Association of Vegetarian Diet with Chronic Kidney Disease



Abstract
1. Introduction
2. Materials and Methods
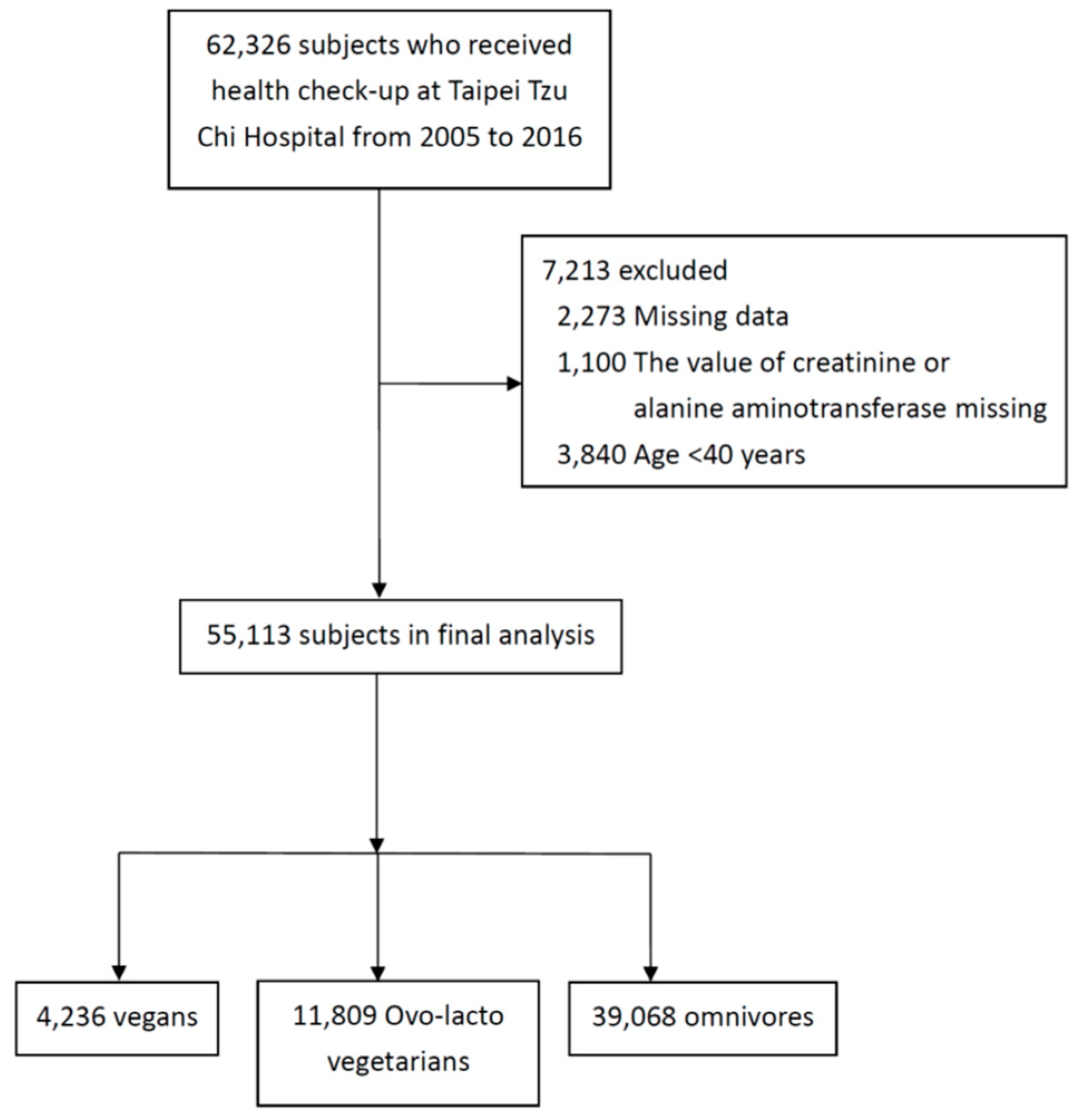
2.1. Design and Study Participants
2.2. Clinical Assessment
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Association of Vegetarian Diets with CKD
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Collins, A.; Foley, R.; Gilbertson, D.; Chen, S. United States Renal Data System public health surveillance of chronic kidney disease and end-stage renal disease. Kidney Int. Suppl. 2015, 5, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Go, A.; Chertow, G.; Fan, D.; McCulloch, C.; Hsu, C. Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Selvin, E.; Stevens, L.; Manzi, J.; Kusek, J.; Eggers, P.; Van Lente, F.; Levey, A. Prevalence of Chronic Kidney Disease in the United States. JAMA 2007, 298, 2038. [Google Scholar] [CrossRef] [PubMed]
- Bouya, S.; Balouchi, A.; Rafiemanesh, H.; Hesaraki, M. Prevalence of Chronic Kidney Disease in Iranian General Population: A Meta-Analysis and Systematic Review. Ther. Apher. Dial. 2018, 22, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Hwang, S. Incidence, prevalence and mortality trends of dialysis end-stage renal disease in Taiwan from 1990 to 2001: The impact of national health insurance. Nephrol. Dial. Transplant. 2008, 23, 3977–3982. [Google Scholar] [CrossRef] [PubMed]
- Klag, M.; Whelton, P.; Randall, B.; Neaton, J.; Brancati, F.; Ford, C.; Shulman, N.; Stamler, J. Blood Pressure and End-Stage Renal Disease in Men. N. Engl. J. Med. 1996, 334, 13–18. [Google Scholar] [CrossRef]
- Stevens, P. Evaluation and Management of Chronic Kidney Disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann. Intern. Med. 2013, 158, 825. [Google Scholar] [CrossRef]
- Foster, M.; Hwang, S.; Massaro, J.; Jacques, P.; Fox, C.; Chu, A. Lifestyle Factors and Indices of Kidney Function in the Framingham Heart Study. Am. J. Nephrol. 2015, 41, 267–274. [Google Scholar] [CrossRef]
- Chauveau, P.; Koppe, L.; Combe, C.; Lasseur, C.; Trolonge, S.; Aparicio, M. Vegetarian diets and chronic kidney disease. Nephrol. Dial. Transplant. 2018. [Google Scholar] [CrossRef]
- Kuo, K.; Liu, H.; Liu, J. Vegetarian diet and blood pressure in a hospital-based study. Ci Ji Yi Xue Za Zhi 2018, 30, 176. [Google Scholar] [CrossRef]
- WHO. Diet, Nutrition and the Prevention of Chronic Diseases. A Report of the WHO Study Group on Diet, Nutrition and Prevention of Noncommunicable Diseases. Nutr. Rev. 1991, 49, 291–301. [Google Scholar] [CrossRef]
