Energy Drink Consumption, Depression, and Salutogenic Sense of Coherence Among Adolescents and Young Adults

Abstract
1. Introduction
2. Methods
2.1. Participants and Procedure
2.2. Measurements
2.3. Sense of Coherence
2.4. Beck Depression Inventory
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Sample Characteristics
3.2. Motivations for Energy Drink Consumption
3.3. Energy Drink Consumption and Simultaneous Use with Alcohol
3.4. Side Effects of Energy Drink Consumption
3.5. Multivariate Analysis of Factors Leading to Energy Drink (ED) Addiction 1
3.6. Multivariate Analysis of Variables Leading to ED Addiction 2
4. Discussion
5. Conclusions
6. Strengths and Limitations of the Study
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Alsunni, A.A.E. Energy Drink Consumption: Beneficial and Adverse Health Effects. Int. J. Health Sci. 2015, 9, 468–474. [Google Scholar] [CrossRef]
- Alford, C.; Cox, H.; Wescott, R. The effects of red bull energy drink on human performance and mood. Amino Acids 2001, 21, 139–150. [Google Scholar] [CrossRef]
- Seidl, R.; Peyrl, A.; Nicham, R.; Hauser, E. A taurine and caffeine-containing drink stimulates cognitive performance and well-being. Amino Acids 2000, 19, 635–642. [Google Scholar] [CrossRef]
- Campbell, B.; Wilborn, C.; La Bounty, P.; Taylor, L.; Nelson, M.; Greenwood, M.; Ziegenfuss, T.; Lopez, H.; Hoffman, J.; Stout, J.; et al. International Society of Sports Nutrition position stand: Energy drinks. JISSN 2013, 10, 1. [Google Scholar] [CrossRef]
- Kammerer, M.; Jaramillo, J.A.; García, A.; Calderín, J.C.; Luis, H.; Valbuena, L.H. Effects of energy drink major bioactive compounds on the performance of young adults in fitness and cognitive tests: A randomized controlled trial. JISSN 2014, 11, 44. [Google Scholar] [CrossRef]
- Higgins, J.P.; Ortiz, B.L. Energy drink ingredients and their effect on endothelial function: A Review. IJCCR 2014, 1, 1–6. [Google Scholar] [CrossRef]
- Scholey, A.; Kennedy, D. Cognitive and physiological effects of an „energy drink”: An evaluation of the whole drink and of glucose, caffeine and herbal flavouring fractions. Psychopharmacology 2004, 176, 320–330. [Google Scholar] [CrossRef]
- Geiß, K.; Jester, I.; Falke, W.; Hamm, M.; Waag, K. The effect of a taurine containing drink on performance in 10 endurance-athletes. Amino Acids 1994, 7, 45–56. [Google Scholar] [CrossRef]
- Beckford, K.; Grimes, C.A.; Riddell, L.J. Australian children’s consumption of caffeinated, formulated beverages: A cross-sectional analysis. BMC Public Health 2015, 15, 70. [Google Scholar] [CrossRef]
