
Online Information of COVID-19: Visibility and Characterization of Highest Positioned Websites by Google between March and April 2020—A Cross-Country Analysis

 , , ,
, , ,  and
and
Abstract
:1. Introduction
- -
- Characterization and analysis of websites typology by Google based on “COVID-19”, “Coronavirus”, “SARS-CoV-2” and “fake news” key words;
- -
- Characterization and analysis of online information returned by Google based on “COVID-19”, “Coronavirus” and “SARS-CoV-2” key words;
- -
- Calculating frequency of fake news on “COVID-19”, “Coronavirus”, “SARS-CoV-2” key words;
- -
- Characterization and analysis of online information returned by Google based on “fake news” key words;
- -
- Analysis of associations between results and epidemiological data on COVID-19, such as: number of deaths, number of infections, number of SARS-CoV-2 tests performed;
- -
- Characterization and analysis of online information returned by Google based on “COVID-19”, “Coronavirus”, “SARS-CoV-2” and “fake news” about celebrities, religion and testimonials;
- -
- Analysis of the Journal of the American Medical Association (JAMA score).
2. Materials and Methods
2.1. Websites
2.2. Keywords
2.3. Content Analysis
2.4. Websites Typology
- -
- Government (G): websites of governmental bodies, local authorities; e.g., www.whitehouse.gov, www.epa.gov; (accessed on 30 March 2020)
- -
- Health Portal (HP): websites with information on a variety of health topics, e.g., www.medscape.com (accessed on 30 March 2020);
- -
- News (N): websites of newspapers, magazines or TV; e.g., www.cbsnews.com (accessed on 30 March 2020), www.nytimes.com (accessed on 30 March 2020);
- -
- Non-Profit (NP): websites of non-profit organization, e.g., https://choice.npr.org (accessed on 30 March 2020);
