Effect of Behavioral Weight Management Interventions Using Lifestyle mHealth Self-Monitoring on Weight Loss: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Risk of Bias Assessment
2.4. Statistical Analysis and Data Synthesis
3. Results
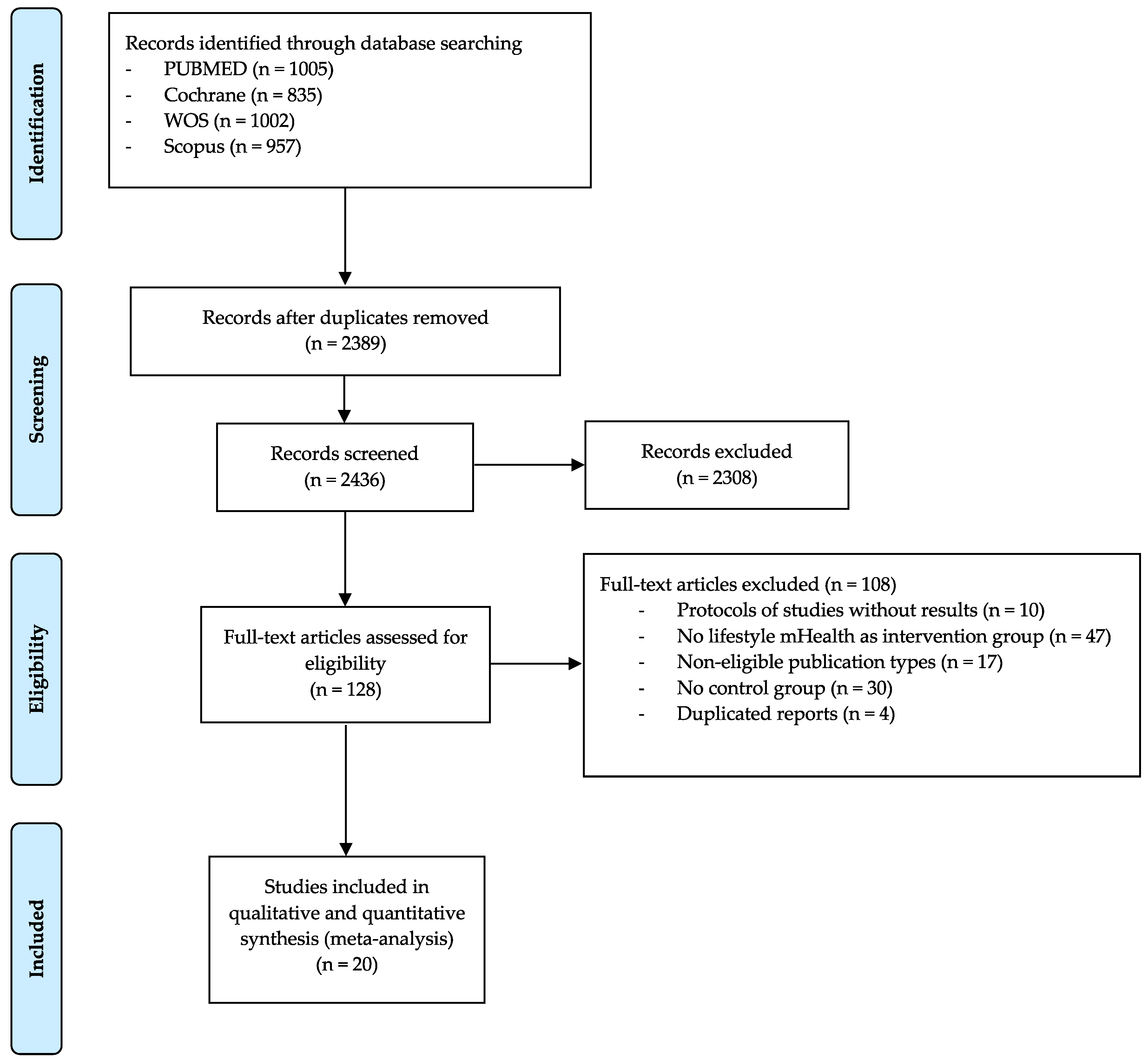
3.1. Systematic Review
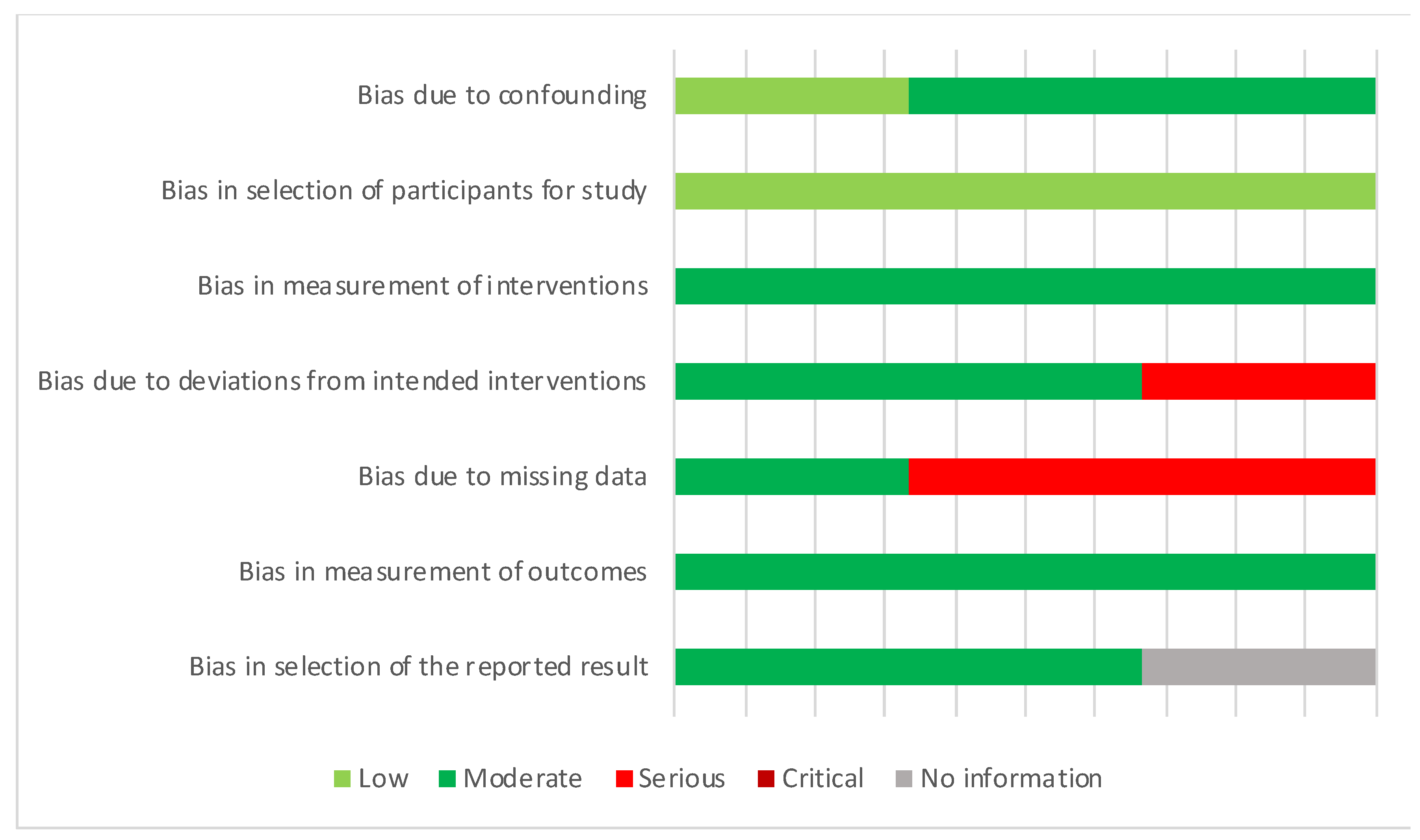
3.2. Risk of Bias
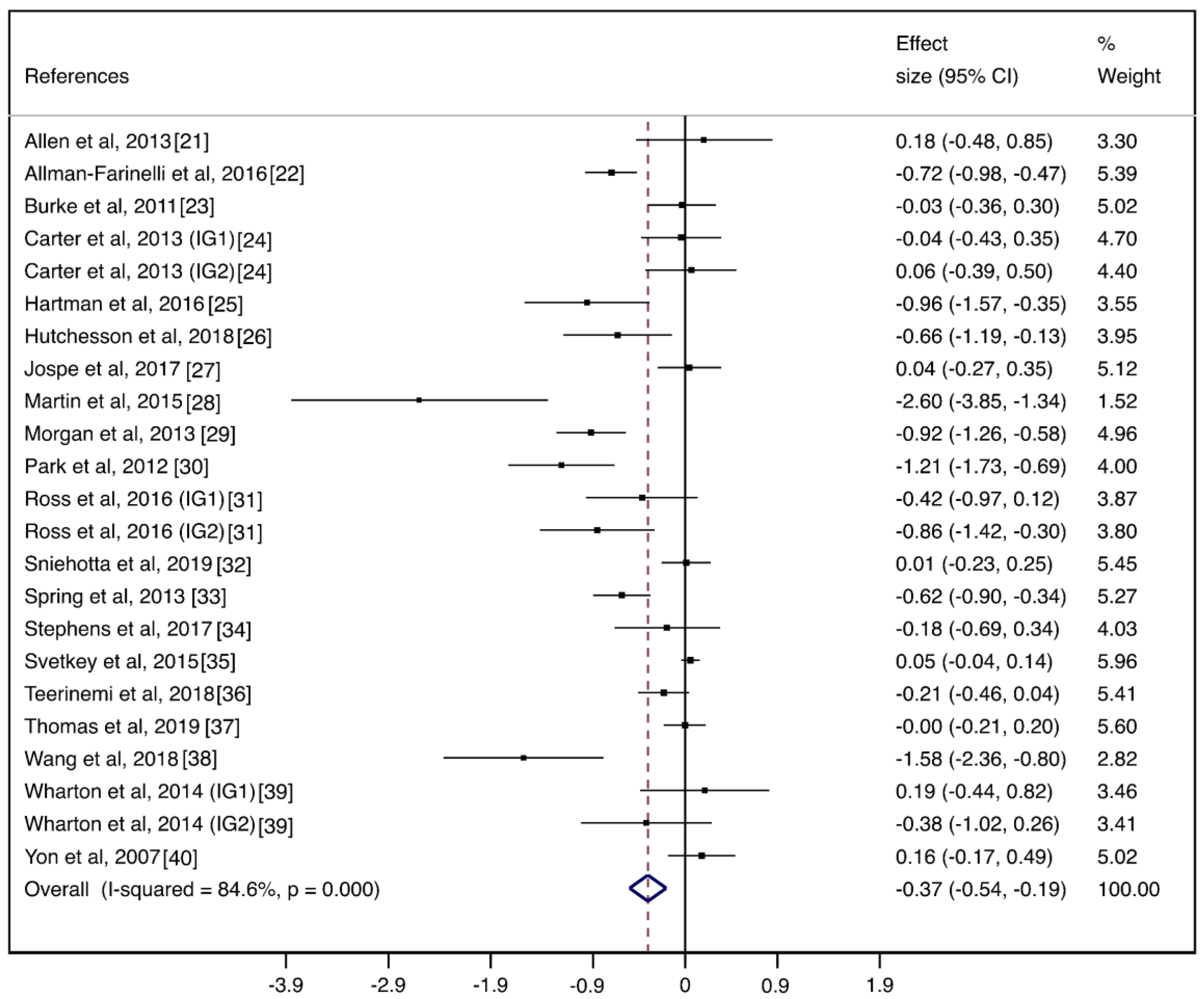
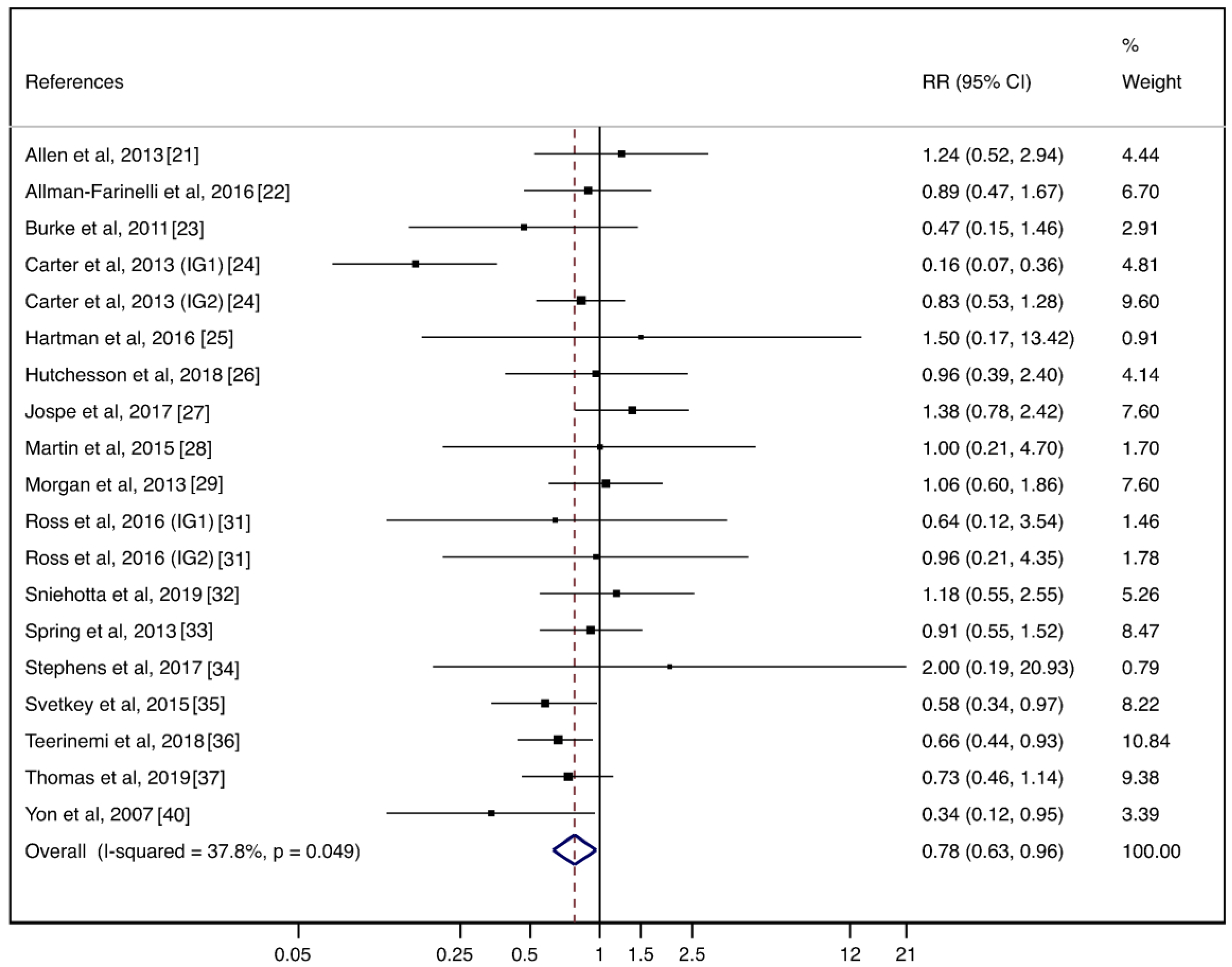
3.3. Meta-Analysis
3.4. Subgroup Analyses
3.5. Sensitivity Analyses
3.6. Meta-Regressions
3.7. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Set Medline | Search Set Medline |
|---|---|
| #1 smartphone technology [All Fields] #2 smartphone application [All Fields] #3 electronic self-monitoring [All Fields] #4 self-monitoring technology [All Fields] #5 self-monitoring [All Fields] #6 dietary self-monitoring [All Fields] #7 website [All Fields] #8 technology [Mesh Terms] #9 technology [All Fields] #10 8 OR 9 #11 telephone [Mesh Terms] #12 telephone [All Fields] #13 phone [All Fields] #14 11 OR 12 OR 13 #15 phone-based [All Fields] #16 smartphone [Mesh Terms] #17 smartphone [All Fields] #18 16 OR 17 #19 smartphone-based [All Fields] #20 smartphone app [All Fields] #21 personal digital assistant [All Fields] #22 PDA [All Fields] | #23 telemedicine [Mesh Terms] #24 telemedicine [All Fields] #25 ehealth [All Fields] #26 23 OR 24 OR 25 #27 mobile devices [All Fields] #28 mobile [All Fields] #29 connected tools [All Fields] #30 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 10 OR 14 OR 15 OR 18 OR 19 OR 20 OR 21 OR 22 OR 26 OR 27 OR 28 OR 29 #31 obesity treatment [All Fields] #32 weight loss [All Fields] #33 weight advice [All Fields] #34 weight management [All Fields] #35 31 OR 32 OR 33 OR 34 #36 randomized controlled pilot study [All Fields] #37 pilot randomized controlled trial [All Fields] #38 randomized pilot study [All Fields] #39 randomized controlled trial [All Fields] #40 RCT [All Fields] #41 randomized trial [All Fields] #42 36 OR 37 OR 38 OR 39 OR 40 OR 41 #43 30 AND35 AND 42 |
| Effect on Weight Loss | Adherence to mHealth | |||||
|---|---|---|---|---|---|---|
| Variable | n | Coefficient (95%CI) | p | n | Coefficient (95%CI) | p |
| Age (years) | 23 | −0.01 (−0.04, 0.01) | 0.365 | 19 | 0.01 (−0.02, 0.04) | 0.462 |
| Baseline mean weight (kg) | 21 | 0.06 (−0.03, 0.04) | 0.724 | 17 | 0.01 (−0.03, 0.04) | 0.593 |
| Baseline mean BMI (kg/m2) | 20 | 0.04 (−0.07, 0.15) | 0.440 | 17 | 0.00 (−0.13, 0.13) | 0.979 |
| Baseline mean WC (cm) | 9 | 0.01 (−0.05, 0.08) | 0.677 | 9 | −0.01 (−0.06, 0.03) | 0.428 |


References
- Mathers, C.; Stevens, G.; Mascarenhas, M. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2015 (GBD 2015) Obesity and Overweight Prevalence 1980–2015; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2017. [Google Scholar]