- Visram, S.; Cheetham, M.; Riby, D.M.; Stephen, J.; Crossley, S.J.; Lake, A.A. Consumption of energy drinks by children and young people: A rapid review examining evidence of physical effects and consumer attitudes. BMJ Open 2016, 6, e010380. [Google Scholar] [CrossRef]
- Terry-McElrath, Y.M.; O’Malley, P.M.; Johnston, L.D. Energy drinks, soft drinks, and substance use among United States secondary school students. JAM 2014, 8, 6–13. [Google Scholar] [CrossRef]
- Ruiz, L.D.; Scherr, R.E. Risk of Energy Drink Consumption to Adolescent Health. AJLM 2019, 13, 22–25. [Google Scholar] [CrossRef]
- Miller, K.E.; Dermen, K.H.; Lucke, J.F. Caffeinated energy drink use by U.S. adolescents aged 13–17: A national profile. Psychol. Addict. Behav. 2018, 32, 647–659. [Google Scholar] [CrossRef]
- Leal, W.E.; Jackson, D.B. Energy drinks and escalation in drug use severity: An emergent hazard to adolescent health. Prev. Med. 2018, 111, 391–396. [Google Scholar] [CrossRef]
- Schwartz, D.L.; Glistad-Hayden, K.; Caroll-Scott, A.; Grilo, S.A.; McCaslin, C.; Schwartz, M.; Ickovics, J.R. Energy drinks and youth self-reported hyperactivity/inattention symptoms. Acad. Pediatr. 2015, 15, 297–304. [Google Scholar] [CrossRef]
- Kristjansson, A.L.; Sigfusdottir, I.D.; Frost, S.S.; James, J.E. Adolescent caffeine consumption and self-reported violence and conduct disorder. JYA 2013, 42, 1053–1062. [Google Scholar] [CrossRef]
- Higgins, J.P.; Babu, K.M. Caffeine reduces myocardial blood flow during exercise. AJM 2013, 126, 730.e1–730.e8. [Google Scholar] [CrossRef]
- Wolk, B.J.; Ganetsky, M.; Babu, K.M. Toxicity of energy drinks. Curr. Opin. Pediatrics 2012, 24, 243–251. [Google Scholar] [CrossRef]
- Huhtinen, H.; Lindfors, P.; Rimpelä, A. Adolescents’ use of energy drinks and caffeine induced health complaints in Finland. EJPH 2013, 23 (Suppl. S1), 166. [Google Scholar] [CrossRef]
- Dörner, J. MRI tecnique shows how energy drinks alter hear function. Radiol. News Edu. 2013. Available online: www.auntminnie.com/Redirect/Redirect.aspx?ItemId=105781 (accessed on 26 November 2016).
- Kerrigan, S.; Lindsey, T. Fatal caffeine overdose: Two case reports. Forensic Sci. Int. 2005, 153, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Kristjansson, A.L.; Sigfusdottir, I.D.; Mann, M.J.; James, J.E. Caffeinated sugar-sweetened beverages and common physical complaints in Icelandic children aged 10–12 years. Prev. Med. 2014, 58, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Seifert, S.M.; Schaechter, J.L.; Hershorin, E.R.; Lipshultz, S.E. Health Effects of Energy Drinks on Children, Adolescents, and Young Adults. Pediatrics 2011, 127, 511–528. [Google Scholar] [CrossRef]
