Design and Validation of a Diet Rich in Slowly Digestible Starch for Type 2 Diabetic Patients for Significant Improvement in Glycemic Profile

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. High-SDS Diet and Low-SDS Diet Design
2.2. Study Design
2.3. Diet Composition, Compliance, and Acceptance
2.4. Population
2.5. Postprandial Glycemic Response
2.6. Statistical Analyses
3. Results
3.1. SDS Analysis of Commercial Food Products and Diet Design for the Study
3.2. Study Population Characteristics
3.3. Diets Composition
3.4. Contribution of Various Food Groups to the SDS Intake for Both Diets
3.5. Compliance to the Diet Interventions
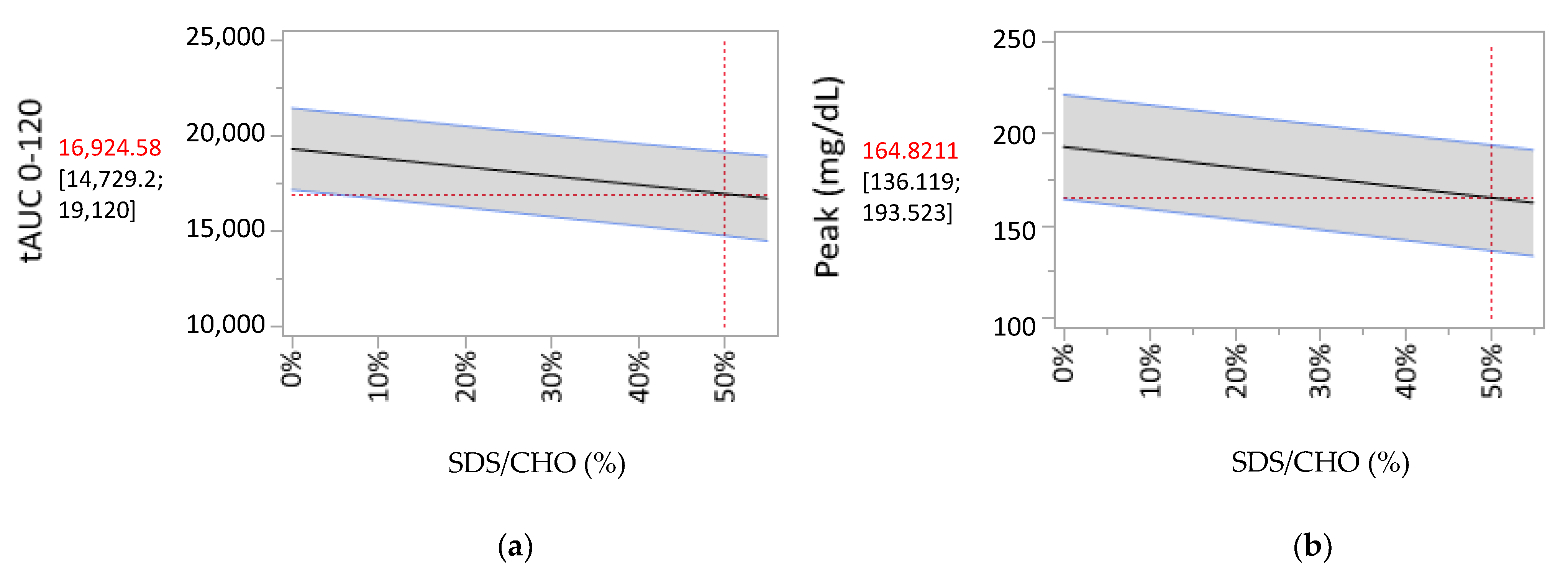
3.6. Correlation between the SDS/Carbohydrates Ratio for a Meal and the Postprandial Glycemic Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas. Available online: https://www.diabetesatlas.org/en/ (accessed on 19 June 2020).
