
Association between Coffee Consumption/Physical Exercise and Gastric, Hepatic, Colon, Breast, Uterine Cervix, Lung, Thyroid, Prostate, and Bladder Cancer


Abstract
:1. Introduction
2. Materials and Methods
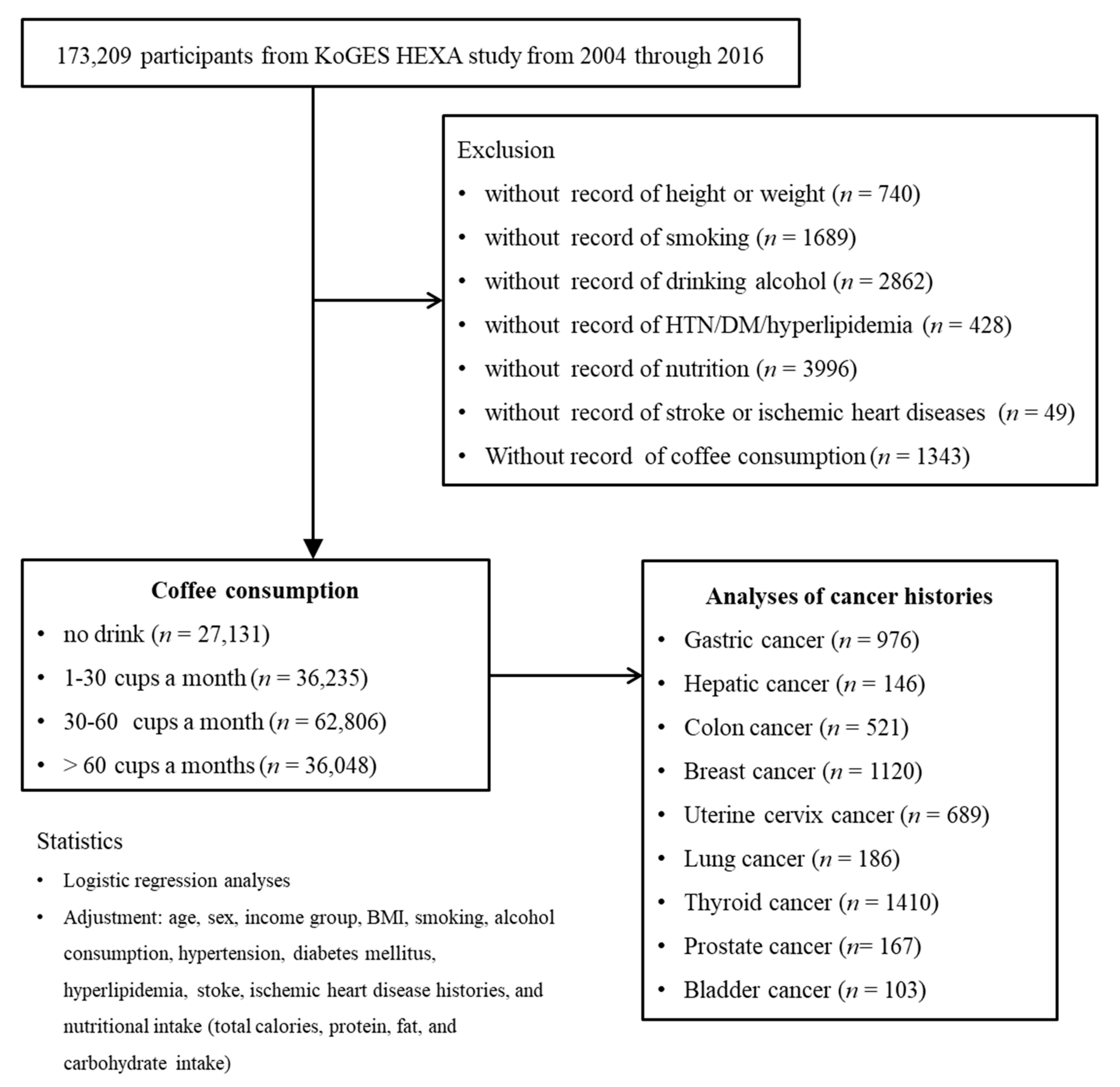
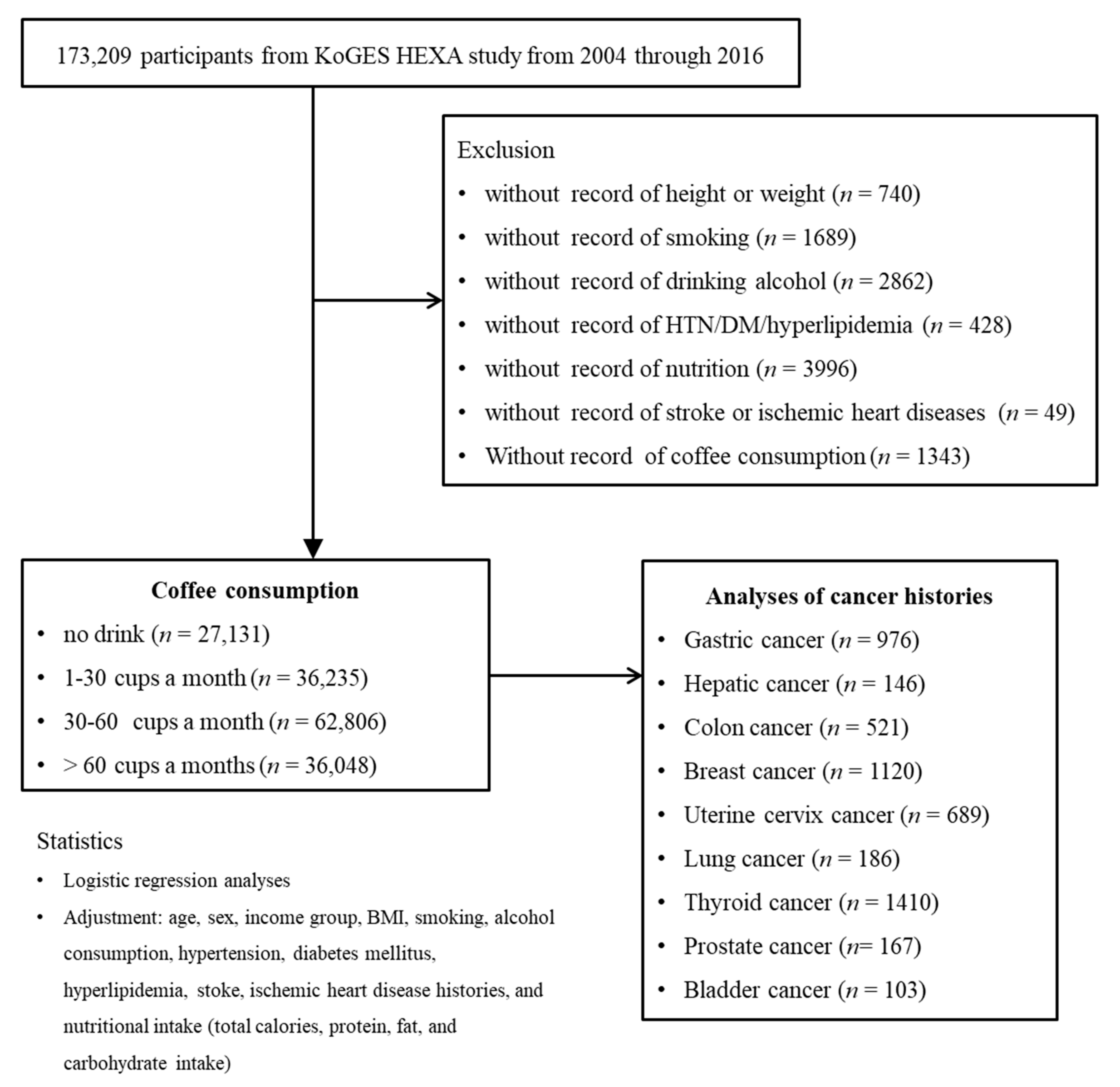
2.1. Study Population and Data Collection
2.2. Selection of Participants
2.3. Survey
2.3.1. Exposure
2.3.2. Outcome
2.3.3. Covariates
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bułdak, R.J.; Hejmo, T.; Osowski, M.; Bułdak, L.; Kukla, M.; Polaniak, R.; Birkner, E. The Impact of Coffee and Its Selected Bioactive Compounds on the Development and Progression of Colorectal Cancer In Vivo and In Vitro. Molecules 2018, 23, 3309. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Lee, J.E.; Loftfield, E.; Shu, X.-O.; Abe, S.K.; Rahman, S.; Saito, E.; Islam, R.; Tsugane, S.; Sawada, N.; et al. Coffee and tea consumption and mortality from all causes, cardiovascular disease and cancer: A pooled analysis of prospective studies from the Asia Cohort Consortium. Int. J. Epidemiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hayakawa, S.; Ohishi, T.; Miyoshi, N.; Oishi, Y.; Nakamura, Y.; Isemura, M. Anti-Cancer Effects of Green Tea Epigallocatchin-3-Gallate and Coffee Chlorogenic Acid. Molecules 2020, 25, 4553. [Google Scholar] [CrossRef] [PubMed]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef] [Green Version]
- Alicandro, G.; Tavani, A.; La Vecchia, C. Coffee and cancer risk: A summary overview. Eur. J. Cancer Prev. 2017, 26, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Micek, A.; Marranzano, M.; Salomone, F.; Del Rio, D.; Ray, S. Coffee Consumption and Risk of Biliary Tract Cancers and Liver Cancer: A Dose–Response Meta-Analysis of Prospective Cohort Studies. Nutrients 2017, 9, 950. [Google Scholar] [CrossRef] [Green Version]
- Sartini, M.; Bragazzi, N.L.; Spagnolo, A.M.; Schinca, E.; Ottria, G.; Dupont, C.; Cristina, M.L.; Sartini, M.; Bragazzi, N.L.; Spagnolo, A.M.; et al. Coffee Consumption and Risk of Colorectal Cancer: A Systematic Review and Meta-Analysis of Prospective Studies. Nutrients 2019, 11, 694. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.C.; Mack, T.M.; Hanisch, R.; Cicioni, C.; Henderson, B.E. Cigarette smoking, obesity, diuretic use, and coffee consumption as risk factors for renal cell carcinoma. J. Natl. Cancer Inst. 1986, 77, 351–356. [Google Scholar] [PubMed]
- Tahbaz, R.; Schmid, M.; Merseburger, A.S. Prevention of kidney cancer incidence and recurrence: Lifestyle, medication and nutrition. Curr. Opin. Urol. 2018, 28, 62–79. [Google Scholar] [CrossRef]
- Research WCRFAIfC. Non-Alcoholic Drinks. Available online: https://www.wcrf.org/dietandcancer/non-alcoholic-drinks/ (accessed on 3 September 2021).
