
A Systematic Review on Processed/Ultra-Processed Foods and Arterial Hypertension in Adults and Older People

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy/Inclusion and Exclusion Criteria
- -
- PubMed: (“ultra-processed food” OR “ultra-processed foods” OR “ultraprocessed food” OR “ultraprocessed foods” OR “ultra-processed product” OR “ultra-processed products” OR “ultra-processing” OR “food processing” OR “processed food” OR “processed foods” OR “NOVA” OR “NOVA system” OR “NOVA food classification” OR “NOVA classification system”) AND (hypertension OR “high blood pressure” OR “high blood pressures” OR “blood pressure” OR “systolic pressure” OR “diastolic pressure” OR “systolic blood pressure” OR “diastolic blood pressure”) AND (adult OR adults OR aged OR “middle aged” OR elderly OR “older adult”).
- -
- Embase: (“ultra-processed food” OR “ultra-processed foods” OR “ultraprocessed food” OR “ultraprocessed foods” OR “ultra-processed product” OR “ultra-processed products” OR “ultra-processing” OR “food processing” OR “processed food” OR “processed foods” OR “NOVA” OR “NOVA system” OR “NOVA food classification” OR “NOVA classification system”) AND (hypertension OR “high blood pressure” OR “high blood pressures” OR “blood pressure” OR “systolic pressure” OR “diastolic pressure” OR “systolic blood pressure” OR “diastolic blood pressure”) AND (adult OR adults OR aged OR “middle aged” OR elderly OR “older adult”).
- -
- LILACS: (“alimento ultra-processado” OR “alimentos ultra-processados” OR “alimento ultraprocessado” OR “alimentos ultraprocessados” OR “produto ultra-processado” OR “produtos ultra-processados” OR “ultra-processamento” OR “processamento de alimento” OR “alimento processado” OR “alimentos processados” OR “NOVA” OR “sistema NOVA” OR “classificação de alimentos NOVA” OR “sistema de classificação de alimentos NOVA”) AND (hipertensão OR “hipertensão arterial sistêmica” OR “pressão arterial elevada” OR “pressão arterial” OR “pressão sistólica” OR “pressão diastólica” OR “pressão arterial sistólica” OR “pressão arterial diastólica”) AND (adulto OR adultos OR idoso OR idosos).
2.2. Article Selection Process and Data Extraction
2.3. Appraisal of Methodological Quality
3. Results
