The Effects of Physical Activity and Diet Interventions on Body Mass Index in Latin American Children and Adolescents: A Systematic Review and Meta-Analysis

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
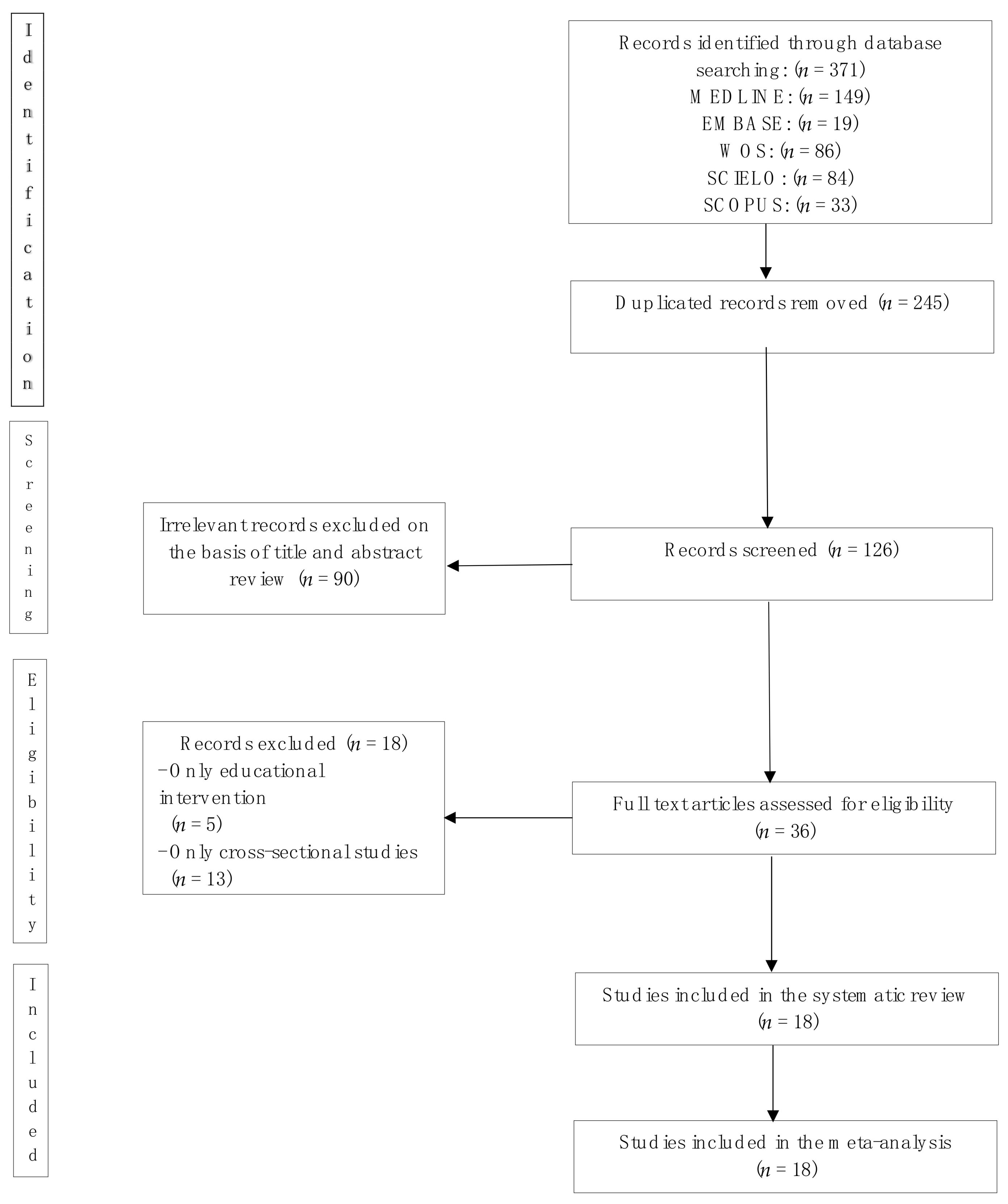
3.1. Systematic Review
3.2. Quality Assessment
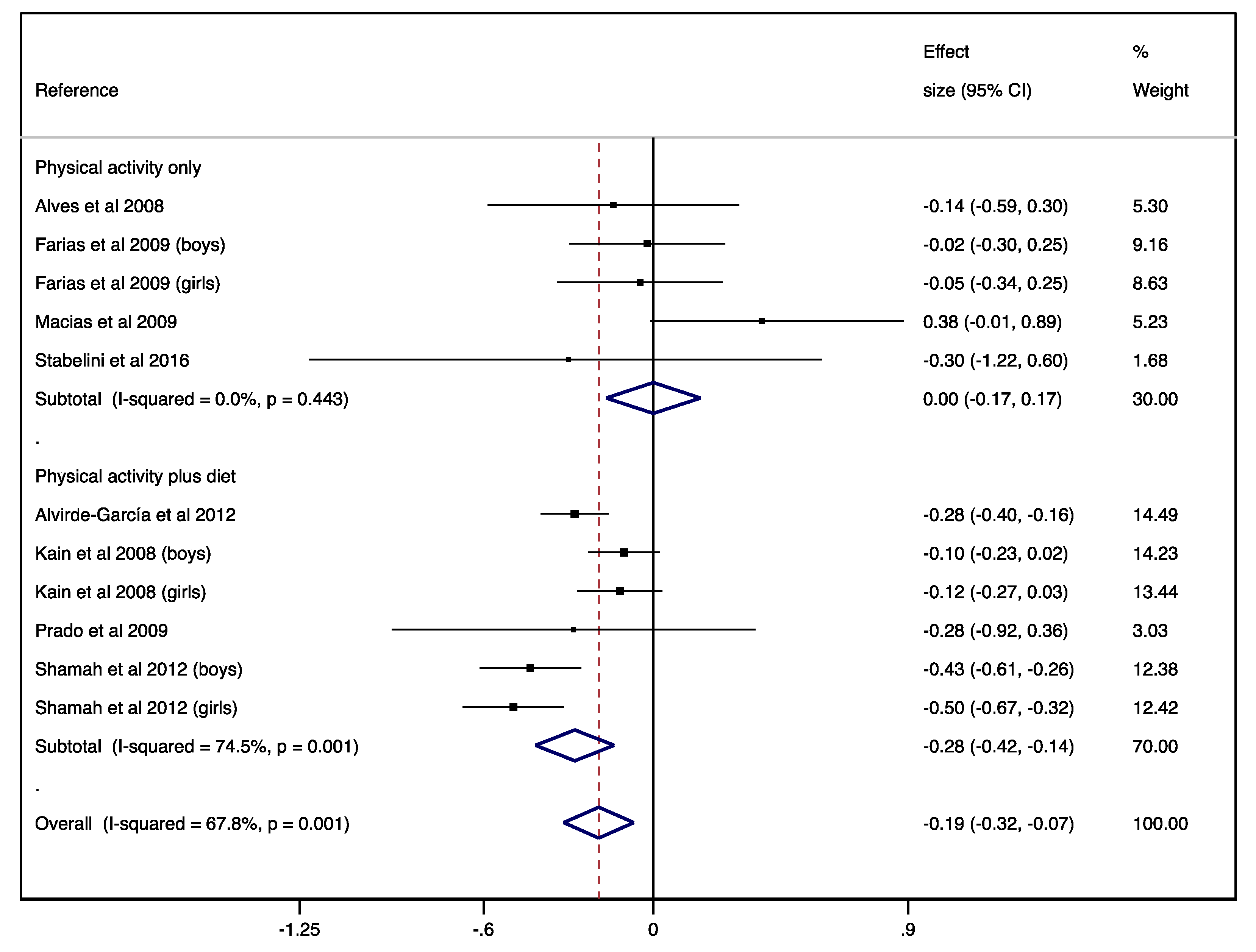
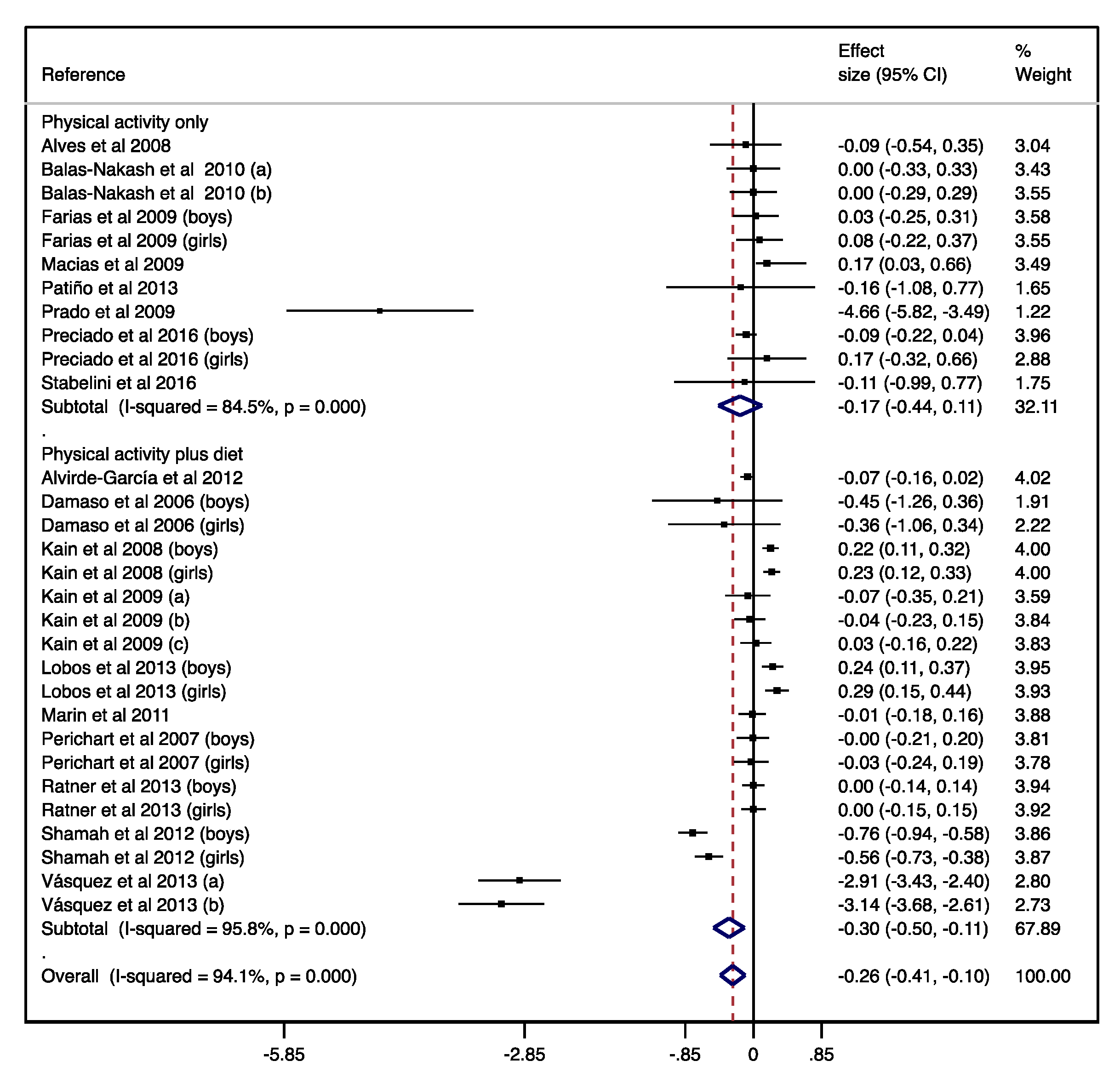
3.3. Meta-Analysis
3.4. Sensitivity Analysis
3.5. Sub-Group Analysis
3.6. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rivera, J.Á.; Cossío, T.G.; Pedraza, L.S.; Aburto, T.C.; Sánchez, T.G.; Martorell, R. Childhood and adolescent overweight and obesity in Latin America: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 321–332. [Google Scholar] [CrossRef]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodle, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- Paulis, W.D.; Silva, S.; Koes, B.W.; Van Middelkoop, M. Overweight and obesity are associated with musculoskeletal complaints as early as childhood: A systematic review. Obes. Rev. 2014, 15, 52–67. [Google Scholar] [CrossRef] [PubMed]
- Arens, R.; Muzumdar, H. Childhood obesity and obstructive sleep apnea. J. Appl. Physiol. 2010, 108, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, L.J.; Parsons, T.J.; Hill, A.J. Self-esteem and quality of life in obese children and adolescents: A systematic review. Int. J. Pediatr. Obes. 2010, 5, 282–304. [Google Scholar] [CrossRef]
- Freedman, D.S.; Mei, Z.; Srinivasan, S.R.; Berenson, G.S.; Dietz, W.H. Cardiovascular Risk Factors and Excess Adiposity Among Overweight Children and Adolescents: The Bogalusa Heart Study. J. Pediatr. 2007, 150, 12–17. [Google Scholar] [CrossRef]
- Collaboration, P.S.; Whitlock, G.; Lewington, S.; Sherliker, P.; Clarker, R.; Emberson, J.; Halsey, J.; Qisilbash, N.; Collins, R.; Peto, R.; et al. Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef]