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014 (No. WHO/NMH/NVI/15.1); World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef]
- Burke, L.E.; Wang, J.; Sevick, M.A. Self-monitoring in weight loss: A systematic review of the literature. J. Am. Diet. Assoc. 2011, 111, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Foster, G.D.; Makris, A.P.; Bailer, B.A. Behavioral treatment of obesity. Am. J. Clin. Nutr. 2005, 82, 230S–235S. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Sealey-Potts, C.; Rodriguez, J. Dietary self-monitoring in weight management: Current evidence on efficacy and adherence. J. Acad. Nutr. Diet. 2015, 115, 1931–1933. [Google Scholar] [CrossRef] [PubMed]
- Gilmore, L.A.; Duhé, A.F.; Frost, E.A.; Redman, L.M. The technology boom: A new era in obesity management. J. Diabetes Sci. Technol. 2014, 8, 596–608. [Google Scholar] [CrossRef] [PubMed]
- DiClemente, R.; Nowara, A.; Shelton, R.; Wingood, G. Need for innovation in public health research. Am. J. Public Health 2019, 109, S117–S120. [Google Scholar] [CrossRef] [PubMed]
- WHO. mHealth: New Horizons for Health through Mobile Technologies; WHO Library Cataloguing-in-Publication Data; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Kozak, A.T.; Buscemi, J.; Hawkins, M.A.; Wang, M.L.; Breland, J.Y.; Ross, K.R.; Kommu, A. Technology-based interventions for weight management: Current randomized controlled trial evidence and future directions. J. Behav. Med. 2017, 40, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Dounavi, K.; Tsoumani, O. Mobile health applications in weight management: A systematic literature review. Am. J. Prev. Med. 2019, 56, 894–903. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. 5.1.0 (Updated March 2011); The Cochrane Collaboration: London, UK, 2011; Available online: https://handbook.cochrane.org (accessed on 1 May 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Higgins, J.P.; Sterne, J.A.C.; Savovic, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10, 29–31. [Google Scholar]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: Hillsdale, MI, USA, 1988; pp. 20–26. [Google Scholar]
- Sterne, J.A.C.; Egger, M.; Smith, G.D. Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ 2001, 323, 101–105. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Allen, J.K.; Stephens, J.; Himmelfarb, D.C.R.; Stewart, K.J.; Hauck, S. Randomized controlled pilot study testing use of smartphone technology for obesity treatment. J. Obes. 2013, 2013, 151597. [Google Scholar] [CrossRef]
