Classification of Fatigue Phases in Healthy and Diabetic Adults Using Wearable Sensor

 , , and
, , and
Abstract
1. Introduction
2. Background
2.1. Machine Learning and Tremor Recognition
2.2. Machine Learning and Fatigue Phases Recognition
3. Experimental Setup and Data Processing
3.1. Participants
3.2. Procedure
3.3. Wearable Tremor Detection System
3.4. Data Processing
4. Results
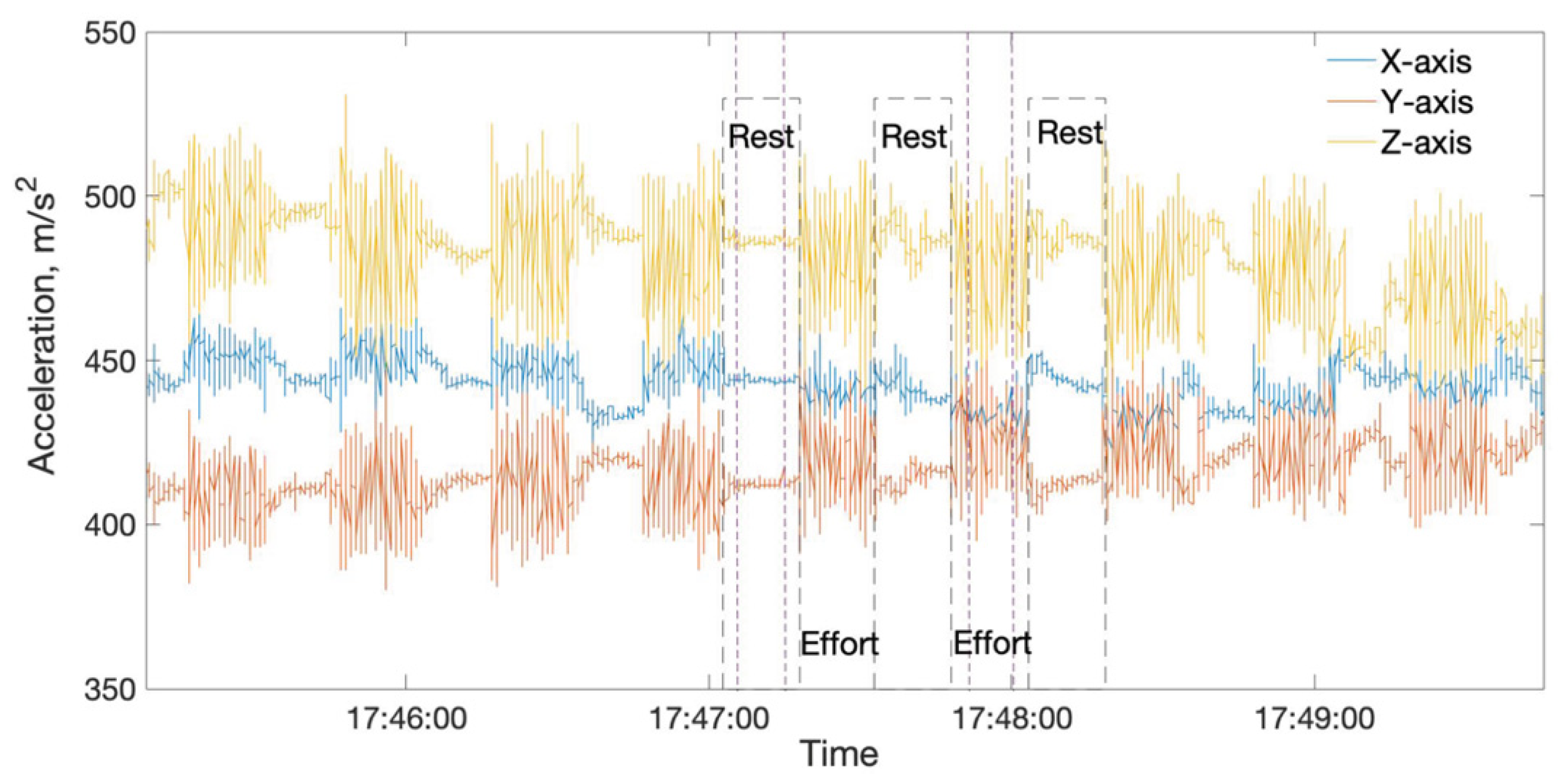
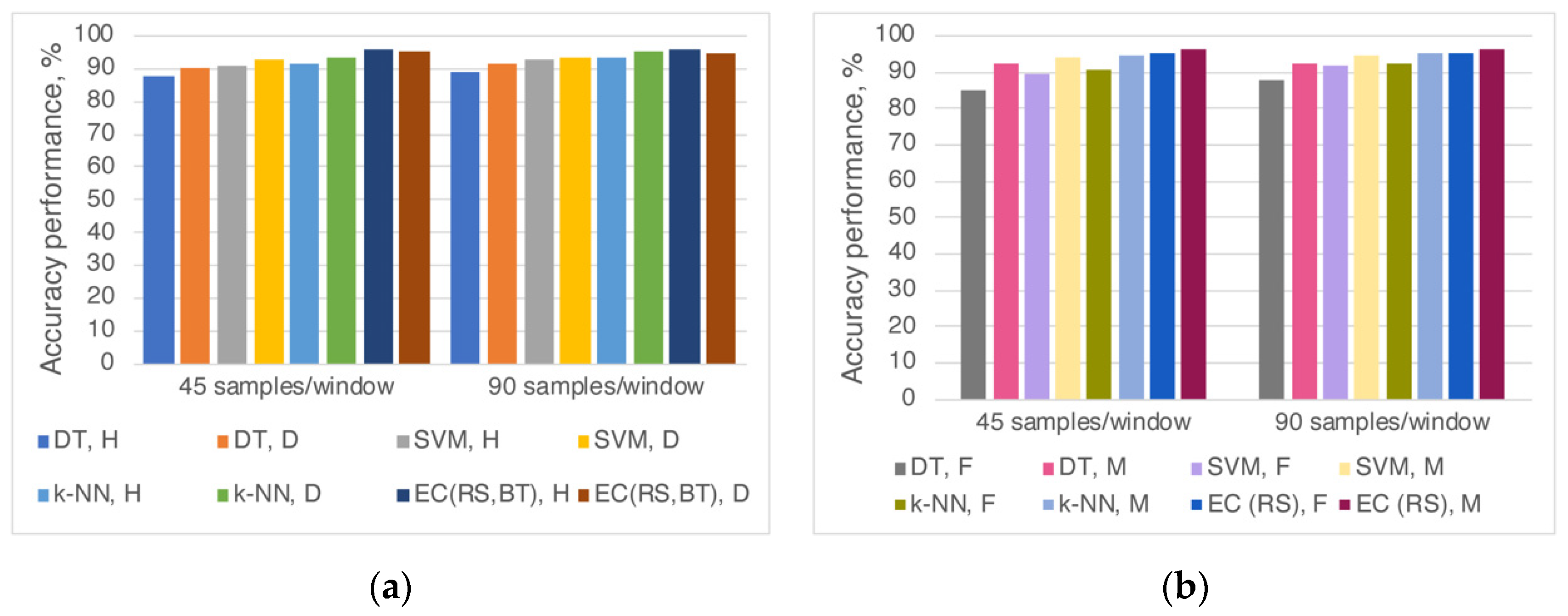
4.1. Rest and Effort Recognition
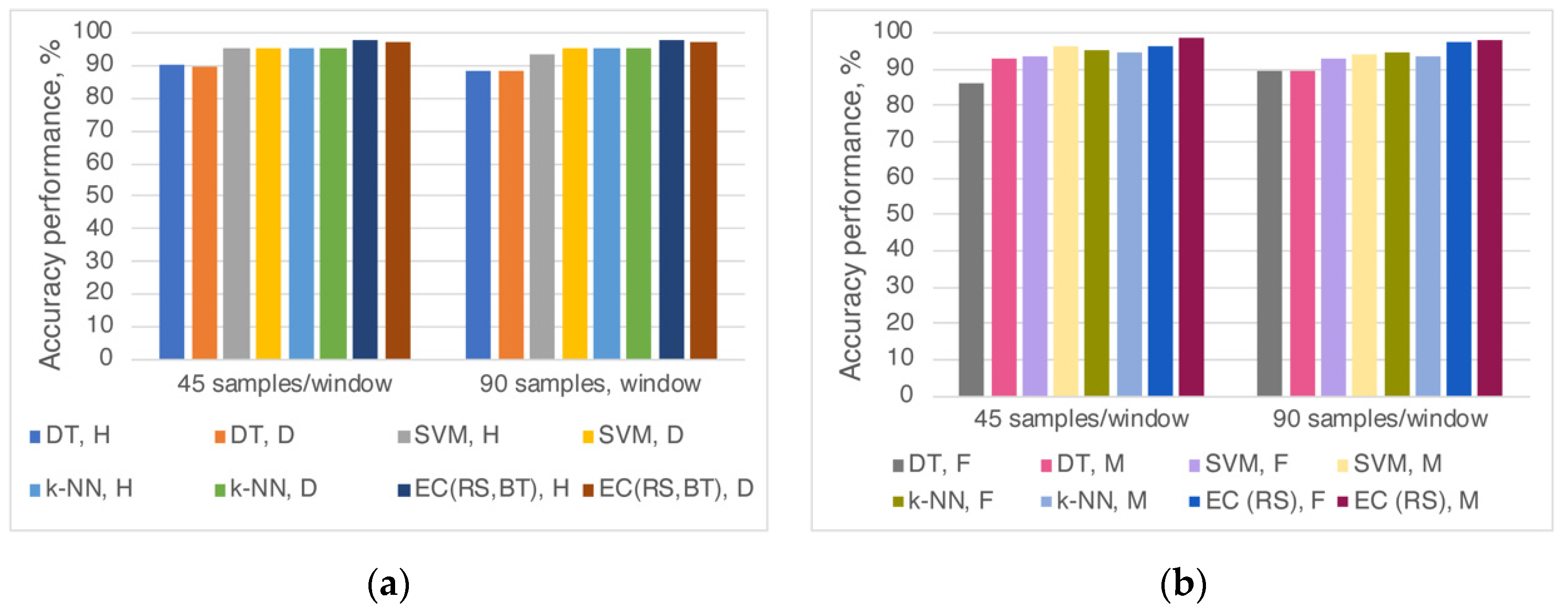
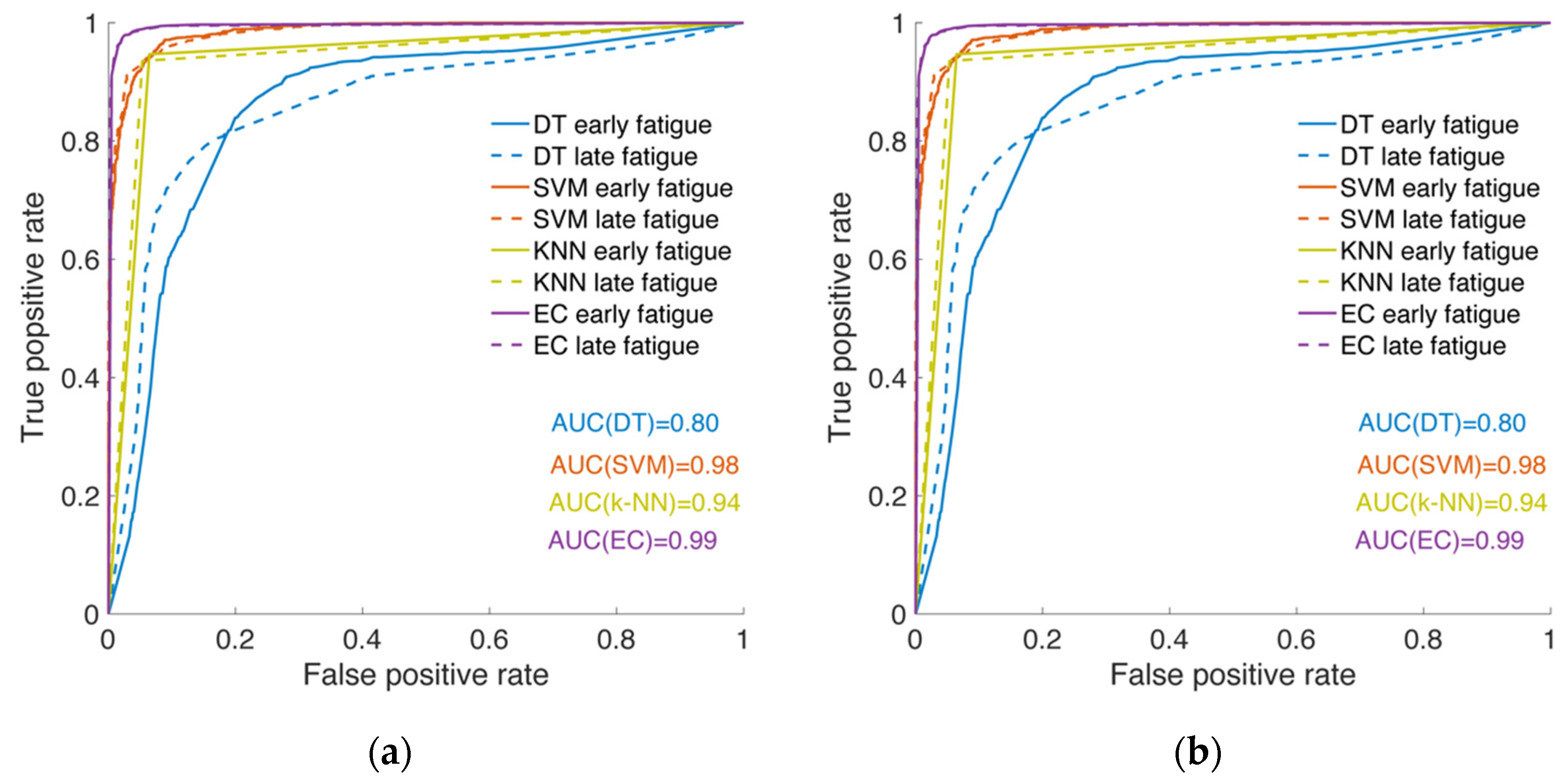
4.2. Early and Late Fatigue Recognition
5. Discussion
5.1. Rest and Effort Recognition
5.2. Early and Late Fatigue Recognition
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vøllestad, N.K. Measurement of human muscle fatigue. J. Neurosci. Methods 1997, 74, 219–227. [Google Scholar] [CrossRef]
- Fritschi, C.; Quinn, L. Fatigue in patients with diabetes: A review. J. Psychosom. Res. 2010, 69, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.-J.; Qin, Z.; Wang, P.-Y.; Sun, Y.; Liu, X. Muscle fatigue: General understanding and treatment. Exp. Mol. Med. 2017, 49, e384. [Google Scholar] [CrossRef] [PubMed]
- Nordlund, M.M.; Thorstensson, A.; Cresswell, A.G. Central and peripheral contributions to fatigue in relation to level of activation during repeated maximal voluntary isometric plantar flexions. J. Appl. Physiol. 2004, 96, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Slack, P.S.; Coulson, C.J.; Ma, X.; Pracy, P.; Parmar, S.; Webster, K. The effect of operating time on surgeon’s hand tremor. Eur. Arch. Oto-Rhino-Laryngol. 2009, 266, 137. [Google Scholar] [CrossRef] [PubMed]
- Gajewski, J. Fatigue-induced changes in tremor caused by physical efforts of different volume and intensity. Acta Bioeng. Biomech. 2006, 8, 103. [Google Scholar]
- Yung, M.; Manji, R.; Wells, R.P. Exploring the relationship of task performance and physical and cognitive fatigue during a daylong light precision task. Hum. Factors 2017, 59, 1029–1047. [Google Scholar] [CrossRef]