- Wormser, D.; Kaptoge, S.; Di Angelantonio, E.; Wood, A.M.; Pennells, L.; Thompson, A.; Sarwar, N.; Kizer, J.R.; Lawlor, D.A.; Nordestgaard, B.G.; et al. Separate and combined associations of body-mass index and abdominal adiposity with cardiovascular disease: Collaborative analysis of 58 prospective studies. Lancet 2011, 377, 1085–1095. [Google Scholar]
- Danaei, G.; Ding, E.L.; Mozaffarian, D.; Taylor, B.; Rehm, J.; Murray, C.J.; Ezzati, M. The Preventable Causes of Death in the United States: Comparative Risk Assessment of Dietary, Lifestyle, and Metabolic Risk Factors. PLoS Med. 2009, 6, e1000058. [Google Scholar] [CrossRef]
- Wang, L.Y.; Chyen, D.; Lee, S.; Lowry, R. The Association Between Body Mass Index in Adolescence and Obesity in Adulthood. J. Adolesc. Heal 2008, 42, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Ward, Z.J.; Cradock, A.L.; Gortmaker, S.L.; Resch, S.C.; Long, M.W.; Giles, C.M. Simulation of Growth Trajectories of Childhood Obesity into Adulthood. N. Engl. J. Med. 2017, 377, 2145–2153. [Google Scholar] [CrossRef]
- Dietz, W.H.; Robinson, T.N. Use of the body mass index (BMI) as a measure of overweight in children and adolescents. J. Pediatr. 1998, 132, 191–193. [Google Scholar] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Faith, M.S.; Pietrobelli, A.; Heo, M. What is the best measure of adiposity change in growing children: BMI, BMI %, BMI z-score or BMI centile? Eur. J. Clin. Nutr. 2005, 59, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef]
- Poskitt, E. Body mass index and child obesity: Are we nearing a definition? Acta Paediatr. 2007, 89, 507–509. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Faith, M.S.; Allison, D.B.; Gallagher, D.; Chiumello, G.; Heymsfield, S.B. Body mass index as a measure of adiposity among children and adolescents: A validation study. J. Pediatr. 1998, 132, 204–210. [Google Scholar] [CrossRef]