- -
- Professional (P): websites created by health professional organizations (medical school, clinic/hospitals, medical boards); e.g., https://sph.nus.edu.sg (accessed on 30 March 2020);
- -
- Commercial (C): websites selling drugs, supplements or other; e.g., https://www.diagnostictechnology.com.au/ (accessed on 30 March 2020);
- -
- Scientific journal (SJ): websites of academic journals, e.g., www.thelancet.com (accessed on 30 March 2020).
2.5. Selection of Countries
2.6. Inclusion and Exclusion Criteria
2.7. JAMA Score
2.8. Epidemiological Data and Statistical Analysis
3. Results
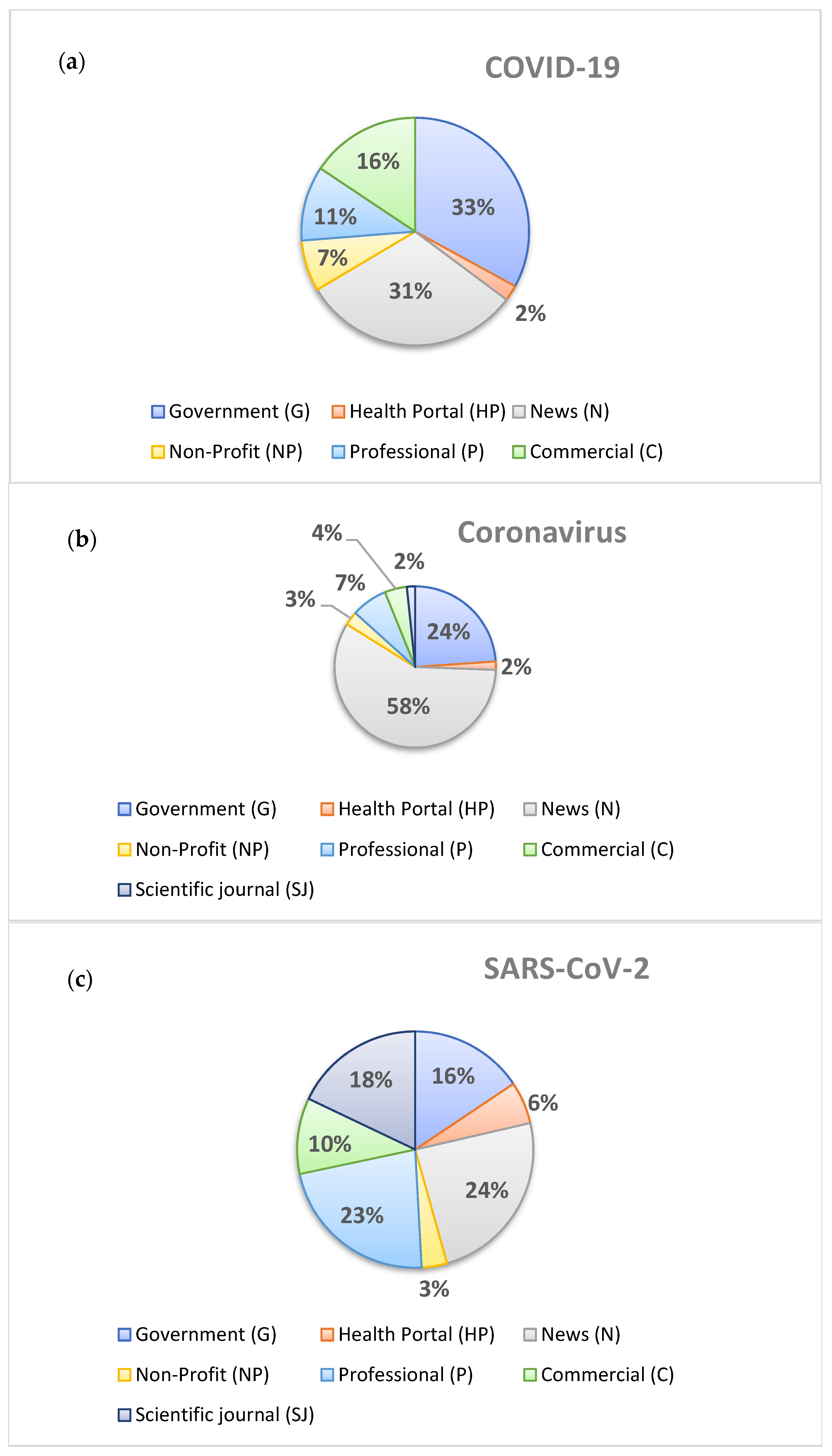
3.1. Characterization and Analysis of Websites Typology by Google Based on the Keywords “COVID-19”, “Coronavirus”, “SARS-CoV-2” and “Fake News”
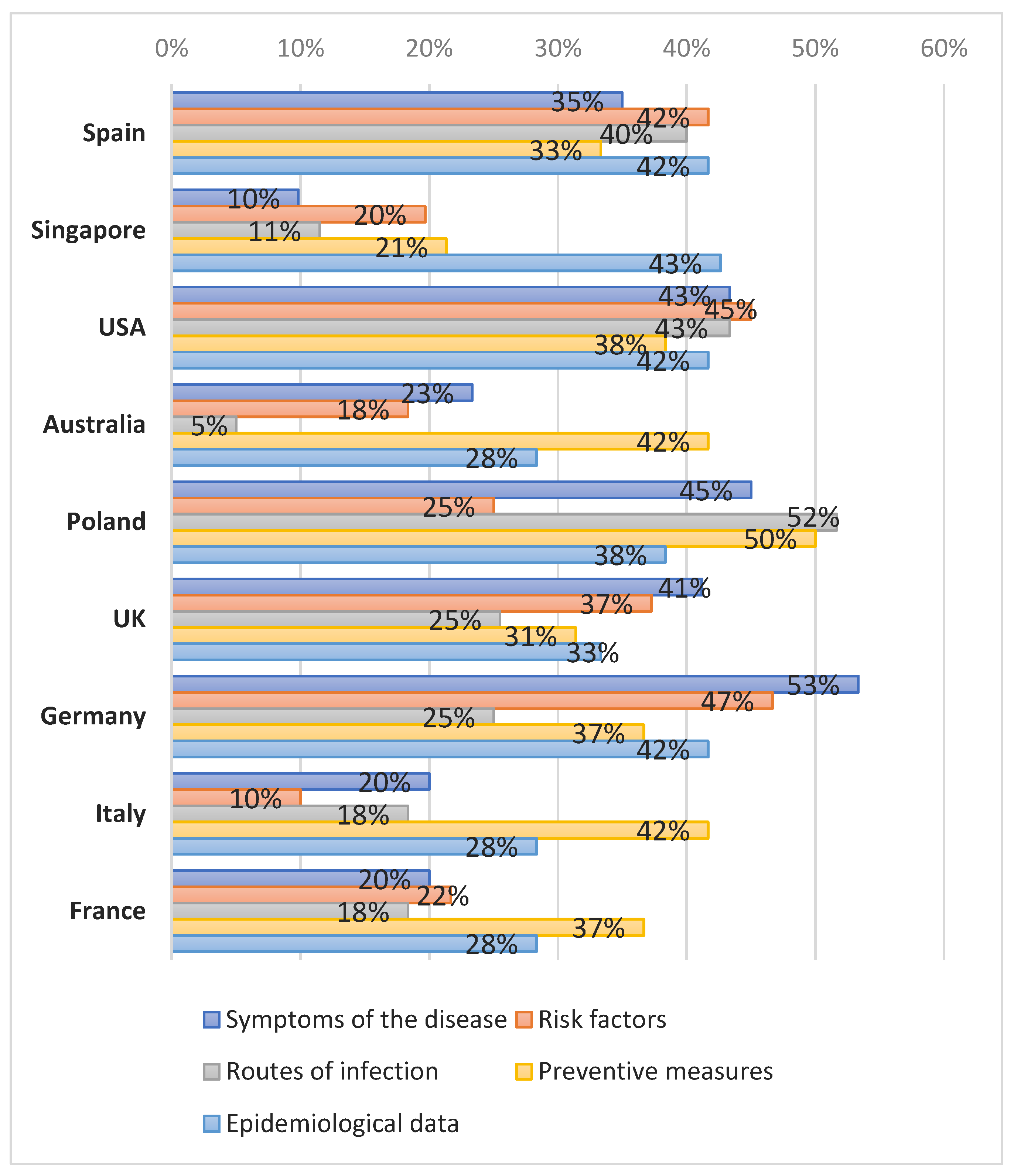
3.2. Characterization and Analysis of Online Information Returned by Google Based on the “COVID-19”, “Coronavirus” and “SARS-CoV-2” Keywords
3.3. Calculating the Frequency of Fake News Referrals from the “COVID-19”, “Coronavirus” and “SARS-CoV-2” Keywords
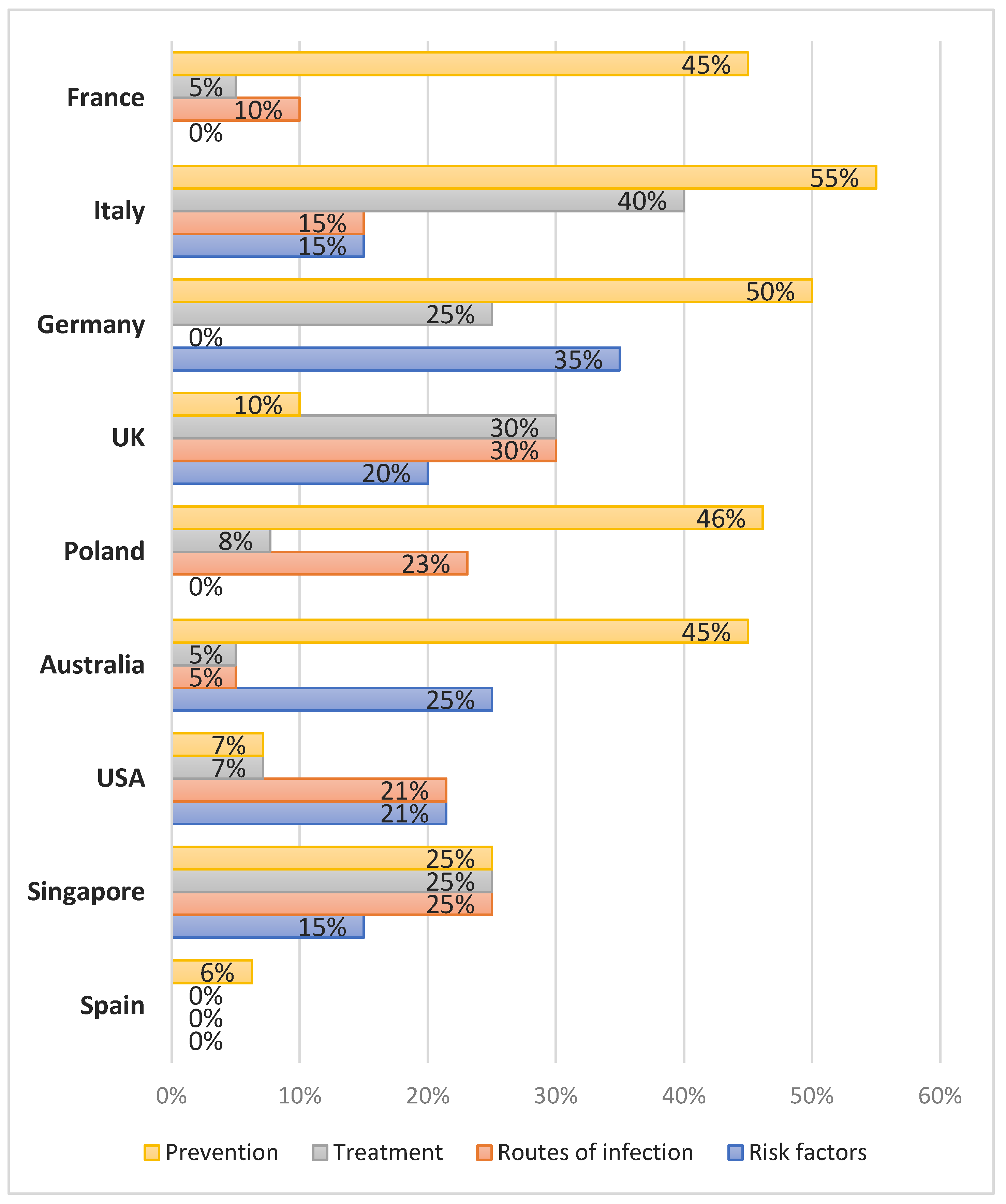
3.4. Characterization and Analysis of Online Information Returned by Google Based on the “Fake News” Keyword
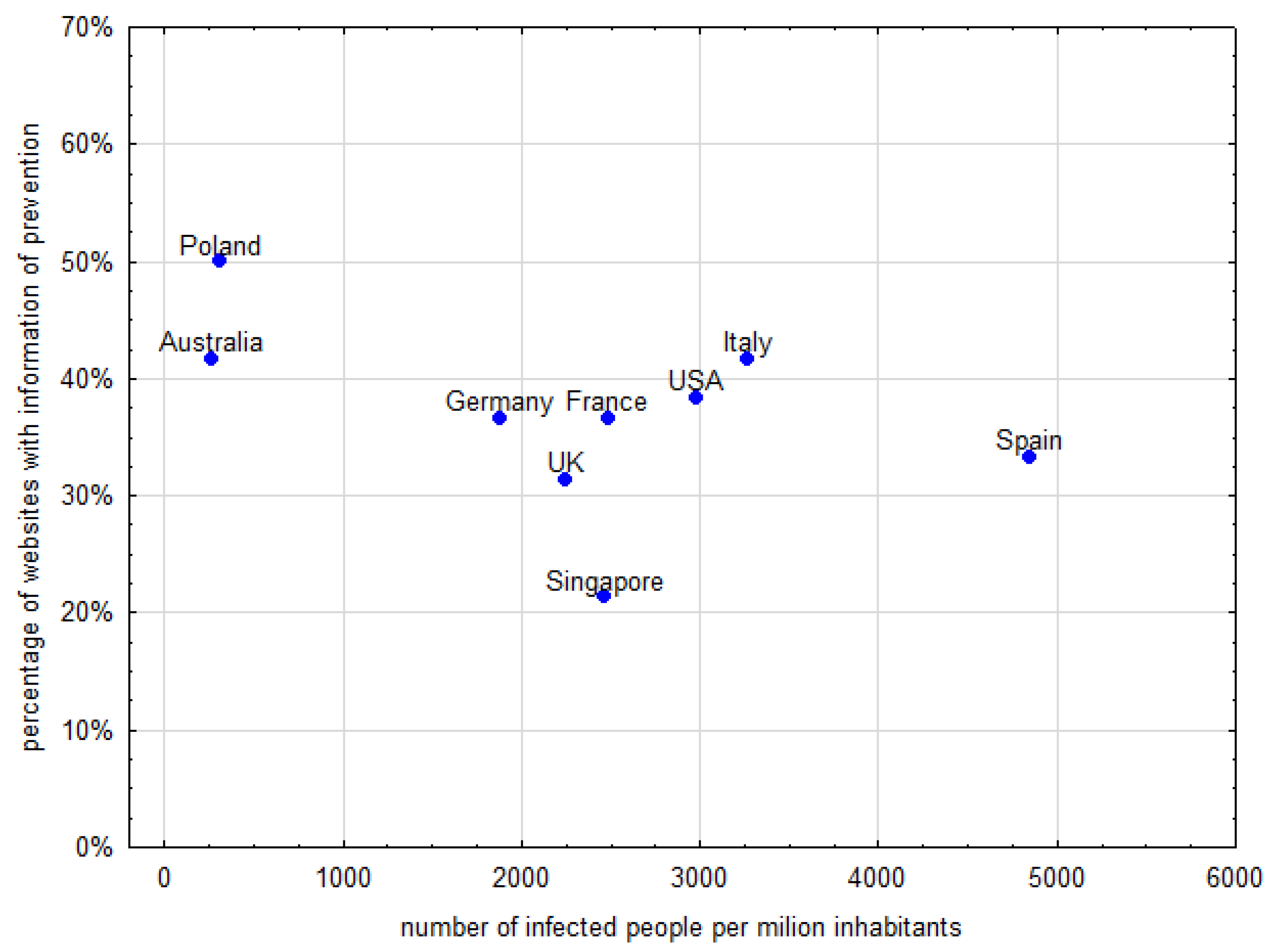
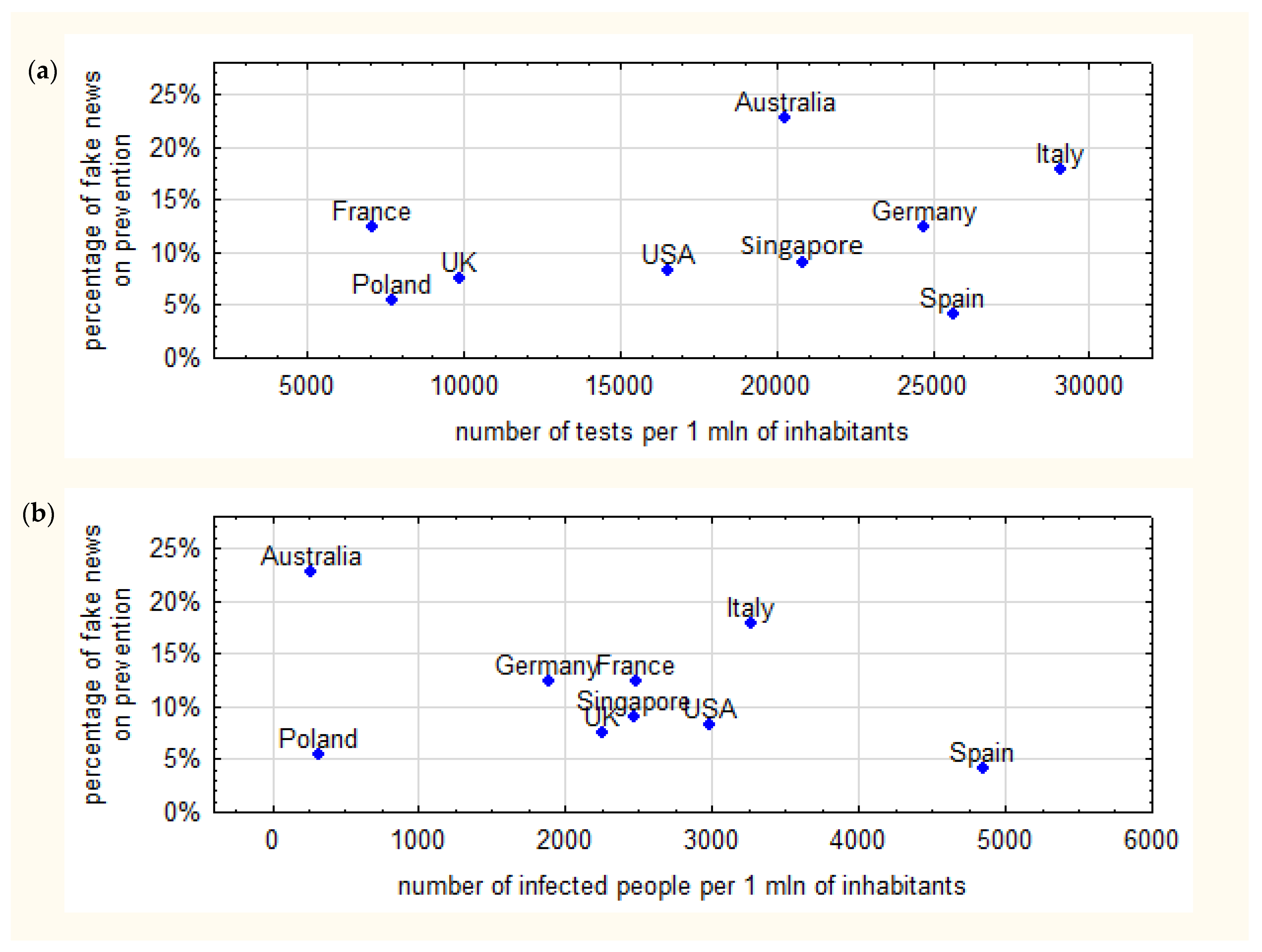
3.5. Analysis of Associations between Results and Epidemiological Data on COVID-19
3.6. Characterization and Analysis of Online Information Returned by Google Based on the “COVID-19”, “Coronavirus”, “SARS-CoV-2” and “Fake News” Keywords about Celebrities, Religion and Testimonials
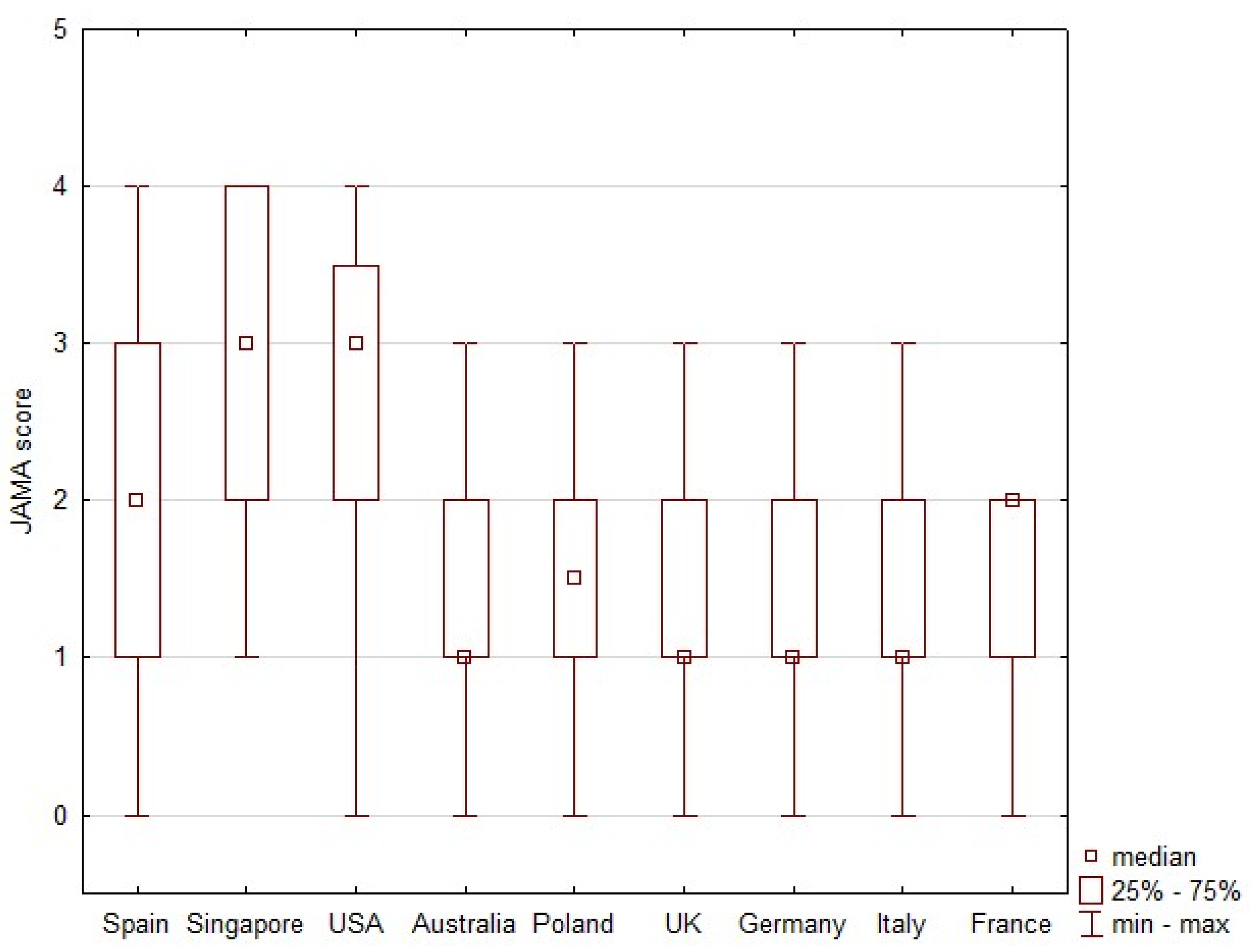
3.7. JAMA Score
4. Discussion