- Yung, M.; Bigelow, P.L.; Hastings, D.M.; Wells, R.P. Detecting within-and between-day manifestations of neuromuscular fatigue at work: An exploratory study. Ergonomics 2014, 57, 1562–1573. [Google Scholar] [CrossRef]
- Chaudhuri, A.; Behan, P.O. Fatigue and basal ganglia. J. Neurol. Sci. 2000, 179, 34–42. [Google Scholar] [CrossRef]
- Elble, R.J.; Higgins, C.; Moody, C.J. Stretch reflex oscillations and essential tremor. J. Neurol. Neurosurg. Psychiatry 1987, 50, 691–698. [Google Scholar] [CrossRef]
- Ebenbichler, G.R.; Kollmitzer, J.; Erim, Z.; Löscher, W.N.; Kerschan, K.; Posch, M.; Nowotny, T.; Kranzl, A.; Wöber, C.; Bochdansky, T. Load-dependence of fatigue related changes in tremor around 10 Hz. Clin. Neurophysiol. 2000, 111, 106–111. [Google Scholar] [CrossRef]
- Morrison, S.; Kavanagh, J.; Obst, S.; Irwin, J.; Haseler, L. The effects of unilateral muscle fatigue on bilateral physiological tremor. Exp. Brain Res. 2005, 167, 609–621. [Google Scholar] [CrossRef]
- Elble, R.J. Tremor. In Neuro-Geriatrics; Springer: Berlin/Heidelberg, Germany, 2017; pp. 311–326. [Google Scholar]
- Garcia, R.G.; Ballado, A.H.; Paglinawan, A.C.; Paglinawan, C.C.; Gavino, R.B.; Magcamit, B.A.J.; Miranda, J.C.S.; Tiongson, M.F. Hand tremor analyzer using accelerometry for preliminary diagnosis, classification and monitoring of selected movement disorders. In Proceedings of the 2016 6th IEEE International Conference on Control System, Computing and Engineering (ICCSCE), Penang, Malaysia, 25–27 November 2016; pp. 392–396. [Google Scholar]
- Perumal, S.V.; Sankar, R. Gait and tremor assessment for patients with Parkinson’s disease using wearable sensors. ICT Express 2016, 2, 168–174. [Google Scholar] [CrossRef]
- Liu, Z.; Luo, J.; Wang, L.; Zhang, Y.; Philip Chen, C.; Chen, X. A time-sequence-based fuzzy support vector machine adaptive filter for tremor cancelling for microsurgery. Int. J. Syst. Sci. 2015, 46, 1131–1146. [Google Scholar] [CrossRef]
- Jeon, H.; Lee, W.; Park, H.; Lee, H.J.; Kim, S.K.; Kim, H.B.; Jeon, B.; Park, K.S. High-accuracy automatic classification of Parkinsonian tremor severity using machine learning method. Physiol. Meas. 2017, 38, 1980. [Google Scholar] [CrossRef]