- Allman-Farinelli, M.; Partridge, S.R.; McGeechan, K.; Balestracci, K.; Hebden, L.; Wong, A.; Phongsavan, P.; Denney-Wilson, E.; Harris, M.F.; Bauman, A. A mobile health lifestyle program for prevention of weight gain in young adults (TXT2BFiT): Nine-month outcomes of a randomized controlled trial. JMIR Mhealth Uhealth 2016, 4, e78. [Google Scholar] [CrossRef]
- Burke, L.E.; Conroy, M.B.; Sereika, S.M.; Elci, O.U.; Styn, M.A.; Acharya, S.D.; Sevick, M.A.; Ewing, L.J.; Glanz, K. The effect of electronic self-monitoring on weight loss and dietary intake: A randomized behavioral weight loss trial. Obesity 2011, 19, 338–344. [Google Scholar] [CrossRef]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. Adherence to a smartphone application for weight loss compared to website and paper diary: Pilot randomized controlled trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef]
- Hartman, S.J.; Nelson, S.H.; Cadmus-Bertram, L.A.; Patterson, R.E.; Parker, B.A.; Pierce, J.P. Technology-and phone-based weight loss intervention: Pilot RCT in women at elevated breast cancer risk. Am. J. Prev. Med. 2016, 51, 714–721. [Google Scholar] [CrossRef]
- Hutchesson, M.J.; Callister, R.; Morgan, P.J.; Pranata, I.; Clarke, E.D.; Skinner, G.; Ashton, L.M.; Whatnall, M.C.; Jones, M.; Oldmeadow, C.; et al. A targeted and tailored ehealth weight loss program for young women: The be positive be healthe randomized controlled trial. Healthcare 2018, 6, 39. [Google Scholar] [CrossRef]
- Jospe, M.R.; Roy, M.; Brown, R.C.; Williams, S.M.; Osborne, H.R.; Meredith-Jones, K.A.; McArthur, J.R.; Fleming, E.A.; Taylor, R.W. The effect of different types of monitoring strategies on weight loss: A randomized controlled trial. Obesity 2017, 25, 1490–1498. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.K.; Miller, A.C.; Thomas, D.M.; Champagne, C.M.; Han, H.; Church, T. Efficacy of Smart LossSM, a smartphone-based weight loss intervention: Results from a randomized controlled trial. Obesity 2015, 23, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Callister, R.; Collins, C.E.; Plotnikoff, R.C.; Young, M.D.; Berry, N.; McElduff, P.; Burrows, T.; Aguiar, E.; Saunders, K.L. The SHED-IT community trial: A randomized controlled trial of internet-and paper-based weight loss programs tailored for overweight and obese men. Ann. Behav. Med. 2013, 45, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Park, M.J.; Kim, H.S. Evaluation of mobile phone and Internet intervention on waist circumference and blood pressure in post-menopausal women with abdominal obesity. Int. J. Med. Inform. 2012, 81, 388–394. [Google Scholar] [CrossRef]
- Ross, K.M.; Wing, R.R. Impact of newer self-monitoring technology and brief phone-based intervention on weight loss: A randomized pilot study. Obesity 2016, 24, 1653–1659. [Google Scholar] [CrossRef]