4.1. Characterization and Analysis f Websites Typology by Google Based on the “COVID-19”, “Coronavirus”, “SARS-CoV-2” and “Fake News” Keywords
4.2. Characterization and Analysis of Online Information Returned by Google Based on the “COVID-19”, “Coronavirus” and “SARS-CoV-2” Keywords
4.3. Characterization and Analysis of the Online Information Returned by Google Based on the “Fake News” Keywords
4.4. Frequency of Fake News on Webpages from the “COVID-19”, “Coronavirus”, “SARS-CoV-2” Keyword Searches
4.5. Analysis of Associations between Results and Epidemiological Data on COVID-19
4.6. Practical Implications and Future Research
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| C | Commercial |
| CDC | Centers for Disease Control and Prevention |
| CFR | Case Fatality Ratio |
| G | Government |
| GIS | Chief Sanitary Inspectorate “Główny Inspektorat Sanitarny” |
| HP | Health Portal |
| MZ | Ministry of Health “Ministerstwo Zdrowia” |
| N | News |
| NHS | National Health Service |
| NP | Non-Profit |
| SERP | search engine result page |
| SJ | Scientific journal |
| P | Professional |
| WHO | World Health Organization |
References
- Lazer, D.M.J.; Baum, M.A.; Benkler, Y.; Berinsky, A.J.; Greenhill, K.M.; Menczer, F.; Metzger, M.J.; Nyhan, B.; Pennycook, G.; Rothschild, D.; et al. The science of fake news. Science 2018, 359, 1094–1096. [Google Scholar] [CrossRef] [PubMed]
- Mann, D.L. Fake news, alternative facts, and things that just are not true can science survive the post-truth era? JACC Basic Transl. Sci. 2018, 3, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Bhansali, R.; Schaposnik, L.P. A trust model for spreading gossip in social networks: A multi-type bootstrap percolation model. Proc. Math. Phys. Eng. Sci. 2020, 476, 