
Vegetable Extracts and Nutrients Useful in the Recovery from Helicobacter pylori Infection: A Systematic Review on Clinical Trials

 ,
,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
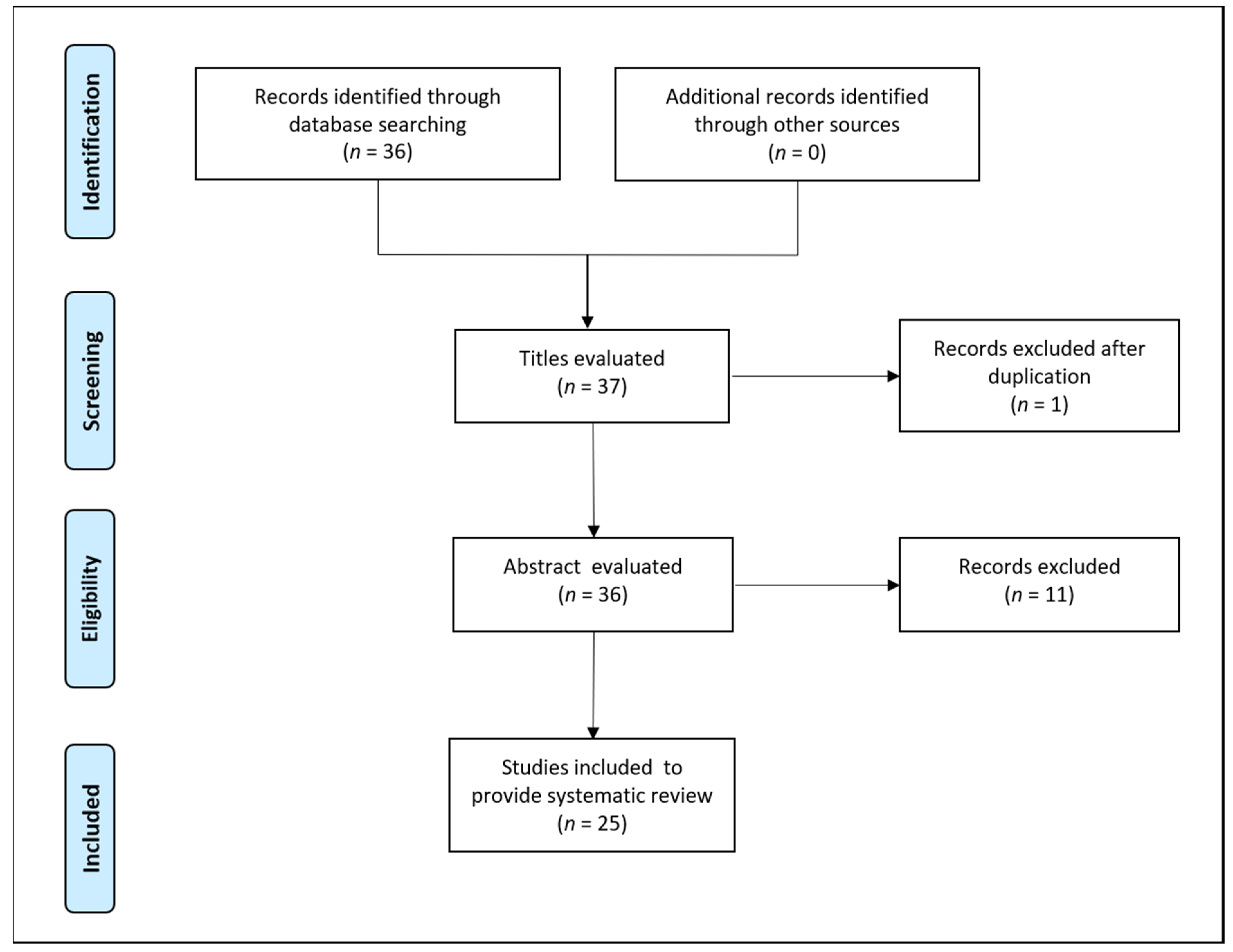
2. Methodology
3. Preclinical Studies on H. pylori Infections
4. Vegetable Extracts and H. pylori Infections: Clinical Studies
5. Micronutrients and H. pylori Infections: Clinical Studies
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lahner, E.; Persechino, S.; Annibale, B. Micronutrients (Other than Iron) and Helicobacter Pylori Infection: A Systematic Review. Helicobacter 2012, 17, 1–15. [Google Scholar] [CrossRef]
- Tonkic, A.; Tonkic, M.; Lehours, P.; Mégraud, F. Epidemiology and Diagnosis of Helicobacter Pylori Infection. Helicobacter 2012, 17, 1–8. [Google Scholar] [CrossRef]
- Ayala, G.; Escobedo-Hinojosa, W.I.; de la Cruz-Herrera, C.F.; Romero, I. Exploring Alternative Treatments for Helicobacter Pylori Infection. World J. Gastroenterol. 2014, 20, 1450–1469. [Google Scholar] [CrossRef] [PubMed]
- Schistosomes, Liver Flukes and Helicobacter Pylori. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. In Proceedings of the IARC monographs on the evaluation of carcinogenic risks to humans/World Health Organization, International Agency for Research on Cancer, Lyon, France, 7–14 June 1994; pp. 1–241.