- Maynard, L.M.; Wisemandle, W.; Roche, A.F.; Chumlea, W.C.; Guo, S.S.; Siervogel, R.M. Childhood body composition in relation to body mass index. Pediatrics 2001, 107, 344–350. [Google Scholar] [CrossRef]
- Demerath, E.W.; Schubert, C.M.; Maynard, L.M.; Sun, S.S.; Chumlea, W.C.; Pickoff, A.; Czerwinski, S.A.; Towne, B.; Siervogel, R.M. Do changes in body mass index percentile reflect changes in body composition in children? Data from the Fels Longitudinal Study. Pediatrics 2006, 117, 487–495. [Google Scholar] [CrossRef]
- McGovern, L.; Johnson, J.N.; Paulo, R.; Hettinger, A.; Shinghal, V.; Kamath, C.; Erwin, P.J.; Montori, V.M. Treatment of pediatric obesity: A systematic review and meta-analysis of randomized trials. J. Clin. Endocrinol. Metab. 2008, 93, 4600–4605. [Google Scholar] [CrossRef]
- Kamath, C.C.; Vickers, K.S.; Ehrlich, A.; McGovern, L.; Shinghal, V.; Paulo, R.; Hettinger, A.; Erwin, P.J.; Montori, V.M. Behavioral interventions to prevent childhood obesity: A systematic review and metaanalyses of randomized trials. J. Clin. Endocrinol. Metab. 2008, 93, 4606–4615. [Google Scholar] [CrossRef] [PubMed]
- Lipnowski, S.; LeBlanc, C. Healthy active living: Physical activity guidelines for children and adolescents. Paediatr. Child. Health 2012, 17, 209–210. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S. Effects of Exercise in the Treatment of Overweight and Obese Children and Adolescents: A Systematic Review of Meta-Analyses. J. Obes. 2013, 2013, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.; Davis, K. Obesity and Physical Activity. Psychiatr. Clin. N. Am. 2011, 34, 829–840. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Estrategia Mundial Sobre Regimen Alimentario, Actividad Física Y Salud. Resolución 57.17. Available online: https://www.who.int/dietphysicalactivity/strategy/eb11344/strategy_spanish_web.pdf (accessed on 21 January 2020).