- McEvoy, C.; Temple, N.; Woodside, J. Vegetarian diets, low-meat diets and health: a review. Public Health Nutr. 2012, 15, 2287–2294. [Google Scholar] [CrossRef] [PubMed]
- Orlich, M.; Fraser, G. Vegetarian diets in the Adventist Health Study 2: A review of initial published findings. Am. J. Clin. Nutr. 2014, 100, 353S–358S. [Google Scholar] [CrossRef] [PubMed]
- Sabaté, J.; Wien, M. A perspective on vegetarian dietary patterns and risk of metabolic syndrome. Br. J. Nutr. 2015, 113, S136–S143. [Google Scholar] [CrossRef] [PubMed]
- Wiwanitkit, V. Renal Function Parameters of Thai Vegans Compared with Non-Vegans. Ren. Fail. 2007, 29, 219–220. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Luo, F.; Plummer, N.; Hostetter, T.; Meyer, T. The Production of p-Cresol Sulfate and Indoxyl Sulfate in Vegetarians Versus Omnivores. Clin. J. Am. Soc. Nephrol. 2012, 7, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Haghighatdoost, F.; Bellissimo, N.; Totosy de Zepetnek, J.; Rouhani, M. Association of vegetarian diet with inflammatory biomarkers: A systematic review and meta-analysis of observational studies. Public Health Nutr. 2017, 20, 2713–2721. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Cho, S.; Park, Y. Long-term vegetarians have low oxidative stress, body fat, and cholesterol levels. Nutr. Res. Pract. 2012, 6, 155. [Google Scholar] [CrossRef]
- Azadbakht, L.; Atabak, S.; Esmaillzadeh, A. Soy Protein Intake, Cardiorenal Indices, and C-Reactive Protein in Type 2 Diabetes with Nephropathy: A longitudinal randomized clinical trial. Diabetes Care 2008, 31, 648–654. [Google Scholar] [CrossRef]
- Kontessis, P.; Jones, S.; Dodds, R.; Trevisan, R.; Nosadini, R.; Fioretto, P.; Borsato, M.; Sacerdoti, D.; Viberti, G. Renal, metabolic and hormonal responses to ingestion of animal and vegetable proteins. Kidney Int. 1990, 38, 136–144. [Google Scholar] [CrossRef]
- Pasco, J.; Holloway, K.; Dobbins, A.; Kotowicz, M.; Williams, L.; Brennan, S. Body mass index and measures of body fat for defining obesity and underweight: A cross-sectional, population-based study. BMC Obes. 2014, 1. [Google Scholar] [CrossRef] [PubMed]
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002, 106, 3143–3421. [CrossRef]