- Sniehotta, F.F.; Evans, E.H.; Sainsbury, K.; Adamson, A.; Batterham, A.; Becker, F.; Brown, H.; Dombrowski, S.U.; Jackson, D.; Howell, D.; et al. Behavioural intervention for weight loss maintenance versus standard weight advice in adults with obesity: A randomised controlled trial in the UK (NULevel Trial). PLoS Med. 2019, 16, e1002793. [Google Scholar] [CrossRef]
- Spring, B.; Duncan, J.M.; Janke, E.A.; Kozak, A.T.; McFadden, H.G.; DeMott, A.; Pictor, A.; Epstein, L.H.; Siddique, J.; Pellegrini, C.A.; et al. Integrating technology into standard weight loss treatment: A randomized controlled trial. JAMA Intern. Med. 2013, 173, 105–111. [Google Scholar] [CrossRef]
- Stephens, J.D.; Yager, A.M.; Allen, J. Smartphone technology and text messaging for weight loss in young adults: A randomized controlled trial. J. Cardiovasc. Nurs. 2017, 32, 39. [Google Scholar] [CrossRef]
- Svetkey, L.P.; Batch, B.C.; Lin, P.H.; Intille, S.S.; Corsino, L.; Tyson, C.C.; Bosworth, H.B.; Grambow, S.C.; Voils, C.; Loria, C.; et al. Cell phone intervention for you (CITY): A randomized, controlled trial of behavioral weight loss intervention for young adults using mobile technology. Obesity 2015, 23, 2133–2141. [Google Scholar] [CrossRef]
- Teeriniemi, A.M.; Salonurmi, T.; Jokelainen, T.; Vähänikkila, H.; Alahäivälä, T.; Karppinen, P.; Enwald, H.; Huotari, M.-L.; Laitinen, J.; Oinas-Kukkonen, H.; et al. A randomized clinical trial of the effectiveness of a Web-based health behaviour change support system and group lifestyle counselling on body weight loss in overweight and obese subjects: 2-year outcomes. J. Intern. Med. 2018, 284, 534–545. [Google Scholar] [CrossRef]
- Thomas, J.G.; Bond, D.S.; Raynor, H.A.; Papandonatos, G.D.; Wing, R.R. Comparison of Smartphone-Based Behavioral Obesity Treatment With Gold Standard Group Treatment and Control: A Randomized Trial. Obesity 2019, 27, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cai, C.; Padhye, N.; Orlander, P.; Zare, M. A behavioral lifestyle intervention enhanced with multiple-behavior self-monitoring using mobile and connected tools for underserved individuals with type 2 diabetes and comorbid overweight or obesity: Pilot comparative effectiveness trial. JMIR Mhealth Uhealth 2018, 6, e92. [Google Scholar] [CrossRef] [PubMed]
- Wharton, C.M.; Johnston, C.S.; Cunningham, B.K.; Sterner, D. Dietary self-monitoring, but not dietary quality, improves with use of smartphone app technology in an 8-week weight loss trial. J. Nutr. Educ. Behav. 2014, 46, 440–444. [Google Scholar] [CrossRef]
- Yon, B.A.; Johnson, R.K.; Harvey-Berino, J.; Gold, B.C.; Howard, A. Personal digital assistants are comparable to traditional diaries for dietary self-monitoring during a weight loss program. J. Behav. Med. 2007, 30, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Barbabella, F.; Melchiorre, M.G.; Quattrini, S.; Papa, R.; Lamura, G. How Can eHealth Improve Care for People with Multimorbidity in Europe? World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2017. [Google Scholar]