- Chandra, S.; Hayashibe, M.; Thondiyath, A. Muscle fatigue induced hand tremor clustering in dynamic laparoscopic manipulation. IEEE Trans. Syst. Man Cybern. Syst. 2018, 50, 5420–5431. [Google Scholar] [CrossRef]
- Yang, C.; Luo, J.; Pan, Y.; Liu, Z.; Su, C.-Y. Personalized variable gain control with tremor attenuation for robot teleoperation. IEEE Trans. Syst. Man Cybern. Syst. 2017, 48, 1759–1770. [Google Scholar] [CrossRef]
- Sandroni, P.; Young, R. Tremor: Classification, diagnosis and management. Am. Fam. Physician 1994, 50, 1505–1512. [Google Scholar]
- Abdulhay, E.; Arunkumar, N.; Narasimhan, K.; Vellaiappan, E.; Venkatraman, V. Gait and tremor investigation using machine learning techniques for the diagnosis of Parkinson disease. Future Gener. Comput. Syst. 2018, 83, 366–373. [Google Scholar] [CrossRef]
- Ataş, M. Hand tremor based biometric recognition using leap motion device. IEEE Access 2017, 5, 23320–23326. [Google Scholar] [CrossRef]
- Veluvolu, K.C.; Ang, W.T. Estimation of physiological tremor from accelerometers for real-time applications. Sensors 2011, 11, 3020–3036. [Google Scholar] [CrossRef]
- Pierleoni, P.; Palma, L.; Belli, A.; Pernini, L. A real-time system to aid clinical classification and quantification of tremor in Parkinson’s disease. In Proceedings of the IEEE-EMBS International Conference on Biomedical and Health Informatics (BHI), Valencia, Spain, 1–4 June 2014; pp. 113–116. [Google Scholar]
- Bazgir, O.; Habibi, S.A.H.; Palma, L.; Pierleoni, P.; Nafees, S. A classification system for assessment and home monitoring of tremor in patients with Parkinson’s disease. J. Med. Signals Sens. 2018, 8, 65. [Google Scholar] [CrossRef]
- Smaga, S. Tremor. Am. Fam. Physician 2003, 68, 1545–1552. [Google Scholar]
- McAuley, J.; Marsden, C. Physiological and pathological tremors and rhythmic central motor control. Brain 2000, 123, 1545–1567. [Google Scholar] [CrossRef]
