; Haugh, M.G.; Voisin, M.C.; Tallon, D.; McNamara, L.M. Thermally induced osteocyte damage initiates a remodelling signaling cascade. PLoS ONE 2015, 10, e0119652. [Google Scholar] [CrossRef]
- Birkeland, O.; Espehaug, B.; Havelin, L.I.; Furnes, O. Bone cement product and failure in total knee arthroplasty. Acta Orthop. 2017, 88, 75–81. [Google Scholar] [CrossRef]
- Aita, H.; Att, W.; Ueno, T.; Yamada, M.; Hori, N.; Iwasa, F.; Tsukimura, N.; Ogawa, T. Ultraviolet light-mediated photofunctionalization of titanium to promote human mesenchymal stem cell migration, attachment, proliferation and differentiation. Acta Biomater. 2009, 5, 3247–3257. [Google Scholar] [CrossRef]
- Att, W.; Hori, N.; Takeuchi, M.; Ouyang, J.; Yang, Y.; Anpo, M.; Ogawa, T. Time-dependent degradation of titanium osteoconductivity: An implication of biological aging of implant materials. Biomaterials 2009, 30, 5352–5363. [Google Scholar] [CrossRef] [PubMed]
- Tsukimura, N.; Yamada, M.; Iwasa, F.; Minamikawa, H.; Att, W.; Ueno, T.; Saruwatari, L.; Aita, H.; Chiou, W.A.; Ogawa, T. Synergistic effects of UV photofunctionalization and micro-nano hybrid topography on the biological properties of titanium. Biomaterials 2011, 32, 4358–4368. [Google Scholar] [CrossRef] [PubMed]
- Taniyama, T.; Saruta, J.; Mohammadzadeh Rezaei, N.; Nakhaei, K.; Ghassemi, A.; Hirota, M.; Okubo, T.; Ikeda, T.; Sugita, Y.; Hasegawa, M.; et al. UV-Photofunctionalization of Titanium Promotes Mechanical Anchorage in A Rat Osteoporosis Model. Int. J. Mol. Sci. 2020, 21, 1235. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, H.; Hirota, M.; Iwai, T.; Hamajima, K.; Ozawa, R.; Hayashi, Y.; Yajima, Y.; Iida, M.; Koizumi, T.; Kioi, M.; et al. Computational Fluid Simulation of Fibrinogen around Dental Implant Surfaces. Int. J. Mol. Sci. 2020, 21, 660. [Google Scholar] [CrossRef]
- Anagnostakos, K. Therapeutic Use of Antibiotic-loaded Bone Cement in the Treatment of Hip and Knee Joint Infections. J. Bone Jt. Infect. 2017, 2, 29–37. [Google Scholar] [CrossRef]
- Bistolfi, A.; Massazza, G.; Verne, E.; Masse, A.; Deledda, D.; Ferraris, S.; Miola, M.; Galetto, F.; Crova, M. Antibiotic-loaded cement in orthopedic surgery: A review. ISRN Orthop. 2011, 2011, 290851. [Google Scholar] [CrossRef]
- Jameson, S.S.; Asaad, A.; Diament, M.; Kasim, A.; Bigirumurame, T.; Baker, P.; Mason, J.; Partington, P.; Reed, M. Antibiotic-loaded bone cement is associated with a lower risk of revision following primary cemented total knee arthroplasty: An analysis of 731,214 cases using National Joint Registry data. Bone Joint J. 2019, 101-B, 1331–1347. [Google Scholar] [CrossRef]
- Zhang, X.; Kang, T.; Liang, P.; Tang, Y.; Quan, C. Biological Activity of an Injectable Biphasic Calcium Phosphate/PMMA Bone Cement for Induced Osteogensis in Rabbit Model. Macromol. Biosci. 2018, 18, 1700331. [Google Scholar] [CrossRef]
- Phakatkar, A.H.; Shirdar, M.R.; Qi, M.L.; Taheri, M.M.; Narayanan, S.; Foroozan, T.; Sharifi-Asl, S.; Huang, Z.; Agrawal, M.; Lu, Y.P.; et al. Novel PMMA bone cement nanocomposites containing magnesium phosphate nanosheets and hydroxyapatite nanofibers. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 109, 110497. [Google Scholar] [CrossRef]
- Lam, W.M.; Pan, H.B.; Fong, M.K.; Cheung, W.S.; Wong, K.L.; Li, Z.Y.; Luk, K.D.; Chan, W.K.; Wong, C.T.; Yang, C.; et al. In Vitro characterization of low modulus linoleic acid coated strontium-substituted hydroxyapatite containing PMMA bone cement. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 96, 76–83. [Google Scholar] [CrossRef]