- Research WCRFAIfC. Physical Activity. Available online: https://www.wcrf.org/dietandcancer/physical-activity/ (accessed on 3 September 2021).
- Ochiai, R.; Tomonobu, K.; Ikushima, I. Effect of chlorogenic acids on fatigue and sleep in healthy males: A randomized, double-blind, placebo-controlled, crossover study. Food Sci. Nutr. 2018, 6, 2530–2536. [Google Scholar] [CrossRef]
- Torquati, L.; Peeters, G.; Brown, W.J.; Skinner, T.L. A Daily Cup of Tea or Coffee May Keep You Moving: Association between Tea and Coffee Consumption and Physical Activity. Int. J. Environ. Res. Public Health 2018, 15, 1812. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.C.; Winters-Stone, K.; Lee, A.; Schmitz, K.H. Cancer, Physical Activity, and Exercise. Compr. Physiol. 2012, 2, 2775–2809. [Google Scholar] [CrossRef] [Green Version]
- Bower, J.E. Cancer-related fatigue—Mechanisms, risk factors, and treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.-S.; Lee, C.H.; Sim, S.; Hong, S.K.; Choi, H.G. Physical Activity, Sedentary Habits, Sleep, and Obesity are Associated with Asthma, Allergic Rhinitis, and Atopic Dermatitis in Korean Adolescents. Yonsei Med. J. 2017, 58, 1040–1046. [Google Scholar] [CrossRef]
- Xie, Y.; Huang, S.; He, T.; Su, Y. Coffee consumption and risk of gastric cancer: An updated meta-analysis. Asia Pac. J. Clin. Nutr. 2016, 25, 578–588. [Google Scholar]
- Parra-Lara, L.G.; Mendoza-Urbano, D.M.; Bravo, J.C.; Salamanca, C.H.; Zambrano, A.R. Coffee Consumption and Its Inverse Relationship with Gastric Cancer: An Ecological Study. Nutrients 2020, 12, 3028. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Hishida, A.; Wakai, K. Coffee consumption and liver cancer risk in Japan: A meta-analysis of six prospective cohort studies. Nagoya J. Med. Sci. 2019, 81, 143–150. [Google Scholar] [CrossRef]
- Sánchez-Quesada, C.; Romanos-Nanclares, A.; Navarro, A.M.; Gea, A.; Cervantes, S.; Martínez-González, M.A.; Toledo, E. Coffee consumption and breast cancer risk in the SUN project. Eur. J. Nutr. 2020, 59, 3461–3471. [Google Scholar] [CrossRef] [PubMed]
- Han, M.A.; Kim, J.H. Coffee Consumption and the Risk of Thyroid Cancer: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2017, 14, 129. [Google Scholar] [CrossRef] [Green Version]
- Bae, J.-M. Coffee Consumption and Colon Cancer Risk: A Meta-Epidemiological Study of Asian Cohort Studies. Asian Pac. J. Cancer Prev. 2020, 21, 1177–1179. [Google Scholar] [CrossRef]
- Micek, A.; Gniadek, A.; Kawalec, P.; Brzostek, T. Coffee consumption and colorectal cancer risk: A dose-response meta-analysis on prospective cohort studies. Int. J. Food Sci. Nutr. 2019, 70, 986–1006. [Google Scholar] [CrossRef] [PubMed]
