
Strain Echocardiography to Predict Postoperative Atrial Fibrillation


Abstract

1. Introduction
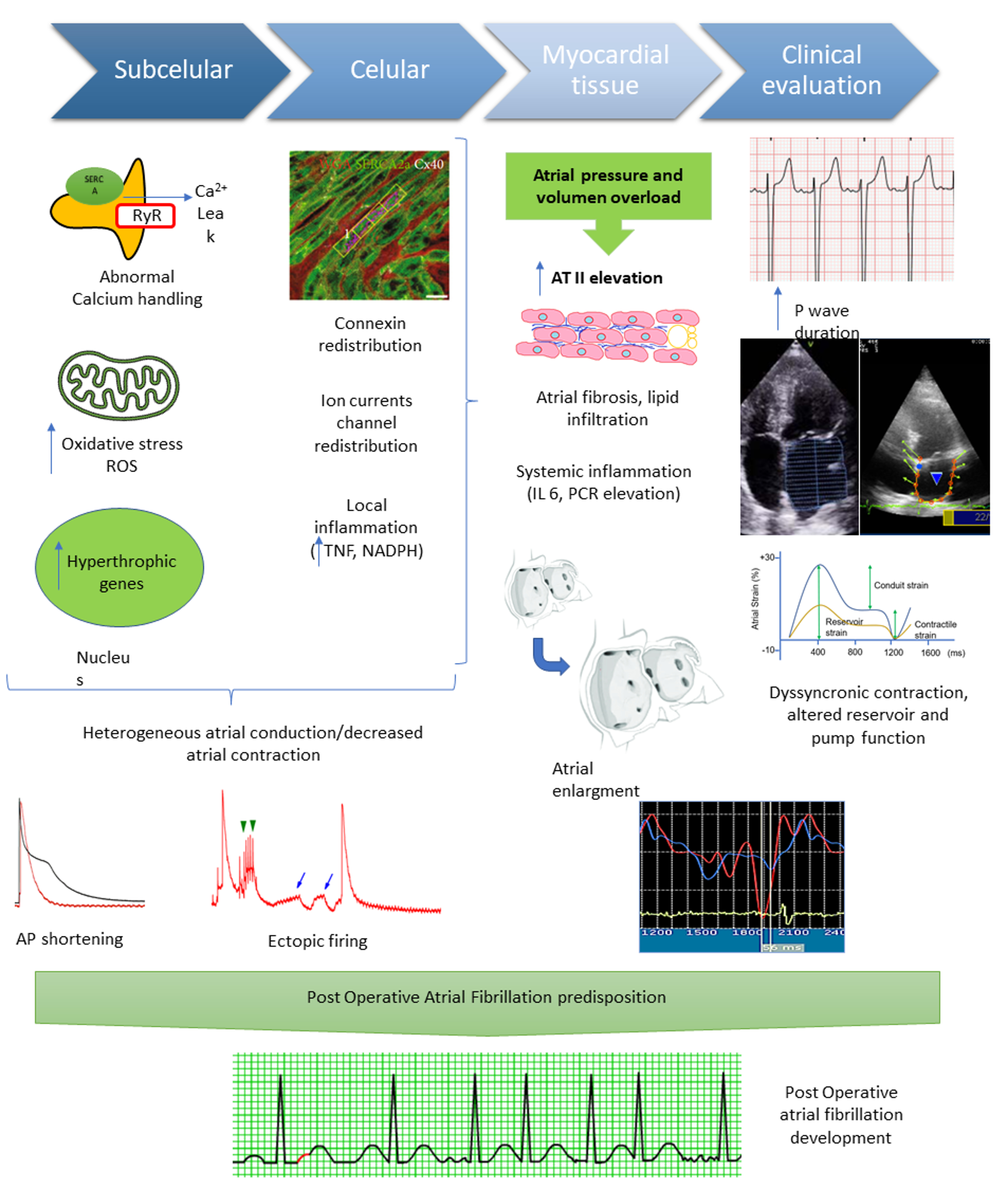
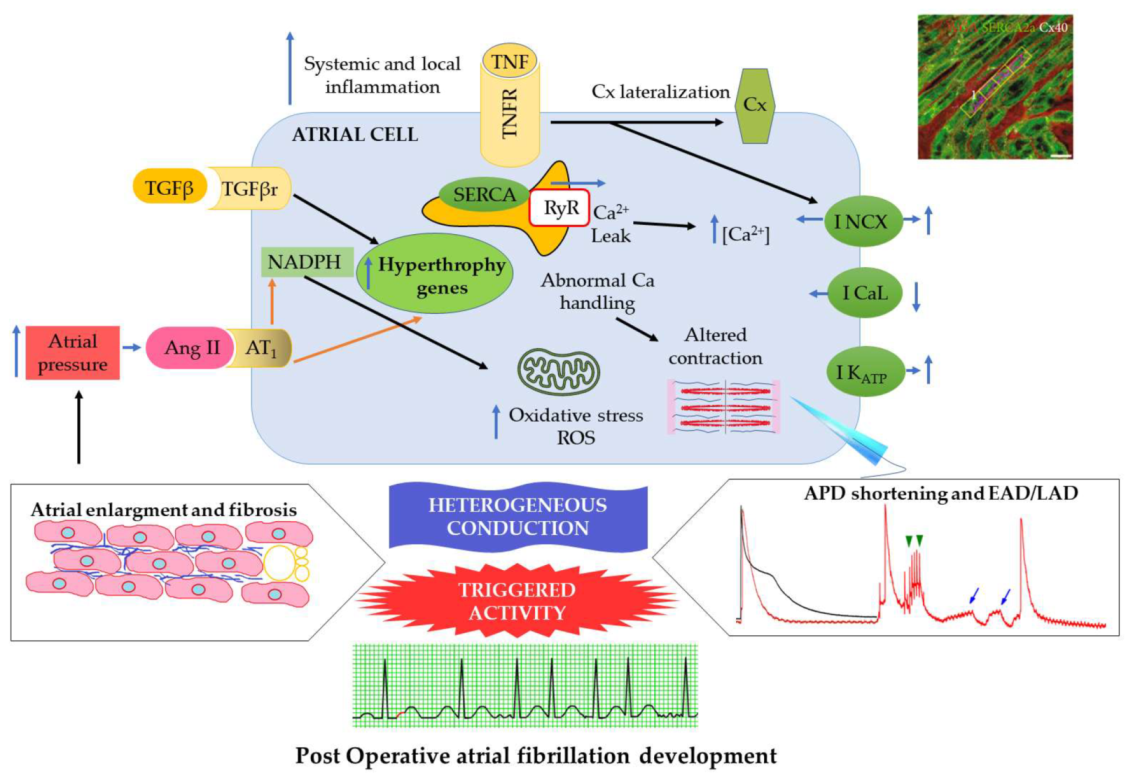
2. Mechanisms of POAF
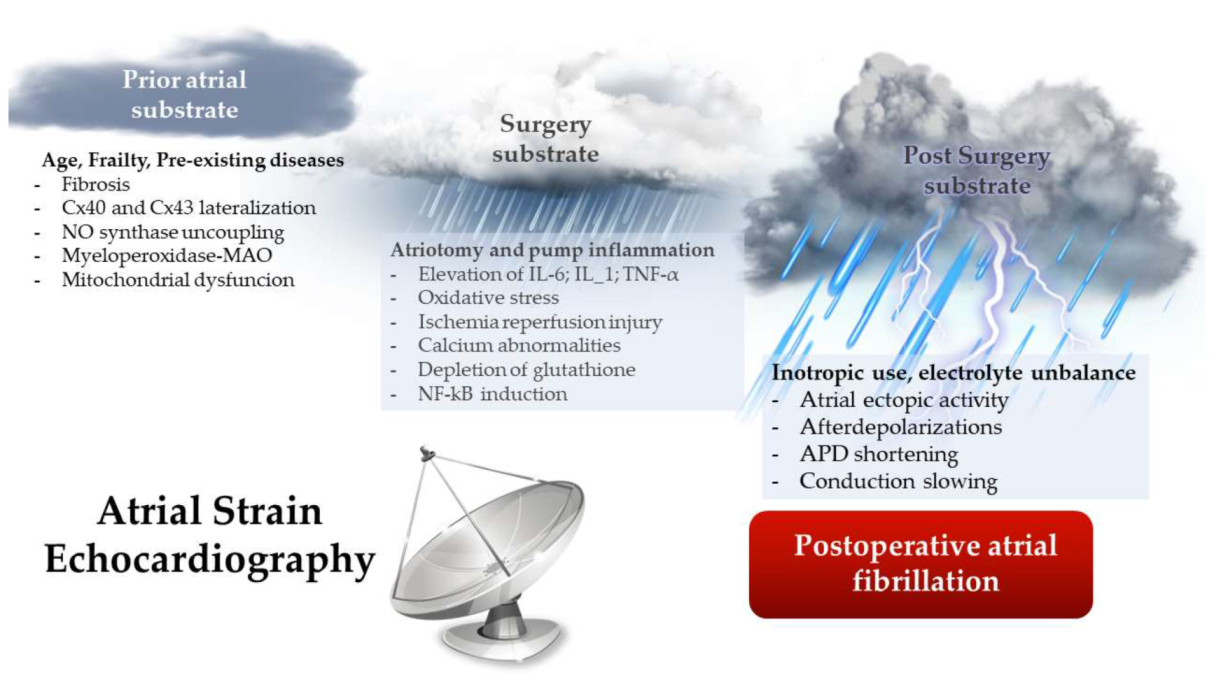
2.1. Preoperative Substrate for the Development of POAF
2.2. Surgery Substrate for the Development of POAF
2.3. Postoperative Substrate for the Development of POAF
3. Atrial Function Alteration: Strain Echocardiography as a Predictor of POAF
- Reservoir phase: It starts at the end of ventricular diastole (mitral valve closure) and continues until mitral valve opening. It involves the time of left ventricular isovolumic contraction, ejection, and isovolumic relaxation. The atria fill with blood from the pulmonary veins or the cava veins during this phase.
- Conduit phase: It comprises from mitral valve opening through diastasis until the onset of LA contraction in patients in sinus rhythm.
- Contraction phase: It covers from the onset of LA contraction until the end of ventricular diastole (mitral valve closure) in patients in sinus rhythm [62].
4. Electrical and Structural Changes in Atrial Tissue Associated with Echocardiographic Findings in the Preoperative Setting
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Júnior, F.P.; Filho, G.F.T.; Sant’anna, J.R.M.; Py, P.M.; Prates, P.R.; Nesralla, I.A.; Kalil, R.A. Idade avançada e incidência de fibrilação atrial em pós-operatório de troca valvar aórtica. Braz. J. Cardiovasc. Surg. 2014, 29, 45–50. [Google Scholar] [CrossRef]
- Greenberg, J.W.; Lancaster, T.S.; Schuessler, R.B.; Melby, S.J. Postoperative atrial fibrillation following cardiac surgery: A persistent complication. Eur. J. Cardio-Thorac. Surg. 2017, 52, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, B.A.; Zhao, Y.; He, X.; Hernandez, A.F.; Fullerton, D.A.; Thomas, K.L.; Mills, R.; Klaskala, W.; Peterson, E.D.; Piccini, J.P. Quality and Outcomes Management of Postoperative Atrial Fibrillation and Subsequent Outcomes in Contemporary Patients Undergoing Cardiac Surgery: Insights From the Society of Thoracic Surgeons CAPS-Care Atrial Fibrillation Registry. Clin. Cardiol. 2014, 13, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Akintoye, E.; Sellke, F.; Marchioli, R.; Tavazzi, L.; Mozaffarian, D. Factors associated with postoperative atrial fibrillation and other adverse events after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2018, 155, 242–251.e10. [Google Scholar] [CrossRef]
- Maesen, B.; Nijs, J.; Maessen, J.; Allessie, M.; Schotten, U. Post-operative atrial fibrillation: A maze of mechanisms. Europace 2012, 14, 159–174. [Google Scholar] [CrossRef]
- Laredo, M.; Waldmann, V.; Khairy, P.; Nattel, S. Age as a Critical Determinant of Atrial Fibrillation: A Two-sided Relationship. Can. J. Cardiol. 2018, 34, 1396–1406. [Google Scholar] [CrossRef]
- Jansen, H.J.; Moghtadaei, M.; MacKasey, M.; Rafferty, S.A.; Bogachev, O.; Sapp, J.L.; Howlett, S.E.; Rose, R.A. Atrial structure, function and arrhythmogenesis in aged and frail mice. Sci. Rep. 2017, 7, 44336. [Google Scholar] [CrossRef] [PubMed]
- Liberale, L.; Montecucco, F.; Tardif, J.-C.; Libby, P.; Camici, G.G. Inflamm-ageing: The role of inflammation in age-dependent cardiovascular disease. Eur. Heart J. 2020, 41, 2974–2982. [Google Scholar] [CrossRef]
- Stojanović, S.D.; Fiedler, J.; Bauersachs, J.; Thum, T.; Sedding, D.G. Senescence-induced inflammation: An important player and key therapeutic target in atherosclerosis. Eur. Heart J. 2020, 41, 2983–2996. [Google Scholar] [CrossRef]
- Zakkar, M.; Ascione, R.; James, A.F.; Angelini, G.D.; Suleiman, M.S. Inflammation, oxidative stress and postoperative atrial fibrillation in cardiac surgery. Pharmacol. Ther. 2015, 154, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Boos, C.J.; Anderson, R.A.; Lip, G.Y.H. Is atrial fibrillation an inflammatory disorder? Eur. Heart J. 2006, 27, 136–149. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Guzik, T.J.; Zhang, Y.H.; Zhang, M.H.; Kattach, H.; Ratnatunga, C.; Pillai, R.; Channon, K.M.; Casadei, B. A myocardial Nox2 containing NAD(P)H oxidase contributes to oxidative stress in human atrial fibrillation. Circ. Res. 2005, 97, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.G.; Editor, G.; Oxidase, N.A.D.P.H.; Griendling, K.K.; Sorescu, D.; Ushio-fukai, M. NAD(P)H Oxidase. Curr. Opin. Immunol. 2000, 16, 494–501. [Google Scholar]