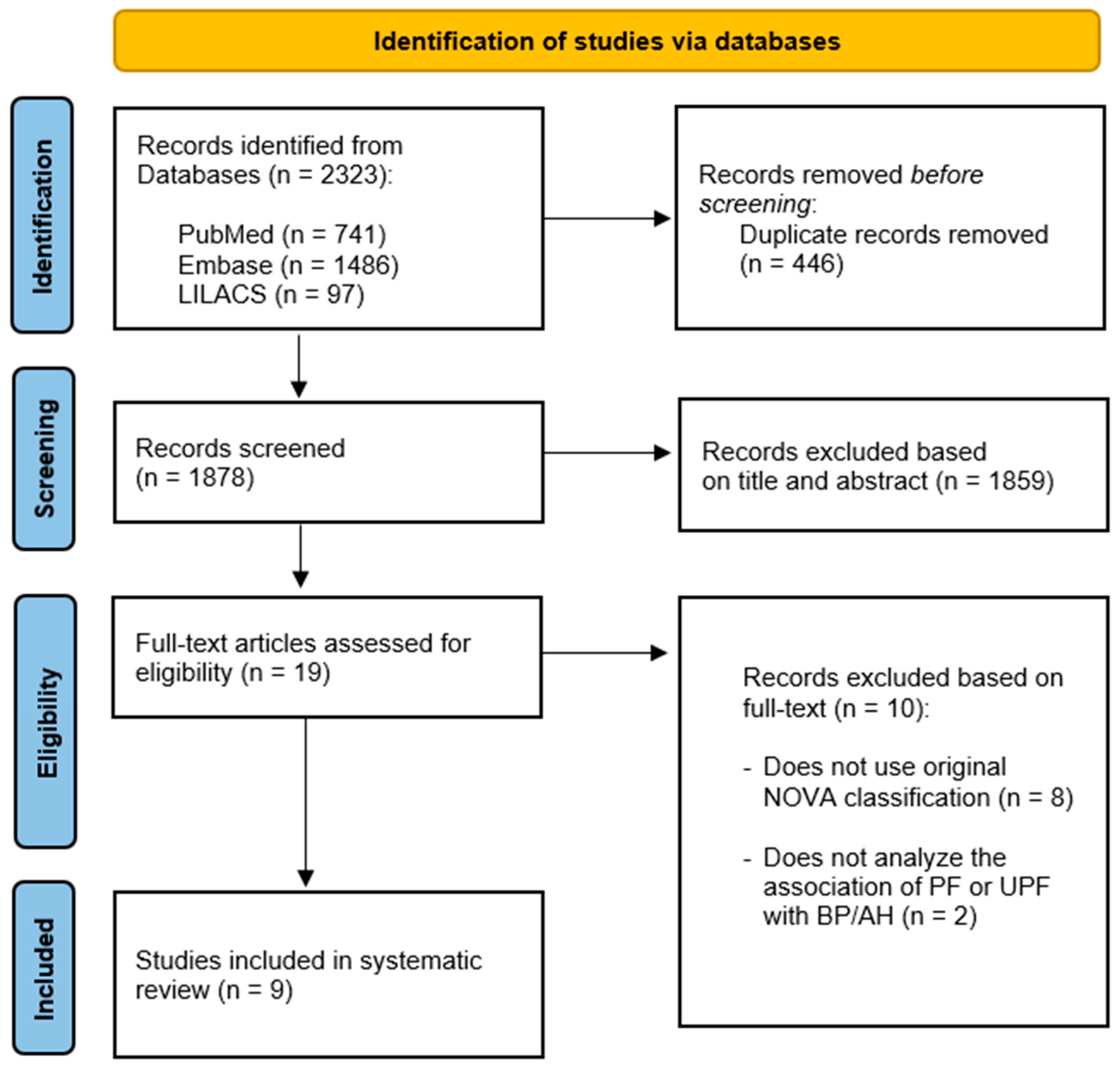
3.1. Article Selection Process
3.2. Overview and Characteristics of Studies
3.3. Processed and Ultra-Processed Food Consumption
3.4. Association between Processing of Food and Arterial Hypertension
3.5. Quality Appraisal
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- De Deus Mendonça, R.; Lopes, A.C.S.; Pimenta, A.M.; Gea, A.; Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Ultra-Processed Food Consumption and the Incidence of Hypertension in a Mediterranean Cohort: The Seguimiento Universidad de Navarra Project. Am. J. Hypertens. 2017, 30, 358–366. [Google Scholar] [CrossRef] [Green Version]
- Rezende-Alves, K.; Hermsdorff, H.H.M.; Miranda, A.E.D.S.; Lopes, A.C.S.; Bressan, J.; Pimenta, A.M. Food processing and risk of hypertension: Cohort of Universities of Minas Gerais, Brazil (CUME Project). Public Health Nutr. 2020, 24, 4071–4079. [Google Scholar] [CrossRef]
- Nardocci, M.; Polsky, J.Y.; Moubarac, J.-C. Consumption of ultra-processed foods is associated with obesity, diabetes and hypertension in Canadian adults. Can. J. Public Health 2020, 112, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Word Health Organization. Technical Package for Cardiovascular Disease Management in primary Health Care: Healthy-Lifestyle Counselling; WHO: Geneva, Switzerland, 2018; 28p. [Google Scholar]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; de Castro, I.R.R.; Cannon, G. Uma nova classificação de alimentos baseada na extensão e propósito do seu processamento. Cad. Saúde Pública 2010, 26, 2039–2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Costa Louzada, M.L.; Ricardo, C.Z.; Steele, E.M.; Levy, R.B.; Cannon, G.; Monteiro, C.A. The Share of Ultra-Processed Foods Determines the Overall Nutritional Quality of Diets in Brazil. Public Health Nutr. 2018, 21, 94–102. [Google Scholar] [CrossRef] [Green Version]
- Baker, P.; Machado, P.; Santos, T.; Sievert, K.; Backholer, K.; Hadjikakou, M.; Russell, C.; Huse, O.; Bell, C.; Scrinis, G.; et al. Ultra-processed foods and the nutrition transition: Global, regional and national trends, food systems transformations and political economy drivers. Obes. Rev. 2020, 21, e13126. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Lawrence, M.; Louzada, M.L.C.; Machado, P.P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; FAO: Rome, Italy, 2019; 48p. [Google Scholar]