- Blaak, E.E.; Antoine, J.-M.; Benton, D.; Björck, I.; Bozzetto, L.; Brouns, F.; Diamant, M.; Dye, L.; Hulshof, T.; Holst, J.J.; et al. Impact of postprandial glycaemia on health and prevention of disease. Obes. Rev. 2012, 13, 923–984. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forouhi, N.G.; Misra, A.; Mohan, V.; Taylor, R.; Yancy, W. Dietary and nutritional approaches for prevention and management of type 2 diabetes. BMJ 2018, 361, k2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansen, M.Y.; Macdonald, C.S.; Hansen, K.B.; Karstoft, K.; Christensen, R.; Pedersen, M.; Hansen, L.S.; Zacho, M.; Wedell-Neergaard, A.-S.; Nielsen, S.T.; et al. Effect of an Intensive Lifestyle Intervention on Glycemic Control in Patients with Type 2 Diabetes. JAMA 2017, 318, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.I.; De Leeuw, I.; Hermansen, K.; Karamanos, B.; Karlström, B.; Katsilambros, N.; Riccardi, G.; Rivellese, A.; Rizkalla, S.; Slama, G.; et al. Evidence-Based nutritional approaches to the treatment and prevention of diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2004, 14, 373–394. [Google Scholar] [CrossRef]
- Société Francophone du Diabète. Référentiel De Bonnes Pratiques—Nutrition & Diététique—Diabète De Type 2 De L’Adulte. Med. Mal. Metab. 2014, 8, 1–84. [Google Scholar] [CrossRef]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.; et al. Dietary Glycemic Index and Load and the Risk of Type 2 Diabetes: A Systematic Review and Updated Meta-Analyses of Prospective Cohort Studies. Nutrients 2019, 11, 1280. [Google Scholar] [CrossRef] [Green Version]
- Martínez-González, M.; Fernandez-Lazaro, C.; Toledo, E.; Díaz-López, A.; Corella, D.; Goday, A.; Romaguera, D.; Vioque, J.; Alonso-Gómez, A.M.; Wärnberg, J.; et al. Carbohydrate quality changes and concurrent changes in cardiovascular risk factors: A longitudinal analysis in the Predimed-Plus randomized trial. Am. J. Clin. Nutr. 2019, 111, 291–306. [Google Scholar] [CrossRef]
- Englyst, H.N.; Kingman, S.M.; Cummings, J.H. Classification and Measurement of Nutritionally Important Starch Fractions. Eur. J. Clin. Nutr. 1992, 46, 33–50. [Google Scholar]
- Englyst, K.; Goux, A.; Meynier, A.; Quigley, M.; Englyst, H.; Brack, O.; Vinoy, S. Inter-Laboratory validation of the starch digestibility method for determination of rapidly digestible and slowly digestible starch. Food Chem. 2018, 245, 1183–1189. [Google Scholar] [CrossRef]
- Meynier, A.; Goux, A.; Atkinson, F.; Brack, O.; Vinoy, S. Postprandial glycaemic response: How is it influenced by characteristics of cereal products? Br. J. Nutr. 2015, 113, 1931–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinoy, S.; Lesdéma, A.; Cesbron-Lavau, G.; Goux, A.; Meynier, A. Creating Food Products with a lower Glycemic Index. In The Glycemic Index—Applications in Practice; Philippou, E., Ed.; CRC Press in Taylor & Francis Group: Abingdon, UK, 2016; pp. 285–318. [Google Scholar]
