
Acute Fluid Intake Impacts Assessment of Body Composition via Bioelectrical Impedance Analysis. A Randomized, Controlled Crossover Pilot Trial

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Assessment of Eligibility
2.3. Study Design
2.4. Trial Visits
2.5. Statistical Analysis
3. Results
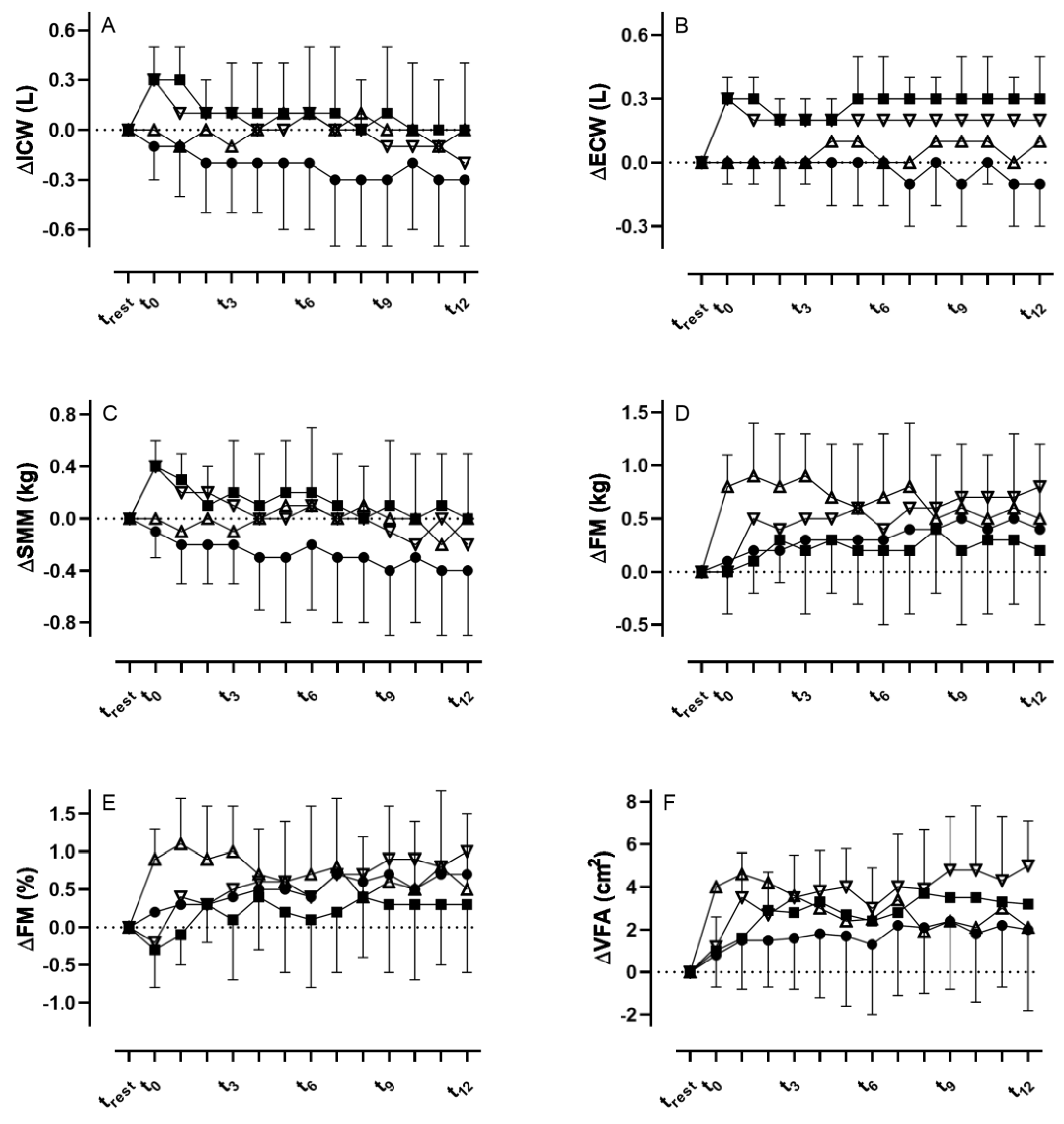
3.1. Intracellular Water
3.2. Extracellular Water
3.3. Total Body Water
3.4. Skeletal Muscle Mass
3.5. Body Fat Mass
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thibault, R.; Genton, L.; Pichard, C. Body composition: Why, when and for who? Clin. Nutr. 2012, 31, 435–447. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, A.; Piazza, P.; Noventa, D.; Pillon, L.; Zaccaria, M. A new method for monitoring hydration at high altitude by bioimpedance analysis. Med. Sci. Sport. Exerc. 1996, 28, 1517–1522. [Google Scholar] [CrossRef] [PubMed]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the bedside: Current applications, limitations, and opportunities. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef] [Green Version]
- Roumelioti, M.-E.; Glew, R.H.; Khitan, Z.J.; Rondon-Berrios, H.; Argyropoulos, C.P.; Malhotra, D.; Raj, D.S.; Agaba, E.I.; Rohrscheib, M.; Murata, G.H.; et al. Fluid balance concepts in medicine: Principles and practice. World J. Nephrol. 2018, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Gibas, C.; Grunewald, A.; Wunderlich, H.-W.; Marx, P.; Bruck, R. A wearable EIT system for detection of muscular activity in the extremities. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 2496–2499. [Google Scholar]
- Lobo, B.; Hermosa, C.; Abella, A.; Gordo, F. Electrical impedance tomography. Ann. Transl. Med. 2018, 6, 26. [Google Scholar] [CrossRef]
- Coutinho, A.B.B.; Jotta, B.; Werneck-De-Castro, J.P.; Pino, A.; Souza, M.N. Invasive electrical impedance myography at different levels of contraction of gastrocnemius muscle of rat. Rev. Sci. Instrum. 2020, 91, 084103. [Google Scholar] [CrossRef]
- Ngo, C.; Munoz, C.; Lueken, M.; Hülkenberg, A.; Bollheimer, C.; Briko, A.; Kobelev, A.; Shchukin, S.; Leonhardt, S. A Wearable, Multi-Frequency Device to Measure Muscle Activity Combining Simultaneous Electromyography and Electrical Impedance Myography. Sensors 2022, 22, 1941. [Google Scholar] [CrossRef]
- Park, J.-W.; Baek, S.-H.; Sung, J.H.; Kim, B.-J. Predictors of Step Length from Surface Electromyography and Body Impedance Analysis Parameters. Sensors 2022, 22, 5686. [Google Scholar] [CrossRef]