- Mente, A.; Dehghan, M.; Rangarajan, S.; McQueen, M.; Dagenais, G.; Wielgosz, A.; Lear, S.; Li, W.; Chen, H.; Yi, S.; et al. Association of dietary nutrients with blood lipids and blood pressure in 18 countries: A cross-sectional analysis from the PURE study. Lancet Diabetes Endocrinol. 2017, 5, 774–787. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Trieu, K.; Yoshimura, S.; Neal, B.; Woodward, M.; Campbell, N.R.C.; Li, Q.; Lackland, D.T.; Leung, A.A.; Anderson, C.A.M.; et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: Systematic review and meta-analysis of randomised trials. BMJ 2020, 368, m315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santana, N.M.T.; Mill, J.G.; Velasquez-Melendez, G.; Moreira, A.; Barreto, S.; Viana, M.C.; Molina, M.D.C.B. Consumption of alcohol and blood pressure: Results of the ELSA-Brasil study. PLoS ONE 2018, 13, e0190239. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Fang, X.; Wei, X.; Liu, Y.; Jin, Z.; Chen, Q.; Fan, Z.; Aaseth, J.; Hiyoshi, A.; He, J.; et al. Dose-response relationship between dietary magnesium intake, serum magnesium concentration and risk of hypertension: A systematic review and meta-analysis of prospective cohort studies. Nutr. J. 2017, 16, 26. [Google Scholar] [CrossRef]
- Mohammadifard, N.; Gotay, C.; Humphries, K.H.; Ignaszewski, A.; Esmaillzadeh, A.; Sarrafzadegan, N. Electrolyte minerals intake and cardiovascular health. Crit. Rev. Food Sci. Nutr. 2019, 59, 2375–2385. [Google Scholar] [CrossRef] [PubMed]
- Jaime, P.; Campello, T.; Monteiro, C.; Bortoletto, A.P.; Yamaoka, M.; Bomfim, M. Diálogo sobre Ultraprocessados: Soluções para Sistemas Alimentares Saudáveis e Sustentáveis; Universidade de São Paulo: São Paulo, Brazil, 2021; 45p. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm. (accessed on 25 August 2021).
- The Modified Newcastle Ottawa Scale for Cross Sectional Studies. Available online: http://journals.plos.org/plosone/article/file?id=info%3Adoi/10.1371/journal.pone.0136065.s004&type=supplementary (accessed on 25 August 2021).
