
Wearable Sensor for Assessing Gait and Postural Alterations in Patients with Diabetes: A Scoping Review

 ,
, 



Abstract
:1. Introduction
2. Methods
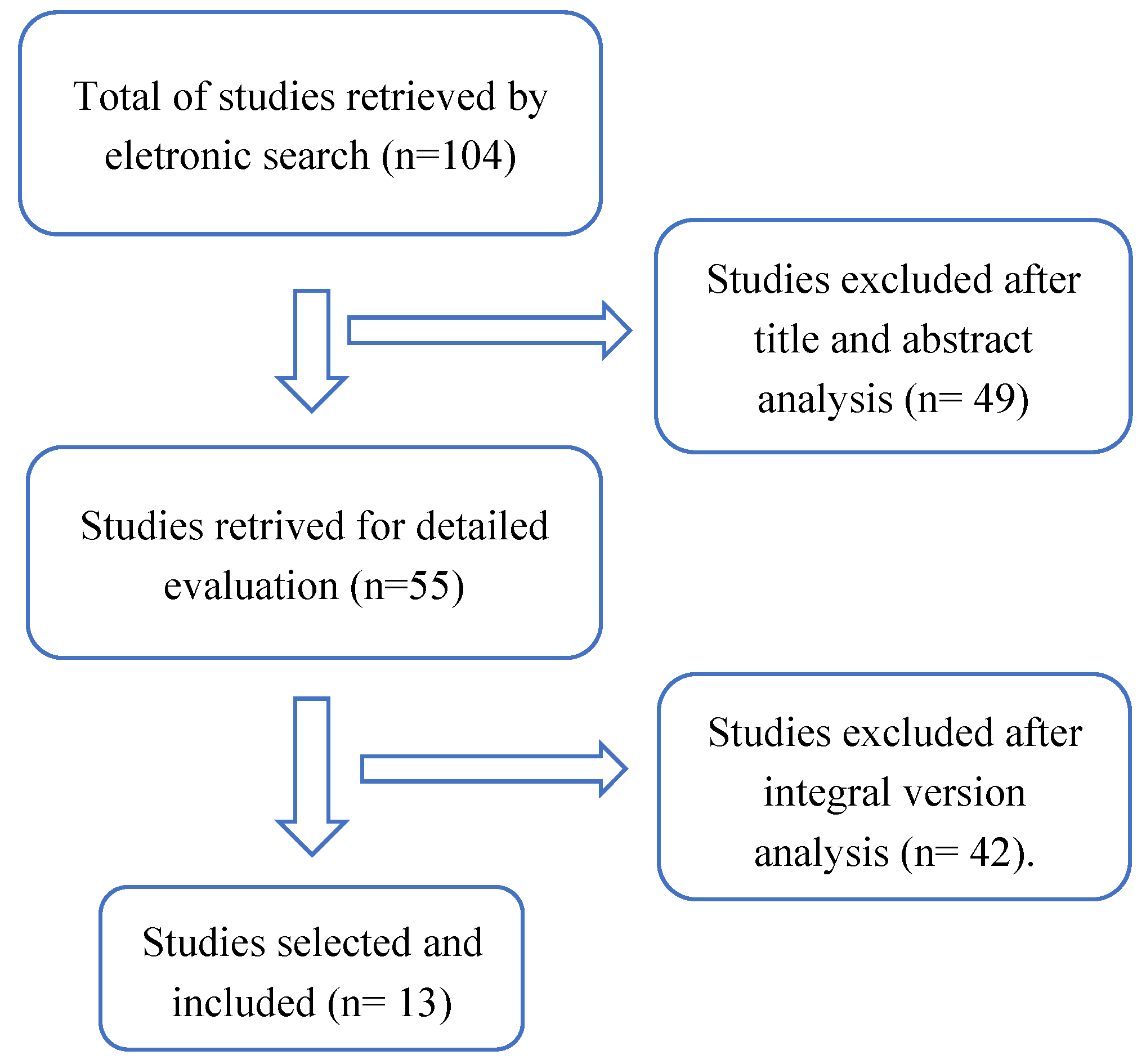
Review Process: Search Strategy and Selection Criteria
3. Results
3.1. Characteristics of Patients
3.2. Sensor Number and Placement
3.3. Spatiotemporal Parameters
3.4. Differences in Gait Analysis and Spatiotemporal Parameters between Patients with Diabetes (with or without DPN) and Healthy Individuals
3.5. Protocol and Analysis of Posture Parameters
3.6. Comparisons of Gait and Postural Alterations in Diabetic Patients Using Wearable Sensors and Other Methods which Assess Motor and Sensitive Alterations
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dingwell, J.B.; Cavanagh, P.R. Increased Variability of Continuous Overground Walking in Neuropathic Patients is only Indirectly Related to Sensory Loss. Gait Posture 2001, 14, 1–10. [Google Scholar] [CrossRef]
- Richardson, J.K. Factors Associated with Falls in Older Patients with Diffuse Polyneuropathy. J. Am. Geriatr. Soc. 2002, 50, 1767–1773. [Google Scholar] [CrossRef] [Green Version]
- Sacco, I.; Amadio, A. A Study of Biomechanical Parameters in Gait Analysis and Sensitive Cronaxie of Diabetic Neuropathic Patients. Clin. Biomech. 2000, 15, 196–202. [Google Scholar] [CrossRef]
- Mueller, M.J.; Salsich, G.; Bastian, A.J. Differences in the Gait Characteristics of People with Diabetes and Transmetatarsal Amputation Compared with Age-Matched Controls. Gait Posture 1998, 7, 200–206. [Google Scholar] [CrossRef]
- Menz, H.; Lord, S.R.; George, R.S.; Fitzpatrick, R.C. Walking Stability and Sensorimotor Function in Older People with Diabetic Peripheral Neuropathy. Arch. Phys. Med. Rehabil. 2004, 85, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Allet, L.; Armand, S.; Golay, A.; Monnin, D.; De Bie, R.A.; de Bruin, E.D. Gait Characteristics of Diabetic Patients: A Systematic Review. Diabetes/Metabolism Res. Rev. 2008, 24, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.-Y.; Minor, S.D.; Maluf, K.S.; Mueller, M.J. Comparison of Muscle Activity during Walking in Subjects with and without Diabetic Neuropathy. Gait Posture 2003, 18, 105–113. [Google Scholar] [CrossRef]
- Yavuzer, G.; Yetkin, I.; Toruner, F.B.; Koca, N.; Bolukbasi, N. Gait Deviations of Patients with Diabetes Mellitus: Looking beyond Peripheral Neuropathy. Eur. Med. 2006, 42, 127–133. [Google Scholar]
- Sacco, I.C.; Hamamoto, A.N.; Tonicelli, L.M.; Watari, R.; Ortega, N.R.; Sartor, C. Abnormalities of Plantar Pressure Distribution in Early, Intermediate, and Late Stages of Diabetic Neuropathy. Gait Posture 2014, 40, 570–574. [Google Scholar] [CrossRef]