- Zieliński, G.; Byś, A.; Szkutnik, J.; Majcher, P.; Ginszt, M. Electromyographic Patterns of Masticatory Muscles in Relation to Active Myofascial Trigger Points of the Upper Trapezius and Temporomandibular Disorders. Diagnostics 2021, 11, 580. [Google Scholar] [CrossRef]
- Ward, L.C. Bioelectrical impedance analysis for body composition assessment: Reflections on accuracy, clinical utility, and standardisation. Eur. J. Clin. Nutr. 2018, 73, 194–199. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Johnson, P.E.; Bolonchuk, W.W.; Lykken, G.I. Assessment of fat-free mass using bioelectrical impedance measurements of the human body. Am. J. Clin. Nutr. 1985, 41, 810–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erselcan, T.; Candan, F.; Saruhan, S.; Ayca, T. Comparison of Body Composition Analysis Methods in Clinical Routine. Ann. Nutr. Metab. 2000, 44, 243–248. [Google Scholar] [CrossRef]
- Gomez, T.; Mole, P.A.; Collins, A. Dilution of body fluid electrolytes affects bioelectrical impedance measurements. Sport. Med. Train. Rehabil. 1993, 4, 291–298. [Google Scholar] [CrossRef]
- Roos, A.N.; Westendorp, R.G.; Frölich, M.; E Meinders, A. Tetrapolar body impedance is influenced by body posture and plasma sodium concentration. Eur. J. Clin. Nutr. 1992, 46, 53–60. [Google Scholar] [PubMed]
- Berneis, K.; Keller, U. Bioelectrical impedance analysis during acute changes of extracellular osmolality in man. Clin. Nutr. 2000, 19, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.J.; Cornish, B.H.; Ward, L.C.; Jacobs, A. Bioimpedance: Is it a predictor of true water volume? Ann. N. Y. Acad. Sci. 1999, 873, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Abu Khaled, M.; McCutcheon, M.J.; Reddy, S.; Pearman, P.L.; Hunter, G.R.; Weinsier, R.L. Electrical impedance in assessing human body composition: The BIA method. Am. J. Clin. Nutr. 1988, 47, 789–792. [Google Scholar] [CrossRef]
- O’Brien, C.; Young, A.J.; Sawka, M.N. Bioelectrical impedance to estimate changes in hydration status. Int. J. Sport. Med. 2002, 23, 361–366. [Google Scholar] [CrossRef]
- Schoeller, D.A. Changes in total body water with age. Am. J. Clin. Nutr. 1989, 50, 1176–1181. [Google Scholar] [CrossRef]
- Greendale, G.A.; Sternfeld, B.; Huang, M.; Han, W.; Karvonen-Gutierrez, C.; Ruppert, K.; Cauley, J.A.; Finkelstein, J.S.; Jiang, S.-F.; Karlamangla, A.S. Changes in body composition and weight during the menopause transition. JCI Insight 2019, 4, e124865. [Google Scholar] [CrossRef]
- Urbaniak, G.C.; Plous, S. Research Randomizer (Version 4.0) [Computer Software] [Internet]. Available online: https://randomizer.org/%0Aabout/ (accessed on 7 July 2021).