20190826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J.; Howland, B.; Mobius, M.; Rothschild, D.; Watts, D.J. Evaluating the fake news problem at the scale of the information ecosystem. Sci. Adv. 2020, 6, eaay3539. [Google Scholar] [CrossRef] [Green Version]
- Lara-Navarra, P.; Falciani, H.; Sánchez-Pérez, E.A.; Ferrer-Sapena, A. Information Management in Healthcare and Environment: Towards an Automatic System for Fake News Detection. Int. J. Environ. Res. Public Health 2020, 17, 1066. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, C.; Murphy, M. Going viral: Doctors must tackle fake news in the covid-19 pandemic. BMJ 2020, 369, m1587. [Google Scholar] [CrossRef]
- Arif, N.; Al-Jefri, M.; Bizzi, I.H.; Perano, G.B.; Goldman, M.; Haq, I.; Chua, K.L.; Mengozzi, M.; Neunez, M.; Smith, H.; et al. Fake News or Weak Science? Visibility and Characterization of Antivaccine Webpages Returned by Google in Different Languages and Countries. Front. Immunol. 2018, 9, 1215. [Google Scholar] [CrossRef] [Green Version]
- Carrieri, V.; Madio, L.; Principe, F. Vaccine hesitancy and (fake) news: Quasi-experimental evidence from Italy. Health Econ. 2019, 28, 1377–1382. [Google Scholar] [CrossRef]
- Dias da Silva, M.A.; Walmsley, A.D. Fake news and dental education. Br. Dent. J. 2019, 226, 397–399. [Google Scholar] [CrossRef] [Green Version]
- Vitale, F.; Misseri, G.; Ingoglia, G.; Bonanno, G.; Gregoretti, C.; Giarratano, A.; Cortegiani, A. Fake news and patient-family-physician interaction in critical care: Concepts, beliefs and potential countermeasures. Anestezjol. Intensywna Ter. 2020, 52, 42–46. [Google Scholar] [CrossRef]
- Worldometers.info. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 27 April 2020).