- Bleich, S.N.; Vercammen, K.A.; Zatz, L.Y.; Frelier, J.M.; Ebbeling, C.B.; Peeters, A. Intevrentions to prevent global childhood overweight and obesity: A systematic review. Lancet Diabetes Endocrinol. 2018, 6, 332–346. [Google Scholar] [CrossRef]
- Friedrich, R.; Schuch, I.; Wagner, M. Effect of interventions on the body mass index of school-age students. Rev. Saúde Pública 2012, 46, 551–560. [Google Scholar] [CrossRef]
- Hoehner, C.M.; Soares, J.; Parra-Pérez, D.; Ribeiro, I.C.; Joshu, C.E.; Pratt, M.; Legetic, B.D.; Malta, D.C.; Matsudo, B.R.; Ramos, L.R.; et al. Physical Activity Interventions in Latin America. Am. J. Prev. Med. 2008, 34, 224–233. [Google Scholar] [CrossRef]
- Nagle, B.J.; Holub, C.K.; Barquera, S.; Sánchez-Romero, L.; Eisenberg, C.; Rivera-Dommarco, J.; Mehta, S.; Lobelo, F.; Arredondo, E.; Elder, J. Interventions for the treatment of obesity among children and adolescents in Latin America: A systematic review. Salud Publica Mex. 2013, 55, 434–440. [Google Scholar] [CrossRef]
- Navarrete, J.A.M.; Villamil, S.S.G.; Bautista, J.E.C.; Meneses-Echávez, J.F.; González-Jiménez, E.; Schmidt-Riovalle, J. Efectividad de las intervenciones educativas realizadas en América Latina para la prevención del sobrepeso y obesidad infantil en niños escolares de 6 a 17 años: Una revisión sistemática. Nutr. Hosp. 2015, 31, 102–114. [Google Scholar]
- Lobelo, F.; Garcia de Quevedo, I.; Holub, C.K.; Nagle, B.J.; Arredondo, E.M.; Barquera, S.; Elder, J.P. School-based programs aimed at the prevention and treatment of obesity: Evidence-based interventions for youth in latin america. J. Sch. Health 2013, 83, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Larissa, S.; Clarke, M.; Ghersi, D.; Liberati, A.; Peticrew, M.; Stewart, L.A.; PRISMA-P, G. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Review of Interventions. 5.1.0. (Updated March 2011). The Cochare Collaboration, UK. 2011. Available online: https://handbook.cochrane.org (accessed on 1 May 2019).
- Godoy-Cumillaf, A.; Díaz, A.; Álvarez-Bueno, C.; Martínez-Vizcaíno, V.; Cavero-Redondo, I. Effects of physical-activity interventions on the body mass index of children and adolescents in Latin America: A protocol for a systematic review and meta-analysis. BMJ Open 2019, 9, e030332. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.; Campbell, M.; Campbell, M.; Dahota, A.; Giraudeau, B.; Higgins, J.; Reeves, B.; Siegfried, N. Revised Cochrane risk of Bias Tool for Randomized Trials (RoB 2.0): Additional Considerations for Cluster-Randomized Trials. The Cochrane Collaboration. Available online: https://www.riskofbias.info (accessed on 13 November 2019).
- Hamilton, O.; McMaster, U. National Collaborating Centre for Methods and Tool. Qual. Assess. Tool Quant. Stud. 2008. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: Hillsdale, MI, USA, 1988; pp. 20–26. [Google Scholar]
- Langan, D.; Higgins, J.P.T.; Jackson, D.; Bowner, J.; Kontopantelis, E.; Viechtbauer, W.; Simmonds, M. A comparison of heterogeneity variance estimators in simulated random-effects meta-analyses. Res. Synth. Methods 2019, 10, 83–98. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M.; Smith, G.D. Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ 2001, 323, 101–105. [Google Scholar] [CrossRef]
- Alves, J.G.B.; Galé, C.R.; Souza, E.; Batty, G.D. Efeito do exercício físico sobre peso corporal em crianças com excesso de peso: Ensaio clínico comunitário randomizado em uma favela no Brasil. Cad. Saude Publica 2008, 24, 353–359. [Google Scholar] [CrossRef]
- Alvirde-García, U.; Rodríguez-Guerrero, A.J.; Henao-Morán, S.; Gómez-Pérez, F.J.; Aguilar-Salinas, C.A. Resultados de un programa comunitario de intervención en el estilo de vida en niños. Salud Publica Mex. 2013, 55, 406–414. [Google Scholar]
- Balas-Nakash, M.; Benítez-Arciniega, A.; Perichart-Perera, O.; Valdés-Ramos, R.; Vadillo-Ortega, F. The effect of exercise on cardiovascular risk markers in Mexican school-aged children: Comparison between two structured group routines. Salud Publica Mex. 2010, 52, 398–405. [Google Scholar] [CrossRef]