- Farley, H. Promoting self-efficacy in patients with chronic disease beyond traditional education: A literature review. Nurs. Open 2020, 7, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Murray, E.; Burns, J.; Tai, S.S.; Lai, R.; Nazareth, I. Interactive Health Communication Applications for people with chronic disease. Cochrane Database Syst. Rev. 2005, 4, CD004274. [Google Scholar] [CrossRef]
- Elbert, N.J.; van Os-Medendorp, H.; van Renselaar, W.; Ekeland, A.G.; Hakkaart-van Roijen, L.; Raat, H.; Nijsten, T.E.C.; Pasmans, S.G.M.A. Effectiveness and cost-effectiveness of ehealth interventions in somatic diseases: A systematic review of systematic reviews and meta-analyses. J. Med. Internet Res. 2014, 16, e110. [Google Scholar] [CrossRef]
- Montesi, L.; El Ghoch, M.; Brodosi, L.; Calugi, S.; Marchesini, G.; Dalle Grave, R. Long-term weight loss maintenance for obesity: A multidisciplinary approach. Diabetes Metab. Syndr. Obes. 2016, 9, 37. [Google Scholar]
- Vlahu-Gjorgievska, E.; Mulakaparambil Unnikrishnan, S.; Win, K.T. mHealth applications: A tool for behaviour change in weight management. Stud. Health Technol. Inform. 2018, 252, 158–163. [Google Scholar]
- Robbins, R.; Krebs, P.; Jagannathan, R.; Jean-Louis, G.; Duncan, D.T. Health app use among US mobile phone users: Analysis of trends by chronic disease status. JMIR Mhealth Uhealth 2017, 5, e197. [Google Scholar] [CrossRef]
- Gordon, W.J.; Landman, A.; Zhang, H.; Bates, D.W. Beyond validation: Getting health apps into clinical practice. NPJ Digit. Med. 2020, 3, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.C.; Thomas, E.; Snoswell, C.L.; Haydon, H.; Mehrotra, A.; Clemensen, J.; Caffery, L.J. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J. Telemed. Telecare 2020. [Google Scholar] [CrossRef] [PubMed]



| Reference | Country | Study Design | Mean Age (Years) | Sample Size | Baseline Weight (kg Mean ± SD) | Baseline BMI (kg/m2 Mean ± SD) | Baseline WC (cm Mean ± SD) |
|---|---|---|---|---|---|---|---|
| Allen et al., 2013 [21] | USA | RCT | CG: 42.5 ± 12.1 IG: 45.3 ± 13.2 | CG: 18 IG: 17 | CG: 96.0 ± 17.4 IG: 96.4 ± 16.9 | CG: 34.1 ± 4.1 IG: 35.3 ± 4.1 | CG: 112.4 ± 11.5 IG: 109.7 ± 17.1 |
| Allman-Farinelli et al., 2016 [22] | Australia | RCT | CG: 27.2 ± 4.9 IG: 28.1 ± 4.9 | CG: 125 IG: 123 | CG: 79.3 ± 12.6 IG: 78.4 ± 11.2 | CG: 27.0 ± 2.7 IG: 27.3 ± 2.3 | NR |
| Burke et al., 2011 [23] | USA | RCT | CG: 47.4 ± 8.5 IG: 46.7 ± 9.2 | CG: 72 IG: 68 | NR | CG: 33.9 ± 4.6 IG: 33.5 ± 3.8 | CG: 109.5 ± 11.6 IG: 111.3 ± 11.1 |