- Jelavic, B.; Petricevic, J.; Marijanović, I.; Bevanda, M. Helicobacter Pylori in Otorhinolaryngology: Cause or Bystander. Eurasian J. Med. 2019, 51, 195–201. [Google Scholar] [CrossRef]
- Capurso, G.; Lahner, E.; Marcheggiano, A.; Caruana, P.; Carnuccio, A.; Bordi, C.; Delle Fave, G.; Annibale, B. Involvement of the Corporal Mucosa and Related Changes in Gastric Acid Secretion Characterize Patients with Iron Deficiency Anaemia Associated with Helicobacter Pylori Infection. Aliment. Pharmacol. Ther. 2001, 15, 1753–1761. [Google Scholar] [CrossRef] [PubMed]
- Pellicano, R.; Franceschi, F.; Saracco, G.; Fagoonee, S.; Roccarina, D.; Gasbarrini, A. Helicobacters and Extragastric Diseases. Helicobacter 2009, 14, 58–68. [Google Scholar] [CrossRef]
- Arnold, D.M.; Bernotas, A.; Nazi, I.; Stasi, R.; Kuwana, M.; Liu, Y.; Kelton, J.G.; Crowther, M.A. Platelet Count Response to H. Pylori Treatment in Patients with Immune Thrombocytopenic Purpura with and without H. Pylori Infection: A Systematic Review. Haematologica 2009, 94, 850–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GSh, I.; ER, A.; IuV, V.; OK, P.; EV, M. Helicobacter Pylori in Patients with Disorders of Hepatobiliary System. Zh. Mikrobiol. Epidemiol. Immunobiol. 2009, 2, 96–101. [Google Scholar]
- Pirouz, T.; Zounubi, L.; Keivani, H.; Rakhshani, N.; Hormazdi, M. Detection of Helicobacter Pylori in Paraffin-Embedded Specimens from Patients with Chronic Liver Diseases, Using the Amplification Method. Dig. Dis. Sci. 2009, 54, 1456–1459. [Google Scholar] [CrossRef] [PubMed]
- Wijarnpreecha, K.; Thongprayoon, C.; Panjawatanan, P.; Manatsathit, W.; Jaruvongvanich, V.; Ungprasert, P. Helicobacter Pylori and Risk of Nonalcoholic Fatty Liver Disease. J. Clin. Gastroenterol. 2018, 52, 386–391. [Google Scholar] [CrossRef]
- Zhou, X.; Zhang, C.; Wu, J.; Zhang, G. Association between Helicobacter Pylori Infection and Diabetes Mellitus: A Meta-Analysis of Observational Studies. Diabetes Res. Clin. Pract. 2013, 99, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.W.; Kwon, H.T.; Kang, J.M.; Park, J.H.; Choi, H.C.; Park, M.S.; Park, S.M.; Son, K.Y.; Cho, B. Association between Metabolic Syndrome and Helicobacter Pylori Infection Diagnosed by Histologic Status and Serological Status. J. Clin. Gastroenterol. 2012, 46, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, F.; Navarese, E.; Mollo, R.; Giupponi, B.; de Marco, G.; Merra, G.; Gasbarrini, G.; NG, S. Helicobacter Pylori and Atherosclerosis. A Review of the Literature. Recenti Prog. Med. 2009, 100, 91–96. [Google Scholar] [PubMed]
- Rogha, M.; Nikvarz, M.; Pourmoghaddas, Z.; Shirneshan, K.; Dadkhah, D.; Pourmoghaddas, M.M. Is Helicobacter Pylori Infection a Risk Factor for Coronary Heart Disease. ARYA Atheroscler. 2012, 8, 5. [Google Scholar]
- Albaret, G.; Sifré, E.; Floch, P.; Laye, S.; Aubert, A.; Dubus, P.; Azzi-Martin, L.; Giese, A.; Salles, N.; Mégraud, F.; et al. Alzheimer’s Disease and Helicobacter Pylori Infection: Inflammation from Stomach to Brain? J. Alzheimer’s Dis. 2020, 73, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Dardiotis, E.; Tsouris, Z.; Mentis, A.F.A.; Siokas, V.; Michalopoulou, A.; Sokratous, M.; Dastamani, M.; Bogdanos, D.P.; Deretzi, G.; Kountouras, J.H. Pylori and Parkinson’s Disease: Meta-Analyses Including Clinical Severity. Clin. Neurol. Neurosurg. 2018, 175, 16–24. [Google Scholar] [CrossRef]
- Izzotti, A.; Saccà, S.C.; Bagnis, A.; Recupero, S.M. Glaucoma and Helicobacter Pylori Infection: Correlations and Controversies. Br. J. Ophthalmol. 2009, 93, 1420–1427. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Fisher, A.; Smith, P.N. Clinical Medicine Helicobacter Pylori Related Diseases and Osteoporotic Fractures (Narrative Review). J. Clin. Med. 2020, 9, 3253. [Google Scholar] [CrossRef]
- Pan, B.L.; Huang, C.F.; Chuah, S.K.; Chiang, J.C.; Loke, S.S. Relationship between Helicobacter Pylori Infection and Bone Mineral Density: A Retrospective Cross-Sectional Study. BMC Gastroenterol. 2018, 18. [Google Scholar] [CrossRef] [Green Version]
- Gennari, L.; Merlotti, D.; Figura, N.; Mingiano, C.; Franci, M.B.; Lucani, B.; Picchioni, T.; Alessandri, M.; Campagna, M.S.; Gonnelli, S.; et al. Infection by CagA-Positive Helicobacter Pylori Strains and Bone Fragility: A Prospective Cohort Study. J. Bone Miner. 2020, 36, 80–89. [Google Scholar] [CrossRef]
- Hamann, C.; Kirschner, S.; Günther, K.P.; Hofbauer, L.C. Bone, Sweet Bone—Osteoporotic Fractures in Diabetes Mellitus. Nat. Rev. Endocrinol. 2012, 8, 297–305. [Google Scholar] [CrossRef]
