A Review of the State of the Art in Non-Contact Sensing for COVID-19


 , , ,
, , ,  ,
, 
Abstract
1. Introduction
Search Strategy
2. Non-Contact Sensing to Detect COVID-19 Symptoms
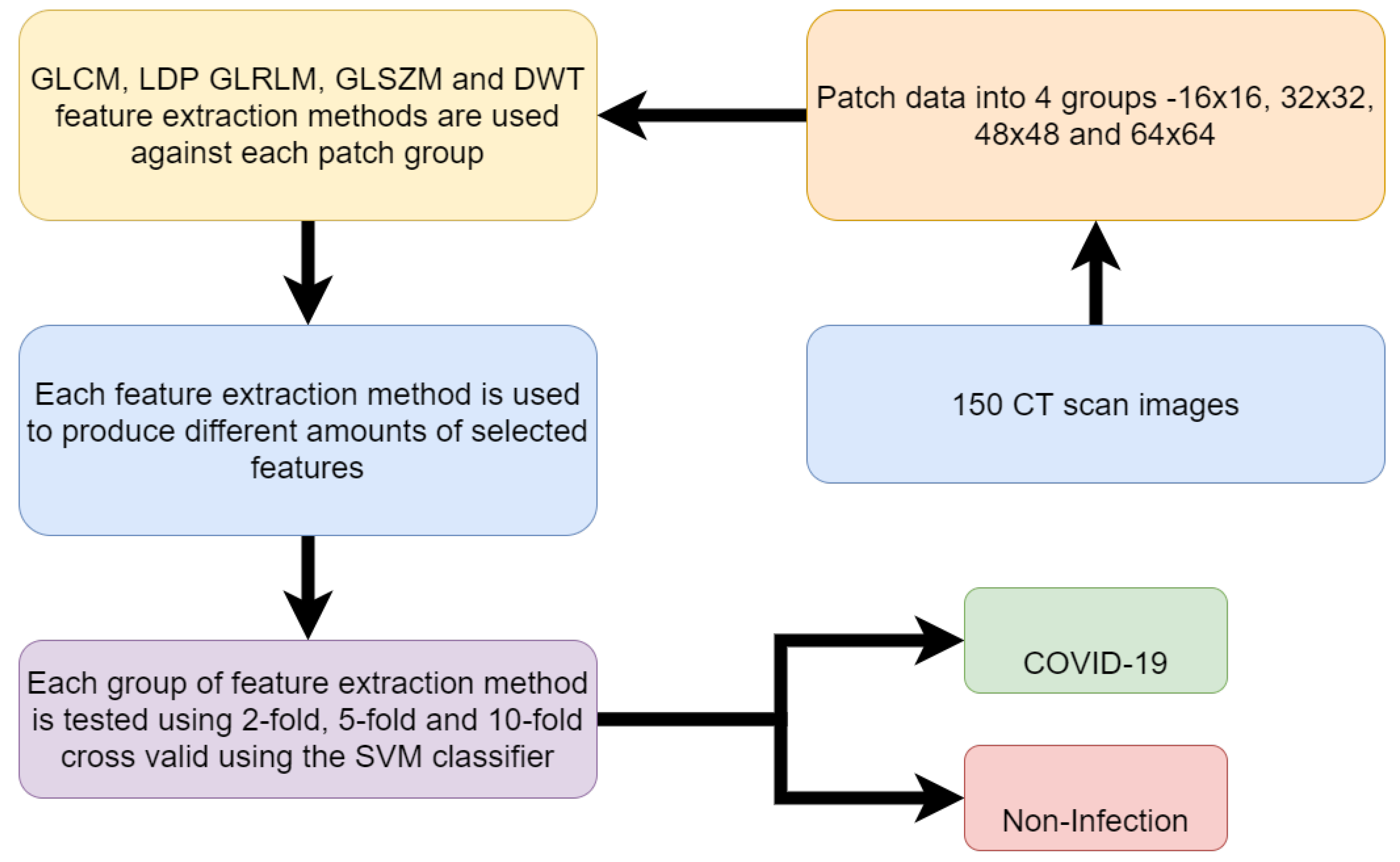
2.1. CT Scanning
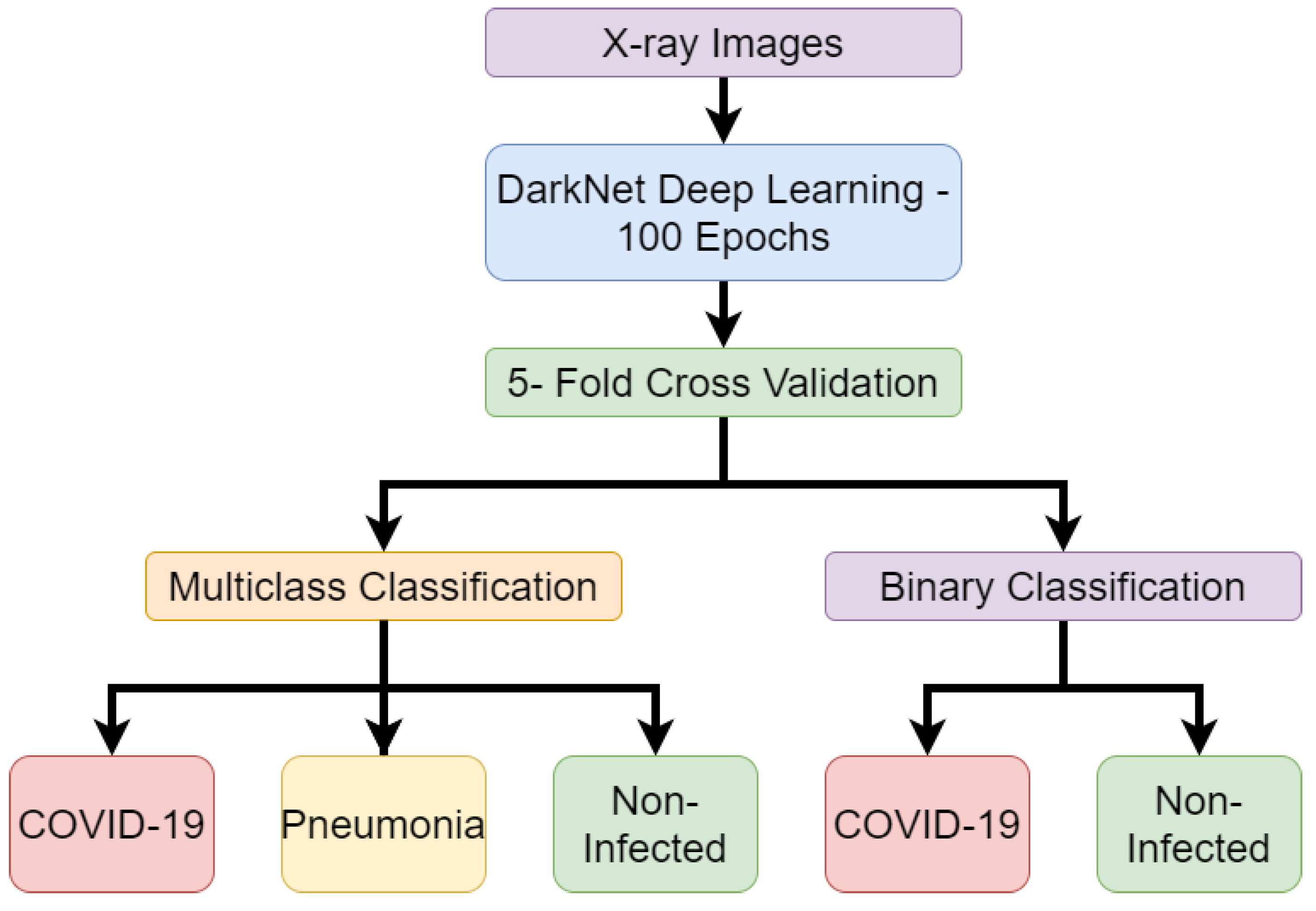
2.2. X-Ray Imaging
2.3. Camera Technology
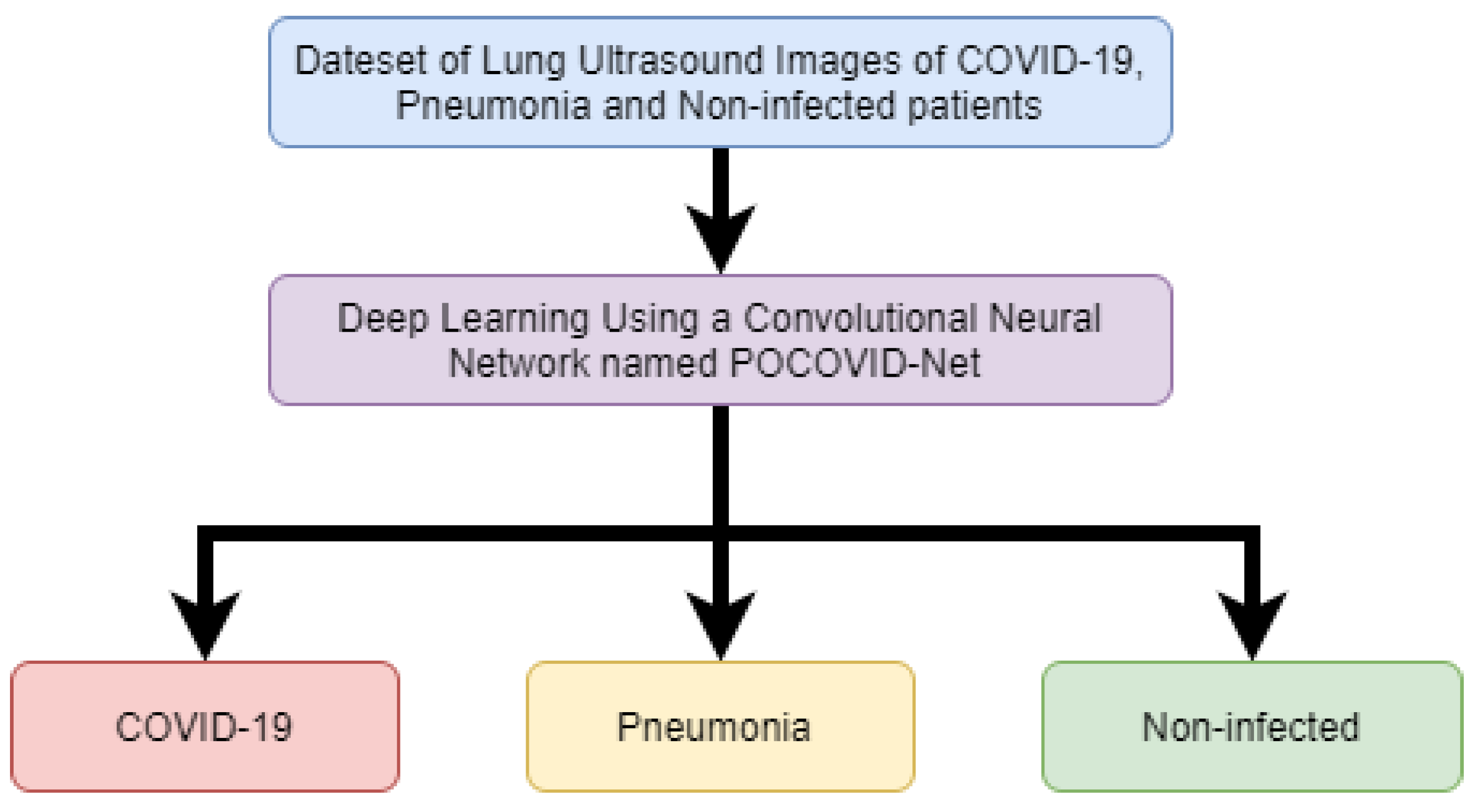
2.4. Ultrasound Technology
2.5. Radar Technology
2.6. Radio Frequency Signals
2.7. Thermography
2.8. Terahertz
2.9. Comparison to Contact Methods
2.10. Future Directions
- One of the biggest challenges with CT scanning to diagnose COVID-19 is the lack of portability. This means that although the method is non-contact, its use still requires individuals to travel to a location where the machine is available. As the CT images can provide high resolution, the AI can be used for the detection of COVID-19. Therefore, future directions of this method should look to creating highly accurate models that can eventually lead to the automation of COVID-19 detection. This can allow for faster diagnosis, which can allow for more patients to be tested and increase availability of staff operating and analyzing CT scans.