- Steck, S.E.; Murphy, E.A. Dietary patterns and cancer risk. Nat. Rev. Cancer 2019, 20, 125–138. [Google Scholar] [CrossRef]
- Deng, Y. Rectal Cancer in Asian vs. Western Countries: Why the Variation in Incidence? Curr. Treat. Options Oncol. 2017, 18, 64. [Google Scholar] [CrossRef] [PubMed]
- Mojica, B.E.; Fong, L.E.; Biju, D.; Muharram, A.; Davis, I.M.; Vela, K.O.; Rios, D.; Osorio-Camacena, E.; Kaur, B.; Rojas, S.M.; et al. The Impact of the Roast Levels of Coffee Extracts on their Potential Anticancer Activities. J. Food Sci. 2018, 83, 1125–1130. [Google Scholar] [CrossRef]
- Gaascht, F.; Dicato, M.; Diederich, M. Coffee provides a natural multitarget pharmacopeia against the hallmarks of cancer. Genes Nutr. 2015, 10, 1–17. [Google Scholar] [CrossRef]
- Yamagata, K. Do Coffee Polyphenols Have a Preventive Action on Metabolic Syndrome Associated Endothelial Dysfunctions? An Assessment of the Current Evidence. Antioxidants 2018, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Grubben, M.J.; Van Den Braak, C.C.; Broekhuizen, R.; De Jong, R.; Van Rijt, L.; De Ruijter, E.; Peters, W.H.; Katan, M.B.; Nagengast, F.M. The effect of unfiltered coffee on potential biomarkers for colonic cancer risk in healthy volunteers: A randomized trial. Aliment. Pharmacol. Ther. 2000, 14, 1181–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, J.; Smith-Warner, S.A.; Yu, D.; Zhang, X.; Blot, W.J.; Xiang, Y.; Sinha, R.; Park, Y.; Tsugane, S.; White, E.; et al. Associations of coffee and tea consumption with lung cancer risk. Int. J. Cancer 2020, 148, 2457–2470. [Google Scholar] [CrossRef]
- Seow, W.J.; Koh, W.-P.; Jin, A.; Wang, R.; Yuan, J.-M. Associations between tea and coffee beverage consumption and the risk of lung cancer in the Singaporean Chinese population. Eur. J. Nutr. 2019, 59, 3083–3091. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, Y.; Tao, Z.; Wang, K. Coffee consumption and risk of prostate cancer: A systematic review and meta-analysis. BMJ Open 2021, 11, e038902. [Google Scholar] [CrossRef]
- Dai, Z.-W.; Cai, K.-D.; Li, F.-R.; Wu, X.-B.; Chen, G.-C. Association between coffee consumption and risk of bladder cancer in a meta-analysis of 16 prospective studies. Nutr. Metab. 2019, 16, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.C.; Lee, I.M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; de Gonzalez, A.B.; Hartge, P.; et al. Association of Leisure-Time Physical Activity with Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef]
- Kenfield, S.A.; Stampfer, M.J.; Giovannucci, E.; Chan, J. Physical Activity and Survival after Prostate Cancer Diagnosis in the Health Professionals Follow-Up Study. J. Clin. Oncol. 2011, 29, 726–732. [Google Scholar] [CrossRef]