- Nazare, J.-A.; De Rougemont, A.; Normand, S.; Sauvinet, V.; Sothier, M.; Vinoy, S.; Désage, M.; Laville, M. Effect of postprandial modulation of glucose availability: Short- and long-term analysis. Br. J. Nutr. 2009, 103, 1461–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert-Porcheron, S.; Normand, S.; Blond, E.; Sothier, M.; Roth, H.; Meynier, A.; Vinoy, S.; Laville, M.; Nazare, J.-A. Modulation of Starch Digestibility in Breakfast Cereals Consumed by Subjects with Metabolic Risk: Impact on Markers of Oxidative Stress and Inflammation during Fasting and the Postprandial Period. Mol. Nutr. Food Res. 2017, 61, 1700212. [Google Scholar] [CrossRef] [PubMed]
- Péronnet, F.; Meynier, A.; Sauvinet, V.; Normand, S.; Bourdon, E.; Mignault, D.; St-Pierre, D.H.; Laville, M.; Rabasa-Lhoret, R.; Vinoy, S. Plasma glucose kinetics and response of insulin and GIP following a cereal breakfast in female subjects: Effect of starch digestibility. Eur. J. Clin. Nutr. 2015, 69, 740–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinoy, S.; Normand, S.; Meynier, A.; Sothier, M.; Louche-Pelissier, C.; Peyrat, J.; Maitrepierre, C.; Nazare, J.-A.; Brand-Miller, J.C.; Laville, M. Cereal Processing Influences Postprandial Glucose Metabolism as Well as the GI Effect. J. Am. Coll. Nutr. 2015, 32, 79–91. [Google Scholar] [CrossRef] [Green Version]
- Harbis, A.; Perdreau, S.; Vincent-Baudry, S.; Charbonnier, M.; Bernard, M.-C.; Raccah, D.; Senft, M.; Lorec, A.-M.; Defoort, C.; Portugal, H.; et al. Glycemic and insulinemic meal responses modulate postprandial hepatic and intestinal lipoprotein accumulation in obese, insulin-resistant subjects. Am. J. Clin. Nutr. 2004, 80, 896–902. [Google Scholar] [CrossRef]
- De Rougemont, A.; Normand, S.; Nazare, J.-A.; Skilton, M.R.; Sothier, M.; Vinoy, S.; Laville, M. Beneficial effects of a 5-week low-glycaemic index regimen on weight control and cardiovascular risk factors in overweight non-diabetic subjects. Br. J. Nutr. 2007, 98, 1288–1298. [Google Scholar] [CrossRef]
- Seal, C.J.; Daly, M.E.; Thomas, L.C.; Bal, W.; Birkett, A.M.; Jeffcoat, R.; Mathers, J.C. Postprandial carbohydrate metabolism in healthy subjects and those with type 2 diabetes fed starches with slow and rapid hydrolysis rates determined in vitro. Br. J. Nutr. 2003, 90, 853–864. [Google Scholar] [CrossRef] [Green Version]
- Axelsen, M.; Lenner, R.A.; Lönnroth, P.; Smith, U. Breakfast glycaemic response in patients with type 2 diabetes: Effects of bedtime dietary carbohydrates. Eur. J. Clin. Nutr. 1999, 53, 706–710. [Google Scholar] [CrossRef] [Green Version]
- Axelsen, M.; Lönnroth, P.; Lenner, R.A.; Taskinen, M.-R.; Smith, U. Suppression of nocturnal fatty acid concentrations by bedtime carbohydrate supplement in type 2 diabetes: Effects on insulin sensitivity, lipids, and glycemic control. Am. J. Clin. Nutr. 2000, 71, 1108–1114. [Google Scholar] [CrossRef]
