Novel e-Health Applications for the Management of Cardiometabolic Risk Factors in Children and Adolescents in Greece

 , , ,
, , ,  , , and
, , and 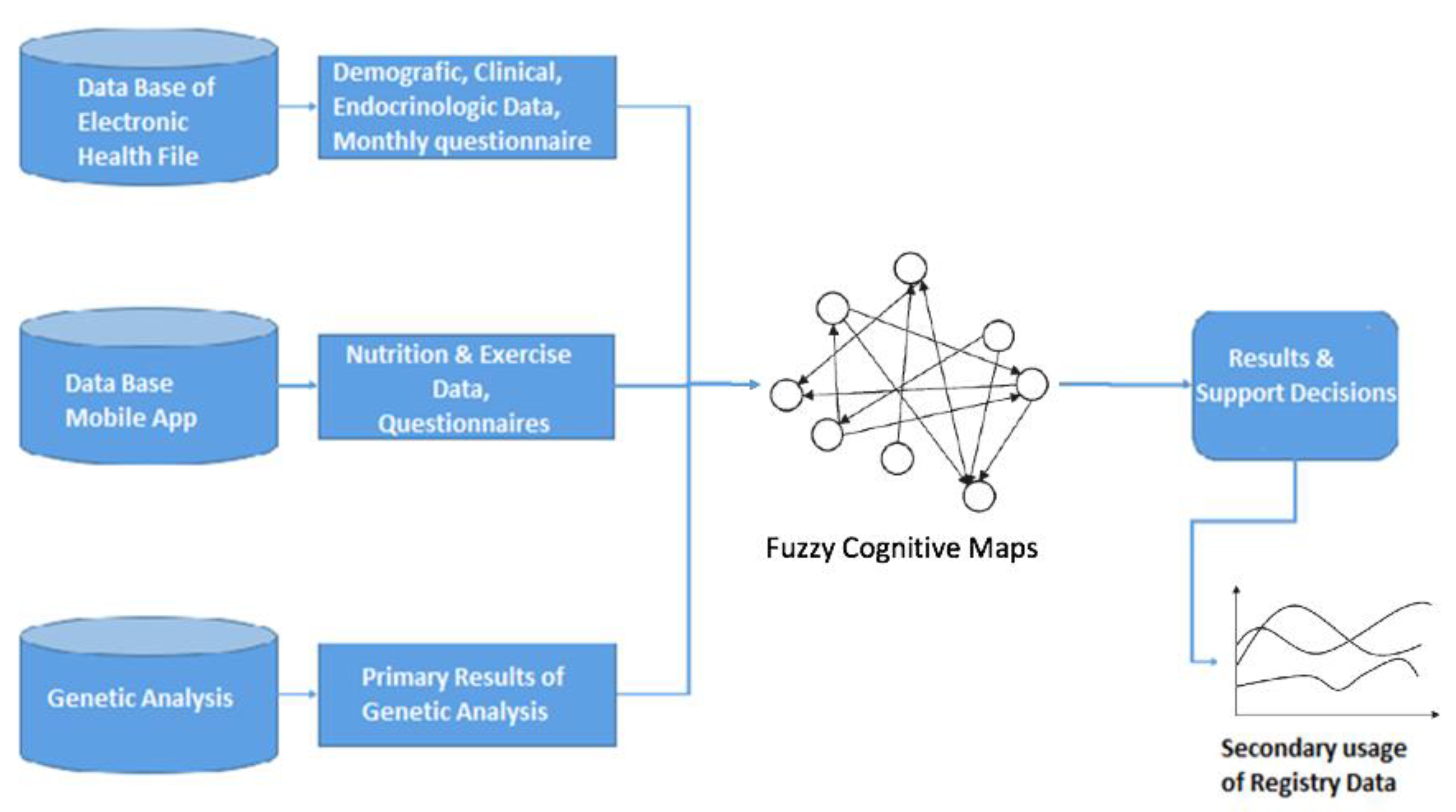{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. A/The Hellenic National Registry for the Prevention and Management of Overweight and Obesity in Childhood and Adolescence