- Pedersen, L.; Idorn, M.; Olofsson, G.H.; Lauenborg, B.; Nookaew, I.; Hansen, R.H.; Johannesen, H.H.; Becker, J.C.; Pedersen, K.S.; Dethlefsen, C.; et al. Voluntary Running Suppresses Tumor Growth through Epinephrine- and IL-6-Dependent NK Cell Mobilization and Redistribution. Cell Metab. 2016, 23, 554–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ligibel, J.A.; Basen-Engquist, K.; Bea, J.W. Weight Management and Physical Activity for Breast Cancer Prevention and Control. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, e22–e33. [Google Scholar] [CrossRef] [PubMed]
- KKim, Y.; Han, B.-G. Ko GESg. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2016, 46, e20. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Participants | p Value | ||||
|---|---|---|---|---|---|---|
| No Drink | 1–30 Cups/Month | 30–60 Cups/Month | >60 Cups/Month | |||
| Number (n) | 27,131 | 36,235 | 62,806 | 36,048 | ||
| Age (mean, SD, y) | 55.7 (8.3) | 53.7 (8.3) | 53.1 (8.3) | 51.0 (8.0) | <0.001 * | |
| Sex (n, %) | <0.001 * | |||||
| Male | 7145 (26.3) | 11,092 (30.6) | 19,986 (31.8) | 17,387 (48.2) | ||
| Female | 19,986 (73.7) | 25,143 (69.4) | 42,820 (68.2) | 18,661 (51.8) | ||
| Obesity (BMI, kg/m2, n, %) | <0.001 * | |||||
| Underweight (<18.5) | 781 (2.9) | 613 (1.7) | 979 (1.6) | 533 (1.5) | ||
| Normal (18.5–23) | 11,487 (42.3) | 13,618 (37.6) | 22,993 (36.6) | 12,604 (35.0) | ||
| Overweight (23–25) | 7373 (27.2) | 10,148 (28.0) | 17,562 (28.0) | 9985 (27.7) | ||
| Obese (≥ 25) | 7490 (27.6) | 11,856 (32.7) | 21,272 (33.9) | 12,926 (35.9) | ||
| Income (n, %) | <0.001 * | |||||
| Missing, no response | 4328 (16.0) | 5439 (15.0) | 7258 (11.6) | 3667 (10.2) | ||
| Lowest | 9386 (34.6) | 10,539 (29.1) | 17,459 (27.8) | 8597 (23.8) | ||
| Middle | 8935 (32.9) | 12,965 (35.8) | 24,042 (38.3) | 14,591 (40.5) | ||
| Highest | 4482 (16.5) | 7292 (20.1) | 14,047 (22.4) | 9193 (25.5) | ||
| Smoking status (n, %) | <0.001 * | |||||
| Never smoker | 22,552 (83.1) | 28,298 (78.1) | 47,058 (74.9) | 20,405 (56.6) | ||
| Former smoker | 3142 (11.6) | 4951 (13.7) | 9230 (14.7) | 6465 (17.9) | ||
| Current smoker | 1437 (5.3) | 2986 (8.2) | 6518 (10.4) | 9178 (25.5) | ||
| Alcohol consumption (n, %) | <0.001 * | |||||
| Never drinker | 18,248 (67.3) | 19,385 (53.5) | 31,008 (49.4) | 13,986 (38.8) | ||
| Former drinker | 1171 (4.3) | 1472 (4.1) | 2076 (3.3) | 1533 (4.3) | ||
| Current drinker | 7712 (28.4) | 15,378 (42.4) | 29,722 (47.3) | 20,529 (56.9) | ||
| Hypertension (n, %) | 6946 (25.6) | 8624 (23.8) | 14,374 (22.9) | 6604 (18.3) | <0.001 * | |