- Urita, Y.; Watanabe, T.; Kawagoe, N.; Takemoto, I.; Tanaka, H.; Kijima, S.; Kido, H.; Maeda, T.; Sugasawa, Y.; Miyazaki, T.; et al. Role of Infected Grandmothers in Transmission of Helicobacter Pylori to Children in a Japanese Rural Town. J. Paediatr. Child Health 2013, 49, 394–398. [Google Scholar] [CrossRef]
- Bastos, J.; Carreira, H.; la Vecchia, C.; Lunet, N. Childcare Attendance and Helicobacter Pylori Infection: Systematic Review and Meta-Analysis. Eur. J. Cancer Prev. 2013, 22, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Fuccio, L.; Laterza, L.; Zagari, R.M.; Cennamo, V.; Grilli, D.; Bazzoli, F. Treatment of Helicobacter Pylori Infection. BMJ 2008, 337, 746–750. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Lu, C.W.; Lin, C.J. Treatment of Helicobacter Pylori Infection: Current Status and Future Concepts. World J. Gastroenterol. 2014, 20, 5283. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.; Bazzoli, F.; El-Omar, E.; Graham, D.; Hunt, R.; Rokkas, T.; Vakil, N.; Kuipers, E.J. Current Concepts in the Management of Helicobacter Pylori Infection: The Maastricht III Consensus Report. Gut 2007, 56, 772–781. [Google Scholar] [CrossRef]
- Coelho, L.G.V.; León-Barúa, R.; Quigley, E.M.M. Latin-American Consensus Conference on Helicobacter Pylori Infection. Am. J. Gastroenterol. 2000, 95, 2688. [Google Scholar] [CrossRef] [PubMed]
- Chey, W.D.; Wong, B.C.Y. American College of Gastroenterology Guideline on the Management of Helicobacter Pylori Infection. Am. J. Gastroenterol. 2007, 102, 1808–1825. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Selgrad, M. Helicobacter Pylori Infection and Current Clinical Areas of Contention. Curr. Opin. Gastroenterol. 2010, 26, 618–623. [Google Scholar] [CrossRef]
- Graham, D.Y.; Fischbach, L. Helicobacter Pylori Treatment in the Era of Increasing Antibiotic Resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef]
- Al Mofleh, I.A. Spices, Herbal Xenobiotics and the Stomach: Friends or Foes? World J. Gastroenterol. 2010, 16, 2710. [Google Scholar] [CrossRef]
- Wang, Y.-C. Medicinal Plant Activity on Helicobacter Pylori Related Diseases. World J. Gastroenterol. 2014, 20, 10368–10382. [Google Scholar] [CrossRef]
- Ghasemian, A.; Fattahi, A.; Shokouhi Mostafavi, S.K.; Almarzoqi, A.H.; Memariani, M.; ben Braiek, O.; Yassine, H.M.; Mostafavi, N.S.S.; Ahmed, M.M.; Mirforughi, S.A. Herbal Medicine as an Auspicious Therapeutic Approach for the Eradication of Helicobacter Pylori Infection: A Concise Review. J. Cell. Physiol. 2019, 34, 16847–16860. [Google Scholar] [CrossRef]
- Amaral, O.; Fernandes, I.; Veiga, N.; Pereira, C.; Chaves, C.; Nelas, P.; Silva, D. Living Conditions and Helicobacter Pylori in Adults. Biomed Res. Int. 2017, 2017, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Mard, S.A.; Haghighian, H.K.; Sebghatulahi, V.; Ahmadi, B. Dietary Factors in Relation to Helicobacter Pylori Infection. Gastroenterol. Res. Pract. 2014, 2014, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Q.; Meng, X.; Li, Y.; Zhao, C.N.; Tang, G.Y.; Li, S.; Gan, R.Y.; Li, H.B. Natural Products for the Prevention and Management of Helicobacter Pylori Infection. Compr. Rev. Food Sci. Food Saf. 2018, 17, 937–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, C.Y.; Lin, Y.T.; Labbe, R.G.; Shetty, K. Inhibition of Helicobacter Pylori by Phenolic Extracts of Sprouted Peas (Pisum Sativum L.). J. Food Biochem. 2006, 30, 21–34. [Google Scholar] [CrossRef]
- Kudo, H.; Takeuchi, H.; Shimamura, T.; Kadota, Y.; Sugiura, T.; Ukeda, H. In Vitro Anti-Helicobacter Pylori Activity of Chinese Chive (Allium Tuberosum). Food Sci. Technol. Res. 2011, 17, 505–513. [Google Scholar] [CrossRef]
- Romero, C.; Medina, E.; Vargas, J.; Brenes, M.; de Castro, A. In Vitro Activity of Olive Oil Polyphenols against Helicobacter Pylori. J. Agric. Food Chem. 2007, 55, 680–686. [Google Scholar] [CrossRef]
- O’Gara, E.A.; Hill, D.J.; Maslin, D.J. Activities of Garlic Oil, Garlic Powder, and Their Diallyl Constituents against Helicobacter Pylori. Appl. Environ. Microbiol. 2000, 66, 2269–2273. [Google Scholar] [CrossRef] [Green Version]
- Iimuro, M.; Shibata, H.; Kawamori, T.; Matsumoto, T.; Arakawa, T.; Sugimura, T.; Wakabayashi, K. Suppressive Effects of Garlic Extract on Helicobacter Pylori-Induced Gastritis in Mongolian Gerbils. Cancer Lett. 2002, 187, 61–68. [Google Scholar] [CrossRef]
- Fahey, J.W.; Haristoy, X.; Dolan, P.M.; Kensler, T.W.; Scholtus, I.; Stephenson, K.K.; Talalay, P.; Lozniewski, A. Sulforaphane Inhibits Extracellular, Intracellular, and Antibiotic-Resistant Strains of Helicobacter Pylori and Prevents Benzo[a]Pyrene-Induced Stomach Tumors. Proc. Natl. Acad. Sci. USA 2002, 99, 7610–7615. [Google Scholar] [CrossRef] [Green Version]