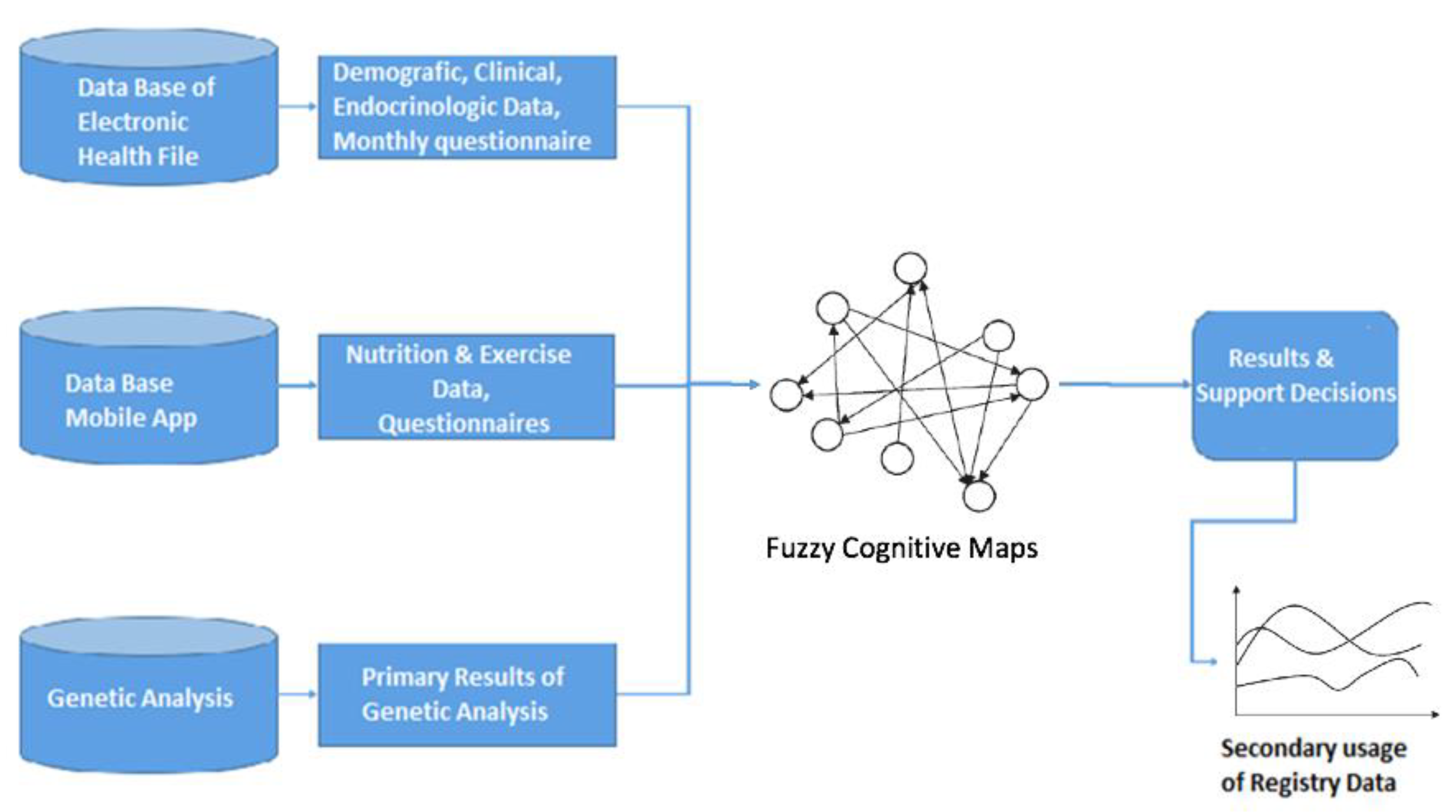
3. B/Development of Intelligent Multi-Level Information Systems and Specialized Artificial Intelligence Algorithms for Personalized Management of Obesity in Childhood and Adolescence
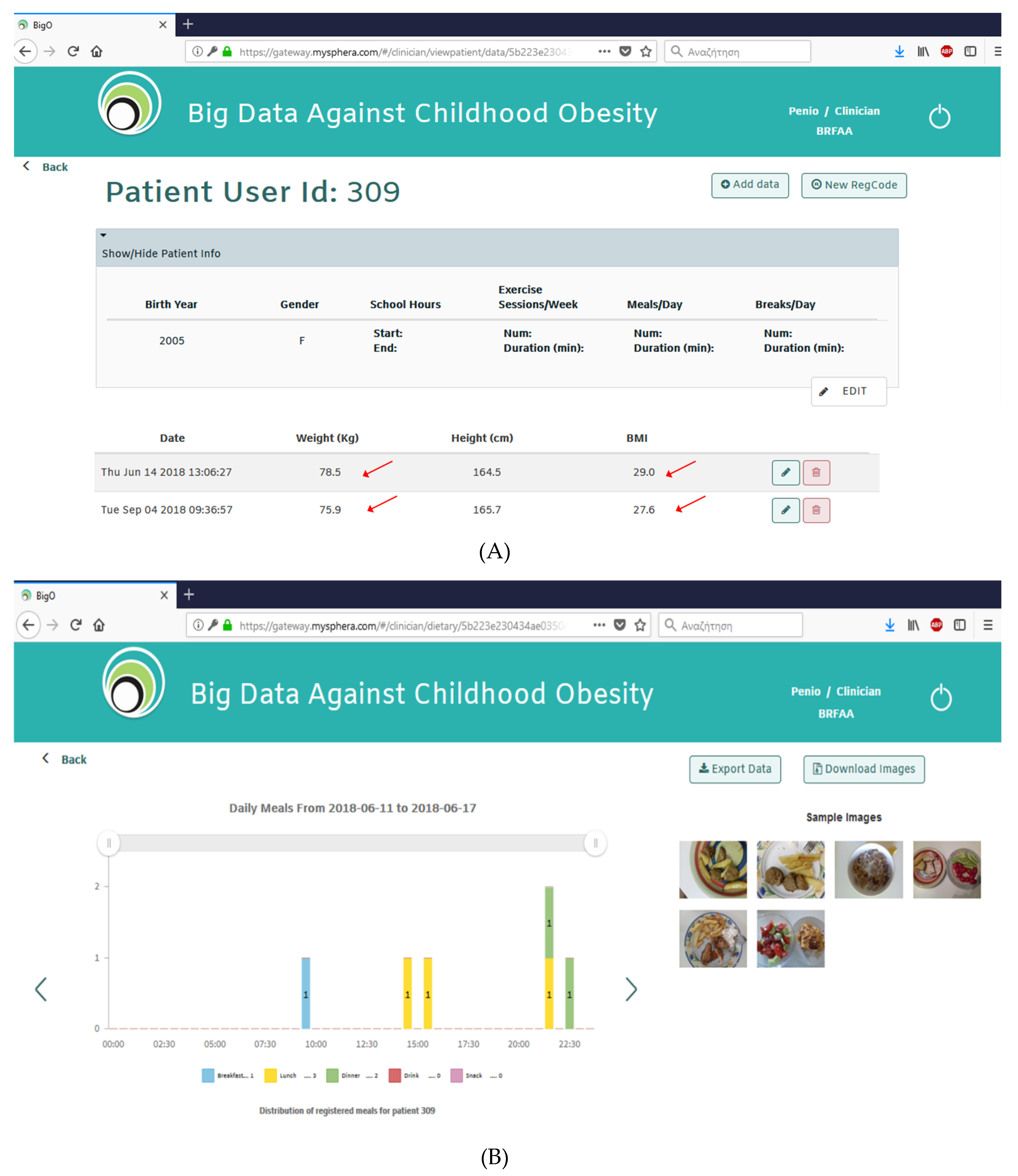
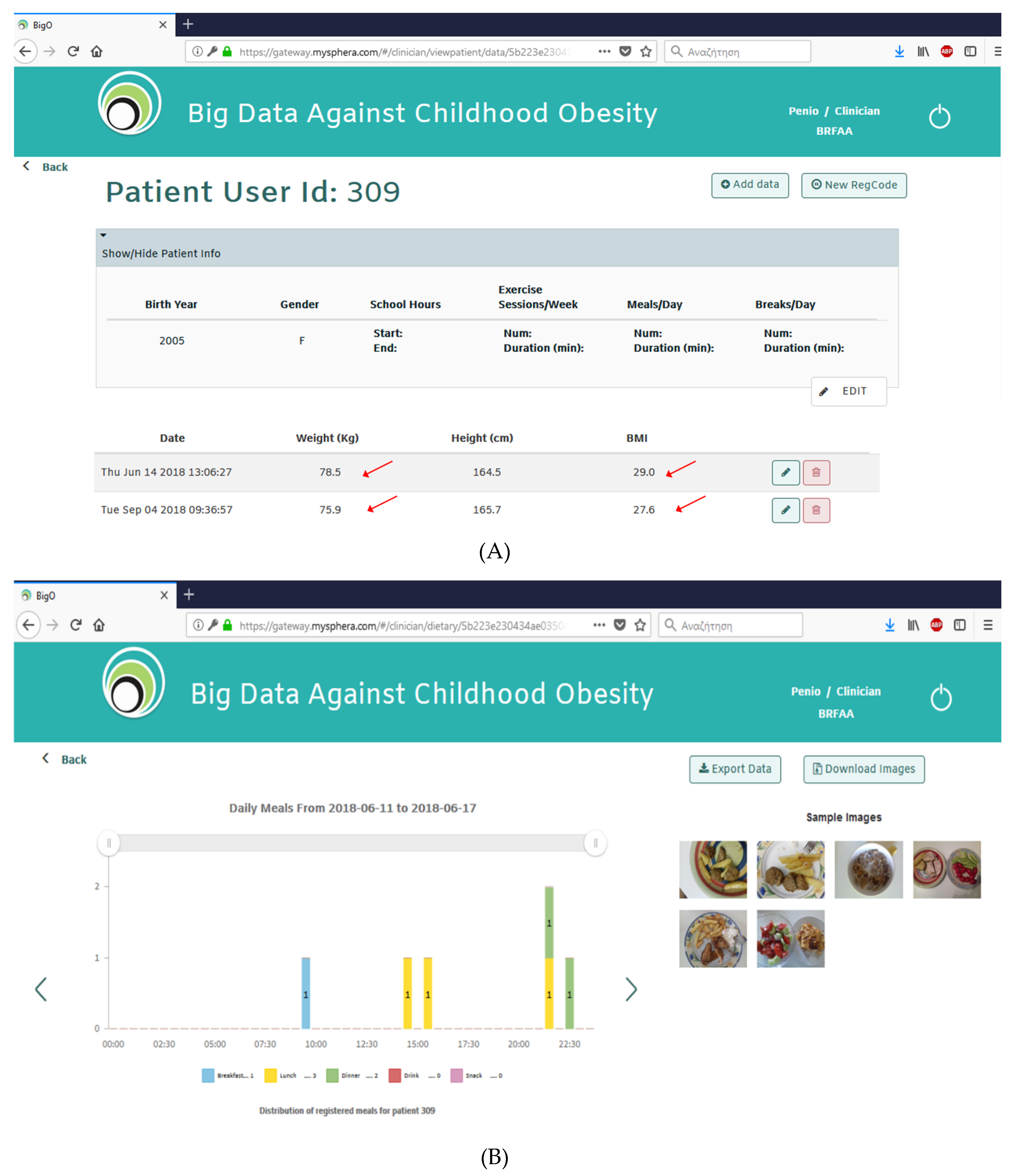
4. C/Big Data against Childhood Obesity
5. D/Decision Support Tool (DST) for Pediatric Health Care Professionals
6. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Berenson, G.S.; Srinivasan, S.R.; Bao, W. Precursors of cardiovascular risk in young adults from a biracial (black-white) population: The Bogalusa Heart Study. Ann. N. Y. Acad. Sci. 1997, 817, 189–198. [Google Scholar] [CrossRef]
- Lee, H.; Lee, D.; Guo, G.; Harris, K.M. Trends in Body Mass Index in Adolescence and Young Adulthood in the United States: 1959–2002. J. Adolesc. Health 2011, 49, 601–608. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Childhood Overweight and Obesity; WHO: Geneva, Switzerland, 2016; Available online: https://www.who.int/dietphysicalactivity/childhood/en/ (accessed on 11 May 2020).
