
Hepatocrinology


Abstract
1. Introduction
2. The Liver as an Endocrine Organ
2.1. Insulin-Like Growth Factor and Insulin-Like Growth Factor Binding Proteins
2.2. Angiotensinogen
2.3. Thrombopoietin
2.4. Betatrophin and Proprotein Convertase Subtilsin-Kexin Type 9 (PCSK9)
2.5. Hormone-Transport Proteins
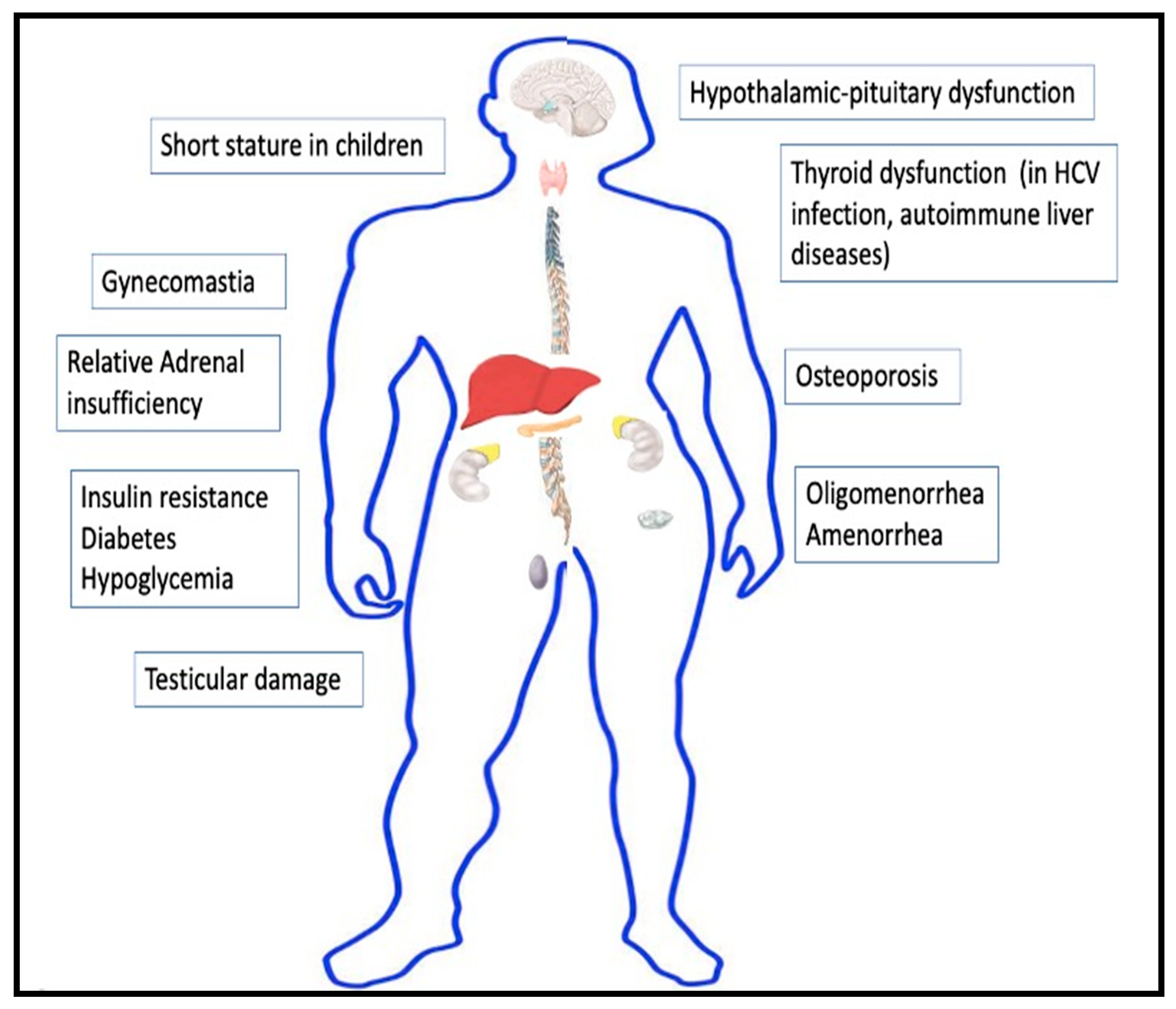
3. Endocrine Manifestations of Hepatic Disease
3.1. Insulin Resistance and Diabetes
3.2. Hypoglycemia
3.3. Gonadal Dysfunction
3.4. Skeletal Manifestations
3.5. Thyroid Disorders
3.6. Adrenal Insufficiency
3.7. Growth Disorders in Children
4. Hepatic Manifestations of Endocrine Disease
4.1. Non-Alcoholic Fatty Liver Disease
4.2. Secondary NAFLD from Other Endocrine Disorders
4.3. Other Hepatic Manifestations of Endocrine Disorders
5. Sexual Dimorphism in Liver Disorders
6. Liver Function Biochemical Markers as Predictors of Endocrine Dysfunction
7. Hepato-Endocrine Syndromes
8. Hepatic Effect of Endocrine Drugs
9. Endocrine Effects of Drugs Used in Hepatology
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wewer Albrechtsen, N.J.; Pedersen, J.; Galsgaard, K.D.; Winther-Sørensen, M.; Suppli, M.P.; Janah, L.; Gromada, J.; Vilstrup, H.; Knop, F.K.; Holst, J.J. The Liver-α-Cell Axis and Type 2 Diabetes. Endocr. Rev. 2019, 40, 1353–1366. [Google Scholar] [CrossRef]
- Bach, L.A. IGF-binding proteins. J. Mol. Endocrinol. 2018, 61, T11–T28. [Google Scholar] [CrossRef] [PubMed]
- Raghow, R. Betatrophin: A liver-derived hormone for the pancreatic β-cell proliferation. World J. Diabetes 2013, 4, 234–237. [Google Scholar] [CrossRef]
- Matsusaka, T.; Niimura, F.; Shimizu, A.; Pastan, I.; Saito, A.; Kobori, H.; Nishiyama, A.; Ichikawa, I. Liver Angiotensinogen Is the Primary Source of Renal Angiotensin II. J. Am. Soc. Nephrol. 2012, 23, 1181–1189. [Google Scholar] [CrossRef]
- Ruchala, P.; Nemeth, E. The pathophysiology and pharmacology of hepcidin. Trends Pharmacol. Sci. 2014, 35, 155–161. [Google Scholar] [CrossRef]
- Hitchcock, I.S.; Kaushansky, K. Thrombopoietin from beginning to end. Br. J. Haematol. 2014, 165, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Yadav, K.; Sharma, M.; Ferdinand, K. Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors: Present perspectives and future horizons. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Allard, J.B.; Duan, C. IGF-Binding Proteins: Why Do They Exist and Why Are There So Many? Front. Endocrinol. 2018, 9, 117. [Google Scholar] [CrossRef]
- Selby, C. Sex Hormone Binding Globulin: Origin, Function and Clinical Significance. Ann. Clin. Biochem. Int. J. Lab. Med. 1990, 27, 532–541. [Google Scholar] [CrossRef]
- Schussler, G.C. The Thyroxine-Binding Proteins. Thyroid 2000, 10, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Palha, J.A. Transthyretin as a Thyroid Hormone Carrier: Function Revisited. Clin. Chem. Lab. Med. 2002, 40, 1292–1300. [Google Scholar] [CrossRef]
- Breuner, C.W.; Beyl, H.E.; Malisch, J.L. Corticosteroid-binding globulins: Lessons from biomedical research. Mol. Cell. Endocrinol. 2020, 514, 110857. [Google Scholar] [CrossRef]
- Bouillon, R.; Schuit, F.; Antonio, L.; Rastinejad, F. Vitamin D Binding Protein: A Historic Overview. Front. Endocrinol. 2020, 10, 910. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Zhou, X.-X.; Hu, Y.; Li, G.; Wang, Y. The Roles of Insulin-Like Growth Factor Binding Protein Family in Development and Diseases. Adv. Ther. 2021, 38, 885–903. [Google Scholar] [CrossRef] [PubMed]
- Scharf, J.; Ramadori, G.; Braulke, T.; Hartmann, H. Synthesis of insulinlike growth factor binding proteins and of the acid-labile subunit in primary cultures of rat hepatocytes, of Kupffer cells, and in cocultures: Regulation by insulin, insulinlike growth factor, and growth hormone. Hepatology 1996, 23, 818–827. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Leví, A.M.; Marazuela, M. Treatment of adult growth hormone deficiency with human recombinant growth hormone: An update on current evidence and critical review of advantages and pitfalls. Endocrine 2018, 60, 203–218. [Google Scholar] [CrossRef]
- Engström, W.; Shokrai, A.; Otte, K.; Granerus, M.; Gessbo, A.; Bierke, P.; Madej, A.; Sjolund, M.; Ward, A. Transcriptional regulation and biological significance of the insulin like growth factor II gene. Cell Prolif. 1998, 31, 173–189. [Google Scholar] [CrossRef]
- Adamek, A.; Kasprzak, A. Insulin-Like Growth Factor (IGF) System in Liver Diseases. Int. J. Mol. Sci. 2018, 19, 1308. [Google Scholar] [CrossRef] [PubMed]
- Colakoğlu, O.; Taşkiran, B.; Colakoğlu, G.; Kizildağ, S.; Ari Ozcan, F.; Unsal, B. Serum insulin like growth factor-1 (IGF-1) and insulin like growth factor binding protein-3 (IGFBP-3) levels in liver cirrhosis. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2007, 18, 245–249. [Google Scholar]