- Yanaka, A.; Fahey, J.W.; Fukumoto, A.; Nakayama, M.; Inoue, S.; Zhang, S.; Tauchi, M.; Suzuki, H.; Hyodo, I.; Yamamoto, M. Dietary Sulforaphane-Rich Broccoli Sprouts Reduce Colonization and Attenuate Gastritis in Helicobacter Pylori-Infected Mice and Humans. Cancer Prev. Res. 2009, 2, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Messing, J.; Niehues, M.; Shevtsova, A.; Borén, T.; Hensel, A. Antiadhesive Properties of Arabinogalactan Protein from Ribes Nigrum Seeds against Bacterial Adhesion of Helicobacter Pylori. Molecules 2014, 19, 3696–3717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thöle, C.; Brandt, S.; Ahmed, N.; Hensel, A. Acetylated Rhamnogalacturonans from Immature Fruits of Abelmoschus Esculentus Inhibit the Adhesion of Helicobacter Pylori to Human Gastric Cells by Interaction with Outer Membrane Proteins. Molecules 2015, 20, 16770–16787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Mahony, R.; Al-Khtheeri, H.; Weerasekera, D.; Fernando, N.; Vaira, D.; Holton, J.; Basset, C. Bactericidal and Anti-Adhesive Properties of Culinary and Medicinal Plants against Helicobacter Pylori. World J. Gastroenterol. 2005, 11, 7499. [Google Scholar] [CrossRef] [PubMed]
- Fukai, T.; Marumo, A.; Kaitou, K.; Kanda, T.; Terada, S.; Nomura, T. Anti-Helicobacter Pylori Flavonoids from Licorice Extract. Life Sci. 2002, 71, 1449–1463. [Google Scholar] [CrossRef]
- Krausse, R.; Bielenberg, J.; Blaschek, W.; Ullmann, U. In Vitro Anti-Helicobacter Pylori Activity of Extractum Liquiritiae, Glycyrrhizin and Its Metabolites. J. Antimicrob. Chemother. 2004, 54, 243–246. [Google Scholar] [CrossRef] [Green Version]
- Asha, M.K.; Debraj, D.; Prashanth, D.; Edwin, J.R.; Srikanth, H.S.; Muruganantham, N.; Dethe, S.M.; Anirban, B.; Jaya, B.; Deepak, M.; et al. In Vitro Anti-Helicobacter Pylori Activity of a Flavonoid Rich Extract of Glycyrrhiza Glabra and Its Probable Mechanisms of Action. J. Ethnopharmacol. 2013, 145, 581–586. [Google Scholar] [CrossRef]
- Kim, J.M.; Zheng, H.M.; Lee, B.Y.; Lee, W.K.; Lee, D.H. Anti-Helicobacter Pylori Properties of Gut Gard. Prev. Nutr. Food Sci. 2013, 18, 104. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.; Lim, J.W.; Kim, H.; Kim, H. Supplementation with Angelica Keiskei Inhibits Expression of Inflammatory Mediators in the Gastric Mucosa of Helicobacter Pylori-Infected Mice. Nutr. Res. 2016, 36, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Huwez, F.U.; Thirlwell, D.; Cockayne, A.; Ala’Aldeen, D.A.A. Mastic Gum Kills Helicobacter Pylori. N. Engl. J. Med. 1998, 339, 1946. [Google Scholar] [CrossRef] [PubMed]
- Meriem, M.; Rachida, A.; Housseyn, M.; Farida, T.; Abdelaziz, M.; Fouzia, M. Antimicrobial Activity of the Essential Oil Isolated from Pistacia Lentiscus Leaves Against Helicobacter Pylori Algerian Clinical Isolates. J. Essent. Oil-Bear. Plants 2016, 19, 466–474. [Google Scholar] [CrossRef]
- Paraschos, S.; Magiatis, P.; Mitakou, S.; Petraki, K.; Kalliaropoulos, A.; Maragkoudakis, P.; Mentis, A.; Sgouras, D.; Skaltsounis, A.L. In Vitro and in Vivo Activities of Chios Mastic Gum Extracts and Constituents against Helicobacter Pylori. Antimicrob. Agents Chemother. 2007, 51, 551–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akyön, Y. Effect of Antioxidants on the Immune Response of Helicobacter Pylori. Clin. Microbiol. Infect. 2002, 8, 438–441. [Google Scholar] [CrossRef] [Green Version]
- Jarosz, M.; Dzieniszewski, J.; Dabrowska-Ufniarz, E.; Wartanowicz, M.; Ziemlanski, S.; Reed, I.P. Effects of High Dose Vitamin C Treatment on Helicobacter Pylori Infection and Total Vitamin C Concentration in Gastric Juice. Eur. J. Cancer Prev. 1998, 7, 449–454. [Google Scholar] [CrossRef]
- Shi, L.Q.; Zheng, R.L. DNA Damage and Oxidative Stress Induced by Helicobacter Pylori in Gastric Epithelial Cells: Protection by Vitamin C and Sodium Selenite. Pharmazie 2006, 61, 631–637. [Google Scholar]
- Zhang, H.M.; Wakisaka, N.; Maeda, O.; Yamamoto, T. Vitamin C Inhibits the Growth of a Bacterial Risk Factor for Gastric Carcinoma: Helicobacter Pylori. Cancer 1997, 80, 1897–1903. [Google Scholar] [CrossRef]
- Wang, X.; Willen, R.; Wadstrom, T. Astaxanthin-Rich Algal Meal and Vitamin C Inhibit Helicobacter Pylori Infection in BALB/cA Mice. Antimicrob. Agents Chemother. 2000, 44, 2452–2457. [Google Scholar] [CrossRef] [Green Version]
- Bennedsen, M.; Wang, X.; Willén, R.; Wadström, T.; Andersen, L.P. Treatment of H. Pylori Infected Mice with Antioxidant Astaxanthin Reduces Gastric Inflammation, Bacterial Load and Modulates Cytokine Release by Splenocytes. Immunol. Lett. 2000, 70, 185–189. [Google Scholar] [CrossRef]