- Brug, J.; Van Stralen, M.M.; Chinapaw, M.J.M.; De Bourdeaudhuij, I.; Lien, N.; Bere, E.; Singh, A.S.; Maes, L.; Moreno, L.; Jan, N.; et al. Differences in weight status and energy-balance related behaviours according to ethnic background among adolescents in seven countries in Europe: The ENERGY-project. Pediatr. Obes. 2012, 7, 399–411. [Google Scholar] [CrossRef]
- Nigro, J.; Osman, N.; Dart, A.; Little, P.J. Insulin Resistance and Atherosclerosis. Endocr. Rev. 2006, 27, 242–259. [Google Scholar] [CrossRef] [Green Version]
- Baker, J.L.; Olsen, L.W.; Sørensen, T.I. Childhood body-mass index and the risk of coronary heart disease in adulthood. N. Engl. J. Med. 2007, 357, 2329–2337. [Google Scholar] [CrossRef]
- Tirosh, A.; Shai, I.; Afek, A.; Dubnov-Raz, G.; Ayalon, N.; Gordon, B.; Derazne, E.; Tzur, R.; Shamis, A.; Vinker, S.; et al. Adolescent BMI trajectory and risk of diabetes versus coronary disease. N. Engl. J. Med. 2011, 364, 1315–1325. [Google Scholar] [CrossRef] [Green Version]
- Juonala, M.; Magnussen, C.G.; Berenson, G.S.; Venn, A.; Burns, T.L.; Sabin, M.A.; Srinivasan, S.R.; Daniels, S.R.; Davis, P.H.; Chen, W.; et al. Childhood Adiposity, Adult Adiposity, and Cardiovascular Risk Factors. N. Engl. J. Med. 2011, 365, 1876–1885. [Google Scholar] [CrossRef] [Green Version]
- Franks, P.W.; Hanson, R.L.; Knowler, W.C.; Sievers, M.L.; Bennett, P.H.; Looker, H.C. Childhood obesity, other cardiovascular risk factors, and premature death. N. Engl. J. Med. 2010, 362, 485–493. [Google Scholar] [CrossRef]
- De Gonzalez, A.B.; Hartge, P.; Cerhan, J.R.; Flint, A.J.; Hannan, L.; MacInnis, R.J.; Moore, S.C.; Tobias, G.; Anton-Culver, H.; Freeman, L.B.; et al. Body-mass index and mortality among 1.46 million white adults. N. Engl. J. Med. 2010, 363, 2211–2219. [Google Scholar] [CrossRef] [Green Version]
- Dobbs, R.; Sawers, C.; Thompson, F.; Manyika, J.; Woetzel, J.; Child, P.; McKenna, S.; Spatharou, A. Overcoming Obesity: An Initial Economic Analysis; McKinsey Global Institute: Jakarta, Indonesia, 2014; pp. 1–120. [Google Scholar]
- Dombrowski, S.U.; Knittle, K.; Avenell, A.; Araujo-Soares, V.; Sniehotta, F.F. Long term maintenance of weight loss with non-surgical interventions in obese adults: Systematic review and meta-analyses of randomized controlled trials. BMJ 2014, 348, 2646. [Google Scholar] [CrossRef] [Green Version]
- Khoury, M.J.; Iademarco, M.F.; Riley, W.T. Precision Public Health for the Era of Precision Medicine. Am. J. Prev. Med. 2015, 50, 398–401. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Kassari, P.; Papaioannou, P.; Billiris, A.; Karanikas, H.; Eleftheriou, S.; Thireos, E.; Manios, Y.; Chrousos, G.P.; Charmandari, E. Electronic registry for the management of childhood obesity in Greece. Eur. J. Clin. Investig. 2018, 48. [Google Scholar] [CrossRef]
- Genitsaridi, S.; Karampatsou, S.; Papageorgiou, I.; Papadopoulos, G.; Farakla, I.; Koui, E.; Georgiou, A.; Romas, S.; Terzioglou, E.; Papathanasiou, C.; et al. A Comprehensive and Multidisciplinary Management Plan is Extremely Effective at Reducing the Prevalence of Overweight and Obesity in Childhood and Adolescence. In Proceedings of the 55th Annual Meeting of the European Society for Paediatric Endocrinology (ESPE), Paris, France, 10–12 September 2016. [Google Scholar]