- Mula-Abed, W.; Al Rasadi, K.; Al Riyami, D. Estimated Glomerular Filtration Rate (eGFR): A Serum Creatinine-Based Test for the Detection of Chronic Kidney Disease and its Impact on Clinical Practice. Oman Med. J. 2012, 27, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Jenkins, W.; Richardson, H.; Sarmanova, A.; Abhishek, A.; Ashton, D.; Barclay, C.; Doherty, S.; Duley, L.; Hatton, R.; et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: A randomised controlled trial. Lancet 2018, 392, 1403–1412. [Google Scholar] [CrossRef]
- Payne, B.; Ryan, H.; Bone, J.; Magee, L.; Aarvold, A.; Mark Ansermino, J.; Bhutta, Z.; Bowen, M.; Guilherme Cecatti, J.; et al. Development and internal validation of the multivariable CIPHER (Collaborative Integrated Pregnancy High-dependency Estimate of Risk) clinical risk prediction model. Crit. Care 2018, 22, 278. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, M.; Hunt, R.; Goodwin, A.; Gross, J.; Keen, H.; Viberti, G. Dietary Composition and Renal Function in Healthy Subjects. Nephron 1987, 46, 37–42. [Google Scholar] [CrossRef] [PubMed]
- De Mello, V.; Zelmanovitz, T.; Perassolo, M.; Azevedo, M.; Gross, J. Withdrawal of red meat from the usual diet reduces albuminuria and improves serum fatty acid profile in type 2 diabetes patients with macroalbuminuria. Am. J. Clin. Nutr. 2006, 83, 1032–1038. [Google Scholar] [CrossRef]
- Lin, C.; Lin, D.; Yen, C.; Chen, S.; Chen, C.; Wang, T.; Chou, M.; Chang, H.; Lee, M. Comparison of Renal Function and Other Health Outcomes in Vegetarians versus Omnivores in Taiwan. J. Health Popul. Nutr. 2010, 28. [Google Scholar] [CrossRef]
- Tonstad, S.; Stewart, K.; Oda, K.; Batech, M.; Herring, R.; Fraser, G. Vegetarian diets and incidence of diabetes in the Adventist Health Study-2. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 292–299. [Google Scholar] [CrossRef]
- Pettersen, B.; Anousheh, R.; Fan, J.; Jaceldo-Siegl, K.; Fraser, G. Vegetarian diets and blood pressure among white subjects: Results from the Adventist Health Study-2 (AHS-2). Public Health Nutr. 2012, 15, 1909–1916. [Google Scholar] [CrossRef]
- Fraser, G.; Katuli, S.; Anousheh, R.; Knutsen, S.; Herring, P.; Fan, J. Vegetarian diets and cardiovascular risk factors in black members of the Adventist Health Study-2. Public Health Nutr. 2014, 18, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Nishimura, K.; Barnard, N.; Takegami, M.; Watanabe, M.; Sekikawa, A.; Okamura, T.; Miyamoto, Y. Vegetarian Diets and Blood Pressure. JAMA Intern. Med. 2014, 174, 577. [Google Scholar] [CrossRef] [PubMed]