- Nir, Y.; Potasman, I.; Stermer, E.; Tabak, M.; Neeman, I. Controlled Trial of the Effect of Cinnamon Extract on Helicobacter Pylori. Helicobacter 2000, 5, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Bahadoran, Z.; Golzarand, M.; Zojaji, H.; Azizi, F. A Comparative Study of Broccoli Sprouts Powder and Standard Triple Therapy on Cardiovascular Risk Factors Following H. Pylori Eradication: A Randomized Clinical Trial in Patients with Type 2 Diabetes. J. Diabetes Metab. Disord. 2014, 13, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.W.; Jang, J.Y.; Kim, Y.H.; Kim, J.-W.; Shim, J.-J. The Effects of Broccoli Sprout Extract Containing Sulforaphane on Lipid Peroxidation and Helicobacter Pylori Infection in the Gastric Mucosa. Gut Liver 2015, 9, 486–493. [Google Scholar] [CrossRef] [Green Version]
- Di Mario, F.; Cavallaro, L.G.; Nouvenne, A.; Stefani, N.; Cavestro, G.M.; Iori, V.; Maino, M.; Comparato, G.; Fanigliulo, L.; Morana, E.; et al. A Curcumin-Based 1-Week Triple Therapy for Eradication of Helicobacter Pylori Infection: Something to Learn from Failure? Helicobacter 2007, 12, 238–243. [Google Scholar] [CrossRef]
- Khonche, A.; Biglarian, O.; Panahi, Y.; Valizadegan, G.; Soflaei, S.S.; Ghamarchehreh, M.E.; Majeed, M.; Sahebkar, A. Adjunctive Therapy with Curcumin for Peptic Ulcer: A Randomized Controlled Trial. Drug Res. 2016, 66, 444–448. [Google Scholar] [CrossRef] [Green Version]
- Judaki, A.; Rahmani, A.; Feizi, J.; Asadollahi, K.; Ahmadi, M.R.H. Curcumin in Combination with Triple Therapy Regimes Ameliorates Oxidative Stress and Histopathologic Changes in Chronic Gastritis– Associated Helicobacter Pylori Infection. Arq. Gastroenterol. 2017, 54, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Hekmatdoost, A.; Ghobeh, M.; Shaker-Hosseini, R.; MirSattari, D.; Rastmanesh, R.; Rashidkhani, B.; Navai, L. The Effect of Garlic Consumption on Helicobacter Pylori Treatment Using Urea Breath Test: A Randomized Clinical Trial. J. Nutr. Sci. Diet. 2015, 1, 21–27. [Google Scholar]
- McNulty, C.A.M.; Wilson, M.P.; Havinga, W.; Johnston, B.; O’Gara, E.A.; Maslin, D.J. A Pilot Study to Determine the Effectiveness of Garlic Oil Capsules in the Treatment of Dyspeptic Patients with Helicobacter Pylori. Helicobacter 2001, 6, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Anderson, S.Y.; Lang, T. Garlic or Jalapeno Peppers for Treatment of Helicobacter Pylori Infection. Am. J. Gastroenterol. 1999, 94, 1200–1202. [Google Scholar] [CrossRef]
- Yen, C.H.; Chiu, H.F.; Huang, S.Y.; Lu, Y.Y.; Han, Y.C.; Shen, Y.C.; Venkatakrishnan, K.; Wang, C.K. Beneficial Effect of Burdock Complex on Asymptomatic Helicobacter Pylori-Infected Subjects: A Randomized, Double-Blind Placebo-Controlled Clinical Trial. Helicobacter 2018, 23, e12469. [Google Scholar] [CrossRef]
- Puram, S.; Suh, H.C.; Kim, S.U.; Bethapudi, B.; Joseph, J.A.; Agarwal, A.; Kudiganti, V. Effect of Gutgard in the Management of Helicobacter Pylori: A Randomized Double Blind Placebo Controlled Study. Evid. Based Complementary Altern. Med. 2013, 2013, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salem, E.M.; Yar, T.; Bamosa, A.O.; Al-Quorain, A.; Yasawy, M.I.; Alsulaiman, R.M.; Randhawa, M.A. Comparative Study of Nigella Sativa and Triple Therapy in Eradication of Helicobacter Pylori in Patients with Non-Ulcer Dyspepsia. Saudi J. Gastroenterol. 2010, 16, 207–214. [Google Scholar] [CrossRef]
- Yoon, J.Y.; Cha, J.M.; Hong, S.S.; Kim, H.K.; Kwak, M.S.; Jeon, J.W.; Shin, H.P. Fermented Milk Containing Lactobacillus Paracasei and Glycyrrhiza Glabra Has a Beneficial Effect in Patients with Helicobacter Pylori Infection. Medicine 2019, 98, e16601. [Google Scholar] [CrossRef] [PubMed]
- Hajiaghamohammadi, A.A.; Zargar, A.; Oveisi, S.; Samimi, R.; Reisian, S. To Evaluate of the Effect of Adding Licorice to the Standard Treatment Regimen of Helicobacter Pylori. Braz. J. Infect. Dis. 2016, 20, 534–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohtashami, R.; Huseini, H.F.; Heydari, M.; Amini, M.; Sadeqhi, Z.; Ghaznavi, H.; Mehrzadi, S. Efficacy and Safety of Honey Based Formulation of Nigella Sativa Seed Oil in Functional Dyspepsia: A Double Blind Randomized Controlled Clinical Trial. J. Ethnopharmacol. 2015, 175, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Dabos, K.J.; Sfika, E.; Vlatta, L.J.; Giannikopoulos, G. The Effect of Mastic Gum on Helicobacter Pylori: A Randomized Pilot Study. Phytomedicine 2010, 17, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Zojaji, H.; Talaie, R.; Mirsattari, D.; Haghazali, M.; Molaei, M.; Mohsenian, N.; Derakhshan, F.; Zali, M.R. The Efficacy of Helicobacter Pylori Eradication Regimen with and without Vitamin C Supplementation. Dig. Liver Dis. 2009, 41, 644–647. [Google Scholar] [CrossRef]