- Sanchez, F.J.; Gonzalez, V.A.; Farrando, M.; Baigorria Jayat, A.O.; Segovia-Roldan, M.; Garciá-Mendívil, L.; Ordovás, L.; Prado, N.J.; Pueyo, E.; Diez, E.R. Atrial Dyssynchrony Measured by Strain Echocardiography as a Marker of Proarrhythmic Remodeling and Oxidative Stress in Cardiac Surgery Patients. Oxid. Med. Cell. Longev. 2020, 2020, 8895078. [Google Scholar] [CrossRef] [PubMed]
- Cavolli, R.; Kaya, K.; Aslan, A.; Emiroglu, O.; Erturk, S.; Korkmaz, O.; Oguz, M.; Tasoz, R.; Ozyurda, U. Does sodium nitroprusside decrease the incidence of atrial fibrillation after myocardial revascularization? A pilot study. Circulation 2008, 118, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Kattach, H.; Ratnatunga, C.; Pillai, R.; Channon, K.M.; Casadei, B. Association of Atrial Nicotinamide Adenine Dinucleotide Phosphate Oxidase Activity With the Development of Atrial Fibrillation After Cardiac Surgery. J. Am. Coll. Cardiol. 2008, 51, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, E.R.; Tangney, J.R.; Omens, J.H.; McCulloch, A.D. Biomechanics of cardiac electromechanical coupling and mechanoelectric feedback. J. Biomech. Eng. 2014, 136, 021007. [Google Scholar] [CrossRef] [PubMed]
- Fonslow, B.R.; Stein, B.D.; Webb, K.J.; Xu, T.; Choi, J.; Kyu, S.; Iii, J.R.Y. Calcium Leak Through Ryanodine Receptors Leads To Atrial Fibrillation In Three Mouse Models of Catecholaminergic Polymorphic Ventricular Tachycardia. Circ. Res. 2013, 10, 54–56. [Google Scholar] [CrossRef]
- Voigt, N.; Li, N.; Wang, Q.; Wang, W.; Trafford, A.W.; Abu-Taha, I.; Sun, Q.; Wieland, T.; Ravens, U.; Nattel, S.; et al. Enhanced sarcoplasmic reticulum Ca2+ Leak and increased Na+-Ca2+ exchanger function underlie delayed afterdepolarizations in patients with chronic atrial fibrillation. Circulation 2012, 125, 2059–2070. [Google Scholar] [CrossRef]
- Swartz, M.F.; Fink, G.W.; Sarwar, M.F.; Hicks, G.L.; Yu, Y.; Hu, R.; Lutz, C.J.; Taffet, S.M.; Jalife, J. Elevated pre-operative serum peptides for collagen i and III synthesis result in post-surgical atrial fibrillation. J. Am. Coll. Cardiol. 2012, 60, 1799–1806. [Google Scholar] [CrossRef]
- Karam, B.S.; Chavez-Moreno, A.; Koh, W.; Akar, J.G.; Akar, F.G. Oxidative stress and inflammation as central mediators of atrial fibrillation in obesity and diabetes. Cardiovasc. Diabetol. 2017, 16, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Workman, A.J.; Pau, D.; Redpath, C.J.; Marshall, G.E.; Russell, J.A.; Kane, K.A.; Norrie, J.; Rankin, A.C. Post-operative atrial fibrillation is influenced by beta-blocker therapy but not by pre-operative atrial cellular electrophysiology. J. Cardiovasc. Electrophysiol. 2006, 17, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Lezoualc’h, F.; Steplewski, K.; Sartiani, L.; Mugelli, A.; Fischmeister, R.; Bril, A. Quantitative mRNA analysis of serotonin 5-HT4 receptor isoforms, calcium handling proteins and ion channels in human atrial fibrillation. Biochem. Biophys. Res. Commun. 2007, 357, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Swartz, M.F.; Fink, G.W.; Lutz, C.J.; Taffet, S.M.; Berenfeld, O.; Vikstrom, K.L.; Kasprowicz, K.; Bhatta, L.; Puskas, F.; Kalifa, J.; et al. Left versus right atrial difference in dominant frequency, K+ channel transcripts, and fibrosis in patients developing atrial fibrillation after cardiac surgery. Hear. Rhythm 2009, 6, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Dobrev, D.; Wettwer, E.; Kortner, A.; Knaut, M.; Schüler, S.; Ravens, U. Human inward rectifier potassium channels in chronic and postoperative atrial fibrillation. Cardiovasc. Res. 2002, 54, 397–404. [Google Scholar] [CrossRef]