- Dixon, C.B.; Ramos, L.; Fitzgerald, E.; Reppert, D.; Andreacci, J.L. The effect of acute fluid consumption on measures of impedance and percent body fat estimated using segmental bioelectrical impedance analysis. Eur. J. Clin. Nutr. 2009, 63, 1115–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemmey, A.; Eston, R.; Moloney, S.; Yeomans, J. Effects of hydration state and rehydration method on bioelectrical impedance analysis. S. Afr. J. Sport. Med. 2000, 7, 8–12. [Google Scholar]
- Androutsos, O.; Gerasimidis, K.; Karanikolou, A.; Reilly, J.J.; Edwards, C.A. Impact of eating and drinking on body composition measurements by bioelectrical impedance. J. Hum. Nutr. Diet. 2015, 28, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Liang, M.T.C.; Su, H.-F.; Lee, N.-Y. Skin temperature and skin blood flow affect bioelectric impedance study of female fat-free mass. Med. Sci. Sport. Exerc. 2000, 32, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Cornish, B.; Thomas, B.; Ward, L. Effect of temperature and sweating on bioimpedance measurements. Appl. Radiat. Isot. 1998, 49, 475–476. [Google Scholar] [CrossRef] [PubMed]
- Kukliński, J.; Steckiewicz, K.P.; Sekuła, B.; Aszkiełowicz, A.; Owczuk, R. The influence of fasting and carbohydrate-enriched drink administration on body water amount and distribution: A volunteer randomized study. Perioper. Med. 2021, 10, 27. [Google Scholar] [CrossRef]
- Slinde, F.; Grönberg, A.M.; Engström, C.P.; Rossander-Hulthén, L.; Larsson, S. Body composition by bioelectrical impedance predicts mortality in chronic obstructive pulmonary disease patients. Respir. Med. 2005, 99, 1004–1009. [Google Scholar] [CrossRef] [Green Version]
- Haverkort, E.B.; Reijven, P.L.M.; Binnekade, J.M.; De Van Der Schueren, M.A.E.; Earthman, C.P.; Gouma, D.J.; De Haan, R.J. Bioelectrical impedance analysis to estimate body composition in surgical and oncological patients: A systematic review. Eur. J. Clin. Nutr. 2014, 69, 3–13. [Google Scholar] [CrossRef]
- Fredrix, E.W.; Saris, W.H.; Soeters, P.B.; Wouters, E.F.; Kester, A.D.; Von Meyenfeldt, M.F.; Westerterp, K.R. Estimation of body composition by bioelectrical impedance in cancer patients. Eur. J. Clin. Nutr. 1990, 44, 749–752. [Google Scholar]

{kind=link}
| 0.9% Sodium Chloride | Ringer | G5 | |
|---|---|---|---|
| Na+ (mmol∙L−1) | 154 | 147 | 0 |
| Cl− (mmol∙L−1) | 154 | 156 | 0 |
| Ka+ (mmol∙L−1) | 0 | 4 | 0 |
| Ca2+ (mmol∙L−1) | 0 | 2.2 | 0 |
| Glucose (g) | 0 | 0 | 50 |