- Ghani, A.C.; Donnelly, C.A.; Cox, D.R.; Griffin, J.T.; Fraser, C.; Lam, T.H.; Ho, L.M.; Chan, W.S.; Anderson, R.M.; Hedley, A.J.; et al. Methods for Estimating the Case Fatality Ratio for a Novel, Emerging Infectious Disease. Am. J. Epidemiol. 2005, 162, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Own Calculations Based on Data on COVID-19 (Coronavirus) by Our World in Data. Available online: https://github.com/owid/covid-19-data/blob/master/public/data/README.md (accessed on 27 April 2020).
- Abd-Alrazaq, A.; Alhuwail, D.; Househ, M.; Hamdi, M.; Shah, Z. Top Concerns of Tweeters During the COVID-19 Pandemic: Infoveillance Study. J. Med. Internet Res. 2020, 22, e19016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Advice for the Public: Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 10 October 2021).
- Moscadelli, A.; Albora, G.; Biamonte, M.A.; Giorgetti, D.; Innocenzio, M.; Paoli, S.; Lorini, C.; Bonanni, P.; Bonaccorsi, G. Fake News and Covid-19 in Italy: Results of a Quantitative Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 5850. [Google Scholar] [CrossRef] [PubMed]
- WHO. Novel Coronavirus (2019-nCoV) Situation Report—1; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf?sfvrsn=20a99c10_4 (accessed on 27 April 2020).
- WHO. Novel Coronavirus(2019-nCoV) Situation Report—11; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200131-sitrep-11-ncov.pdf?sfvrsn=de7c0f7_4 (accessed on 27 April 2020).
- WHO. Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 27 April 2020).
- WHO. Classifications. Emergency Use ICD Codes for COVID-19 Disease Outbreak. Available online: https://www.who.int/classifications/icd/covid19/en/ (accessed on 27 April 2020).
- WHO. International Guidelines for Certification and Classification (Coding) of Covid-19 as Cause of Death Based on ICD International Statistical Classification of Diseases; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/classifications/icd/Guidelines_Cause_of_Death_COVID-19.pdf (accessed on 27 April 2020).
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report—51; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed on 27 April 2020).
- WHO. Novel Coronavirus(2019-nCoV) Situation Report—13; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200202-sitrep-13-ncov-v3.pdf (accessed on 27 April 2020).
- Hua, J.; Shaw, R. Corona Virus (COVID-19) “Infodemic” and Emerging Issues through a Data Lens: The Case of China. Int. J. Environ. Res. Public Health 2020, 17, 2309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunther, E. Infodemiology: Tracking Flu-Related Searches on the Web for Syndromic Surveillance. AMIA Annu. Symp. Proc. 2006, 2006, 244–248. [Google Scholar]
- Gunther, E. Infodemiology and Infoveillance: Framework for an Emerging Set of Public Health Informatics Methods to Analyze Search, Communication and Publication Behavior on the Internet. J. Med. Internet Res. 2009, 11, e11. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Olkun, H.K.; Demirkaya, A.A. Evaluation of Internet Information about Lingual Orthodontics Using DISCERN and JAMA Tools. Turk. J. Orthod. 2018, 31, 50–54. [Google Scholar] [CrossRef]
- Husnayain, A.; Shim, E.; Fuad, A.; Su, E.C. Understanding the Community Risk Perceptions of the COVID-19 Outbreak in South Korea: Infodemiology Study. J. Med. Internet Res. 2020, 22, e19788. [Google Scholar] [CrossRef]
- Badell-Grau, R.A.; Cuff, J.P.; Kelly, B.P.; Waller-Evans, H.; Lloyd-Evans, E. Investigating the Prevalence of Reactive Online Searching in the COVID-19 Pandemic: Infoveillance Study. J. Med. Internet Res. 2020, 22, e19791. [Google Scholar] [CrossRef]
- Lee, J.; Kwan, Y.; Lee, J.Y.; Shin, J.I.; Lee, K.H.; Hong, S.H.; Han, Y.J.; Kronbichler, A.; Smith, L.; Koyanagi, A.; et al. Public Interest in Immunity and the Justification for Intervention in the Early Stages of the COVID-19 Pandemic: Analysis of Google Trends Data. J. Med. Internet Res. 2021, 18, e26368. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Vidal-Alaball, J.; Downing, J.; Lopez Seguí, F. Dangerous Messages or Satire? Analysing the Conspiracy Theory Linking 5G to COVID-19 through Social Network Analysis. J. Med. Internet Res. 2020, 22, e19458. [Google Scholar] [CrossRef] [PubMed]
- Okan, O.; Bollweg, T.M.; Berens, E.-M.; Hurrelmann, K.; Bauer, U.; Schaeffer, D. Coronavirus-Related Health Literacy: A Cross-Sectional Study in Adults during the COVID-19 Infodemic in Germany. Int. J. Environ. Res. Public Health 2020, 17, 5503. [Google Scholar] [CrossRef] [PubMed]
- Rovetta, A.; Bhagavathula, A.S. COVID-19-Related Web Search Behaviors and Infodemic Attitudes in Italy: Infodemiological Study. JMIR Public Health Surveill. 2020, 6, e19374. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease (COVID-19) Advice for the Public: Myth Busters; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters (accessed on 27 April 2020).
- Haddad, M.P. Coronavirus: Comment le Gouvernement et les Réseaux Sociaux Luttent Contre les “Fake News”. RTL. 11 March 2020. Available online: https://www.rtl.fr/actu/politique/coronavirus-comment-le-gouvernement-et-les-reseaux-sociaux-luttent-contre-les-fake-news-7800193222 (accessed on 27 April 2020).