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [Green Version]
- Da Conceição, A.R.; Fonseca, P.C.D.A.; Morais, D.D.C.; De Souza, E.C.G. Association of the degree of food processing with the consumption of nutrients and blood pressure. O Mundo da Saúde 2019, 43, 512–529. [Google Scholar] [CrossRef]
- Scaranni, P.d.O.d.S.; Cardoso, L.d.O.; Chor, D.; Melo, E.C.P.; Matos, S.M.A.; Giatti, L.; Barreto, S.M.; Fonseca, M.d.J.M.d. Ultra-processed foods, changes in blood pressure and incidence of hypertension: The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Public Health Nutr. 2021, 24, 3352–3360. [Google Scholar] [CrossRef] [PubMed]
- Smiljanec, K.; Mbakwe, A.U.; Ramos-Gonzalez, M.; Mesbah, C.; Lennon, S.L. Associations of Ultra-Processed and Unprocessed/Minimally Processed Food Consumption with Peripheral and Central Hemodynamics and Arterial Stiffness in Young Healthy Adults. Nutrients 2020, 12, 3229. [Google Scholar] [CrossRef] [PubMed]
- Martínez Steele, E.; Juul, F.; Neri, D.; Rauber, F.; Monteiro, C.A. Dietary Share of Ultra-Processed Foods and Metabolic Syndrome in the US Adult Population. Prev. Med. 2019, 125, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Monge, A.; Canella, D.S.; López-Olmedo, N.; Lajous, M.; Cortés-Valencia, A.; Stern, D. Ultraprocessed beverages and processed meats increase the incidence of hypertension in Mexican women. Br. J. Nutr. 2020, 126, 600–611. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Perez, C.; San-Cristobal, R.; Guallar-Castillon, P.; Martínez-González, M.; Salas-Salvadó, J.; Corella, D.; Castañer, O.; Martinez, J.; Alonso-Gómez, A.M.; Wärnberg, J.; et al. Use of Different Food Classification Systems to Assess the Association between Ultra-Processed Food Consumption and Cardiometabolic Health in an Elderly Population with Metabolic Syndrome (PREDIMED-Plus Cohort). Nutrients 2021, 13, 2471. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA Food Classification and the Trouble with Ultra-Processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; de Castro, I.R.; Cannon, G. Increasing Consumption of Ultra-Processed Foods and Likely Impact on Human Health: Evidence from Brazil. Public Health Nutr. 2011, 14, 5–13. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Levy, R.; Moubarac, J.C.; Jaime, P.; Martins, A.P.; Canella, D.; Louzada, M.; Parra, D. NOVA. The star shines bright. World Nutr. 2016, 7, 28–38. [Google Scholar]
- Moubarac, J.-C.; Batal, M.; Martins, A.P.B.; Claro, R.; Levy, R.B.; Cannon, G.; Monteiro, C. Processed and Ultra-processed Food Products: Consumption Trends in Canada from 1938 to 2011. Can. J. Diet. Pract. Res. 2014, 75, 15–21. [Google Scholar] [CrossRef]
- Moubarac, J.-C.; Batal, M.; Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A. Consumption of Ultra-Processed Foods Predicts Diet Quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef]
- Martínez Steele, E.; Baraldi, L.G.; da Costa Louzada, M.L.; Moubarac, J.-C.; Mozaffarian, D.; Monteiro, C.A. Ultra-Processed Foods and Added Sugars in the US Diet: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [Green Version]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of ultra-processed foods and health status: A systematic review and meta-analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef]
- De Araújo, T.; de Moraes, M.; Magalhães, V.; Afonso, C.; Santos, C.; Rodrigues, S. Ultra-Processed Food Availability and Noncommunicable Diseases: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7382. [Google Scholar] [CrossRef]
- Marino, M.; Puppo, F.; Del Bo’, C.; Vinelli, V.; Riso, P.; Porrini, M.; Martini, D. A Systematic Review of Worldwide Consumption of Ultra-Processed Foods: Findings and Criticisms. Nutrients 2021, 13, 2778. [Google Scholar] [CrossRef]