- Fakuade, F.E.; Steckmeister, V.; Seibertz, F.; Gronwald, J.; Kestel, S.; Menzel, J.; Pronto, J.R.D.; Taha, K.; Haghighi, F.; Kensah, G.; et al. Altered atrial cytosolic calcium handling contributes to the development of postoperative atrial fibrillation. Cardiovasc. Res. 2020, 117, 1790–1801. [Google Scholar] [CrossRef]
- Zaman, J.A.B.; Harling, L.; Ashrafian, H.; Darzi, A.; Gooderham, N.; Athanasiou, T.; Peters, N.S. Post-operative atrial fibrillation is associated with a pre-existing structural and electrical substrate in human right atrial myocardium. Int. J. Cardiol. 2016, 220, 580–588. [Google Scholar] [CrossRef]
- Jeganathan, J.; Saraf, R.; Mahmood, F.; Pal, A.; Bhasin, M.K.; Huang, T.; Mittel, A.; Knio, Z.; Simons, R.; Khabbaz, K.; et al. Mitochondrial Dysfunction in Atrial Tissue of Patients Developing Postoperative Atrial. Ann. Thorac. Surg. 2017, 104, 1547–1555. [Google Scholar] [CrossRef]
- Grammer, J.B.; Böhm, J.; Dufour, A.; Benz, M.; Lange, R.; Bauernschmitt, R. Atrial fibrosis in heart surgery patients. Decreased collagen III/I ratio in postoperative atrial fibrillation. Basic Res. Cardiol. 2005, 100, 288–294. [Google Scholar] [CrossRef]
- Rizvi, F.; Mirza, M.; Olet, S.; Albrecht, M.; Edwards, S.; Kress, D.; Ross, G.R.; Holmuhamedov, E.; Tajik, A.J.; Khanderia, B.K.; et al. Noninvasive biomarker-based risk stratification for development of new onset atrial fibrillation after coronary artery bypass surgery. Int. J. Cardiol. 2020, 15, 55–62. [Google Scholar] [CrossRef]
- Tinica, G.; Mocanu, V.; Zugun-Eloae, F.; Butcovan, D. Clinical and histological predictive risk factors of atrial fibrillation in patients undergoing open-heart surgery. Exp. Ther. Med. 2015, 10, 2299–2304. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dupont, E.; Ko, Y.S.; Rothery, S.; Coppen, S.R.; Baghai, M.; Haw, M.; Severs, N.J. The gap-junctional protein connexin40 is elevated in patients susceptible to postoperative atrial fibrillation. Circulation 2001, 103, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, M.; Kirste, W.; Kuly, S.; Amann, K.; Neuhuber, W.; Weyand, M.; Daniel, W.G.; Garlichs, C. Atrial distribution of connexin 40 and 43 in patients with intermittent, persistent, and postoperative atrial fibrillation. Hear. Lung Circ. 2006, 15, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Kourliouros, A.; Yin, X.; Didangelos, A.; Hosseini, M.T.; Valencia, O.; Mayr, M.; Jahangiri, M. Substrate modifications precede the development of atrial fibrillation after cardiac surgery: A proteomic study. Ann. Thorac. Surg. 2011, 92, 104–110. [Google Scholar] [CrossRef]
- Reilly, S.N.; Jayaram, R.; Nahar, K.; Antoniades, C.; Verheule, S.; Channon, K.M.; Alp, N.J.; Schotten, U.; Casadei, B. Atrial sources of reactive oxygen species vary with the duration and substrate of atrial fibrillation: Implications for the antiarrhythmic effect of statins. Circulation 2011, 124, 1107–1117. [Google Scholar] [CrossRef]
- Yao, C.; Veleva, T.; Scott, L.; Cao, S.; Li, L.; Chen, G.; Jeyabal, P.; Pan, X.; Alsina, K.M.; Abu-Taha, I.; et al. Enhanced Cardiomyocyte NLRP3 Inflammasome Signaling Promotes Atrial Fibrillation. Circulation 2018, 138, 2227–2242. [Google Scholar] [CrossRef] [PubMed]
- Heijman, J.; Voigt, N.; Nattel, S.; Dobrev, D. Cellular and molecular electrophysiology of atrial fibrillation initiation, maintenance, and progression. Circ. Res. 2014, 114, 1483–1499. [Google Scholar] [CrossRef]
- Kaireviciute, D.; Lip, G.Y.H.; Balakrishnan, B.; Uzdavinys, G.; Norkunas, G.; Kalinauskas, G.; Sirvydis, V.; Aidietis, A.; Zanetto, U.; Sihota, H.; et al. Intracardiac expression of markers of endothelial damage/dysfunction, inflammation, thrombosis, and tissue remodeling, and the development of postoperative atrial fibrillation. J. Thromb. Haemost. 2011, 9, 2345–2352. [Google Scholar] [CrossRef]
- Yamac, A.H.; Kucukbuzcu, S.; Ozansoy, M.; Gok, O.; Oz, K.; Erturk, M.; Yilmaz, E.; Ersoy, B.; Zeybek, R.; Goktekin, O.; et al. Altered expression of micro-RNA 199a and increased levels of cardiac SIRT1 protein are associated with the occurrence of atrial fibrillation after coronary artery bypass graft surgery. Cardiovasc. Pathol. 2016, 25, 232–236. [Google Scholar] [CrossRef]