- Kassari, P.; Billiris, A.; Karanikas, H.; Thireos, E.; Drakoulis, N.; Manios, I.; Charmandari, E. P2-140, PEDOBESITY: Development of Intelligent Multi-level Information Systems and Specialized Artificial Intelligence Algorithms for Personalized Management of Obesity in C hildhood and Adolescence. In Proceedings of the 58th Annual Meeting of the European Society for Paediatric Endocrinology (ESPE), Vienna, Austria, 19–21 September 2019. [Google Scholar]
- Diou, C.; Ioakeimidis, I.; Charmandari, E.; Kassari, P.; Lekka, I.; Mars, M.; Bergh, C.; Kechadi, T.; Doyle, G.; O’Malley, G.; et al. P3-P127, BigO: Big Data Against Childhood Obesity. In Proceedings of the 57th Annual Meeting of the European Society for Paediatric Endocrinology (ESPE), Athens, Greece, 27–29 September 2018. [Google Scholar]
- Bergh, C.; Callmar, M.; Danemar, S.; Hölcke, M.; Isberg, S.; Leon, M.; Lindgren, J.; Lundqvist, A.; Niinimaa, M.; Olofsson, B.; et al. Effective treatment of eating disorders: Results at multiple sites. Behav. Neurosci. 2013, 127, 878–889. [Google Scholar] [CrossRef] [Green Version]
- Zandian, M.; Ioakimidis, I.; Bergh, C.; Brodin, U.; Sodersten, P. Decelerated and linear eaters: Effect of eating rate on food intake and satiety. Physiol. Behav. 2009, 96, 270–275. [Google Scholar] [CrossRef]
- Diou, C.; Sarafis, I.; Papapanagiotou, V.; Ioakimidis, I.; Delopoulos, A. A methodology for obtaining objective measurements of population obesogenic behaviors in relation to the environment. Stat. J. IAOS 2019, 35, 677–690. [Google Scholar] [CrossRef] [Green Version]
- Kröll, M.; Schnell, R. Anonymisation of geographical distance matrices via Lipschitz embedding. Int. J. Health Geogr. 2016, 15, 1. [Google Scholar] [CrossRef] [Green Version]
- Tragomalou, A.; Kassari, P.; Ioakeimidis, I.; Filis, K.; Theodoropoulou, E.; Lymperopoulos, G.; Perez-Cuevas, I.; Karavidopoulou, Y.; Diou, C.; Maramis, C.; et al. P3-101, BigO: The use of new technologies for the management of childhood obesity–A clinical pilot study. In Proceedings of the 58thAnnual Meeting of the European Society for Paediatric Endocrinology (ESPE), Vienna, Austria, 19–21 September 2019. [Google Scholar]
- Moschonis, G.; Michalopoulou, M.; Tsoutsoulopoulou, K.; Vlachopapadopoulou, E.; Michalacos, S.; Charmandari, E.; Chrousos, G.P.; Manios, Y. Assessment of the Effectiveness of a Computerised Decision-Support Tool for Health Professionals for the Prevention and Treatment of Childhood Obesity. Results from a Randomised Controlled Trial. Nutrients 2019, 11, 706. [Google Scholar] [CrossRef] [Green Version]
- Manios, Y.; on behalf of the “Healthy Growth Study” group; Birbilis, M.; Moschonis, G.; Birbilis, G.; Mougios, V.; Lionis, C.; Chrousos, G.P. Childhood Obesity Risk Evaluation based on perinatal factors and family sociodemographic characteristics: CORE Index. Eur. J. Nucl. Med. Mol. Imaging 2013, 172, 551–555. [Google Scholar] [CrossRef]
- Manios, Y.; Vlachopapadopoulou, E.; Moschonis, G.; Karachaliou, F.; Psaltopoulou, T.; Koutsouki, D.; Bogdanis, G.C.; Carayanni, V.; Hatzakis, A.; Michalacos, S. Utility and applicability of the “Childhood Obesity Risk Evaluation” (CORE)-index in predicting obesity in childhood and adolescence in Greece from early life: The “National Action Plan for Public Health”. Eur. J. Nucl. Med. Mol. Imaging 2016, 175, 1989–1996. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids; National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- World Health Organization. Food and Agriculture Organization of the United Nations. In Diet, Nutrition and the Prevention of Chronic Diseases; Report of a joint WHO/FAO expert consultation; World Health Organization: Geneva, Switzerland, 2003; Available online: http://www.fao.org/docrep/005/AC911E/AC911E00.htm (accessed on 11 May 2020).