- Kavanagh, J.J.; Cresswell, A.G.; Sabapathy, S.; Carroll, T.J. Bilateral tremor responses to unilateral loading and fatiguing muscle contractions. J. Neurophysiol. 2013, 110, 431–440. [Google Scholar] [CrossRef]
- Wang, L.; Huang, Z.; Hao, S.; Cheng, Y.; Yang, Y. A heterogeneous ensemble learning voting method for fatigue detection in daily activities. J. Adv. Comput. Intell. Intell. Inform. 2018, 22, 88–96. [Google Scholar] [CrossRef]
- Zhu, Y.; Mehta, R.K.; Erraguntla, M.; Sasangohar, F.; Qaraqe, K. Quantifying Accelerometer-based Tremor Features of Neuromuscular Fatigue in Healthy and Diabetic Adults. IEEE Sens. J. 2020, 20, 11183–11190. [Google Scholar] [CrossRef]
- Almeida, S.; Riddell, M.; Cafarelli, E. Slower conduction velocity and motor unit discharge frequency are associated with muscle fatigue during isometric exercise in type 1 diabetes mellitus. Muscle Nerve Off. J. Am. Assoc. Electrodiagn. Med. 2008, 37, 231–240. [Google Scholar] [CrossRef]
- Darnall, N.D.; Donovan, C.K.; Aktar, S.; Tseng, H.Y.; Barthelmess, P.; Cohen, P.R.; Lin, D.C. Application of machine learning and numerical analysis to classify tremor in patients affected with essential tremor or Parkinson’s disease. Gerontechnology 2012, 10, 208–219. [Google Scholar] [CrossRef]
- Zheng, X.; Vieira, A.; Marcos, S.L.; Aladro, Y.; Ordieres-Meré, J. Activity-aware essential tremor evaluation using deep learning method based on acceleration data. Parkinsonism Relat. Disord. 2019, 58, 17–22. [Google Scholar] [CrossRef]
- Kubota, K.J.; Chen, J.A.; Little, M.A. Machine learning for large-scale wearable sensor data in Parkinson’s disease: Concepts, promises, pitfalls, and futures. Mov. Disord. 2016, 31, 1314–1326. [Google Scholar] [CrossRef]
- Tatinati, S.; Veluvolu, K.C.; Ang, W.T. Multistep prediction of physiological tremor based on machine learning for robotics assisted microsurgery. IEEE Trans. Cybern. 2014, 45, 328–339. [Google Scholar] [CrossRef]
- Yao, L.; Brown, P.; Shoaran, M. Resting Tremor Detection in Parkinson’s Disease with Machine Learning and Kalman Filtering. In Proceedings of the 2018 IEEE Biomedical Circuits and Systems Conference (BioCAS), Cleveland, OH, USA, 17–19 October 2018; pp. 1–4. [Google Scholar]