- X-rays, similarly to CT scans, are not portable. Like CT scans, professionals are required to operate these machines and analyze the X-ray images. The research presented in this paper has shown that AI can be used to make predictions if COVID-19 is present in the lungs. This can be useful similarly to CT scans where AI can be applied to make the predictions and speed up the process. The more data collected, the more advanced the model will become. Perhaps initially the predictions will need to be confirmed by humans but eventually the checks can become less frequent. Since the research above has displayed an ability of AI to distinguish between not just COVID-19 and non-infected but also pneumonia at high accuracy, then the AI has proved to be capable of accurate classifications.
- Thermal and depth cameras can detect the irregular breathing patterns that are associated with COVID-19 symptoms. The issue here is that even though the camera can detect the irregular breathing pattern, it is unable to categorically define COVID-19 as the cause for individuals displaying the irregular breathing patterns. In a real-life situation, the camera method may be better suited to monitoring vulnerable people who are considered high risk from COVID-19. Then once the monitoring system has identified the irregular breathing patterns, an alarm can be raised with a career or family member. Then, appropriate action can be taken for greater accuracy such as diagnosis with CT scanning or X-ray scanning.
- Ultrasound technology can take moving images of the lungs and detect COVID-19. This can also be made portable by using mobile devices. AI can be applied to recognize if COVID-19 or pneumonia is present in the lungs. This research can be further applied to develop applications on a mobile device that can capture an ultrasound of the lungs then compare it to an AI model to predict if COVID-19 is present. Although not all phones may not have the necessary hardware to achieve this, the non-contact method can allow for others to be able to use the devices for diagnosis at a safe distance.
- Radar technology can identify the breathing patterns of individuals. Much like camera technology, the identification of breathing patterns can raise cause of concern but it cannot isolate COVID-19 as the sole cause. Radar technology can again be used to monitor individuals but due to the high costs it is more likely to be used as a monitoring system within a hospital and not a home environment.
- Any future directions should consider the use of RF signals to detect the breathing patterns which give indication of COVID-19 symptoms. The RF systems can be implemented inexpensively using existing WiFi technology present within many homes. This allows for the monitoring of individuals without the costs incurred in implementing radar or camera technologies highlighted in this paper.
- Thermography has shown in previous research to be able to detect body temperatures of large amounts of people in previous pandemics. Therefore, it can be implemented in mass screening in the current COVID-19 pandemic. With the use of thermography being able to detect respiratory issues, it is clear that these systems can also be implemented for COVID-19 detection.
- Terahertz can provide deeper penetration and detect smaller movements such as the chest movements while breathing. This can therefore be used in early detection of COVID-19. The earlier the disease is detected, the sooner isolation can begin and ensure that further spread is reduced.
3. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singhal, T. A review of coronavirus disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C.; et al. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: A descriptive, cross-sectional, multicenter study. Am. J. Gastroenterol. 2020, 115. [Google Scholar] [CrossRef] [PubMed]
- Poyiadji, N.; Shahin, G.; Noujaim, D.; Stone, M.; Patel, S.; Griffith, B. COVID-19—Associated acute hemorrhagic necrotizing encephalopathy: CT and MRI features. Radiology 2020, 201187. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Wu, X.; Nethery, R.C.; Sabath, B.M.; Braun, D.; Dominici, F. Exposure to air pollution and COVID-19 mortality in the United States. medRxiv 2020. [Google Scholar] [CrossRef]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Sun, F.; et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, 488–496. [Google Scholar] [CrossRef]
- Jiang, S.; Xia, S.; Ying, T.; Lu, L. A novel coronavirus (2019-nCoV) causing pneumonia-associated respiratory syndrome. Cell. Mol. Immunol. 2020, 17, 554. [Google Scholar] [CrossRef]
- Khan, M.A.; Atangana, A. Modeling the dynamics of novel coronavirus (2019-nCov) with fractional derivative. Alex. Eng. J. 2020, 59, 2379–2389. [Google Scholar] [CrossRef]
- Nishiura, H.; Linton, N.M.; Akhmetzhanov, A.R. Initial cluster of novel coronavirus (2019-nCoV) infections in Wuhan, China is consistent with substantial human-to-human transmission. J. Clin. Med. 2020, 9, 488. [Google Scholar] [CrossRef]
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020, 24, 91–98. [Google Scholar] [CrossRef]
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 105924. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Jiang, J.Z.; Wan, X.F.; Hua, Y.; Li, L.; Zhou, J.; Wang, X.; Hou, F.; Chen, J.; Zou, J.; et al. Are pangolins the intermediate host of the 2019 novel coronavirus (SARS-CoV-2)? PLoS Pathog. 2020, 16, e1008421. [Google Scholar] [CrossRef]