| Osm 1 (mOsm∙L−1) | 308 | 309 | 278 |
| Mean ± SD | 95% CI | p-Value | ||
|---|---|---|---|---|
| TBW (L) | CON | 41.3 ± 8.9 | 36.9–45.8 | >0.99 |
| ISO | 41.6 ± 9.0 | 36.9–46.2 | >0.99 | |
| GLU | 41.3 ± 9.1 | 36.7–45.8 | >0.99 | |
| RIN | 42.1 ± 2.8 | 37.3–47.0 | >0.99 | |
| ICW (L) | CON | 26.0 ± 5.6 | 23.2–28.8 | >0.99 |
| ISO | 26.1 ± 5.6 | 23.2–29.0 | >0.99 | |
| GLU | 26.5 ± 5.7 | 23.4–29.5 | >0.99 | |
| RIN | 25.9 ± 5.7 | 23.1–28.8 | >0.99 | |
| ECW (L) | CON | 15.4 ± 3.3 | 13.7–17.0 | >0.99 |
| ISO | 15.4 ± 3.4 | 13.7–17.2 | >0.99 | |
| GLU | 15.7 ± 3.4 | 13.8–17.5 | >0.99 | |
| RIN | 15.4 ± 3.4 | 13.7–17.0 | >0.99 | |
| SMM (kg) | CON | 31.9 ± 7.3 | 28.3–35.5 | >0.99 |
| ISO | 32.1 ± 7.3 | 28.3–25.9 | >0.99 | |
| GLU | 32.6 ± 7.5 | 28.6–36.5 | >0.99 | |
| RIN | 31.8 ± 7.5 | 28.1–35.5 | >0.99 | |
| FM (kg) | CON | 13.0 ± 3.9 | 11.0–14.9 | >0.99 |
| ISO | 14.7 ± 6.1 | 11.5–17.8 | >0.99 | |
| GLU | 12.6 ± 3.7 | 10.7–14.6 | >0.99 | |
| RIN | 13.3 ± 3.6 | 11.5–15.1 | >0.99 | |
| FM (%) | CON | 19.0 ± 5.4 | 16.3–21.7 | >0.99 |
| ISO | 19.4 ± 5.1 | 16.8–22.0 | >0.99 | |
| GLU | 18.3 ± 5.3 | 15.5–21.2 | >0.99 | |
| RIN | 19.4 ± 5.3 | 16.8–22.1 | >0.99 | |
| VFA (cm2) | CON | 51.3 ± 19.9 | 41.4–61.2 | >0.99 |
| ISO | 52.8 ± 18.3 | 43.4–62.2 | >0.99 | |
| GLU | 49.7 ± 19.2 | 39.4–59.9 | >0.99 | |
| RIN | 52.6 ± 18.4 | 43.5–61.8 | >0.99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schierbauer, J.; Günther, S.; Haupt, S.; Zimmer, R.T.; Herz, D.; Voit, T.; Zimmermann, P.; Wachsmuth, N.B.; Aberer, F.; Moser, O. Acute Fluid Intake Impacts Assessment of Body Composition via Bioelectrical Impedance Analysis. A Randomized, Controlled Crossover Pilot Trial. Metabolites 2023, 13, 473. https://doi.org/10.3390/metabo13040473
Schierbauer J, Günther S, Haupt S, Zimmer RT, Herz D, Voit T, Zimmermann P, Wachsmuth NB, Aberer F, Moser O. Acute Fluid Intake Impacts Assessment of Body Composition via Bioelectrical Impedance Analysis. A Randomized, Controlled Crossover Pilot Trial. Metabolites. 2023; 13(4):473. https://doi.org/10.3390/metabo13040473
Chicago/Turabian StyleSchierbauer, Janis, Svenja Günther, Sandra Haupt, Rebecca T. Zimmer, Daniel Herz, Thomas Voit, Paul Zimmermann, Nadine B. Wachsmuth, Felix Aberer, and Othmar Moser. 2023. "Acute Fluid Intake Impacts Assessment of Body Composition via Bioelectrical Impedance Analysis. A Randomized, Controlled Crossover Pilot Trial" Metabolites 13, no. 4: 473. https://doi.org/10.3390/metabo13040473