| Diabetes mellitus (n, %) | 2701 (10.0) | 3201 (8.8) | 4836 (7.7) | 2231 (6.2) | <0.001 * | |
| Hyperlipidemia (n, %) | 4042 (14.9) | 5317 (14.7) | 8304 (13.2) | 4023 (11.2) | <0.001 * | |
| Stroke (n, %) | 566 (2.1) | 493 (1.4) | 809 (1.3) | 411 (1.1) | <0.001 * | |
| Ischemic heart disease (n, %) | 1077 (4.0) | 1163 (3.2) | 1781 (2.8) | 929 (2.6) | <0.001 * | |
| Nutritional intake (mean, SD) | ||||||
| Total calories (kcal/d) | 1631.8 (545.9) | 1666.3 (591.0) | 1774 (539.8) | 1901.9 (631.2) | <0.001 * | |
| Protein (g/d) | 55.3 (25.5) | 56.0 (27.6) | 60.4 (24.7) | 65.4 (29.3) | <0.001 * | |
| Fat (g/d) | 23.1 (16.4) | 25.3 (18.7) | 28.6 (16.8) | 33.6 (20.5) | <0.001 * | |
| Carbohydrate (g/d) | 296.4 (91.7) | 298.9 (96.4) | 315.0 (90.0) | 330.1 (101.7) | <0.001 * | |
| Exercise | <0.001 * | |||||
| No regular exercise | 13,541 (49.9) | 17,099 (47.2) | 31,241 (49.7) | 20,214 (56.1) | ||
| <150 min/week | 3698 (13.6) | 6079 (16.8) | 8948 (14.2) | 4942 (13.7) | ||
| ≥150 min/week | 9892 (36.5) | 13,057 (36.0) | 22,617 (36.0) | 10,892 (30.2) | ||
| Gastric cancer | 237 (0.9) | 188 (0.5) | 360 (0.6) | 191 (0.5) | <0.001 * | |
| Hepatic cancer | 42 (0.2) | 26 (0.1) | 60 (0.1) | 18 (0.0) | <0.001 * | |
| Colon cancer | 130 (0.5) | 121 (0.3) | 194 (0.3) | 76 (0.2) | <0.001 * | |
| Breast cancer † | 310 (1.6) | 275 (1.1) | 408 (1.0) | 124 (0.7) | <0.001 * | |
| Uterine cervix cancer † | 153 (0.8) | 165 (0.7) | 259 (0.6) | 112 (0.6) | <0.001 * | |
| Lung cancer | 47 (0.2) | 40 (0.1) | 60 (0.1) | 39 (0.1) | 0.016 * | |
| Thyroid cancer | 301 (1.1) | 363 (1.0) | 527 (0.8) | 219 (0.6) | <0.001 * | |
| Prostate cancer † | 30 (0.4) | 39 (0.4) | 62 (0.3) | 36 (0.2) | 0.946 | |
| Bladder cancer | 19 (0.1) | 19 (0.1) | 39 (0.1) | 26 (0.1) | 0.724 | |
| Type of Cancer | N of Cancer | N of Control | OR (95% CI) | ||
|---|---|---|---|---|---|
| (Exposure/Total, %) | (Exposure/Total, %) | Crude | Adjusted † | ||
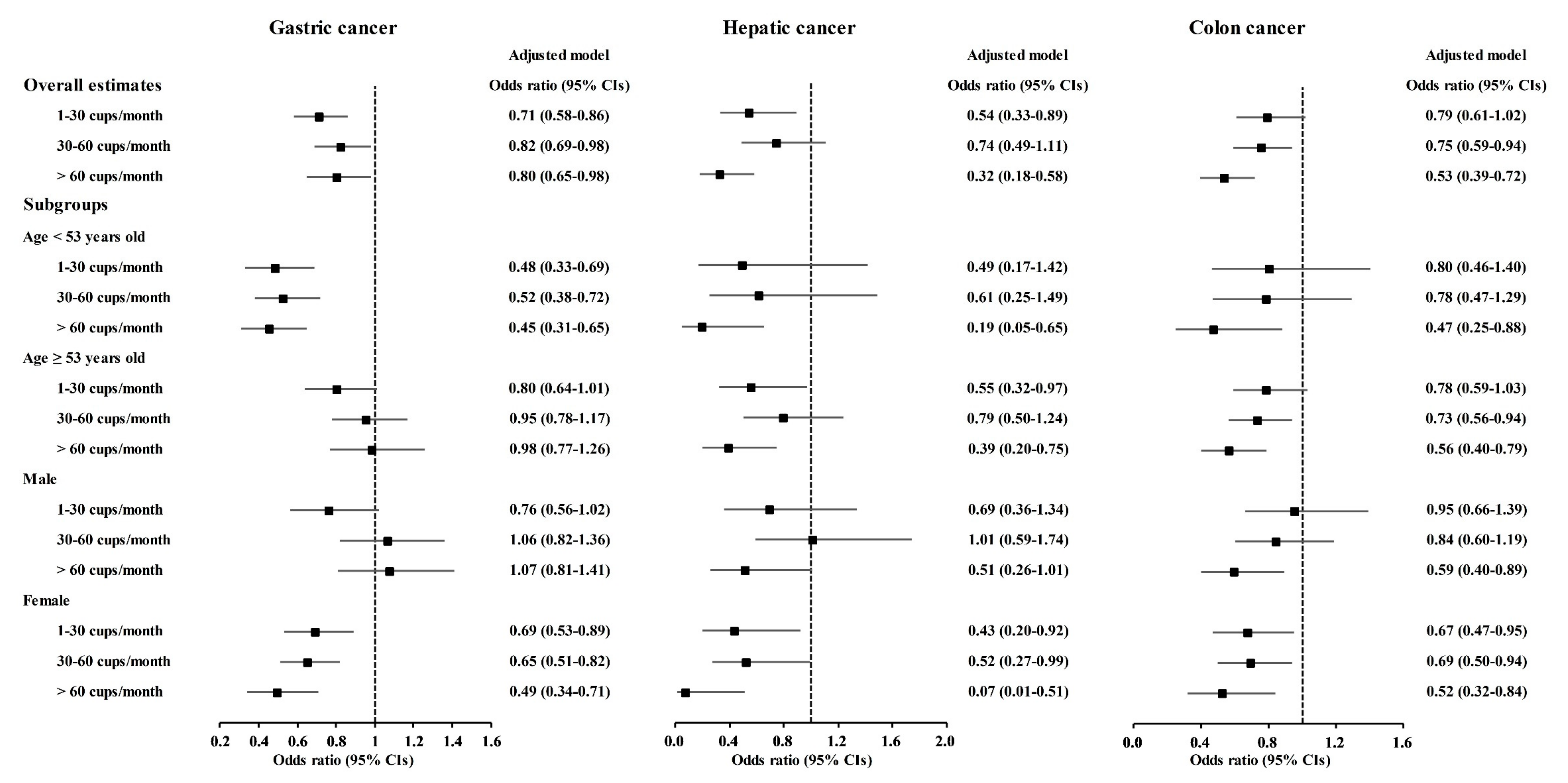
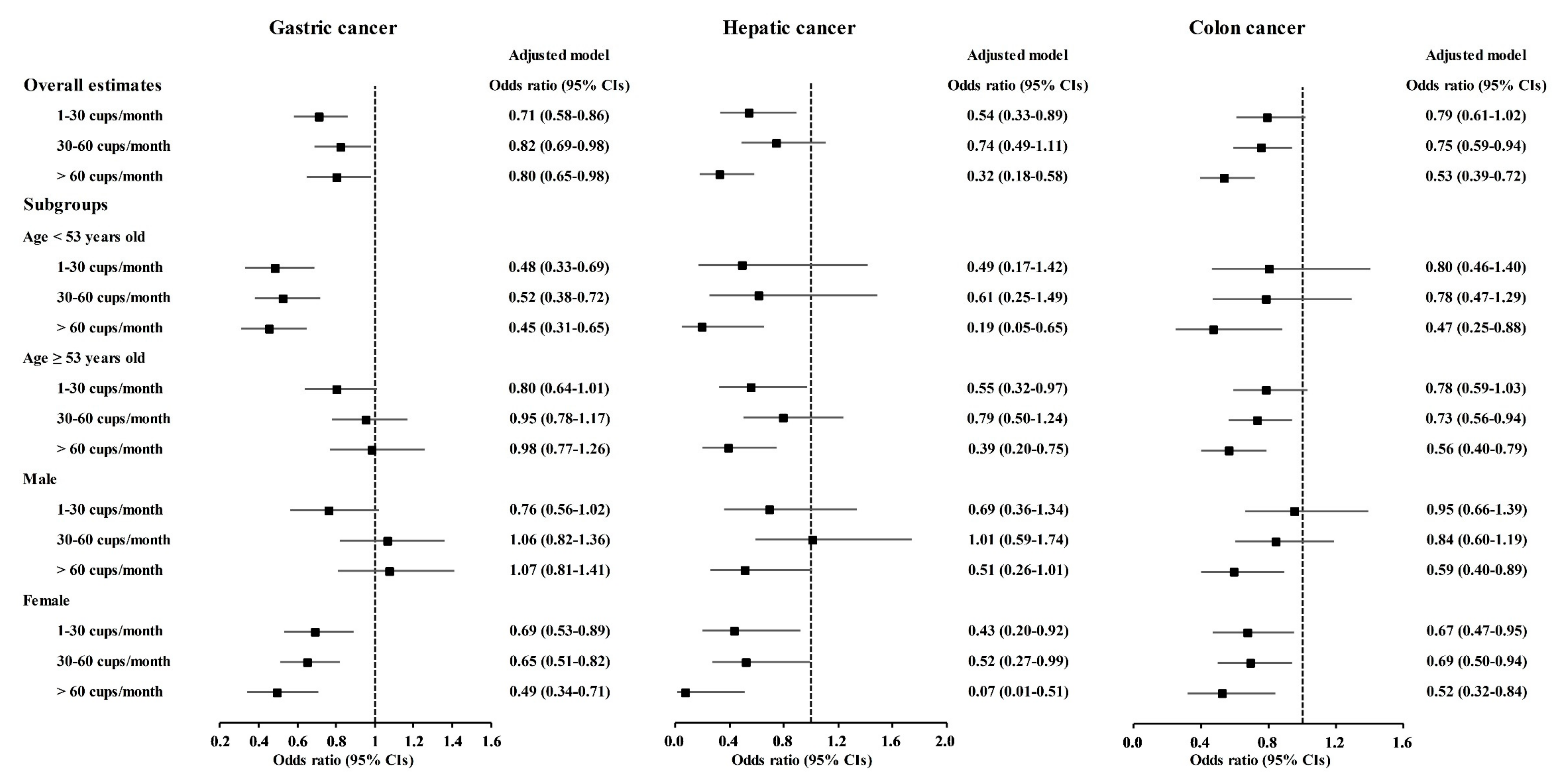
| Gastric cancer | |||||
| No drink | 237/976 (24.3%) | 26,894/161,244 (16.7%) | 1.00 | 1.00 | |
| 1–30 cups/month | 188/976 (19.3%) | 36,047/161,244 (22.4%) | 0.59 (0.49–0.72) * | 0.71 (0.58–0.86) * | |
| 30–60 cups/month | 360/976 (36.9%) | 62,446/161,244 (38.7%) | 0.65 (0.56–0.77) * | 0.82 (0.69–0.98) * | |
| >60 cups/month | 191/976 (19.6%) | 35,857/161,244 (22.2%) | 0.60 (0.50–0.73) * | 0.80 (0.65–0.98) * | |
| Hepatic cancer | |||||
| No drink | 42/146 (27.8%) | 27,089/162,074 (16.7%) | 1.00 | 1.00 | |
| 1–30 cups/month | 26/146 (17.8%) | 36,209/162,074 (22.3%) | 0.46 (0.28–0.76) * | 0.54 (0.33–0.89) * | |