- Li, H.O.; Bailey, A.; Huynh, D.; Chan, J. YouTube as a source of information on COVID-19: A pandemic of misinformation? BMJ Glob. Health 2020, 5, e002604. [Google Scholar] [CrossRef]
- Huynh Dagher, S.; Lamé, G.; Hubiche, T.; Ezzedine, K.; Duong, T.A. The Influence of Media Coverage and Governmental Policies on Google Queries Related to COVID-19 Cutaneous Symptoms: Infodemiology Study. JMIR Public Health Surveill. 2021, 7, e25651. [Google Scholar] [CrossRef]
- Zeng, K.; Bernardo, S.N.; Havins, W.E. The Use of Digital Tools to Mitigate the COVID-1 Pandemic: Comparative Retrospective Study of Six Countries. JMIR Public Health Surveill. 2020, 6, e24598. [Google Scholar] [CrossRef]
- European Commission. A Multi-Dimensional Approach to Disinformation. Report of the Independent High Level Group on Fake News and Online Disinformation. Bruxelles. 11 March 2020. Available online: https://ec.europa.eu/digital-single-market/en/news/final-report-high-level-expert-group-fake-news-and-online-disinformation (accessed on 27 April 2020).
- House of Commons. Disinformation and ‘Fake News’: Interim Report. Digital, Culture, Media and Sport Committee, 29 July 2018. Available online: https://publications.parliament.uk/pa/cm201719/cmselect/cmcumeds/363/363.pdf (accessed on 27 April 2020).
- UK Parliament. Parliamentarians from Across the World Sign Declaration on the ‘Principles of the Law Governing the Internet’. London. 27 November 2018. Available online: https://www.parliament.uk/business/committees/committees-a-z/commons-select/digital-culture-media-and-sport-committee/news/declaration-internet-17-19/ (accessed on 27 April 2020).
- Republic of Singapore Government Gazette Acts Supplement. Protection from Online Falsehoods and Manipulation Act 2019 (No. 18 of 2019). Singapore; 3 June 2019. Available online: https://sso.agc.gov.sg/Act/POFMA2019?TransactionDate=20191001235959 (accessed on 27 April 2020).
- Hernández-García, I.; Giménez-Júlvez, T. Assessment of Health Information About COVID-19 Prevention on the Internet: Infodemiological Study. JMIR Public Health Surveill. 2020, 6, e18717. [Google Scholar] [CrossRef] [Green Version]
- Park, H.W.; Park, S.; Chong, M. An Infodemiological Study on Novel Coronavirus (COVID-19) in South Korea: Conversations and Medical News Frames on Twitter. J. Med. Internet Res. 2020, 22, e18897. [Google Scholar] [CrossRef]
- Tapia, L. Novel Coronavirus Disease (COVID-19) and Fake News in the Dominican Republic. Am. J. Trop. Med. Hyg. 2020, 102, 1172–1174. [Google Scholar] [CrossRef]
- Shimizu, K. 2019-nCoV, fake news, and racism. Lancet 2020, 395, 685–686. [Google Scholar] [CrossRef]
- Orso, D.; Federici, N.; Copetti, R.; Vetrugno, L.; Bove, T. Infodemic and the spread of fake news in the COVID-19-era. Eur. J. Emerg. Med. 2020, 27, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B.; White, K.; West, J.; Criezis, M.; Zhou, C.; Bartholomew, S. Cultural Variance in Reception and Interpretation of Social Media COVID-19 Disinformation in French-Speaking Regions. Int. J. Environ. Res. Public Health 2021, 18, 12624. [Google Scholar] [CrossRef] [PubMed]
- iProspect Search Engine User Behaviour Study. 2006. Available online: http://district4.extension.ifas.ufl.edu/Tech/TechPubs/WhitePaper_2006_SearchEngineUserBehavior.pdf (accessed on 8 January 2022).
- Szmuda, T.; Özdemir, C.; Ali, S.; Singh, A.; Syed, M.T.; Słoniewski, P. Readability of online patient education material for the novel coronavirus disease (COVID-19): A cross-sectional health literacy study. Public Health 2020, 185, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Rodrıguez, M.; Llorca, J. Bias. J. Epidemiol. Community Health 2004, 58, 635–641. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Li, H.; Farnoush, A.; Jiang, W. Understanding patterns of COVID infodemic: A systematic and pragmatic approach to curb fake news. J. Bus. Res. 2022, 140, 670–683. [Google Scholar] [CrossRef]
- Isaakidou, M.; Diomidous, M. The Contribution of Informatics to Overcoming the Covid-19 Fake News Outbreak by Learning to Navigate the Infodemic. Stud. Health Technol. Inform. 2022, 289, 456–459. [Google Scholar] [CrossRef]
- Khan, S.; Hakak, S.; Deepa, N.; Prabadevi, B.; Dev, K.; Trelova, S.O. Detecting COVID-19-Related Fake News Using Feature Extraction. Front. Public Health 2022, 9, 788074. [Google Scholar] [CrossRef]
- Gisondi, M.A.; Barber, R.; Faust, J.S.; Raja, A.; Strehlow, M.; Westafer, L.; Gottlieb, M. A Deadly Infodemic: Social Media and the Power of COVID-19 Misinformation. J. Med. Internet Res. 2022. Advance online publication. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | “Key Word” | Government (G) | Health Portal (HP) | News (N) | Non-Profit (NP) | Professional (P) | Commercial (C) | Scientific Journal (SJ) | TOTAL SERP |
|---|---|---|---|---|---|---|---|---|---|
| Spain | COVID-19 | 7 | 0 | 5 | 2 | 4 | 2 | 0 | 20 |
| Coronavirus | 3 | 1 | 14 | 1 | 0 | 1 | 0 | 20 | |
| SARS-CoV-2 | 3 | 3 | 4 | 2 | 6 | 1 | 1 | 20 | |
| Fake news | 0 | 0 | 10 | 0 | 1 | 5 | 0 | 16 | |
| total | 13 | 4 | 33 | 5 | 11 | 9 | 1 | 76 | |
| Singapore | COVID-19 | 5 | 0 | 4 | 2 | 1 | 9 | 0 | 21 |
| Coronavirus | 2 | 0 | 12 | 2 | 1 | 2 | 1 | 20 | |
| SARS-CoV-2 | 2 | 1 | 0 | 0 | 0 | 6 | 11 | 20 | |
| Fake news | 0 | 0 | 14 | 3 | 0 | 3 | 0 | 20 | |
| total | 9 | 1 | 30 | 7 | 2 | 20 | 12 | 81 | |
| USA | COVID-19 | 11 | 0 | 2 | 2 | 1 | 4 | 0 | 20 |
| Coronavirus | 13 | 0 | 1 | 1 | 4 | 1 | 0 | 20 | |
| SARS-CoV-2 | 2 | 1 | 0 | 0 | 2 | 4 | 11 | 20 | |
| Fake news | 0 | 0 | 9 | 1 | 0 | 4 | 0 | 14 | |
| total | 26 | 1 | 12 | 4 | 7 | 13 | 11 | 74 | |
| Australia | COVID-19 | 15 | 0 | 4 | 0 | 1 | 0 | 0 | 20 |
| Coronavirus | 12 | 0 | 5 | 1 | 1 | 0 | 1 | 20 | |
| SARS-CoV-2 | 4 | 0 | 5 | 2 | 5 | 3 | 1 | 20 | |