- Golay, A.; Koellreutter, B.; Bloise, D.; Assal, J.-P.; Würsch, P. The effect of muesli or cornflakes at breakfast on carbohydrate metabolism in type 2 diabetic patients. Diabetes Res. Clin. Pr. 1992, 15, 135–141. [Google Scholar] [CrossRef]
- Englyst, K.N.; Englyst, H.N.; Hudson, G.J.; Cole, T.J.; Cummings, J.H. Rapidly available glucose in foods: An in vitro measurement that reflects the glycemic response. Am. J. Clin. Nutr. 1999, 69, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Breyton, A.E.; Goux, A.; Lambert-Porcheron, S.; Meynier, A.; Sothier, M.; Van Den Berghe, L.; Brack, O.; Disse, E.; Laville, M.; Vinoy, S.; et al. Effect of Starch Digestibility Modulation on Glycemic Variability and Postprandial Glycemic Excursions in Subjects with Type 2 Diabetes: A Randomized Controlled Cross-Over Trial. Nutr. Metab. Cardiovas. 2020. accepted. [Google Scholar]
- Wachters-Hagedoorn, R.E.; Priebe, M.G.; Heimweg, J.A.J.; Heiner, A.M.; Englyst, K.N.; Holst, J.J.; Stellaard, F.; Vonk, R.J. The Rate of Intestinal Glucose Absorption Is Correlated with Plasma Glucose-Dependent Insulinotropic Polypeptide Concentrations in Healthy Men. J. Nutr. 2006, 136, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Traianedes, K.; O’Dea, K. Commercial canning increases the digestibility of beans in vitro and postprandial metabolic responses to them in vivo. Am. J. Clin. Nutr. 1986, 44, 390–397. [Google Scholar] [CrossRef] [Green Version]
- Ek, K.L.; Wang, S.; Copeland, L.; Miller, J.C.B. Discovery of a low-glycaemic index potato and relationship with starch digestion in vitro. Br. J. Nutr. 2013, 111, 699–705. [Google Scholar] [CrossRef] [Green Version]
- Scazzina, F.; Dall’Asta, M.; Casiraghi, M.C.; Sieri, S.; Del Rio, D.; Pellegrini, N.; Brighenti, F. Glycemic index and glycemic load of commercial Italian foods. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 419–429. [Google Scholar] [CrossRef]
- Ajala, O.; English, P.; Pinkney, J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. Am. J. Clin. Nutr. 2013, 97, 505–516. [Google Scholar] [CrossRef] [Green Version]
- Groupe de travail SFD Paramédical et AFDN. Regard Nouveau sur les Glucides Pour la Pratique en Diabetologie. Available online: https://www.sfdiabete.org/recommandations/referentiels (accessed on 19 June 2020).
- Englyst, K.; Vinoy, S.; Englyst, H.N.; Lang, V. Glycaemic index of cereal products explained by their content of rapidly and slowly available glucose. Br. J. Nutr. 2003, 89, 329–339. [Google Scholar] [CrossRef]
- VanRullen, I.B.; Volatier, J.-L.; Bertaut, A.; Dufour, A.; Dallongeville, J. Characteristics of energy intake under-reporting in French adults. Br. J. Nutr. 2013, 111, 1292–1302. [Google Scholar] [CrossRef] [Green Version]