- Barnard, N.; Levin, S.; Yokoyama, Y. A Systematic Review and Meta-Analysis of Changes in Body Weight in Clinical Trials of Vegetarian Diets. J. Acad. Nutr. Diet. 2015, 115, 954–969. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Huang, C.; Hu, F.; Chavarro, J. Vegetarian Diets and Weight Reduction: A Meta-Analysis of Randomized Controlled Trials. J. Gen. Intern. Med. 2015, 31, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.; Kass, E. Low blood pressure in vegetarians: Effects of specific foods and nutrients. Am. J. Clin. Nutr. 1988, 48, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.; Moore, T.; Obarzanek, E.; Vollmer, W.; Svetkey, L.; Sacks, F.; Bray, G.; Vogt, T.; Cutler, J.; Windhauser, M.; et al. A Clinical Trial of the Effects of Dietary Patterns on Blood Pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Whelton, S.; Hyre, A.; Pedersen, B.; Yi, Y.; Whelton, P.; He, J. Effect of dietary fiber intake on blood pressure: a meta-analysis of randomized, controlled clinical trials. J. Hypertens. 2005, 23, 475–481. [Google Scholar] [CrossRef]
- Altorf–van der Kuil, W.; Engberink, M.; Brink, E.; van Baak, M.; Bakker, S.; Navis, G.; van’t Veer, P.; Geleijnse, J. Dietary Protein and Blood Pressure: A Systematic Review. PLoS ONE 2010, 5, e12102. [Google Scholar] [CrossRef]
- Kuo, C.; Lai, N.; Ho, L.; Lin, C. Insulin sensitivity in Chinese ovo-lactovegetarians compared with omnivores. Eur. J. Clin. Nutr. 2004, 58, 312–316. [Google Scholar] [CrossRef]
- Tonstad, S.; Butler, T.; Yan, R.; Fraser, G. Type of Vegetarian Diet, Body Weight, and Prevalence of Type 2 Diabetes. Diabetes Care 2009, 32, 791–796. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.; Harris, M. Key Elements of Plant-Based Diets Associated with Reduced Risk of Metabolic Syndrome. Curr. Diab. Rep. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Kurella, M. Metabolic Syndrome and the Risk for Chronic Kidney Disease among Nondiabetic Adults. J. Am. Soc. Nephrol. 2005, 16, 2134–2140. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Vegans | Ovo-Lacto Vegetarians | Omnivores | p-Value | |
|---|---|---|---|---|
| N | 4,236 | 11,809 | 39,068 | |
| Age, years | 64.2(9.9) | 60.4(9.1) | 62.1(10.1) | <0.001 |
| Age group | <0.001 | |||
| 40–49, n (%) | 240(5.7) | 1098(9.3) | 6,934(17.7) | |
| 50–59, n (%) | 963(22.7) | 3305(28.0) | 11,771(30.1) | |
| 60–69, n (%) | 1623(38.3) | 4589(38.9) | 12,542(32.1) | |
| ≥70, n (%) | 1410(33.3) | 2817(23.9) | 7821(20.0) | |
| Gender | <0.001 | |||
| Male, n (%) | 1412(33.3) | 3966(33.6) | 19,864(50.8) | |
| Female, n (%) | 2824(66.7) | 7843(66.4) | 19,204(49.2) | |
| Comorbidity | ||||