- Chu, K.T.; Oshida, Y.; Hancock, E.B.; Kowolik, M.J.; Barco, T.; Zunt, S.L. Hydroxyapatite/PMMA composites as bone cements. Biomed. Mater. Eng. 2004, 14, 87–105. [Google Scholar] [PubMed]
- Minamikawa, H.; Yamada, M.; Iwasa, F.; Ueno, T.; Deyama, Y.; Suzuki, K.; Yawaka, Y.; Ogawa, T. Amino acid derivative-mediated detoxification and functionalization of dual cure dental restorative material for dental pulp cell mineralization. Biomaterials 2010, 31, 7213–7225. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Miura, K.; Liu, X.; Zweier, J.L. Biphasic regulation of leukocyte superoxide generation by nitric oxide and peroxynitrite. J. Biol. Chem. 2000, 275, 38965–38972. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, F.; Shoji, H.; Lee, M.C. Vascular effects of singlet oxygen (1O2) generated by photo-excitation on adrenergic neurotransmission in isolated rabbit mesenteric vein. Redox Rep. 2002, 7, 266–270. [Google Scholar] [CrossRef]
- Lee, M.C.; Yoshino, F.; Shoji, H.; Takahashi, S.; Todoki, K.; Shimada, S.; Kuse-Barouch, K. Characterization by electron spin resonance spectroscopy of reactive oxygen species generated by titanium dioxide and hydrogen peroxide. J. Dent. Res. 2005, 84, 178–182. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bone Cement Type | Ingredients |
|---|---|
| PMMA-BPO1(Endurance MV, DePuy Orthopaedics) | Powder: Polymethyl methacrylate (PMMA) (67.05%) Methyl methacrylate/styrene copolymer (21.10%) Benzoyl peroxide (BPO) initiator (1.85%) Barium sulphate (10.00%) Liquid: Methyl methacrylate (MMA) (98.00%) N,N-dimethyl-p-toluidine (DmpT)(<2.00%) Hydroquinone (HQ) (75 ppm) |
| PMMA-BPO2(Surgical Simplex P, Stryker) | Powder: Polymethyl methacrylate (PMMA) (15.00%) Methyl methacrylate-styrene copolymer (73.70%) Benzoyl Peroxide (BPO) initiator (1.30%) Barium sulfate (10.00%) Liquid: Methyl methacrylate (MMA) (97.40%) N,N-dimethyl p-toluidine (DmpT) (2.60%) Hydroquinone (HQ) (75 ppm) |
| PMMA-TBB(Experimental) | Powder: Polymethyl methacrylate (PMMA) (90.00%) Barium sulfate (10.00%) Liquid: Methyl methacrylate (MMA) (91.00%) tri-n-butyl borane (TBB) initiator (9.00%) Hydroquinone (HQ) (50 ppm) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamajima, K.; Ozawa, R.; Saruta, J.; Saita, M.; Kitajima, H.; Taleghani, S.R.; Usami, D.; Goharian, D.; Uno, M.; Miyazawa, K.; et al. The Effect of TBB, as an Initiator, on the Biological Compatibility of PMMA/MMA Bone Cement. Int. J. Mol. Sci. 2020, 21, 4016. https://doi.org/10.3390/ijms21114016
Hamajima K, Ozawa R, Saruta J, Saita M, Kitajima H, Taleghani SR, Usami D, Goharian D, Uno M, Miyazawa K, et al. The Effect of TBB, as an Initiator, on the Biological Compatibility of PMMA/MMA Bone Cement. International Journal of Molecular Sciences. 2020; 21(11):4016. https://doi.org/10.3390/ijms21114016
Chicago/Turabian StyleHamajima, Kosuke, Ryotaro Ozawa, Juri Saruta, Makiko Saita, Hiroaki Kitajima, Samira Rahim Taleghani, Dan Usami, Donya Goharian, Mitsunori Uno, Ken Miyazawa, and et al. 2020. "The Effect of TBB, as an Initiator, on the Biological Compatibility of PMMA/MMA Bone Cement" International Journal of Molecular Sciences 21, no. 11: 4016. https://doi.org/10.3390/ijms21114016
APA StyleHamajima, K., Ozawa, R., Saruta, J., Saita, M., Kitajima, H., Taleghani, S. R., Usami, D., Goharian, D., Uno, M., Miyazawa, K., Goto, S., Tsukinoki, K., & Ogawa, T. (2020). The Effect of TBB, as an Initiator, on the Biological Compatibility of PMMA/MMA Bone Cement. International Journal of Molecular Sciences, 21(11), 4016. https://doi.org/10.3390/ijms21114016