- Cole, B.T.; Roy, S.H.; De Luca, C.J.; Nawab, S.H. Dynamic neural network detection of tremor and dyskinesia from wearable sensor data. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 6062–6065. [Google Scholar]
- Cole, B.T.; Roy, S.H.; De Luca, C.J.; Nawab, S.H. Dynamical learning and tracking of tremor and dyskinesia from wearable sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 982–991. [Google Scholar] [CrossRef]
- Kostikis, N.; Hristu-Varsakelis, D.; Arnaoutoglou, M.; Kotsavasiloglou, C. A smartphone-based tool for assessing parkinsonian hand tremor. IEEE J. Biomed. Health Inform. 2015, 19, 1835–1842. [Google Scholar] [CrossRef]
- Jeon, H.; Lee, W.; Park, H.; Lee, H.J.; Kim, S.K.; Kim, H.B.; Jeon, B.; Park, K.S. Automatic classification of tremor severity in Parkinson’s disease using a wearable device. Sensors 2017, 17, 2067. [Google Scholar] [CrossRef]
- Cherubini, A.; Nisticó, R.; Novellino, F.; Salsone, M.; Nigro, S.; Donzuso, G.; Quattrone, A. Magnetic resonance support vector machine discriminates essential tremor with rest tremor from tremor-dominant Parkinson disease. Mov. Disord. 2014, 29, 1216–1219. [Google Scholar] [CrossRef]
- Wile, D.J.; Ranawaya, R.; Kiss, Z.H. Smart watch accelerometry for analysis and diagnosis of tremor. J. Neurosci. Methods 2014, 230, 1–4. [Google Scholar] [CrossRef]
- Soran, B.; Hwang, J.; Lee, S.; Shapiro, L. Tremor detection using motion filtering and SVM. In Proceedings of the 21st International Conference on Pattern Recognition (ICPR2012), Tsukuba, Japan, 11–15 November 2012; pp. 178–181. [Google Scholar]
- Alam, M.N.; Johnson, B.; Gendreau, J.; Tavakolian, K.; Combs, C.; Fazel-Rezai, R. Tremor quantification of Parkinson‘s disease—A pilot study. In Proceedings of the 2016 IEEE International Conference on Electro Information Technology (EIT), Grand Forks, ND, USA, 19–21 May 2016; pp. 755–759. [Google Scholar]
- Dobrea, D.M.; Teodorescu, H.N. Classifying and assessing tremor movements for applications in man-machine intelligent user interfaces. In Proceedings of the 9th International Conference on Intelligent User Interfaces, Madeira, Portugal, 13–16 January 2004; pp. 238–240. [Google Scholar]