- Abate, M.; Schiavone, C.; Salini, V.; Andia, I. Management of Limited Joint Mobility in Diabetic Patients. Diabetes Metab. Syndr. Obesity Targets Ther. 2013, 6, 197–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couppé, C.; Svensson, R.B.; Kongsgaard, M.; Kovanen, V.; Grosset, J.-F.; Snorgaard, O.; Bencke, J.; Larsen, J.O.; Bandholm, T.; Christensen, T.M.; et al. Human Achilles Tendon Glycation and Function in Diabetes. J. Appl. Physiol. 2016, 120, 130–137. [Google Scholar] [CrossRef]
- Karamanidis, K.; Arampatzis, A.; Mademli, L. Age-Related Deficit in Dynamic Stability Control after Forward Falls is Affected by Muscle Strength and Tendon Stiffness. J. Electromyogr. Kinesiol. 2008, 18, 980–989. [Google Scholar] [CrossRef]
- Alam, U.; Riley, D.R.; Jugdey, R.S.; Azmi, S.; Rajbhandari, S.; D’Août, K.; Malik, R.A. Diabetic Neuropathy and Gait: A Review. Diabetes Ther. 2017, 8, 1253–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simoneau, G.G.; Ulbrecht, J.S.; Derr, J.A.; Becker, M.B.; Cavanagh, P.R. Postural Instability in Patients with Diabetic Sensory Neuropathy. Diabetes Care 1994, 17, 1411–1421. [Google Scholar] [CrossRef]
- Vaz, M.M.; Costa, G.C.; Reis, J.G.; Junior, W.M.; de Paula, F.; de Abreu, D.C. Postural Control and Functional Strength in Patients with Type 2 Diabetes Mellitus with and without Peripheral Neuropathy. Arch. Phys. Med. Rehabil. 2013, 94, 2465–2470. [Google Scholar] [CrossRef]
- Bonnet, C.; Carello, C.; Turvey, M.T. Diabetes and Postural Stability: Review and Hypotheses. J. Mot. Behav. 2009, 41, 172–190. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, C.T.; Ray, C. Peripheral Neuropathy may not be the only Fundamental Reason Explaining Increased Sway in Diabetic Individuals. Clin. Biomech. 2011, 26, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.R. Quantification of Human Motion: Gait Analysis—Benefits and Limitations to its Application to Clinical Problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait Analysis Using Wearable Sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef]
- Prasanth, H.; Caban, M.; Keller, U.; Courtine, G.; Ijspeert, A.; Vallery, H.; von Zitzewitz, J. Wearable Sensor-Based Real-Time Gait Detection: A Systematic Review. Sensors 2021, 21, 2727. [Google Scholar] [CrossRef]
- Hsu, W.-C.; Sugiarto, T.; Lin, Y.-J.; Yang, F.-C.; Lin, Z.-Y.; Sun, C.-T.; Hsu, C.-L.; Chou, K.-N. Multiple-Wearable-Sensor-Based Gait Classification and Analysis in Patients with Neurological Disorders. Sensors 2018, 18, 3397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storm, F.A.; Cesareo, A.; Reni, G.; Biffi, E. Wearable Inertial Sensors to Assess Gait during the 6-Minute Walk Test: A Systematic Review. Sensors 2020, 20, 2660. [Google Scholar] [CrossRef]
- Kang, G.E.; Zhou, H.; Varghese, V.; Najafi, B. Characteristics of the gait Initiation Phase in Older Adults with Diabetic Peripheral Neuropathy Compared to Control Older Adults. Clin. Biomech. 2020, 72, 155–160. [Google Scholar] [CrossRef]