| 30–60 cups/month | 60/146 (41.1%) | 62,746/162,074 (38.7%) | 0.62 (0.42–0.92) * | 0.74 (0.49–1.11) | |
| >60 cups/month | 18/146 (12.3%) | 36,030/162,074 (22.2%) | 0.32 (0.19–0.56) * | 0.32 (0.18–0.58) * | |
| Colon cancer | |||||
| No drink | 130/521 (24.9%) | 27,001/161,699 (16.7%) | 1.00 | 1.00 | |
| 1–30 cups/month | 121/521 (23.2%) | 36,114/161,699 (22.3%) | 0.70 (0.54–0.89) * | 0.79 (0.61–1.02) | |
| 30–60 cups/month | 194/521 (37.2%) | 62,612/161,699 (38.7%) | 0.64 (0.52–0.80) * | 0.75 (0.59–0.94) * | |
| >60 cups/month | 76/521 (14.6%) | 35,972/161,699 (22.2%) | 0.44 (0.33–0.58) * | 0.53 (0.39–0.72) * | |
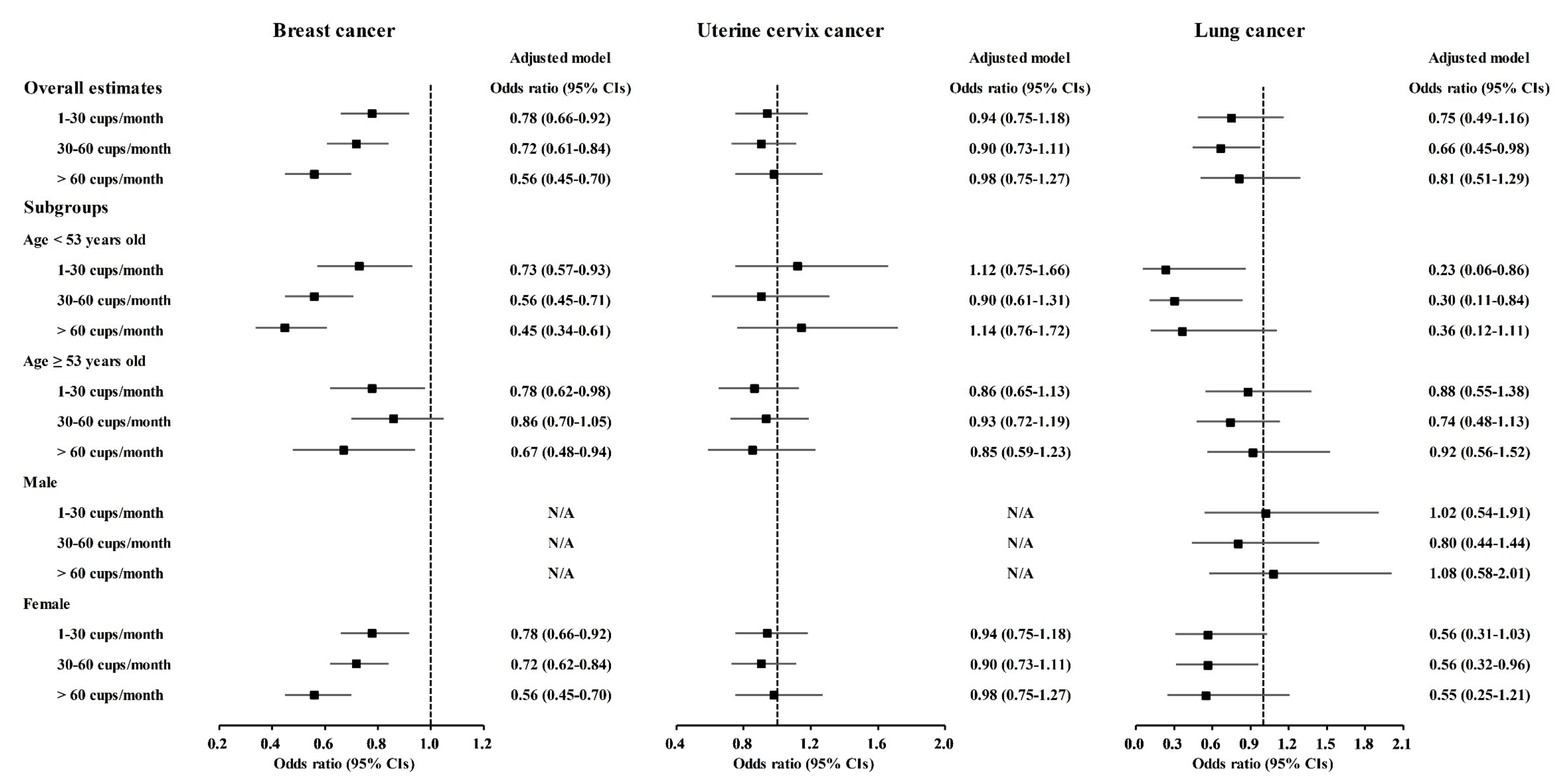
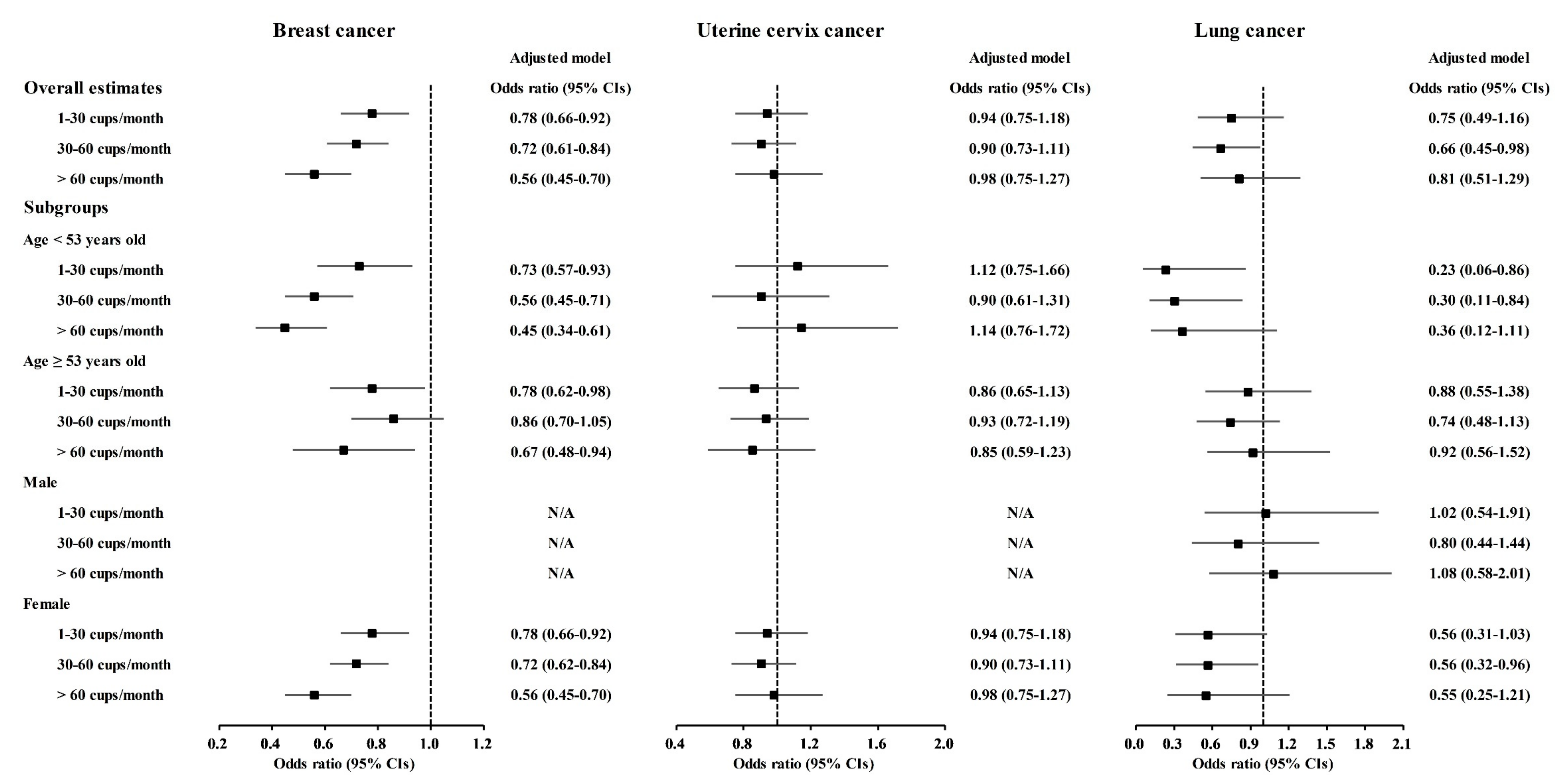
| Breast cancer ‡ | |||||
| No drink | 310/1117 (27.8%) | 19,676/105,493 (18.7%) | 1.00 | 1.00 | |
| 1–30 cups/month | 275/1117 (24.6%) | 24,868/105,493 (23.6%) | 0.70 (0.60–0.83) * | 0.78 (0.66–0.92) * | |
| 30–60 cups/month | 408/1117 (36.5%) | 42,412/105,493 (40.2%) | 0.61 (0.53–0.71) * | 0.72 (0.61–0.84) * | |
| >60 cups/month | 124/1117 (11.1%) | 18,537/105,493 (17.6%) | 0.43 (0.34–0.52) * | 0.56 (0.45–0.70) * | |
| Uterine cervix cancer ‡ | |||||
| No drink | 153/689 (22.2%) | 19,833/105,921 (18.7%) | 1.00 | 1.00 | |
| 1–30 cups/month | 165/689 (23.9%) | 24,978/105,921 (23.6%) | 0.86 (0.69–1.07) | 0.94 (0.75–1.18) | |
| 30–60 cups/month | 259/689 (37.6%) | 42,561/105,921 (40.2%) | 0.79 (0.65–0.96) * | 0.90 (0.73–1.11) | |
| >60 cups/month | 112/689 (16.3%) | 18,549/105,921 (17.5%) | 0.78 (0.61–1.00) * | 0.98 (0.75–1.27) | |
| Lung cancer | |||||
| No drink | 47/186 (25.3%) | 27,084/162,034 (16.7%) | 1.00 | 1.00 | |
| 1–30 cups/month | 40/186 (21.5%) | 36,195/162,034 (22.3%) | 0.64 (0.42–0.97) * | 0.75 (0.49–1.16) | |
| 30–60 cups/month | 60/186 (32.3%) | 62,746/162,034 (38.7%) | 0.55 (0.38–0.81) * | 0.66 (0.45–0.98) * | |
| >60 cups/month | 39/186 (21.0%) | 36,009/162,034 (22.2%) | 0.62 (0.41–0.95) * | 0.81 (0.51–1.29) | |
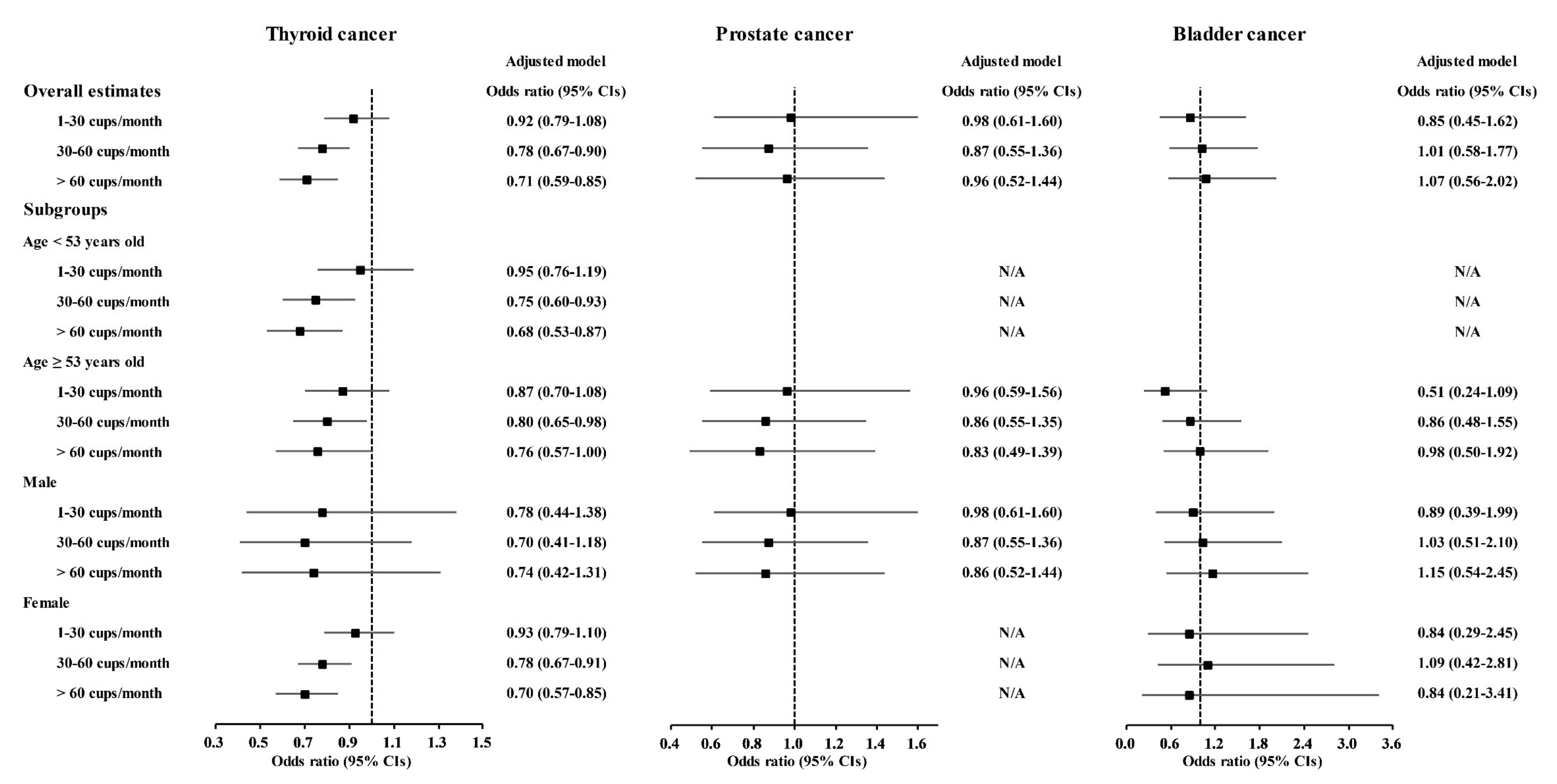
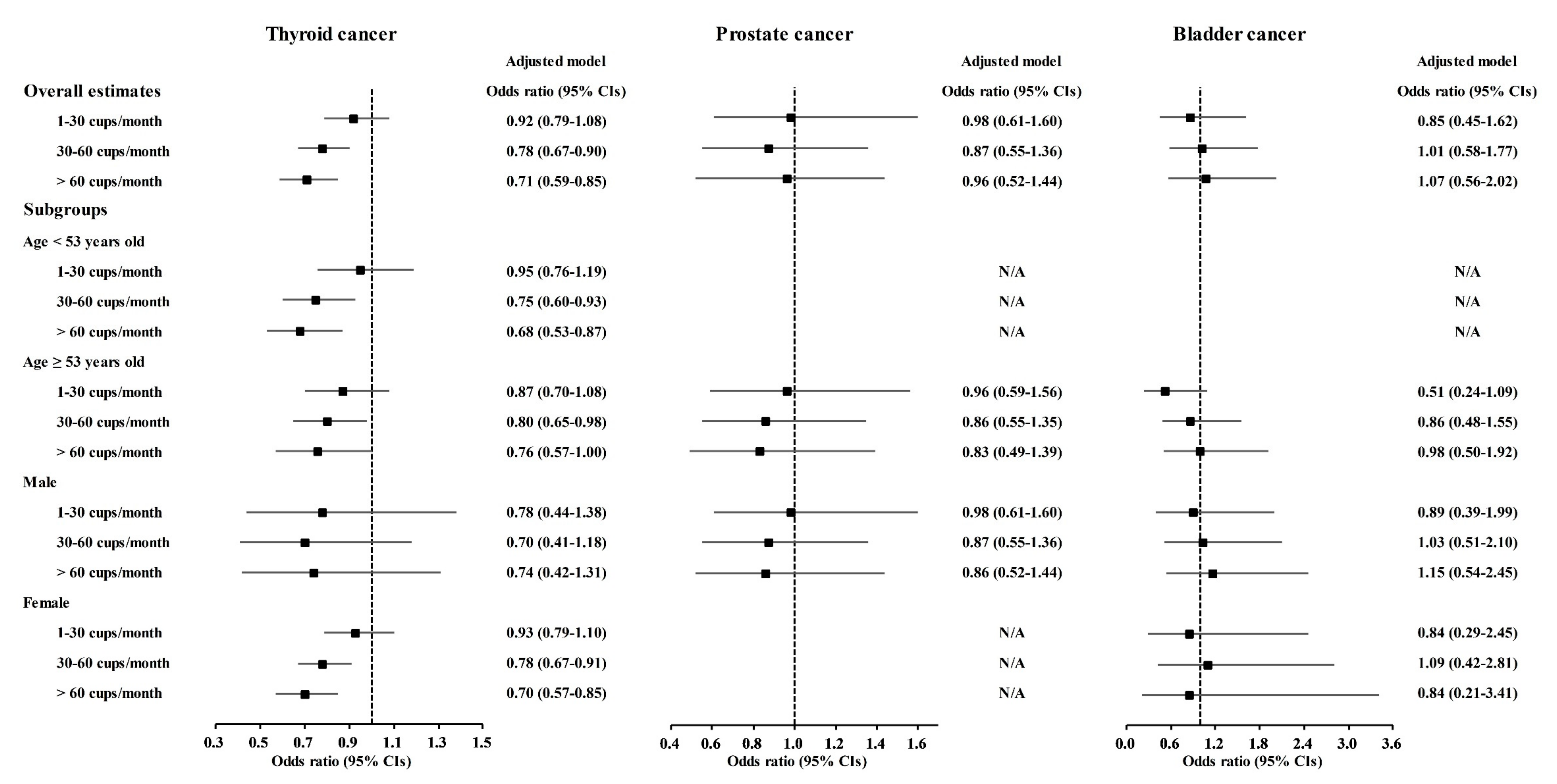
| Thyroid cancer | |||||
| No drink | 301/1410 (21.3%) | 26,830/160,810 (16.7%) | 1.00 | 1.00 | |
| 1–30 cups/month | 363/1410 (25.7%) | 35,872/160,810 (22.3%) | 0.90 (0.77–1.05) | 0.92 (0.79–1.08) | |
| 30–60 cups/month | 527/1410 (37.4%) | 62,279/160,810 (38.7%) | 0.75 (0.65–0.87) * | 0.78 (0.67–0.90) * | |
| >60 cups/month | 219/1410 (15.5%) | 35,829/160,810 (22.3%) | 0.55 (0.46–0.65) * | 0.71 (0.59–0.85) * | |
| Prostate cancer ‡ | |||||
| No drink | 30/167 (18.0%) | 7115/55,443 (12.8%) | 1.00 | 1.00 | |
| 1–30 cups/month | 39/167 (23.3%) | 11,053/55,443 (19.9%) | 0.84 (0.52–1.35) | 0.98 (0.61–1.60) | |
| 30–60 cups/month | 62/167 (37.1%) | 19,924/55,443 (35.9%) | 0.74 (0.48–1.14) | 0.87 (0.55–1.36) | |