- Xiao, K.; Zhai, J.; Feng, Y.; Zhou, N.; Zhang, X.; Zou, J.J.; Li, N.; Guo, Y.; Li, X.; Shen, X.; et al. Isolation and characterization of 2019-nCoV-like coronavirus from Malayan pangolins. BioRxiv 2020. [Google Scholar] [CrossRef]
- Novel, C.P.E.R.E. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua liu xing bing xue za zhi= Zhonghua liuxingbingxue zazhi 2020, 41, 145. [Google Scholar]
- Spinelli, A.; Pellino, G. COVID-19 pandemic: Perspectives on an unfolding crisis. Br. J. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Tang, Z.; Wang, S.; Hui, H.; Gong, L.; Lu, Y.; Xue, Z.; Liao, H.; Chen, F.; Yang, F.; et al. The role of imaging in the detection and management of COVID-19: A review. IEEE Rev. Biomed. Eng. 2020. [Google Scholar] [CrossRef]
- Cai, J.; Sun, W.; Huang, J.; Gamber, M.; Wu, J.; He, G. Indirect virus transmission in cluster of COVID-19 cases, Wenzhou, China, 2020. Emerg. Infect. Dis. 2020, 26. [Google Scholar] [CrossRef]
- Jones, N.R.; Qureshi, Z.U.; Temple, R.J.; Larwood, J.P.; Greenhalgh, T.; Bourouiba, L. Two metres or one: What is the evidence for physical distancing in covid-19? BMJ 2020, 370. [Google Scholar] [CrossRef]
- Schroter, R.C. Social distancing for covid-19: Is 2 metres far enough? BMJ 2020, 369. [Google Scholar] [CrossRef]
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 434–436. [Google Scholar] [CrossRef]
- Howard, J.; Huang, A.; Li, Z.; Tufekci, Z.; Zdimal, V.; van der Westhuizen, H.M.; von Delft, A.; Price, A.; Fridman, L.; Tang, L.H.; et al. Face masks against COVID-19: An evidence review. Gen. Med Res. 2020. [Google Scholar] [CrossRef]
- World Health Organization. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations: Scientific Brief, 27 March 2020; Technical Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Kooraki, S.; Hosseiny, M.; Myers, L.; Gholamrezanezhad, A. Coronavirus (COVID-19) outbreak: What the department of radiology should know. J. Am. Coll. Radiol. 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Dowd, J.B.; Andriano, L.; Brazel, D.M.; Rotondi, V.; Block, P.; Ding, X.; Liu, Y.; Mills, M.C. Demographic science aids in understanding the spread and fatality rates of COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 9696–9698. [Google Scholar] [CrossRef]
- Salathé, M.; Althaus, C.L.; Neher, R.; Stringhini, S.; Hodcroft, E.; Fellay, J.; Zwahlen, M.; Senti, G.; Battegay, M.; Wilder-Smith, A.; et al. COVID-19 epidemic in Switzerland: On the importance of testing, contact tracing and isolation. Swiss Med Wkly. 2020, 150, w20225. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Lo, N.C. Scientific and ethical basis for social-distancing interventions against COVID-19. Lancet. Infect. Dis. 2020, 20, 631. [Google Scholar] [CrossRef]
- Willan, J.; King, A.J.; Jeffery, K.; Bienz, N. Challenges for NHS hospitals during COVID-19 epidemic. BMJ 2020, 368, m1117. [Google Scholar] [CrossRef]
- Yang, X.; Ren, X.; Chen, M.; Wang, L.; Ding, Y. Human Posture Recognition in Intelligent Healthcare. In Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2020; Volume 1437, p. 012014. [Google Scholar]
- Abbasi, Q.H.; Rehman, M.U.; Qaraqe, K.; Alomainy, A. Advances in Body-Centric Wireless Communication: Applications and State-of-the-Art; Institution of Engineering and Technology: Stevenage, UK, 2016. [Google Scholar]
- Taylor, W.; Shah, S.A.; Dashtipour, K.; Zahid, A.; Abbasi, Q.H.; Imran, M.A. An intelligent non-invasive real-time human activity recognition system for next-generation healthcare. Sensors 2020, 20, 2653. [Google Scholar] [CrossRef]
- Tan, B.; Chen, Q.; Chetty, K.; Woodbridge, K.; Li, W.; Piechocki, R. Exploiting WiFi channel state information for residential healthcare informatics. IEEE Commun. Mag. 2018, 56, 130–137. [Google Scholar] [CrossRef]
- Marini, J.J.; Gattinoni, L. Management of COVID-19 respiratory distress. JAMA 2020, 323, 2329–2330. [Google Scholar] [CrossRef]
- Fan, D.; Ren, A.; Zhao, N.; Yang, X.; Zhang, Z.; Shah, S.A.; Hu, F.; Abbasi, Q.H. Breathing rhythm analysis in body centric networks. IEEE Access 2018, 6, 32507–32513. [Google Scholar] [CrossRef]
- Your Coronavirus Test Result. Available online: https://www.nhs.uk/conditions/coronavirus-covid-19/testing-and-tracing/what-your-test-result-means/ (accessed on 23 September 2020).
- Wang, Y.; Hu, M.; Li, Q.; Zhang, X.P.; Zhai, G.; Yao, N. Abnormal respiratory patterns classifier may contribute to large-scale screening of people infected with COVID-19 in an accurate and unobtrusive manner. arXiv 2020, arXiv:2002.05534. [Google Scholar]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Artificial intelligence distinguishes COVID-19 from community acquired pneumonia on chest CT. Radiology 2020, 200905. [Google Scholar] [CrossRef] [PubMed]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks. arXiv 2020, arXiv:2003.10849. [Google Scholar]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 103792. [Google Scholar] [CrossRef]
- Islam, S.M. Can Radar Remote Life Sensing Technology Help to Combat COVID-19? TechRxiv. Preprint 2020. [Google Scholar] [CrossRef]
- Jiang, Z.; Hu, M.; Fan, L.; Pan, Y.; Tang, W.; Zhai, G.; Lu, Y. Combining visible light and infrared imaging for efficient detection of respiratory infections such as COVID-19 on portable device. arXiv 2020, arXiv:2004.06912. [Google Scholar]
- Barstugan, M.; Ozkaya, U.; Ozturk, S. Coronavirus (covid-19) classification using ct images by machine learning methods. arXiv 2020, arXiv:2003.09424. [Google Scholar]
- CSAIL Device Lets Doctors Monitor COVID-19 Patients from a Distance. Available online: https://www.csail.mit.edu/news/csail-device-lets-doctors-monitor-covid-19-patients-distance (accessed on 23 September 2020).
