The Impact of Ramadan Fasting on the Reduction of PASI Score, in Moderate-To-Severe Psoriatic Patients: A Real-Life Multicenter Study

 ,
,  ,
,  ,
,  and
and
Abstract
1. Background
2. Material and Methods
2.1. Patients Selection and Inclusion
2.2. Statistical Analysis
3. Results
4. Discussion
Limitations and Future Prospects
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Langley, R.G.; Krueger, G.G.; Griffiths, C.E. Psoriasis: Epidemiology, clinical features, and quality of life. Ann. Rheum. Dis. 2005, 64 (Suppl. 2), ii18–ii23. [Google Scholar] [CrossRef] [PubMed]
- Staubach, P.; Zimmer, S. Plaque psoriasis – more than a skin disorder. Med. Monatsschr. Pharm. 2017, 40, 231–233. [Google Scholar] [PubMed]
- Sbidian, E.; Chaimani, A.; Garcia-Doval, I.; Do, G.; Hua, C.; Mazaud, C.; Droitcourt, C.; Hughes, C.; Ingram, J.R.; Naldi, L.; et al. Systemic pharmacological treatments for chronic plaque psoriasis: A network meta-analysis. Cochrane Database Syst. Rev. 2017, 12, CD011535. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Wu, M.X. A clinical review of phototherapy for psoriasis. Lasers Med. Sci. 2018, 33, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.; Shifrin, N.; Nektalova, T.; Goldenberg, G. Diet and dermatology: Google search results for acne, psoriasis, and eczema. Cutis 2018, 102, 44, 46–48. [Google Scholar] [PubMed]
- Zuccotti, E.; Oliveri, M.; Girometta, C.; Ratto, D.; Di Iorio, C.; Occhinegro, A.; Rossi, P. Nutritional strategies for psoriasis: Current scientific evidence in clinical trials. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8537–8551. [Google Scholar] [PubMed]
- Rouhani, M.H.; Azadbakht, L. Is Ramadan fasting related to health outcomes? A review on the related evidence. J. Res. Med. Sci. 2014, 19, 987–992. [Google Scholar] [PubMed]
- Bragazzi, N.L.; Watad, A. The Impact of Fasting on Rheumatic Diseases. Isr. Med. Assoc. J. 2017, 19, 378–379. [Google Scholar] [PubMed]
- Bragazzi, N.L. Ramadan fasting and chronic kidney disease: A systematic review. J. Res. Med. Sci. 2014, 19, 665–676. [Google Scholar] [PubMed]