- Kang, G.E.; Yang, J.; Najafi, B. Does the Presence of Cognitive Impairment Exacerbate the Risk of Falls in People with Peripheral Neuropathy? An Application of Body-Worn Inertial Sensors to Measure Gait Variability. Sensors 2020, 20, 1328. [Google Scholar] [CrossRef] [Green Version]
- Caron, N.; Peyrot, N.; Caderby, T.; Verkindt, C.; Dalleau, G. Effect of Type 2 Diabetes on Energy Cost and Preferred Speed of Walking. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 118, 2331–2338. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Al-Ali, F.; Rahemi, H.; Kulkarni, N.; Hamad, A.; Ibrahim, R.; Talal, T.K.; Najafi, B. Hemodialysis Impact on Motor Function beyond Aging and Diabetes-Objectively Assessing Gait and Balance by Wearable Technology. Sensors 2018, 18, 3939. [Google Scholar] [CrossRef] [Green Version]
- Esser, P.; Collett, J.; Maynard, K.; Steins, D.; Hillier, A.; Buckingham, J.; Tan, G.D.; King, L.; Dawes, H. Single Sensor Gait Analysis to Detect Diabetic Peripheral Neuropathy: A Proof of Principle Study. Diabetes Metab. J. 2018, 42, 82–86. [Google Scholar] [CrossRef]
- Ling, E.; Lepow, B.; Zhou, H.; Enriquez, A.; Mullen, A.; Najafi, B. The Impact of Diabetic Foot Ulcers and Unilateral Offloading Footwear on Gait in People with Diabetes. Clin. Biomech. 2019, 73, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Talal, T.K.; Grewal, G.S.; Menzies, R.; Armstrong, D.G.; Lavery, L.A. Using Plantar Electrical Stimulation to Improve Postural Balance and Plantar Sensation Among Patients with Diabetic Peripheral Neuropathy: A Randomized Double Blinded Study. J. Diabetes Sci. Technol. 2017, 11, 693–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bruin, E.D.; Hubli, M.; Hofer, P.; Wolf, P.; Murer, K.; Zijlstra, W. Validity and Reliability of Accelerometer-Based Gait Assessment in Patients with Diabetes on Challenging Surfaces. J. Aging Res. 2012, 2012, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Khan, T.; Fleischer, A.; Wrobel, J. The Impact of Footwear and Walking Distance on Gait Stability in Diabetic Patients with Peripheral Neuropathy. J. Am. Podiatr. Med Assoc. 2013, 103, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Horn, D.; Marclay, S.; Crews, R.; Wu, S.; Wrobel, J.S. Assessing Postural Control and Postural Control Strategy in Diabetes Patients Using Innovative and Wearable Technology. J. Diabetes Sci. Technol. 2010, 4, 780–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toosizadeh, N.; Mohler, J.; Armstrong, D.G.; Talal, T.K.; Najafi, B. The Influence of Diabetic Peripheral Neuropathy on Local Postural Muscle and Central Sensory Feedback Balance Control. PLoS ONE 2015, 10, e0135255. [Google Scholar] [CrossRef] [Green Version]
- D’Silva, L.J.; Kluding, P.M.; Whitney, S.L.; Dai, H.; Santos, M. Postural Sway in Individuals with Type 2 Diabetes and Concurrent Benign Paroxysmal Positional Vertigo. Int. J. Neurosci. 2017, 127, 1065–1073. [Google Scholar] [CrossRef]
- Aminian, K.; Najafi, B. Capturing Human Motion Using Body-Fixed Sensors: Outdoor Measurement and Clinical Applications. Comput. Animat. Virtual Worlds 2004, 15, 79–94. [Google Scholar] [CrossRef]