- Marchibroda, J.M. The impact of health information technology on collaborative chronic care management. J. Manag. Care Pharm. 2008, 14, 3–11. [Google Scholar]
- Van Gemert-Pijnen, L.J.; Nijland, N.; Van Limburg, M.; Ossebaard, H.C.; Kelders, S.M.; Eysenbach, G.; Seydel, E.R.; Esser, P.; Vincent, C.; Isa, W.A.R.W.M. A Holistic Framework to Improve the Uptake and Impact of eHealth Technologies. J. Med Internet Res. 2011, 13, e111. [Google Scholar] [CrossRef]
- Dansky, K.H.; Thompson, D.; Sanner, T. A framework for evaluating eHealth research. Eval. Program Plan. 2006, 29, 397–404. [Google Scholar] [CrossRef]
- Flodgren, G.; Bradley, D.G.; Summerbell, C. Interventions to change the behaviour of health professionals and the organisation of care to promote weight reduction in children and adults with overweight or obesity. Cochrane Database Syst. Rev. 2017, 2017, CD000984. [Google Scholar] [CrossRef]
- Datta, A.K.; Jackson, V.; Nandkumar, R.; Sproat, J.; Zhu, W.; Krahling, H. CHOIS: Enabling grid technologies for obesity surveillance and control. Stud. Health Technol. Inform. 2010, 159, 191–202. [Google Scholar]
- Lycett, K.; Wittert, G.A.; Gunn, J.; Hutton, C.; Clifford, S.; Wake, M. The challenges of real-world implementation of web-based shared care software: The HopSCOTCH Shared-Care Obesity Trial in Children. BMC Med. Inform. Decis. Mak. 2014, 14, 61. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.; Lee, B.M.; Lee, Y. Development of Child-Teen Obesity Treatment Service Platform. Health Inform. Res. 2016, 22, 243–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bussenius, H.; Zeck, A.M.; Williams, B.; Haynes-Ferere, A. Surveillance of Pediatric Hypertension Using Smartphone Technology. J. Pediatr. Health Care 2018, 32, e98–e104. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Hardy, D.; Caplan, L.S. The need for culturally-tailored smartphone applications for weight control. J. Ga. Public Health Assoc. 2016, 5, 228–232. [Google Scholar] [PubMed]
- Fagerberg, P.; Langlet, B.; Oravsky, A.; Sandborg, J.; Löf, M.; Ioakimidis, I. Ultra-processed food advertisements dominate the food advertising landscape in two Stockholm areas with low vs high socioeconomic status. Is it time for regulatory action? BMC Public Health 2019, 19, 1717. [Google Scholar] [CrossRef] [PubMed]
- Maramis, C.; Ioakimidis, I.; Kilintzis, V.; Stefanopoulos, L.; Lekka, I.; Papapanagiotou, V.; Diou, C.; Delopoulos, A.; Kassari, P.; Charmandari, E.; et al. Developing a novel citizen-scientist smartphone app for collecting behavioral and affective data from children populations. In Proceedings of the MobiHealth 2019—8th EAI International Conference on Wireless Mobile Communication and Healthcare, University College Dublin, Dublin, Ireland, November 2019; Available online: https://www.researchgate.net/publication/337486336_Developing_a_novel_citizen-scientist_smartphone_app_for_collecting_behavioral_and_affective_data_from_children_population (accessed on 11 May 2020).