- Maman, Z.S.; Chen, Y.-J.; Baghdadi, A.; Lombardo, S.; Cavuoto, L.A.; Megahed, F.M. A data analytic framework for physical fatigue management using wearable sensors. Expert Syst. Appl. 2020, 155, 113405. [Google Scholar] [CrossRef]
- Strohrmann, C.; Rossi, M.; Arnrich, B.; Troster, G. A data-driven approach to kinematic analysis in running using wearable technology. In Proceedings of the 2012 Ninth International Conference on Wearable and Implantable Body Sensor Networks, London, UK, 9–12 May 2012; pp. 118–123. [Google Scholar]
- Karg, M.; Kühnlenz, K.; Buss, M.; Seiberl, W.; Tusker, F.; Schmeelk, M.; Schwirtz, A. Expression and automatic recognition of exhaustion in natural walking. In Proceedings of the IADIS International Conference on Interfaces and Human Computer Interaction (IHCI), Amsterdam, The Netherlands, 25–27 July 2008; pp. 165–172. [Google Scholar]
- Karg, M.; Venture, G.; Hoey, J.; Kulić, D. Human movement analysis as a measure for fatigue: A hidden Markov-based approach. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 470–481. [Google Scholar] [CrossRef]
- Gallego, J.A.; Rocon, E.; Ibañez, J.; Dideriksen, J.L.; Koutsou, A.; Paradiso, R.; Popovic, M.B.; Belda-Lois, J.M.; Gianfelici, F.; Farina, D. A soft wearable robot for tremor assessment and suppression. In Proceedings of the 2011 IEEE International Conference on Robotics and Automation, Shanghai, China, 9–13 May 2011; pp. 2249–2254. [Google Scholar]
- Duan, X.; Rhee, J.; Mehta, R.K.; Srinivasan, D. Neuromuscular control and performance differences associated with gender and obesity in fatiguing tasks performed by older adults. Front. Physiol. 2018, 9, 800. [Google Scholar] [CrossRef]
- Mehta, R.K.; Cavuoto, L.A. The effects of obesity, age, and relative workload levels on handgrip endurance. Appl. Ergon. 2015, 46, 91–95. [Google Scholar] [CrossRef]
- Mathworks. Available online: https://www.mathworks.com/help/stats/choose-a-classifier.html#bunt0n0-1 (accessed on 17 September 2019).