- Nordt, S.P.; Vilke, G.M.; Clark, R.F.; Lee Cantrell, F.; Chan, T.C.; Galinato, M.; Nguyen, V.; Castillo, E.M. Energy drink use and adverse effects among emergency department patients. JCH 2012, 37, 976–981. [Google Scholar] [CrossRef]
- Verster, J.C.; Benjaminsen, J.M.; van Lanen, J.H.; van Stavel, N.M.; Olivier, B. Effects of mixing alcohol with energy drink on objective and subjective intoxication: Results from a Dutch on-premise study. Psychopharmacology 2015, 232, 835–842. [Google Scholar] [CrossRef]
- Bonar, E.E.; Cunningham, R.M.; Polshkova, S.; Chermack, S.T.; Blow, F.C.; Walton, M.A. Alcohol and energy drink use among adolescents seeking emergency department care. Addict. Behav. 2015, 43, 11–17. [Google Scholar] [CrossRef]
- Scalese, M.; Denoth, F.; Siciliano, V.; Bastiani, L.; Cotichini, R.; Cutilli, A.; Molinaro, S. Energy Drink and Alcohol mixed Energy Drink use among high school adolescents: Association with risk taking behavior, social characteristics. Addict. Behav. 2017, 72, 93–99. [Google Scholar] [CrossRef]
- Miller, K.E. Energy Drinks, Race, and Problem Behaviors among College Students. J. Adolesc. Health 2008, 43, 490–497. [Google Scholar] [CrossRef]
- Rossheim, M.E.; Thombs, D.L.; Weiler, R.M.; Barry, A.E.; Suzuki, S.; Walters, S.T.; Barnett, T.E.; Paxton, R.J.; Pealer, L.N.; Cannell, B. Alcohol mixed with energy drink: Use may be a consequence of heavy drinking. Addict. Behav. 2016, 57, 55–61. [Google Scholar] [CrossRef]
- Zucconi, S.; Volpatoa, C.; Adinofia, F.; Gandinia, E.; Gentileb, E.; Loib, A.; Fioritib, L. Gathering consumption data on specific consumer groups of energy drinks. Support. Publ. 2013, 10, 394. [Google Scholar] [CrossRef]
- Gradvohl, E.; Vida, K.; Rácz, J. Fill it up… Survey of the relationship between alcohol and energy drink consumption and risky behaviour among young adults. Hung. Med. J. 2015, 156, 1100–1108. [Google Scholar] [CrossRef]
- Soós, R.; Tékus, É.; Bodó, D.; Wilhelm, M. Side effects of energy drinks and caffeinated beverages. In Book of Abstracts of the 21st Annual Congress of the European College of Sport Science, Vienna, Austria, 6–9 June 2016; Baca, A., Wessner, B., Diketmüller, R., Tschan, H., Hofmann, M., Kornfeind, P., Tsolakidis, E., Eds.; European College of Sport Science: Vienna, Austria, 2016; ISBN 978-3-00-053383-9. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well, 1st ed.; Jossey-Bass: San Fransisco, CA, USA, 1987. [Google Scholar]
- Sipos, E.; Jeges, S.; Tóth, Á. Sport; Sense of Coherence, and Self-Esteem among 16 and 17-Years-Olds. EJMH 2015, 10, 62–78. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck depression inventory-II. San Antonio. 1996, 78, 490–498. [Google Scholar]