- Stanley, T.L.; Fourman, L.T.; Zheng, I.; McClure, C.M.; Feldpausch, M.N.; Torriani, M.; E Corey, K.; Chung, R.T.; Lee, H.; E Kleiner, D.; et al. Relationship of IGF-1 and IGF-Binding Proteins to Disease Severity and Glycemia in Nonalcoholic Fatty Liver Disease. J. Clin. Endocrinol. Metab. 2021, 106, e520–e533. [Google Scholar] [CrossRef] [PubMed]
- Miyauchi, S.; Miyake, T.; Miyazaki, M.; Eguchi, T.; Niiya, T.; Yamamoto, S.; Senba, H.; Furukawa, S.; Matsuura, B.; Hiasa, Y. Insulin-like growth factor-1 is inversely associated with liver fibrotic markers in patients with type 2 diabetes mellitus. J. Diabetes Investig. 2018, 10, 1083–1091. [Google Scholar] [CrossRef]
- Takahashi, Y. The Role of Growth Hormone and Insulin-Like Growth Factor-I in the Liver. Int. J. Mol. Sci. 2017, 18, 1447. [Google Scholar] [CrossRef]
- Christopoulos, P.F.; Msaouel, P.; Koutsilieris, M. The role of the insulin-like growth factor-1 system in breast cancer. Mol. Cancer 2015, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Bleach, R.; Sherlock, M.; O’Reilly, M.W.; McIlroy, M. Growth Hormone/Insulin Growth Factor Axis in Sex Steroid Associated Disorders and Related Cancers. Front. Cell Dev. Biol. 2021, 9, 630503. [Google Scholar] [CrossRef] [PubMed]
- Morgan, L.; Pipkin, F.B.; Kalsheker, N. Angiotensinogen: Molecular biology, biochemistry and physiology. Int. J. Biochem. Cell Biol. 1996, 28, 1211–1222. [Google Scholar] [CrossRef]
- Leenen, F.H.H.; Blaustein, M.P.; Hamlyn, J.M. Update on angiotensin II: New endocrine connections between the brain, adrenal glands and the cardiovascular system. Endocr. Connect. 2017, 6, R131–R145. [Google Scholar] [CrossRef] [PubMed]
- Sarzani, R.; Giulietti, F.; Di Pentima, C.; Giordano, P.; Spannella, F. Disequilibrium between the classic renin-angiotensin system and its opposing arm in SARS-CoV-2-related lung injury. Am. J. Physiol. Lung Cell Mol. Physiol. 2020, 319, L325–L336. [Google Scholar] [CrossRef]
- Datta, P.K.; Liu, F.; Fischer, T.; Rappaport, J.; Qin, X. SARS-CoV-2 pandemic and research gaps: Understanding SARS-CoV-2 interaction with the ACE2 receptor and implications for therapy. Theranostics 2020, 10, 7448–7464. [Google Scholar] [CrossRef] [PubMed]
- Drachman, J.G. Role of thrombopoietin in hematopoietic stem cell and progenitor regulation. Curr. Opin. Hematol. 2000, 7, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Abu-Farha, M.; Al Madhoun, A.; Abubaker, J. The Rise and the Fall of Betatrophin/ANGPTL8 as an Inducer of β-Cell Proliferation. J. Diabetes Res. 2016, 2016, 4860595. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Teng, C. Angiopoietin-like proteins 3, 4 and 8: Regulating lipid metabolism and providing new hope for metabolic syndrome. J. Drug Target. 2014, 22, 679–687. [Google Scholar] [CrossRef]
- Navaeian, M.; Asadian, S.; Yazdi, H.A.; Gheibi, N. ANGPTL8 roles in proliferation, metabolic diseases, hypothyroidism, polycystic ovary syndrome, and signaling pathways. Mol. Biol. Rep. 2021, 1–13. [Google Scholar] [CrossRef]
- Reiss, A.B.; Shah, N.; Muhieddine, D.; Zhen, J.; Yudkevich, J.; Kasselman, L.J.; DeLeon, J. PCSK9 in cholesterol metabolism: From bench to bedside. Clin. Sci. 2018, 132, 1135–1153. [Google Scholar] [CrossRef]
- Wong, N.D.; Rosenblit, P.D.; Greenfield, R.S. Advances in dyslipidemia management for prevention of atherosclerosis: PCSK9 monoclonal antibody therapy and beyond. Cardiovasc. Diagn. Ther. 2017, 67, S11–S20. [Google Scholar] [CrossRef] [PubMed]
- Henley, D.; Lightman, S. New insights into corticosteroid-binding globulin and glucocorticoid delivery. Neuroscience 2011, 180, 1–8. [Google Scholar] [CrossRef]
- Qu, X.; Donnelly, R. Sex Hormone-Binding Globulin (SHBG) as an Early Biomarker and Therapeutic Target in Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2020, 21, 8191. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.J.; Kratzsch, J. Corticosteroid-binding globulin: Modulating mechanisms of bioavailability of cortisol and its clinical implications. Best Pract. Res. Clin. Endocrinol. Metab. 2015, 29, 761–772. [Google Scholar] [CrossRef]
- Tahboub, R.; Arafah, B.M. Sex steroids and the thyroid. Best. Pract. Res. Clin. Endocrinol. Metab. 2009, 23, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Bragança, A.C.C.; Alvares-Da-Silva, M.R. Prevalence of diabetes mellitus and impaired glucose tolerance in patients with decompensated cirrhosis being evaluated for liver transplantation: The utility of oral glucose tolerance test. Arq. Gastroenterol. 2010, 47, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Marselli, L.; De Simone, P.; Morganti, R.; Coletti, L.; Carrai, P.; Catalano, G.; Tincani, G.; Ghinolfi, D.; Occhipinti, M.; Filipponi, F.; et al. Frequency and characteristics of diabetes in 300 pre-liver transplant patients. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 441–442. [Google Scholar] [CrossRef] [PubMed]
- Holstein, A.; Hinze, S.; Thiessen, E.; Plaschke, A.; Egberts, E.-H. Clinical implications of hepatogenous diabetes in liver cirrhosis. J. Gastroenterol. Hepatol. 2002, 17, 677–681. [Google Scholar] [CrossRef]