- Sezikli, M.; Çetinkaya, Z.A.; Güzelbulut, F.; Yeşil, A.; Coşgun, S.; Kurdaş, O.Ö. Supplementing Vitamins C and e to Standard Triple Therapy for the Eradication of Helicobacter Pylori. J. Clin. Pharm. Ther. 2012, 37, 282–285. [Google Scholar] [CrossRef]
- Sezikli, M.; Çetinkaya, Z.A.; Sezikli, H.; Güzelbulut, F.; Tiftikçi, A.; Tüzün Ince, A.; Gökden, Y.; Yaşar, B.; Atalay, S.; Övünç Kurdaş, O. Oxidative Stress in Helicobacter Pylori Infection: Does Supplementation with Vitamins C and e Increase the Eradication Rate? Helicobacter 2009, 14, 280–285. [Google Scholar] [CrossRef]
- Everett, S.M.; Drake, I.M.; White, K.L.M.; Mapstone, N.P.; Chalmers, D.M.; Schorah, C.J.; Axon, A.T.R. Antioxidant Vitamin Supplements Do Not Reduce Reactive Oxygen Species Activity in Helicobacter Pylori Gastritis in the Short Term. Br. J. Nutr. 2002, 87, 3–11. [Google Scholar] [CrossRef]
- Chuang, C.H.; Sheu, B.S.; Kao, A.W.; Cheng, H.C.; Huang, A.H.; Yang, H.B.; Wu, J.J. Adjuvant Effect of Vitamin C on Omeprazole-Amoxicillin-Clarithromycin Triple Therapy for Helicobacter Pylori Eradication. Hepatogastroenterology 2007, 54, 320–324. [Google Scholar]
- Demirci, H.; Ilikhan, S.U.; Öztürk, K.; Üstündağ, Y.; Kurt, Ö.; Bilici, M.; Köktürk, F.; Uygun, A. Influence of Vitamin C and E Supplementation on the Eradication Rates of Triple and Quadruple Eradication Regimens for Helicobacter Pylori Infection. Turk. J. Gastroenterol. 2015, 26, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.; Luo, H.Q.; Xu, H.; Lv, N.H.; Shi, R.H.; Luo, H.S.; Li, J.S.; Ren, J.L.; Zou, Y.Y.; Li, Y.Q.; et al. Polaprezinc Combined with Clarithromycin Based Triple Therapy for Helicobacter Pylori Associated Gastritis: A Prospective, Multicenter, Randomized Clinical Trial. PLoS ONE 2017, 12, e0175625. [Google Scholar] [CrossRef] [PubMed]
- Kashimura, H.; Suzuki, K.; Hassan, M.; Ikezawa, K.; Sawahata, T.; Watanabe, T.; Nakahara, A.; Mutoh, H.; Tanaka, N. Polaprezinc, a Mucosal Protective Agent, in Combination with Lansoprazole, Amoxycillin and Clarithromycin Increases the Cure Rate of Helicobacter Pylori Infection. Aliment. Pharmacol. Ther. 1999, 13, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, K.; Parhizkar, B.; Sheikhesmaeili, F.; Roshani, M.; Nayebi, M.; Gharibi, F. Efficacy of Zinc Sulfate in Peptic Ulcer Disease: A Randomized Double-Blind Clinical Trial Study. J. Clin. Diagn. Res. 2016, 10, OC11. [Google Scholar] [CrossRef]

{kind=link}
| Study Design | Study Sample | Experimental Intervention | Control Intervention | Main Outcomes | References |
|---|---|---|---|---|---|
| RCT | 32 patients underwent gastroscopy (23 patients completed trial) | Cinnamon extract (40 mg twice daily) for 4 weeks | Placebo | Slight and non-significant improvement in urea breath counts. | [62] |
| RCT | 86 diabetic patients with positive H. pylori stool antigen test (77 patients completed trial) | Broccoli sprouts powder (6 g/day) alone or in combination with standard triple therapy for 4 weeks | Standard triple therapy (omeprazole 20 mg, clarithromycin 500 mg, amoxicillin 1000 mg) | H. pylori eradication rates with Broccoli sprouts powder, standard triple therapy, and combination of both were 56%, 89.3% and 91.7%, respectively. | [63] |
| RCT | 89 volunteer subjects randomized in group A (H. pylori positive, broccoli sprout extract containing sulforaphane), group B (placebo) and group C (H. pylori negative, broccoli sprout extract containing sulforaphane). | One capsule containing 250 mg broccoli sprout extract yielding 1000 μg sulforaphane. | Placebo | No significant effect was found in treatment group regards to H. pylori infection density. MDA concentration was significantly reduced in groups A and C with broccoli sprout treatment. | [64] |
| Controlled clinical trial | 25 H. pylori positive patients (mean age: 50 ± 12 years) with functional dyspepsia | Curcumin 30 mg, bovine lactoferrin 100 mg, N-acetylcysteine 600 mg, and pantoprazole 20 mg twice daily for 7 days | - | Significant improvement of the severity of symptoms and serologic signs of gastric inflammation. 12% H. pylori eradication rate. | [65] |
| RCT | 68 H. pylori positive patients aged 20–50 years with peptic ulcer (60 patients, 30 in each group completed study) | Curcumin 500 mg/day, as adjunct to standard triple therapy (clarithromycin 500 mg, amoxicillin 1000 mg, and pantoprazole 40 mg twice daily) | Placebo | Improvement of dyspepsia in curcumin group was significantly higher (27.6%) vs. placebo (6.7%). H. pylori eradication rate was 73.3% in both groups. | [66] |