| Fake news | 0 | 0 | 18 | 0 | 2 | 0 | 0 | 20 | |
| total | 31 | 0 | 32 | 3 | 9 | 3 | 2 | 80 | |
| Poland | COVID-19 | 4 | 3 | 10 | 0 | 0 | 3 | 0 | 20 |
| Coronavirus | 2 | 2 | 13 | 0 | 1 | 2 | 0 | 20 | |
| SARS-CoV-2 | 4 | 3 | 9 | 0 | 3 | 1 | 0 | 20 | |
| Fake news | 0 | 0 | 5 | 1 | 1 | 6 | 0 | 13 | |
| total | 10 | 8 | 37 | 1 | 5 | 12 | 0 | 73 | |
| UK | COVID-19 | 2 | 0 | 2 | 7 | 4 | 4 | 0 | 19 |
| Coronavirus | 2 | 0 | 14 | 0 | 2 | 1 | 1 | 20 | |
| SARS-CoV-2 | 1 | 2 | 0 | 0 | 1 | 3 | 5 | 12 | |
| Fake news | 0 | 0 | 8 | 1 | 0 | 1 | 0 | 10 | |
| total | 5 | 2 | 24 | 8 | 7 | 9 | 6 | 61 | |
| Germany | COVID-19 | 5 | 1 | 10 | 0 | 2 | 2 | 0 | 20 |
| Coronavirus | 0 | 0 | 18 | 0 | 2 | 0 | 0 | 20 | |
| SARS-CoV-2 | 5 | 0 | 4 | 0 | 11 | 0 | 0 | 20 | |
| Fake news | 1 | 0 | 19 | 0 | 0 | 0 | 0 | 20 | |
| total | 11 | 1 | 51 | 0 | 15 | 2 | 0 | 80 | |
| Italy | COVID-19 | 6 | 0 | 5 | 0 | 5 | 3 | 0 | 19 |
| Coronavirus | 6 | 0 | 12 | 0 | 1 | 1 | 0 | 20 | |
| SARS-CoV-2 | 2 | 0 | 11 | 0 | 7 | 0 | 1 | 21 | |
| Fake news | 1 | 0 | 18 | 1 | 0 | 0 | 0 | 20 | |
| total | 15 | 0 | 46 | 1 | 13 | 4 | 1 | 80 | |
| France | COVID-19 | 4 | 0 | 14 | 0 | 1 | 1 | 0 | 20 |
| Coronavirus | 3 | 0 | 16 | 0 | 1 | 0 | 0 | 20 | |
| SARS-CoV-2 | 4 | 0 | 9 | 2 | 4 | 0 | 1 | 20 | |
| Fake news | 0 | 0 | 20 | 0 | 0 | 0 | 0 | 20 | |
| total | 11 | 0 | 59 | 2 | 6 | 1 | 1 | 80 | |
| TOTAL N | 131 | 17 | 324 | 31 | 75 | 73 | 34 | 685 | |
| TOTAL % | 19% | 2% | 47% | 5% | 11% | 11% | 5% | 100% | |
| G | HP | N | NP | P | C | SJ | TOTAL | |
|---|---|---|---|---|---|---|---|---|
| Spain | 13 (22%) | 4 (7%) | 23 (38%) | 5 (8%) | 10 (17%) | 4 (7%) | 1 (2%) | 60 (100%) |
| Singapore | 9 (15%) | 1 (2%) | 16 (26%) | 4 (7%) | 2 (3%) | 17 (28%) | 12 (20%) | 61 (100%) |
| USA | 26 (43%) | 1 (2%) | 3 (5%) | 3 (5%) | 7 (12%) | 9 (15%) | 11 (18%) | 60 (100%) |
| Australia | 31 (52%) | 0 (0%) | 14 (23%) | 3 (5%) | 7 (12%) | 3 (5%) | 2 (3%) | 60 (100%) |
| Poland | 10 (17%) | 8 (13%) | 32 (53%) | 0 (0%) | 4 (7%) | 6 (10%) | 0 (0%) | 60 (100%) |
| UK | 5 (10%) | 2 (4%) | 16 (31%) | 7 (14%) | 7 (14%) | 8 (16%) | 6 (12%) | 51 (100%) |
| Germany | 10 (17%) | 1 (2%) | 32 (53%) | 0 (0%) | 15 (25%) | 2 (3%) | 0 (0%) | 60 (100%) |
| Italy | 14 (23%) | 0 (0%) | 28 (40%) | 0 (0%) | 13 (22%) | 4 (7%) | 1 (2%) | 60 (100%) |
| France | 11 (18%) | 0 (0%) | 39 (65%) | 2 (3%) | 6 (10%) | 1 (2%) | 1 (2%) | 60 (100%) |
| Fake News Topic | Spain | Singapore | USA | Australia | Poland | UK | Germany | Italy | France | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Coronavirus developed by humans (e.g., in Wuhan, in the Pasteir Instutute in France, by Americans) | 3 | 3 | 5 | 5 | 3 | 1 | 7 | 3 | 11 | 41 | 9% |
| “Miraculous” ways of prevention (e.g., Drinking alcohol or hot water every 15 min, heroin intake, drinking bleach, vitamin C, holding breath) | 6 | 13 | 12 | 33 | 8 | 11 | 18 | 26 | 18 | 145 | 32% |
| Spread of the virus (e.g., Home animals, mosquitos, wrappings, distance between people, deliveries from China) | - | 2 | - | 12 | 5 | 1 | 2 | 12 | 5 | 39 | 9% |
| Underestimating the virus (Coronavirus does not exist; just another flu) | - | 1 | 1 | 2 | 2 | - | 8 | 2 | - | 16 | 4% |
| “Harmful” technologies that favor the pandemic (5G) | - | 1 | 2 | 8 | 3 | 2 | 5 | 6 | 3 | 30 | 7% |
| Children, youth and black people are resistant to COVID-19 (disease attacks seniors only) | - | 1 | - | 3 | 1 | 1 | 1 | 2 | 1 | 10 | 2% |
| “Effective” treatment (e.g., antibiotics treatment) | 1 | 7 | 8 | 3 | 9 | - | 8 | 8 | 1 | 45 | 10% |
| Local sensations referring to the virus (e.g., swans in Venice, elephants in tea plantations) | 8 | 5 | 5 | 3 | 7 | 3 | 14 | 7 | 4 | 56 | 13% |
| Instructions on how to avoid the virus (e.g., Troops blocking cities, bodies in street, disinfection from air, quarantining politicians on an island) | 1 | 2 | 1 | - | - | - | - | - | - | 4 | 1% |
| Other (BCG vaccine protects against coronavirus, flu vaccines and other) | 3 | 1 | 14 | 6 | 7 | 3 | 11 | 8 | 9 | 62 | 14% |
| Total | 22 | 36 | 48 | 75 | 45 | 22 | 74 | 74 | 52 | 448 | 100% |
| Country | Example |
|---|---|
| Poland |
|
| Singapore |
|
| UK |
|
| USA |
|
| Spain |
|
| Germany |
|
| France |
|
| Italy |
|
| Australia |
|
| SERPs for the “COVID-19”, “Coronavirus”, “SARS-CoV-2” Keywords | ||
|---|---|---|
| Country | Type | Example |
| Poland | testimonial | “Jason Hargrove, a bus driver from Detroit, was irritated with passengers coughing all the time and posted a video in which he called for hygiene during the pandemic. He died 11 days later due to the coronavirus”. |
| Singapore | NA | |
| UK | testimonial | “A museum boss says he had hallucinations filled with “visions of snakes” after being struck down by coronavirus”. |
| USA | celebrity | “In London, British Prime Minister Boris Johnson has been moved into intensive care. The announcement came a day after he was admitted to a London hospital with what his office called “persistent symptoms of coronavirus””. |
| Spain | religion | “La peregrinación a La Meca —hach— es el viaje que deben emprender los fieles musulmanes al menos una vez en la vida. (…) Y de riesgo, sobre todo en tiempos del COVID-19. No hay sector inmune al coronavirus; el comercio, el deporte, la cultura e incluso la fe son víctimas del patógeno, que ya ha causado la cancelación del Carnaval de Venecia, las Fallas de Valencia y decenas de giras”. |
| Germany | testimonial | “Über seine persönliche Situation sagt der 40-Jährige im Interview mit spot on news: “Für mich ist es nicht so schlimm. Ich muss beim Einkaufen nicht zwangsläufig kommunizieren und sehe ja noch die Augen und die Augenbrauen. Das hilft. Bei anderen wichtigen Sachen, wie zum Beispiel beim Arzt, kann ich es aufschreiben”. Und was hält er von Mundschutzmasken mit Sichtfeld? “Im Krankenhaus würde ich mir wünschen, dass alle transparente Masken tragen. So kann man die Menschen lachen sehen-es ist wichtig, die Emotionen weiterhin zu sehen””. |