- Orsi, E.; Grancini, V.; Menini, S.; Aghemo, A.; Pugliese, G. Hepatogenous diabetes: Is it time to separate it from type 2 diabetes? Liver Int. 2016, 37, 950–962. [Google Scholar] [CrossRef]
- Kumar, R. Hepatogenous diabetes: An underestimated problem of liver cirrhosis. Indian J. Endocrinol. Metab. 2018, 22, 552–559. [Google Scholar] [CrossRef]
- Petrides, A.S.; Stanley, T.; Matthews, D.E.; Vogt, C.; Bush, A.J.; Lambeth, H. Insulin resistance in cirrhosis: Prolonged reduction of hyperinsulinemia normalizes insulin sensitivity. Hepatology 1998, 28, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Fernando, D.H.; Forbes, J.M.; Angus, P.W.; Herath, C.B. Development and Progression of Non-Alcoholic Fatty Liver Disease: The Role of Advanced Glycation End Products. Int. J. Mol. Sci. 2019, 20, 5037. [Google Scholar] [CrossRef] [PubMed]
- Gao, T.-T.; Qin, Z.-L.; Ren, H.; Zhao, P.; Qi, Z.-T. Inhibition of IRS-1 by hepatitis C virus infection leads to insulin resistance in a PTEN-dependent manner. Virol. J. 2015, 12, 12. [Google Scholar] [CrossRef]
- Bose, S.K.; Shrivastava, S.; Meyer, K.; Ray, R.B.; Ray, R.B.; Ray, R. Hepatitis C Virus Activates the mTOR/S6K1 Signaling Pathway in Inhibiting IRS-1 Function for Insulin Resistance. J. Virol. 2012, 86, 6315–6322. [Google Scholar] [CrossRef] [PubMed]
- Lerat, H.; Imache, M.R.; Polyte, J.; Gaudin, A.; Mercey, M.; Donati, F.; Baudesson, C.; Higgs, M.R.; Picard, A.; Magnan, C.; et al. Hepatitis C virus induces a prediabetic state by directly impairing hepatic glucose metabolism in mice. J. Biol. Chem. 2017, 292, 12860–12873. [Google Scholar] [CrossRef]
- Manco, M. Insulin Resistance and NAFLD: A Dangerous Liaison beyond the Genetics. Children 2017, 4, 74. [Google Scholar] [CrossRef]
- Armandi, A.; Rosso, C.; Caviglia, G.; Bugianesi, E. Insulin Resistance across the Spectrum of Nonalcoholic Fatty Liver Disease. Metabolites 2021, 11, 155. [Google Scholar] [CrossRef]
- Nouel, O.; Bernuau, J.; Rueff, B.; Benhamou, J.P. Hypoglycemia. A common complication of septicemia in cirrhosis. Arch. Intern. Med. 1981, 141, 1477–1478. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.-J.; Liao, C.-J. Predisposing factors for hypoglycaemia in the emergency department. J. Int. Med. Res. 2019, 47, 2404–2412. [Google Scholar] [CrossRef]
- Kaur, S.; Kumar, P.; Kumar, V.; Sarin, S.K.; Kumar, A. Etiology and prognostic factors of acute liver failure in children. Indian Pediatr. 2013, 50, 677–679. [Google Scholar] [CrossRef]
- Pfortmueller, C.A.; Wiemann, C.; Funk, G.-C.; Leichtle, A.B.; Fiedler, G.M.; Exadaktylos, A.K.; Lindner, G. Hypoglycemia is associated with increased mortality in patients with acute decompensated liver cirrhosis. J. Crit. Care 2014, 29, 316.e7–316.e12. [Google Scholar] [CrossRef] [PubMed]
- Anno, T.; Kaneto, H.; Shigemoto, R.; Kawasaki, F.; Kawai, Y.; Urata, N.; Kawamoto, H.; Kaku, K.; Okimoto, N. Hypoinsulinemic hypoglycemia triggered by liver injury in elderly subjects with low body weight: Case reports. Endocrinol. Diabetes Metab. Case Rep. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Oldenbeuving, G.; McDonald, J.R.; Goodwin, M.L.; Sayilir, R.; Reijngoud, D.J.; Gladden, L.B.; Nijsten, M.W.N. A patient with acute liver failure and extreme hypoglycaemia with lactic acidosis who was not in a coma: Causes and consequences of lactate-protected hypoglycaemia. Anaesth. Intensive Care 2014, 42, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Liang, X.; Chen, Y.; Huang, F.; Fan, W.; Xue, J.; Li, C. Hepatocellular carcinoma with worsened hypoglycemia after transarterial chemoembolization: A case report and systematic review. Int. J. Clin. Exp. Pathol. 2020, 13, 3167–3173. [Google Scholar]
- Yu, B.; Douli, R.; Suarez, J.A.; Gutierrez, V.P.; Aldiabat, M.; Khan, M. Non-islet cell tumor hypoglycemia as an initial presentation of hepatocellular carcinoma coupled with end-stage liver cirrhosis: A case report and review of literature. World J. Hepatol. 2020, 12, 519–524. [Google Scholar] [CrossRef]
- Garg, M.K.; Puri, P.; Brar, K.S.; Pandit, A.; Srivastava, S.; Kharb, S. Assessment of thyroid and gonadal function in liver diseases. Indian J. Endocrinol. Metab. 2015, 19, 89–94. [Google Scholar] [CrossRef]
- Kumar, K.V.S.H.; Pawah, A.K.; Manrai, M. Occult endocrine dysfunction in patients with cirrhosis of liver. J. Fam. Med. Prim. Care 2016, 5, 576–580. [Google Scholar] [CrossRef]
- Valimäki, M.; Pelkonen, R.; Salaspuro, M.; Härkönen, M.; Hirvonen, E.; Ylikahri, R. Sex Hormones in Amenorrheic Women with Alcoholic Liver Disease. J. Clin. Endocrinol. Metab. 1984, 59, 133–138. [Google Scholar] [CrossRef]
- Cundy, T.F.; Butler, J.; Pope, R.M.; Saggar-Malik, A.K.; Wheeler, M.J.; Williams, R. Amenorrhoea in women with non-alcoholic chronic liver disease. Gut 1991, 32, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Foresta, C.; Schipilliti, M.; Ciarleglio, F.A.; Lenzi, A.; D’Amico, D. Male hypogonadism in cirrhosis and after liver transplantation. J. Endocrinol. Investig. 2008, 31, 470–478. [Google Scholar] [CrossRef]