- Tsoporis, J.N.; Fazio, A.; Rizos, I.K.; Proteau, G.; Salpeas, V.; Rigopoulos, A. Increased right atrial appendage apoptosis is associated with differential regulation of candidate MicroRNAs 1 and 133A in patients who developed atrial fibrillation after cardiac surgery. J. Mol. Cell. Cardiol. 2018, 121, 25–32. [Google Scholar] [CrossRef]
- Antoniades, C.; Demosthenous, M.; Reilly, S.; Margaritis, M.; Zhang, M.H.; Antonopoulos, A.; Marinou, K.; Nahar, K.; Jayaram, R.; Tousoulis, D.; et al. Myocardial redox state predicts in-hospital clinical outcome after cardiac surgery: Effects of short-term pre-operative statin treatment. J. Am. Coll. Cardiol. 2012, 59, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Corradi, D.; Saffitz, J.E.; Novelli, D.; Asimaki, A.; Simon, C.; Oldoni, E.; Masson, S.; Meessen, J.M.T.A.; Monaco, R.; Manuguerra, R.; et al. Prospective Evaluation of Clinico-pathological Predictors of Post-operative Atrial Fibrillation: An Ancillary Study from the OPERA Trial. Circ. Arrhythmia Electrophysiol. 2020, 13, e008382. [Google Scholar] [CrossRef] [PubMed]
- Adam, O.; Lavall, D.; Theobald, K.; Hohl, M.; Grube, M.; Ameling, S.; Sussman, M.A.; Rosenkranz, S.; Kroemer, H.K.; Schäfers, H.J.; et al. Rac1-Induced Connective Tissue Growth Factor Regulates Connexin 43 and N-Cadherin Expression in Atrial Fibrillation. J. Am. Coll. Cardiol. 2010, 55, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Slagsvold, K.H.; Rognmo, O.; Høydal, M.A.; Wisløff, U.; Wahba, A.; Res, C. Remote Ischemic Preconditioning Preserves Mitochondrial Function and Influences Myocardial MicroRNA Expression in Atrial Myocardium During Coronary Bypass Surgery The online version of this article, along with updated information and services, is locate. Circ. Res. 2013, 114, 851–859. [Google Scholar] [CrossRef]
- Elahi, M.M.; Flatman, S.; Matata, B.M. Tracing the origins of postoperative atrial fibrillation: The concept of oxidative stress-mediated myocardial injury phenomenon. Eur. J. Prev. Cardiol. 2008, 15, 735–741. [Google Scholar] [CrossRef]
- Willeford, A.; Suetomi, T.; Nickle, A.; Hoffman, H.M.; Miyamoto, S.; Heller Brown, J. CaMKIIδ-mediated inflammatory gene expression and inflammasome activation in cardiomyocytes initiate inflammation and induce fibrosis. JCI Insight 2018, 3, e97054. [Google Scholar] [CrossRef]
- Jeong, E.; Liu, M.; Sturdy, M.; Gao, G.; Varghese, S.T.; Sovari, A.A.; Dudley, S.C.D., Jr. Metabolic stress, reactive oxygen species, and arrhythmia. J. Mol. Cell. Cardiol. 2012, 52, 454–463. [Google Scholar] [CrossRef]
- Li, J.Y.; Lai, Y.J.; Yeh, H.I.; Chen, C.L.; Sun, S.; Wu, S.J.; Lin, F.Y. Atrial gap junctions, NF-κB and fibrosis in patients undergoing coronary artery bypass surgery: The relationship with postoperative atrial fibrillation. Cardiology 2008, 112, 81–88. [Google Scholar] [CrossRef]
- Jayaram, R.; Goodfellow, N.; Zhang, M.H.; Reilly, S.; Crabtree, M.; De Silva, R.; Sayeed, R.; Casadei, B. Molecular mechanisms of myocardial nitroso-redox imbalance during on-pump cardiac surgery. Lancet 2015, 385, S49. [Google Scholar] [CrossRef]
- Ishii, Y.; Schuessler, R.B.; Gaynor, S.L.; Yamada, K.; Fu, A.S.; Boineau, J.P.; Damiano, R.J. Inflammation of atrium after cardiac surgery is associated with inhomogeneity of atrial conduction and atrial fibrillation. Circulation 2005, 111, 2881–2888. [Google Scholar] [CrossRef]