- Bragazzi, N.L.; Briki, W.; Khabbache, H.; Rammouz, I.; Chamari, K.; Demaj, T.; Re, T.S.; Zouhir, M. Ramadan Fasting and Patients with Cancer: State-of-the-Art and Future Prospects. Front. Oncol. 2016, 6, 27. [Google Scholar] [CrossRef]
- Debbaneh, M.; Millsop, J.W.; Bhatia, B.K.; Koo, J.; Liao, W. Diet and psoriasis, part I: Impact of weight loss interventions. J. Am. Acad. Dermatol. 2014, 71, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Katta, R.; Kramer, M.J. Skin and Diet: An Update on the Role of Dietary Change as a Treatment Strategy for Skin Disease. Skin Therapy Lett. 2018, 23, 1–5. [Google Scholar] [PubMed]
- Ford, A.R.; Siegel, M.; Bagel, J.; Cordoro, K.M.; Garg, A.; Gottlieb, A.; Green, L.J.; Gudjonsson, J.E.; Koo, J.; Lebwohl, M.; et al. Dietary Recommendations for Adults With Psoriasis or Psoriatic Arthritis From the Medical Board of the National Psoriasis Foundation: A Systematic Review. JAMA. Dermatol. 2018, 154, 934–950. [Google Scholar] [CrossRef] [PubMed]
- Afifi, L.; Danesh, M.J.; Lee, K.M.; Beroukhim, K.; Farahnik, B.; Ahn, R.S.; Yan, D.; Singh, R.K.; Nakamura, M.; Koo, J.; et al. Dietary Behaviors in Psoriasis: Patient-Reported Outcomes from a U.S. National Survey. Dermatol. Ther. (Heidelb.) 2017, 7, 227–242. [Google Scholar] [CrossRef]
- Li, H.; Zuo, J.; Tang, W. Phosphodiesterase-4 Inhibitors for the Treatment of Inflammatory Diseases. Front. Pharmacol. 2018, 9, 1048. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, C.; Kathale, N.D.; Liu, D.; Lee, C.; Freeman, D.A.; Hogenesch, J.B.; Cao, R.; Liu, A.C. mTOR signaling regulates central and peripheral circadian clock function. PLoS. Genet. 2018, 14, e1007369. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Dacso, C.C.; O’Malley, B.W. Unveiling “Musica Universalis” of the Cell: A Brief History of Biological 12-Hour Rhythms. J. Endocr. Soc. 2018, 2, 727–752. [Google Scholar] [CrossRef] [PubMed]
- Cao, R.; Li, A.; Cho, H.Y.; Lee, B.; Obrietan, K. Mammalian target of rapamycin signaling modulates photic entrainment of the suprachiasmatic circadian clock. J. Neurosci. 2010, 30, 6302–6314. [Google Scholar] [CrossRef]