- Cavanaugh, J.; Niewoehner, C.B.; Nuttall, F.Q. Gynecomastia and cirrhosis of the liver. Arch. Intern. Med. 1990, 150, 563–565. [Google Scholar] [CrossRef] [PubMed]
- Neong, S.F.; Billington, E.O.; Congly, S.E. Sexual Dysfunction and Sex Hormone Abnormalities in Patients with Cirrhosis: Review of Pathogenesis and Management. Hepatology 2018, 69, 2683–2695. [Google Scholar] [CrossRef]
- Sinclair, M.; Grossmann, M.; Gow, P.J.; Angus, P.W. Testosterone in men with advanced liver disease: Abnormalities and implications. J. Gastroenterol. Hepatol. 2015, 30, 244–251. [Google Scholar] [CrossRef]
- Zifroni, A.; Schiavi, R.C.; Schaffner, F. Sexual function and testosterone levels in men with nonalcoholic liver disease. Hepatology 1991, 14, 479–482. [Google Scholar] [CrossRef]
- Grossmann, M.; Hoermann, R.; Gani, L.; Chan, I.; Cheung, A.; Gow, P.J.; Li, A.; Zajac, J.D.; Angus, P. Low testosterone levels as an independent predictor of mortality in men with chronic liver disease. Clin. Endocrinol. 2012, 77, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Zietz, B.; Lock, G.; Plach, B.; Drobnik, W.; Grossmann, J.; Schölmerich, J.; Straub, R.H. Dysfunction of the hypothalamic-pituitary-glandular axes and relation to Child-Pugh classification in male patients with alcoholic and virus-related cirrhosis. Eur. J. Gastroenterol. Hepatol. 2003, 15, 495–501. [Google Scholar]
- Gluud, C.; Bahnsen, M.; Bennett, P.; Brodthagen, U.A.; Dietrichson, O.; Johnsen, S.G.; Nielsen, J.; Micic, S.; Svendsen, L.B.; Svenstrup, B. Hypothalamic-pituitary-gonadal function in relation to liver function in men with alcoholic cirrhosis. Scand. J. Gastroenterol. 1983, 18, 939–944. [Google Scholar] [CrossRef]
- Ehnert, S.; Aspera-Werz, R.H.; Ruoß, M.; Dooley, S.; Hengstler, J.G.; Nadalin, S.; Relja, B.; Badke, A.; Nussler, A.K. Hepatic Osteodystrophy-Molecular Mechanisms Proposed to Favor Its Development. Int. J. Mol. Sci. 2019, 20, 2555. [Google Scholar] [CrossRef] [PubMed]
- Guarino, M.; Loperto, I.; Camera, S.; Cossiga, V.; Di Somma, C.; Colao, A.; Caporaso, N.; Morisco, F. Osteoporosis across chronic liver disease. Osteoporos. Int. 2016, 27, 1967–1977. [Google Scholar] [CrossRef] [PubMed]
- Glass, L.M.; Su, G.L.-C. Metabolic Bone Disease in Primary Biliary Cirrhosis. Gastroenterol. Clin. N. Am. 2016, 45, 333–343. [Google Scholar] [CrossRef]
- Barbu, E.-C.; Chiţu-Tișu, C.-E.; Lazar, M.; Olariu, C.; Bojincă, M.; Ionescu, R.A.; Ion, D.A.; Badarau, I.A. Hepatic Osteodystrophy: A Global (Re)View of the Problem. Acta Clin. Croat. 2017, 56, 512–525. [Google Scholar] [CrossRef]
- Silveira, M.G.; Mendes, F.D.; Diehl, N.N.; Enders, F.T.; Lindor, K.D. Thyroid dysfunction in primary biliary cirrhosis, primary sclerosing cholangitis and non-alcoholic fatty liver disease. Liver Int. 2009, 29, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Ferri, C.; Fallahi, P.; Ferrari, S.M.; Ghinoi, A.; Rotondi, M.; Ferrannini, E. Thyroid Disorders in Chronic Hepatitis C Virus Infection. Thyroid. Off. J. Am. Thyroid. Assoc. 2006, 16, 563–572. [Google Scholar] [CrossRef]
- Wang, P.; Jing, Z.; Liu, C.; Xu, M.; Wang, P.; Wang, X.; Yin, Y.; Cui, Y.; Ren, D.; Rao, X. Hepatitis C virus infection and risk of thyroid cancer: A systematic review and meta-analysis. Arab. J. Gastroenterol. 2017, 18, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kalk, W.J.; Kew, M.C.; Danilewitz, M.D.; Jacks, F.; Van Der Walt, L.A.; Levin, J. Thyroxine Binding Globulin and Thyroid Function Tests in Patients with Hepatocellular Carcinoma. Hepatology 2007, 2, 72S–76S. [Google Scholar] [CrossRef] [PubMed]
- Nagasue, N.; Ohmori, H.; Hashimoto, N.; Tachibana, M.; Kubota, H.; Uchida, M.; Yu, L. Thyroxine-binding globulin and thyroid hormones after resection of hepatocellular carcinoma. Am. J. Gastroenterol. 1997, 92, 1187–1189. [Google Scholar]
- Fede, G.; Spadaro, L.; Tomaselli, T.; Privitera, G.; Germani, G.; Tsochatzis, E.; Thomas, M.; Bouloux, P.-M.; Burroughs, A.K.; Purrello, F. Adrenocortical dysfunction in liver disease: A systematic review. Hepatology 2012, 55, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Trifan, A.; Chiriac, S.; Stanciu, C. Update on adrenal insufficiency in patients with liver cirrhosis. World J. Gastroenterol. 2013, 19, 445–456. [Google Scholar] [CrossRef]
- Alonso, E.M. Growth and developmental considerations in pediatric liver transplantation. Liver Transplant. 2008, 14, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Bucuvalas, J.C.; Cutfield, W.; Horn, J.; Sperling, M.A.; Heubi, J.E.; Campaigne, B.; Chernausek, S.D. Resistance to the growth-promoting and metabolic effects of growth hormone in children with chronic liver disease. J. Pediatr. 1990, 117, 397–402. [Google Scholar] [CrossRef]