- Gareth, R.; Smith, A.P. A Review of Energy Drinks and Mental Health, with a Focus on Stress, Anxiety, and Depression. J. Caffeine Res. 2016, 6, 49–63. [Google Scholar] [CrossRef]
- Breda, J.J.; Whiting, S.H.; Encarnação, R.; Norberg, S.; Jones, R.; Reinap, M.; Jewell, J. Energy Drink Consumption in Europe: A Review of the Risks, Adverse Health Effects, and Policy Options to Respond. Front. Public Health 2014, 2, 134. [Google Scholar] [CrossRef]
- Friis, K.; Lyng, I.J.; Lasgaard, M.; Finn, B.; Larsen, F.B. Energy drink consumption and the relation to socio-demographic factors and health behaviour among young adults in Denmark. A population-based study. Eur. J. Public Health 2014, 24, 840–844. [Google Scholar] [CrossRef]
- Azagba, S.; Langille, D.; Asbridge, M. An emerging adolescent health risk: Caffeinated energy drink consumption patterns among high school students. Prev. Med. 2016, 62, 54–59. [Google Scholar] [CrossRef]
- Miyake, E.R.; Marmorstein, N.R. Energy drink consumption and later alcohol use among early adolescents. Addict. Behav. 2015, 43, 60–65. [Google Scholar] [CrossRef]
- Malinauskas, B.M.; Aeby, V.G.; Overton, R.F.; Carpenter-Aeby, T.; Barber-Heidal, K. A survey of energy drink comsumption patterns among college students. Nutr. J. 2007, 6. [Google Scholar] [CrossRef]
- Costa, B.M.; Hayley, A.; Miller, P. Young adolescents’ perceptions, patterns, and contexts of energy drink use. A focus group study. Appetite 2014, 80, 183–189. [Google Scholar] [CrossRef]
- Sagy, S.; Antonovsky, H. The development of the sense of coherence: A retrospective study of early life experiences in the family. Int. J. Aging Hum. Dev. 2000, 51, 155–166. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Male (n = 284) | Female (n = 347) | Statistics | Total (n = 631) | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p (U test) | Mean | SD | |
| Age | 19.5 | 2.0 | 19.2 | 2.0 | n.s. | 19.3 | 2.0 |
| Depression | 3.8 | 4.3 | 5.9 | 5.9 | <0.001 | 4.9 | 5.4 |
| Sense of coherence | 59.0 | 10.3 | 55.2 | 11.5 | <0.001 | 56.9 | 11.1 |
| Comprehensibility | 21.8 | 4.8 | 19.3 | 5.1 | <0.001 | 20.5 | 5.1 |
| Manageability | 18.4 | 4.2 | 17.1 | 4.3 | <0.001 | 17.7 | 4.3 |
| Meaningfulness | 18.7 | 4.2 | 18.8 | 4.2 | n.s. | 18.8 | 4.2 |
| Energy drink use | n | % | n | % | p (Wald stat.) | n | % |
| Does not consume energy drinks | 45 | 15.8 | 79 | 22.8 | --- | 124 | 19.7 |
| Very rare consumption | 118 | 41.5 | 193 | 55.6 | 0.748 | 311 | 49.3 |
| 1-2 times per month | 54 | 19.0 | 24 | 6.9 | 0.000 | 78 | 12.4 |
| 1-2 times per week | 34 | 12.0 | 31 | 8.9 | 0.035 | 65 | 10.3 |
| More than twice a week | 8 | 2.8 | 5 | 1.4 | 0.085 | 13 | 2.1 |