- Kumagai, K.; Nakashima, H.; Saku, K. The HMG-CoA reductase inhibitor atorvastatin prevents atrial fibrillation by inhibiting inflammation in a canine sterile pericarditis model. Cardiovasc. Res. 2004, 62, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, Y.T.; Shan, Z.L.; Guo, H.Y.; Guan, Y.; Yuan, H.T. Role of inflammation in the initiation and maintenance of atrial fibrillation and the protective effect of atorvastatin in a goat model of aseptic pericarditis. Mol. Med. Rep. 2015, 11, 2615–2623. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.N.; Ryu, K.; Khrestian, C.; Wagoner, D.R.V.A.N.; Waldo, A.L. Prednisone Prevents Inducible Atrial Flutter in the Canine Sterile Pericarditis Model. J. Cardiovasc. Electrophysiol. 2008, 19, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Ryu, K.; Li, L.; Khrestian, C.M.; Matsumoto, N.; Sahadevan, J.; Ruehr, M.L.; Van Wagoner, D.R.; Efimov, I.R.; Waldo, A.L. Effects of sterile pericarditis on connexins 40 and 43 in the atria: Correlation with abnormal conduction and atrial arrhythmias. Am. J. Physiol.-Heart Circ. Physiol. 2007, 44106, H1231–H1241. [Google Scholar] [CrossRef]
- Tselentakis, E.V.; Woodford, E.; Chandy, J.; Gaudette, G.R.; Saltman, A.E. Inflammation Effects on the Electrical Properties of Atrial Tissue and Inducibility of Postoperative Atrial Fibrillation. J. Surg. Res. 2006, 75, 68–75. [Google Scholar] [CrossRef]
- Fu, X.; Zhao, N.; Dong, Q.; Du, L.; Chen, X. Interleukin-17A contributes to the development of post-operative atrial fibrillation by regulating inflammation and fibrosis in rats with sterile pericarditis. Int. J. Mol. Med. 2015, 36, 83–92. [Google Scholar] [CrossRef]
- Huang, Z.; Chen, X.; Qian, C.; Dong, Q. Signal Transducer and Activator of Transcription 3/MicroRNA-21 Feedback Loop Contributes to Atrial Fibrillation by Promoting Atrial Fibrosis in a Rat Sterile Pericarditis Model. Circ. Arrhythmia Electrophysiol. 2016, 9, e003396. [Google Scholar] [CrossRef]
- Edler, I.; Lindström, K. Historical Review The history of echocardiography. Ultrasound Med. Biol. 2004, 30, 1565–1644. [Google Scholar] [CrossRef]
- Ciuffo, L.; Tao, S.; Gucuk Ipek, E.; Zghaib, T.; Balouch, M.; Lima, J.A.C.; Nazarian, S.; Spragg, D.D.; Marine, J.E.; Berger, R.D.; et al. Intra-Atrial Dyssynchrony During Sinus Rhythm Predicts Recurrence After the First Catheter Ablation for Atrial Fibrillation. JACC Cardiovasc. Imaging 2019, 12, 310–319. [Google Scholar] [CrossRef]
- Xu, C.; Chen, K.; Yu, F.; Wang, Q.; Su, H.; Yang, D.; Xu, J.; Yan, J. Atrial Dyssynchrony: A New Predictor for Atrial High-Rate Episodes in Patients with Cardiac Resynchronization Therapy. Cardiol. 2019, 144, 18–26. [Google Scholar] [CrossRef]
- Melduni, R.M.; Suri, R.M.; Seward, J.B.; Bailey, K.R.; Ammash, N.M.; Oh, J.K.; Schaff, H.V.; Gersh, B.J.; Hil, D.P. Diastolic Dysfunction in Patients Undergoing Cardiac Surgery. J. Am. Coll. Cardiol. 2011, 58, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Pathan, F.; D’Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70.e8. [Google Scholar] [CrossRef] [PubMed]
- Merckx, K.L.; De Vos, C.B.; Palmans, A.; Habets, J.; Tieleman, R.G. Atrial Activation Time Determined by Transthoracic Doppler Tissue Imaging Can Be Used as an Estimate of the Total Duration of Atrial Electrical Activation. J. Am. Soc. Echocardiogr. 2005, 18, 940–944. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.M.; Hars, C.; Schiedat, F.; Osche, L.I.B.; Gotzmann, M.; Strauch, J.; Dietrich, J.W.; Vogt, M.; Tannapfel, A.; Deneke, T.; et al. Correlation Between Total Atrial Conduction Time Estimated via Tissue Doppler Imaging ( PA-TDI Interval ), Structural Atrial Remodeling and New-Onset of Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2013, 24, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Tayyareci, Y.; Yildirimtürk, O.; Aytekin, V.; Memic, K.; Behramoglu, F.; Cemsid Demiroglu, I.C.; Aytekin, S. Preoperative left atrial mechanical dysfunction predicts postoperative atrial fibrillation after coronary artery bypass graft operation: A velocity vector imaging-based study. Circ. J. 2010, 74, 2109–2117. [Google Scholar] [CrossRef]
- Kawczynski, M.J.; Gilbers, M.; Van De Walle, S.; Schalla, S.; Crijns, H.J.; Maessen, J.G.; Schotten, U.; Maesen, B.; Bidar, E. Role of pre-operative transthoracic echocardiography in predicting post-operative atrial fibrillation after cardiac surgery: A systematic review of the literature and meta-analysis. EP Eur. 2021, 23, 1731–1743. [Google Scholar] [CrossRef]