- Mohammad, S.; Grimberg, A.; Rand, E.; Anand, R.; Yin, W.; Alonso, E.M. Long-Term Linear Growth and Puberty in Pediatric Liver Transplant Recipients. J. Pediatr. 2013, 163, 1354–1360. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef]
- Watt, M.J.; Miotto, P.M.; De Nardo, W.; Montgomery, M. The Liver as an Endocrine Organ—Linking NAFLD and Insulin Resistance. Endocr. Rev. 2019, 40, 1367–1393. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, L.; Pafundi, P.; Galiero, R.; Caturano, A.; Morone, M.; Silvestri, C.; Giordano, M.; Salvatore, T.; Sasso, F. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrative Review. Antioxidants 2021, 10, 270. [Google Scholar] [CrossRef]
- Parthasarathy, G.; Revelo, X.; Malhi, H. Pathogenesis of Nonalcoholic Steatohepatitis: An Overview. Hepatol. Commun. 2020, 4, 478–492. [Google Scholar] [CrossRef]
- Seppälä-Lindroos, A.; Vehkavaara, S.; Häkkinen, A.-M.; Goto, T.; Westerbacka, J.; Sovijärvi, A.; Halavaara, J.; Yki-Järvinen, H. Fat Accumulation in the Liver Is Associated with Defects in Insulin Suppression of Glucose Production and Serum Free Fatty Acids Independent of Obesity in Normal Men. J. Clin. Endocrinol. Metab. 2002, 87, 3023–3028. [Google Scholar] [CrossRef]
- Ibrahim, S.H.; Kohli, R.; Gores, G.J. Mechanisms of Lipotoxicity in NAFLD and Clinical Implications. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 131–140. [Google Scholar] [CrossRef]
- Baffy, G.; Brunt, E.M.; Caldwell, S.H. Hepatocellular carcinoma in non-alcoholic fatty liver disease: An emerging menace. J. Hepatol. 2012, 56, 1384–1391. [Google Scholar] [CrossRef]
- Kutlu, O.; Kaleli, H.N.; Ozer, E. Molecular Pathogenesis of Nonalcoholic Steatohepatitis-(NASH-) Related Hepatocellular Carcinoma. Can. J. Gastroenterol. Hepatol. 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- De Minicis, S.; Agostinelli, L.; Rychlicki, C.; Sorice, G.P.; Saccomanno, S.; Candelaresi, C.; Giaccari, A.; Trozzi, L.; Pierantonelli, I.; Mingarelli, E.; et al. HCC development is associated to peripheral insulin resistance in a mouse model of NASH. PLoS ONE 2014, 9, e97136. [Google Scholar] [CrossRef] [PubMed]
- Janku, F.; Kaseb, A.O.; Tsimberidou, A.M.; Wolff, R.A.; Kurzrock, R. Identification of novel therapeutic targets in the PI3K/AKT/mTOR pathway in hepatocellular carcinoma using targeted next generation sequencing. Oncotarget 2014, 5, 3012–3022. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Liu, G. Targeting the Ras/Raf/MEK/ERK pathway in hepatocellular carcinoma. Oncol. Lett. 2017, 13, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Bellentani, S. The epidemiology of non-alcoholic fatty liver disease. Liver Int. Off. J. Int. Assoc. Study Liver 2017, 37 (Suppl. S1), 81–84. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Mantovani, A.; Lugari, S.; Targher, G. NAFLD in Some Common Endocrine Diseases: Prevalence, Pathophysiology, and Principles of Diagnosis and Management. Int. J. Mol. Sci. 2019, 20, 2841. [Google Scholar] [CrossRef]
- Guo, Z.; Li, M.; Han, B.; Qi, X. Association of non-alcoholic fatty liver disease with thyroid function: A systematic review and meta-analysis. Dig. Liver Dis. 2018, 50, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Sanguankeo, A.; Upala, S. Nonalcoholic Fatty Liver Disease Is Not Associated with Thyroid Hormone Levels and Hypothyroidism: A Systematic Review and Meta-Analysis. Eur. Thyroid. J. 2017, 6, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Lugari, S.; Mantovani, A.; Nascimbeni, F.; Lonardo, A. Hypothyroidism and nonalcoholic fatty liver disease—A chance association? Horm. Mol. Biol. Clin. Investig. 2018, 41, 347–353. [Google Scholar] [CrossRef]
- Ahmed, A.; Rabbitt, E.; Brady, T.; Brown, C.; Guest, P.; Bujalska, I.J.; Doig, C.; Newsome, P.N.; Hubscher, S.; Elias, E.; et al. A Switch in Hepatic Cortisol Metabolism across the Spectrum of Non Alcoholic Fatty Liver Disease. PLoS ONE 2012, 7, e29531. [Google Scholar]
- Tarantino, G.; Finelli, C. Pathogenesis of hepatic steatosis: The link between hypercortisolism and non-alcoholic fatty liver disease. World J. Gastroenterol. 2013, 19, 6735–6743. [Google Scholar] [CrossRef] [PubMed]
- Macut, D.; Bjekić-Macut, J.; Livadas, S.; Stanojlović, O.; Hrnčić, D.; Rašić-Marković, A.; Milutinović, D.V.; Mladenović, V.; Andrić, Z. Nonalcoholic Fatty Liver Disease in Patients with Polycystic Ovary Syndrome. Curr. Pharm. Des. 2019, 24, 4593–4597. [Google Scholar] [CrossRef] [PubMed]
- de Ridder, J.; de Wilt, J.H.W.; Simmer, F.; Overbeek, L.; Lemmens, V.; Nagtegaal, I. Incidence and origin of histologically confirmed liver metastases: An explorative case-study of 23,154 patients. Oncotarget 2016, 7, 55368–55376. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Lee, L.; Jensen, R.T. Carcinoid-syndrome: Recent advances, current status and controversies. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 22–35. [Google Scholar] [CrossRef]