- Ai, L.; Wang, J.; Yao, R. Classification of parkinsonian and essential tremor using empirical mode decomposition and support vector machine. Digit. Signal Process. 2011, 21, 543–550. [Google Scholar] [CrossRef]
- Gul, A.; Perperoglou, A.; Khan, Z.; Mahmoud, O.; Miftahuddin, M.; Adler, W.; Lausen, B. Ensemble of a subset of kNN classifiers. Adv. Data Anal. Classif. 2018, 12, 827–840. [Google Scholar] [CrossRef]
- Zhang, Y.; Cao, G.; Wang, B.; Li, X. A novel ensemble method for k-nearest neighbor. Pattern Recognit. 2019, 85, 13–25. [Google Scholar] [CrossRef]
- Ho, T.K. Nearest neighbors in random subspaces. In Proceedings of the Joint IAPR International Workshops on Statistical Techniques in Pattern Recognition (SPR) and Structural and Syntactic Pattern Recognition (SSPR), Sydney, Australia, 11–13 August 1998; pp. 640–648. [Google Scholar]
- Louis, E.D.; Cubo, E.; Trejo-Gabriel-Galán, J.M.; Villaverde, V.A.; Benito, V.D.; Velasco, S.S.; Vicente, J.M.; Guevara, J.C.; Benito-León, J. Tremor in school-aged children: A cross-sectional study of tremor in 819 boys and girls in Burgos, Spain. Neuroepidemiology 2011, 37, 90–95. [Google Scholar] [CrossRef]
- Hubble, J.P. Gender Differences in Tremor. In Essential Tremor: What the Experts Say, 3rd ed.; IETF: Lenexa, KS, USA, 2014. [Google Scholar]
- Endo, H.; Kawahara, K. Gender differences in hand stability of normal young people assessed at low force levels. Ergonomics 2011, 54, 273–281. [Google Scholar] [CrossRef]
- Elble, R.J. Characteristics of physiologic tremor in young and elderly adults. Clin. Neurophysiol. 2003, 114, 624–635. [Google Scholar] [CrossRef]
- Raethjen, J.; Pawlas, F.; Lindemann, M.; Wenzelburger, R.; Deuschl, G. Determinants of physiologic tremor in a large normal population. Clin. Neurophysiol. 2000, 111, 1825–1837. [Google Scholar] [CrossRef]
- Griggs, S.; Morris, N.S. Fatigue among adults with type 1 diabetes mellitus and implications for self-management: An integrative review. Diabetes Educ. 2018, 44, 325–339. [Google Scholar] [CrossRef]
- Li, K.; Hogrel, J.-Y.; Duchêne, J.; Hewson, D.J. Analysis of fatigue and tremor during sustained maximal grip contractions using Hilbert-Huang Transformation. Med. Eng. Phys. 2012, 34, 832–840. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Algorithm | Samples/Window | |
|---|---|---|
| 45 | 90 | |
| DT | 90.0% (fine) | 90.5% (fine) |
| SVM | 92.4% (fine) | 93.3% (cubic) |
| k-NN | 93.2% (weight) | 94.2% (weight) |
| EC | 96.1% (subspace) | 95.5% (subspace) |
| Algorithm | Samples/Window | |
|---|---|---|
| 45 | 90 | |
| DT | 84.1% (fine) | 83.1% (fine) |
| SVM | 94.5% (fine Gaussian) | 91.8% (fine Gaussian) |
| k-NN | 96.0% (weight) | 94.2% (fine) |
| EC | 97.8% (subspace) | 97.9% (subspace) |
| 45 Samples/Window | 90 Samples/Window | |||||||||
| Accuracy, % | Recall, % | Spec., % | PPV, % | F1-Score, % | Accuracy, % | Recall, % | Spec., % | PPV, % | F1-Score, % | |
| All participants | ||||||||||
| DT | 79.89 | 83.72 | 76.08 | 77.71 | 80.61 | 82.52 | 91.35 | 73.69 | 77.64 | 83.94 |
| SVM | 94.39 | 90.65 | 98.12 | 97.96 | 94.16 | 93.06 | 89.37 | 96.75 | 96.50 | 92.80 |
| k-NN | 96.00 | 96.85 | 95.16 | 95.23 | 96.03 | 94.23 | 94.41 | 94.05 | 94.08 | 94.24 |
| EC | 97.71 | 98.02 | 97.40 | 97.41 | 97.71 | 97.39 | 97.66 | 97.12 | 97.13 | 97.40 |
| Healthy participants | ||||||||||
| DT | 89.73 | 93.32 | 86.16 | 87.02 | 90.06 | 87.73 | 87.36 | 88.10 | 88.01 | 87.69 |