| Diabetes, n (%) | 269(9.4) | 717(6.1) | 2622(6.7) | 0.042 |
| Hypertension, n (%) | 845(19.9) | 2306(19.5) | 7601(19.5) | 0.074 |
| Systolic BP (mmHg) | 121(16) | 120(15) | 121(16) | <0.001 |
| Diastolic BP(mmHg) | 73(12) | 72(12) | 75(12) | <0.001 |
| BMI (kg/m2) | 23.1(3.3) | 23.2(3.2) | 24.1(17.5) | <0.001 |
| Abdominal obesity, n (%) | 56(1.3) | 171(1.4) | 1205(3.1) | <0.001 |
| ALT (mg/dL) | 25(18) | 26(19) | 32(27) | <0.001 |
| Total cholesterol (mg/dL) | 179(35) | 183(36) | 194(37) | <0.001 |
| Low HDL, n (%) | 1459(34.4) | 4153(35.2) | 9330(23.9) | <0.001 |
| High TG, n (%) | 957(22.6) | 2345(19.9) | 9840(25.2) | <0.001 |
| Proteinuria, n (%) | 114(2.7) | 464(3.9) | 1271(3.3) | <0.001 |
| eGFR(CKD-EPI) | 84(13) | 84(13) | 85(14) | <0.001 |
| CKD | 625(14.8) | 2361(20.0) | 6316(16.2) | <0.001 |
| Variable | Unadjusted Model | Model 1 a | Model 2 b | Model 3 c |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Age (years) | 1.03 (1.03–1.03) | 1.03 (1.03–1.03) | 1.01 (1.011–1.02) | 1.01 (1.01–1.02) |
| Gender (Male) | 1.39 (1.33–1.45) | 1.43 (1.36–1.49) | 1.27 (1.19–1.36) | 1.27 (1.19–1.35) |
| Diabetes | 2.53 (2.35–2.73) | 1.59 (1.42–1.78) | 1.52 (1.36–1.69) | |
| Hypertension | 2.19 (2.09–2.31) | 1.48 (1.37–1.60) | 1.40 (1.30–1.52) | |
| Abdominal obesity | 1.37 (1.21–1.56) | 1.01 (0.83–1.21) | ||
| Systolic BP (per 10 mmHg) | 1.15 (1.13–1.16) | 1.03 (1.01–1.05) | ||
| Low HDL | 1.60 (1.53–1.68) | 1.20 (1.12–1.28) | ||
| High TG | 1.34 (1.28–1.41) | 1.12 (1.04–1.21) | ||
| Omnivores | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) |
| Vegan | 0.90 (0.82–0.98) | 0.83 (0.76–0.91) | 0.85 (0.74–0.97) | 0.86 (0.75–0.97) |
| Ovo-lacto vegetarian | 1.30 (1.23–1.37) | 1.31 (1.24–1.38) | 0.83 (0.77–0.89) | 0.82 (0.77–0.88) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, H.-W.; Tsai, W.-H.; Liu, J.-S.; Kuo, K.-L. Association of Vegetarian Diet with Chronic Kidney Disease. Nutrients 2019, 11, 279. https://doi.org/10.3390/nu11020279
Liu H-W, Tsai W-H, Liu J-S, Kuo K-L. Association of Vegetarian Diet with Chronic Kidney Disease. Nutrients. 2019; 11(2):279. https://doi.org/10.3390/nu11020279
Chicago/Turabian StyleLiu, Hao-Wen, Wen-Hsin Tsai, Jia-Sin Liu, and Ko-Lin Kuo. 2019. "Association of Vegetarian Diet with Chronic Kidney Disease" Nutrients 11, no. 2: 279. https://doi.org/10.3390/nu11020279
APA StyleLiu, H.-W., Tsai, W.-H., Liu, J.-S., & Kuo, K.-L. (2019). Association of Vegetarian Diet with Chronic Kidney Disease. Nutrients, 11(2), 279. https://doi.org/10.3390/nu11020279