| Carter et al., 2013 [24] | UK | RCT | CG: 42.5 ± 8.3 IG1: 41.2 ± 8.5 IG2: 41.9 ± 10.6 | CG: 19 IG1: 40 IG2: 20 | CG: 97.9 ± 18.7 IG1: 96.4 ± 16.0 IG2: 96.4 ± 19.9 | CG: 34.5 ± 5.7 IG1: 33.7 ± 4.2 IG2: 34.5 ± 5.6 | NR |
| Hartman et al., 2016 [25] | USA | RCT | CG: 59.8 ± 5.9 IG: 59.4 ± 5.6 | CG: 17 IG: 33 | CG: 85.3 ± 10.5 IG: 86.3 ± 10.2 | CG: 31.3 ± 3.7 IG: 32.2 ± 3.4 | NR |
| Hutchesson et al., 2018 [26] | Australia | RCT | CG: 27.9 ± 5 IG: 27.1 ± 4.7 | CG: 28 IG: 29 | CG: 79.2 ± 10.3 IG: 79.8 ± 10 | CG: 29.4 ± 2.5 IG: 29.3 ± 2.5 | CG: 88.2 ± 8.0 IG: 88.8 ± 9.0 |
| Jospe et al., 2017 [27] | New Zealand | RCT | CG: 46.7 ± 11.4 IG: 44.4 ± 10.2 | CG: 36 IG: 36 | CG: 91.0 ± 14.9 IG: 99.1 ± 17.3 | CG: 32.3 ± 4.3 IG: 33.2 ± 4.8 | CG: 99.8 ± 11.0 IG: 102.7 ± 12.8 |
| Martin et al., 2015 [28] | USA | RCT | CG: 43.3 ± 2.6 IG: 45.6 ± 2.7 | CG: 20 IG: 20 | CG: 80.6 ± 2.9 IG: 80.0 ± 2.3 | CG: 29.5 ± 3.2 IG: 30.2 ± 2.7 | CG: 94.5 ± 2.1 IG: 93.2 ± 2.2 |
| Morgan et al., 2013 [29] | Australia | RCT | CG1: 48.0 ± 11.2 CG2: 48.0 ± 10.8 IG: 46.5 ± 11.1 | CG1: 52 CG2: 54 IG: 53 | CG1: 103.8 ± 15.0 CG2: 101.8 ± 12.4 IG: 104.7 ± 14.5 | CG1: 33.1 ± 3.9 CG2: 32.4 ± 3.3 IG: 32.8 ± 3.4 | CG1: 113.6 ± 9.9 CG2: 112.6 ± 9.2 IG: 113.7 ± 9.7 |
| Park et al., 2012 [30] | South Korea | Non-RCT | CG: 57.6 ± 5.5 IG: 55.8 ± 5.7 | CG: 33 IG: 34 | CG: 62.5 ± 9.0 IG: 62.1 ± 7.1 | NR | CG: 89.6 ± 9.9 IG: 89.9 ± 5.5 |
| Ross et al., 2016 [31] | USA | RCT | CG: 54.2 ± 9.5 IG1: 46.2 ± 13.5 IG2: 52.9 ± 10.3 | CG: 26 IG1: 27 IG2: 27 | CG: 91.6 ± 14.5 IG1: 89.2 ± 15.6 IG2: 87.1 ± 12.4 | NR | NR |
| Sniehotta et al., 2019 [32] | UK | RCT | CG: 41.6 ± 11.4 IG: 42.0 ± 11.6 | CG: 133 IG: 131 | CG: 85.2 ± 15.7 IG: 85.1 ± 17.5 | CG: 30.8 ± 5.2 IG: 30.9 ± 5.5 | CG: 94.6 ± 14.7 IG: 93.6 ± 13.4 |
| Spring et al., 2013 [33] | USA | RCT | CG: 57.7 ± 10.2 IG: 57.7 ± 13.5 | CG: 35 IG: 34 | CG: 110.1 ± 15.1 IG: 113.7 ± 16.1 | CG: 35.8 ± 3.8 IG: 36.9 ± 5.4 | CG: 120.4 ± 8.9 IG: 120.4 ± 14.0 |
| Stephens et al., 2017 [34] | USA | RCT | CG: 20.5 ± 1.7 IG: 20.8 ± 2.0 | CG: 30 IG: 29 | CG: 79.6 ± 11.8 IG: 86.0 ± 16.3 | CG: 29.5 ± 4.3 IG: 30.9 ± 4.4 | CG: 97.0 ± 11.3 IG: 98.5 ± 10.8 |
| Svetkey et al., 2015 [35] | USA | RCT | CG: 29.6 ± 4.3 IG: 29.2 ± 4.2 | CG: 123 IG: 122 | NR | CG: 35.1 ± 7.5 IG: 35.7 ± 8.2 | NR |
| Teerinemi et al., 2018 [36] | Finland | RCT | CG:46.5 ± 10.2 IG:47.0 ± 9.4 | CG: 59 IG: 70 | CG: 88.6 ± 11.1 IG: 88.7 ± 10.9 | CG: 30.5 ± 2.3 IG: 30.3 ± 2.0 | NR |
| Thomas et al., 2019 [37] | USA | RCT | 55.1 ± 9.9 | CG: 56 IG: 114 | 95.9 ± 17.0 | 35.2 ± 5.0 | NR |
| Wang et al., 2018 [38] | USA | RCT | CG1: 49.2 ± 10.2 CG2: 56.1 ± 5.4 IG: 58.8 ± 5.9 | CG1: 6 CG2: 9 IG: 11 | CG1: 92.1 ± 2.4 CG2: 116.9 ± 13.1 IG: 106.9 ± 15.1 | CG1: 33.7 ± 2.7 CG2: 40.1 ± 7.0 IG: 38.9 ± 9.0 | NR |