| SVM | 95.47 | 96.47 | 94.46 | 94.55 | 95.50 | 96.10 | 97.02 | 95.17 | 95.26 | 96.13 |
| k-NN | 95.37 | 96.47 | 94.28 | 94.37 | 95.41 | 94.05 | 94.80 | 93.31 | 93.41 | 94.10 |
| EC | 97.39 | 98.14 | 97.60 | 97.60 | 97.87 | 97.40 | 98.14 | 96.65 | 96.70 | 97.42 |
| Diabetes patients | ||||||||||
| DT | 88.40 | 87.61 | 89.20 | 89.01 | 88.30 | 91.24 | 92.66 | 89.82 | 90.14 | 91.38 |
| SVM | 95.86 | 96.16 | 95.47 | 95.49 | 95.83 | 95.10 | 96.15 | 94.04 | 94.18 | 95.16 |
| k-NN | 95.12 | 94.94 | 95.30 | 95.27 | 95.11 | 95.62 | 97.20 | 94.04 | 94.24 | 95.70 |
| EC | 95.82 | 94.24 | 97.39 | 97.30 | 95.74 | 97.90 | 98.95 | 96.84 | 96.92 | 97.92 |
| Males | ||||||||||
| DT | 91.80 | 94.31 | 89.30 | 89.74 | 91.97 | 89.22 | 88.63 | 89.80 | 89.68 | 89.15 |
| SVM | 96.09 | 97.45 | 94.75 | 94.85 | 96.13 | 94.71 | 94.9 | 94.51 | 94.53 | 94.72 |
| k-NN | 95.61 | 97.25 | 93.97 | 94.12 | 95.66 | 95.10 | 96.47 | 93.73 | 93.89 | 95.16 |
| EC | 97.36 | 97.65 | 97.08 | 97.08 | 97.36 | 98.04 | 98.82 | 97.25 | 97.30 | 98.05 |
| Females | ||||||||||
| DT | 89.70 | 91.35 | 88.06 | 88.41 | 89.85 | 87.31 | 87.67 | 86.96 | 87.09 | 87.38 |
| SVM | 93.85 | 90.68 | 97.01 | 96.80 | 93.64 | 93.49 | 94.67 | 92.31 | 92.51 | 93.57 |
| k-NN | 94.85 | 94.51 | 95.19 | 95.14 | 94.82 | 96.49 | 95.33 | 97.66 | 97.61 | 96.46 |
| EC | 97.76 | 98.67 | 96.85 | 96.90 | 97.77 | 97.66 | 98.00 | 97.32 | 97.35 | 97.67 |
| ML Algorithm | Recognition | Sensor | Accuracy Performance | Reference |
| Voluntary effort recognition | ||||
| DT, SVM, k-NN, EC | Rest and effort events | Accelerometer | 90.0–96.1% | Table 1 |
| Naïve Bayesian k-NN SVM ANN | Rest, posture, and kinetic tremor | Accelerometer | 97% 87% 70% 91% | [25] |
| SVM | Rest tremor | Accelerometer+ Gyroscope | 88.6–88.9% | [44] |
| SVM DT k-NN DT | Rest tremor Rest tremor with mental stress Postural tremor Intention tremor | Accelerometer+ Gyroscope | 92.3% 86.2% 92.1% 89.2% | [17] |
| Fatigue stages recognition | ||||
| DT, SVM, k-NN, EC | Early and late fatigue phases | Accelerometer | 79.89–97.71% | Table 2 |
| Heterogenous EC | Fatigue stages | Accelerometer+ Gyroscope | 92% | [29] |
| Random forest SVM | Fatigue managing framework | Accelerometer+ Gyroscope | 89.7%; 87.9% 78.7%; 82% | [46] |
| SVM | Tired state Rest state | 3D-sensing device | 31.57% 85.71% | [45] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljihmani, L.; Kerdjidj, O.; Zhu, Y.; Mehta, R.K.; Erraguntla, M.; Sasangohar, F.; Qaraqe, K. Classification of Fatigue Phases in Healthy and Diabetic Adults Using Wearable Sensor. Sensors 2020, 20, 6897. https://doi.org/10.3390/s20236897
Aljihmani L, Kerdjidj O, Zhu Y, Mehta RK, Erraguntla M, Sasangohar F, Qaraqe K. Classification of Fatigue Phases in Healthy and Diabetic Adults Using Wearable Sensor. Sensors. 2020; 20(23):6897. https://doi.org/10.3390/s20236897
Chicago/Turabian StyleAljihmani, Lilia, Oussama Kerdjidj, Yibo Zhu, Ranjana K. Mehta, Madhav Erraguntla, Farzan Sasangohar, and Khalid Qaraqe. 2020. "Classification of Fatigue Phases in Healthy and Diabetic Adults Using Wearable Sensor" Sensors 20, no. 23: 6897. https://doi.org/10.3390/s20236897
APA StyleAljihmani, L., Kerdjidj, O., Zhu, Y., Mehta, R. K., Erraguntla, M., Sasangohar, F., & Qaraqe, K. (2020). Classification of Fatigue Phases in Healthy and Diabetic Adults Using Wearable Sensor. Sensors, 20(23), 6897. https://doi.org/10.3390/s20236897