- Brand-Miller, J.C.; Hayne, S.; Petocz, P.; Colagiuri, S. Low-Glycemic index diets in the management of diabetes: A meta-analysis of randomized controlled trials. Diabetes. Care 2003, 26, 2261–2267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinoy, S.; Meynier, A.; Goux, A.; Jourdan-Salloum, N.; Normand, S.; Rabasa-Lhoret, R.; Brack, O.; Nazare, J.-A.; Peronnet, F.; Laville, M. The Effect of a Breakfast Rich in Slowly Digestible Starch on Glucose Metabolism: A Statistical Meta-Analysis of Randomized Controlled Trials. Nutrients 2017, 9, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boers, H.M.; Alssema, M.; Mela, D.J.; Peters, H.P.F.; Vonk, R.J.; Priebe, M.G. The Rate of Glucose Appearance Is Related to Postprandial Glucose and Insulin Responses in Adults: A Systematic Review and Meta-analysis of Stable Isotope Studies. J. Nutr. 2019, 149, 1896–1903. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Food Group | High-SDS Diet | Low-SDS Diet | ||
|---|---|---|---|---|
| SDS Range: Min–Max (g/100 g) | Number of Analyses | SDS Range: Min–Max (g/100 g) | Number of Analyses | |
| Biscuits | 21–25 | 34 | NA | 0 |
| Rice | 14–27 | 18 | 3–5 | 5 |
| Pasta | 13–22 | 21 | 2–12 | 14 |
| Other wheat products | 10–13 | 3 | 1–4 | 5 |
| Bread/bread substitutes | 2 *–12.5 | 7 | 0–4 | 6 |
| Legumes | 3–9 | 4 | 0–2 | 6 |
| Other cereal products | NA | 0 | 0–5 | 4 |
| Potatoes | 1 * | 4 | 0–1 | 5 |
| Dietary Intake | High-SDS Diet | Low-SDS Diet | p Value |
|---|---|---|---|
| Total daily energy intake (kcal) | 1647 ± 58 | 1518 ± 68 | <0.05 |
| Available carbohydrates (g) | 203 ± 9 | 178 ± 8 | <0.001 |
| Available carbohydrates (% of TDEI) | 49 ± 1 | 47 ± 2 | NS |
| Of Which SDS (g) | 62 ± 5 | 12 ± 1 | <0.0001 |
| Of Which SDS (% of TDEI) | 15 ± 1 | 3 ± 0 | <0.0001 |
| Proteins (g) | 72 ± 4 | 70 ± 4 | NS |
| Proteins (% of TDEI) | 17 ± 1 | 19 ± 1 | NS |
| Lipids (g) | 56 ± 4 | 53 ± 6 | NS |
| Lipids (% of TDEI) | 30 ± 2 | 31 ± 3 | NS |
| Dietary fibers (g) | 24 ± 1 | 20 ± 1 | <0.01 |
| Dietary fibers (% of TDEI) | 2.9 ± 0.1 | 2.6 ± 0.1 | <0.05 |
| SDS Intake | High-SDS Diet | Low-SDS Diet | p Value * | ||
|---|---|---|---|---|---|
| SDS (g/Day) | SDS/CHO (%) | SDS (g/Day) | SDS/CHO (%) | ||
| SDS (g)/day | 62 ± 5 | 30 ± 1 | 12 ± 1 | 6 ± 0.3 | <0.0001 |
| SDS (g)/breakfast | 12 ± 2 | 27 ± 2 | 1 ± 0.3 | 3 ± 1 | <0.0001 |
| SDS (g)/lunch | 23 ± 2 | 30 ± 2 | 8 ± 0.8 | 10 ± 1 | <0.0001 |
| SDS (g)/dinner | 26 ± 3 | 32 ± 1 | 3 ± 0.3 | 4 ± 0.3 | <0.0001 |
| Food Group | High-SDS Diet (%) | Low-SDS Diet (%) | ||||||
|---|---|---|---|---|---|---|---|---|
| SDS Intake (g/6 Days) | Contribution to SDS Intake (%) | CHO Intake (g/6 Days) | Contribution to CHO Intake (%) | SDS Intake (g/6 Days) | Contribution to SDS Intake (%) | CHO Intake (g/6 Days) | Contribution to CHO Intake (%) | |
| Biscuits | 69 ± 9 | 18.7 % | 204 ± 28 | 22.1 % | NA | NA | NA | NA |
| Rice | 79 ± 10 | 21.5 % | 159 ± 20 | 17.3 % | 13 ± 2 | 18.7 % | 89 ± 11 | 8.6 % |
| Pasta | 152 ± 15 | 41.3 % | 250 ± 25 | 27.1 % | 26 ± 2 | 38.5 % | 124 ± 11 | 16.0 % |