| Wharton et al., 2014 [39] | USA | Non-RCT | CG: 40.8 ± 3.8 IG1: 43.7 ± 3.5 IG2: 41.5 ± 4 | CG: 20 IG1: 19 IG2: 18 | CG: 82.2 ± 20.3 IG1: 84.2 ± 13.4 IG2: 86.1 ± 22.3 | CG: 28.9 ± 1.0 IG1: 29.9 ± 0.9 IG2: 31.0 ± 1.7 | NR |
| Yon et al., 2007 [40] | USA | Non-RCT | CG: 46.1 ± 9.2 IG: 48.2 ± 8.7 | CG:93 IG: 57 | CG: 86.4 ± 13.7 IG: 90.2 ± 14.0 | CG: 30.9 ± 3.5 IG: 32.3 ± 3.4 | NR |
| Reference | Intervention | Comparison | Length (Months) | Dropouts (%) |
|---|---|---|---|---|
| Allen et al., 2013 [21] | Smartphone (Lose It!) | Usual care | 6 | CG: 33.3 IG: 41.2 |
| Allman-Farinelli et al., 2016 [22] | Web-based (TXT2BFiT) | Usual care | 9 | CG: 14.4 IG: 12.8 |
| Burke et al., 2011 [23] | PDA (Dietmate Pro) | Paper record | 6 | CG: 12.5 IG: 5.9 |
| Carter et al., 2013 [24] | IG1: Smartphone (My Meal Mate) IG2: Web-based | Paper record | 1.5 and 6 | 6-week follow-up: CG: 34.9 IG1: 9.3 IG2: 35.7 6-month follow-up: CG: 53.5 IG1: 7.0 IG2: 54.8 |
| Hartman et al., 2016 [25] | Smartphone (MyFitnessPal) | Usual care | 6 | CG: 5.6 IG: 8.3 |
| Hutchesson et al., 2018 [26] | Smartphone (Be Positive Be Healthy) | Wait-list | 6 | CG: 25.0 IG: 24.1 |
| Jospe et al., 2017 [27] | Smartphone (MyFitnessPal) | Usual care | 6 and 12 | 6-month follow-up: CG: 8.3 IG: 20.0 12-month follow-up: CG: 25.0 IG: 28.0 |
| Martin et al., 2015 [28] | Smartphone (SmartLoss) | Usual care | 1, 2 and 3 | CG: 5.0 IG: 5.0 |
| Morgan et al., 2013 [29] | Web-based (CalorieKing) | CG1: Wait-list CG2: Usual care | 3 | CG1: 7.7 CG1: 9.2 IG: 9.4 |
| Park et al., 2012 [30] | Web-based | Wait-list | 3 | NR |
| Ross et al., 2016 [31] | IG1: Smartphone (Fitbit) IG2: Smartphone (Fitbit) + phone call | Paper record | 6 | CG: 11.5 IG1: 7.4 IG2: 11.1 |
| Sniehotta et al., 2019 [32] | Web-based | Usual care | 12 | CG: 7.6 IG: 9.0 |
| Spring et al., 2013 [33] | PDA | Usual care | 3, 6 and 9 | 3-month follow-up: CG: 14.3 IG: 11.8 6-month follow-up: CG: 20.0 IG: 14.7 9-month follow-up: CG: 17.1 IG: 20.6 |
| Stephens et al., 2017 [34] | Smartphone (LoseIt!) | Usual care | 3 | CG: 3.2 IG: 6.5 |
| Svetkey et al., 2015 [35] | Smartphone (CalorieKing) | Wait-list | 6, 12 and 24 | 6-month follow-up: CG: 15.4 IG: 5.7 12-month follow-up: CG: 13.8 IG: 10.7 24-month follow-up: CG: 14.6 IG: 14.8 |
| Teerinemi et al., 2018 [36] | Web-based | Usual care | 12 and 24 | 12-month follow-up: CG: 23.6 IG: 13.2 24-month follow-up: CG: 10.1 IG: 9.9 |
| Thomas et al., 2019 [37] | Smartphone (MyFitnessPal) | Paper record | 6, 12 and 18 | 6-month follow-up: CG: 14.3 IG: 7.9 12-month follow-up: CG: 28.6 IG: 22.8 18-month follow-up: CG: 33.9 IG: 19.3 |
| Wang et al., 2018 [38] | Smartphone (LoseIt!) | CG1: Usual care CG2: Paper record | 3 and 6 | NR |