| >60 cups/month | 36/167 (21.6%) | 17,351/55,443 (31.3%) | 0.49 (0.30–0.80) * | 0.86 (0.52–1.44) | |
| Bladder cancer | |||||
| No drink | 19/103 (18.4%) | 27,112/162,117 (16.7%) | 1.00 | 1.00 | |
| 1–30 cups/month | 19/103 (18.4%) | 36,216/162,117 (22.3%) | 0.75 (0.40–1.41) | 0.85 (0.45–1.62) | |
| 30–60 cups/month | 39/103 (37.9%) | 62,767/162,117 (38.7%) | 0.89 (0.51–1.53) | 1.01 (0.58–1.77) | |
| >60 cups/month | 26/103 (25.2%) | 36,022/162,117 (22.2%) | 1.03 (0.57–1.86) | 1.07 (0.56–2.02) | |
| Type of Cancer | N of Cancer | N of Control | OR (95% CI) | ||
|---|---|---|---|---|---|
| (Exposure/Total, %) | (Exposure/Total, %) | Crude | Adjusted † | ||
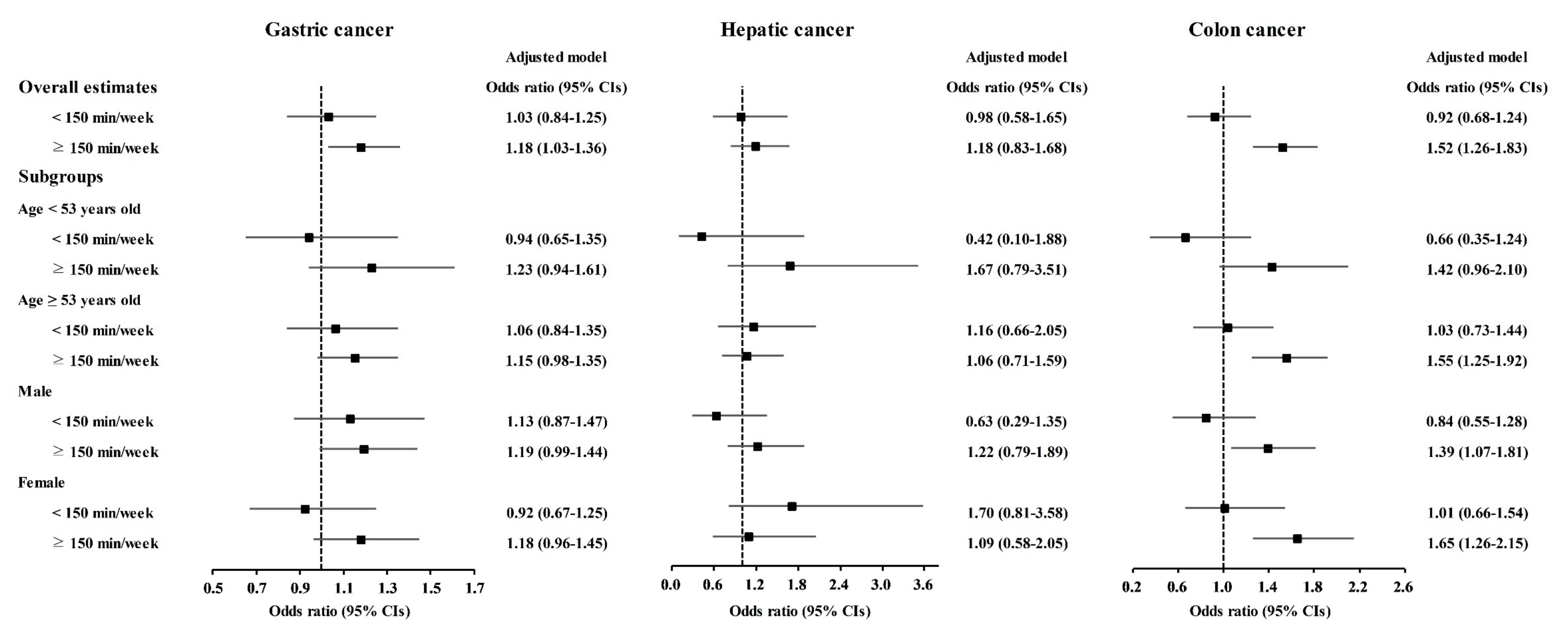
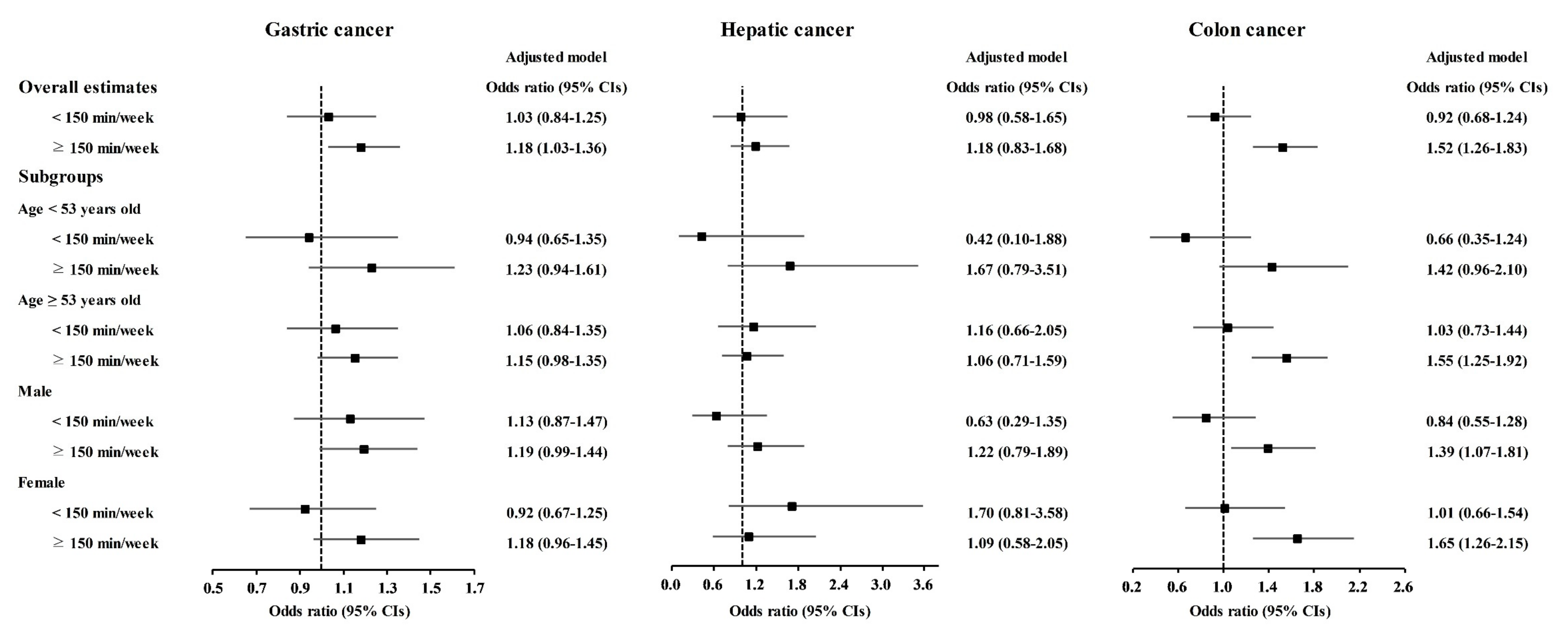
| Gastric cancer | |||||
| No regular exercise | 444/976 (45.5%) | 81,651/161,244 (50.6%) | 1.00 | 1.00 | |
| <150 min/week | 128/976 (13.1%) | 23,539/161,244 (14.6%) | 1.00 (0.82–1.22) | 1.03 (0.84–1.25) | |
| ≥150 min/week | 404/976 (41.4%) | 56,054/161,244 (34.8%) | 1.33 (1.16–1.52) * | 1.18 (1.03–1.36) * | |
| Hepatic cancer | |||||
| No regular exercise | 66/146 (45.2%) | 82,029/162,074 (50.6%) | 1.00 | 1.00 | |
| <150 min/week | 18/146 (12.3%) | 23,649/162,074 (14.6%) | 0.95 (0.56–1.59) | 0.98 (0.58–1.65) | |
| ≥150 min/week | 62/146 (42.5%) | 56,396/162,074 (34.8%) | 1.37 (0.97–1.93) | 1.18 (0.83–1.68) | |
| Colon cancer | |||||
| No regular exercise | 211/521 (40.5%) | 81,884/161,699 (50.6%) | 1.00 | 1.00 | |
| <150 min/week | 55/521 (10.6%) | 23,612/161,699 (14.6%) | 0.90 (0.67–1.22) | 0.92 (0.68–1.24) | |
| ≥150 min/week | 255/521 (48.9%) | 56,203/161,699 (34.8%) | 1.76 (1.47–2.11) * | 1.52 (1.26–1.83) * | |
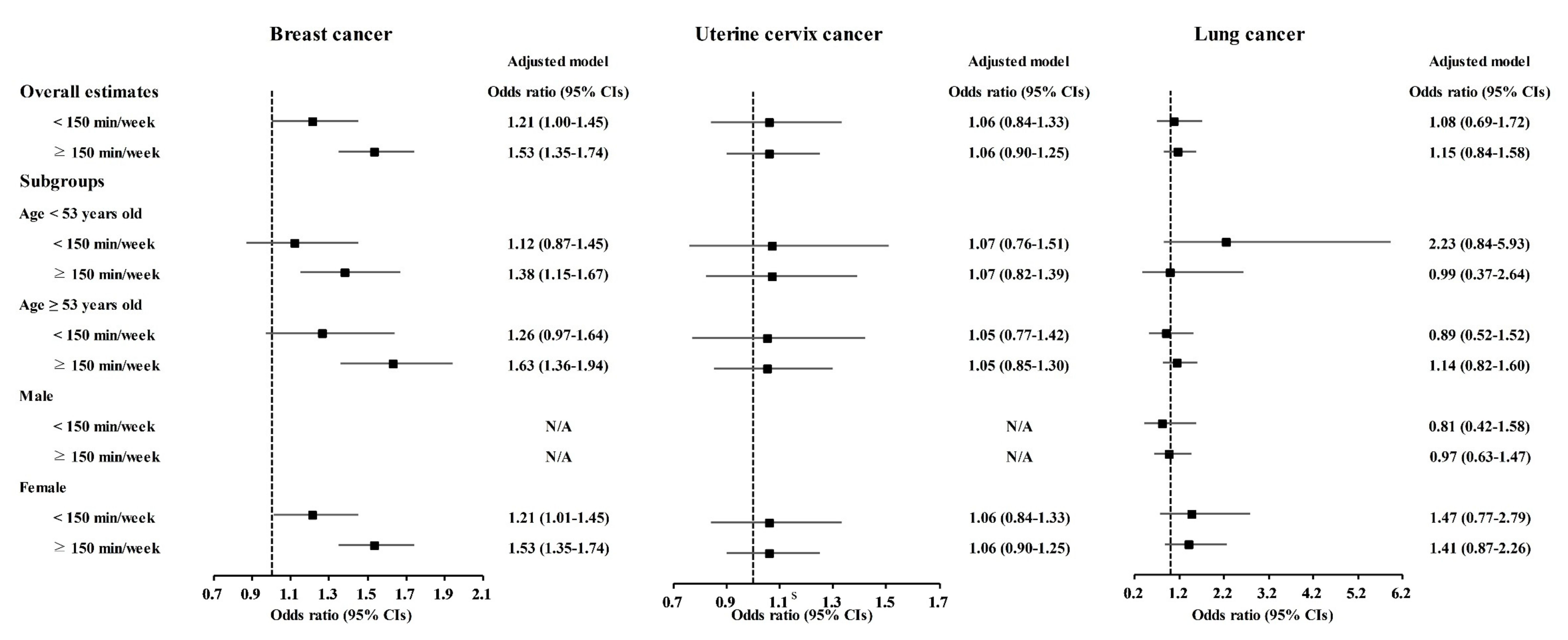
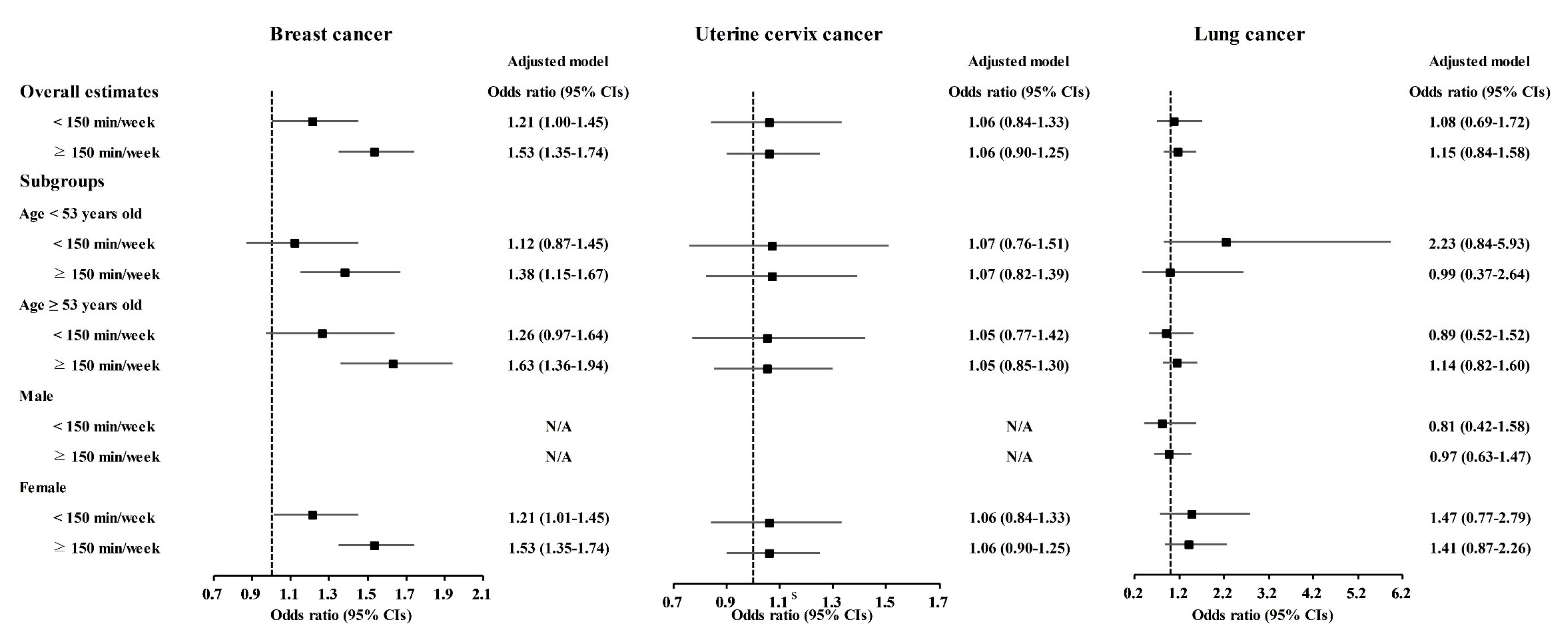
| Breast cancer ‡ | |||||
| No regular exercise | 476/1120 (42.5%) | 81,619/161,100 (50.7%) | 1.00 | 1.00 | |
| <150 min/week | 155/1120 (13.8%) | 23,512/161,100 (14.6%) | 1.13 (0.94–1.36) | 1.21 (1.00–1.45) * | |
| ≥150 min/week | 489/1120 (43.7%) | 55,969/161,100 (34.7%) | 1.50 (1.32–1.70) * | 1.53 (1.35–1.74) * | |
| Uterine cervix cancer ‡ | |||||
| No regular exercise | 355/689 (51.5%) | 81,740/161,531 (50.6%) | 1.00 | 1.00 | |
| <150 min/week | 94/689 (13.6%) | 23,573/161,531 (14.6%) | 0.92 (0.73–1.15) | 1.06 (0.84–1.33) | |
| ≥150 min/week | 240/689 (34.8%) | 56,218/161,531 (34.8%) | 0.98 (0.83–1.16) | 1.06 (0.90–1.25) | |
| Lung cancer | |||||
| No regular exercise | 83/186 (44.6%) | 82,012/162,034 (50.6%) | 1.00 | 1.00 | |
| <150 min/week | 24/186 (12.9%) | 23,646/162,034 (14.6%) | 1.00 (0.64–1.58) | 1.08 (0.69–1.72) | |