- Zhang, J.; Xie, Y.; Li, Y.; Shen, C.; Xia, Y. COVID-19 screening on chest X-ray images using deep learning based anomaly detection. arXiv 2020, arXiv:2003.12338. [Google Scholar]
- Shan, F.; Gao, Y.; Wang, J.; Shi, W.; Shi, N.; Han, M.; Xue, Z.; Shi, Y. Lung infection quantification of covid-19 in ct images with deep learning. arXiv 2020, arXiv:2003.04655. [Google Scholar]
- Born, J.; Brändle, G.; Cossio, M.; Disdier, M.; Goulet, J.; Roulin, J.; Wiedemann, N. POCOVID-Net: Automatic detection of COVID-19 from a new lung ultrasound imaging dataset (POCUS). arXiv 2020, arXiv:2004.12084. [Google Scholar]
- Yang, W.; Sirajuddin, A.; Zhang, X.; Liu, G.; Teng, Z.; Zhao, S.; Lu, M. The role of imaging in 2019 novel coronavirus pneumonia (COVID-19). Eur. Radiol. 2020, 1–9. [Google Scholar] [CrossRef]
- Udugama, B.; Kadhiresan, P.; Kozlowski, H.N.; Malekjahani, A.; Osborne, M.; Li, V.Y.; Chen, H.; Mubareka, S.; Gubbay, J.B.; Chan, W.C. Diagnosing COVID-19: The disease and tools for detection. ACS Nano 2020, 14, 3822–3835. [Google Scholar] [CrossRef] [PubMed]
- Ceniccola, G.D.; Castro, M.G.; Piovacari, S.M.F.; Horie, L.M.; Corrêa, F.G.; Barrere, A.P.N.; Toledo, D.O. Current technologies in body composition assessment: Advantages and disadvantages. Nutrition 2019, 62, 25–31. [Google Scholar] [CrossRef]
- Brenner, D.J. Radiation risks potentially associated with low-dose CT screening of adult smokers for lung cancer. Radiology 2004, 231, 440–445. [Google Scholar] [CrossRef]
- Shi, F.; Wang, J.; Shi, J.; Wu, Z.; Wang, Q.; Tang, Z.; He, K.; Shi, Y.; Shen, D. Review of artificial intelligence techniques in imaging data acquisition, segmentation and diagnosis for COVID-19. IEEE Rev. Biomed. Eng. 2020. [Google Scholar] [CrossRef]
- Sethy, P.K.; Behera, S.K. Detection of coronavirus disease (COVID-19) based on deep features. Preprints 2020, 2020030300, 2020. [Google Scholar]
- Wang, L.; Wong, A. COVID-Net: A Tailored Deep Convolutional Neural Network Design for Detection of COVID-19 Cases from Chest X-Ray Images. arXiv 2020, arXiv:2003.09871. [Google Scholar]
- Ghoshal, B.; Tucker, A. Estimating uncertainty and interpretability in deep learning for coronavirus (COVID-19) detection. arXiv 2020, arXiv:2003.10769. [Google Scholar]
- Nam, Y.; Kong, Y.; Reyes, B.; Reljin, N.; Chon, K.H. Monitoring of heart and breathing rates using dual cameras on a smartphone. PLoS ONE 2016, 11, e0151013. [Google Scholar] [CrossRef]
- Bhattacharya, A.; Vaughan, R. Deep learning radar design for breathing and fall detection. IEEE Sensors J. 2020, 20, 5072–5085. [Google Scholar] [CrossRef]
- Elphick, H.E.; Alkali, A.H.; Kingshott, R.K.; Burke, D.; Saatchi, R. Exploratory study to evaluate respiratory rate using a thermal imaging camera. Respiration 2019, 97, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Powles, A.E.; Martin, D.J.; Wells, I.T.; Goodwin, C.R. Physics of ultrasound. Anaesth. Intensive Care Med. 2018, 19, 202–205. [Google Scholar] [CrossRef]
- Mojoli, F.; Bouhemad, B.; Mongodi, S.; Lichtenstein, D. Lung ultrasound for critically ill patients. Am. J. Respir. Crit. Care Med. 2019, 199, 701–714. [Google Scholar] [CrossRef]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Is there a role for lung ultrasound during the COVID-19 pandemic? J. Ultrasound Med. 2020. [Google Scholar] [CrossRef]
- Buonsenso, D.; Pata, D.; Chiaretti, A. COVID-19 outbreak: Less stethoscope, more ultrasound. Lancet Respir. Med. 2020, 8, e27. [Google Scholar] [CrossRef]
- Arlotto, P.; Grimaldi, M.; Naeck, R.; Ginoux, J.M. An ultrasonic contactless sensor for breathing monitoring. Sensors 2014, 14, 15371–15386. [Google Scholar] [CrossRef]
- Al-Naji, A.; Al-Askery, A.J.; Gharghan, S.K.; Chahl, J. A system for monitoring breathing activity using an ultrasonic radar detection with low power consumption. J. Sens. Actuator Netw. 2019, 8, 32. [Google Scholar] [CrossRef]
- Wang, T.; Zhang, D.; Wang, L.; Zheng, Y.; Gu, T.; Dorizzi, B.; Zhou, X. Contactless respiration monitoring using ultrasound signal with off-the-shelf audio devices. IEEE Internet Things J. 2018, 6, 2959–2973. [Google Scholar] [CrossRef]
- Kim, K.C.; Kim, M.J.; Joo, H.S.; Lee, W.; Yoon, C.; Song, T.K.; Yoo, Y. Smartphone-based portable ultrasound imaging system: A primary result. In Proceedings of the 2013 IEEE International Ultrasonics Symposium (IUS), Prague, Czech Republic, 21–25 July 2013; pp. 2061–2063. [Google Scholar]
- Genc, A.; Ryk, M.; Suwała, M.; Żurakowska, T.; Kosiak, W. Ultrasound imaging in the general practitioner’s office–A literature review. J. Ultrason. 2016, 16, 78. [Google Scholar] [CrossRef]