| Wharton et al., 2014 [39] | IG1: Smartphone (LoseIt!) IG2: Smartphone (Memo function of the smartphone) | Paper record | 2 | NR |
| Yon et al., 2007 [40] | PDA (Calorie King’s Handheld Diet Diary) | Paper record | 6 | CG: 19.0 IG: 7.0 |
| Effect on Weight Loss | Adherence to mHealth | |||||||
|---|---|---|---|---|---|---|---|---|
| Subgroup | n | Effect Size (95%CI) | I2 | p | n | Relative Risk (95%CI) | I2 | p |
| Type of mHealth intervention | ||||||||
| Smartphone | 14 | −0.36 (−0.58, −0.13) | 56.4 | 0.005 | 11 | 0.76 (0.51, 1.16) | 54.5 | 0.015 |
| PDA | 4 | −0.17 (−0.46, 0.13) | 62.7 | 0.045 | 3 | 0.61 (0.32, 1.15) | 40.6 | 0.186 |
| Web-based | 2 | 0.02 (−0.21, 0.24) | 0.0 | 0.838 | 5 | 0.83 (0.66, 1.04) | 0.0 | 0.556 |
| Type of Comparison | ||||||||
| Usual care | 10 | −0.51 (−0.83, −0.20) | 84.0 | <0.001 | 10 | 0.97 (0.72, 1.30) | 0.0 | 0.677 |
| Paper record | 11 | −0.22 (−0.46, 0.02) | 68.4 | <0.001 | 7 | 0.63 (0.44, 0.91) | 20.9 | 0.270 |
| Wait-list | 4 | −0.56 (−1.14, 0.01) | 94.1 | <0.001 | 3 | 0.93 (0.59, 1.48) | 0.0 | 0.697 |
| Length of Intervention | ||||||||
| ≤3 months | 14 | −1.08 (−1.55, −0.62) | 87.6 | <0.001 | 7 | 0.91 (0.61, 1.35) | 0.0 | 0.474 |
| Six months | 15 | −0.23 (−0.44, −0.02) | 70.4 | <0.001 | 15 | 0.76 (0.59, 0.97) | 46.0 | 0.035 |
| ≥12 months | 5 | 0.02 (−0.07, 0.11) | 0.0 | 0.432 | 6 | 0.79 (0.64, 0.96) | 0.0 | 0.530 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavero-Redondo, I.; Martinez-Vizcaino, V.; Fernandez-Rodriguez, R.; Saz-Lara, A.; Pascual-Morena, C.; Álvarez-Bueno, C. Effect of Behavioral Weight Management Interventions Using Lifestyle mHealth Self-Monitoring on Weight Loss: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1977. https://doi.org/10.3390/nu12071977
Cavero-Redondo I, Martinez-Vizcaino V, Fernandez-Rodriguez R, Saz-Lara A, Pascual-Morena C, Álvarez-Bueno C. Effect of Behavioral Weight Management Interventions Using Lifestyle mHealth Self-Monitoring on Weight Loss: A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(7):1977. https://doi.org/10.3390/nu12071977
Chicago/Turabian StyleCavero-Redondo, Iván, Vicente Martinez-Vizcaino, Rubén Fernandez-Rodriguez, Alicia Saz-Lara, Carlos Pascual-Morena, and Celia Álvarez-Bueno. 2020. "Effect of Behavioral Weight Management Interventions Using Lifestyle mHealth Self-Monitoring on Weight Loss: A Systematic Review and Meta-Analysis" Nutrients 12, no. 7: 1977. https://doi.org/10.3390/nu12071977
APA StyleCavero-Redondo, I., Martinez-Vizcaino, V., Fernandez-Rodriguez, R., Saz-Lara, A., Pascual-Morena, C., & Álvarez-Bueno, C. (2020). Effect of Behavioral Weight Management Interventions Using Lifestyle mHealth Self-Monitoring on Weight Loss: A Systematic Review and Meta-Analysis. Nutrients, 12(7), 1977. https://doi.org/10.3390/nu12071977