- Hirose, T.; Kawasaki, M.; Tanaka, R.; Ono, K.; Watanabe, T.; Iwama, M.; Noda, T.; Watanabe, S.; Takemura, G.; Minatoguchi, S. Left atrial function assessed by speckle tracking echocardiography as a predictor of new-onset non-valvular atrial fibrillation: Results from a prospective study in 580 adults. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 243–250. [Google Scholar] [CrossRef]
- Gasparovic, H.; Cikes, M.; Kopjar, T.; Hlupic, L.; Velagic, V.; Milicic, D.; Bijnens, B.; Colak, Z.; Biočina, B. Atrial apoptosis and fibrosis adversely affect atrial conduit, reservoir and contractile functions. Interact. Cardiovasc. Thorac. Surg. 2014, 19, 223–230. [Google Scholar] [CrossRef]
- Mandoli, G.E.; Pastore, M.C.; Benfari, G.; Bisleri, G.; Maccherini, M.; Lisi, G.; Cameli, P.; Lisi, M.; Dokollari, A.; Carrucola, C.; et al. Left atrial strain as a pre-operative prognostic marker for patients with severe mitral regurgitation. Int. J. Cardiol. 2020, 41, ehaa946.0054. [Google Scholar] [CrossRef]
- Pessoa-Amorim, G.; Mancio, J.; Vouga, L.; Ribeiro, J.; Gama, V.; Bettencourt, N.; Fontes-Carvalho, R. Impaired Left Atrial Strain as a Predictor of New-onset Atrial Fibrillation After Aortic Valve Replacement Independently of Left Atrial Size. Rev. Española Cardiol. 2017, 71, 466–476. [Google Scholar] [CrossRef]
- Poulin, F.; Thavendiranathan, P.; Carasso, S.; Rakowski, H.; Horlick, E.M.; Osten, M.D.; Cusimano, R.J.; Woo, A. Left Atrial Phasic Function and Its Association With Atrial Fibrillation in Patients After Transcatheter Aortic Valve Implantation. Can. J. Cardiol. 2017, 33, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Pernigo, M.; Benfari, G.; Geremia, G.; Noni, M.; Borio, G.; Mazzali, G.; Zamboni, M.; Onorati, F.; Faggian, G.; Vassanelli, C.; et al. Atrial Function as an Independent Predictor of Postoperative Atrial Fibrillation in Patients Undergoing Aortic Valve Surgery for Severe Aortic Stenosis. J. Am. Soc. Echocardiogr. 2017, 30, 956–965.e1. [Google Scholar] [CrossRef] [PubMed]
- Imanishi, J.; Tanaka, H.; Sawa, T.; Motoji, Y.; Miyoshi, T.; Mochizuki, Y.; Fukuda, Y.; Tatsumi, K.; Matsumoto, K.; Okita, Y.; et al. Left atrial booster-pump function as a predictive parameter for new-onset postoperative atrial fibrillation in patients with severe aortic stenosis. Int. J. Cardiovasc. Imaging 2014, 30, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Candan, O.; Ozdemir, N.; Aung, S.M.; Hatipoglu, S.; Karabay, C.Y.; Guler, A.; Gecmen, C.; Dogan, C.; Omaygenc, O.; Bakal, R.B. Atrial longitudinal strain parameters predict left atrial reverse remodeling after mitral valve surgery: A speckle tracking echocardiography study. Int. J. Cardiovasc. Imaging 2014, 30, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- Sabry, A.M.; Mansour, H.A.E.; El-azm, T.H.A.; Mostafa, S.A.; Zahid, B.S. Echocardiographic predictors of atrial fibrillation after mitral valve replacement. Egypt. Hear. J. 2017, 69, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Aksu, U.; Kalkan, K.; Gulcu, O.; Aksakal, E.; Öztürk, M.; Topcu, S. The role of the right atrium in development of postoperative atrial fibrillation: A speckle tracking echocardiography study. J. Clin. Ultrasound 2019, 47, 470–476. [Google Scholar] [CrossRef]
- Kawakami, H.; Ramkumar, S.; Nolan, M.; Wright, L.; Yang, H.; Negishi, K.; Marwick, T.H. Left Atrial Mechanical Dispersion Assessed by Strain Echocardiography as an Independent Predictor of New-Onset Atrial Fibrillation: A Case-Control Study. J. Am. Soc. Echocardiogr. 2019, 32, 1268–1276.e3. [Google Scholar] [CrossRef]
- Kowallick, J.T.; Kutty, S.; Edelmann, F.; Chiribiri, A.; Villa, A.; Steinmetz, M.; Sohns, J.M.; Staab, W.; Bettencourt, N.; Unterberg-Buchwald, C.; et al. Quantification of left atrial strain and strain rate using Cardiovascular Magnetic Resonance myocardial feature tracking: A feasibility study. J. Cardiovasc. Magn. Reson. 2014, 16, s12968–s13014. [Google Scholar] [CrossRef]