| Once a day | 13 | 4.6 | 9 | 2.6 | 0.049 | 22 | 3.5 |
| More than once a day | 12 | 4.2 | 6 | 1.7 | 0.019 | 18 | 2.9 |
| The following consume energy drinks regularly | p (chi2 test) | ||||||
| Parents (yes-no) | 57 | 20.1 | 49 | 14.1 | 0.047 | 106 | 16.8 |
| Sibling (yes-no) | 117 | 41.2 | 123 | 35.4 | n.s. | 240 | 38.0 |
| Friend/boyfriend/girlfriend (yes-no) | 149 | 52.5 | 220 | 63.4 | 0.006 | 369 | 58.5 |
| Availability of energy drinks at home | p (chi2 test) | ||||||
| Yes | 87 | 30.6 | 78 | 22.5 | n.s. | 165 | 26.1 |
| No | 193 | 68.0 | 264 | 76.1 | 457 | 72.4 | |
| Reasons for Energy Drink Consumption | Males (n = 121) | Females (n = 75) | p (chi2 Test) | ||
|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | ||
| For fun | 16.5 | 10.9–24.1 | 5.3 | 2.1–12.9 | 0.020 |
| Tastes good | 43.8 | 35.3–52.7 | 56.0 | 44.8–66.7 | ns |
| Stimulation | 16.5 | 10.9–24.1 | 18.7 | 11.5–28.9 | ns |
| Fatigue | 33.1 | 25.3–41.9 | 64.0 | 52.7–73.9 | <0.010 |
| Revs me up | 17.4 | 11.6–25.1 | 21.3 | 13.6–31.9 | ns |
| Quenches thirst | 11.6 | 7.0–18.5 | 12.0 | 6.4–21.3 | ns |
| Cool/trendy | 2.5 | 2.4–7.0 | 0.0 | 0.0–4.9 | ns |
| Enhanced performance | 12.4 | 7.7–19.4 | 6.7 | 2.9–14.7 | ns |
| Work-out | 11.6 | 7.0–18.5 | 2.7 | 0.7–9.2 | 0.027 |
| Which Adverse Effects Did You Experience Following Energy Drink Consumption? | Males (n = 121) | Females (n = 75) | p (chi2 Test) | ||
|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | ||
| Headache | 21.5 | 15.1–29.6 | 16.0 | 9.4–25.9 | ns |
| Nausea | 11.6 | 7.0–18.5 | 6.7 | 2.9–14.7 | ns |
| Weakness | 12.4 | 7.7–19.4 | 14.7 | 8.4–24.4 | ns |
| Tremors | 28.1 | 20.9–36.7 | 30.7 | 21.4–41.8 | ns |
| Dizziness | 8.3 | 4.6–14.6 | 13.3 | 7.4–22.8 | ns |
| Loss of consciousness | 2.5 | 0.9–7.0 | 0.0 | 0.0–4.9 | ns |
| Insomnia | 26.4 | 19.4–34.9 | 38.7 | 28.5–49.9 | ns |
| Irritability | 2.5 | 0.9–7.0 | 8.0 | 3.7–16.4 | ns |
| Tachycardia | 32.2 | 24.6–40.1 | 38.7 | 28.5–49.9 | ns |
| Breathlessness | 2.5 | 0.9–7.0 | 4.0 | 1.4–11.1 | ns |
| Fear | 0.8 | 0.2–4.5 | 8.0 | 3.7–16.4 | 0.013 |
| Diarrhea | 1.7 | 0.5–5.8 | 2.7 | 0.7–9.2 | ns |
| Model 1 | B | S.E. | Sig. | Exp(B) | ||
| Lower | Upper | |||||
| Sex | −0.745 | 0.228 | 0.001 | 0.475 | 0.304 | 0.743 |
| Age | −0.261 | 0.064 | 0.000 | 0.770 | 0.679 | 0.874 |
| Depression | 0.059 | 0.019 | 0.002 | 1.060 | 1.022 | 1.100 |
| Model 2 | B | S.E. | Sig. | Exp(B) | 95% C.I. for EXP(B) | |
| Lower | Upper | |||||
| Sex | −0.778 | 0.229 | 0.001 | 0.460 | 0.293 | 0.720 |
| Age | −0.242 | 0.065 | 0.000 | 0.785 | 0.692 | 0.891 |
| Sense of coherence_rev * | 0.037 | 1.402 | 0.000 | 1.037 | 1.017 | 1.058 |
| Model 3 | B | S.E. | Sig. | Exp(B) | 95% C.I. for EXP(B) | |