- Subramanian, V.; Ferrante, A.W., Jr. Obesity, inflammation, and macrophages. Nestle Nutr. Workshop Ser. Pediatr. Program 2009, 63, 151–159. [Google Scholar] [PubMed] [Green Version]
- Manios, Y.; Moschonis, G.; Chrousos, G.P.; Lionis, C.; Mougios, V.; Kantilafti, M.; Tzotzola, V.; Skenderi, K.P.; Petridou, A.; Tsalis, G.; et al. The double burden of obesity and iron deficiency on children and adolescents in Greece: The Healthy Growth Study. J. Hum. Nutr. Diet. 2012, 26, 470–478. [Google Scholar] [CrossRef]
- Huma, N.; Salim Ur, R.; Anjum, F.M.; Murtaza, M.A.; Sheikh, M.A. Food fortification strategy–Preventing iron deficiency anemia: A review. Crit. Rev. Food Sci. Nutr. 2007, 47, 259–265. [Google Scholar] [CrossRef]
- Kawade, R. Zinc status and its association with the health of adolescents: A review of studies in India. Glob. Health Action 2012, 5, 7353. [Google Scholar] [CrossRef] [PubMed]
- Kurpad, A.V.; Edward, B.S.; Aeberli, I. Micronutrient supply and health outcomes in children. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Manios, Y.; Karatzi, K.; Moschonis, G.; Ioannou, G.; Androutsos, O.; Lionis, C.; Chrousos, G. Lifestyle, anthropometric, socio-demographic and perinatal correlates of early adolescence hypertension: The Healthy Growth Study. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Villalba-Mora, E.; Casas, I.; Lupiáñez-Villanueva, F.; Maghiros, I. Adoption of health information technologies by physicians for clinical practice: The Andalusian case. Int. J. Med. Inform. 2015, 84, 477–485. [Google Scholar] [CrossRef] [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tragomalou, A.; Moschonis, G.; Manios, Y.; Kassari, P.; Ioakimidis, I.; Diou, C.; Stefanopoulos, L.; Lekka, E.; Maglaveras, N.; Delopoulos, A.; et al. Novel e-Health Applications for the Management of Cardiometabolic Risk Factors in Children and Adolescents in Greece. Nutrients 2020, 12, 1380. https://doi.org/10.3390/nu12051380
Tragomalou A, Moschonis G, Manios Y, Kassari P, Ioakimidis I, Diou C, Stefanopoulos L, Lekka E, Maglaveras N, Delopoulos A, et al. Novel e-Health Applications for the Management of Cardiometabolic Risk Factors in Children and Adolescents in Greece. Nutrients. 2020; 12(5):1380. https://doi.org/10.3390/nu12051380
Chicago/Turabian StyleTragomalou, Athanasia, George Moschonis, Yannis Manios, Penio Kassari, Ioannis Ioakimidis, Christos Diou, Leandros Stefanopoulos, Eirini Lekka, Nicos Maglaveras, Anastasios Delopoulos, and et al. 2020. "Novel e-Health Applications for the Management of Cardiometabolic Risk Factors in Children and Adolescents in Greece" Nutrients 12, no. 5: 1380. https://doi.org/10.3390/nu12051380