- Dâmaso, A.R.; Tock, L.; Tufik, S.; Prado, W.; Stella, S.; Fisberg, M.; Cintra, I.; Caranti, D.; Siquiera, K.; Nascimento, C.; et al. Tratamento multidisciplinar reduz o tecido adiposo visceral, leptina, grelina e a prevalência de esteatose hepática não alcoólica (NAFLD) em adolescentes obesos. Rev. Bras. Med. Esporte. 2006, 12, 263–267. [Google Scholar] [CrossRef][Green Version]
- Farias, E.S.; Paula, F.; Carvalho, W.R.G.; Gonçalves, E.M.; Baldin, A.D.; Guerra, G. Efeito da atividade física programada sobre a composiçã o corporal em escolares adolescentes. J. Pediatr. (Rio J.) 2009, 85, 28–34. [Google Scholar]
- Kain, J.; Uauy, R.; Leyton, B.; Cerda, R.; Olivares, S.; Vio, F. Effectiveness of a dietary and physical activity intervention to prevent obesity in school age children. Rev. Med. Chil. 2008, 136, 22–30. [Google Scholar] [PubMed]
- Kain, J.; Concha, F.; Salazar, G.; Leyton, B.; Rodríguez, M.; Ceballos, X.; Vio, F. Prevención de obesidad de preescolares y escolares de escuelas municipales de una comuna de Santiago de Chile: Proyecto piloto 2006. ALAN 2009, 59, 139–146. [Google Scholar]
- Lobos, L.; Leyton, B.; Kain, J.; Vio, F. Evaluación de una intervención educativa para la prevención de la obesidad infantil en escuelas básicas de Chile. Nutr. Hosp. 2013, 28, 1156–1164. [Google Scholar]
- Macias-Cervantes, M.H.; Malacara, J.M.; Garay-Sevilla, M.E.; Díaz-Cisneros, F.J. Effect of recreational physical activity on insulin levels in Mexican/Hispanic children. Eur. J. Pediatr. 2009, 168, 1195–1202. [Google Scholar] [CrossRef]
- Marín, B.V.; Rodríguez, O.L.; Buscaglione, A.R.; Aguirre, M.; Burrows, R.; Hodgson, M.; Pizarro, T. Programa MINSAL-FONASA para Tratamiento de la Obesidad Infanto-Juvenil. Rev. Chil. Pediatría 2011, 82, 21–28. [Google Scholar] [CrossRef]
- Patiño, F.; Márquez, J.; Uscátegui, R.; Estrada, A.; Agudelo, G.; Manjarrés, L.; Parra, B.; Parra, M.; Bedoya, J.; Velásquez, C. Efecto de una intervención con ejercicio físico y orientación nutricional sobre componentes del síndrome metabólico en jóvenes con exceso de peso. Iatreia. 2013, 26, 34–43. [Google Scholar]
- Perichart-Perera, O.; Balas-Nakash, M.; Ortiz-Rodríguez, V.; Morán-Zenteno, J.; Guerrero-Ortiz, J.; Vadillo-Ortega, F. Programa para mejorar marcadores de riesgo cardiovascular en escolares mexicanos. Salud Publica Mex. 2008, 50, 218–226. [Google Scholar] [CrossRef]
- Prado, D.M.; Silva, A.G.; Trombetta, I.C.; Ribeiro, M.; Nicolau, C.; Guazzelli, I.; Matos, L.; Negrao, C.; Villares, S. Weight loss associated with exercise training restores ventilatory efficiency in obese children. Int. J. Sports Med. 2009, 30, 821–826. [Google Scholar] [CrossRef]
- Preciado-Martínez, D.C.; Mancera-Soto, E.M.; Hernández-Álvarez, E.D.; Zapata, D.M.; Mena-Bejarano, B. Eficacia de las modalidades deportivas del programa 40 × 40 en escolares con sobrepeso y obesidad. Rev. Fac. Med. 2016, 64, 143–150. [Google Scholar] [CrossRef]
- Ratner, G.; Durán, S.; Garrido, M.J.; Balmaceda, S.; Jadue, L.; Atalah, E. Impacto de una intervención en alimentación y actividad física sobre la prevalencia de obesidad en escolares. Nutr. Hosp. 2013, 28, 1508–1514. [Google Scholar]
- Shamah, L.; Morales, C.; Amaya, C.; Salazar, A.; Jiménez, A.; Méndez, I. Effectiveness of a diet and physical activity promotion strategy on the prevention of obesity in Mexican school children. BMC Public Health 2012, 12, 152. [Google Scholar] [CrossRef] [PubMed]
- Stabelini, A.; Corrêa, R.C.; De Farias, J.P.; Castilho, G.; Ferreira, C.; Márques, R.; Ferreira, W. Effects of an intervention with pedometer on metabolic risk in obese children. Rev. Bras. Med. Esporte. 2016, 22, 476–479. [Google Scholar]
- Vásquez, F.; Díaz, E.; Lera, L.; Meza, J.; Salas, I.; Rojas, P.; Atalah, E.; Burrows, R. Impacto del ejercicio de fuerza muscular en la prevención secundaria de la obesidad infantil; Intervención al interior del sistema escolar. Nutr. Hosp. 2013, 28, 347–356. [Google Scholar]
- Gonzalez-Suarez, C.; Worley, A.; Grimmer-Somers, K.; Dones, V. School-Based Interventions on Childhood Obesity. A Meta-Analysis. Am. J. Prev. Med. 2009, 37, 418–427. [Google Scholar] [CrossRef]