| Lower | Upper | |||||
| Sex | −1.232 | 0.206 | 0.000 | 0.292 | 0.195 | 0.437 |
| Age | −0.206 | 0.053 | 0.000 | 0.813 | 0.733 | 0.903 |
| Depression | 0.026 | 0.023 | 0.260 | 1.026 | 0.981 | 1.074 |
| Sense of coherence_rev * | 0.029 | 0.012 | 0.017 | 1.029 | 1.005 | 1.054 |
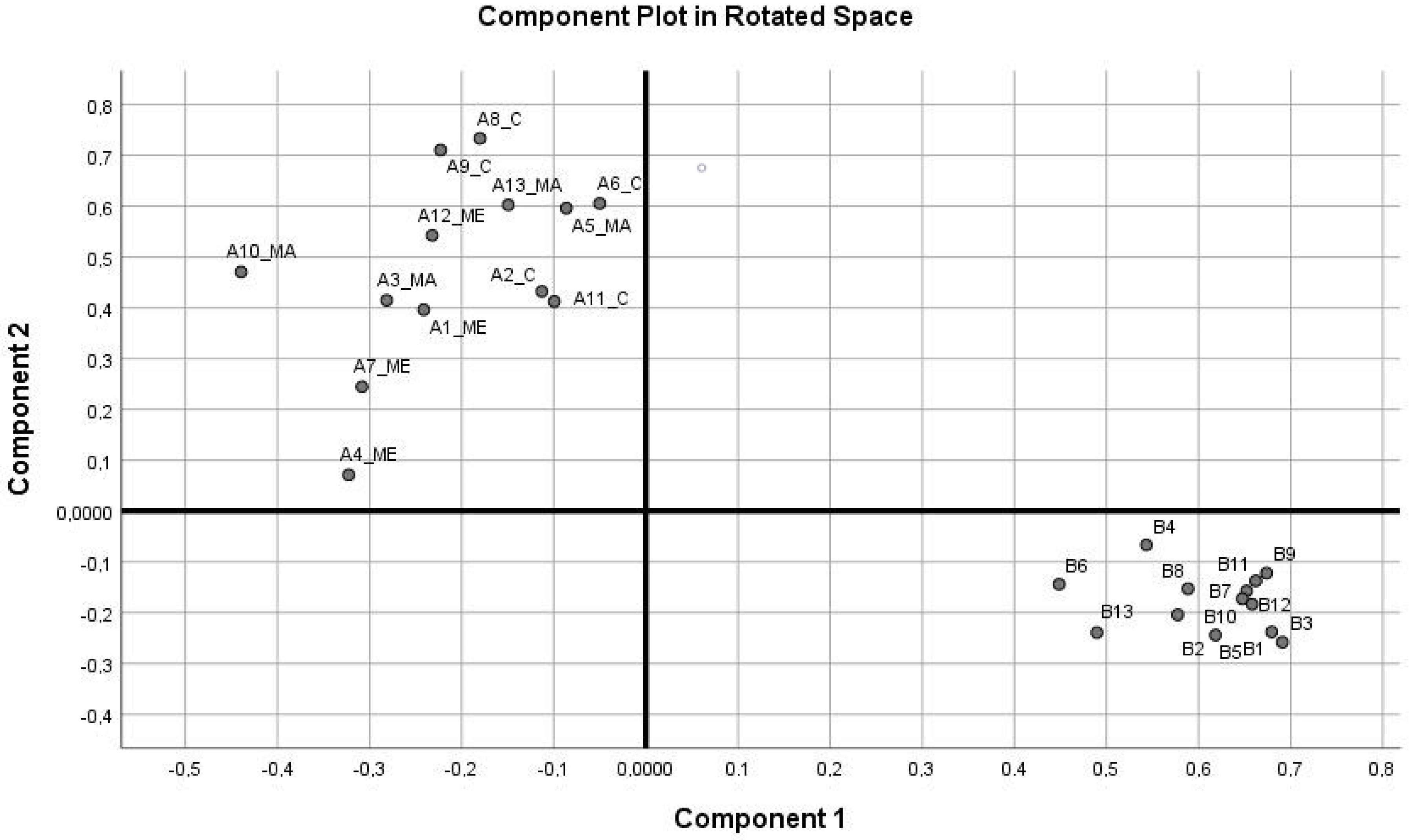
| Item with Factor Loadings > 0.600 | Component | |
|---|---|---|
| 1 | 2 | |
| B3 Past Failure | 0.691 | |
| B1 Sadness | 0.679 | |
| B9 Indecisiveness | 0.674 | |
| B11 Tiredness or Fatigue | 0.662 | |
| B12 Loss of Energy | 0.658 | |
| B7 Suicidal Thoughts or Wishes | 0.652 | |
| B10 Change in body image | 0.647 | |
| A8_C Do you have very mixed-up feelings and ideas? | 0.733 | |
| A9_C Does it happen that you have feelings inside you would rather not feel? | 0.710 | |
| A6_C Do you have the feeling that you’re being treated unfairly? | 0.605 | |
| A13_ME How often do you have feeling that you’re not sure you can keep under control? | 0.603 | |
| Variables | B | S.E. | Sig. | Exp(B) | 95% C.I. for Exp(B) | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Sex | −0.906 | 0.226 | 0.000 | 0.404 | 0.259 | 0.629 |
| Age | −0.270 | 0.065 | 0.000 | 0.763 | 0.672 | 0.866 |
| Dep-factor | 0.251 | 0.099 | 0.011 | 1.285 | 1.058 | 1.561 |
| SOC-factor_rev * | 0.333 | 0.109 | 0.002 | 1.395 | 1.127 | 1.726 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tóth, Á.; Soós, R.; Szovák, E.; M. Najbauer, N.; Tényi, D.; Csábí, G.; Wilhelm, M. Energy Drink Consumption, Depression, and Salutogenic Sense of Coherence Among Adolescents and Young Adults. Int. J. Environ. Res. Public Health 2020, 17, 1290. https://doi.org/10.3390/ijerph17041290
Tóth Á, Soós R, Szovák E, M. Najbauer N, Tényi D, Csábí G, Wilhelm M. Energy Drink Consumption, Depression, and Salutogenic Sense of Coherence Among Adolescents and Young Adults. International Journal of Environmental Research and Public Health. 2020; 17(4):1290. https://doi.org/10.3390/ijerph17041290
Chicago/Turabian StyleTóth, Ákos, Rita Soós, Etelka Szovák, Noemi M. Najbauer, Dalma Tényi, Györgyi Csábí, and Márta Wilhelm. 2020. "Energy Drink Consumption, Depression, and Salutogenic Sense of Coherence Among Adolescents and Young Adults" International Journal of Environmental Research and Public Health 17, no. 4: 1290. https://doi.org/10.3390/ijerph17041290
APA StyleTóth, Á., Soós, R., Szovák, E., M. Najbauer, N., Tényi, D., Csábí, G., & Wilhelm, M. (2020). Energy Drink Consumption, Depression, and Salutogenic Sense of Coherence Among Adolescents and Young Adults. International Journal of Environmental Research and Public Health, 17(4), 1290. https://doi.org/10.3390/ijerph17041290