| ≥150 min/week | 79/186 (42.5%) | 53,679/162,034 (34.8%) | 1.38 (1.02–1.88) * | 1.15 (0.84–1.58) | |
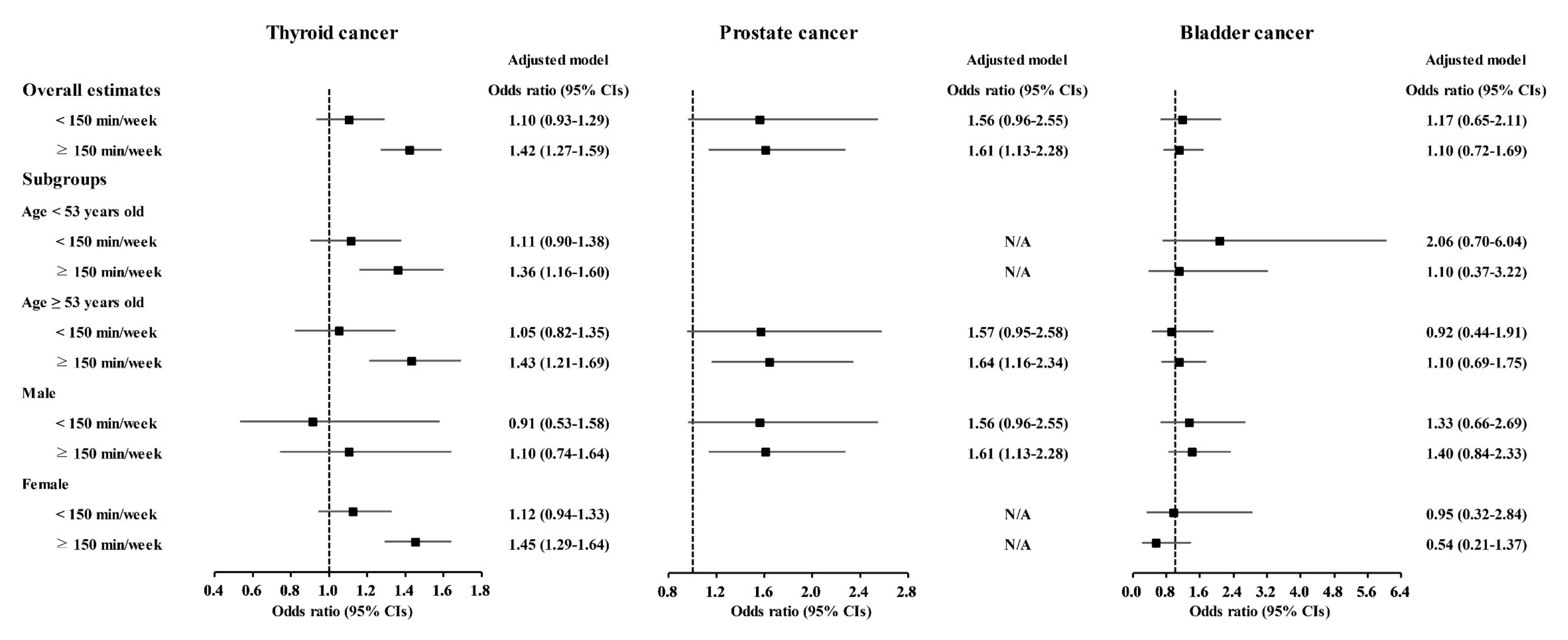
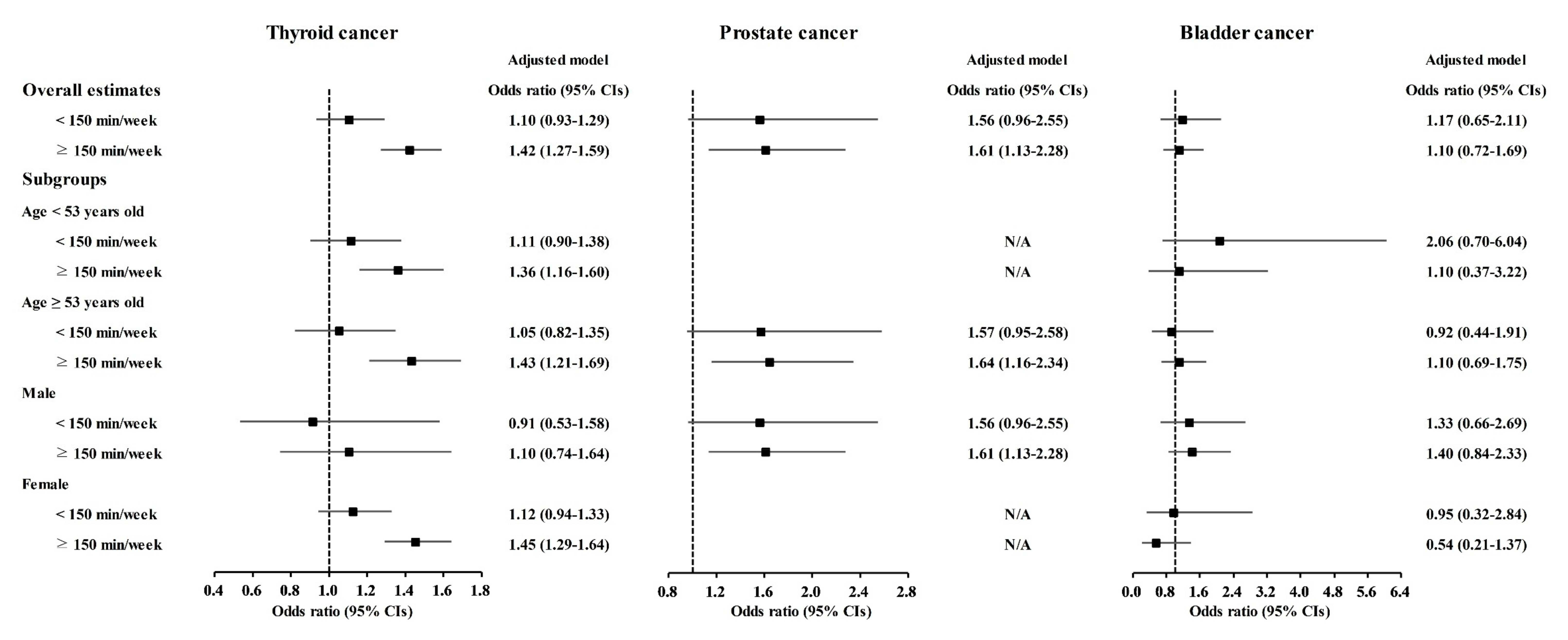
| Thyroid cancer | |||||
| No regular exercise | 616/1410 (43.7%) | 81,479/160,810 (50.7%) | 1.00 | 1.00 | |
| <150 min/week | 191/1410 (13.5%) | 23,476/160,810 (14.6%) | 1.08 (0.91–1.27) | 1.10 (0.93–1.29) | |
| ≥150 min/week | 603/1410 (42.8%) | 55,855/160,810 (34.7%) | 1.43 (1.28–1.60) * | 1.42 (1.27–1.59) * | |
| Prostate cancer ‡ | |||||
| No regular exercise | 53/167 (31.7%) | 82,042/162,053 (50.6%) | 1.00 | 1.00 | |
| <150 min/week | 24/167 (14.4%) | 23,643/162,053 (14.6%) | 1.57 (0.97–2.55) | 1.56 (0.96–2.55) | |
| ≥150 min/week | 90/167 (53.9%) | 56,368/162,053 (34.8%) | 2.47 (1.76–3.47) * | 1.61 (1.13–2.28) * | |
| Bladder cancer | |||||
| No regular exercise | 46/103 (44.7%) | 82,049/162,117 (50.6%) | 1.00 | 1.00 | |
| <150 min/week | 15/103 (14.6%) | 23,652/162,117 (14.6%) | 1.13 (0.63–2.03) | 1.17 (0.65–2.11) | |
| ≥150 min/week | 42/103 (40.8%) | 56,416/162,117 (34.8%) | 1.33 (0.87–2.02) | 1.10 (0.72–1.69) | |
| Type of Cancer | Interaction | |
|---|---|---|
| Crude (p Value) | Adjusted † (p Value) | |
| Gastric cancer | 0.298 | 0.230 |
| Hepatic cancer | 0.215 | 0.125 |
| Colon cancer | 0.190 | 0.380 |
| Breast cancer ‡ | 0.946 | 0.370 |
| Uterine cervix cancer ‡ | 0.937 | 0.366 |
| Lung cancer | 0.791 | 0.840 |
| Thyroid cancer | 0.113 | 0.002 * |
| Prostate cancer ‡ | 0.032 * | 0.102 |
| Bladder cancer | 0.046 * | 0.185 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Yoo, D.M.; Min, C.; Choi, H.G. Association between Coffee Consumption/Physical Exercise and Gastric, Hepatic, Colon, Breast, Uterine Cervix, Lung, Thyroid, Prostate, and Bladder Cancer. Nutrients 2021, 13, 3927. https://doi.org/10.3390/nu13113927
Kim SY, Yoo DM, Min C, Choi HG. Association between Coffee Consumption/Physical Exercise and Gastric, Hepatic, Colon, Breast, Uterine Cervix, Lung, Thyroid, Prostate, and Bladder Cancer. Nutrients. 2021; 13(11):3927. https://doi.org/10.3390/nu13113927
Chicago/Turabian StyleKim, So Young, Dae Myoung Yoo, Chanyang Min, and Hyo Geun Choi. 2021. "Association between Coffee Consumption/Physical Exercise and Gastric, Hepatic, Colon, Breast, Uterine Cervix, Lung, Thyroid, Prostate, and Bladder Cancer" Nutrients 13, no. 11: 3927. https://doi.org/10.3390/nu13113927
APA StyleKim, S. Y., Yoo, D. M., Min, C., & Choi, H. G. (2021). Association between Coffee Consumption/Physical Exercise and Gastric, Hepatic, Colon, Breast, Uterine Cervix, Lung, Thyroid, Prostate, and Bladder Cancer. Nutrients, 13(11), 3927. https://doi.org/10.3390/nu13113927