- Piantanida, E.; Ippolito, S.; Gallo, D.; Masiello, E.; Premoli, P.; Cusini, C.; Rosetti, S.; Sabatino, J.; Segato, S.; Trimarchi, F.; et al. The interplay between thyroid and liver: Implications for clinical practice. J. Endocrinol. Investig. 2020, 43, 885–899. [Google Scholar] [CrossRef]
- Chan, U.; Chan, W.-T.; Ting, W.-H.; Ho, C.-S.; Liu, H.-C.; Lee, H.-C. Cholestasis caused by panhypopituitarism and acquired cytomegalovirus infection in a 2-month-old male infant: A case report. Medicine 2017, 96, e6757. [Google Scholar] [CrossRef]
- Korkmaz, L.; Akın, M.A.; Güneş, T.; Daar, G.; Baştuğ, O.; Yıkılmaz, A.; Kurtoğlu, S. Unusual Course of Congenital Hypothyroidism and Route of the L-Thyroxine Treatment in a Preterm Newborn. J. Clin. Res. Pediatric Endocrinol. 2014, 6, 177–179. [Google Scholar] [CrossRef]
- Villalba, N.L.; Zulfiqar, A.-A.; Saint-Mezard, V.; Alonso, M.B.; Kechida, M.; Zamorano, N.F.; Ortega, S.S. Myxedema coma: Four patients diagnosed at the Internal Medicine Department of the Dr. Negrin University Hospital in Spain. Pan Afr. Med. J. 2019, 34, 7. [Google Scholar] [CrossRef]
- Abebe, A.; Eck, L.M.; Holyoak, M. Severe cholestatic jaundice associated with Graves’ disease. Clin. Case Rep. 2018, 6, 2240–2245. [Google Scholar] [CrossRef]
- Subedi, A.; Kumar, V.C.S.; Sharma, A.; Hoilat, G.; John, S. Persistent lactic acidosis in the Mauriac syndrome in type 1 diabetes mellitus. Bayl. Univ. Med Cent. Proc. 2021, 34, 382–383. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Ballestri, S.; Fairweather, D.; Win, S.; Than, T.A.; Abdelmalek, M.F.; Suzuki, A. Sex Differences in Nonalcoholic Fatty Liver Disease: State of the Art and Identification of Research Gaps. Hepatology 2019, 70, 1457–1469. [Google Scholar] [CrossRef] [PubMed]
- Kur, P.; Kolasa-Wołosiuk, A.; Misiakiewicz-Has, K.; Wiszniewska, B. Sex Hormone-Dependent Physiology and Diseases of Liver. Int. J. Environ. Res. Public Health 2020, 17, 2620. [Google Scholar] [CrossRef] [PubMed]
- Agabio, R.; Pisanu, C.; Gessa, G.L.; Franconi, F. Sex Differences in Alcohol Use Disorder. Curr. Med. Chem. 2017, 24, 2661–2670. [Google Scholar] [CrossRef]
- Biswas, S.; Ghose, S. Divergent impact of gender in advancement of liver injuries, diseases, and carcinogenesis. Front. Biosci. Sch. Ed. 2018, 10, 65–100. [Google Scholar] [CrossRef][Green Version]
- Kaneko, K.; Yatsuya, H.; Li, Y.; Uemura, M.; Chiang, C.; Hirakawa, Y.; Ota, A.; Tamakoshi, K.; Aoyama, A. Association of gamma-glutamyl transferase and alanine aminotransferase with type 2 diabetes mellitus incidence in middle-aged Japanese men: 12-year follow up. J. Diabetes Investig. 2018, 10, 837–845. [Google Scholar] [CrossRef]
- Koenig, G.; Seneff, S. Gamma-Glutamyltransferase: A Predictive Biomarker of Cellular Antioxidant Inadequacy and Disease Risk. Dis. Markers 2015, 2015, 1–18. [Google Scholar] [CrossRef]
- Lee, S.M.; Park, J.S.; Han, Y.J.; Kim, W.; Bang, S.H.; Kim, B.J.; Park, C.-W.; Kim, M.Y. Elevated Alanine Aminotransferase in Early Pregnancy and Subsequent Development of Gestational Diabetes and Preeclampsia. J. Korean Med Sci. 2020, 35, e198. [Google Scholar] [CrossRef]
- Zhao, W.; Zhang, L.; Zhang, G.; Varkaneh, H.K.; Rahmani, J.; Clark, C.; Ryan, P.M.; Abdulazeem, H.; Salehisahlabadi, A. The association of plasma levels of liver enzymes and risk of gestational diabetes mellitus: A systematic review and dose–response meta-analysis of observational studies. Acta Diabetol. 2019, 57, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, G.; Avagnina, S.; Barantani, E.G.; Ciccarone, A.M.; Corica, F.; Dall’Aglio, E.; Grave, R.D.; Morpurgo, P.S.; Tomasi, F.; Vitacolonna, E. Aminotransferase and gamma-glutamyltranspeptidase levels in obesity are associated with insulin resistance and the metabolic syndrome. J. Endocrinol. Investig. 2005, 28, 333–339. [Google Scholar] [CrossRef]
- Crownover, B.K.; Covey, C.J. Hereditary hemochromatosis. Am. Fam. Physician 2013, 87, 183–190. [Google Scholar]
- Mulligan, C.; Bronstein, J.M. Wilson Disease: An Overview and Approach to Management. Neurol. Clin. 2020, 38, 417–432. [Google Scholar] [CrossRef]
- Kahaly, G.J.; Frommer, L. Polyglandular autoimmune syndromes. J. Endocrinol. Investig. 2018, 41, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.A.; Jones, T.L.; Ianna, E.A.; Foy, A.; Reeves, G.E.M. Thyroid disease in chronic hepatitis C infection treated with combination interferon-α and ribavirin: Management strategies and future perspective. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2013, 19, 292–300. [Google Scholar] [CrossRef]
- Ellingwood, S.S.; Cheng, A. Biochemical and clinical aspects of glycogen storage diseases. J. Endocrinol. 2018, 238, R131–R141. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.S.; Chang, Y.; Ryu, S.; Cainzos-Achirica, M.; Kwon, M.-J.; Zhang, Y.; Choi, Y.; Ahn, J.; Rampal, S.; Zhao, D.; et al. Hepatitis B and C virus infection and diabetes mellitus: A cohort study. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef]