- Ding, C.; Zou, Y.; Sun, L.; Hong, H.; Zhu, X.; Li, C. Fall detection with multi-domain features by a portable FMCW radar. In Proceedings of the 2019 IEEE MTT-S International Wireless Symposium (IWS), Guangzhou, China, 19–22 May 2019; pp. 1–3. [Google Scholar]
- Shah, S.A.; Yang, X.; Abbasi, Q.H. Cognitive health care system and its application in pill-rolling assessment. Int. J. Numer. Model. Electron. Netw. Devices Fields 2019, 32, e2632. [Google Scholar] [CrossRef]
- Yang, X.; Fan, D.; Ren, A.; Zhao, N.; Shah, S.A.; Alomainy, A.; Ur-Rehman, M.; Abbasi, Q.H. Diagnosis of the Hypopnea syndrome in the early stage. Neural Comput. Appl. 2020, 32, 855–866. [Google Scholar] [CrossRef]
- Shah, S.A.; Tahir, A.; Ahmad, J.; Zahid, A.; Parvez, H.; Shah, S.Y.; Ashleibta, A.M.A.; Hasanali, A.; Khattak, S.; Abbasi, Q.H. Sensor fusion for identification of freezing of gait episodes using Wi-Fi and radar imaging. IEEE Sensors J. 2020. [Google Scholar] [CrossRef]
- Fioranelli, F.; Shah, S.A.; Li, H.; Shrestha, A.; Yang, S.; Le Kernec, J. Radar sensing for healthcare. Electron. Lett. 2019, 55, 1022–1024. [Google Scholar] [CrossRef]
- Gennarelli, G.; Ludeno, G.; Soldovieri, F. Real-time through-wall situation awareness using a microwave Doppler radar sensor. Remote. Sens. 2016, 8, 621. [Google Scholar] [CrossRef]
- Yang, X.; Shah, S.A.; Ren, A.; Fan, D.; Zhao, N.; Cao, D.; Hu, F.; Rehman, M.U.; Wang, W.; Von Deneen, K.M.; et al. Detection of essential tremor at the s-band. IEEE J. Transl. Eng. Health Med. 2018, 6, 1–7. [Google Scholar] [CrossRef]
- Alizadeh, M.; Shaker, G.; De Almeida, J.C.M.; Morita, P.P.; Safavi-Naeini, S. Remote monitoring of human vital signs using mm-Wave FMCW radar. IEEE Access 2019, 7, 54958–54968. [Google Scholar] [CrossRef]
- Fioranelli, F.; Le Kernec, J.; Shah, S.A. Radar for health care: Recognizing human activities and monitoring vital signs. IEEE Potentials 2019, 38, 16–23. [Google Scholar] [CrossRef]
- Shah, S.A.; Fioranelli, F. Human activity recognition: Preliminary results for dataset portability using FMCW radar. In Proceedings of the 2019 International Radar Conference (RADAR), Toulon, France, 23–27 September 2019. [Google Scholar]
- Kim, S.H.; Han, G.T. 1D CNN based human respiration pattern recognition using ultra wideband radar. In Proceedings of the 2019 International Conference on Artificial Intelligence in Information and Communication (ICAIIC), Jeju Island, Korea, 11–13 February 2019; pp. 411–414. [Google Scholar]
- Christenson, P.D.; Yang, C.X.; Kaabouch, N. A low cost through-wall radar for vital signs monitoring. In Proceedings of the 2019 IEEE International Conference on Electro Information Technology (EIT), Brookings, SD, USA, 31 July–1 August 2019; pp. 567–571. [Google Scholar]
- Liu, J.; Chen, Y.; Wang, Y.; Chen, X.; Cheng, J.; Yang, J. Monitoring vital signs and postures during sleep using WiFi signals. IEEE Internet Things J. 2018, 5, 2071–2084. [Google Scholar] [CrossRef]
- Dong, B.; Ren, A.; Shah, S.A.; Hu, F.; Zhao, N.; Yang, X.; Haider, D.; Zhang, Z.; Zhao, W.; Abbasi, Q.H. Monitoring of atopic dermatitis using leaky coaxial cable. Healthc. Technol. Lett. 2017, 4, 244–248. [Google Scholar] [CrossRef]
- Haider, D.; Ren, A.; Fan, D.; Zhao, N.; Yang, X.; Tanoli, S.A.K.; Zhang, Z.; Hu, F.; Shah, S.A.; Abbasi, Q.H. Utilizing a 5G spectrum for health care to detect the tremors and breathing activity for multiple sclerosis. Trans. Emerg. Telecommun. Technol. 2018, 29, e3454. [Google Scholar] [CrossRef]
- Yang, X.; Shah, S.A.; Ren, A.; Zhao, N.; Zhao, J.; Hu, F.; Zhang, Z.; Zhao, W.; Rehman, M.U.; Alomainy, A. Monitoring of patients suffering from REM sleep behavior disorder. IEEE J. Electromagn. Microwaves Med. Biol. 2018, 2, 138–143. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Y.; Chen, Y.; Yang, J.; Chen, X.; Cheng, J. Tracking vital signs during sleep leveraging off-the-shelf WiFi. In Proceedings of the 16th ACM International Symposium on Mobile Ad Hoc Networking and Computing, Hangzhou, China, 7–12 June 2015; pp. 267–276. [Google Scholar]
- Zhao, J.; Liu, L.; Wei, Z.; Zhang, C.; Wang, W.; Fan, Y. R-DEHM: CSI-based robust duration estimation of human motion with WiFi. Sensors 2019, 19, 1421. [Google Scholar] [CrossRef] [PubMed]
- Chopra, N.; Yang, K.; Abbasi, Q.H.; Qaraqe, K.A.; Philpott, M.; Alomainy, A. THz time-domain spectroscopy of human skin tissue for in-body nanonetworks. IEEE Trans. Terahertz Sci. Technol. 2016, 6, 803–809. [Google Scholar] [CrossRef]