- Elizabeth, L.; Machado, P.; Zinöcker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, Z.; Yang, H.; Qiu, P.; Wang, H.; Wang, F.; Zhao, Q.; Fang, J.; Nie, J. Consumption of ultra-processed foods and health outcomes: A systematic review of epidemiological studies. Nutr. J. 2020, 19, 86. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension global hypertension practice guidelines. J. Hypertens. 2020, 38, 982–1004. [Google Scholar] [CrossRef]
- Barroso, W.K.S.; Rodrigues, C.I.S.; Bortolotto, L.A.; Mota-Gomes, M.A.; Brandão, A.A.; Feitosa, A.D.D.M.; Machado, C.A.; Poli-De-Figueiredo, C.E.; Amodeo, C.; Mion, D.; et al. Diretrizes Brasileiras de Hipertensão Arterial—2020. Arq. Bras. Cardiol. 2021, 116, 516–658. [Google Scholar] [CrossRef]
- Motta, V.W.d.L.; Lima, S.C.V.C.; Marchioni, D.M.L.; Lyra, C.D.O. Food frequency questionnaire for adults in Northeast Region of Brazil: Emphasis on extent and purpose of food processing. Rev. Saúde Pública 2021, 55, 51. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations. Dietary Assessment: A Resource Guide to Method Selection and Application in Low Resource Settings; FAO: Rome, Italy, 2018; 152p. [Google Scholar]
- Monteiro, C.A.; Moubarac, J.-C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-Processed Products Are Becoming Dominant in the Global Food System. Obes. Rev. 2013, 14 (Suppl. 2), 21–28. [Google Scholar] [CrossRef]
- Matos, R.A.; Adams, M.; Sabaté, J. Review: The Consumption of Ultra-Processed Foods and Non-communicable Diseases in Latin America. Front. Nutr. 2021, 8, 110. [Google Scholar] [CrossRef]
- Juul, F.; Vaidean, G.; Lin, Y.; Deierlein, A.L.; Parekh, N. Ultra-Processed Foods and Incident Cardiovascular Disease in the Framingham Offspring Study. J. Am. Coll. Cardiol. 2021, 77, 1520–1531. [Google Scholar] [CrossRef]
- Fardet, A. Characterization of the Degree of Food Processing in Relation With Its Health Potential and Effects. Adv. Food Nutr. Res. 2018, 85, 79–129. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations and National Research Institute for Agriculture, Food and Environment. Enabling Sustainable Food Systems: Innovators’ Handbook; FAO and INRAE: Rome, Italy, 2020; 233p. [Google Scholar] [CrossRef]
- Martines, R.M.; Machado, P.; Neri, D.A.; Levy, R.B.; Rauber, F. Association between watching TV whilst eating and children’s consumption of ultraprocessed foods in United Kingdom. Matern. Child Nutr. 2019, 15, e12819. [Google Scholar] [CrossRef]
- Noll, P.R.E.S.; Noll, M.; de Abreu, L.C.; Baracat, E.C.; Silveira, E.A.; Sorpreso, I.C.E. Ultra-processed food consumption by Brazilian adolescents in cafeterias and school meals. Sci. Rep. 2019, 9, 7162. [Google Scholar] [CrossRef] [Green Version]
- Gomes, C.D.B.; Malta, M.B.; Louzada, M.L.D.C.; Benício, M.H.D.; Barros, A.J.D.; Carvalhaes, M.A.D.B.L. Ultra-processed Food Consumption by Pregnant Women: The Effect of an Educational Intervention with Health Professionals. Matern. Child Health J. 2019, 23, 692–703. [Google Scholar] [CrossRef]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77.e3. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Author (Year) | Language of Publication | Objective of Study | Denomination and Description of Dietary Component Evaluated |
|---|---|---|---|
| Conceição et al., (2018) [19] | English | Evaluate whether intake of macronutrients and micronutrients and blood pressure (BP) levels are associated with degree of food processing | PFs: Salt, sugar or other substance of culinary use added to the food in natura or minimally processed (roasted biscuit; mozzarella; salted bread; whole grain bread; Minas cheese; toast). UPFs: essentially industrial food, ready to eat, multi-ingredient products involving multiple steps and processing techniques (chocolate; normal and whole grain salt and water crackers; corn starch and polvilho crackers; pasta with tomato sauce; margarine; light margarine; instant powder for porridge; cream cheese; salami; artificial strawberry and grape juices. |