- Mărgulescu, A.D.; Nuñez-Garcia, M.; Alarcón, F.; Benito, E.M.; Enomoto, N.; Cozzari, J.; Chipa, F.; Fernandez, H.; Borras, R.; Guasch, E.; et al. Reproducibility and accuracy of late gadolinium enhancement cardiac magnetic resonance measurements for the detection of left atrial fibrosis in patients undergoing atrial fibrillation ablation procedures. EP Eur. 2019, 21, 724–731. [Google Scholar] [CrossRef]
- Başaran, Ö.; Tigen, K.; Gözübüyük, G.; Dündar, C.; Güler, A.; Taşar, O.; Biteker, M.; Karabay, C.Y.; Bulut, M.; Karaahmet, T.; et al. Predictive role of left atrial and ventricular mechanical function in postoperative atrial fibrillation: A two-dimensional speckle-tracking echocardiography study. Turk Kardiyol. Dern. Ars. 2016, 44, 45–52. [Google Scholar] [CrossRef]
- Parsaee, M.; Moradi, B.; Esmaeilzadeh, M.; Haghjoo, M.; Bakhshandeh, H.; Sari, L. New onset atrial fibrillation after coronary artery bypasses grafting; an evaluation of mechanical left atrial function. Arch. Iran. Med. 2014, 17, 501–506. [Google Scholar] [PubMed]
- Osranek, M.; Kaniz, F.; Fatema, Q.; Al-Saileek, A.; Barnes, M.E.; Bailey, K.R. Left Atrial Volume Predicts the Risk of Atrial Fibrillation After Cardiac Surgery A Prospective Study. J. Am. Coll. Cardiol. 2006, 48, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Conde, D.; Van Oosten, E.M.; Hamilton, A.; Petsikas, D.; Payne, D.; Redfearn, D.P.; Hopman, W.M.; Bayés De Luna, A.; Baranchuk, A. Prevalence of interatrial block in patients undergoing coronary bypass graft surgery. Int. J. Cardiol. 2014, 171, e98–e99. [Google Scholar] [CrossRef] [PubMed]
- Bayés De Luna, A.; Platonov, P.; Cosio, F.G.; Cygankiewicz, I.; Pastore, C.; Baranowski, R.; Bayés-Genis, A.; Guindo, J.; Viñolas, X.; Garcia-Niebla, J.; et al. Interatrial blocks. A separate entity from left atrial enlargement: A consensus report. J. Electrocardiol. 2012, 45, 445–451. [Google Scholar] [CrossRef]
- Hatam, N.; Aljalloud, A.; Mischke, K.; Karfis, E.A.; Autschbach, R.; Hoffmann, R.; Goetzenich, A. Interatrial conduction disturbance in postoperative atrial fibrillation: A comparative study of P-wave dispersion and Doppler myocardial imaging in cardiac surgery. J. Cardiothorac. Surg. 2014, 9, 114. [Google Scholar] [CrossRef][Green Version]
- García-Izquierdo Jaén, E.; Rodríguez, P.C.; Solís, L.S.; Trung, C.P.; Sánchez, D.J.; García, M.S.; Urda, V.C.; Ramos, J.T.; Lozano, I.F. Bayes’ syndrome in cardiac surgery: Prevalence of interatrial block in patients younger than 65 years undergoing cardiac surgery and association with postoperative atrial fibrillation. Arch. Cardiol. Mex. 2018, 88, 369–375. [Google Scholar] [CrossRef]
- Korantzopoulos, P.; Letsas, K.; Fragakis, N.; Tse, G.; Liu, T. Oxidative stress and atrial fibrillation: An update. Free Radic. Res. 2018, 52, 1199–1209. [Google Scholar] [CrossRef]
- Smyth, J.W.; Hong, T.T.; Gao, D.; Vogan, J.M.; Jensen, B.C.; Fong, T.S.; Simpson, P.C.; Stainier, D.Y.R.; Chi, N.C.; Shaw, R.M. Limited forward trafficking of connexin 43 reduces cell-cell coupling in stressed human and mouse myocardium. J. Clin. Investig. 2010, 120, 266–279. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preoperative Risk Factors | Intra-Operative Risk Factors | Postoperative Risk Factors |
|---|---|---|
| Advanced age | Aortic cross-clamp time | Respiratory compromise |
| Male sex | Type of surgery | Red cell transfusion |
| Hypertension | On-pump time | Use of adrenergic drugs |
| COPD | Bicaval canulation | |
| Heart failure | Systemic hypothermia | |
| Left ventricular hypertrophy | ||
| Renal failure | ||
| Obesity | ||
| Withdrawal of beta-blockers | ||
| Diabetes mellitus |
| Substrate | Tissue | Molecular/Function | References |
|---|---|---|---|
| Electrophysiology | ↔/↓ dV/dtmax | ↔ SCN5A | [14,22] |
| ↔ APD/ERP ↓ APD | ↔ ICa,L ↔ IK1 ↔ IK,Ach ↔ IKur ↔ Ito, ↑ IKATP | [14,22,23,24,25] | |
| calcium handling | ↓ sarcolipin ↔ SERCA2a ↔ phospholamban ↔ RYR2 ↔ IP3R ↔ Na+/Ca2+ exchanger | [23,26,27] | |
| Structural remodeling | ↔/↑ RA fibrosis ↑ LA fibrosis | ↑ TGFβ1 ↔/↑ type I and type III collagen | [20,28] [24,29,30] |
| ↔/↑ apoptosis ↑ myocytolysis | ↑ Apoptosis-inducing factor ↔ p-BCL-2 ↔ Caspase 3 | [31] | |
| ↑ Myocyte hypertrophy | ↓ Myosin 6 ↑ Myosin 7 | [31] | |