- Ms, A.A.G.; Ms, A.N.O.; Pt, M.E.O.; Pripas, D.; Mezzarane, R.A.; Sacco, I.C.N. Electromyography and Kinematic Changes of Gait Cycle at Different Cadences in Diabetic Neuropathic Individuals. Muscle Nerve 2011, 44, 258–268. [Google Scholar] [CrossRef]
- Savelberg, H.H.; Ilgin, D.; Angin, S.; Willems, P.J.; Schaper, N.C.; Meijer, K. Prolonged Activity of Knee Extensors and Dorsal Flexors is Associated with Adaptations in Gait in Diabetes and Diabetic Polyneuropathy. Clin. Biomech. 2010, 25, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Sawacha, Z.; Gabriella, G.; Cristoferi, G.; Guiotto, A.; Avogaro, A.; Cobelli, C. Diabetic Gait and Posture Abnormalities: A Biomechanical Investigation through Three Dimensional Gait Analysis. Clin. Biomech. 2009, 24, 722–728. [Google Scholar] [CrossRef]
- Fernando, M.; Crowther, R.; Lazzarini, P.; Sangla, K.; Cunningham, M.; Buttner, P.; Golledge, J. Biomechanical Characteristics of Peripheral Diabetic Neuropathy: A Systematic Review and Meta-Analysis of Findings from the Gait Cycle, Muscle Activity and Dynamic Barefoot Plantar Pressure. Clin. Biomech. 2013, 28, 831–845. [Google Scholar] [CrossRef]
- Mustapa, A.; Justine, M.; Mustafah, N.M.; Jamil, N.; Manaf, H. Postural Control and Gait Performance in the Diabetic Peripheral Neuropathy: A Systematic Review. BioMed Res. Int. 2016, 2016, 9305025. [Google Scholar] [CrossRef] [Green Version]
- Minetti, A.E.; Capelli, C.; Zamparo, P.; DI Prampero, P.E.; Saibene, F. Effects of Stride Frequency on Mechanical Power and Energy Expenditure of Walking. Med. Sci. Sports Exerc. 1995, 27, 1194–1202. [Google Scholar] [CrossRef]
- Reeves, N.; Orlando, G.; Brown, S. Sensory-Motor Mechanisms Increasing Falls Risk in Diabetic Peripheral Neuropathy. Medicina 2021, 57, 457. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Bai, J.-J. Balance Training in the Intervention of Fall Risk in Elderly with Diabetic Peripheral Neuropathy: A Review. Int. J. Nurs. Sci. 2014, 1, 441–445. [Google Scholar] [CrossRef] [Green Version]
- Lima, R.A.D.O.; Piemonte, G.A.; Nogueira, C.R.; Nunes-Nogueira, V.D.S. Efficacy of Exercise on Balance, Fear of Falling, and Risk of Falls in Patients with Diabetic Peripheral Neuropathy: A Systematic Review and Meta-Analysis. Arch. Endocrinol. Metab. 2021. [Google Scholar] [CrossRef] [PubMed]
- Beeve, A.; Brazill, J.M.; Scheller, E.L. Peripheral Neuropathy as a Component of Skeletal Disease in Diabetes. Curr. Osteoporos. Rep. 2019, 17, 256–269. [Google Scholar] [CrossRef] [Green Version]