| Martinez-Peres et al., (2021) [24] | English | Assess the impact of the food classification system on the association between the consumption of UPFs and cardiometabolic health using the same dataset. | UPFs: article followed description proposed by Monteiro et al., (2018) [25], Monteiro et al., (2011) [26], Monteiro et al., (2016) [27]. |
| Mendonça et al., (2017) [1] | English | Evaluate potential association between consumption of UPFs and risk of AH | AUPs: carbonated drinks, processed meat, biscuits, cookies, candy, confectionery, ‘instant’ packaged soups and noodles, sweet or savory packaged snacks, and sugared milk and fruit drinks. Article followed description proposed by Monteiro et al., (2010), Monteiro et al., (2016), Moubarac et al., (2014) [5,27,28]. |
| Monge et al., (2021) [23] | English | Estimate association between incidence of AH and consumption of UPFs (liquids and solids) as well as subgroups of UPFs | UPFs: industrial formulations with multiple ingredients that are usually not used for cooking (like food additives), such as sugar-sweetened beverages (SSB), packed snacks and candies. The UPFs were classified into subgroups dairy products (yogurt, ice cream, petite suisse, Yakult), added fats (cream, margarine, cream cheese), sugary products (jello, flan, sweet breads, cakes, cookies, candies, chocolate, honey, jelly and fruit paste candy), SSB (soya milk, orange juice, soda, flavored water), alcoholic beverages, processed meats (bacon, sausage, ham, chorizo, longaniza (a spicy pork sausage) and other deli meats), cereals (processed oats, low- and high-fiber breakfast cereals, cereal bars, white and whole-grain loaf of bread), salty snacks (chips and saltines) and fast food (burgers, hotdogs, pizza, tortas). |
| Nardocci et al., (2020) [3] | English | Evaluate associations between consumption of UPFs and obesity, diabetes, AH and heart disease | UPFs: article followed description proposed by Moubarac et al., (2017) for UPFs [29]. |
| Rezende-Alves el at., (2020) [2] | English | Analyze association between consumption of foods according to degree of processing and incidence of AH | PFs and UPFs: complete list of PFs and UPFs in supplementary material of article by Rezende-Alves et al., (2020) based on description proposed by Monteiro et al., (2018) [25]. |
| Scaranni et al., (2021) [20] | English | Estimate changes in BP and incidence of AH associated with consumption of UPFs in adults | UPFs: According to Monteiro et al., (2016) [27]. |
| Smiljanec et al., (2020) [21] | English | Investigate association between consumption of UPFs/in natura/minimally processed foods and peripheral/central BP | UPFs: breakfast cereals, packaged bread, flavored yogurt and dairy products, half and half, lactose-free milk, milk alternatives, packaged sliced, processed, and creamed cheese, processed meats, meat alternatives, packaged (instant) soups and noodles, pasta sauces, ready-to-eat frozen dishes, condiments, sweet or salty packaged snacks, ice cream, confectionery, sugar-sweetened beverages, hard liquor). Cheese and dried, cured, or smoked meats were included in the UPFs category as they contain additives such as colors, preservatives, and stabilizers. |
| Steele et al., (2019) [22] | English | Examine association between participation of UPFs in diet and metabolic syndrome | UPFs: Article followed description by Monteiro et al., (2019) and Martinez Steele et al., (2016) for PFs and UPFs [8,30]. |
| First Author (Year) | Study Design (Study Period)/Country | Population (Sample Size/Age) | Food Consumption Assessment Method | Dietary Components | Diagnostic Criteria for Hypertension | Energy Contribution of PFs/UPFs (%) | Statistical Analysis Association between Food Processing and Hypertension |