- Qu, Q.; Wang, S.; Chen, S.; Zhou, L.; Rui, J.-A. Prognostic role and significance of paraneoplastic syndromes in hepatocellular carcinoma. Am. Surg. 2014, 80, 191–196. [Google Scholar] [CrossRef]
- Niedfeldt, M.W. Anabolic Steroid Effect on the Liver. Curr. Sports Med. Rep. 2018, 17, 97–102. [Google Scholar] [CrossRef]
- Ponnatapura, J.; Kielar, A.; Burke, L.M.; Lockhart, M.E.; Abualruz, A.-R.; Tappouni, R.; Lalwani, N. Hepatic complications of oral contraceptive pills and estrogen on MRI: Controversies and update-Adenoma and beyond. Magn. Reson. Imaging 2019, 60, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Akmal, A.; Kung, J. Propylthiouracil, and methimazole, and carbimazole-related hepatotoxicity. Expert Opin. Drug Saf. 2014, 13, 1397–1406. [Google Scholar] [CrossRef]
- Zoubek, M.E.; Pinazo-Bandera, J.; Ortega-Alonso, A.; Hernández, N.; Crespo, J.; Contreras, F.; Medina-Cáliz, I.; Sanabria-Cabrera, J.; Sanjuan-Jiménez, R.; González-Jiménez, A.; et al. Liver injury after methylprednisolone pulses: A disputable cause of hepatotoxicity. A case series and literature review. United Eur. Gastroenterol. J. 2019, 7, 825–837. [Google Scholar] [CrossRef]
- Filippatos, T.D.; Derdemezis, C.S.; Gazi, I.F.; Nakou, E.S.; Mikhailidis, D.P.; Elisaf, M.S. Orlistat-associated adverse effects and drug interactions: A critical review. Drug Saf. 2008, 31, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Sumida, Y.; Yoneda, M. Current and future pharmacological therapies for NAFLD/NASH. J. Gastroenterol. 2018, 53, 362–376. [Google Scholar] [CrossRef] [PubMed]
- Terziroli Beretta-Piccoli, B.; Mieli-Vergani, G.; Vergani, D. Autoimmune hepatitis: Standard treatment and systematic review of alternative treatments. World J. Gastroenterol. 2017, 23, 6030–6048. [Google Scholar] [CrossRef] [PubMed]
- Bunchorntavakul, C.; Reddy, K.R. Pharmacologic Management of Portal Hypertension. Clin. Liver Dis. 2019, 23, 713–736. [Google Scholar] [CrossRef] [PubMed]
- Witchel, S.F.; Oberfield, S.E.; Peña, A.S. Polycystic Ovary Syndrome: Pathophysiology, Presentation, and Treatment with Emphasis on Adolescent Girls. J. Endocr. Soc. 2019, 3, 1545–1573. [Google Scholar] [CrossRef]
- Lainscak, M.; Pelliccia, F.; Rosano, G.; Vitale, C.; Schiariti, M.S.M.; Greco, C.; Speziale, G.; Gaudio, C. Safety profile of mineralocorticoid receptor antagonists: Spironolactone and eplerenone. Int. J. Cardiol. 2015, 200, 25–29. [Google Scholar] [CrossRef]
- Jadali, Z. Autoimmune thyroid disorders in hepatitis C virus infection: Effect of interferon therapy. Indian J. Endocrinol. Metab. 2013, 17, 69–75. [Google Scholar] [CrossRef]
- Sharp, R.P.; Gales, B.J. Nebivolol versus other beta blockers in patients with hypertension and erectile dysfunction. Ther. Adv. Urol. 2017, 9, 59–63. [Google Scholar] [CrossRef]
- Chang, H.-T.; Pan, H.-J.; Lee, C.-H. Prevention of Tamoxifen-related Nonalcoholic Fatty Liver Disease in Breast Cancer Patients. Clin. Breast Cancer 2018, 18, e677–e685. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Beland, F.; Chen, S.; Liu, F.; Guo, L.; Fang, J.-L. Mechanisms of tolvaptan-induced toxicity in HepG2 cells. Biochem. Pharmacol. 2015, 95, 324–336. [Google Scholar] [CrossRef] [PubMed]
- Di Ciaula, A.; Wang, D.Q.-H.; Portincasa, P. Cholesterol cholelithiasis: Part of a systemic metabolic disease, prone to primary prevention. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 157–171. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Action | Hormones | Reference |
|---|---|---|
| Hormone synthesis | IGF-1 | Bach [2] |
| Angiotensinogen | Matsuaska [4] | |
| Thrombopoietin | Hitchcock [6] | |
| Hepcidin | Ruchala [5] | |
| Betatrophin | Raghow [3] | |
| Proprotein convertase subtilsin-kexin type 9 | Yadav [7] | |
| Hormone action modulation | IGF binding protein 1 to 6 | Allard [8] |
| Sex hormone-binding globulin | Selby [9] | |
| Thyroid hormone-binding globulin | Schussler [10] | |
| Transthyretin | Palha [11] | |
| Corticosteroid binding globulin | Breuner [12] | |
| Vitamin D binding protein | Bouillon [13] |
| Hepatic Manifestation | Endocrine Disorders | References |
|---|---|---|
| Non-alcoholic fatty liver disease | Insulin resistance, diabetes, obesity, and dyslipidemia | Watt [86] |
| Hepatic steatosis or steato-hepatitis | Cushing’s syndrome, acromegaly, Graves’ disease and other causes of thyrotoxicosis, polycystic ovary syndrome, male hypogonadism, and pheochromocytoma | Lonardo [97] |
| Hepatic metastasis | Adrenal cancer, pancreatic cancer, ovarian and testicular neoplasm, and malignant pheochromocytoma | Ridder [104] |
| Neonatal cholestasis | Congenital combined pituitary hormone deficiency, congenital hypothyroidism, and HNF1B-MODY (previously MODY-5) | Chan [107], Korkmaz [108] |
| Acute hepatic congestion (with jaundice) | Myxedema coma | Villalba [109] |
| Cholestasis | Thyrotoxicosis | Abebe [110] |
| Congestive hepatomegaly | Thyrotoxic heart failure | Piantanida [106] |