- Plikus, M.V.; Van Spyk, E.N.; Pham, K.; Geyfman, M.; Kumar, V.; Takahashi, J.S.; Andersen, B. The circadian clock in skin: Implications for adult stem cells, tissue regeneration, cancer, aging, and immunity. J. Biol. Rhythms 2015, 30, 163–182. [Google Scholar] [CrossRef]
- Vaughn, A.R.; Clark, A.K.; Sivamani, R.K.; Shi, V.Y. Circadian rhythm in atopic dermatitis-Pathophysiology and implications for chronotherapy. Pediatr. Dermatol. 2018, 35, 152–157. [Google Scholar] [CrossRef]
- Ozturk, N.; Ozturk, D.; Pala-Kara, Z.; Kaptan, E.; Sancar-Bas, S.; Ozsoy, N.; Cinar, S.; Deniz, G.; Li, X.M.; Giacchetti, S.; et al. The immune system as a chronotoxicity target of the anticancer mTOR inhibitor everolimus. Chronobiol. Int. 2018, 35, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Gelfant, S.; Ozawa, A.; Chalker, D.K.; Smith, J.G. Circadian rhythms and differences in epidermal and in dermal cel proliferation in uninvolved and involved psoriatic skin in vivo. J. Investig. Dermatol. 1982, 78, 58–62. [Google Scholar] [CrossRef]
- Radaelli, A.; Carandente, F.; Tadini, G.; Ronchi, M.; Zoccoli, A.; Caccialanza, P. Circadian temporal structure in psoriasis. Chronobiologia 1982, 9, 203–209. [Google Scholar]
- Ando, N.; Nakamura, Y.; Aoki, R.; Ishimaru, K.; Ogawa, H.; Okumura, K.; Shibata, S.; Shimada, S.; Nakao, A. Circadian Gene Clock Regulates Psoriasis-Like Skin Inflammation in Mice. J. Investig. Dermatol. 2015, 135, 3001–3008. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Qureshi, A.A.; Schernhammer, E.S.; Han, J. Rotating night-shift work and risk of psoriasis in US women. J. Investig. Dermatol. 2013, 133, 565–567. [Google Scholar] [CrossRef]
- BaHammam, A.; Alrajeh, M.; Albabtain, M.; Bahammam, S.; Sharif, M. Circadian pattern of sleep, energy expenditure, and body temperature of young healthy men during the intermittent fasting of Ramadan. Appetite 2010, 54, 426–429. [Google Scholar] [CrossRef] [PubMed]
- Almeneessier, A.S.; BaHammam, A.S. How does diurnal intermittent fasting impact sleep, daytime sleepiness, and markers of the biological clock? Current insights. Nat. Sci. Sleep 2018, 10, 439–452. [Google Scholar] [CrossRef]
- Melikoglu, M. Sleep Quality and its Association with Disease Severity in Psoriasis. Eurasian J. Med. 2017, 49, 124–127. [Google Scholar] [CrossRef]