|---|---|---|---|---|---|---|---|
| Conceição et al., (2018) [19] | Cross-sectional (2014–2015) Brazil | 64 adults 25–57 years | One-day 24 hR/ NOVA classification (Monteiro, 2010) | PFs UPFs | Measurement of BP using digital meter according to 6th Brazilian Arterial Hypertension Guidelines (2010). | PFs: 6.5% UPFs: 7.7% | Student’s t-test No significant difference in mean SBP or DBP in comparison of individuals based on consumption of food groups (p > 0.05) |
| Martinez-Peres et al., (2021) [24] | Transversal (2020) Spain | 5636 adults and older people 55–75 years (mean age: 65 years) | Semi-quantitative FFQ with 143 items (validated *)/NOVA classification (Monteiro, 2010) | UPFs | Use of anti-hypertensive agent and BP equal to or higher than 130/85 mmHg. | UPF: 7.9% ** | Linear regression. No significant association between consumption of UPFs and SBP and DBP in adjusted models (β = −0.17 mmHg; CI = −0.5, 0.16; p = −0.08 e β = 0.08 mmHg; CI = −0.1, 0.26; p = 0.383, respectively). |
| Mendonça et al., (2017) [1] | Cohort (1999–2015) Spain | 14790 middle-aged adults | Self-administered semi-quantitative FFQ with 136 items (validated *)/NOVA (servings/day and caloric contribution) | UPFs | Self-declared medical diagnosis. | UPFs: 2.1 to 5 servings/day *** | Cox regression Positive association between consumption of UPFs and AH. Highest tercile of consumption of UPFs had greater risk of developing AH compared to lowest tercile (HR adjusted by multivariable analysis = 1.21 [95% CI: 1.06–137]). |
| Monge et al., (2021) [23] | Cohort (2006–2010) Mexico | 64 934 women 41.7 (SD: 7.2) years | Semi-quantitative FFQ with 140 items (validated *)/NOVA (caloric contribution) | UPFs | Self-declared medical diagnosis or use of antihypertensive. | UPFs: Total—29.8% (SD: 9.4) Liquid—6.4% (SD: 4.8) Solid—23.4% (SD: 8.9) | Poisson regression Total consumption of UPFs and consumption of solid UPFs not associated with AH (IRR = 0.96, 95% CI: 0.79, 1.16; IRR = 0.91, 95% CI: 0.82, 1.01, respectively). Ultra-processed beverages and processed meats associated with increase in incidence of AH (IRR = 1.32, 95% CI: 1.10, 1.65; IRR = 1.17, 95% CI: 1.01, 1.36, respectively). |
| Nardocci et al., (2020) [3] | Cross-sectional (2015) Canada | 13,608 adults ≥ 19 years | 24 hR/NOVA classification (Monteiro, 2010), caloric contribution | UPFs | Self-declared AH—answer to question on long-term health conditions diagnosed by healthcare provider: “Do you have diabetes/high blood pressure?” | UPFs: 47% | Linear regression UPFs significantly associated with greater likelihood of developing AH. In adjusted models, 10 percentage point increase in relative energy from UPFs associated with 9% increase in likelihood of AH. Adults in highest tercile of consumption of UPFs 60% more likely to have AH (OR = 1.60, 95% CI: 1.26–2.03) compared to those in lower terciles. Odds ratio used for 10% increase in relative intake of UPFs (% of total energy intake) |
| Rezende-Alves et al., (2020) [2] | Cohort (2016–2018) Brazil | 1221 Adults (mean age: 35.2 years) | FFQ (validated *)/ NOVA classification (caloric contribution) | PFs UPFs | Self-declared medical diagnosis or use of antihypertensive or self-declared high BP (≥130/80 mmHg) according to recent cutoff points proposed by ACC/AHA. | PFs: 9.9% (SD: 5.8) UPFs: 25.8% (SD: 11) | Poisson regression Highest quintile of consumption of UPFs had increased risk of AH (RR: 1.35; 95% CI: 1.01, 1.81). When alcohol intake was excluded from caloric percentage of UPFs, greater consumption of these foods remained independently associated with increase in incidence of AH (RR: 1.35; 95% CI: 1.01, 1.82). No association identified between PFs and AH. |