- Lavelle, H.V.; MacKay, D.F.; Pell, J.P. Systematic review and meta-analysis of school-based interventions to reduce body mass index. J. Public Heal (United Kingdom) 2012, 34, 360–369. [Google Scholar]
- Martín-Matillas, M.; Carbonell-Baeza, A.; Aparicio, V.A.; Delgado-Fernández, M.; Rocha, D. Efectos de los programas de intervencion enfocados al tratamiento del sobrepeso/obesidad infantil y adolescente. Rev. Andaluza Med. Deport. 2014, 7, 33–43. [Google Scholar]
- Pozuelo-Carrascosa, D.P.; García-Hermoso, A.; Álvarez-Bueno, C.; Sánchez-López, M.; Martinez-Vizcaino, V. Effectiveness of school-based physical activity programmes on cardiorespiratory fitness in children: A meta-Analysis of randomised controlled trials. Br. J. Sports Med. 2018, 52, 1234–1240. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S.; Pate, R.R. Exercise and BMI in Overweight and Obese Children and Adolescents: A Systematic Review and Trial Sequential Meta-Analysis. Biomed. Res. Int. 2015, 2015, 1–17. [Google Scholar] [CrossRef]
- Zolotarjova, J.; ten Velde, G.; Vreugdenhil, A.C.E. Effects of multidisciplinary interventions on weight loss and health outcomes in children and adolescents with morbid obesity. Obes. Rev. 2018, 19, 931–946. [Google Scholar] [CrossRef]
- Mead, E.; Brown, T.; Rees, K.; Azevedo, L.B.; Whittaker, V.; Jones, D.; Olajide, J.; Mainardi, G.M.; Corpeleijn, E.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 2017, 22, CD012651. [Google Scholar] [CrossRef] [PubMed]
- Al-khudayry, L.; Loveman, E.; Colquitt, J.L.; Mead, E.; Johnson, R.E.; Fraser, H.; Olajide, J.; Murphy, M.; Velho, R.M.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane Database Syst. Rev. 2017, 22, CD012691. [Google Scholar] [CrossRef] [PubMed]
- Lehnert, T.; Sonntag, D.; Konnopka, A.; Riedel-Heller, S.; KöniG, H.H. Economic costs of overweight and obesity. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Bürgi, F.; Meyer, U.; Granacher, U.; Schindler, C.; Marques-Vidal, P.; Kriemler, S.; Puder, J.J. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: A cross-sectional and longitudinal study (Ballabeina). Int. J. Obes. 2011, 35, 937–944. [Google Scholar] [CrossRef]
- Tanaka, C.; Hikihara, Y.; Ohkawara, K.; Tanaka, S. Locomotive and non-locomotive activity as determined by triaxial accelerometry and physical fitness in Japanese preschool children. Pediatr. Exerc. Sci. 2012, 24, 420–434. [Google Scholar] [CrossRef]
- Tomporowski, P.D.; Davis, C.L.; Miller, P.H.; Naglieri, J.A. Exercise and children’s intelligence, cognition, and academic achievement. Educ. Psychol. Rev. 2008, 20, 111–131. [Google Scholar] [CrossRef]
- Vameghi, R.; Shams, A.; Dehkordi, P.S. The effect of age, sex and obesity on fundamental motor skills among 4 to 6 years-old children. Pak. J. Med. Sci. 2012, 29, 586–590. [Google Scholar] [CrossRef]
- Brown, T.; Summerbell, C. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: An update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obes. Rev. 2009, 10, 110–141. [Google Scholar] [CrossRef]
- Katz, D.L. School-Based Interventions for Health Promotion and Weight Control: Not Just Waiting on the World to Change. Annu. Rev. Public Health 2009, 30, 253–272. [Google Scholar] [CrossRef]
- Waters, E.; De Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C. Interventions for preventing obesity in children. Sao Paulo Med. J. 2014, 132, 128–129. [Google Scholar] [CrossRef]
- Khambalia, A.Z.; Dickinson, S.; Hardy, L.L.; Gill, T.; Baur, L.A. A synthesis of existing systematic reviews and meta-analyses of school-based behavioural interventions for controlling and preventing obesity. Obes. Rev. 2012, 13, 214–233. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.S.; Mulder, C.; Twisk, J.W.R.; Van Mechelen, W.; Chinapaw, M.J.M. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Organizacion de las Naciones Unidas para la Alimentacion y la Agricultura-FAO y la Organizacion Panamericana de la Salud-OPS. América Latina y el Caribe: Panorama de La Seguridad Alimentaria y Nutricional; Organización Panamericana de la Salud: Santiago de, Chile, 2017; Available online: http://www.fao.org/3/CA2127ES/ca2127es.pdf (accessed on 10 January 2020).