- Shah, S.A.; Fioranelli, F. RF sensing technologies for assisted daily living in healthcare: A comprehensive review. IEEE Aerosp. Electron. Syst. Mag. 2019, 34, 26–44. [Google Scholar] [CrossRef]
- Zeng, Y.; Wu, D.; Xiong, J.; Yi, E.; Gao, R.; Zhang, D. FarSense: Pushing the range limit of WiFi-based respiration sensing with CSI ratio of two antennas. Proc. Acm Interactive Mobile, Wearable Ubiquitous Technol. 2019, 3, 1–26. [Google Scholar] [CrossRef]
- Rocamora, J.; Ho, I.W.H.; Mak, M.W.; Lau, A. Survey of CSI fingerprinting-based indoor positioning and mobility tracking systems. IET Signal Process. 2020. [Google Scholar] [CrossRef]
- Al-qaness, M.A.; Abd Elaziz, M.; Kim, S.; Ewees, A.A.; Abbasi, A.A.; Alhaj, Y.A.; Hawbani, A. Channel state information from pure communication to sense and track human motion: A survey. Sensors 2019, 19, 3329. [Google Scholar] [CrossRef]
- Ekici, S.; Jawzal, H. Breast cancer diagnosis using thermography and convolutional neural networks. Med. Hypotheses 2020, 137, 109542. [Google Scholar] [CrossRef]
- Liu, X.; Tian, G.; Chen, Y.; Luo, H.; Zhang, J.; Li, W. Non-contact degradation evaluation for IGBT modules using eddy current pulsed thermography approach. Energies 2020, 13, 2613. [Google Scholar] [CrossRef]
- Silvino, V.O.; Gomes, R.B.B.; Ribeiro, S.L.G.; de Lima Moreira, D.; dos Santos, M.A.P. Identifying febrile humans using infrared thermography screening: Possible applications during COVID-19 outbreak. Rev. Contexto SaÚDe 2020, 20, 5–9. [Google Scholar] [CrossRef]
- Silva, T.A.E.D.; Silva, L.F.D.; Muchaluat-Saade, D.C.; Conci, A. A computational method to assist the diagnosis of breast disease using dynamic thermography. Sensors 2020, 20, 3866. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Wu, J.; Hong, L.; Luo, Y.; Song, Q.; Chen, D. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: An observational cohort study. Lancet Infect. Dis. 2020, 20, 689–696. [Google Scholar] [CrossRef]
- Chen, J.; Qi, T.; Liu, L.; Ling, Y.; Qian, Z.; Li, T.; Li, F.; Xu, Q.; Zhang, Y.; Xu, S.; et al. Clinical progression of patients with COVID-19 in Shanghai, China. J. Infect. 2020, 80. [Google Scholar] [CrossRef]
- Jagadev, P.; Giri, L.I. Non-contact monitoring of human respiration using infrared thermography and machine learning. Infrared Phys. Technol. 2020, 104, 103117. [Google Scholar] [CrossRef]
- Ulhaq, A.; Khan, A.; Gomes, D.; Pau, M. Computer vision for COVID-19 Control: A survey. arXiv 2020, arXiv:2004.09420. [Google Scholar]
- Farooq, M.A.; Corcoran, P. Infrared imaging for human thermography and breast tumor classification using thermal images. In Proceedings of the 2020 31st Irish Signals and Systems Conference (ISSC), Maynooth, Ireland, 17–18 June 2020; pp. 1–6. [Google Scholar]
- Rodriguez-Lozano, F.J.; León-García, F.; Ruiz de Adana, M.; Palomares, J.M.; Olivares, J. Non-invasive forehead segmentation in thermographic imaging. Sensors 2019, 19, 4096. [Google Scholar] [CrossRef]
- Rong, Y.; Theofanopoulos, P.C.; Trichopoulos, G.C.; Bliss, D.W. Cardiac sensing exploiting an ultra-wideband terahertz sensing system. In Proceedings of the 2020 IEEE International Radar Conference (RADAR), Basel, Switzerland, 27 April 27–1 May 2020; pp. 1002–1006. [Google Scholar]
- Matsumoto, H.; Watanabe, I.; Kasamatsu, A.; Monnai, Y. Integrated terahertz radar based on leaky-wave coherence tomography. Nat. Electron. 2020, 3, 122–129. [Google Scholar] [CrossRef]
- Tao, Y.H.; Fitzgerald, A.J.; Wallace, V.P. Non-contact, non-destructive testing in various industrial sectors with terahertz technology. Sensors 2020, 20, 712. [Google Scholar] [CrossRef]
- Petkie, D.T.; Bryan, E.; Benton, C.; Phelps, C.; Yoakum, J.; Rogers, M.; Reed, A. Remote respiration and heart rate monitoring with millimeter-wave/terahertz radars. In Proceedings of the Millimetre Wave and Terahertz Sensors and Technology, Cardiff, UK, 17–18 September 2008; p. 71170I. [Google Scholar]
- Yan, W.; Chen, D.; Kong, F.; Bai, X. FDTD simulation of terahertz wave propagation in time-varying plasma. In Proceedings of the 2019 Photonics & Electromagnetics Research Symposium-Fall (PIERS-Fall), Xiamen, China, 17–20 December 2019; pp. 699–701. [Google Scholar]
- Saeed, N.; Loukil, M.H.; Sarieddeen, H.; Al-Naffouri, T.Y.; Alouini, M.S. Body-Centric Terahertz Networks: Prospects and Challenges. Available online: https://www.techrxiv.org/articles/preprint/Body-Centric_Terahertz_Networks_Prospects_and_Challenges/12923498 (accessed on 23 September 2020).