- Hewston, P.; Deshpande, N. Falls and Balance Impairments in Older Adults with Type 2 Diabetes: Thinking Beyond Diabetic Peripheral Neuropathy. Can. J. Diabetes 2016, 40, 6–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, S.R.; Ward, J.A.; Williams, P.; Anstey, K. Physiological Factors Associated with Falls in Older Community-Dwelling Women. J. Am. Geriatr. Soc. 1994, 42, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Fernando, M.E.; Crowther, R.G.; Lazzarini, P.A.; Sangla, K.S.; Buttner, P.; Golledge, J. Gait Parameters of People with Diabetes-Related Neuropathic Plantar Foot Ulcers. Clin. Biomech. 2016, 37, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Halim, A.; Abdellatif, A.; Awad, I.M.; Atia, A.M.R. Prediction of Human Gait Activities Using Wearable Sensors. Proc. Inst. Mech. Eng. Part H: J. Eng. Med. 2021, 235, 676–687. [Google Scholar] [CrossRef]
- Nouredanesh, M.; Godfrey, A.; Howcroft, J.; Lemaire, E.D.; Tung, J. Fall Risk Assessment in the Wild: A Critical Examination of Wearable Sensor Use in Free-Living Conditions. Gait Posture 2021, 85, 178–190. [Google Scholar] [CrossRef]
- Brognara, L.; Navarro-Flores, E.; Iachemet, L.; Serra-Catalá, N.; Cauli, O. Beneficial Effect of Foot Plantar Stimulation in Gait Parameters in Individuals with Parkinson’s Disease. Brain Sci. 2020, 10, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brognara, L.; Cauli, O. Mechanical Plantar Foot Stimulation in Parkinson’s Disease: A Scoping Review. Diseases 2020, 8, 12. [Google Scholar] [CrossRef]
- Pardoel, S.; Shalin, G.; Nantel, J.; Lemaire, E.; Kofman, J. Early Detection of Freezing of Gait during Walking Using Inertial Measurement Unit and Plantar Pressure Distribution Data. Sensors 2021, 21, 2246. [Google Scholar] [CrossRef] [PubMed]
- Boekesteijn, R.J.; Smolders, J.M.H.; Busch, V.J.J.F.; Geurts, A.C.H.; Smulders, K. Independent and Sensitive Gait Parameters for Objective Evaluation in Knee and Hip Osteoarthritis Using Wearable Sensors. BMC Musculoskelet. Disord. 2021, 22, 242. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, H.; Yao, Y.; Liu, J.; Sun, X.; Gu, D. Walking Stability in Patients with Benign Paroxysmal Positional Vertigo: An objective assessment using wearable accelerometers and machine learning. J. Neuroeng. Rehabil. 2021, 18, 1–9. [Google Scholar] [CrossRef]
- Kim, J.-K.; Bae, M.-N.; Lee, K.; Hong, S. Identification of Patients with Sarcopenia Using Gait Parameters Based on Inertial Sensors. Sensors 2021, 21, 1786. [Google Scholar] [CrossRef] [PubMed]
- DiLiberto, F.E.; Baumhauer, J.F.; Nawoczenski, D.A. The Prevention of Diabetic Foot Ulceration: How Biomechanical Research Informs Clinical Practice. Braz. J. Phys. Ther. 2016, 20, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Flores, E. Quality of Life in Individuals with Diabetic Foot Syndrome. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 1365–1372. [Google Scholar] [CrossRef]
- MejiaCruz, Y.; Franco, J.; Hainline, G.; Fritz, S.; Jiang, Z.; Caicedo, J.M.; Davis, B.; Hirth, V. Walking Speed Measurement Technology: A Review. Curr. Geriatr. Rep. 2021, 10, 32–41. [Google Scholar] [CrossRef]
- Grewal, G.S.; Sayeed, R.; Schwenk, M.; Bharara, M.; Menzies, R.; Talal, T.K.; Armstrong, D.G.; Najafi, B. Balance Rehabilitation. J. Am. Podiatr. Med Assoc. 2013, 103, 498–507. [Google Scholar] [CrossRef]