| France | testimonial | “« On a arrêté de travailler pour respecter la discipline du confinement, alors qu’on doit manger et nourrir nos enfants, explique le père de famille âgé de 30 ans. Pour moi, c’était être indiscipliné ou partir. » Alors avant l’aube, il a pris ses deux enfants et un vélo chargé de maigres bagages pour rejoindre la ville d’Antsirabe, sa femme et le reste de sa famille, à plus de 150 kilomètres et trois jours de marche de là”. |
| celebrity | “« Ça n’a jamais été dans mon tempérament de pousser des coups de gueule, j’ai plutôt tendance à prendre le temps de discuter, d’expliquer les choses avec pédagogie. Mais, cette fois, je me suis rendu compte qu’on avait un poids trop faible, j’étais obligé de réagir. » C’est sur les réseaux sociaux, qu’ Arnaud Assoumani, multimédaillé paralympique au saut en longueur et au triple saut, a finalement manifesté son ras-le-bol après le report des Jeux olympiques de Tokyo en raison de l’épidémie de coronavirus”. | |
| celebrity | “Un exercice facile à réaliser et, qui selon Sharon Stone, peut être utile pour se protéger des maladies”. “Cela permet à la cage thoracique de s’étirer à leur capacité maximale pour vous rendre plus forts. Alors je veux que vous fassiez ça pour renforcer vos poumons, vos côtes pour être prêt à affronter ce qu’il faudrait”, a-t-elle déclaré”. | |
| Italy | testimonial | “Per lo Stato sono classificati come ‘microimpresa’, ma per i bambini sono una seconda casa. Eppure questi luoghi colorati, pieni di disegni appesi alle pareti, dove migliaia di piccoli hanno mosso i primi passi, e grazie ai quali altrettante mamme hanno potuto dedicarsi al proprio lavoro, rischiano di non riaprire quando l’emergenza Covid19 sarà rientrata”. |
| testimonial | “«Ma 102 anni sono pochi, posso prestargliene qualcuno, anzi no meglio che ognuno si tenga suoi» scherza al telefono. «Ne ho vissute tante, sì. Ho visto la guerra e i tedeschi fare del male, c’era la paura». E il coronavirus? «Ne ho viste così tante che di questo coronavirus quasi non me ne sono accorta. Prima facevo la postina a Bergamo, poi qui andavo a fregare i pavimenti, facevo le pulizie nelle case. Ho sempre lavorato”. | |
| celebrity | “Nel Regno Unito intanto il premier Boris Johnson—risultato positivo—è stato ricoverato e il Times scrive che in ospedale ha ricevuto ossigeno. Ieri sera la Regina Elisabetta ha parlato alla nazione: un evento raro, capitato solo 4 volte in 68 anni di regno”. | |
| Australia | celebrity | “’The Prime Minister has been moved this evening from intensive care back to the ward, where he will receive close monitoring during the early phase of his recovery’, a Downing Street spokesman said today”. |
| SERP for the “Fake News” Key Word | ||
| Country | Type | Example |
| Poland | NA | |
| Singapore | testimonial | “Coronavirus fake news: Kenyan woman ‘killed off’ by false WhatsApp rumour. WhatsApp message (…) give information about the death of Uganda’s fourth coronavirus victim, but the picture used in the post was of Elsie, a Kenyan woman living in London”. |
| celebrity | “Cristiano Ronaldo and the pope tested positive”. | |
| UK | celebrity | “Fans who believed Ronaldo to be sick might still have been thrilled to shake his hand; and no one is besieging virology labs to demand the truth”. |
| USA | NA | |
| Spain | NA | |
| Germany | religion | “Da es vermehrt zu Fake-News zu diesem Thema kam, noch einmal deutlich: Der Veranstalter hat der Stadt #Dortmund schon vor einiger Zeit mitgeteilt, dass die Veranstaltung Festi Ramazan 2020 in den @Westfalenhallen nicht stattfindet”. |
| France | celebrity | ““L’intégralité des cours manqués à cause du COVID-19 seront donc rattrapés pendant les vacances d’été”. La nouvelle est apparue sous la forme d’une capture d’écran d’un prétendu tweet d’Emmanuel Macron. Il s’agit évidemment d’un faux, puisque le compte à l’origine de la publication est @EmmanuelMecron” |
| Italy | NA | |
| Australia | religion | “Chinese people are not converting to Islam because of the outbreak”. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kłak, A.; Grygielska, J.; Mańczak, M.; Ejchman-Pac, E.; Owoc, J.; Religioni, U.; Olszewski, R. Online Information of COVID-19: Visibility and Characterization of Highest Positioned Websites by Google between March and April 2020—A Cross-Country Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1491. https://doi.org/10.3390/ijerph19031491
Kłak A, Grygielska J, Mańczak M, Ejchman-Pac E, Owoc J, Religioni U, Olszewski R. Online Information of COVID-19: Visibility and Characterization of Highest Positioned Websites by Google between March and April 2020—A Cross-Country Analysis. International Journal of Environmental Research and Public Health. 2022; 19(3):1491. https://doi.org/10.3390/ijerph19031491
Chicago/Turabian StyleKłak, Anna, Jolanta Grygielska, Małgorzata Mańczak, Ewelina Ejchman-Pac, Jakub Owoc, Urszula Religioni, and Robert Olszewski. 2022. "Online Information of COVID-19: Visibility and Characterization of Highest Positioned Websites by Google between March and April 2020—A Cross-Country Analysis" International Journal of Environmental Research and Public Health 19, no. 3: 1491. https://doi.org/10.3390/ijerph19031491
APA StyleKłak, A., Grygielska, J., Mańczak, M., Ejchman-Pac, E., Owoc, J., Religioni, U., & Olszewski, R. (2022). Online Information of COVID-19: Visibility and Characterization of Highest Positioned Websites by Google between March and April 2020—A Cross-Country Analysis. International Journal of Environmental Research and Public Health, 19(3), 1491. https://doi.org/10.3390/ijerph19031491