| Scaranni et al., (2021) [20] | Cohort (2008–2010) Brazil | 8171 adults and older people 35–74 years (mean: 49 years) | FFQ with 114 items (validated *)/ NOVA (caloric contribution) | UPFs | Measurement of BP (SBP ≥ 140 mmHg or DBP ≥ 90 mmHg) and use of anti-hypertensive in previous two weeks. | UPFs: 25.2% (14.5–35.4%) | Mixed-effects linear regression to evaluate changes in BP and logistic regression to evaluated incidence of AH Greater consumption of UPFs associated with 23% greater risk of developing AH (OR = 1.23, 95% CI: 1.06, 1.44). No association between consumption of UPFs and changes in BP (mean SBP and DBP increased over time and varied slightly with consumption of UPFs). |
| Smiljanec et al., (2020) [21] | Cross-sectional USA | 40 adults 18–45 years | Three-day food record/ NOVA classification (Monteiro, 2010) | UPFs | BP measured by outpatient monitoring. Central and peripheral BP measured by SBP, DBP, MBP, PP and aortic pressure. Monitoring outside clinic followed recommendations of Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement (2015). | UPFs: 50.0 ± 2.4% | Multiple linear regression Positive association between UPFs and general and diurnal SBP (B = 0.25, 95% CI: 0.03, 0.46, p = 0.029; B = 0.32, 95% CI: 0.09, 0.56, p = 0.008, respectively), diurnal DBP (B = 0.18, 95% CI: 0.01, 0.36, p = 0.049) and diurnal peripheral PP (B = 0.22, 95% CI: 0.03, 0.41, p = 0.027). After adjustments, UPFs positively associated with SBP (1% increase in consumption of UPFs associated with 0.25 mmHg and 0.32 mmHg increase in general and diurnal SBP, respectively), peripheral and central DBP. No significant association between consumption of UPFs and BP in men, but tendency toward positive association between UPFs and BP. 95% CI and p < 0.05 used. |
| Steele et al., (2019) [22] | Cross-sectional (2009–2014) USA | 6385 adults ≥ 20 years and older people | Two-day R24/NOVA classification (Monteiro, 2010) (caloric contribution) | UPFs | Measurement of BP (SBP ≥ 130 mmHg and/or DBP ≥ 85 mmHg based on Centers for Disease Control and Prevention 2009–2010; 2011–2012; 2013–2014) or use of antihypertensive. | UPFs: 55.5% | Poisson regression Significant association between consumption quintiles of UPFs and increase in BP (PR = 1.19; 95% CI: 1.03, 1.38) in adjusted multivariate models. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbosa, S.S.; Sousa, L.C.M.; de Oliveira Silva, D.F.; Pimentel, J.B.; Evangelista, K.C.M.d.S.; Lyra, C.d.O.; Lopes, M.M.G.D.; Lima, S.C.V.C. A Systematic Review on Processed/Ultra-Processed Foods and Arterial Hypertension in Adults and Older People. Nutrients 2022, 14, 1215. https://doi.org/10.3390/nu14061215
Barbosa SS, Sousa LCM, de Oliveira Silva DF, Pimentel JB, Evangelista KCMdS, Lyra CdO, Lopes MMGD, Lima SCVC. A Systematic Review on Processed/Ultra-Processed Foods and Arterial Hypertension in Adults and Older People. Nutrients. 2022; 14(6):1215. https://doi.org/10.3390/nu14061215
Chicago/Turabian StyleBarbosa, Suamy Sales, Layanne Cristini Martin Sousa, David Franciole de Oliveira Silva, Jéssica Bastos Pimentel, Karine Cavalcanti Maurício de Sena Evangelista, Clélia de Oliveira Lyra, Márcia Marília Gomes Dantas Lopes, and Severina Carla Vieira Cunha Lima. 2022. "A Systematic Review on Processed/Ultra-Processed Foods and Arterial Hypertension in Adults and Older People" Nutrients 14, no. 6: 1215. https://doi.org/10.3390/nu14061215
APA StyleBarbosa, S. S., Sousa, L. C. M., de Oliveira Silva, D. F., Pimentel, J. B., Evangelista, K. C. M. d. S., Lyra, C. d. O., Lopes, M. M. G. D., & Lima, S. C. V. C. (2022). A Systematic Review on Processed/Ultra-Processed Foods and Arterial Hypertension in Adults and Older People. Nutrients, 14(6), 1215. https://doi.org/10.3390/nu14061215