| ↔ β1-AR, ↔ β2-AR | [23] | ||
| Cell–cell coupling | Connexin 40 lateralization | ↔/↑ Connexin 40 | [14] |
| Connexin 43 lateralization | ↔ Connexin 43 | [14] | |
| ↔ Connexin 45 | [32] | ||
| ↓ Connexin 40:connexin 43 ratio | [33] | ||
| Oxidative stress | ↑ ROS ↓ Peroxiredoxin 1 ↑ NOX2 ↑ p22phox ↔ MnSOD | [34,35,36] | |
| ↑ 3-nitrotyrosine | Peroxinitrites | [14] | |
| Inflammation | ↑ TNFα | ↑/↓ NF-κB ↔/↑ IL-6 ↑ TLR4 ↑ NLRP3 ↑transferrin | [34,35,37,38] |
| MicroRNAs | ↓ MicroRNA-195 ↓ MicroRNA-199a ↔ MicroRNA-1 ↔ MicroRNA-133a | [39,40] |
| Study (Year, Type Surgery) | N° Patients | POAF (%) | Results |
|---|---|---|---|
| Tayyareci et al. (2010, CABG) | 96 | 26 | LA reservoir strain < 44% predicted POAF (Se: 88.7%; Sp: 96%; p: 0.0001) |
| LA systolic strain rate < 1.7 s−1 predicted POAF (Se: 88%; Sp: 86.2%; p: 0.0001) | |||
| LA conduit strain rate < 1.95 s−1 predicted POAF (Se: 72%; Sp: 70.4% p: 0.0001) | |||
| Gabrielli et al. (2011, CABG) | 70 | 26 | LA contractile strain rate impairment predicted POAF (p: <0.01) |
| LA reservoir strain rate impairment predicted POAF (p: <0.01) | |||
| Her et al. (2013, CABG) | 53 | 24 | LA reservoir global strain < 27.7% predicted POAF (Se: 81%; Sp: 69%; p: <0.003) |
| Imanishi et al. (2014, AVR) | 27 | 56 | LA contractile strain rate > 0.79 s−1 predicted POAF (Se: 60%; Sp: 92%; p: <0.0001) |
| Cameli et al. (2014, AVR) | 76 | 19.7 | LA reservoir global strain < 16.8% predicted POAF (p: <0.0001; HR 6.55; Se: 86%; Sp: 91%) |
| Verdejo et al. (2016, CABG) | 70 | 38.5 | LA reservoir global strain impairment predicted POAF (p: <0.001) |
| Basaran et al. (2016, CABG) | 90 | 25.6 | LA reservoir impairment predicted POAF (p: <0.0001) |
| Pernigo et al. (2017, AVR) | 60 | 43.3 | LA strain reservoir < 23% predicted POAF (p: 0.0001) |
| Atrial strain before contraction < 10% predicted POAF (p: 0.0001) | |||
| Sabry et al. (2017, MVR) | 50 | 44 | LA reservoir strain < 23% predicted POAF (Se: 90.9%; Sp: 93.33%; p: 0.003) |
| Pessoa-Amorin et al. (2017, MVR) | 115 | 36.7 | LA strain reservoir < 18.7% predicted POAF independent of atrial volume (p: 0.039) |
| Atrial strain before contraction < 7.9% predicted POAF (p: 0.038) | |||
| Lisi et al. (2018, MVR) | 36 | 32 | Lower values of LA reservoir strain were associated with POAF (p: 0.0001) |
| Aksu et al. (2019, CABG) | 74 | 50 | RA reservoir strain < 11 predicted POAD (Se: 72%; Sp: 65% p: 0.001) |
| Study (Year) | N° Patients | Endpoint | p Value | Echocardiographic Alteration | Substrate Alteration |
|---|---|---|---|---|---|
| Sanchez et al. (2020) | 45 | POAF | 0.0416 | Interatrial dyssyncrhony | AP shortening, Cx40 lateralization, higher nitrotyrosine signal, KATP increased signal |
| Fakuade et al. (2020) | 202 | POAF | <0.05/<0.01 | Reduced pump and reservoir function | Reduction of SR Ca2+ release in atrial myocytes. |
| Mandoli et al. (2020) | 65 | HF and mortality | 0.0001 | Reservoir LA strain | Atrial fibrosis |
| Gasparovic et al. (2014) | 44 | Effect of AR on atrial strain rate | 0.006/0.001 | Strain rate reservoir and pump atrial function | Atrial fibrosis and apoptosis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez, F.J.; Pueyo, E.; Diez, E.R. Strain Echocardiography to Predict Postoperative Atrial Fibrillation. Int. J. Mol. Sci. 2022, 23, 1355. https://doi.org/10.3390/ijms23031355
Sánchez FJ, Pueyo E, Diez ER. Strain Echocardiography to Predict Postoperative Atrial Fibrillation. International Journal of Molecular Sciences. 2022; 23(3):1355. https://doi.org/10.3390/ijms23031355
Chicago/Turabian StyleSánchez, Francisco Javier, Esther Pueyo, and Emiliano Raúl Diez. 2022. "Strain Echocardiography to Predict Postoperative Atrial Fibrillation" International Journal of Molecular Sciences 23, no. 3: 1355. https://doi.org/10.3390/ijms23031355
APA StyleSánchez, F. J., Pueyo, E., & Diez, E. R. (2022). Strain Echocardiography to Predict Postoperative Atrial Fibrillation. International Journal of Molecular Sciences, 23(3), 1355. https://doi.org/10.3390/ijms23031355