| RCT | H. pylori patients were randomized in two groups, 50 patients each, with mean age of 54.65 ± 16.54 in triple therapy group, and 53.65 ± 15.65 in triple therapy + curcumin group. | Triple therapy twice a day for one week + turmeric tablets (700 mg) thrice a day for 28 days. | Triple therapy (omeprazole, amoxicillin, and metronidazole) twice a day for one week. | Significantly decrease in MDA levels and increase in TAC of the gastric mucosa in triple therapy + curcumin treated patients. | [67] |
| RCT | 36 patients (47% males and 53% females) with mean age of 40.87 ± 16.45 years in the treatment group and 35.40 ± 11.26 years in the control group | 2 tablets of garlic powder daily (2 g each) for 8 weeks. | Placebo | 87% H. pylori negative cases in Garlic treated group and 73% H. pylori negative cases in placebo group, as confirmed by UBT. | [68] |
| Pilot study | 20 dyspeptic patients aged 18–75 years with positive H. pylori (5 patients completed study) | Garlic oil capsule (4 mg) four times daily for 14 days | - | No improvement in H. pylori symptoms or eradication | [69] |
| Single-center, prospective crossover study | 12 healthy H. pylori infected adults (average age: 41.4 years) |
| Bismuth subsalicylate (2 tablets) with 3 meals per test day | No beneficial effects by garlic or capsaicin on H. pylori. Median urease activity before and after therapy for garlic was 28.5 vs. 39.8, for capsaicin was 43.7 vs. 46.6, and for bismuth was 55.8 vs. 14.3. | [70] |
| RCT | 40 volunteers with H. pylori infection | Burdock complex (Arctium lappa, Angelica sinensis, Lithospermum erythrorhizon, and Sesamum indicum oil) 2 bottles (2 × 10 mL) every day after breakfast and dinner, for 8 weeks. | Placebo | A significant decrease in urea breath counts and inflammatory markers (TNF-α and IL-8), and improved antioxidant capacity, with Burdock complex | [71] |
| RCT | 107 participants with H. pylori infection, aged 18–45 years | GutGard (Root extract of Glycyrrhiza glabra) 150 mg for 60 days | Placebo | H. pylori stool antigen (HpSA) was negative in 56% and 4% of patients treated with GutGard or placebo, respectively | [72] |
| RCT | 88 H. pylori patients, with non-ulcer dyspepsia (age range of 18–65 years) | 1-, 2- or 3-g Nigella sativa + 40 mg omeprazole | Standard triple therapy (clarithromycin, amoxicillin, and omeprazole) | No significant difference in H. pylori eradication rate between triple therapy (82.6%) and 2-g N. sativa (66.7%). Effect on dyspeptic symptoms was similar in all groups. | [73] |
| RCT | 142 patients aged 19–70 years were enrolled in the trial. | Fermented milk containing 1.0 × 106 CFU/mL L. paracasei HP7 and 100 mg G. glabra. | Placebo | Significant improvement in GI symptoms, 13C-UBT scores, and chronic inflammation was observed in treatment group. | [74] |
| RCT | 120 patients suffering from non-ulcer dyspepsia or peptic ulcer disease randomized into treatment group (mean age: 38.8 years) or control group (mean age: 40.1 years). | Clarithromycin based triple regimen + G. glabra 380 mg twice daily, for 2 weeks. | Clarithromycin based triple regimen (clarithromycin twice daily, amoxicillin once daily, omeprazole twice daily), for 2 weeks. | H. pylori eradication rate for treatment and control groups was found as 83.3% and 62.5%, respectively. | [75] |
| RCT | 70 patients were randomized in treatment (mean age: 42.31713.85) and control (mean age: 36.31713.64) groups. | Anti-secretory agent 1 + honey-based formulation of N. sativa (5 mL N. sativa) once daily, for 8 weeks. | Placebo | The mean Hong Kong index of dyspepsia scores and H. pylori infection rates were significantly lower in treatment group. | [76] |
| RCT | 52 H. pylori positive patients were randomized in group A (low dose mastic gum), group B (high dose mastic gum), group C (pantoprazole), and group D (standard therapy). | Pure mastic gum [350 mg (group A) or 1 g (group B) thrice daily] or combination of pure mastic gum (350 mg thrice daily) and pantoprazole (20 mg twice daily) (group C). | Standard therapy (pantoprazole 20 mg, amoxicillin 1 g and clarithromycin 500 mg) for 10 days (group D). | H. pylori eradication was observed in 4/13 patients in group A, 5/13 patients in group B, none of the patients in group C, and 10/13 patients in group D. No significant differences were found in mean UBT values in groups A, B and C. | [77] |
| Study Design | Study Samples | Experimental Intervention | Control Intervention | Main Outcomes | References |
|---|---|---|---|---|---|
| RCT | 312 patients, with an indication for endoscopy of dyspeptic symptoms were randomized in group A (n = 162; mean age: 45 years) and group B (n = 150; mean age: 43 years). | Standard therapy (amoxicillin 1 g, metronidazole 500 mg, bismuth 240 mg and omeprazole 40 mg) plus Vitamin C 500 mg/day (Group B). | Standard therapy (amoxicillin 1 g, metronidazole 500 mg, bismuth 240 mg and omeprazole 40 mg) (Group A). | H. pylori eradication rates in group B was significantly higher (78%) than group A (48.8%). | [78] |