| Mauriac syndrome | Poorly controlled diabetes mellitus | Subedi [111] |
| Abnormality in Liver Function | Significance | References |
|---|---|---|
| Raised GGT | Probable role in the prediction of future risk of diabetes | Kaneko [116] |
| Elevated ALT | Probable role in the prediction of future risk of diabetes | Kaneko [116] |
| Elevated ALT and GGT in early pregnancy | Correlates with development of gestational diabetes mellitus | Lee [118], Zhao [119] |
| Elevated liver enzymes | Possible marker of insulin resistance and metabolic syndrome | Marchesini [120] |
| Disease | Hepatic Manifestation | Endocrine Dysfunctions |
| Metabolic disorders | ||
| Hemochromatosis [121] | Hepatic fibrosis, cirrhosis, and hepatocellular carcinoma | Diabetes, hypopituitarism, secondary hypogonadism, and secondary hypothyroidism |
| Wilson’s disease [122] | Transaminitis, steatosis, acute hepatitis and acute liver failure (with an associated Coombs-negative hemolytic anemia), chronic hepatitis, and cirrhosis | Fanconi syndrome, distal renal tubular acidosis, nephrolithiasis, gigantism, hypoparathyroidism, pancreatitis, impotence, infertility, and repeated spontaneous abortions |
| Glycogen storage disorders: Glycogen storage disease I (von Gierke disease)—90% of cases [125] | Glucose-6-phosphatase deficiency in liver and muscle, hepatomegaly, and hepatic adenomas | Hypoglycemia, lactic acidosis, hypertriglyceridemia, and hyperuricemia; short stature, and delayed puberty |
| Autoimmune disorders | ||
| Polyglandular autoimmune syndrome 1 [123] | Autoimmune hepatitis | Hypoparathyroidism and autoimmune adrenal insufficiency (along with chronic mucocutaneous candidiasis) |
| Polyglandular autoimmune syndrome 2 [123] | Primary biliary cirrhosis | Addison’s disease plus either an autoimmune thyroid disease or type 1 diabetes mellitus associated with hypogonadism, and other endocrinopathies |
| Infections | ||
| Hepatitis C infection [124] | Chronic hepatitis C, cirrhosis, and hepatocellular carcinoma | Thyroid autoimmunity, hypothyroidism, and higher prevalence of thyroid cancer |
| Hepatitis B infection [126] | Chronic hepatitis B, cirrhosis, and hepatocellular carcinoma | Increased risk of diabetes mellitus |
| Malignancy | ||
| Paraneoplastic endocrine syndromes [127] | Hepatocellular carcinoma | Hypoglycemia, hypercholesterolemia, and hypercalcemia |
| Hepatic Effects of Endocrine Drugs | |
| Drugs | Adverse Effects |
| Anabolic androgenic steroid [128] | Hepatic adenoma, hepatocellular carcinoma, cholestasis, and peliosis hepatis. |
| Estrogen/oral contraceptive pills [129] | Intrahepatic canalicular cholestasis, hepatic adenomas, focal nodular hyperplasia, hemangioma or hamartoma, peliosis hepatis, and Budd Chiari syndrome |
| Tamoxifen [140] | NAFLD |
| Propylthiouracil, methimazole, carbimazole [130] | Hepatitis, cholestasis, and acute liver failure |
| Corticosteroids [131] | Hepatic enlargement, steatosis, glycogenosis. NAFLD, exacerbate chronic viral hepatitis, and high doses of intravenous methylprednisolone—acute liver failure (sometimes fatal) |
| Vasopressin receptor antagonist [141] | Transaminitis and acute liver failure |
| Orlistat [132] | Cholelithiasis, cholestatic hepatitis, and acute and subacute liver failure |
| Drugs | Beneficial effects |
| Pioglitazone [133] | Beneficial effect on NAFLD |
| GLP-1RA [133] | Possible beneficial effect on NAFLD |
| SGLT-2 inhibitors [133] | Possible beneficial effect on NAFLD |
| Saroglitazar [133] | Possible beneficial effect on NAFLD |
| Corticosteroids [134] | Treatment of autoimmune hepatitis and prevention of rejection of liver transplant |
| Somatostatin analogs (octreotide and others) [135] | Treatment of variceal bleeding (decreases portal blood flow) |
| Vasopressin analogs (terlipressin) [135] | Treatment of variceal bleeding (decreases portal blood flow) |
| Endocrine Effects of Drugs Used in Hepatology | |
| Drugs | Adverse effects |
| Spironolactone [137] | Gynaecomastia, and hypogonadism in men |
| Beta-blockers [139] | Erectile dysfunction |
| Interferon-alpha [138] | Hypothyroidism, autoimmune (Hashimoto’s) thyroiditis, destructive thyroiditis, and Graves’ disease |
| Drugs | Beneficial effects |
| Ursodeoxycholic acid [142] | Possible beneficial effect in metabolic syndrome |
| Spironolactone [136] | Treatment of PCOS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalra, S.; Bhattacharya, S.; Rawal, P. Hepatocrinology. Med. Sci. 2021, 9, 39. https://doi.org/10.3390/medsci9020039
Kalra S, Bhattacharya S, Rawal P. Hepatocrinology. Medical Sciences. 2021; 9(2):39. https://doi.org/10.3390/medsci9020039
Chicago/Turabian StyleKalra, Sanjay, Saptarshi Bhattacharya, and Pawan Rawal. 2021. "Hepatocrinology" Medical Sciences 9, no. 2: 39. https://doi.org/10.3390/medsci9020039
APA StyleKalra, S., Bhattacharya, S., & Rawal, P. (2021). Hepatocrinology. Medical Sciences, 9(2), 39. https://doi.org/10.3390/medsci9020039