| Other wheat products | 17 ± 2 | 4.6 % | 27 ± 5 | 2.9 % | 7 ± 1 | 10.4 % | 67 ± 9 | 8.6 % |
| Bread/bread substitutes | 22 ± 3 | 6.1 % | 171 ± 22 | 18.5 % | 13 ± 2 | 18.8 % | 327 ± 28 | 42.2 % |
| Legumes | 7 ± 1 | 1.9 % | 19 ± 3 | 2.1 % | 4 ± 1 | 5.9 % | 44 ± 4 | 5.7 % |
| Other cereal products | NA | NA | NA | NA | 5 ± 2 | 7.7 % | 44 ± 9 | 5.7 % |
| Potatoes | 22 ± 2 | 5.9 % | 47 ± 5 | 5.1 % | 0 | 0 % | 34 ± 4 | 4.4 % |
| Other products containing CHO 1 | 0 | 0% | 46 ± 9 | 5.0 % | 0 | 0% | 47 ± 9 | 6.1 % |
| Estimate | p-Value | ||
|---|---|---|---|
| Parameter | Intercept | SDS/CHO | SDS/CHO |
| Analysis of all three postprandial periods (n = 238) | |||
| tAUC 0–120 min | 19,272 | −4694 | 0.0006 |
| Peak value | 193 | −55.4 | <0.0001 |
| Delta peak | 71.3 | −48.3 | <0.0001 |
| Time to reach the peak | 99.5 | 8.34 | 0.6952 |
| Time in Range 0–120 min | |||
| <70 mg/dL | −0.009 | 0.14 | 0.2212 |
| [70–140 mg/dL] | 9.90 | 5.28 | 0.1287 |
| [140–180 mg/dL] | 8.12 | 3.71 | 0.2077 |
| [180–250 mg/dL] | 5.70 | −5.86 | 0.0141 |
| >250 mg/dL 1 | 1.27 | −3.21 | 0.0043 |
| Analysis of lunch and dinner postprandial periods (n = 168) 2 | |||
| tAUC 0–240 min | 35,310 | −2988 | 0.2043 |
| Time in Range 0–240 min | |||
| < 70 mg/dL | −0.012 | 0.19 | 0.2554 |
| [70–140 mg/dL] | 26.9 | −6.10 | 0.3472 |
| [140–180 mg/dL] | 12.6 | 18.3 | 0.0031 |
| [180–250 mg/dL] | 8.35 | −8.41 | 0.0546 |
| > 250 mg/dL | 1.13 | −3.31 | 0.0625 |
| Estimate | p-Value | ||||
|---|---|---|---|---|---|
| Parameter | Intercept | SDS/CHO | (SDS/CHO)2 | SDS/CHO | (SDS/CHO)2 |
| Analysis of all three postprandial periods (n = 238) | |||||
| Time in Range 0–120 min | |||||
| >250 mg/dL | 1.06 | −4.54 | 21.76 | 0.0003 | 0.0177 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goux, A.; Breyton, A.-E.; Meynier, A.; Lambert-Porcheron, S.; Sothier, M.; Van Den Berghe, L.; Brack, O.; Normand, S.; Disse, E.; Laville, M.; et al. Design and Validation of a Diet Rich in Slowly Digestible Starch for Type 2 Diabetic Patients for Significant Improvement in Glycemic Profile. Nutrients 2020, 12, 2404. https://doi.org/10.3390/nu12082404
Goux A, Breyton A-E, Meynier A, Lambert-Porcheron S, Sothier M, Van Den Berghe L, Brack O, Normand S, Disse E, Laville M, et al. Design and Validation of a Diet Rich in Slowly Digestible Starch for Type 2 Diabetic Patients for Significant Improvement in Glycemic Profile. Nutrients. 2020; 12(8):2404. https://doi.org/10.3390/nu12082404
Chicago/Turabian StyleGoux, Aurélie, Anne-Esther Breyton, Alexandra Meynier, Stéphanie Lambert-Porcheron, Monique Sothier, Laurie Van Den Berghe, Olivier Brack, Sylvie Normand, Emmanuel Disse, Martine Laville, and et al. 2020. "Design and Validation of a Diet Rich in Slowly Digestible Starch for Type 2 Diabetic Patients for Significant Improvement in Glycemic Profile" Nutrients 12, no. 8: 2404. https://doi.org/10.3390/nu12082404