{kind=link}
{kind=link}
{kind=link}
| Search Set | Medline | Search Set | Medline |
|---|---|---|---|
| #1 | physical activity [tw] | #18 | paediatric obesity [mh] |
| #2 | physical exercise [tw] | #19 | adolescents [tiab] |
| #3 | physical performance [tw] | #20 | youth [tiab] |
| #4 | exercise program* [tiab] | #21 | 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 |
| #5 | physical fitness [mh] | #22 | underweight [tw] |
| #6 | exercise [mh] | #23 | normal weight [tw] |
| #7 | 1 OR 2 OR 3 OR 4 OR 5 OR 6 | #24 | overweight [tw] |
| #8 | training program* [tiab] | #25 | BMI [tiab] |
| #9 | prevention program* [tiab] | #26 | obesity [tiab] |
| #10 | intervention program* [tiab] | #27 | body mass index [mh] |
| #11 | promotion [tw] | #28 | 22 OR 23 OR 24 OR 25 OR 26 OR 27 |
| #12 | strategy [tw] | #29 | studies [tiab] |
| #13 | 8 OR 9 OR 10 OR 11 OR 12 | #30 | randomised controlled trials [tiab] |
| #14 | childhood obesity [tiab] | #31 | RCT [tiab] |
| #15 | obese children [tiab] | #32 | non-randomised experimental [tiab] |
| #16 | obesity prevention [tiab] | #33 | single-arm pre-post [tiab] |
| #17 | obesity review [tiab] | #34 | 29 OR 30 OR 31 OR 32 OR 33 |
| #35 | 7 AND 13 AND 21 AND 28 AND 34 |
| Population Characteristics | Intervention Characteristics | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Reference | Country | Study Design | Age Distribution | Sample Size | Type of Population | Physical Activity Intervention | Physical Activity Characteristics | Diet Intervention | Diet Characteristics |
| Alves et al. 2008 [41] | Brazil | RCT | 5–10 | 78 | Overweight and obese | In school, RS | 150 min/week, 24 weeks total | - | - |
| Alvirde-García et al. 2013 [42] | Mexico | RCT | 9 (average) | 1224 | General | In school, LA | Not specified | Diet intervention and nutritional education | Intervening in the food provided, informative texts provided to students |
| Balas-Nakash el al. 2010 [43] | Mexico | Pre-post intervention | 8–12 | 319 | General | In school, Gym, AER, and dance | 20–40 min/week, 12 weeks total | - | - |
| Dâmaso et al. 2006 [44] | Brazil | Pre-post intervention | 15–18 | 28 | Obese | In PAL, RS | 120 min/week, 12 weeks total | Diet intervention | Nutritional counselling every 3 weeks with a specialist |
| Farias et al. 2009 [45] | Brazil | Non-RCT | 10–15 | 383 | General | In school, monitored physical activity | 120 min/week, 48 weeks total | - | - |
| Kain et al. 2008 [46] | Chile | Non-RCT | 6–12 | 2039 | General | In school, SW | 90 min/week, 44 weeks total | Nutritional education | Educational material provided to students, teachers, and guardians |
| Kain et al 2009 [47] | Chile | Pre-post intervention | 4–9 | 522 | General | In school, SW | Not specified | Nutritional education | Educational materials provided to students and teachers |
| Lobos et al. 2013 [48] | Chile | Pre-post intervention | 4–11 | 796 | General | In school, physical education classes | 240 min/week, 72 weeks total | Nutritional education | Educational materials about how to select healthy foods |
| Macias et al. 2010 [49] | Mexico | RCT | 6–9 | 76 | General | In school, LA | 180 min/week, 12 weeks total | - | - |
| Marín et al. 2011 [50] | Chile | Pre-post intervention | 6–18 | 268 | Obese | In school, physical activity, AER, ANAER | 60 min/week, 16 weeks total | Nutritional education | Handing out educational material for students and guardians |
| Patiño et al. 2013 [51] | Colombia | Pre-post intervention | 7–11 | 9 | Obese | Health clinic, AER, S | 270 min/week, 12 weeks total | - | - |
| Perichart et al. 2007 [52] | Mexico | Pre-post intervention | 8–14 | 360 | General | In school, exercises: S, FLEX, B, and relaxation | 100 min/week, 16 weeks total | Nutritional counselling | Messages during class time |
| Prado et al. 2009 [53] | Brazil | RCT | 8–12 | 48 | Obese | In PAL, AER, and G | 60 min/week, 16 weeks total | - | - |
| Preciado et al. 2016 [54] | Colombia | Non-RCT | 6–17 | 1003 | General | In school, beginners’ sports | 240 min/week, 8 weeks total | - | - |
| Ratner et al. 2013 [55] | Chile | Pre-post intervention | 6–9 | 2527 | General | In school, games and dance | 90 min/week, 40 weeks total | Nutritional and diet education | Educational meetings about breakfast, nutritional labels, and snacks, among others |
| Shamah et al. 2012 [56] | Mexico | RCT | 10–14 | 997 | Overweight and obese | In school, games during recess | 30 min/week 24 weeks total | Diet intervention | Lowering the caloric content of breakfast and including fruits and vegetables |
| Stabelini et al. 2016 [57] | Brazil | RCT | 8–10 | 19 | Obese | Counselling, increasing the number of steps taken every other day, and games | Every day, 12 weeks total | - | - |
| Vásquez et al. 2013 [58] | Chile | Pre-post intervention | 8–13 | 120 | Obese | In school, strength training | 135 min/week, 12 weeks total | Educational group meetings | Information about nutrition and healthy diet for students and guardians |
| COCHRANE COLLABORATIONS | Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other Bias | Risk of Bias |
|---|---|---|---|---|---|---|---|
| Alves et al. 2008 [41] | Low | Low | Low | Low | Unclear | Unclear | Low |