- Kaaz, K.; Szepietowski, J.C.; Matusiak, Ł. Influence of Itch and Pain on Sleep Quality in Atopic Dermatitis and Psoriasis. Acta Derm. Venereol. 2018, in press. [Google Scholar] [CrossRef]
- Dahan, S.; Segal, Y.; Shoenfeld, Y. Dietary factors in rheumatic autoimmune diseases: A recipe for therapy? Nat. Rev. Rheumatol. 2017, 13, 348–358. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age (years) | 42.84 ± 13.61; 42 |
| Gender (male) | 62 (57.4%) |
| BMI (kg/m2) | 25.48 ± 2.08; 25.7 |
| Disease duration (years) | 12.31 ± 9.12; 10 |
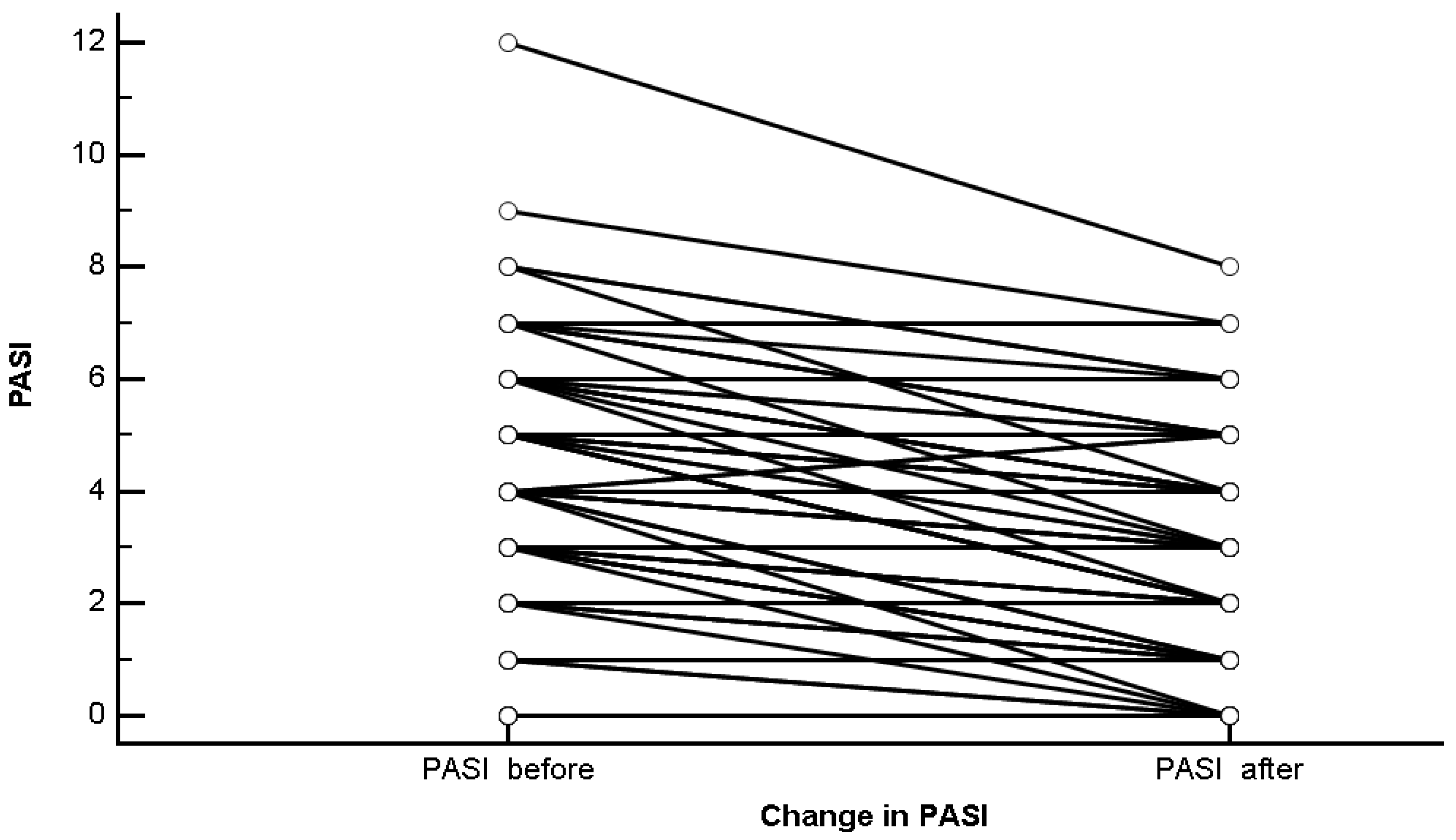
| PASI before Ramadan fasting | 3.54 ± 2.43; 3 |
| PASI after Ramadan fasting | 2.65 ± 2.03; 3 |
| Delta PASI | 0.89 ± 1.21; 0 |
| Topical therapy (two applications/day) | 20 (18.5%) |
| TNF blockers (etanercept 50 mg/week, adalimumab 40 mg/week) | 17 (15.7%) |
| Methotrexate (11 ± 5.5 mg/week) | 15 (13.9%) |
| Apremilast (30 + 30 mg/day as maintaining dose) | 12 (11.1%) |
| NB-UVB (three times/week) | 11 (10.2%) |
| Cyclosporin (5 mg/kg/day as maintaining dose; 420 ± 65 mg/day) | 10 (9.3%) |
| Acitretin (21 ± 12.3 mg/day) | 8 (7.4%) |
| IL-17 blockers (ixekizumab 80 mg/4 weeks as maintaining dose, secukinumab 150 + 150 mg/4 weeks as maintaining dose) | 8 (7.4%) |
| mTOR inhibitors (1 application/day) | 7 (6.5%) |
| Parameter | Value | Statistical Significance (p-Value) |
|---|---|---|
| Age (years) | ||
| ≤42 years | 0.65 ± 0.95 | 0.0801 |
| >42 years | 0.83 ± 1.25 | |
| Gender | ||
| Male | 0.94 ± 1.19 | 0.4771 |
| Female | 0.83 ± 1.25 | |
| BMI | ||
| Normal weight | 0.61 ± 1.05 | 0.1260 |
| Overweight | 1.03 ± 1.27 | |
| Obesity | 1.67 ± 1.53 | |
| Disease duration (years) | ||
| ≤10 years | 0.76 ± 1.19 | 0.1565 |
| >10 years | 1.04 ± 1.23 | |
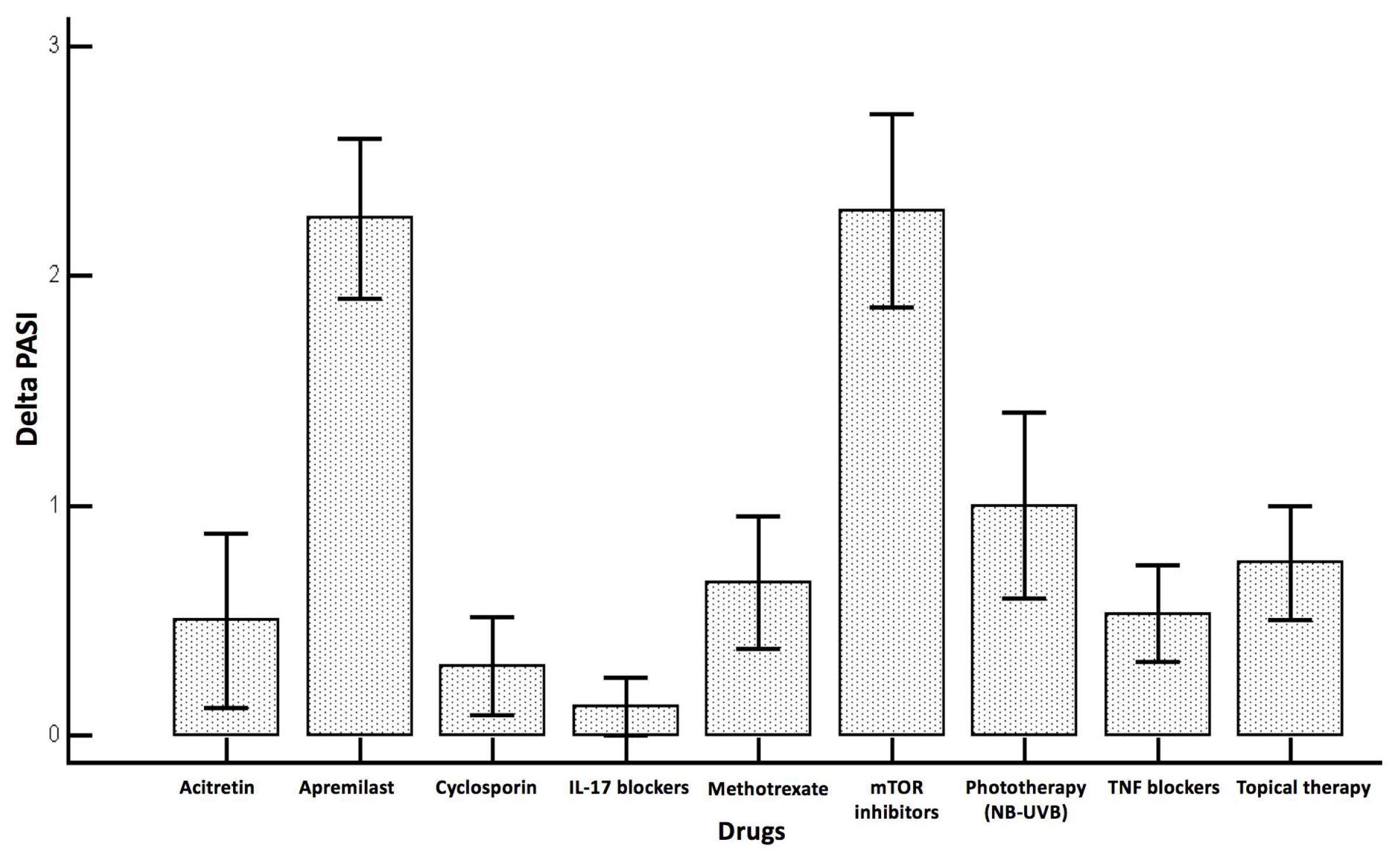
| Drug | ||
| Acitretin | 0.50 ± 1.07 | <0.0001 |
| Apremilast | 2.25 ± 1.22 | |
| Cyclosporin | 0.30 ± 0.67 | |
| NB-UVB | 1.00 ± 1.34 | |
| IL-17 Blockers | 0.13 ± 0.35 | |
| mTOR inhibitors | 2.29 ± 1.11 | |
| Methotrexate | 0.67 ± 1.11 | |
| TNF blockers | 0.53 ± 0.87 | |
| Topical therapy | 0.75 ± 1.12 |