- Punia, S.; Malik, H.K. THz radiation generation in axially magnetized collisional pair plasma. Phys. Lett. A 2019, 383, 1772–1777. [Google Scholar] [CrossRef]
- Rothbart, N.; Holz, O.; Koczulla, R.; Schmalz, K.; Hübers, H.W. Analysis of human breath by millimeter-wave/terahertz spectroscopy. Sensors 2019, 19, 2719. [Google Scholar] [CrossRef] [PubMed]
- Dinh-Le, C.; Chuang, R.; Chokshi, S.; Mann, D. Wearable health technology and electronic health record integration: Scoping review and future directions. JMIR Mhealth Uhealth 2019, 7, e12861. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.J.; Song, W.Z.; Wang, X.X.; Zhang, J.; Fan, Z.; Yu, M.; Ramakrishna, S.; Long, Y.Z. A calibration-free self-powered sensor for vital sign monitoring and finger tap communication based on wearable triboelectric nanogenerator. Nano Energy 2019, 58, 536–542. [Google Scholar] [CrossRef]
- Jeong, H.; Rogers, J.A.; Xu, S. Continuous on-body sensing for the COVID-19 pandemic: Gaps and opportunities. Sci. Adv. 2020, 6, eabd4794. [Google Scholar] [CrossRef]
- Kapoor, A.; Guha, S.; Das, M.K.; Goswami, K.C.; Yadav, R. Digital healthcare: The only solution for better healthcare during COVID-19 pandemic? Indian Heart J. 2020, 72, 61–64. [Google Scholar] [CrossRef]
- Seshadri, D.R.; Davies, E.V.; Harlow, E.R.; Hsu, J.J.; Knighton, S.C.; Walker, T.A.; Voos, J.E.; Drummond, C.K. Wearable sensors for COVID-19: A call to action to harness our digital infrastructure for remote patient monitoring and virtual assessments. Front. Digit. Health 2020, 2, 8. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Accuracy | Cost | Time for Measurement | Time for Results | Harm to Body | Skills of Operators | Possibility of AI |
|---|---|---|---|---|---|---|---|
| CT | High | High | Moderate | Fast | Low | High | Yes |
| X-Ray | High | High | Moderate | Fast | Low | High | Yes |
| Camera | High | Medium | Real Time | Real Time | None | Medium | Yes |
| Ultrasound | High | Medium/High | Moderate | Medium | Low | High | Yes |
| Radar | High | High | Real Time | Real Time | None | Medium | Yes |
| RF | High | Low | Real Time | Real Time | None | Low | Yes |
| IR Thermo | High | Medium | Fast | Fast | None | High | Yes |
| THz | High | Medium | Fast | Fast | None | High | Yes |
| Title of Paper | Citation | Year | Key Themes | Authority |
|---|---|---|---|---|
| Abnormal respiratory patterns classifier may contribute to large-scale screening of people infected with COVID-19 in an accurate and unobtrusive manner | [36] | 2020 | The paper details that COVID-19 patients display tachypnea (Rapid breathing). The paper looks at taking depth images to identify the breathing patterns of volunteers using deep learning | Peer reviewed paper. 24 citations on Google Scholar. |
| Artificial intelligence distinguishes COVID-19 from community acquired pneumonia on chest CT | [37] | 2020 | CT scan images are used in a COVNet neural network to distinguish between COVID-19, Pneumonia and Non-infected scan images. | Peer reviewed paper. 157 citations on Google Scholar. |
| Automatic detection of coronavirus disease (COVID-19) using x-ray images and deep convolutional neural networks | [38] | 2020 | X-ray scan images are used in a ResNet-50 Convolutional Neural Network (CNN) to distinguish between COVID-19 and non-infected scan images. | Peer reviewed paper. 102 citations on Google Scholar. |
| Automated detection of COVID-19 cases using deep neural networks with X-ray images | [39] | 2020 | X-ray images are processed using the DarkNet neural network to test binary classification between COVID and Non-infected and multi-class classification between COVID, Pneumonia and Non-infected. | Peer reviewed paper. 22 citations on Google Scholar. |
| Can Radar Remote Life Sensing Technology Help to Combat COVID-19? | [40] | 2020 | Radar systems have been used to monitor the vital signs of patients in a contact less manner to protect healthcare workers | Paper uploaded on researchgate.net. |
| Combining Visible Light and Infrared Imaging for Efficient Detection of Respiratory Infections such as COVID-19 on Portable Device | [41] | 2020 | RGB-Terminal camera footage used in a BiGRU neural network model between healthy and ill. | Peer reviewed paper. |
| Coronavirus (COVID-19) classification using CT images by machine-learning methods | [42] | 2020 | CT scan images are used to experiment with various methods of feature extraction and deep learning algorithms to achieve the best results | Peer reviewed paper. 157 citations on Google Scholar. 157 citations on Google Scholar. |
| CSAIL device lets doctors monitor COVID-19 patients from a distance | [43] | 2020 | Radio Frequencies have been used to monitor the vital signs of patients in a contactless manner to protect healthcare workers | Article found on MIT Computer Science & Artificial Intelligence Laboratory website. |
| Covid-19 screening on chest x-ray images using deep-learning-based anomaly detection | [44] | 2020 | X-ray images are used with deep learning to identify if samples are COVID-19 or Pneumonia | Peer reviewed paper. 32 citations on Google Scholar. |
| Lung infection quantification of COVID-19 in CT images with deep learning | [45] | 2020 | CT scan images are used in deep learning to identify COVID-19. Human-in-the-loop technique is used to focus on increasing accuracy | Peer reviewed paper. 52 citations on Google Scholar. |
| POCOVID-Net: automatic detection of COVID-19 from a new lung ultrasound imaging data set (POCUS) | [46] | 2020 | Lung Ultrasound videos of COVID-19, Pneumonia and non-infected patients used deep learning for classification. | Peer reviewed paper. 2 citations on Google Scholar. |
| Citation | Training Data | Algorithms | Results |
|---|---|---|---|
| [45] | 249 CT images of COVID-19 showing different levels of infection. | Custom Convolutional neural network (CNN) called “VB-Net” | 91.6% Accuracy |
| [37] | 400 COVID-19 CT images, 1396 Pneumonia CT images and 1173 non-infected CT images | Custom Convolutional neural network (CNN) called “COVNet” | 90% sensitivity of COVID-19 samples. |
| [42] | 150 CT images including 53 COVID-19 cases. | Support Vector Machine | 99.64% Accuracy |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, W.; Abbasi, Q.H.; Dashtipour, K.; Ansari, S.; Shah, S.A.; Khalid, A.; Imran, M.A. A Review of the State of the Art in Non-Contact Sensing for COVID-19. Sensors 2020, 20, 5665. https://doi.org/10.3390/s20195665
Taylor W, Abbasi QH, Dashtipour K, Ansari S, Shah SA, Khalid A, Imran MA. A Review of the State of the Art in Non-Contact Sensing for COVID-19. Sensors. 2020; 20(19):5665. https://doi.org/10.3390/s20195665
Chicago/Turabian StyleTaylor, William, Qammer H. Abbasi, Kia Dashtipour, Shuja Ansari, Syed Aziz Shah, Arslan Khalid, and Muhammad Ali Imran. 2020. "A Review of the State of the Art in Non-Contact Sensing for COVID-19" Sensors 20, no. 19: 5665. https://doi.org/10.3390/s20195665
APA StyleTaylor, W., Abbasi, Q. H., Dashtipour, K., Ansari, S., Shah, S. A., Khalid, A., & Imran, M. A. (2020). A Review of the State of the Art in Non-Contact Sensing for COVID-19. Sensors, 20(19), 5665. https://doi.org/10.3390/s20195665