- Grewal, G.S.; Schwenk, M.; Lee-Eng, J.; Parvaneh, S.; Bharara, M.; Menzies, R.A.; Talal, T.K.; Armstrong, D.G.; Najafi, B. Sensor-Based Interactive Balance Training with Visual Joint Movement Feedback for Improving Postural Stability in Diabetics with Peripheral Neuropathy: A Randomized Controlled Trial. Gerontology 2015, 61, 567–574. [Google Scholar] [CrossRef]
- Richardson, J.K.; Thies, S.; DeMott, T.K.; Ashton-Miller, J.A. Gait Analysis in a Challenging Environment Differentiates between Fallers and Nonfallers among Older Patients with Peripheral Neuropathy. Arch. Phys. Med. Rehabil. 2005, 86, 1539–1544. [Google Scholar] [CrossRef] [PubMed]
- Thies, S.B.; Richardson, J.K.; DeMott, T.; Ashton-Miller, J.A. Influence of an Irregular Surface and Low Light on the Step Variability of Patients with Peripheral Neuropathy During Level Gait. Gait Posture 2005, 22, 40–45. [Google Scholar] [CrossRef]
- Allet, L.; Armand, S.; de Bie, R.A.; Pataky, Z.; Aminian, K.; Herrmann, F.; de Bruin, E.D. Gait Alterations of Diabetic Patients While Walking on Different Surfaces. Gait Posture 2009, 29, 488–493. [Google Scholar] [CrossRef]
- Callaghan, B.C.; Little, A.A.; Feldman, E.; Hughes, R.A.C. Enhanced Glucose Control for Preventing and Treating Diabetic Neuropathy. Cochrane Database Syst. Rev. 2012, 6, CD007543. [Google Scholar] [CrossRef] [PubMed]
- Casadei, G.; Filippini, M.; Brognara, L. Glycated Hemoglobin (HbA1c) as a Biomarker for Diabetic Foot Peripheral Neuropathy. Diseases 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Boucher, P.; Teasdale, N.; Courtemanche, R.; Bard, C.; Fleury, M. Postural Stability in Diabetic Polyneuropathy. Diabetes Care 1995, 18, 638–645. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients, IMU Location and Spatiotemporal Parameters Analysed | Kang et al. (2020) [23] | Kang et al. (2020) [24] | Caron et al. (2018) [25] | Zhou et al. (2018) [26] | Esser et al. (2018) [27] | Ling et al. (2020) [28] | Najafi et al. (2017) [29] | De Bruin et al. (2012) [30] | Najafi et al. (2013) [31] |
|---|---|---|---|---|---|---|---|---|---|
| Number of diabetes subjects | 38 | 44 | 20 | 151 | 17 | 39 | 28 | 31 | 12 |
| Mean age | 72.6 | 66.5 | 57.5 | 78.0 | 63.0 | 64.3 | 56.0 | Not specified (participants had between 50–70 years old) | 60.0 |
| Diabetes history, years | Not reported | Not reported | 10.6 | Not reported | 24 ± 16 | Not reported | Not reported | Not reported | 10 ± 13 |
| Assessment of DPN | X | X | X | X | X | X | |||
| 2 IMUs on both ankles or on both tibias (shanks) | X | X | X | X | X | X | |||
| IMUs on both feet | |||||||||
| IMU on lower back | X | X | X | X | X | X | X | ||
| Other anatomical locations (#IMUs) | 2 on thighs | 2 on thighs | 2 on thighs | 2 on thighs | |||||
| Number of IMUs used for the measurements | 5 | 2 | 1 | 2 | 1 | 5 | 5 | 1 | 5 |