| Parameter | Coefficient | Std. Error | rpartial | t | Statistical Significance (p-Value) |
|---|---|---|---|---|---|
| Delta PASI | |||||
| (Constant) | −1.72 | ||||
| Age | 0.02 | 0.01 | 0.17 | 1.70 | 0.0932 |
| Gender | 0.22 | 0.21 | 0.11 | 1.04 | 0.3034 |
| BMI | 0.07 | 0.05 | 0.13 | 1.28 | 0.2023 |
| Disease duration | −0.04 | 0.01 | −0.27 | −2.72 | 0.0078 |
| Apremilast | 1.82 | 0.51 | 0.35 | 3.58 | 0.0005 |
| Cyclosporin | −0.05 | 0.50 | −0.01 | −0.10 | 0.9205 |
| NB-UVB | 0.37 | 0.48 | 0.08 | 0.77 | 0.4437 |
| IL-17 Blockers | −0.26 | 0.53 | −0.05 | −0.49 | 0.6283 |
| mTOR inhibitors | 1.69 | 0.56 | 0.29 | 3.01 | 0.0034 |
| Methotrexate | 0.32 | 0.47 | 0.07 | 0.70 | 0.4885 |
| TNF blockers | 0.09 | 0.46 | 0.02 | 0.20 | 0.8441 |
| Topics | 0.25 | 0.46 | 0.06 | 0.55 | 0.5859 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damiani, G.; Watad, A.; Bridgewood, C.; Pigatto, P.D.M.; Pacifico, A.; Malagoli, P.; Bragazzi, N.L.; Adawi, M. The Impact of Ramadan Fasting on the Reduction of PASI Score, in Moderate-To-Severe Psoriatic Patients: A Real-Life Multicenter Study. Nutrients 2019, 11, 277. https://doi.org/10.3390/nu11020277
Damiani G, Watad A, Bridgewood C, Pigatto PDM, Pacifico A, Malagoli P, Bragazzi NL, Adawi M. The Impact of Ramadan Fasting on the Reduction of PASI Score, in Moderate-To-Severe Psoriatic Patients: A Real-Life Multicenter Study. Nutrients. 2019; 11(2):277. https://doi.org/10.3390/nu11020277
Chicago/Turabian StyleDamiani, Giovanni, Abdulla Watad, Charlie Bridgewood, Paolo Daniele Maria Pigatto, Alessia Pacifico, Piergiorgio Malagoli, Nicola Luigi Bragazzi, and Mohammad Adawi. 2019. "The Impact of Ramadan Fasting on the Reduction of PASI Score, in Moderate-To-Severe Psoriatic Patients: A Real-Life Multicenter Study" Nutrients 11, no. 2: 277. https://doi.org/10.3390/nu11020277
APA StyleDamiani, G., Watad, A., Bridgewood, C., Pigatto, P. D. M., Pacifico, A., Malagoli, P., Bragazzi, N. L., & Adawi, M. (2019). The Impact of Ramadan Fasting on the Reduction of PASI Score, in Moderate-To-Severe Psoriatic Patients: A Real-Life Multicenter Study. Nutrients, 11(2), 277. https://doi.org/10.3390/nu11020277