| RCT | 200 patients were randomized in group A (mean age: 39.7 ± 10) and group B (mean age: 42.7 ± 10.8). | Standard triple therapy (lansoprazole, amoxicillin, and clarithromycin) for 14 days plus vitamins C (500 mg) and E (200 mg) for 30 days (Group A). | Standard triple therapy alone for 14 days (Group B). | H. pylori eradication rates in group A was significantly higher as compared to group B. | [79] |
| RCT | 160 patients were randomized in group A (mean age: 44 ± 10) and group B (mean age: 43 ± 11) | Conventional therapy for 2 weeks plus vitamins C (1000 mg/day) and E (400 IU/day) for 1 month (Group B). | Conventional anti-H. pylori therapy (lansoprazole, amoxicillin, clarithromycin, and bismuth subcitrate) for 2 weeks (Group A). | H. pylori eradication rates were significantly higher in group B. No difference was found in TAC among both groups. | [80] |
| RCT | 117 patients were randomized into 4 groups: conventional therapy, vitamins (C and E), combination of both or placebo. | Triple therapy alone ( Bismuth chelate, tetracycline, and metronidazole for 2 weeks ), vitamins C (200 mg) and E (50 mg) twice a day for 4 weeks, or combination of both treatments. | Placebo | No significant effect was found on MDA levels and ROS with vitamins supplementation. | [81] |
| RCT | 171 H. pylori infected patients. | One-week triple therapies of omeprazole and amoxicillin, plus on the following twice daily: (1) clarithromycin 250 mg; (2) clarithromycin 250 mg and vitamin C 500 mg; (3) clarithromycin 500 mg | Clarithromycin 250 and 500 mg. | Combination of clarithromycin 250 and vitamin C showed higher eradication rates than clarithromycin 250 mg, and equivalent eradication rates to clarithromycin 500 mg. | [82] |
| RCT | 400 patients, with non-ulcer dyspepsia. The patients were randomized in 4 groups, 100 patients each: Group A aged 26–66 years), Group B (aged 21–65 years), Group C (aged 24–66 years) and Group D (aged 22–65 years). | Triple therapy for 2 weeks plus vitamins C (500 mg/day) and E (100 U/day) for 1 month (Group B).Quadruple therapy for 2 weeks plus vitamins C (500 mg/day) and E (100 U/day) for 1 month (Group D). | Standard triple therapy (amoxicillin, clarithromycin, and lansoprazole) for 2 weeks (Group A). Standard quadruple therapy (amoxicillin, clarithromycin, lansoprazole, and bismuth subcitrate) for 2 weeks (Group C). | No difference was found in H. pylori eradication rates among Groups A and B, and similarly Group C and D. | [83] |
| RCT | 332 patients with H. pylori associated gastritis, aged 18–70 years infection. |
| Triple therapy (omeprazole, amoxicillin, and clarithromycin) for 14 days. | Triple therapy in combination with Polaprezinc 75/150 mg showed higher efficacy in eradication of infection, with no significant difference between both groups. | [84] |
| RCT | 66 patients (mean age: 48.5 years) suffering from dyspeptic symptoms with H. pylori infection. | Triple therapy plus polaprezinc 150 mg twice daily. | Triple therapy (lansoprazole, amoxycillin and clarithromycin) twice daily. | Triple therapy in combination with polaprezinc showed in improvement of infection eradication rates. | [85] |
| RCT | 90 patients with peptic ulcer disease and with mean age 47.5 ± 17.2 years in intervention group, and 52.6 ± 18.4 years in placebo group. | Standard triple therapy plus zinc 220 mg/day for 2 weeks. | Placebo | No significant difference was found between both groups in infection eradication, and improvement of peptic ulcer disease. | [86] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullah, H.; Di Minno, A.; Santarcangelo, C.; Khan, H.; Xiao, J.; Arciola, C.R.; Daglia, M. Vegetable Extracts and Nutrients Useful in the Recovery from Helicobacter pylori Infection: A Systematic Review on Clinical Trials. Molecules 2021, 26, 2272. https://doi.org/10.3390/molecules26082272
Ullah H, Di Minno A, Santarcangelo C, Khan H, Xiao J, Arciola CR, Daglia M. Vegetable Extracts and Nutrients Useful in the Recovery from Helicobacter pylori Infection: A Systematic Review on Clinical Trials. Molecules. 2021; 26(8):2272. https://doi.org/10.3390/molecules26082272
Chicago/Turabian StyleUllah, Hammad, Alessandro Di Minno, Cristina Santarcangelo, Haroon Khan, Jianbo Xiao, Carla Renata Arciola, and Maria Daglia. 2021. "Vegetable Extracts and Nutrients Useful in the Recovery from Helicobacter pylori Infection: A Systematic Review on Clinical Trials" Molecules 26, no. 8: 2272. https://doi.org/10.3390/molecules26082272