| Alvirde et al. 2013 [42] | High | Unclear | Low | High | Unclear | Unclear | High |
| Macías et al. 2009 [49] | Unclear | Unclear | High | Low | Unclear | Unclear | High |
| Prado et al. 2009 [53] | Unclear | Low | Unclear | Unclear | Unclear | Unclear | High |
| Shamah et al. 2012 [56] | Low | Low | Low | Low | Unclear | Unclear | Low |
| Stabelini et al. 2016 [57] | Unclear | Low | Unclear | Unclear | Unclear | Unclear | High |
| EPHPP | Selection bias | Study design | Confounders | blinding | Data collection | Withdrawals/drop-outs | Risk of bias |
| Balas et al. 2010 [43] | Moderate | Weak | Moderate | Weak | Strong | Moderate | Moderate |
| Dâmaso et al. 2006 [44] | Moderate | Moderate | Strong | Moderate | Strong | Moderate | Moderate |
| Farias et al. 2009 [45] | Low | Strong | Moderate | Moderate | Low | Moderate | Moderate |
| Kain et al. 2008 [46] | Low | Moderate | Moderate | Low | Moderate | Moderate | Moderate |
| Kain et al. 2009 [47] | Strong | Moderate | Moderate | Strong | Moderate | Strong | Moderate |
| Lobos et al. 2013 [48] | Moderate | Weak | Strong | Moderate | Moderate | Moderate | Moderate |
| Marín et al. 2011 [50] | Strong | Moderate | Moderate | Moderate | Moderate | Moderate | Moderate |
| Patiño et al. 2013 [51] | Weak | Weak | Moderate | Moderate | Moderate | Weak | Weak |
| Perichart et al. 2008 [52] | Moderate | Weak | Weak | Moderate | Moderate | Moderate | Moderate |
| Preciado et al. 2016 [54] | Moderate | Weak | Moderate | Moderate | Strong | Moderate | Moderate |
| Ratner et al. 2013 [55] | Moderate | Moderate | Strong | Strong | Strong | Moderate | Moderate |
| Vásquez et al. 2013 [58] | Strong | Moderate | Moderate | Strong | Strong | Moderate | Moderate |
| Physical Activity Only | Physical Activity Plus Diet | |||||||
|---|---|---|---|---|---|---|---|---|
| Subgroup | n | ES | I2 | p | n | ES | I2 | p |
| (95%CI) | (95%CI) | |||||||
| Intervention versus control effect | ||||||||
| Study design | ||||||||
| RCT | 3 | 0.05 | 40.8 | 0.185 | 4 | −0.38 | 36.3 | 0.194 |
| (−0.36, 0.46) | (−0.50, −0.26) | |||||||
| Non-RCT | 3 | −0.03 | 0.0 | 0.902 | 2 | −0.11 | 0.0 | 0.887 |
| (−0.23, 0.17) | (−0.21, −0.01) | |||||||
| Sex | ||||||||
| Boys | 1 | −0.02 | - | - | 2 | −0.26 | 88.5 | 0.003 |
| (−0.30, 0.25) | (−0.59, 0.06) | |||||||
| Girls | 1 | −0.05 | - | - | 2 | −0.30 | 90.1 | 0.002 |
| (−0.34, 0.25) | (−0.67, 0.07) | |||||||
| Both | 3 | 0.05 | 40.8 | 0.185 | 2 | −0.28 | 0.0 | 0.991 |
| (−0.36, 0.46) | (−0.40, −0.16) | |||||||
| Weight status | ||||||||
| Overweight/obese | 2 | −0.17 | 0.0 | 0.758 | 3 | −0.46 | 0.0 | 0.772 |
| (−0.57, 0.23) | (−0.58, −0.33) | |||||||
| General population | 3 | 0.05 | 27.9 | 0.250 | 3 | −0.17 | 56.9 | 0.098 |
| (−0.17, 0.27) | (−0.29, −0.06) | |||||||
| Pre-post intervention effect | ||||||||
| Study design | ||||||||
| RCT | 4 | −1.05 | 95.1 | <0.001 | 3 | −0.46 | 96.5 | <0.001 |
| (−2.33, 0.24) | (−0.90, −0.01) | |||||||
| Non-RCT | 4 | −0.04 | 0.0 | 0.552 | 2 | 0.22 | 0.0 | 0.859 |
| (−0.15, 0.07) | (0.15, 0.29) | |||||||
| Single-arm pre-post study | 3 | −0.01 | 0.0 | 0.948 | 14 | −0.38 | 95.5 | <0.001 |
| (−0.22, 0.21) | (−0.64, −0.11) | |||||||
| Sex | ||||||||
| Boys | 2 | −0.07 | 0.0 | 0.451 | 6 | −0.09 | 94.8 | <0.001 |
| (−0.19, 0.05) | (−0.39, 0.21) | |||||||
| Girls | 2 | 0.10 | 0.0 | 0.756 | 6 | −0.04 | 92.9 | <0.001 |
| (−0.15, 0.35) | (−0.30, 0.23) | |||||||
| Both | 7 | −0.49 | 90.4 | <0.001 | 7 | −0.80 | 97.5 | <0.001 |
| (−1.06, 0.08) | (−1.28, −0.33) | |||||||
| Weight status | ||||||||
| Overweight/obese | 3 | −1.20 | 94.4 | <0.001 | 7 | −1.16 | 97.2 | <0.001 |
| (−2.89, 0.49) | (−1.80, −0.52) | |||||||
| General population | 7 | −0.01 | 0.0 | 0.729 | 12 | 0.08 | 76.3 | <0.001 |
| (−0.11, 0.08) | (−0.01, 0.16) | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Godoy-Cumillaf, A.; Fuentes-Merino, P.; Díaz-González, A.; Jiménez-Díaz, J.; Martínez-Vizcaíno, V.; Álvarez-Bueno, C.; Cavero-Redondo, I. The Effects of Physical Activity and Diet Interventions on Body Mass Index in Latin American Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1378. https://doi.org/10.3390/nu12051378
Godoy-Cumillaf A, Fuentes-Merino P, Díaz-González A, Jiménez-Díaz J, Martínez-Vizcaíno V, Álvarez-Bueno C, Cavero-Redondo I. The Effects of Physical Activity and Diet Interventions on Body Mass Index in Latin American Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(5):1378. https://doi.org/10.3390/nu12051378
Chicago/Turabian StyleGodoy-Cumillaf, Andrés, Paola Fuentes-Merino, Armando Díaz-González, Judith Jiménez-Díaz, Vicente Martínez-Vizcaíno, Celia Álvarez-Bueno, and Iván Cavero-Redondo. 2020. "The Effects of Physical Activity and Diet Interventions on Body Mass Index in Latin American Children and Adolescents: A Systematic Review and Meta-Analysis" Nutrients 12, no. 5: 1378. https://doi.org/10.3390/nu12051378
APA StyleGodoy-Cumillaf, A., Fuentes-Merino, P., Díaz-González, A., Jiménez-Díaz, J., Martínez-Vizcaíno, V., Álvarez-Bueno, C., & Cavero-Redondo, I. (2020). The Effects of Physical Activity and Diet Interventions on Body Mass Index in Latin American Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients, 12(5), 1378. https://doi.org/10.3390/nu12051378