| Gait speed (stride velocity) | X | X | X | X | X | X | X | X | X |
| Cadence (or step frequency) | X | X | X | X | X | ||||
| Stride length | X | X | x | X | X | X | |||
| Stride length variability | X | X | |||||||
| Stride time (Gait cycle time) | X | X | |||||||
| Steady-state gait | X | X | X | ||||||
| Step length | X | ||||||||
| Step time | X | X | |||||||
| Step time variability | X | ||||||||
| Double support (time or %) | X | X | |||||||
| Domicile | X | ||||||||
| Distance covered | 12 m | 12 m | 200 m | 15 m | 10 m | 10 m | 31 m | 20 m | |
| Outdoor | X | X | |||||||
| Clinical environment | X | X | X | X | X |
| Patients, IMU Location and Postural Parameters Analysed | Najafi et al. (2010) [32] | Toosizadeh et al. (2015) [33] | D’Silva et al. (2017) [34] | Najafi et al. (2017) [29] |
|---|---|---|---|---|
| # DM subjects | 17 | 18 | 52 | 28 |
| Mean age | 59.2 | 65.0 | Not specified (participants had between 40–65 years old) | 56.0 |
| Diabetes history, years | Not reported | 19 ± 11 | Not reported | not reported |
| DPN | X | X | X | |
| 2 IMUs on both ankles or on both tibias (shanks) | X (shin) | X (shin) | X | |
| IMUs on both feet | ||||
| IMU on lower back | X | X | X | X |
| Other locations (#IMUs) | 2 on thighs | |||
| # IMUs | 2 | 2 | 1 | 5 |
| firm/foam surfaces | X | X | ||
| Eyes closed | X | X | X | X |
| Eyes open | X | X | X | X |
| 30 seconds with feet close together | X | X | X | |
| 15 seconds with feet close together | X | |||
| Hip sway (deg2) | X | X | X | |
| Ankle sway (deg2) | X | X | X | |
| Total sway area (cm2) | X | X | X | X |
| Medial–lateral sway (cm) | X | X | X | X |
| Anterior–posterior sway (cm) | X | X | X | X |
| Range (cm/s2) of acceleration, in AP and ML directions | X | |||
| peak velocity (cm/s) in AP and ML | X | |||
| Domicile | ||||
| Clinical environment | X | X | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brognara, L.; Mazzotti, A.; Di Martino, A.; Faldini, C.; Cauli, O. Wearable Sensor for Assessing Gait and Postural Alterations in Patients with Diabetes: A Scoping Review. Medicina 2021, 57, 1145. https://doi.org/10.3390/medicina57111145
Brognara L, Mazzotti A, Di Martino A, Faldini C, Cauli O. Wearable Sensor for Assessing Gait and Postural Alterations in Patients with Diabetes: A Scoping Review. Medicina. 2021; 57(11):1145. https://doi.org/10.3390/medicina57111145
Chicago/Turabian StyleBrognara, Lorenzo, Antonio Mazzotti, Alberto Di Martino, Cesare Faldini, and Omar Cauli. 2021. "Wearable Sensor for Assessing Gait and Postural Alterations in Patients with Diabetes: A Scoping Review" Medicina 57, no. 11: 1145. https://doi.org/10.3390/medicina57111145
APA StyleBrognara, L., Mazzotti, A., Di Martino, A., Faldini, C., & Cauli, O. (2021). Wearable Sensor for Assessing Gait and Postural Alterations in Patients with Diabetes: A Scoping Review. Medicina, 57(11), 1145. https://doi.org/10.3390/medicina57111145